
Abstract
Purpose:
Adolescents affected by cancer experience unique educational and social challenges during high school due to cancer diagnosis, treatment, and survivorship. High school experiences may also be impacted by developmental stage at diagnosis. This study aims to compare the high school experiences related to age at diagnosis (childhood or adolescence) from adolescent and young adult and parent perspectives.
Methods:
We used purposive sampling to recruit youths and parents to semistructures interviews, including 18 youths (11–23 years), diagnosed during childhood (n = 8; age at diagnosis M = 6.8) and adolescence (n = 10, age at diagnosis M = 13.8), and 13 parents (34–65 years), of youths diagnosed in childhood (n = 8, child age at diagnosis M = 6.9) and adolescence (n = 5, child age at diagnosis M = 13.6). Interviews were transcribed verbatim and analyzed thematically.
Results:
We identified two common themes for youths: Academic Calibration, highlighting the adjustments to academic performance and engagement throughout the cancer journey, and (Dis)connection, describing shifts in social identity and peer relationships. For parents, themes included: Navigating School Engagement, reflecting challenges with education engagement, and Social Flux, capturing changes in social functioning and peer interactions. Distinct subthemes were identified across all youths, including Missing Out, Social Isolation and School Takes a Back Seat, detailing the social and academic experiences of youths diagnosed in adolescence.
Conclusions:
This study underscores the shared and distinct challenges faced by adolescents affected by cancer in high school. Disruptions to social networks faced by adolescents with cancer and enduring academic challenges of adolescents diagnosed in childhood underscore the need for tailored, comprehensive support.
Keywords
Adolescence is a critical developmental stage characterized by significant physical, emotional, and social changes. 1 –3 Cancer adds complexity to this already challenging period, creating risks for poorer long-term health and psychological outcomes compared with peers. 4 –6 Education attainment is a robust determinant of long-term health and social outcomes, such as longevity, lower rates of chronic health conditions, employment, and civic engagement. 7,8 Yet, adolescents diagnosed both in childhood and adolescence are at risk of poorer education attainment across all levels of education attainment and many require increased education support. 9 With advancements in cancer treatment, most children and adolescents now survive their cancer, 10,11 making the intersection of cancer with educational trajectories in adolescence a key focus for research aiming to support long-term outcomes.
Keeping young people engaged and supported in school after a cancer diagnosis is imperative, yet research about their specific experiences during high school is lacking. Youths affected by cancer in high school form a diverse group. They are diagnosed either in childhood or adolescence, with each group facing a unique set of challenges shaped by their developmental stage at diagnosis and proximity to treatment. Yet, research often combines these cohorts, risking oversimplifying their distinct academic and social needs, particularly during 1 high school. 12 For example, adolescents diagnosed in childhood, while cancer-free in adolescence may experience “hidden” challenges at this time, such as ongoing health concerns and late effects, 13,14 need for academic and cognitive accommodations, 15 and challenges with social functioning. 16 In contrast, recently diagnosed adolescents face more immediate challenges, such as acute side-effects of treatment on cognition, physical functioning and body-image, 1 prolonged absences, 17,18 social disconnection and impact on senior high school. 17 These differences highlight the nuanced needs of each group during adolescence.
Education support during adolescence must address the diverse challenges and experiences based on age at diagnosis. Therefore, to better understand the specific academic and social challenges for this cohort, we aimed to examine and compare the high school experiences of adolescents based on age at cancer diagnosis, either during childhood or adolescence, from both youth and parent perspectives.
Methods
Participants
Youths meeting the following criteria, were eligible to participate; (i) aged 0–18 years at cancer diagnosis (childhood diagnosis: aged 0–11 years and adolescent diagnosis: aged 12–18 years, at diagnosis), (ii) currently aged 12–18 years, or were currently in high school (for further information on the Australian education system see Supplementary Data) or had completed high school in the past 5 years, (iii) fluent in English, (iv) were not experiencing psychological risk (e.g., suicidal ideation, complex family dysfunction), and (v) were medically stable. Criteria IV–V were determined by the medical team, based on their clinical judgment. Parents and legal guardians who had children that fit the criteria listed above were eligible to participate. Youth who completed high school in the past 5 years were included in our sample to examine the experience of school completion without burdening youths currently undergoing senior examinations. Youths and parents were not dyads. We aimed to recruit a sample of 20 youths and parents, based on consultation with clinicians regarding the number of eligible youths to facilitate a purposive sampling strategy.
Materials
Background demographic questionnaire. Youths and parents completed a background demographic questionnaire (e.g., age, sex, education, current year at school or education level, cancer diagnosis, age at diagnosis, and number of terms absent from school).
Interview schedule. We developed a semistructured interview schedule based on our research aims and through consultation with experts (oncology hospital-school liaison teachers, adolescent neuropsychologists, and psychologists), and an adult survivor of childhood cancer and relapse in adolescence. We asked open-ended questions about “school life” (see Supplementary Data), which was defined for participants as any aspect of school such as classes, subjects, learning, friendships, sports, extra-curricular activities, and hobbies, allowing participants to explore multifaceted aspects of school. The focus of the interviews was youths’ experiences during high school.
Procedure
The Sydney Children’s Hospitals Network Human Research Ethics Committee granted ethics approval for this study (LNR/16/SCHN/454).
We recruited participants from cancer centers at the Sydney Children’s Hospital, Randwick and Sydney Youth Cancer Service at the Prince of Wales Hospital. We used purposive sampling to recruit participants based on cancer diagnosis, age at diagnosis and sex. Clinical nurse consultants screened patients and survivors against eligibility criteria. The lead author (M.A.B.) discussed the study with eligible participants in-person or via telephone. Those interested in participation were provided with an invitation letter, and information and consent form. Adolescents aged <16 years at the time of the interview provided assent and all others provided consent.
All consenting participants completed demographic questionnaires before the interview. We conducted interviews between February and September, 2020. We offered participants the option to complete face-to-face (three youths, two parents) or telephone interviews. Due to COVID-19 restrictions, all subsequent interviews were telephone-based (15 youths, 10 parents). Interviews were conducted by M.A.B. and lasted approximately 30–60 minutes.
Data analysis
We used IBM SPSS Statistics (Version 27.0) for descriptive statistics. Interviews were audio-recorded, transcribed verbatim by M.A.B. and J.L. (see acknowledgments) and organized using NVivo software. 19 We followed a six-phase thematic analysis 20 to construct codes and themes and followed qualitative analysis reporting guidelines. 21 Authors (M.A.B., C.E.S., C.L.) performed an inductive thematic analysis. C.E.S. and C.L. had no prior relationship with participants. M.A.B. had prior contact through conducting consent procedures, interviews, and preparing de-identified transcripts. Each familiarized themselves with transcripts and kept separate notes throughout the analytic process. These authors have a combined 16 years’ experience in pediatric research focusing on chronic illness and traumatic brain injury, and one author is a survivor of child and adolescent cancer. The authors met to discuss initial interpretations of the data and preliminary codes. Subsequently, the authors further refined codes and identified preliminary candidate themes independently. The authors met to discuss and refine themes and the unifying concepts. Themes were developed separately for youths and parents to contrast unique viewpoints.
Results
In total, 25 youths and 20 parents were identified and contacted to participate. Seven youths and 7 parents were lost to follow-up after being contacted a maximum of three times. We recruited 18 youths (8 diagnosed in childhood and 10 in adolescence), and 13 parents of youths (8 parents children were diagnosed in childhood and 5 diagnosed in adolescence; see Table 1). Among parents, 75% in the childhood-diagnosis group and 100% in the adolescent-diagnosis group were mothers. One youth and their parent completed a phone interview together. Results are displayed across the cancer and school continuum (see Fig. 1) and by developmental stage at diagnosis (See Fig. 2).
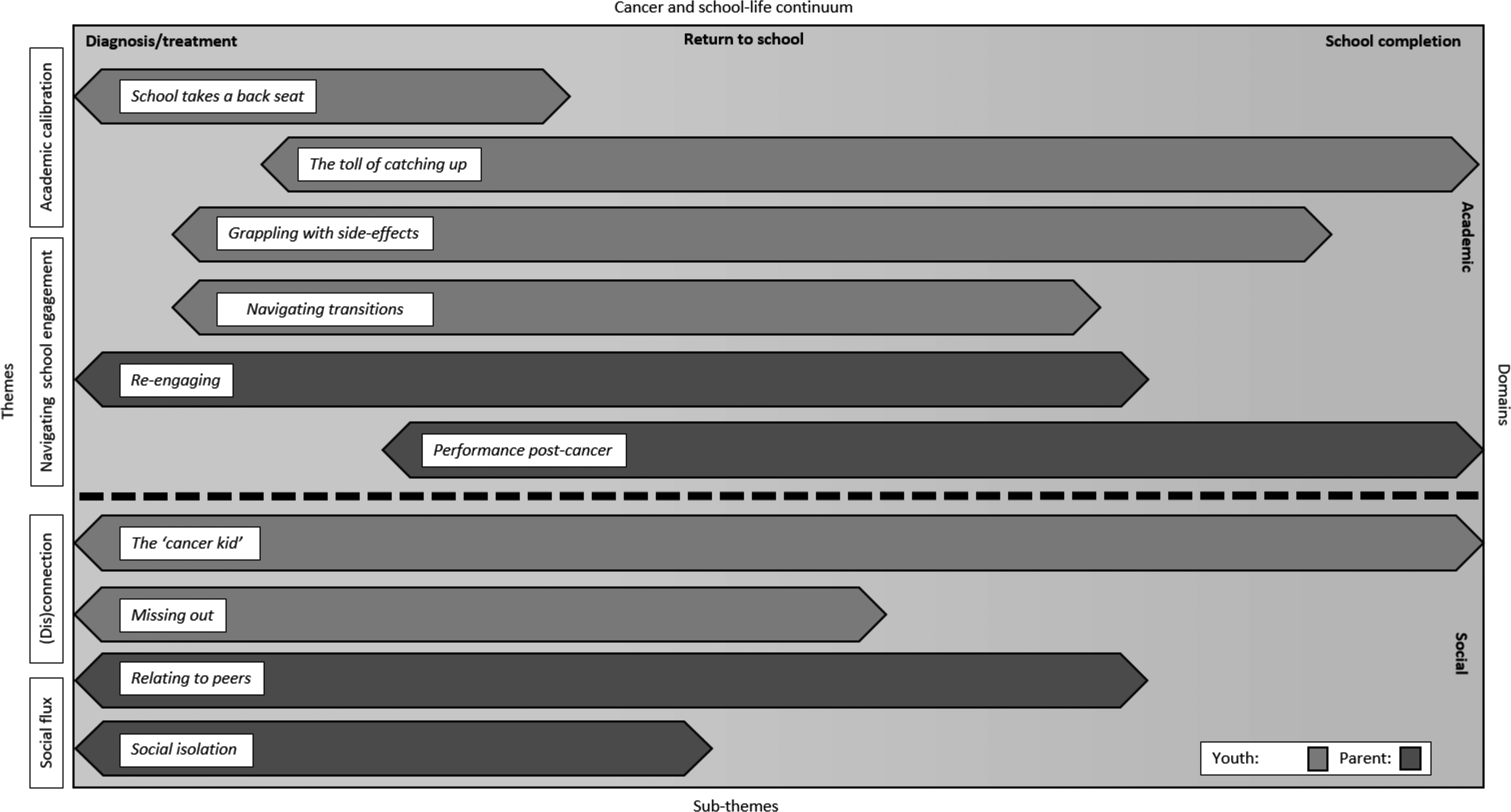
Diagrammatic representation of themes. Themes (left y-axis) and corresponding sub-themes (lower x-axis) are divided by academic and social domains (right y-axis). The relevance of themes and sub-themes are plotted across milestones of the cancer and school life continuum (upper x-axis), which progress across time, not necessarily linearly, from cancer diagnosis and treatment, return to school, until school completion.
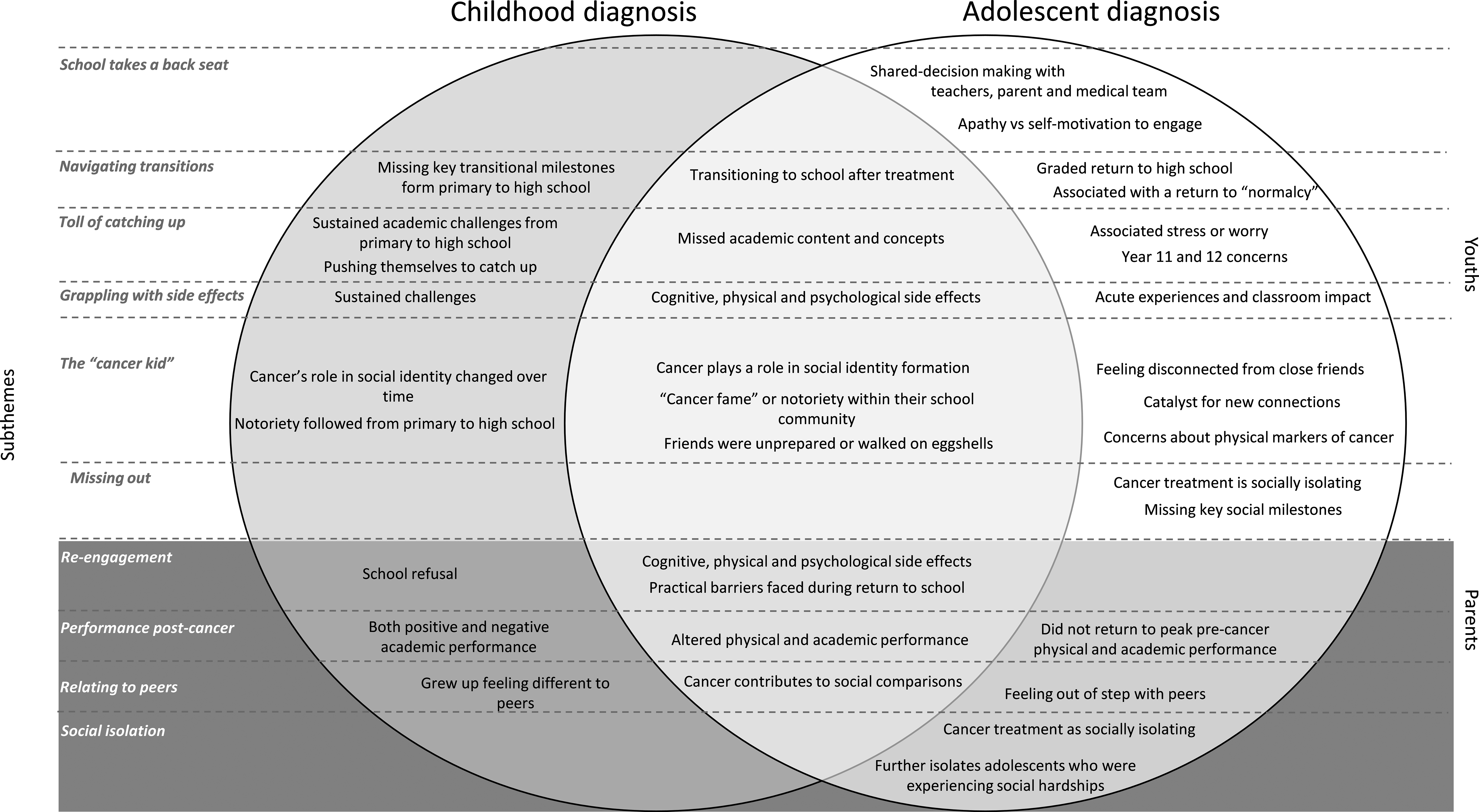
Comparison of youths’ experiences in high school by age at diagnosis.
Participant Demographic, Educational, and Clinical Characteristics
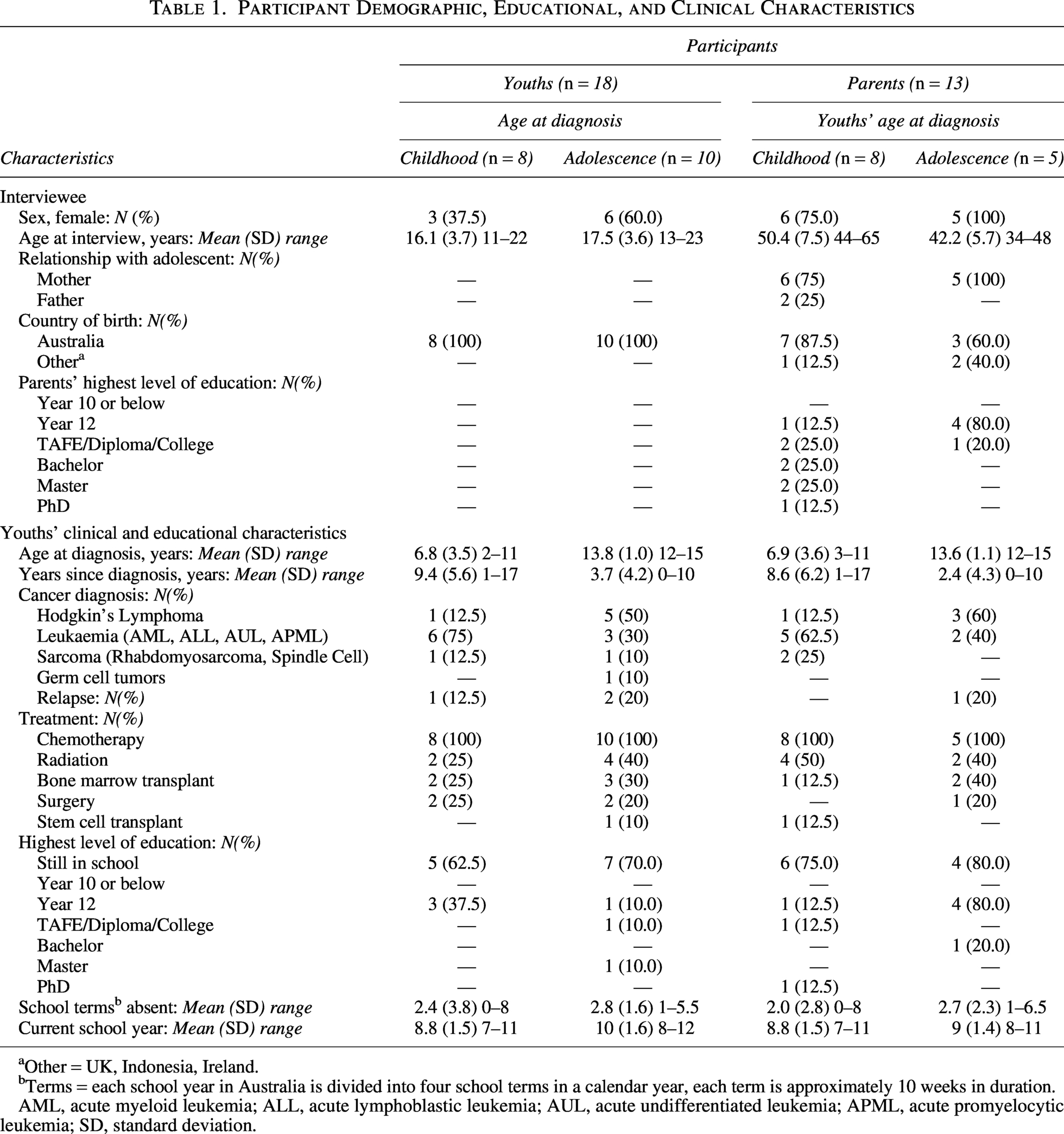
Other = UK, Indonesia, Ireland.
Terms = each school year in Australia is divided into four school terms in a calendar year, each term is approximately 10 weeks in duration.
AML, acute myeloid leukemia; ALL, acute lymphoblastic leukemia; AUL, acute undifferentiated leukemia; APML, acute promyelocytic leukemia; SD, standard deviation.
Thematic analysis: Youths
The analysis produced two main themes: “academic recalibration” and “(dis)connection” (see Table 2).
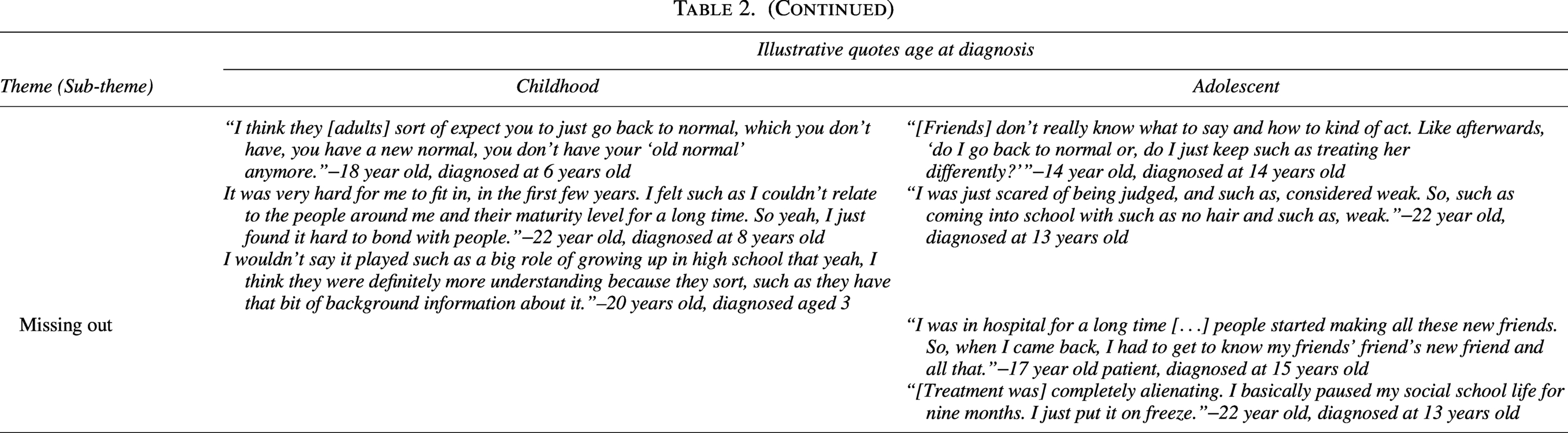
Illustrative Quotes from Youth Interviews
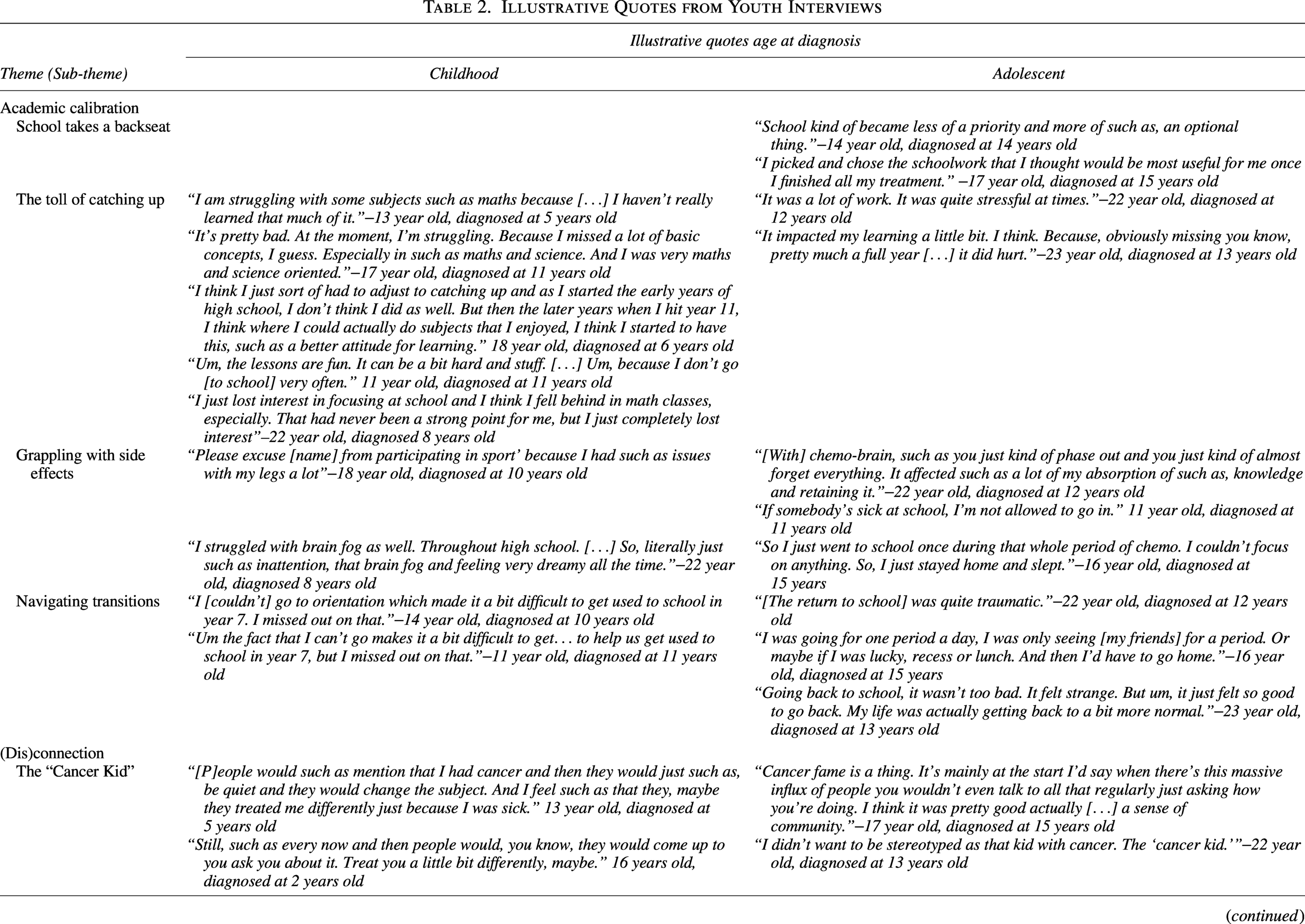
Theme 1. Academic calibration
All youths experienced some degree of emotional and practical adjustments to academic aspects of school life, such as academic performance, schoolwork and attendance, from cancer diagnosis throughout school.
School takes a back seat
For youths diagnosed in adolescence only, school took a back seat during cancer treatment and before returning to high school full-time. Some youths described an apathy toward schoolwork, due to cognitive, psychological, or physical limitations. But most believed that during treatment, schoolwork was simply no longer a “priority” or was secondary to their health. Youths came to this conclusion on their own, or with encouragement from family, school or hospital-based teachers, or medical team.
Navigating transitions
Experiences of attending school during treatment, or transitioning back to school after treatment, were a focal point of youths’ experiences.
Adolescence. Youths predominantly reported a graded return to school to assist in the transition while completing treatment. For most youths, transitioning back to school was associated with their adjustment to “normalcy,” “routine,” and getting back into “the full swing” of things. Others shared how grappling with side-effects and disconnection from friends during the transition back to school was “hard” or in some cases, “traumatic.”
Childhood. Youths treated at the end of primary school or who continued treatment into the initial stages of high school reported a feeling out of sync with high school routines.
The toll of catching up
The majority of youths discussed the emotional impact of missed academic content due to hospitalization.
Adolescence. When faced with catching up, many felt “worried” or “stressed,” with one adolescent recounting that falling behind felt “traumatic.” Adolescents also reported having schoolwork on their mind during treatment — particularly those who were in senior school or were self-motivated to continue with their schoolwork. For these adolescents, the threat of missed assessment deadlines, exams and subject content, particularly mathematics and science, weighed on their mental health. This was particularly poignant for youths navigating senior high school from hospital.
Childhood. Youths felt that missing fundamental concepts in primary school continued to negatively impact their academic performance in high school. Although a few shared that they pushed themselves to eventually regain ground academically and meet the level of peers mid-way through high school.
Grappling with side effects
Almost all youths struggled with cognitive and physical side effects of cancer and treatment, such as difficulties with concentration, memory, and learning, including worsened attention deficit hyperactivity disorder (ADHD) symptoms.
Adolescence. Youths described the acute effects on their schooling, highlighting challenges in maintaining focus, managing fatigue, and coping with physical limitations such as reduced immunity and mobility. Some spoke about the experience of attending school during treatment without hair, with a range of emotional undertones—some feeling neutral and some self-conscious. Many expressed frustration over the psychological toll, particularly the difficulty in explaining their absence or inability to participate in sports and extracurricular activities they once loved.
Childhood. Youths shared experiences of how side-effects persisted over time, impacting them well into high school. Cognitive challenges, such as difficulty retaining information, were common, as were physical limitations. One youth who had a nasogastric tube and frequent absences for medical procedures described feeling self-conscious with long-term classroom support.
Theme 2. (dis)connection
Youths explored how cancer impacted their identity and connection to peers and the school community.
Adolescence. Some, mostly male youths, highlighted their concerns about physical markers of cancer that they equated to weakness, such as baldness, weight gain, or physical frailty, when faced with reintegrating socially to the school environment. Many spoke about how they navigated their “cancer fame,” or a newfound notoriety at school, with some sharing that it caused close friends to act differently toward them. Some youths felt fundamentally different to peers due to cancer. Some saw cancer as a catalyst for new connections with school peers, making them stand out in a positive way. Youths, who were now young adults, spoke about how they now viewed their experiences of being the “cancer kid” more compassionately and wished they had sought support for negative feelings during high school.
Childhood. For youths diagnosed in childhood, many felt that the notoriety of having had cancer followed them from primary school into high school continuing to differentiate them from their peers. Many of these adolescents shared a reluctance toward cancer as a social identity, preferring not to be defined by cancer. Some spoke about differences in maturity between themselves and peers, citing that they grew up fast and that, in comparison with peers focusing on trivial things.
Missing out
Many youths diagnosed in adolescence only felt that they had “missed out,” were socially isolated or failed to keep up with their peers’ social lives during treatment and transition back to school. This included peers’ new friendships, daily rituals such as “train rides into school,” and important milestones such as high school graduation. Many shared that treatment was especially isolating, particularly for those who underwent bone marrow transplants and significant immunosuppression.
Thematic analysis: Parents
The analysis of parent interviews produced two themes, “navigating school engagement” and “social flux” (see Table 3).
Illustrative Quotes from Parent Interviews

Theme 1. Navigating school engagement
Most parents spoke about the impact of cancer on their child’s engagement with school from diagnosis through to school reintegration and completion. With a strong focus on academic achievement and extracurricular interests, parents shared obstacles to re-engaging in school life and changes in performance.
Re-engaging
Many parents spoke about the process of transitioning, or re-engaging, in school life during or after treatment ended.
Adolescence. Parents reported the impact of cognitive and physical side effects of cancer treatment such as “chemo brain,” inattention and fatigue. Many reported practical barriers, including arranging transport and navigating part-time attendance.
Childhood. One parent of an adolescent recently transitioning to high school reported their child’s school refusal, attributing this to their child’s apprehension about social reintegration.
Performance post-cancer
Adolescence. Changing or altered academic and physical capacity and performance featured often in parents’ reports of their children navigating school after cancer. Parents felt their child did not perform as well as before cancer in both academics and physical activities. For example, not returning to their peak physical performance with elite sporting and dance.
Childhood. Parents reported mixed views on their child’s academic progress. Some were impressed with their child’s progress, especially after missing school content. Some lamented that academic challenges were ongoing and that they would never know the full impact of cancer on their child’s academic and social outcomes, owing to diagnoses in early childhood and before school.
Theme 2. Social flux
Social flux was characterized by parents’ perceptions of their child’s changing social functioning, including how cancer impacted their social identity and socialization over time.
Relating to peers
Parents reported that cancer contributed to their child’s social comparisons, beginning as early as primary school and often evolving over time.
Adolescence. Most parents reported situations where their child felt uncomfortable or out of step with their peers. Some cited that friends were overly friendly or behaved out of character, making their child feel uncomfortable or singled out. Parents surmised that their child’s friends were not adequately prepared to cope with changes to friendships due to cancer.
Childhood. Parents shared that their children grew up feeling that physical markers of cancer made them “different” to peers and siblings.
Social isolation
Parents of youths diagnosed in adolescence only reported that their child felt a profound sense of social isolation while undergoing cancer treatment and before returning to school. Most notably, compulsory isolation for bone marrow transplant and lowered immunity further isolated them from their social world and created further social setbacks for children with pre-existing difficulty socializing.
Discussion
The objective of this study was to characterize and contrast high school experiences of youths diagnosed with cancer in childhood and adolescence. Common themes emerged irrespective of the age at diagnoses, reported by youths (Academic Calibration and (Dis)connection) and parents (Navigating School Engagement and Social Flux). Nevertheless, our study revealed distinct subthemes: Missing Out, Social Isolation and School Takes a Back Seat for youths diagnosed in adolescence, but not childhood.
A pronounced difference between youths centered on social isolation, both as a physical and social separation from peers. Youths diagnosed during high school and their parents reported that youths missed day-to-day social interactions, new friendships and shared milestones such as graduation, citing prolonged hospitalizations and immunosuppression as key contributors. This experience is well supported in the literature, 17,22,23 with prolonged school absences ranging from 40-days up to a year 1 and with up to 40% of adolescents reporting changes to friendships after their cancer diagnosis. 24 Given the marked shift in focus from family to burgeoning peer networks during adolescence, 25,26 these disruptions are associated with heightened psychological distress and reduced quality of life. 27 –29 While social isolation can lessen with time and reintegration to school and social settings, 28 some adolescents continue to experience a sense of isolation from peers well into adulthood. 30 Given these differing long-term trajectories, psychosocial guidelines have highlighted that support for social connection from diagnosis throughout school is paramount for adolescents. 31
Academic challenges were common to youths regardless of age at diagnosis, but differed in nature and trajectory. For youths diagnosed during adolescence, disruptions to learning were acute, often coinciding with key academic milestones such as senior assessments. While the initial de-emphasis on academics supported their recovery, it later caused distress related to academic performance and catching up. 1 In contrast, youths diagnosed in childhood generally experienced long-term academic difficulties stemming from missed foundational learning and the cumulative effects of treatment-related cognitive and physical late effects, particularly in content-heavy subjects such as math and science. 32 Aligning with existing literature, these trajectories underscore the need for tailored academic support for both the acute disruptions of treatment and the enduring challenges emerging over time.
Identity development is a central focus of adolescence, 33 with both youths and parents reporting cancer’s profound influence on social identity formation and connectedness to peers. Consistent with previous research, adolescents diagnosed during high school described cancer as a defining aspect of their identity, shaping how they viewed themselves and were perceived by peers. 34,35 By contrast, those further from diagnosis, including youths diagnosed in childhood and young adults diagnosed in adolescence, saw cancer as a more nuanced or peripheral component of their identity. 36 Together, these contrasting perspectives underscore the dynamic nature of identity development during adolescence, reflecting adjustment to illness over time. 36 –38 For adolescents with a foreclosed social identity (e.g., a permanent sense of otherness related to chronic illness), 37 rigidity in identity formation may lead to challenges with self-esteem and social and emotional well-being into adulthood. 39 However, some youths diagnosed in adolescence experienced their cancer identity as a protective factor for social connectedness, primarily as a catalyst for new friendships and generating a sense of school community. Indeed, there is preliminary evidence that interventions for adolescent and young adult cancer patients focusing on social connectedness with peers and meaning-making may relieve depressive symptoms 40 and support an integrated identity post-cancer. 41,42
Strengths and limitations
To our knowledge, this study was the first to report on the similarities and differences in high school experiences of adolescents diagnosed with cancer in either childhood or adolescence from both youth and parent perspectives. Our study highlighted the differences in academic and social aspects of school life, and the evolution of these challenges over time. However, while we aimed for a purposive sample to account for varied diagnoses, age and sex, our sample included only English speakers. Such exclusion has the potential to impact scientific discourse, with minorities less likely to have access to scientifically informed support services. 43,44 There is also evidence that social determinants (e.g., socioeconomic status, parental health, available support) are related to developmental vulnerability. 45 Future research should include culturally inclusive samples and explore the role of social determinants on developmental risk related to age at diagnosis.
Clinical implications and future research
This study highlights the need for developmentally informed, tailored support for adolescents affected by cancer during high school, that considers the timing of diagnosis. Adolescents diagnosed during high school require early support to maintain peer connections, manage impact on identity, and navigate acute academic stress—particularly during senior school. Our results also support ongoing academic monitoring of adolescents diagnosed in childhood, to address the cumulative impact of early learning disruptions in childhood and treatment-related late effects, such as keeping families engaged in comprehensive survivorship care. 46 Comprehensive support should also seek to address social connectedness and identity support, to enhance well-being and social outcomes. 31,40 –42 Collaboration between adolescents, families, medical teams, and educators is essential to deliver comprehensive support that promotes reintegration and long-term well-being. Future research should focus on co-designing interventions with these stakeholders, prioritizing culturally inclusive approaches.
Conclusion
This study highlights shared and distinct academic and social challenges experienced by adolescents affected by cancer during high school, shaped by age at diagnosis. Our findings reinforce the need for developmentally tailored, ongoing, and collaborative support.
Authors’ Contributions
M.A.B.: Conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, visualization, and project administration. S.L.: Conceptualization, writing—review and editing, project administration, and supervision. C.L.: Formal analysis and writing—review and editing. C.E.S.: Formal analysis and writing—review and editing. S.J.E.: Writing—review and editing, and project administration. C.E.W.: Funding acquisition and writing—review and editing. U.M.S.D.: Writing—review and editing. R.J.C.: Funding acquisition and writing—review and editing. G.M.M.: Funding acquisition and writing—review and editing. A.L.: Funding acquisition and writing—review and editing. B.D.: Funding acquisition and writing—review and editing. T.W.: Funding acquisition and writing—review and editing. A.C.: Funding acquisition. P.F.: Funding acquisition and writing—review and editing. C.R.D.L.: Funding acquisition and writing—review and editing. B.B.: Project administration and writing—review and editing. D.D.: Project administration and writing—review and editing, C.O.: Project administration and writing—review and editing. F.M.: Project administration and writing—review and editing. J.E.F.: Conceptualization, writing—review and editing, supervision, project administration, and funding acquisition.
Footnotes
Acknowledgments
The authors would like to thank Jeremy Lu for his contribution to this research and the youths and parents who shared their experiences.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
Ms Mary A. Burns’ PhD is supported by the Kids Cancer Project and the Kids Cancer Alliance. This research is funded by a research grant, awarded to Dr Joanna E. Fardell by The Kids Cancer Project. Dr Fardell is a Maridulu Budyari Gumal (SPHERE) Cancer CAG Senior Research Fellow and is supported by a Cancer Institute NSW Research Capacity Building Grant (2021/CBG003). Dr Sarah Ellis is supported by the Luminesce Alliance – Innovation for Children’s Health, and an Early Career Fellowship from the Cancer Institute NSW (ID: 2025/ECF2619). Claire E. Wakefield is supported by the NHMRC of Australia (APP2008300). Dr Ursula M. Sansom-Daly is supported by an Early Career Fellowship from the Cancer Institute NSW (ID: 2020/ECF1163). During the course of this research, the Behavioural Sciences Unit received support from the Kids with Cancer Foundation. These funding bodies did not have any role in the study, nor did they have a role in the writing of the article or the decision to submit it for publication.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.