
Abstract
Purpose:
While exercise oncology research has led to broad acceptance of exercise programs for cancer patients, the specific needs of young adults (YA) with cancer remain underexplored. The YOUEX study evaluates the effects of tailored online and in-person exercise programs on quality of life (QoL) and cancer-related fatigue (CRF) in YA.
Methods:
This three-arm, non-randomized, preference-based intervention study offered three exercise modules (M1) online supervised group-based, (M2) online unsupervised, and (M3) in-person supervised. YA with cancer (≤39 years) participated in a 12-week intervention with a 12-week follow-up. QoL (EORTC QLQ-C30) and CRF (EORTC FA12, QLQ-C30 fatigue scale) were assessed at baseline (T0), 6 weeks (T1), 12 weeks (T2), and follow-up (T3).
Results:
A total of 92 YA (mean age 31.9 ± 4.9 years, 94% female) participated. M2 was most frequently chosen (54.3%), followed by M1 (34.8%) and M3 (10.9%). Overall QoL improved significantly at follow-up (p < 0.01, r = 0.35). Significant improvements were observed in physical (p < 0.001, r = 0.40), emotional (p < 0.01, r = 0.36), cognitive (p < 0.01, r = 0.34), and social functioning (p < 0.01, r = 0.35) during the intervention, with continued physical and emotional improvements at follow-up. Fatigue symptoms decreased on the QLQ-C30 scale, while FA12 scales remained unchanged. No differences were found between modules.
Conclusion:
Tailored exercise programs positively impact QoL in YA with cancer, with online interventions being particularly well received. Further research is needed to optimize these programs for CRF management and evaluate the effectiveness of online interventions in more detail.
Keywords
Introduction
Every year, half a million people in Germany are diagnosed with cancer, including approximately 15,000 young adults (YA) between the ages of 18 and 39. The most common cancers in young women under 45 are malignant melanoma, thyroid cancer, and breast cancer, while in men, testicular cancer, melanoma, colorectal cancer, and Hodgkin’s disease dominate. Although less common than in older adults, cancers in YA tend to be more aggressive and are the leading cause of death in this age group. 1 Despite an increased 5-year survival rate of over 80%, long-term side effects such as persistent fatigue, decreased quality of life (QoL), fertility problems, cardiovascular disease, osteoporosis, and secondary malignancies remain prevalent. 2 Especially, fatigue is a very common but often overlooked symptom in YA, although a significant and clinically meaningful increase in fatigue after cancer therapy can be measured in most cases. In addition, YA experience significant psychological and social distress due to prolonged treatment, isolation, and disruptions to key life stages, such as career building and family planning.3,4
Extensive research has demonstrated the benefits of structured exercise programs during and after cancer treatment, showing reductions in symptoms such as fatigue, impaired physical function, chemotherapy-induced polyneuropathy, and lymphedema.5,6 In addition, increasing evidence suggests a positive association between physical activity and cancer-specific survival.7,8 However, most studies have focused on older patients, making it unclear how these findings translate to YA. Reports from the German Foundation for Young Adults with Cancer highlight the lack of appealing, tailored exercise programs. 9 Existing oncology exercise programs are often designed for older individuals and do not address YA-specific needs such as financial constraints, time management, family responsibilities, and career obligations. 10 As a result, research on the feasibility and effectiveness of YA-specific exercise programs is limited.11–13
To address these gaps, the YOUEX (YOUng EXercisers) study was developed to assess YA preferences for online and in-person exercise programs and their impact on QoL and cancer-related fatigue (CRF). The first article of the YOUEX study analyzed exercise preferences and module selection in this target group in detail. 14 This second article investigates the effects of the YOUEX exercise modules on QoL, CRF, and levels of distress in YA.
Materials and Methods
Study design
A three-arm, non-randomized, preference-based intervention study was conducted. The intervention period lasted 12 weeks, followed by a 12-week follow-up. Assessments were conducted at four time points: baseline (T0), after 6 weeks (T1), after 12 weeks (T2), and follow-up at 24 weeks (T3). The study was approved by the ethics committee of the medical faculty at Heidelberg University (S-932/2020) and registered at clinicaltrials.gov (NCT05613699).
Participants and recruitment
Eligible participants were YA (18–39 years) who had been diagnosed with cancer within the last 5 years. Exclusion criteria included lack of medical clearance for exercise (e.g., unstable bone metastases), severe cognitive impairment, or insufficient German language skills. Recruitment took place from September 2020 to April 2021 via social media, clinical websites, flyers, and patient support groups of the German Foundation for Young Adults with Cancer. Participants provided written informed consent prior to study enrollment.
YOUEX exercise modules
Before starting, participants received a medical and exercise-related anamnesis and individualized exercise counseling by a sports scientist either by phone or in person. Participants could then choose one of three exercise modules based on their preferences. The modules were developed in collaboration with the German Foundation for Young Adults with Cancer:
Module 1 (M1): Supervised online group exercise
This module consisted of a structured, 60-minute group-based exercise session once a week, conducted via an online video conferencing platform. The training program included endurance, strength, and coordination exercises.
Module 2 (M2): Unsupervised home-based training with an app
Participants in this module received personalized training recommendations via an online app. Training was self-managed and focused primarily on endurance and resistance exercises, recommended 2–3 times per week.
Module 3 (M3): Supervised in-person training
This module allowed participants to train at certified OnkoAktiv exercise facilities, 15 supervised by qualified exercise professionals. The recommendation was 1–2 weekly sessions with an individualized training plan.
At T1 (after 6 weeks), participants could change or combine modules. This choice was repeated at T2. After the 12-week intervention (T2), participants could voluntarily continue their chosen modules for another 12 weeks. Follow-up ended at T3. Participants who initially chose module 3 but could not complete the program due to COVID-19 restrictions were able to switch to the digital programs immediately.
Outcomes and study instruments
Data collection included demographic, diagnostic, and treatment characteristics via self-report questionnaires. QoL was assessed using the EORTC QLQ-C30 (version 3), a validated questionnaire for cancer patients. The QLQ-C30 includes one global health status, five functional scales, and a total of nine symptom scales. All scales range in scores from 0 to 100, with higher scores indicating a higher level of response. Thus, a high score on the global QoL or functional scales represents a high level of QoL or functioning, whereas a high score on the symptom scales represents a high level of symptomatology. 16 CRF was measured using the EORTC QLQ-FA12, which includes subscales for physical, emotional, and cognitive fatigue. Higher scores indicate greater symptom burden. Physical activity levels before and after diagnosis and before and after the intervention were assessed using the Godin-Shephard Leisure-Time Physical Activity Questionnaire. 17 This tool categorizes activity into light, moderate, and vigorous intensity, measured in minutes per week. Psychosocial distress was measured using the National Comprehensive Cancer Network Distress Thermometer, 18 a single-item screening tool ranging from 0 (no distress) to 10 (extreme distress).
Statistical analysis
Data analysis followed an exploratory approach using descriptive and inferential statistical methods. Normality was tested using the Shapiro-Wilk test, complemented by visual inspection (histograms, QQ plots). When data were not normally distributed, nonparametric tests were applied. For within-group comparisons over time, the Wilcoxon test was used. As no changes in QoL and fatigue were assumed at T1 (6 weeks), the analysis was conducted only from T0 to T2 (12 weeks). For module comparisons, changes from T0 to T1 were analyzed using the Mann–Whitney U test. Module 3 (in-person training) was excluded from the module comparison because it could not be carried out as planned due to the restrictions imposed by the pandemic, making comparisons impossible. A 95% confidence interval was applied for all significance tests. Due to the exploratory nature of the study, multiple testing adjustments were not performed. 19 Effect sizes for median differences were calculated using Pearson’s correlation coefficient r, interpreted according to Cohen’s classification (small: ≥0.1; medium: ≥0.3; large: ≥0.5). 20 All statistical analyses were conducted using IBM SPSS Statistics 27 and Microsoft Excel 2016.
Results
A total of 106 YA with cancer contacted the YOUEX study team to participate between September 2020 and April 2021. A total of 104 YA met the inclusion criteria, of which 92 YA signed the informed consent form and received an exercise consultation based on their health status. The distribution of cancer types was 55% breast, 19% (non-)Hodgkin lymphoma, and 15% other cancer types (e.g., ovarian, skin, colon, cervix, testicles, and lung). Table 1 shows patient characteristics at baseline and initial module selection. Module 2 was the most frequently selected module with 54.3% (n = 50), followed by module 1 (34.8%; n = 32) and module 3 (10.9%; n = 10). At T1, 43% (n = 34) of participants replaced or amended their initial module. Eleven participants (14%) replaced their initial module, and 23 participants (29%) amended it. Between T1 and T2, 71% took part in one module, while 29% took part in two different modules.
Patient Characteristics at Baseline and Initial Module Selection
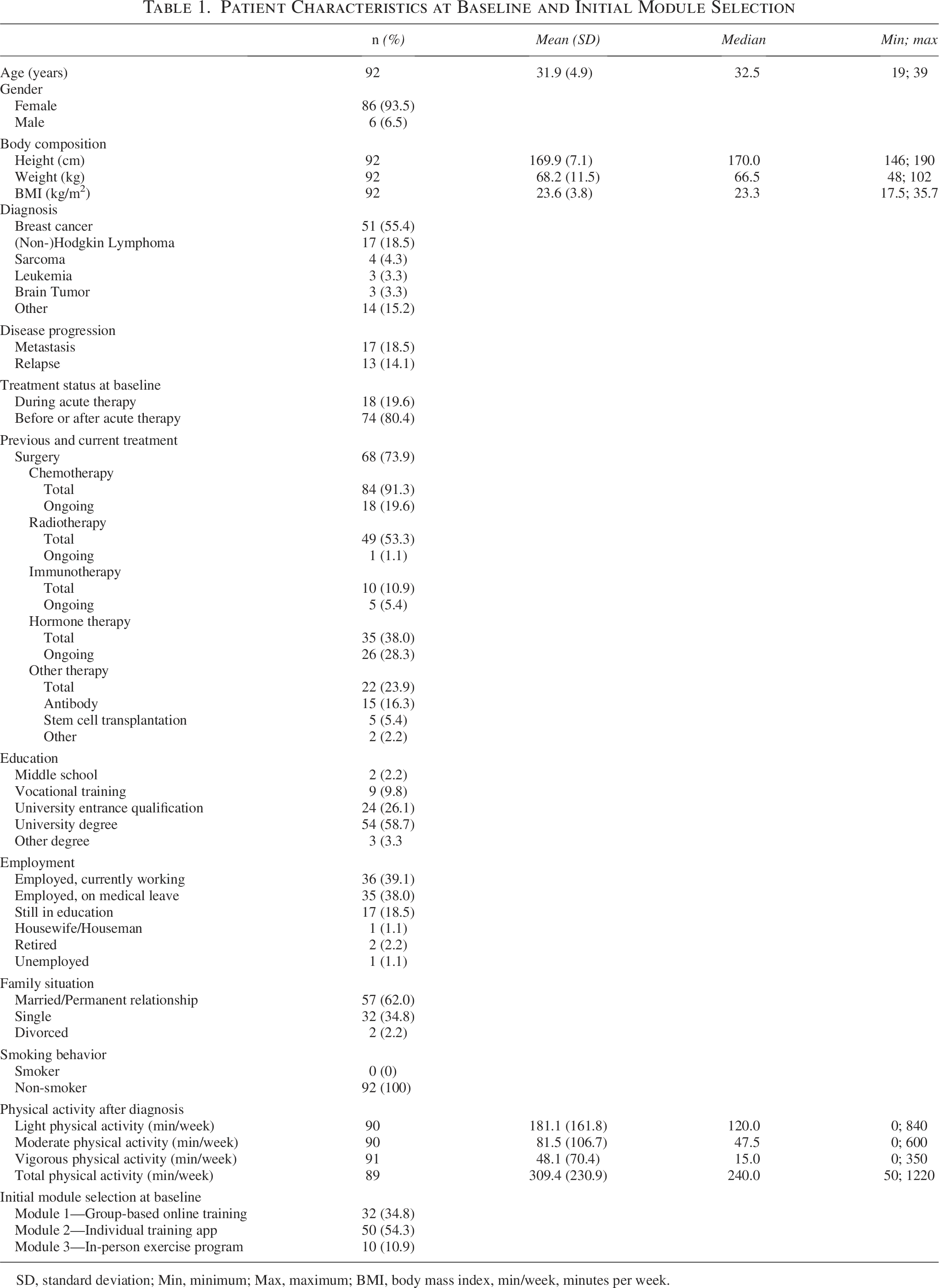
SD, standard deviation; Min, minimum; Max, maximum; BMI, body mass index, min/week, minutes per week.
Changes in quality of life, fatigue, and levels of distress
First, changes in the entire cohort were considered. Table 2 shows the changes in QoL, fatigue, and levels of distress at three time points. The YA overall QoL did not change between T0 and T2 (z = 1.144, p = 0.253, n = 74), but it did improve between T2 and T3 (z = 2.92, p < 0.01, n = 69, r = 0.35). At baseline, 87% of participants scored below the clinically relevant cutoff for emotional functioning (≤71), 73% scored below the cutoff for cognitive functioning (≤75), 58% scored below the cutoff for social functioning (≤58), 53% scored below the cutoff for physical functioning (≤83), and 37% scored below the cutoff for role functioning (≤58). 21 There were significant changes in the subscales of physical and emotional functioning between T0 and T2 (physical: z = 3.475, p > 0.001, n = 74, r = 0.40; emotional: z = 3.066, p < 0.01, n = 74, r = 0.36), as well as between T2 and T3 (physical: z = 3.047, p < 0.01, n = 69, r = 0.37; emotional: z = 2.733, p < 0.01, n = 69, r = 0.33). Cognitive and social functioning changed between T0 and T2 (cognitive: z = 2.958, p < 0.01, n = 74, r = 0.34; social: z = 2.996, p < 0.01, n = 74, r = 0.35) but not between T2 and T3 (cognitive: z = 1.190, p = 0.234, n = 69; social: z = 1.841, p = 0.066, n = 69). The significant changes in the subscales represent medium-sized effects. The functional subscale of role functioning did not change between T0 and T2 (z = 0.700, p = 0.484, n = 74), nor between T2 and T3 (z = 1.662, p = 0.096, n = 69).
Quality of Life, Fatigue and Levels of Distress Before (T0), After the 12-Week YOUEX Intervention (T2) and After the 12-Week Follow-up (T3)

Nonparametric Wilcoxon test for T0–T2 median differences (n = 74) and Pearson’s correlation coefficient r for effect sizes.
Nonparametric Wilcoxon test for T2–T3 median differences (n = 71) and Pearson’s correlation coefficient r for effect sizes.
T0, Baseline; T2, after 12-week intervention; T3, after 12-week follow-up period; IQR, interquartile range; QoL, quality of life; QLQ-C30 fatigue, fatigue symptom scale of the EORTC Core Quality of Life Questionnaire; FA12, fatigue questionnaire of the QLQ-C30; NCCN, National Comprehensive Cancer Network.
At baseline, 76% of all participants reported fatigue above the threshold for clinical importance (QLQ-C30 fatigue scale score ≥ 39). 21 The subscales of physical (z = −0.917, p = 0.359, n = 74), emotional (z = −1.548, p = 0.122, n = 74), and cognitive fatigue (z = 0.063, p = 0.949, n = 74) measured by the QLQ-FA12 did not show significant changes between T0 and T2. Between T2 and T3 changes were found in physical fatigue (z = −2.688, p < 0.01, n = 69, r = 0.32) but not in emotional (z = −1.392, p = 0.164, n = 69) or cognitive fatigue (z = −1.227, p = 0.220, n = 69). However, when looking at the symptom scale of the QLQ-C30, a significant improvement in fatigue was measured between T0 and T2 (z = −3.855, p < 0.001, n = 74, r = 0.45) and between T2 and T3 (z = −3.828, p < 0.001, n = 69, r = 0.46).
Levels of distress improved significantly between T0 and T2 with a large effect (z = −4.896, p < 0.001, n = 74, r = 0.57). No further improvements in levels of distress were found between T2 and T3(z = −0.482, p = 0.630, n = 69).
Comparison of module groups
When comparing the module groups, module 3 (n = 10) was not included because the supervised exercise program could not be performed consistently due to COVID-19 pandemic-related restrictions. Figures 1 and 2 show the changes in QoL and fatigue within the initial module selection between baseline (T0) and after 6 weeks (T1). No significant changes were measured in either QoL or fatigue. The detailed QoL and fatigue change scores can also be found in Supplementary Data. Looking at the QoL data descriptively, there is a trend toward improvement, particularly in social function (see Fig. 1). This seems to be higher in the group that received weekly online training (Module 1) than in the group that received individual home training with an online training app (Module 2). Fatigue symptoms and levels of distress did not appear to differ between the groups (see Fig. 2).
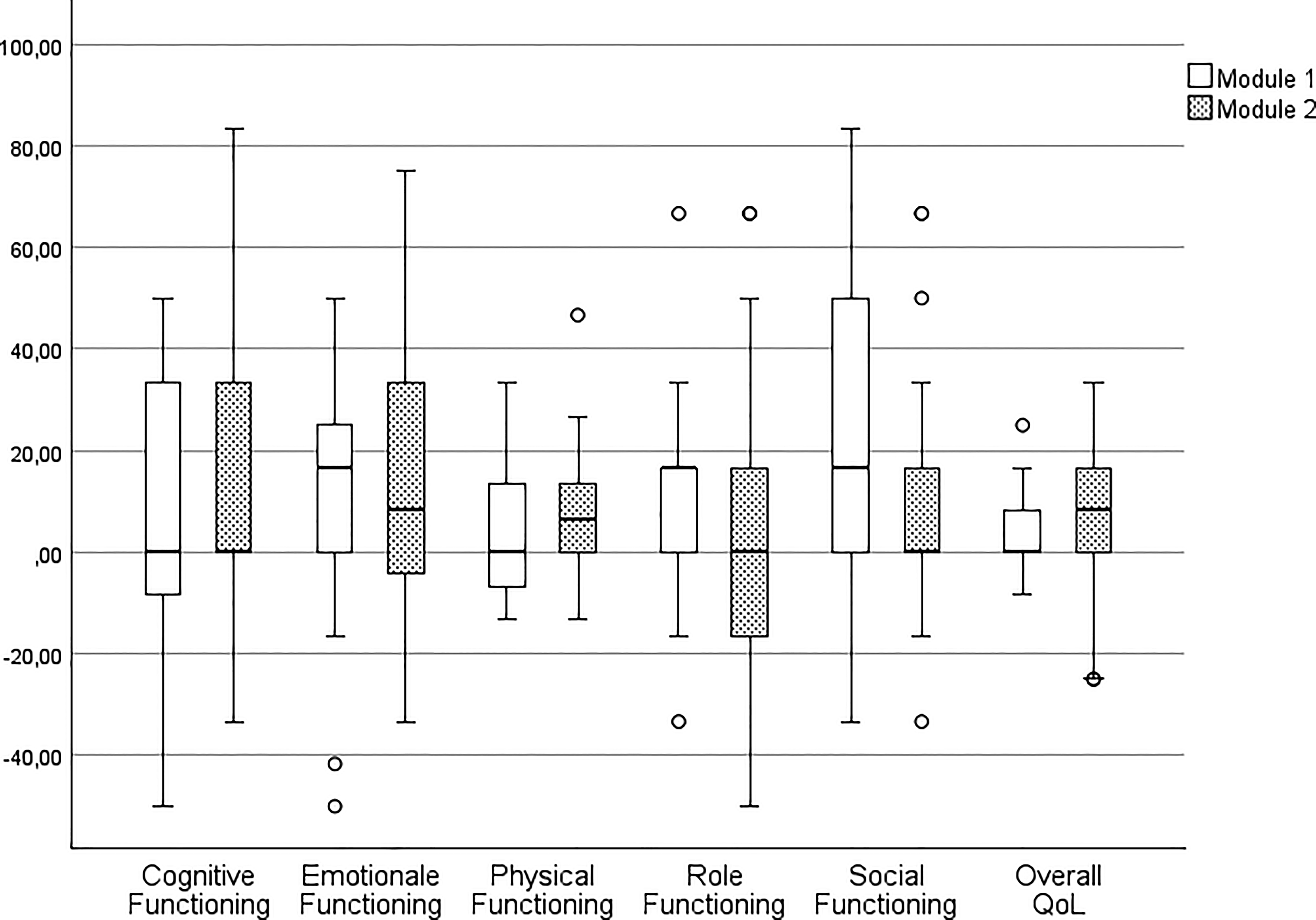
Changes in quality of life between T0 and T1 within the modules. T0: baseline; T1: after 6 weeks of intervention; Module 1: supervised, group-based online exercise program once a week; Module 2: unsupervised, individual home training with online training app at least once a week; ° Outliers.
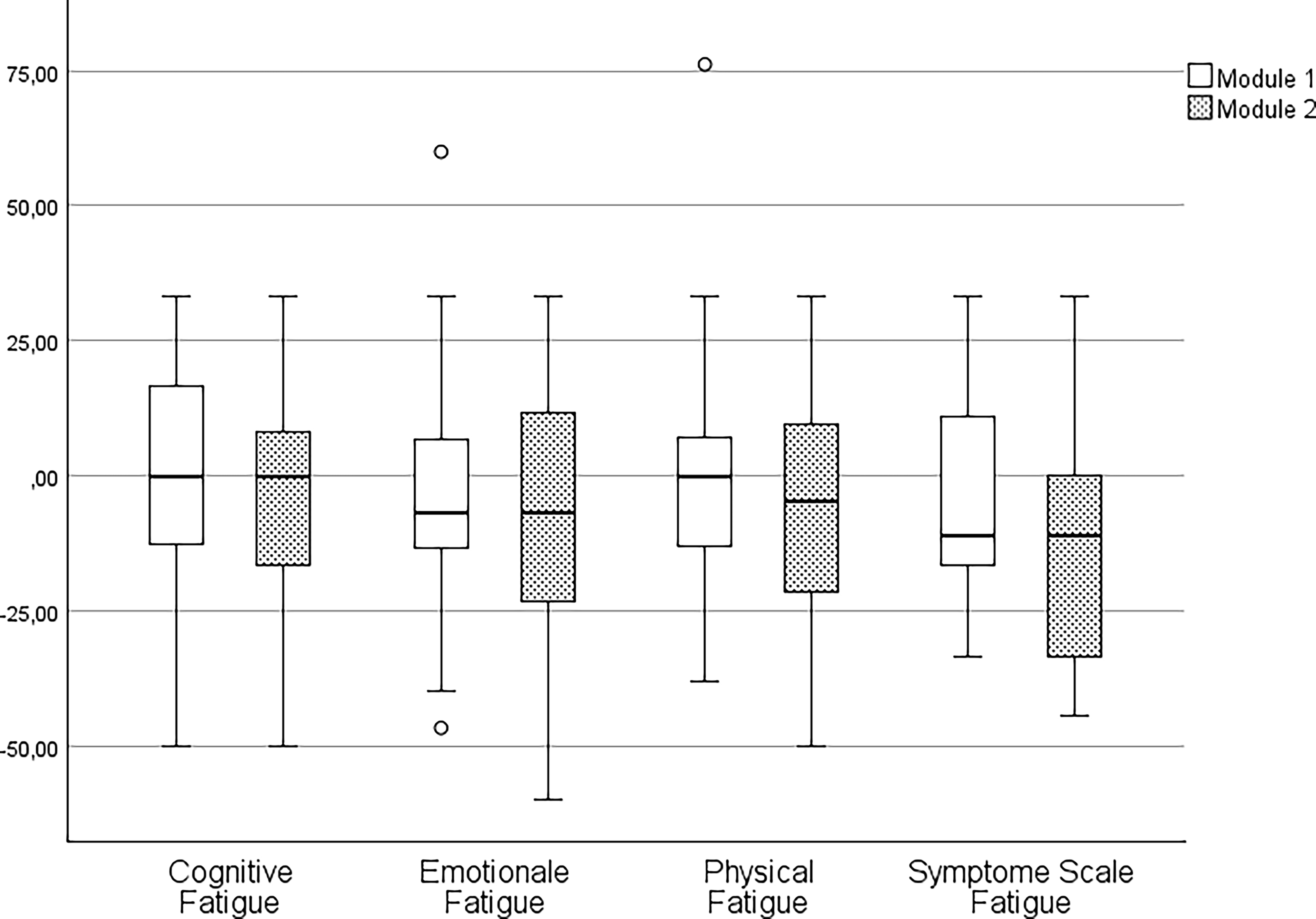
Changes in fatigue between T0 and T1 within the modules. T0: baseline; T1: after 6 weeks of intervention; Module 1: supervised, group-based online exercise program once a week; Module 2: unsupervised, individual home training with online training app at least once a week; ° Outliers.
Discussion
The YOUEX study evaluated the effects of tailored online and in-person exercise programs for YA with cancer, focusing on QoL and CRF. The data presented here showed mostly improved scores on patient-reported outcomes following a 12-week exercise period in the provided exercise modules. Results indicate moderate enhancements in physical, emotional, cognitive, and social functioning, as well as reduced distress. Role functioning remained unchanged, which may be due to the fact that almost half of the participants were on sick leave, and 20% were still in education. Overall QoL did not change during the intervention but improved significantly at follow-up. Fatigue remains an important issue for YA with cancer, affecting almost 80% of the cohort at baseline.21,22 While fatigue, as measured by the EORTC QLQ-C30 subscale, decreased moderately, no changes were observed in the EORTC QLQ-FA12 subscales. This discrepancy may be due to differences in questionnaire design. The EORTC QLQ-C30 fatigue subscale can be interpreted in the context of functional ability, whereas the EORTC QLQ-FA12 captures fatigue as a multidimensional construct, including physical, emotional, and cognitive aspects.23,24 It is possible that the intervention did not sufficiently address cognitive and emotional fatigue, explaining the lack of significant changes in these subscales. Furthermore, the EORTC QLQ-C30 assesses functional domains such as cognition and emotion, whereas the FA12 captures fatigue in the physical, emotional, and cognitive domains. Although these domains are correlated, 25 they represent related but distinct constructs. In their psychometric study, Kecke et al. reported correlations between FA12 dimensions and C30 functional scales ranging from r = −0.53 (physical) to r = −0.65 (emotional), indicating substantial but incomplete overlap. 25 Thus, improvements in emotional and cognitive functioning observed in our study do not necessarily translate directly into reductions in fatigue, because the FA12 specifically measures subjective fatigue rather than functional capacity. Therefore, the directionally consistent but statistically non-significant changes in fatigue are plausible given the partial overlap between functional improvement and fatigue perception.
This cohort had substantial functional impairments comparable to other oncology groups. Fatigue scores were even higher than those reported in metastatic breast cancer patients. 26 In terms of global health status, physical, and role functioning, YA with cancer had scores similar to those of patients with metastatic pancreatic cancer. 27 Compared to breast cancer patients, the YA scored worse in the global health status, with 58–65 points. 28 Social and emotional functioning were particularly affected, with scores even lower than those of pancreatic cancer patients. One reason, this observation may be that YA tend to compare themselves with their healthy peers, who typically score above 90 on functional scales. 29 Social functioning was particularly low, with a median score of 50, significantly below the mean scores of metastatic pancreatic cancer patients (mean: 70) and breast cancer patients (mean: approximately 75).26,27 Compared to healthy YA, social limitations were more than one-third lower (mean: approximately 85). 29 These findings underscore the importance of exercise in supporting psychosocial well-being in this population.
An analysis of changes between baseline (T0) and 6 weeks (T1) showed interesting descriptive trends in social functioning across the different exercise modules. Although group differences were not statistically significant, Module 1 (supervised online group training) showed a mean increase of 21 points—twice the improvement seen in Module 2 (unsupervised home-based training). Differences in social functioning between T1 and T0 were more spread out in Module 1, largely due to individuals with particularly positive improvements (see Fig. 1). In Module 2, the differences in social functioning were comparable to the other endpoints. It should be noted that the intervention took place during the COVID-19 pandemic, which already had a negative impact on the social health dimension due to strict contact restrictions. 30 The strong positive effects seen in Module 1 suggest that even minimal social interaction, such as one virtual session per week as in Module 1, can have significant benefits.
Overall, current oncology exercise recommendations are based on extensive research 31 and international guidelines.32,33 However, most studies have focused on older cancer patients, and tailored exercise programs for YA remain limited. 34 Some promising initiatives exist, such as physical activity counseling and specialized exercise programs, including ski camps for YA with cancer organized by the University Hospital Essen.35–37 The YOUEX study shows that online-based exercise interventions can be a relevant pillar of exercise therapy care that addresses the specific target group of YAs. The question remains to what extent exercise programs need to be supervised or partially supervised in order to achieve the intended effectiveness of the exercise therapy outcomes.
Limitations and future research
The YOUEX study has several limitations. Its non-randomized, uncontrolled design prevents causal conclusions about the effectiveness of exercise in young cancer patients. Exercise adherence was not tracked, limiting insight into the dose-response relationship. Objective performance data, such as daily activity or strength, were not collected. Selection bias likely influenced the results because participants were predominantly physically active, highly motivated, well-educated, female, diagnosed with breast cancer, nonsmokers, and employed or in education. This may limit the generalizability of the findings. The applicability of the results to other patient groups with lower initial motivation needs to be evaluated. Differences between the three exercise modules should be interpreted with caution due to differences in FITT criteria and level of supervision. The study took place during the COVID-19 pandemic, which affected the assessment of QoL.
Despite these limitations, YOUEX provides valuable exploratory insights. Future research should validate the findings in a randomized, controlled trial. The psychosocial needs of YAs should not be ignored at this stage, and specific exercise programs should be implemented and evaluated regardless. The reality of exercise care for YAs shows a lack of age-appropriate exercise programs across Germany. Because of their unique psychosocial situation, it may be useful to focus on the psychosocial elements of exercise therapy when designing and evaluating exercise programs.
Conclusion
The YOUEX study shows that online-based exercise interventions are feasible and beneficial for YA with cancer, improving physical, emotional, cognitive, and social functioning. While overall QoL remained unchanged, improvements were seen at follow-up. CRF showed inconsistent results, highlighting the need for further research. YA with cancer face a multidimensional health burden, particularly in global health status, physical functioning, and role functioning. Tailored programs that address multiple dimensions of health are essential, and exercise—with its physical, psychological, and social benefits—could be key. Despite study limitations, exercise therapy should be a medical priority because of its potential to reduce isolation and the psychosocial impact of cancer.
Authors’ Contributions
Conceptualization; A.V. and J.W. Methodology; A.V. and J.W. Software; A.V. Validation; A.V., V.K., M.G., T.N., and M.K. Formal Analysis; A.V. and V.K. Investigation; A.V., V.K., M.G., T.N., and M.K. Resources; J.W. Data curation; A.V. and V.K. Writing—original draft preparation; A.V. and V.K. Writing—review and editing, M.G., T.N., M.K., and J.W. Visualization; A.V. and V.K. Supervision; J.W. Project administration; A.V. Funding acquisition; J.W. All authors have read and agreed to the published version of the article.
Footnotes
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the medical faculty at Heidelberg University (S-932/2020).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
J.W. invented and founded the network OnkoAktiv and is currently member of the association board. The other authors declare no conflict of interests. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article; or in the decision to publish the results.
Funding Information
This research was funded by German Foundation of Young Adults with Cancer, grant number 17/10/2022.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.