
Abstract
Purpose:
Among cancer patients, social media (SM) significantly influences the adolescent and young adult (AYA) population, serving as both an information source and a communication tool.
Patients and Methods:
In this multicenter study conducted across French cancer care institutions, we investigated the impact of SM on AYA patients’ perception of their disease during treatment. Participants completed a 20-item self-administered questionnaire, and data were descriptively analyzed.
Results:
A total of 108 patients (aged 18–29 years) were enrolled from 10 French centers over a 5-month period. For 59% (n = 64) of patients, time spent on SM increased after diagnosis, mainly due to boredom during treatment. Thirty-three percent (n = 36) shared their personal story on SM, which had a predominantly positive impact (providing support, relief, and meaning), although some experienced increased feelings of loneliness. Seventy percent (n = 76) searched for information about their disease on SM, which led to both positive (receiving answers) and negative (increased anxiety) effects. Notably, 43% (n = 33) of these patients did not verify the information with health care professionals.
Conclusion:
In this study, all AYA patients reported daily use of SM. Their engagement with SM is multifaceted, and health care providers must remain vigilant about potential negative consequences, such as misinformation, social isolation, and addiction. AYA cancer patients represent a unique population with specific psychosocial needs requiring tailored attention.
Introduction
Every year in France, more than 2300 adolescents and young adults (AYAs) are diagnosed with a solid or hematological malignancy. 1 The 5-year survival rate of this specific population remains lower than that of children with the same cancers, underscoring the need for comprehensive improvements in both medical and psychosocial care. 2 Adolescence and young adulthood are periods marked by profound physical, emotional, and social transitions, which present unique challenges in the management of a serious illness such as cancer. 3 SM can deliver different kinds of social support (emotional support, informational support, and esteem support), types of support highly sought by AYA patients, and strengthen the notion that support from others (family, friends, colleagues, strangers) acts as a protective factor against stress, illness, and life difficulties (such as a cancer). 4
Concurrently, patients aged from 15 to 24 years spend an average of 3 hours per day on social media (SM), using platforms to share videos, communicate, and seek information. 5 Although several studies have explored SM use among AYA with cancer, reporting potential adverse effects such as depression, eating disorders, sleep disturbances, behavioral problems, and body image dissatisfaction, these findings should be interpreted with caution. 6 Most available studies are limited by small sample sizes, heterogeneous methodologies, and the absence of validated psychosocial outcome measures, making it difficult to draw firm conclusions. Furthermore, European data remain scarce, as the majority of studies have been conducted in North America, thereby limiting the generalizability of the results to other cultural and health care contexts. These disorders are commonly observed in the oncology setting and may be exacerbated by excessive or maladaptive SM use.
While SM often serves as a source of emotional refuge or a platform for seeking answers, it also raises new challenges regarding the physician–patient relationship and access to accurate medical information. 7 Caregivers have expressed concern about misinformation (“fake news”) encountered online, particularly regarding diagnoses and treatments. Despite growing interest in the influence of SM on young people, studies focusing on this topic remain limited—especially in the fields of oncology and hematology—and frequently involve small patient cohorts.8,9 Previous study including patients with sarcoma has shown that SM may heighten feelings of frustration, social exclusion, and psychological distress. 10
This study seeks to examine whether and how AYA patients and survivors of cancer (leukemia/lymphoma and solid tumors) use SM to obtain information about their disease and learn from others’ experiences. We explored both the positive (based on social support theory: listening, empathy, comfort, affection, encouragement, reinforcement of self-confidence) and negative aspects of this engagement to understand how virtual social relationships may influence physical and mental health, both of which are crucial to enduring demanding medical treatments. While the role of SM in supporting AYAs remains undefined and unregulated, it holds potential to enhance social support. Positive effects such as feeling “normal” and staying connected with peers are particularly meaningful during treatment and go beyond mere distraction. 11 This French study is original in that it includes both solid and hematological malignancies and examines not only the negative (drawbacks) but also the positive (benefits) impacts of SM use (such as Instagram, Facebook, Snapchat, and Twitter/X) among AYA patients and survivors, with the ultimate goal of better understanding and integrating their social experience into holistic medical care.
Patients and Methods
Between November 1, 2024, and March 31, 2025, a total of 108 patients were enrolled from 10 French cancer care institutions. These included the departments of medical oncology and hematology at the Strasbourg University Hospital and the Strasbourg Cancer Institute; the Nancy University Hospital and the Lorraine Cancer Institute; the Besançon University Hospital; and the François Baclesse Institute in Caen.
Participants were identified by the medical team at each participating center—either during active treatment or follow-up—and through each center’s internal databases, based on patient age, diagnosis, and treatment history. Eligible patients were approached consecutively by their health care providers (physicians or AYAs coordinating nurses) and invited to participate. In addition, participants were also recruited through a national patient association, where existing discussion and working groups are organized according to patient age, diagnosis, and duration of remission.
Inclusion criteria were as follows: adult patients aged from 18 to 29 years, either undergoing treatment or in remission (defined as within 5 years after treatment completion) for a hematological or a solid malignancy. While some patients were minors at the time of diagnosis and treatment, all were over 18 years old at the time of anonymous self-administered questionnaire completion.
An anonymous self-administered questionnaire was distributed to patients via mail by their health care providers (physicians or AYA coordinating nurses). It consisted of 20 items covering diagnosis, treatment, and the use and impact of SM. Patients were also given the opportunity to express themselves freely in an open-ended section at the end of the questionnaire regarding the study topic. The questionnaire was also disseminated through patient advocacy groups (AYA Academy, AIDA association), enabling participation from additional French health institutions within the GO-AJA (AYA onco-hematology group) network, including centers in six towns (Montpellier, Nimes, Paris, Perpignan, Rennes, Lyon). All responses were collected through a single online platform, ensuring uniform data collection and centralized management.
Categorical variables were summarized as frequencies and percentages. Comparisons between groups were performed using the chi-square test or Fisher’s exact test, as appropriate. Statistical analyses were conducted using SAS software (SAS Institute Inc., Cary, NC, USA). A p value <0.05 was considered statistically significant.
Ethics approval was not required for this noninterventional study. In accordance with applicable regulations, no informed consent was necessary, as the study was based on an anonymous self-administered questionnaire.
Results
Patients’ characteristics are summarized in Table 1. A total of 108 anonymous self-administered questionnaires were collected from November 1, 2024, to March 31, 2025 (51% and 49% from patients with solid and hematological malignancy, respectively), mainly during post-treatment follow-up (80%).
Characteristics of Patients
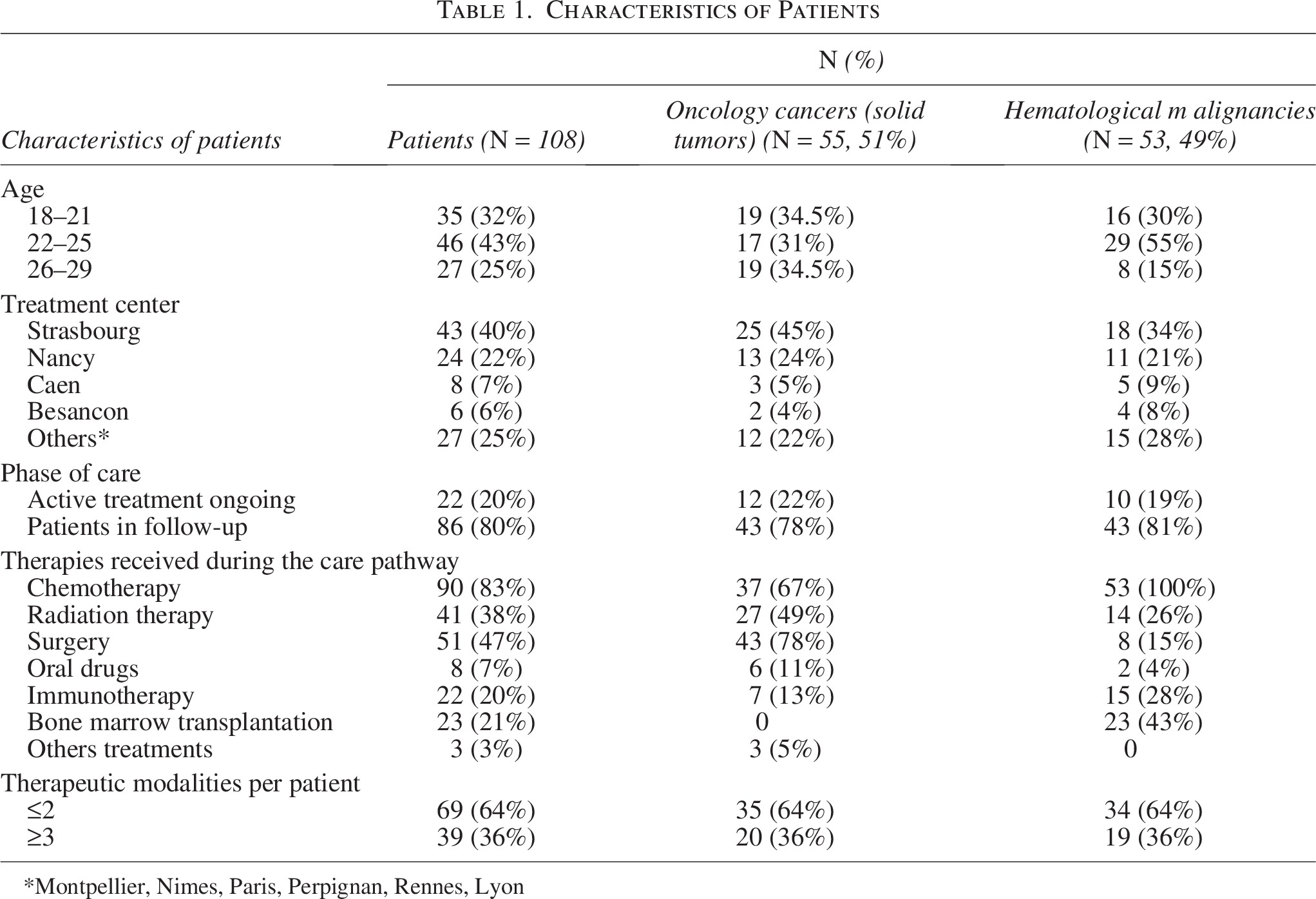
Montpellier, Nimes, Paris, Perpignan, Rennes, Lyon
The most prominent solid tumors were sarcomas (13%, n = 14), germ-cell tumors (12%, n = 13), and brain tumors (9%, n = 10). The other solid tumor types (17%, n = 18) included carcinomas (thyroid, breast, head, and neck), melanomas, and desmoid tumors. In the hematological group, 35 patients (32%) were treated for lymphoma and 17 patients (16%) for acute leukemia.
At the time of data collection, 35 patients (32%) were aged 18–22 years, 46 patients (43%) were 23–25 years, and 27 (25%) were 26–29 years. Twenty patients (19%) were or had been treated in a pediatric department, and only three (<3%) were treated in a specific AYA unit. Fifty-two patients (48%) received chemotherapy, including 23 who underwent bone marrow transplantation (21%). Twenty-two patients (20%) received immunotherapy, and eight (7%) were treated with oral drugs. More than one-third of patients (36%, n = 39) received at least three different therapeutic modalities, reflecting the intensity of their medical care.
Regarding nonsystemic treatments, 51 patients (47%) underwent surgery, and 41 (38%) received radiation therapy.
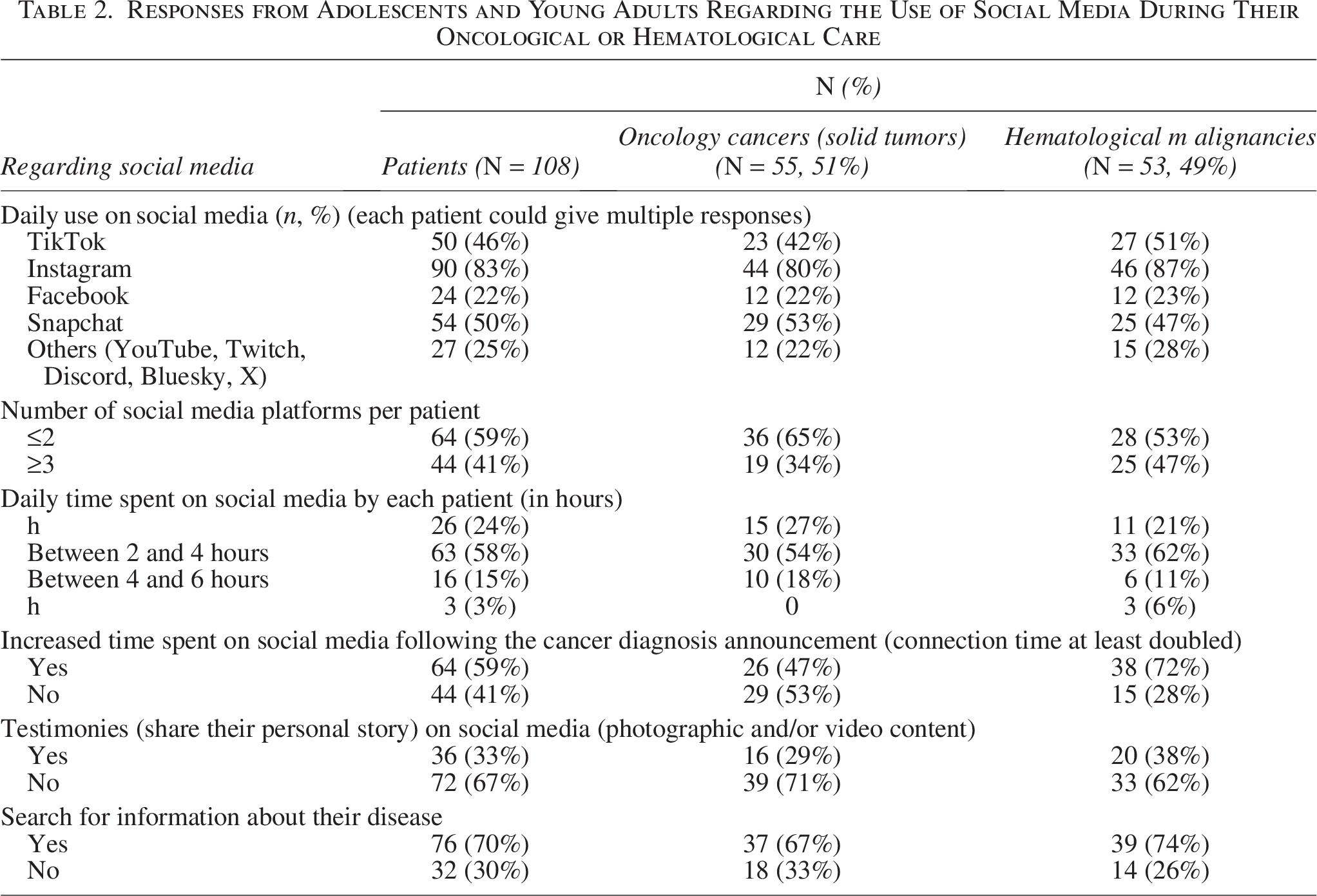
Responses related to SM use are summarized in Table 2. On average, each AYA patient connected to at least two different SM platforms per day (among Facebook, Instagram, TikTok, and Snapchat), with more than half spending between 2 and 4 hours online daily.
Responses from Adolescents and Young Adults Regarding the Use of Social Media During Their Oncological or Hematological Care
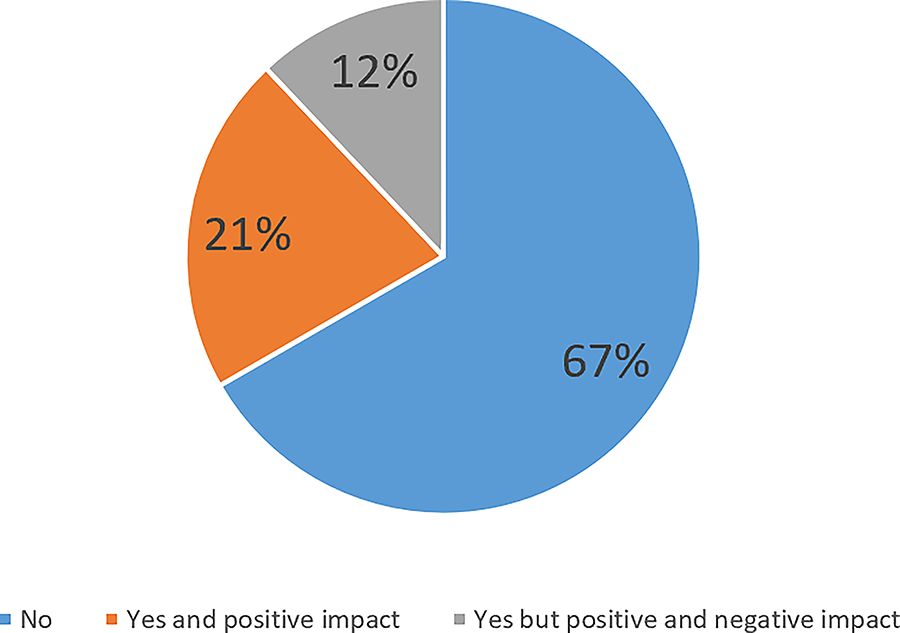
More than two-thirds of patients (70%, n = 76) searched for information on SM related to their disease, including diagnosis, prognosis, treatments, and side effects. This behavior led to both positive outcomes (such as finding answers to their questions and feeling less alone with their cancer; 38%, n = 29) and negative outcomes (such as increasing anxiety; 62%, n = 47), as illustrated in Figure 1. Among these patients, 43% (n = 33) did not verify the relevance of the information with health care professionals (physicians or nurses), as they believed that the information found on SM was accurate or reliable. Finally, six patients reported a lack of information on SM about their specific disease (especially in the case of rare cancers), which contributed to heightened anxiety.

Perceived impact of social media during cancer care among AYAs (108 patients). Search for information on social media related to their disease. AYAs, adolescents and young adults.
Thirty-three patients (n = 36) expressed a desire to share their story on SM, feeling a predominantly positive impact (64%, n = 23), such as receiving support, feeling relief, and finding meaning in their experience. Conversely, for the remaining patients, sharing their story heightened feelings of loneliness and of being different from other AYAs (Fig. 2). Only one patient reported receiving a negative comment in response to their post on SM. Twelve patients wished to share their cancer journey online to raise public awareness but also expressed a desire for support from health care professionals or patient associations when doing so.
Perceived impact of social media during cancer care among AYAs (108 patients). Share their story on social media.
For 59% of patients (n = 64), time spent on SM increased—twofold increase—after diagnosis announcement. Table 3 summarizes the characteristics of patients who reported an increase in SM use. An increase in SM use during treatment was more frequently observed among patients with hematological malignancies and among those who underwent surgery and/or bone marrow transplantation (p < 0.05).
Comparison of Clinical Characteristics According to Change in Social Media Use Following Cancer Diagnosis
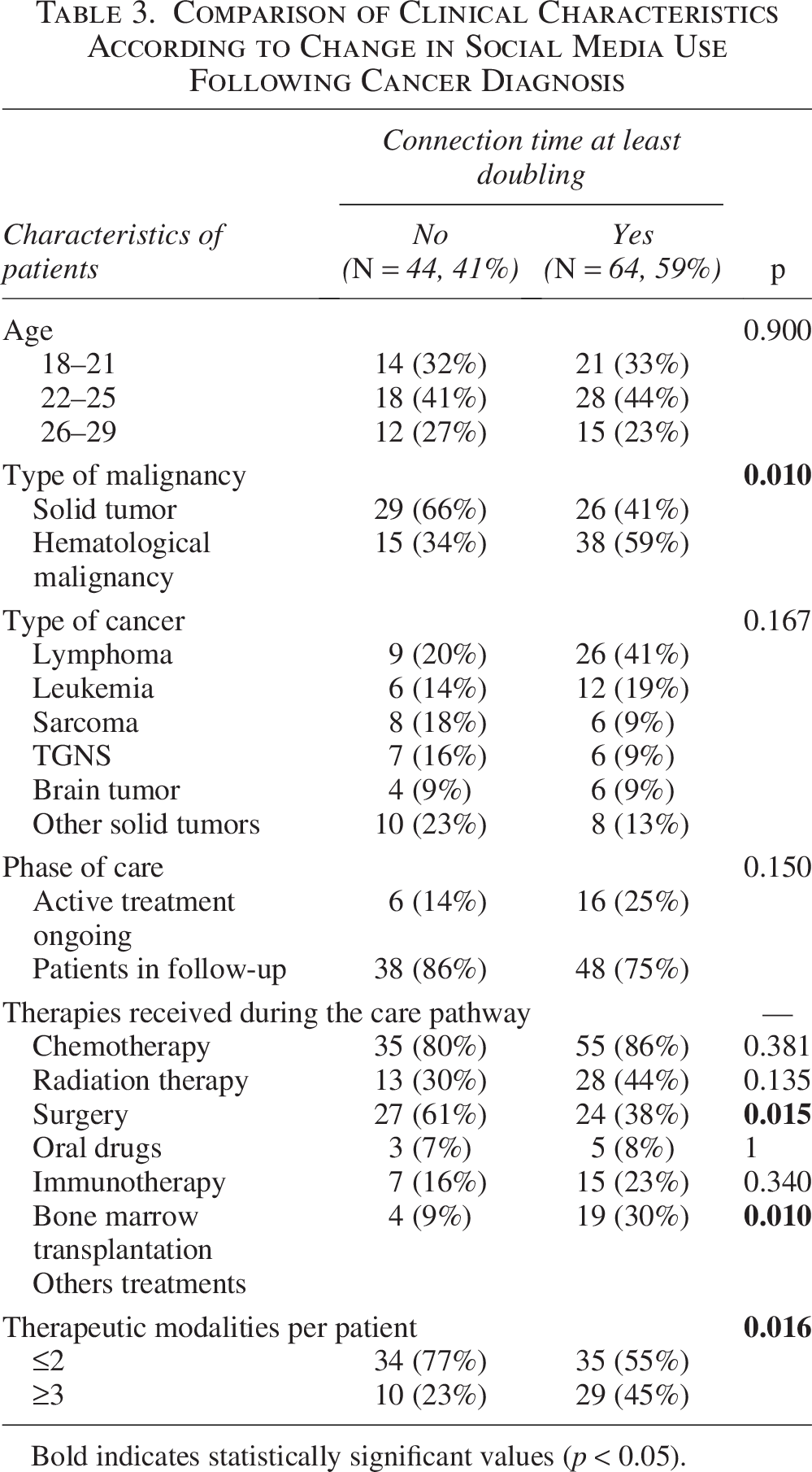
Bold indicates statistically significant values (p < 0.05).
This rise was primarily attributed to boredom experienced during treatment (69%, n = 44). In the free-text section of the self-administered questionnaire, patients explained that during hospital stays lasting several days or weeks, SM served as a distraction and a way to pass the time.
Additionally, nine patients reported signs of SM addiction, including three who spent more than 6 hours per day online.
Discussion
The management of AYA patients in oncology and hematology is both multimodal and multidisciplinary. It increasingly adopts an integrative approach that considers not only medical treatment but also the emotional and psychological dimensions of care. 12 Social well-being is a critical concern for AYAs undergoing treatment or follow-up, as their quality of life is strongly influenced by interactions in the virtual world of SM alongside the real-world support from their family, friends, or other sources of social support that vary according to cultural context. 13
A recent study conducted in March 2024, based on a representative sample of 800 individuals from the French population aged 15–25, highlighted several issues related to screen time and SM use. When asked about health concerns, 85% of AYAs cited “screen addiction” (excessive use of technology leading to dependency on devices such as smartphones, tablets, computers, and televisions), a higher percentage than for other addictions such as smoking, drinking alcohol, or drug use (68%).
Regarding sources of health information, 33% reported consulting specialized websites (17% prioritizing them), while 14% turned to social media (with 8% prioritizing it). Notably, only 21% of AYA responders reported consulting their attending physician first. 14 Most sought information on specific topics such as diet/nutrition, physical activity, fertility, sexual health, and body image via online platforms—often unaware of the existence of hospital-based AYA-specific resources. 15
Introducing the topic of SM during medical consultations could be an effective strategy to mitigate the risks of misinformation and disinformation, especially considering that many AYAs did not verify the accuracy of online content with their health care providers and probably express thoughts, emotions, or behaviors online that they would not usually show in face-to-face interactions (online disinhibition effect). 16 This approach is particularly relevant, as this reduction of inhibitions may lead to either positive behaviors (such as self-disclosure, empathy, and support) or negative behaviors (such as aggression, insults, or harassment). 17
Daniels et al. previously described how SM habits among AYA patients change during treatment, although their findings were based on a much smaller cohort of eight patients. 9 While SM can serve as a space for both direct and indirect social support, AYAs often interpret the meaning of this support in complex and sometimes ambiguous ways, which may increase their emotional vulnerability.
Our study, involving more than 100 patients, supports the same conclusion: it is crucial to provide AYAs with structured guidance on how to navigate and use SM appropriately, but it has several limitations that should be acknowledged. First, no predefined sample size was established, as the study was descriptive and exploratory. The recruitment period was pragmatically set with participating centers to obtain a sufficient sample for meaningful descriptive analysis. Nevertheless, the final sample of 108 participants provides acceptable precision, with a 95% confidence interval of about ±10% for a proportion near 50%, which is considered adequate for this type of observational study.
Moreover, the sample may be subject to a self-selection bias, as participation was voluntary and potentially attracted individuals who are more active on SM or more willing to share their experiences. Second, data were based on self-assessment measures and can reflect subjective perceptions rather than objective behaviors, but we need to evaluate the feelings of the AYAs and not our interpretation of their use of social networks. Recall bias may have influenced the responses, although this represents a pivotal period in their lives, which patients are likely to remember accurately. Further work is needed to explore how health care professionals can integrate SM use into supportive care strategies for young patients with cancer.
During treatment, many AYAs experience social isolation due to prolonged hospitalizations, fatigue, or treatment-related immunosuppression, which often prevents them from attending school or participating in normal social activities. According to our study, AYA patients tend to spend more time on SM after receiving a cancer diagnosis. The primary reason reported was the need for distraction, with SM described as a way to «pass the time» during hospital stays. Given that these hospitalizations can last from several days to several weeks, there is a legitimate concern about the potential development of addictive behaviors—especially considering that SM addiction is already a growing global public health issue. 18 SM therefore becomes an accessible way to maintain social connections, combat boredom, and preserve a sense of normalcy, especially since few recreational or social activities are available in hospital settings.
Additionally, our study revealed that feelings of loneliness are common among AYA patients, even when they are surrounded by family and friends, and supported by medical and paramedical teams. 19 Paradoxically, SM can sometimes intensify these feelings of isolation, highlighting the need to promote authentic, in-person social connections rather than relying solely on virtual interactions. 20
Significant improvements in care are likely to result from the creation of units specifically dedicated to AYA patients, helping to prevent their fragmentation between pediatric and adult services, transitions that are often complex and poorly coordinated. 21 Such dedicated AYA units, already implemented in a few institutions in France (e.g., Leon Berard Hospital and Curie Institute), promote inpatient interactions and peer exchanges, helping patients to feel less isolated. However, these initiatives remain limited in number and are not yet widely accessible.
Integrating discussions about online activities into routine consultations could help identify patients who benefit from positive online interactions, as well as those exposed to misinformation or harmful content. Moreover, developing educational resources or digital support programs in collaboration with patient associations could promote safer and more constructive use of SM during cancer care.
Conclusion
All AYA patients in our study reported daily use of SM for a variety of purposes, including sharing information about their cancer and for leisure, factors that may reduce real-life social interactions in favor of virtual ones. Integrating discussions on digital literacy into patient routine oncological care could help young patients use SM more safely and effectively during cancer treatment. As the number of AYA cancer patients is increasing, this population should be recognized as a distinct group, facing unique and complex psychosocial challenges.22,23 It appears essential to develop specific training programs for AYA-dedicated nurses and psychologists to ensure appropriate supportive care.
Looking ahead, while SM remains a powerful yet underutilized tool, the recent emergence of artificial intelligence—particularly tools that allow patients to ask chatbots detailed questions about their cancer, prognosis, and treatment options—introduces new challenges, while noting that the extent of misinformation linked to chatbots is still to be confirmed. 24 It is therefore urgent for health care professionals to become familiar with these technologies in order to guide their appropriate use and leverage them as daily sources of reliable information for the benefit of patients.
This study provides a valuable first step in understanding the role of SM among AYA cancer patients, but future research should aim to confirm these findings through longitudinal and international studies to explore cultural or health care system differences.
Authors’ Contributions
S.M.: Conceptualization (lead), investigation (lead), data curation (lead), writing original draft (lead), and review and editing (equal). J.G.: Writing original draft (supporting) and review and editing (equal). N.E.-W.: Review and editing (equal). C.P.: Review and editing (equal). K.B.: Review and editing (equal). A.F.: Review and editing (equal). L.G.: Review and editing (equal). F.C.: Review and editing (equal). C.C.G.: Review and editing (equal). S.N.: Review and editing (equal). J.-E.K.: Writing original draft (supporting), review, and editing (equal).
Footnotes
Acknowledgment
The authors thank all the patients and physicians who participated in the study, with special appreciation for the AYA coordinating nurses for their contribution.
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
No funding was received for this article.
Ethics Approval
Ethics approval was not required for this noninterventional study. In accordance with applicable regulations, no informed consent was necessary, as the study was based on an anonymous self-administered questionnaire.