
Abstract
Purpose:
Male childhood cancer survivors (CCS) are at increased risk of hypogonadism, which may be overlooked due to subtle symptoms. Early detection of male hypogonadism remains challenging. In Japan, lacking a nationwide surveillance system for gonadal dysfunction in CCS, few studies focus on male CCS. This study aimed to prospectively identify compensated primary hypogonadism (cPH) among male CCS using a comprehensive medical checkup system.
Methods:
We prospectively recruited CCS aged 18 and older who had been diagnosed with pediatric cancer over 10 years ago and untreated for more than 5 years. Physical checkup and mental health examination were conducted for both CCS and healthy CCS siblings, and analyzed data from male participants. We defined cPH if their testicular volume was 10 mL or lower and/or the follicle-stimulating hormone level was greater than 10 IU/L.
Results:
Among 30 CCS aged 19–41, 12 were identified as having cPH. Factors significantly associated with cPH in CCS included receiving a cyclophosphamide equivalent dose greater than 7.5 g/m2, experiencing secondary cancers, and older age at medical checkup. CCS with cPH exhibited higher fasting blood sugar and elevated luteinizing hormone levels. Furthermore, CCS with cPH reported significantly lower mental component summary scores and reported greater psychological distress.
Conclusion:
Despite the limited sample size, our preliminary findings suggest that this surveillance approach may help identify male CCS at risk for hypogonadism. These survivors warrant monitoring for gonadal dysfunction and associated complications.
Keywords
Introduction
Improved treatments have increased the number of childhood cancer survivors (CCS), who face a significantly higher risk of hypogonadism than the general population.1,2 Unlike in females, where menstrual changes aid diagnosis, early detection in males is challenging because symptoms are often subtle, ranging from metabolic issue to emotional distress.3,4 Testicular volume assessment is a noninvasive surrogate for gonadal function when semen analysis is impractical, though it may be overlooked and lacks direct insight into spermatogenesis. Serum follicle-stimulating hormone (FSH) helps mitigate this limitation. Although semen analysis is the gold standard, its sensitive nature precludes universal surveillance. Male hypogonadism can be broadly classified into primary hypogonadism (PH), caused by testicular dysfunction, and central hypogonadism (CH), resulting from hypothalamic–pituitary impairment. These entities differ in their hormonal profiles and physical findings, which has important implications for surveillance strategies in CCS. The definition of PH is often based on laboratory findings of decreased testosterone and/or elevated luteinizing hormone (LH). 2 However, gonadal function status changes over time as CCS age, and previous reports have found that some initially unaffected participants developed hypogonadism upon follow-up. 5 A challenge also remains for CCS regarding who should be followed up thoroughly for gonadal function to detect hypogonadism.
In Japan, a nationwide and organized follow-up system for CCS, including surveillance for gonadal dysfunction, has not yet been established. To address this gap and better understand the status of gonadal dysfunction among Japanese male CCS, we conducted a prospective study at a single institution. This initial investigation aims to provide foundational data that can inform the development of a nationwide surveillance system in the future.
We hypothesized that early identification of cases of compensated primary hypogonadism (cPH) would allow for prompt intervention to address related complications. Our goal was to prospectively identify CCS with cPH through a comprehensive medical checkup system in order to determine those who require thorough follow-up for their gonadal function.
Methods
Study design and participants
The current study included male participants aged 18 and older who had been diagnosed with pediatric cancer more than 10 years ago and had not received treatment for their primary disease for over 5 years. Recruitment was conducted from December 2015 to March 2019. All participants underwent a comprehensive physical and mental health examination. 6 Additionally, healthy male siblings aged 18 or older were recruited as a control group and underwent the same examination. All participants completed a self-administered questionnaire that included psychosocial questions and questions about fertility. This study is part of a long-term cohort study of CCS, the St. Luke’s Childhood Cancer Survivors Cohort Study (LUKE Cohort Study), which is a follow-up system utilizing a comprehensive medical checkup system. 6 The study protocol was approved by the Ethics Committee of St. Luke’s International Hospital (16-R-061), and informed consent was obtained from all participants prior to enrollment.
Data collection
Medical records were used to retrospectively examine various factors, including age at onset or at the time of study, diagnosis, treatment details, height, weight, Tanner stage for pubic hair, testicular volume, fasting blood sugar, and endocrine parameters such as LH, FSH, and testosterone levels. Health-related quality of life (QOL) was assessed using the 8-item Short Form Health Survey (SF-8), 7 and psychological distress was evaluated using the Kessler Psychological Distress Scale (K10). 8 Participants also completed 11 nonvalidated, exploratory items regarding fertility concerns (e.g., anxiety) off-site. No compensation was provided, though the checkup was free.
Reference values and definitions
The following criteria were used as reference values: LH > 0.7 IU/L, FSH 2.0–10 IU/L, and testosterone >1.3 ng/mL. Testicular volume was assessed for each testis. Preserved testicular volume was defined as ≥12 mL in at least one testis, based on the reported ≤24 mL total volume risk thereshold. 1 Cases with ≤10 mL in both testes was classified as high-risk. For anti-Müllerian hormone (AMH) reference values, we referred to past literature based on the participant’s age: age 15 and over but under 20 (2.26–16.85 ng/mL), age 20 and over but under 39 (2.53–12.73 ng/mL), and age 39 and over (1.72–12.26 ng/mL).9,10 Hypogonadism was defined as gonadal dysfunction encompassing both biochemical hypogonadism (low testosterone: ≤1.3 ng/mL) and cPH (primary testicular impairment, regardless of testosterone levels). Low testosterone alone was not considered synonymous with hypogonadism in this study. Specifically, cPH was defined by elevated FSH levels and/or reduced testicular volume.1,3 Testosterone was excluded from the cPH criteria to avoid underestimating early or subclinical gonadal dysfunction in relatively young CCS, as reliance on testosterone alone lacks sensitivity in this population. CH was defined when both LH and FSH levels were below the reference range.
Chemotherapy dose calculation
For CCSs, the cumulative doses of chemotherapy agents were calculated individually. The doses of alkylating agents were converted to cyclophosphamide equivalent doses (CEDs) per past literature. 11 The thresholds for CEDs were selected based on previous studies reporting that doses ≥4 g/m2 may increase the risk of Leydig cell dysfunction, whereas doses ≥7.5 g/m2 are associated with long-term gonadal damage and infertility.12–14
Statistical analysis
All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University), a modified version of R Commander. 15 Categorical variables are presented as counts and percentages. Fisher’s exact test was used to assess differences between the two cohorts (CCS vs. healthy controls, cPH vs. no PH [excluding CH survivor], low testosterone levels vs. normal testosterone levels) for categorical variables. The Mann–Whitney U test was used to compare continuous variables. A p value of <0.05 was considered statistically significant. Given the exploratory nature of this study, a formal a priori power analysis was not performed.
Results
Participant characteristics
A total of 30 CCS and 12 healthy controls were analyzed (Table 1). Primary diagnoses included acute lymphoblastic leukemia (ALL, n = 19), neuroblastoma (n = 4), and intracranial germinoma (n = 2). Most CCS (n = 26, 89.7%) received alkylating agents, while 5 (17.2%) received platinum agent. Nine patients underwent surgery, including two who had neurosurgery and one who had an orchiectomy. Fourteen patients received radiation therapy: one underwent total body irradiation, 10 received cranial irradiation, including prophylactic or therapeutic whole-brain irradiation (n = 7), craniospinal irradiation (n = 2), and extended ventricular irradiation (n = 1), all of which involved exposure of the hypothalamic–pituitary axis. Three received testicular irradiation. Two patients with ALL received both craniospinal and testicular irradiation. Five patients received hematopoietic stem cell transplantation.
Characteristics of CCS and Healthy Control
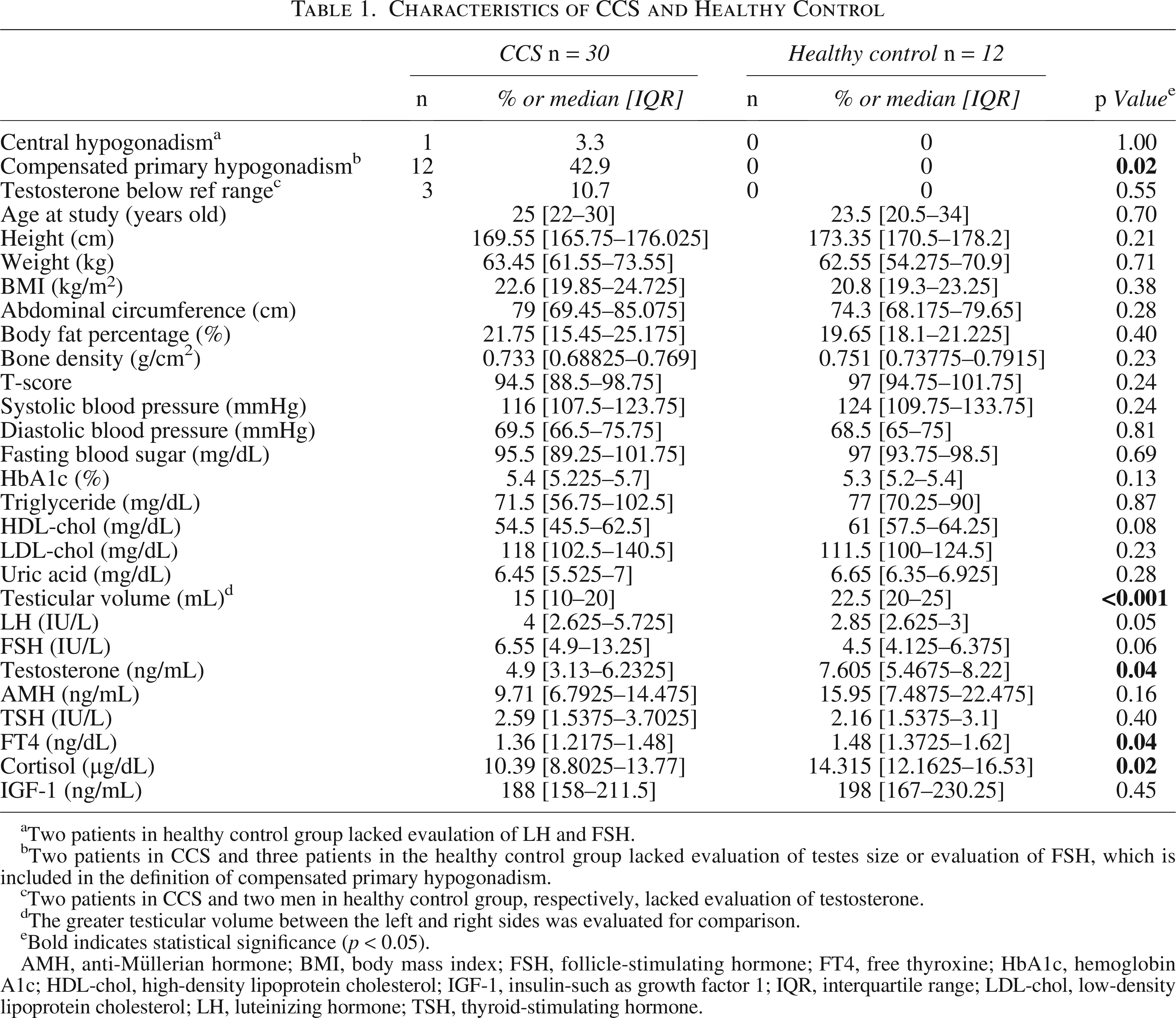
Two patients in healthy control group lacked evaulation of LH and FSH.
Two patients in CCS and three patients in the healthy control group lacked evaluation of testes size or evaluation of FSH, which is included in the definition of compensated primary hypogonadism.
Two patients in CCS and two men in healthy control group, respectively, lacked evaluation of testosterone.
The greater testicular volume between the left and right sides was evaluated for comparison.
Bold indicates statistical significance (p < 0.05).
AMH, anti-Müllerian hormone; BMI, body mass index; FSH, follicle-stimulating hormone; FT4, free thyroxine; HbA1c, hemoglobin A1c; HDL-chol, high-density lipoprotein cholesterol; IGF-1, insulin-such as growth factor 1; IQR, interquartile range; LDL-chol, low-density lipoprotein cholesterol; LH, luteinizing hormone; TSH, thyroid-stimulating hormone.
Physical and endocrine outcomes
No significant differences were found in anthropometric markers, blood pressure, or metabolic profiles (total cholesterol, low-density lipoprotein [LDL] cholesterol, HDL cholesterol, and triglycerides) between CCS and controls (Table 1). However, CCS had significantly smaller testicular volumes than controls (median interquartile range [IQR]: 15 [10–20] mL vs. 22.5 [20–25] mL, p < 0.001). LH and FSH were marginally higher in CCS (median [IQR]: 4.0 [2.625–5.725] IU/L and 6.55 [4.9–13.25] IU/L, respectively) than in controls (2.85 [2.625–3] IU/L and 4.5 [4.125–6.375] IU/L, respectively), with p-values of 0.05 and 0.06, respectively. Free thyroxine and cortisol levels were significantly lower in CCS (p-values 0.04 and 0.02, respectively), whereas AMH levels did not differ significantly between the groups. Despite the observed differences in testicular volume and endocrine parameters, all participants were at Tanner stage 5, except for one participant in the CCS group, who was at Tanner stage 4 and exhibited a low testosterone level.
Prevalence and characteristics of cPH
Definitions of cPH and CH were based on serum gonadotropin and testosterone levels, as described in the Methods section. Twelve CCS were identified to have cPH (Table 2). None of the healthy controls met the criteria for cPH. One CCS with CH was excluded from further sub-analysis. CCS who received a CEDs greater than 7.5 g/m2 were significantly more likely to exhibit features of cPH (p = 0.002), whereas no significant difference was observed at the 4 g/m2 threshold (p = 0.67). There was only one CCS who underwent orchiectomy and three CCS who received testicular irradiation; all of these cases were diagnosed with cPH. However, these factors did not reach statistical significance. CCS who developed secondary cancers (such as bladder cancer, renal cancer, sigmoid colon cancer, or non-Hodgkin lymphoma) were also associated with cPH. At the time of medical checkup, CCS with cPH were significantly older (median age 30 years) compared to those without hypogonadism (median age 25 years, p = 0.009).
Characteristics of CCS with Versus Without Compensated Primary Hypogonadism (Excluding Central Hypogonadism)
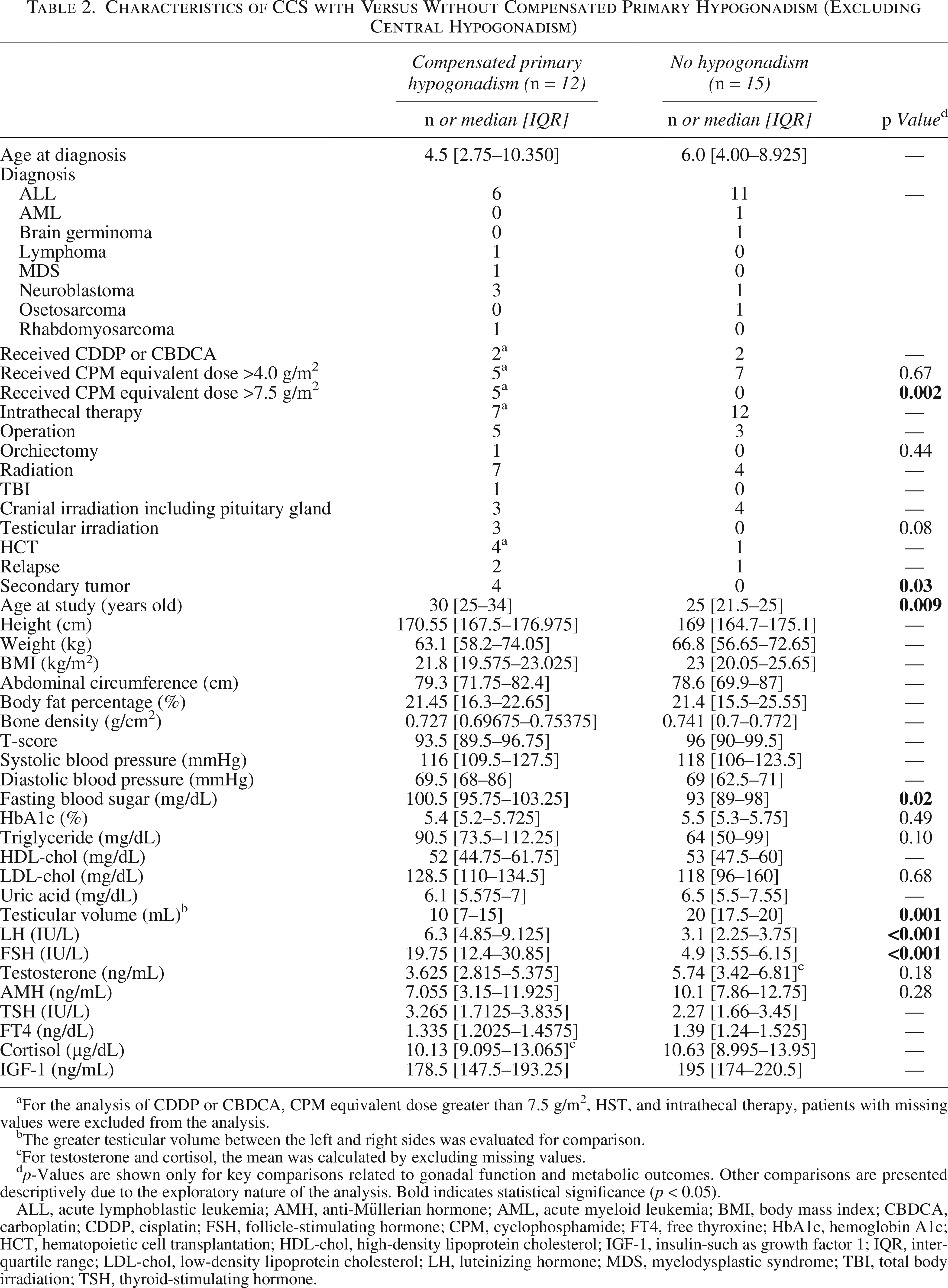
For the analysis of CDDP or CBDCA, CPM equivalent dose greater than 7.5 g/m², HST, and intrathecal therapy, patients with missing values were excluded from the analysis.
The greater testicular volume between the left and right sides was evaluated for comparison.
For testosterone and cortisol, the mean was calculated by excluding missing values.
p-Values are shown only for key comparisons related to gonadal function and metabolic outcomes. Other comparisons are presented descriptively due to the exploratory nature of the analysis. Bold indicates statistical significance (p < 0.05).
ALL, acute lymphoblastic leukemia; AMH, anti-Müllerian hormone; AML, acute myeloid leukemia; BMI, body mass index; CBDCA, carboplatin; CDDP, cisplatin; FSH, follicle-stimulating hormone; CPM, cyclophosphamide; FT4, free thyroxine; HbA1c, hemoglobin A1c; HCT, hematopoietic cell transplantation; HDL-chol, high-density lipoprotein cholesterol; IGF-1, insulin-such as growth factor 1; IQR, interquartile range; LDL-chol, low-density lipoprotein cholesterol; LH, luteinizing hormone; MDS, myelodysplastic syndrome; TBI, total body irradiation; TSH, thyroid-stimulating hormone.
Among CCS with cPH, fasting blood sugar levels were significantly higher (median [IQR]: 100.5 [95.75–103.25] mg/dL) compared to those without cPH (93 [89–98] mg/dL; p = 0.02), although values remained within the normal range. In contrast, HbA1c levels did not differ significantly between the two groups (5.4 [5.2–5.725]% vs. 5.5 [5.3–5.75]%; p = 0.49). Triglyceride levels showed a nonsignificant trend toward elevation in the former group (90.5 [73.5–112.25] mg/dL) compared to the latter (64 [50–99] mg/dL; p = 0.10). While low-density lipoprotein (LDL) cholesterol levels did not differ significantly between groups (128.5 [110–134.5] mg/dL vs. 118 [96–160] mg/dL; p = 0.68), a greater proportion of CCS with cPH (7 of 12; 58%) had borderline high levels (≥120 mg/dL) compared to those without cPH (6 of 15; 40%), although the difference was not statistically significant (p = 0.45). LH levels were elevated in CCS with cPH compared to those without hypogonadism (median [IQR]: 6.3 [4.85–9.125] IU/L vs. 3.1 [2.25–3.75] IU/L; p < 0.001). Other evaluation factors at the medical checkup, including testosterone and AMH levels, did not show significance.
Testosterone deficiency in CCS
Three CCS exhibited low testosterone level: two with cPH and one with CH, including two with ALL and one with brain germinoma (Table 3). Among these three CCS, none had a CEDs greater than 7.5 g/m2. One CCS had undergone an orchiectomy. Whole-brain irradiation was performed on all three CCS, and testicular irradiation was administered to two. Hematopoietic stem cell transplantation was performed in one CCS with low testosterone. Relapse frequency appeared to be higher in testosterone-low CCS (p = 0.02). At the time of medical checkup, age appeared to be higher in testosterone-low CCS (p = 0.01). Testicular volume was smaller in CCS with low testosterone levels (p = 0.007). FSH levels were higher in testosterone-low CCS compared to testosterone-normal CCS, but the difference was not statistically significant (p = 0.41). Additionally, high-density lipoprotein cholesterol and insulin-such as growth factor 1 levels appeared to be lower in testosterone-low CCS (p = 0.04 and p < 0.02, respectively). Two of these CCS had initiated testosterone replacement therapy; however, after transitioning to self-managed outpatient care, the clinic visits of one patient became less frequent due to a busy work schedule, and the other patient’s testosterone levels remained low despite reporting regular attendance. Given the small number of participants with low testosterone levels (n = 3), these findings should be interpreted with caution and regarded as exploratory.
Low Testosterone Cases in CCS
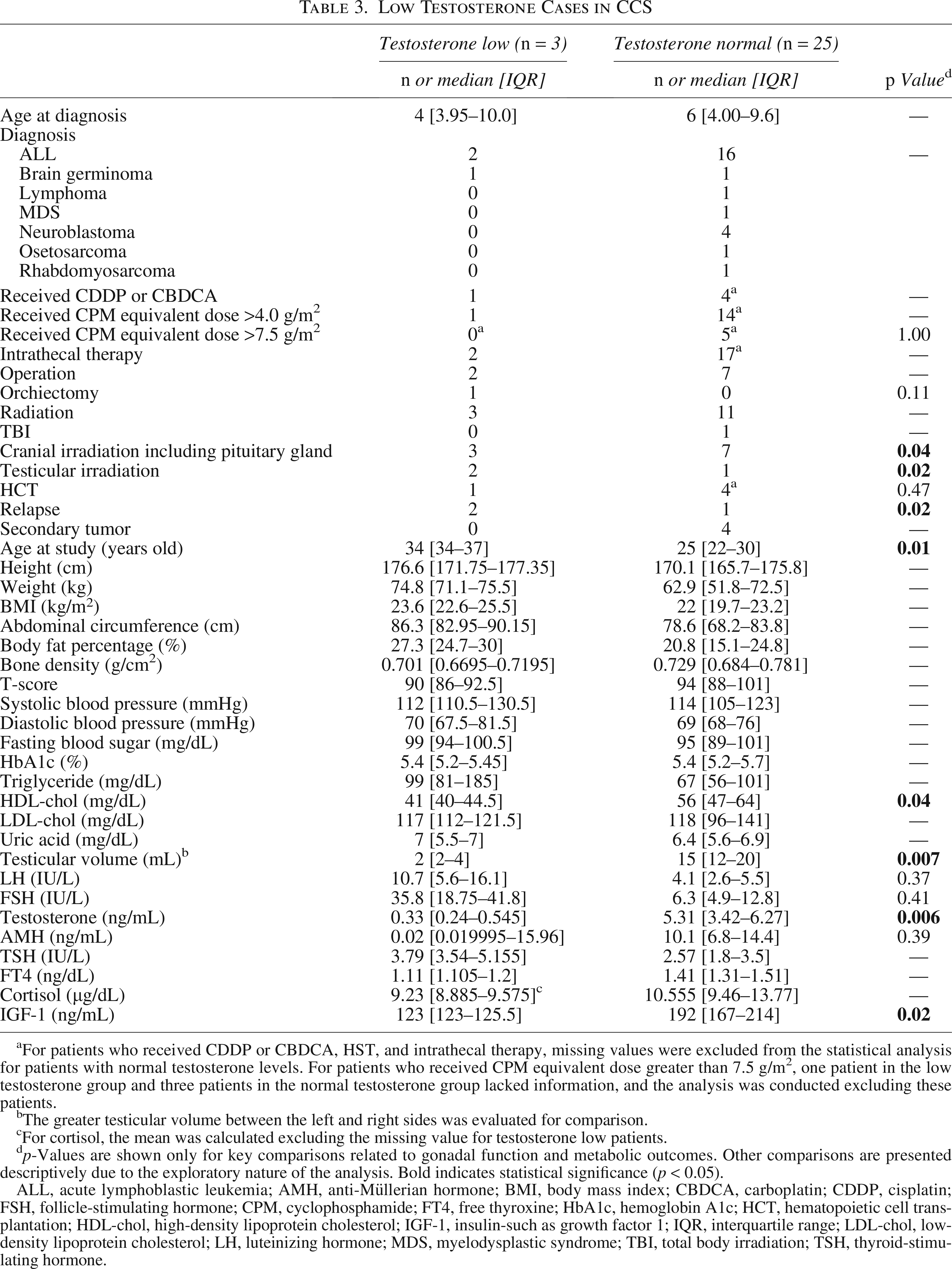
For patients who received CDDP or CBDCA, HST, and intrathecal therapy, missing values were excluded from the statistical analysis for patients with normal testosterone levels. For patients who received CPM equivalent dose greater than 7.5 g/m2, one patient in the low testosterone group and three patients in the normal testosterone group lacked information, and the analysis was conducted excluding these patients.
The greater testicular volume between the left and right sides was evaluated for comparison.
For cortisol, the mean was calculated excluding the missing value for testosterone low patients.
p-Values are shown only for key comparisons related to gonadal function and metabolic outcomes. Other comparisons are presented descriptively due to the exploratory nature of the analysis. Bold indicates statistical significance (p < 0.05).
ALL, acute lymphoblastic leukemia; AMH, anti-Müllerian hormone; BMI, body mass index; CBDCA, carboplatin; CDDP, cisplatin; FSH, follicle-stimulating hormone; CPM, cyclophosphamide; FT4, free thyroxine; HbA1c, hemoglobin A1c; HCT, hematopoietic cell transplantation; HDL-chol, high-density lipoprotein cholesterol; IGF-1, insulin-such as growth factor 1; IQR, interquartile range; LDL-chol, low-density lipoprotein cholesterol; LH, luteinizing hormone; MDS, myelodysplastic syndrome; TBI, total body irradiation; TSH, thyroid-stimulating hormone.
Psychosocial outcomes and quality of life
The SF-8 health-related QOL questionnaire revealed that CCS exhibited significantly greater bodily pain compared to healthy controls (p = 0.003) (Table 4). Conversely, healthy sibling control reported greater impairment in specific domains such as role physical, vitality, social functioning, and role emotional, although no significant differences were observed in the overall Physical and Mental Component Summary scores. The K10 psychological distress scale also indicated higher distress levels among healthy controls than CCS. When comparing CCS with and without cPH, those with cPH demonstrated significantly lower Mental Component Summary scores (p = 0.04). The K10 scale also showed greater psychological distress in CCS with cPH compared to those without (p = 0.02). In addition, based on responses to the exploratory fertility-related questionnaire, CCS with cPH expressed greater concern about potential future infertility, although the difference did not reach statistical significance (p = 0.06).
Health-Related Quality of Life (SF-8) and Psychological Distress (Kessler 10) in Childhood Cancer Survivors
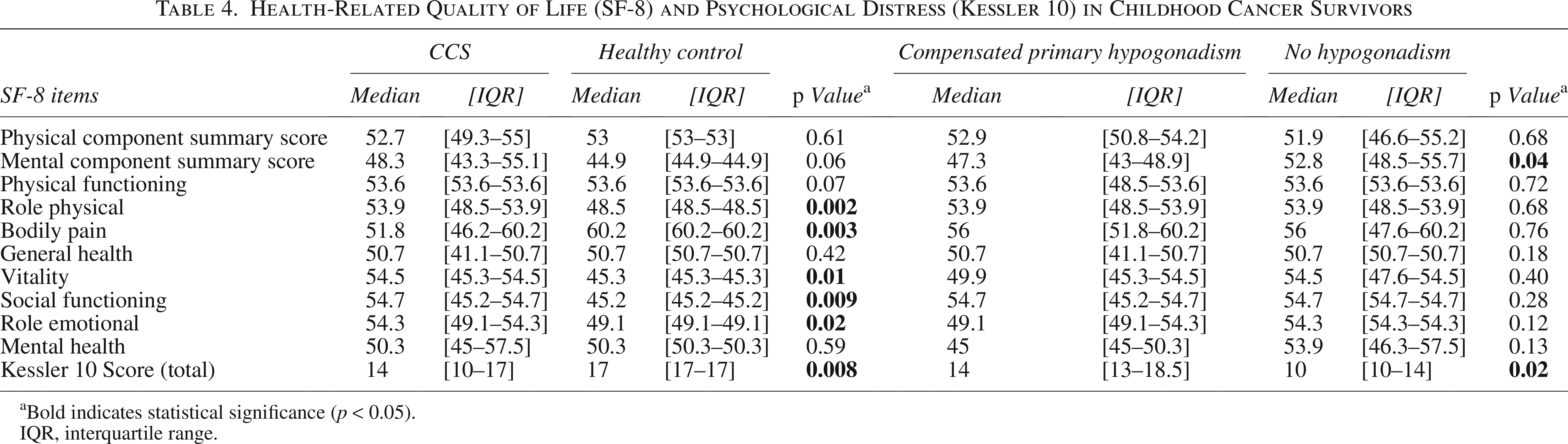
Bold indicates statistical significance (p < 0.05).
IQR, interquartile range.
Discussion
Male CCS face diverse long-term complications from reproductive toxicities, though symptoms are often subtle.4,5 Even CCS with preserved testosterone, such as after unilateral orchiectomy, may experience hormonal aging.16,17
Given these findings, there is a clear need to establish appropriate methods for identifying CCS with hypogonadism. Recommendations for gonadotoxicity surveillance vary considerably among international groups, including differences in diagnostic criteria for PH and CH, screening methods, and management approaches. Some studies define PH in male CCS as testosterone <10 nmol/L (approximately 2.88 ng/mL) and/or LH > 10 IU/L, and compensated hypogonadism as testosterone ≥ 10 nmol/L and LH > 10 IU/L.1,3 Therefore, the Late Effects of Childhood Cancer Guideline Harmonization Group has developed recommendations for gonadotoxicity surveillance in male CCS to standardize these differences. 18 The guideline supports using testicular volume, FSH, and LH to identify hypogonadism when semen analysis is not feasible. Furthermore, recent European Society of Human Reproduction and Embryology guidelines recommend fertility preservation, including testicular tissue cryopreservation, for pediatric males at risk, emphasizing a continuum of reproductive care into survivorship. 19
We followed these recommendations and included testicular volume and FSH in the surveillance method. Our result showed that a testicular volume of 10 mL or lower and/or FSH > 10 IU/L identified CCS with cPH (44% of the cohort). Although the exact definition of cPH differs, this proportion appears higher than previously reported estimates, such as a study in which 20% of male CCSs were found to have Leydig cell dysfunction or failure. 5 Our compensated cases showed higher LH levels, higher fasting blood sugar, lower score in mental component and higher psychological distress. These CCSs are candidates for close observation to monitor whether they may develop hypertension and cardiovascular abnormalities, dyslipidemia, impaired glucose metabolism, low bone mineral density, abdominal obesity, muscle weakness, and low energy expenditure. Additionally, since the age was higher in CCS with cPH, there remains a possibility that CCS who were initially regarded as having no hypogonadism may develop biochemical hypogonadism in the future. This is supported by findings from a previous large cohort study, which showed that 4% of previously unaffected participants, who were followed up later, developed Leydig cell failure and dysfunction. 5
Our findings suggest a possible association between early metabolic changes and cPH in CCS, consistent with prior reports of increased diabetes risk in hypogonadal survivors. 20 Although triglyceride and LDL cholesterol levels did not reach statistical significance, both showed a trend toward higher levels among CCS with cPH, indicating the need for further investigation. CCS with low testosterone are more likely to develop hypertension and dyslipidemia, which may increase the risk of future cardiovascular and cerebrovascular events. 4 Taken together, these findings suggest a possible predisposition to impaired glucose metabolism, dyslipidemia, and elevated blood pressure in CCS with cPH, underscoring the importance of regular monitoring of glucose, lipid profiles, and blood pressure in this population.
The observation that CCS with cPH reported lower Mental Component Summary scores on the SF-8 and higher psychological distress on the K10 suggests reduced energy levels or emotional difficulties related to underlying gonadal dysfunction. Given the possibility for further testosterone decline with aging, longitudinal follow-up focusing on both hormonal and psychosocial health is warranted. In our cohort, CCS with cPH showed a trend toward greater fertility-related anxiety than those without cPH (p = 0.06). As infertility is a primary concern for survivors and their parents, 21 these results underscore the importance of providing targeted counseling for individuals with cPH.
Given its association with hypogonadism, testicular volume remains a valuable indicator, especially in CCS with volume ≤10 mL. We believe that measuring testicular volume is essential for the follow-up of male CCS, and careful observation for low testosterone or hypogonadism symptoms should be continued, especially for CCS with testicular volume of 10 mL or lower in each testis.
We assessed differences in CEDs between CCS with and without cPH. While recent studies have shown that doses ≥4 g/m2 are associated with increased risk of Leydig cell dysfunction, 12 our analysis did not show a significant difference at this threshold (p = 0.67), which should be interpreted cautiously given the limited sample size and exploratory design of the study. In contrast, a cumulative dose ≥7.5 g/m2 was significantly more common in the cPH group (p = 0.002), consistent with earlier studies that identified this threshold as a risk factor for infertility and long-term gonadal damage.13,14 These findings suggest that a dose of ≥7.5 g/m2 clearly reflects clinically relevant gonadotoxicity, whereas doses of ≥4 g/m2 may also have an impact that may not have been detected due to limited sample sizes and therefore require further validation in larger cohorts.
While this single-institution study limits generalizability, it provides valuable preliminary data on Japanese male CCS in the absence of a nationwide follow-up system. These findings highlight the urgent need for a comprehensive national surveillance program.
Our analysis has several limitations. First and foremost, our medical checkup system lacks the ability to gather information on “true” impaired spermatogenesis through semen analysis and physical sexual dysfunction by taking relevant sexual history. However, we did find that CCS are more concerned about the possibility of being unable to have children in the future. While discussing infertility and sexual history is sensitive, we propose focusing fertility counseling on CCS with cPH rather than all CCS; however, this approach requires validation in larger and more diverse populations. Second, the number of male CCS who participated in the study is small compared to previous reports. Therefore, this study should be considered preliminary. The small sample size, particularly in the subgroup with low testosterone levels, limits the statistical power and precludes definitive conclusions regarding these associations. We expect to recruit more CCS and report updated surveillance results in the future. Third, our cohort included a larger number of participants with ALL and fewer with brain tumors. This may affect the results, leading to fewer CH CCS in our cohort. Lastly, CCS who participated in the current medical checkup system may have had physical concerns, which could have motivated them to participate and introduced a bias into the analysis results.
In conclusion, this preliminary prospective surveillance study suggests that testicular volume and FSH levels may help identify male CCS with cPH who warrant careful long-term follow-up for gonadal function and complications associated with hypogonadism, such as cardiovascular disorders and psychosocial problems. To our knowledge, this is the first prospective CCS surveillance study in Japan, and future analyses are planned to include more CCSs who may have been overlooked due to the vague symptoms of male hypogonadism.
Authors’ Contributions
H.Y.: Conceptualization, data curation, formal analysis, investigation, resources, visualization, writing—original draft, and writing—review & editing. S.A.: Conceptualization and writing—review and editing. M.H.: Supervision and writing—review and editing. K.N.: Project administration and writing—review and editing. M.G.: Project administration and writing—review and editing. Y.Y.S.: Methodology, project administration, resources, and writing—review and editing. Y.H.: Methodology, project administration, resources, and writing—review and editing. Y.I.: Supervision and writing—review and editing. K.K.: Funding acquisition, methodology, project administration, resources, and writing—review and editing. A.M.: Resources, supervision and writing—review and editing. D.H.: Methodology, project administration, resources, supervision, and writing—review and editing. M.O.: Funding acquisition, methodology, project administration, resources, supervision, and writing—review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by St. Luke’s Health Science Research Fund (2022–2024), Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan (2014–2019: 26463429 and 2018–2021: 18H03098), Grant-in-Aid for Scientific Research from the Ministry of Health, Labor and Welfare of Japan (2020–2022: 20EA1022 and 2023–2024: 23EA1601), a research grant from Children’s Cancer Association of Japan (2020–2024), a research grant from the Gold Ribbon Network (2017 and 2020), Relay For Life Japan: “Project Future” Research Grant (2016–2017), and Heart Link Working Project: Childhood Cancer Follow-up Research Grant (2014–2015).