
Abstract
Purpose:
Pediatric, adolescent, and young adult (PAYA) cancer survivors face complex long-term medical and psychosocial needs for which many health care professionals lack training. This study evaluated the PAYA Cancer Survivorship Extension for Community Health care Outcomes (ECHO) program, a virtual, case-based telementoring program, in improving health care professionals’ self-reported knowledge and confidence in survivorship care.
Methods:
A mixed-methods evaluation was done for the 12-session ECHO program (June 2024–May 2025). Surveys assessed changes in self-reported knowledge and confidence (5-point Likert scale), likelihood of applying learning, implementation barriers, and session impact. Quantitative data were analyzed using descriptive statistics.
Results:
Participants included 219 health care professionals from 153 organizations across the 36 U.S. states, one federal district, and 5 countries. Average session attendance was 57 (M = 56.83, SD = 13.07). Self-reported knowledge increased from 2.8 to 3.5 with confidence increasing from 2.7 to 3.4; gains were statistically significant across all 11 content sessions (p < 0.05). Participants reported a high likelihood to apply session content (mean ratings 3.1–4.6 on a 5-point scale), with all sessions except Session 1 exceeding 4.2. The most frequently cited barriers to applying content were lack of resources (26%), lack of time (23%), need for more training (23%); 10% reported no opportunities to apply information, and 37% (n = 130) reported no barriers.
Conclusion:
The ECHO program improved health care professionals’ knowledge and confidence in PAYA survivorship care, with high intent to apply learning. Findings informed the launch of additional ECHO programs. Future efforts should further engage primary care providers and address barriers to translating knowledge into practice.
Keywords
Purpose
Although the majority of cancers are diagnosed in adults over 40, an estimated two million individuals in the United States are survivors of pediatric, adolescent, and young adult (PAYA) cancers. With survival rates exceeding 86%, this growing population is living for decades beyond treatment and faces complex medical and psychosocial challenges throughout their lives. 1,2 A majority of PAYA survivors will experience long-term and late effects that can be wide ranging including cardiovascular disease, secondary malignancies, infertility, cognitive changes, anxiety and depression, and negative financial impacts. 3 –5
Cancer survivorship care is designed to meet these needs by addressing both medical and psychosocial effects of cancer and providing continuity of care throughout the lifespan. Despite established long-term follow-up guidelines for PAYA cancer survivors and a growing awareness of survivorship as a distinct phase of the cancer continuum, access to high-quality survivorship services for PAYA cancer survivors remains insufficient. 6 –9
There is a limited number of specialty survivorship clinics for this population, and they are often concentrated in large academic medical centers, and are often inaccessible due to geography, insurance coverage, or resource constraints on both the patient and provider side. 9 –12 As a result, many PAYA cancer survivors seek long-term follow-up care from primary care providers and other nononcology clinicians who may be more accessible but less equipped to meet the unique survivorship needs of this population. 13 However, many health care providers are not prepared to care for PAYA cancer survivors, citing limited knowledge of survivorship care guidelines, low confidence in managing late effects, and uncertainty about their role in survivorship care. 14,15
To advance quality cancer care and close this gap, the American Cancer Society (ACS) developed a Project ECHO® (Extension for Community Health care Outcomes) program to educate multidisciplinary teams about the distinct needs of PAYA cancer survivors and to support implementation of survivorship care best practices. Through its “All Teach, All Learn” approach, the ECHO Model® uses case-based learnings, shared experiences, and best practices through telementoring to build a “community of practice.” 16 ECHO is widely recognized as a scalable approach to improve high-quality, cost-effective care. 17,18
This study evaluates the impact of the PAYA Cancer Survivorship ECHO program in addressing gaps in survivorship care. Specifically, it examines the program’s impact on health care providers’ knowledge and confidence in managing the long-term medical and psychosocial needs of survivors diagnosed with cancer before age 40.
Materials and Methods
Study design
A mixed-methods evaluation was conducted for the PAYA Cancer Survivorship ECHO program designed to address the unmet long-term survivorship needs of survivors of PAYA cancers. The evaluation was based on the Centers for Disease Control and Prevention (CDC) Framework for Program Evaluation and was guided by best practices in telementoring research.
Program description
The ECHO Model® is used to efficiently share evidence-based practices and resources so that health care professionals enhance their skills and knowledge to improve patient outcomes across the cancer continuum and elevate the quality of cancer care. This ensures that health care professionals are equipped to provide the right care at the right time and place, allowing everyone to prevent, detect, treat, and survive cancer.
The ECHO program was delivered between June 2024 and May 2025 and consisted of 1 Kickoff session and 11 content-focused sessions, each lasting 1 hour. Sessions included a brief, 10–15-minute didactic lecture followed by case-based learning and discussion. Curriculum topics consisted of an overview of survivorship for PAYA cancers; models of survivorship care and integration with primary care; late and long-term effects of treatment including secondary malignancies; long-term follow-up guidelines and care plans; psychosocial and financial challenges in survivorship; fertility and hormonal impacts; healthy living strategies; genetic counseling and testing; and resources and referral pathways to support comprehensive survivorship care. The content was targeted to primary care and cancer care teams including physicians, nurses, social workers, patient navigators, and other support health care roles.
Participants
Recruitment was conducted through professional networks, non-profit organizations, and ACS partner organizations as well as targeted social media posts and email outreach. All participants consented to involvement through their registration and attendance to an ECHO program.
Data collection
Participant demographics, participation, and engagement data were collected through iECHO, Project ECHO’s technology platform, program registration and Zoom reports. Additional data were collected through REDCap. Self-reported demographic data, including gender, clinical profession, and years of experience, were collected to assess audience reach. Participants rated (on a 5-point Likert scale) their knowledge, confidence, and likelihood of using what was learned at the end of every session. Participants also answered questions regarding barriers to applying knowledge learned and impact of the program.
Analysis
Quantitative survey data, including changes in self-reported knowledge and confidence, were summarized using descriptive statistics. Item-level survey responses were based on a 5-point Likert scale range and converted into a score of 1 through 5. The average score for each session was calculated across all ECHO sessions. Percentages of responses were calculated from total attendees of each session.
Pre- and post-session ratings of self-reported knowledge and confidence were collected using a 5-point Likert scale and analyzed as paired data. To evaluate changes over time, the Wilcoxon signed-rank test, a nonparametric method suitable for ordinal paired data, was applied to responses from participants who completed the post-session survey. Statistical significance was determined using a two-sided alpha level of 0.05, set a priori.
Ethics
This evaluation was reviewed by the Morehouse School of Medicine Institutional Review Board and determined to be appropriate for exemption under the federal regulations under protocol 2190195-1.
Results
Participation and engagement
The PAYA Cancer Survivorship ECHO program was implemented from June 2024 to May 2025, consisting of 1 Kickoff session and 11 content-focused sessions. Across the program, a total of 219 unique participants were engaged. Participants represented 153 organizations across the 36 U.S. states, one federal district, and five international countries. The average number of participants per session was 57 (M = 56.83, SD = 13.07, range: 39–86). Each participant attended an average of 3 sessions out of the 12 sessions offered (M = 3.09, SD = 2.68, range: 1–12).
Participants represented a diverse range of professional roles within primary care and cancer care teams including physicians, nurses, social workers, research scientists, and other supportive service providers. While each session included a mix of these roles, the most frequently represented roles across the program were allied health professionals (28%), nursing professionals (17%), medical professionals (13%), advanced practice providers (11%), health care administrative roles (9%), research professionals (7%), public health and community care (7%), and health care supportive roles (7%).
Change in knowledge and confidence
Participants reported significant increases in both self-reported knowledge and confidence following each session of the ECHO program. As detailed in Table 1, mean knowledge ratings increased from 2.8 pre- to 3.6 post-program. Confidence mean ratings showed a comparable increase, rising from a pre-mean rating of 2.7 to a post-mean rating of 3.4. Additionally, statistical analyses revealed significant gains in both self-reported knowledge and confidence across all 11 sessions, with p values below the pre-specified threshold of 0.05.
Self-Reported Knowledge and Confidence of Participants by Session for the Pediatric, Adolescent, and Young Adult Cancer Survivorship ECHO Program
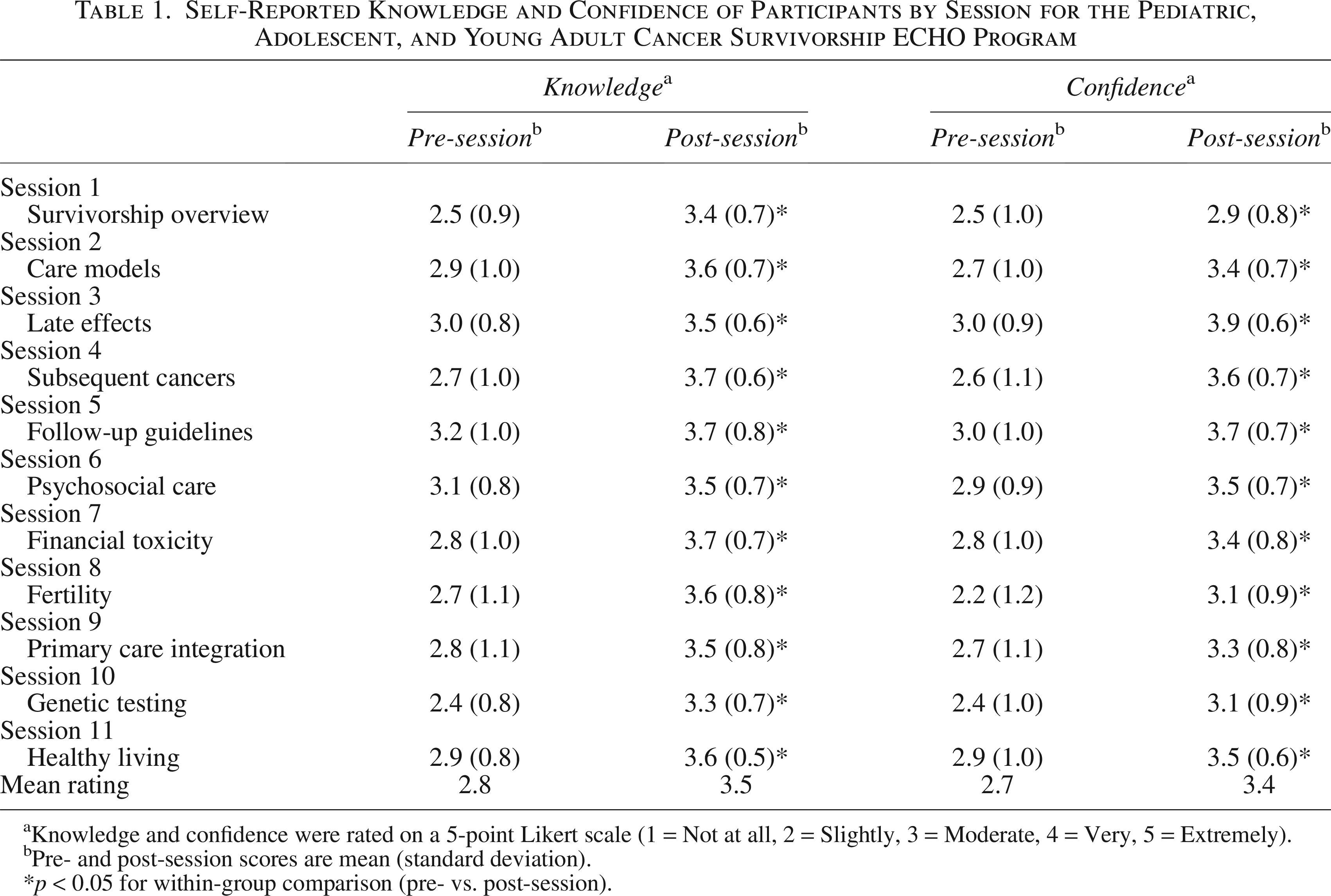
Knowledge and confidence were rated on a 5-point Likert scale (1 = Not at all, 2 = Slightly, 3 = Moderate, 4 = Very, 5 = Extremely).
Pre- and post-session scores are mean (standard deviation).
*p < 0.05 for within-group comparison (pre- vs. post-session).
Likelihood to use what was learned
Participants reported a strong intention to apply session content to their professional work, as shown in Table 2. Across all sessions, participants indicated a high likelihood of incorporating learned material into their professional practice. Mean ratings on a 1–5 scale ranged from 3.1 in Session 1 (Survivorship Overview) to 4.6 in Session 10 (Genetic Testing) and Session 11 (Healthy Living). All sessions, except for Session 1 (Survivorship Overview) had a mean rating between 4.2 and 4.6 indicating consistent confirmation of the relevance and applicability of the materials covered during those sessions.
Mean Participant-Rated Score on Intention to Apply Session Content into Their Work

Likert scale: 1 = Definitely not, 2 = Probably not, 3 = Possibly, 4 = Probably, 5 = Definitely yes.
Barriers to implementation
Participants identified a range of barriers to implementing session content. Table 3 details the most frequently cited barriers were “Lack of resources” (n = 92; 26%), followed by “Lack of time” (n = 81; 23%), and “Need for more training” (n = 80; 23%). Fewer participants indicated “No opportunities to apply information” (n = 35; 10%), suggesting potential system-level barriers rather than participant readiness, while fewer (n = 16; 5%) selected “Other.” Interestingly, the most selected option (n = 130; 37%) was “There are no barriers to using what I learned.” Participant responses by session are also detailed in Table 3 below.
Participant-Identified Barriers to Apply Session Content into Their Work
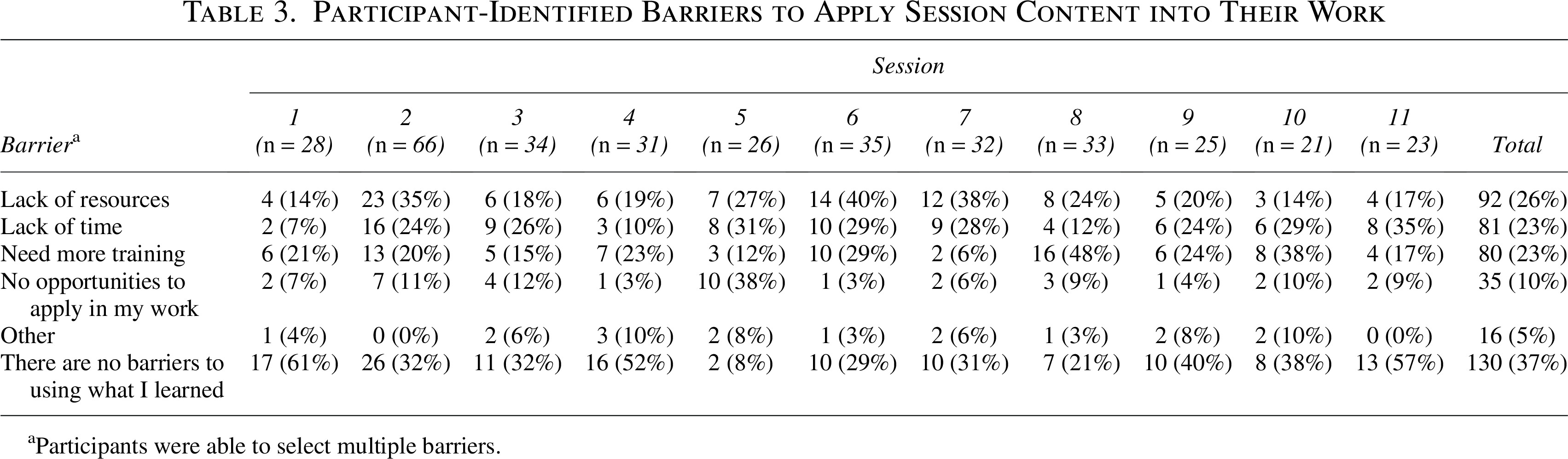
Participants were able to select multiple barriers.
Discussion
This evaluation demonstrates that the PAYA Cancer Survivorship ECHO program improved participants’ self-reported knowledge and confidence in managing long-term medical and psychosocial needs of PAYA cancer survivors, with consistent and meaningful learning across all sessions. These findings align with prior research on other health care topics in different patient populations showing that the ECHO Model® strengthens workforce capacity by expanding access to specialty expertise through virtual telementoring. The program’s reach across 36 states, 1 federal district, and 5 international countries, engaging 219 unique participants from various roles (i.e., nurses, physicians, social workers), further demonstrates the ECHO program’s ability to support a diversity of health care professionals who may lack access to survivorship training.
Participants reported high perceived relevance and strong intention to apply session content within clinical or community-based settings, as well as 130 instances of no identified barriers, suggesting that much of the content was actionable and relevant to their work. The program effectively increased participants’ conceptual understanding and practical competencies, with knowledge cited as the primary impact of 62% of responses. Given the ECHO Model’s case-based, interprofessional discussion format, the observed gains in knowledge and confidence likely also contribute to enhanced collaborative practice and interprofessional dialogue across clinical teams. Importantly, these improvements in provider competence may translate into more timely identification and management of late effects, improved fertility and psychosocial counseling, and strengthened referral pathways, which are all critical components of high-quality survivorship care. Further, the combination of patient and survivor perspectives with case-based learning and shared practical resources were likely facilitators that supported these outcomes.
However, participants highlighted several barriers to implementing survivorship best practices, including limited time and institutional constraints. These findings are consistent with existing literature on challenges in survivorship care delivery, especially in nonspecialty settings. 13,14 The program’s open-access design, which allowed voluntary participation and did not require mandatory attendance may have allowed broader engagement but may have contributed to varied session attendance limiting exposure to the full ECHO program curriculum.
There are several limitations to this evaluation. All outcomes were based on self-reported measures from participants, which may be subject to bias. Additionally, participation in post-session evaluation surveys was voluntary, which may limit the generalizability of the findings. Finally, the evaluation did not assess long-term behavior change or include patient-level outcome data, which would require longitudinal evaluation and limits conclusions about the clinical impact of the program.
Future direction should focus on expanding the program’s reach to include more primary care providers, who are often the point of contact for PAYA cancer survivors despite reporting low preparedness. 14,15 This could be done by advertising the program through state medical licensing boards as well as internal medicine and family medicine society membership societies. Evaluation data revealed persistent gaps in training, most notably the session on “Fertility and Hormonal Impacts of Cancer,” where “need for more training was the most frequently cited implementation barrier.” In direct response, the “Building Pathways to Fertility Preservation in Cancer ECHO” program was launched in 2025 to deliver case-based training and telementoring on fertility preservation for PAYA cancer patients. Future ECHO programs should similarly address high-priority gaps through participant feedback to systematically strengthen workforce capacity across the PAYA cancer continuum. Strategies to overcome barriers, including resource toolkits, guidance, and integrated workflows across multidisciplinary teams will be essential to translate knowledge gains into practice change.
Conclusion
This evaluation demonstrates that the ECHO Model® can improve health care professionals’ knowledge, confidence, and ability to support the distinct needs of PAYA cancer survivors. By expanding survivorship expertise among a multidisciplinary group of health care professionals, the ECHO program helps address gaps and advance high-quality survivorship care for PAYA cancer survivors. Based on the evaluation data, which identified areas of unmet educational need and participant interest, future ECHO programs should focus on topics where knowledge gaps were most pronounced.
Authors’ Contributions
J.M.: Data curation, formal analysis, visualization, writing—original draft, and writing—review and editing. A.R.: Methodology, writing—original draft, writing—review and editing, and project administration. K.P.: Writing—original draft and writing—review and editing. M.R.: Writing—original draft and writing—review and editing. N.K.-L.: Writing—original draft and writing—review and editing. M.M.R.: Conceptualization, methodology, writing—original draft, writing—review and editing, and supervision.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of Kristie Marcelle, MSW, PMP; Rich Killewald, MNM; Nicole L. Stout, DPT, CLT-LANA, FAPTA; and Laura Makaroff, DO, whose leadership and strategic guidance at the ACS were instrumental in the development and implementation of this program. The authors also extend their gratitude to Fumiko Ladd Chino, MD; Jessica Corredor, MS, CGC; Matthew J. Ehrhardt, MD, MS; Terri Lynn Woodard, MD; and John Salsman, PhD, who served as didactic presenters for the PAYA Cancer Survivorship ECHO program and shared their clinical and research expertise with participants. Finally, authors gratefully acknowledge Christabel K. Cheung, PhD, MSW; Hayley Arceneaux; JJ Singleton; Kendall F. Moseley, MD; Reegan George; Lauren Ghazal, PhD, FNP-BC; Mariana Cardenas; Ariane Navarro, MA; Dawn Ritzwoller, MPH; Tiffany Spinos; and Lara Diamond for their invaluable lived experience perspectives, which enriched the program’s discussions and deepened understanding of the survivorship experience.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research, supporting data are not available.
Author Disclosure Statement
The authors have no applicable disclosures.
Funding Information
No funding was received for this article.