
Abstract
Purpose:
Adolescents and young adults (AYAs) with cancer experience unique physical, psychosocial, and developmental challenges that differ from those of children and older patients. While palliative care can address these challenges, the care needs of AYAs with cancer and their families are underrecognized and inadequately supported globally and in South Korea. This study aimed to assess the unmet palliative care needs of AYAs with cancer and their caregivers in South Korea.
Methods:
A cross-sectional survey design was conducted using two validated instruments developed for AYA patients (15–39 years) and their caregivers. Between August 2023 and November 2024, participants were recruited from three major hospitals in South Korea. Descriptive and inferential statistics were used to determine domain-specific needs and group-level differences.
Results:
Communication and information needs were most frequently unmet across all groups, whereas physical needs were often rated as “already provided.” Caregivers—especially of adolescent patients—reported greater unmet needs than patients. Conversely, young adult patients reported the lowest need across all domains. In the caregiver-centered survey, financial and bereavement support were top priorities.
Conclusion:
This study identified unmet palliative care needs, especially nonphysical ones, among AYA patients and their caregivers. The findings underscore the need for age-appropriate, culturally sensitive services, with a greater focus on communication/information and psychosocial care, and the importance of including caregivers’ perspectives in building comprehensive palliative care models. Future studies should explore contextual factors that shape care perceptions and develop standardized screening tools to identify AYAs’ specific needs.
Introduction
Adolescence and young adulthood are distinctive developmental periods marked by unique physical, psychological, and social changes during the transition from childhood to emerging adulthood. 1 The age range of adolescents and young adults (AYAs) varies by country, but is commonly defined as 15–39 years in oncology studies.2,3 In this group, cancer is among the leading causes of death in many countries, with incidence rates rising globally.4,5 Analysis of AYA cancer data from 41 countries between 1988 and 2012 revealed increased AYA cancer rates in over half the countries. 4 Nevertheless, Global Burden of Disease 2021 and Global Cancer Observatory 2022 data highlight improved survival outcomes, reflected in declining mortality rates.6–8 This implies that despite more AYAs being diagnosed with cancer, they are likely to survive; thus, supporting them as they navigate their cancer trajectory is crucial.
Apart from treatment difficulties, AYA patients experience different physical and psychosocial issues compared to children and older adults.5,9,10 AYAs’ epidemiological and biological features result in a unique spectrum of cancer types and tumor genomics, 9 and hormonal changes cause them to respond differently to drugs and experience different side-effects. 11 Furthermore, AYAs undergo critical developmental changes, which can be intensified by a cancer diagnosis.12,13 Disruptions in education and career increase future uncertainty, 14 and AYAs reliance on their caregivers for treatment decisions and emotional support results in a loss of independence. 15 Changes in appearance and lower body confidence further impact AYAs’ self-perception and ability to establish romantic relationships.14,15
In response to these challenges, palliative care can offer crucial support for AYA patients. Palliative care is defined as supportive care provided from diagnosis to end-of-life for patients with life-limiting conditions and their families, aimed at increasing the quality of life (QoL) through physical, psychological, social, and spiritual help. 16 Its positive influence has been well-demonstrated in research; however, providing tailored palliative care services to AYA patients remains a global challenge.17,18 First, low awareness of palliative care contributes to misconceptions that create barriers to accept and engage with palliative care services.19,20 Second, the limited body of research in this area restricts the development of effective, evidence-based palliative care interventions, when numerous interventions already exist for children and adults.18–21 Furthermore, families receive insufficient support despite their key roles emphasized in treatment care and palliative care guidelines.22,23
Providing palliative care services for AYA patients is particularly challenging in South Korea, which has the highest AYA cancer incidence rate globally.5,10 Despite the high rate, AYA patients and their families in South Korea have received insufficient attention and palliative care.24,25 In Korea, palliative care is offered in two forms: adult hospice-palliative care and pediatric palliative care. However, there is no palliative care system dedicated specifically for AYA patients whose ages span both pediatric and adult care boundaries. As a result, AYA patients with pediatric-type cancers typically receive palliative care within pediatric services, leading to increased unmet needs different from younger children. 26 These unmet needs are further compounded by unique challenges of adolescence and young adulthood, as cancer and end-of-life experiences during this period generate more complex needs that reflect developmental disruptions and cultural values.22,27 Moreover, although caregivers are deeply involved in treatment decisions, their needs remain overlooked within palliative care services. 28 This study assesses unmet palliative care needs among AYA patients and their caregivers, to inform the development of more inclusive and tailored palliative care services.
Materials and Methods
This study consisted of two phases: (1) survey development and (2) survey administration.
Phase 1: Survey development
Development of preliminary survey items
Before developing the survey, palliative care reports and guidelines were reviewed to identify key domains: physical, communication/information, psychosocial, and spiritual.29–32 Five major surveys were selected based on the literature; permission to revise and adapt the instruments was granted by the original authors.25,33–36
Two separate surveys were developed to assess AYA patients’ and their caregivers’ palliative care needs. 37 Items were selected during pediatric palliative care team meetings at the primary research institution, based on their relevance to the study through a literature review and/or their recurrence in multiple-referenced surveys. For the AYA patient survey, the selected items were organized into key domains. Consequently, preliminary surveys included 67 items for AYA patients’ and 21 items for caregivers’ care needs. Questionnaire wording for both surveys was revised for clarity where required.
Validity and reliability testing
Preliminary surveys were scrutinized by six experts (three medical oncologists, one professor of nursing, one professor of social welfare, and one child-development senior researcher) to assess clarity, representativeness, and cultural appropriateness. For validity testing, Item-level and Scale-level Validity Index were used. Experts rated each item’s relevance on a 4-point scale (1 = not relevant to 4 = highly relevant). Items with an Item-level Content Validity Index (I-CVI) of 0.78 or higher were retained; lower scores were removed or revised based on experts’ recommendations. 38 Consequently, 10 items were removed from the patient survey. The final versions only included items with acceptable I-CVI and a minimum Scale-level Content Validity Index threshold of 0.80. Internal consistency reliability was also assessed using responses from five patients and five caregivers. For all domains, Cronbach’s alpha was calculated and only accepted when it was in the recommended range of 0.70–0.95. 39
Two final versions of the survey assessing palliative care needs were developed: a patient-centered survey with 57 items and a caregiver-centered survey with 21 items.
Phase 2: Survey administration
Design and methods
A quantitative cross-sectional survey design was conducted. All participants completed a one-time, in-person questionnaire survey in hard-copy form that assessed AYA patients’ palliative care needs. Additionally, caregiver participants were required to complete a separate survey focused on their needs. There were no reminders required because all participants completed the survey at the time of contact. Completed surveys were compiled and analyzed for statistically significant results.
Participants
AYAs with cancer and their caregivers were recruited from three of the largest cancer centers in South Korea. Inclusion criteria for AYA patients were: (1) diagnosed with cancer; (2) aged 15–39 years; (3) actively receiving treatment care; (4) able to understand survey questions; and (5) voluntary consent. Participants aged 15–18 years were classified as adolescents, and those aged 19–39 years were classified as young adults. Individuals providing primary care for AYA patients were identified as caregivers.
Measures
Those who completed less than 90% of the survey were excluded. The survey collected demographics, including sex, birth date, educational background, and religious affiliation. AYA patients self-reported their health status, while caregivers reported those of their patients. Health-status information included diagnosis, time of diagnosis, and types of treatment received (i.e., surgery, chemotherapy, radiation therapy, hematopoietic stem-cell transplantation, or other treatments). Palliative care needs were rated on a 5-point Likert scale (0 = Not applicable, already satisfied; 1 = no need; 2 = low need; 3 = high need; 4 = very high need). Total scores were calculated by summing the responses; higher total scores reflected higher levels of palliative care need.
Data collection
Between August 2023 and November 2024, 193 participants were enrolled, including 95 AYA patients and 98 caregivers. The pediatric team screened eligible participants who visited the inpatient or outpatient pediatric clinic, and explained to them the study purpose and method. All screened participants agreed to participate, provided informed consent, and independently completed the survey; the first author answered questions and provided clarification during the survey administration.
Ethical considerations
This study was approved by the institutional review boards (IRBs) of the
Data analyses
Statistical analyses were conducted using R program. Participants’ demographic characteristics and care needs were analyzed using descriptive statistics. Additionally, the t-test, analysis of variance (ANOVA), and multivariate ANOVA were used to determine differences between groups and between domains.
Results
Characteristics of the participants
A total of 193 participants enrolled: adolescent patients (n = 48; age 15–18), young adult patients (n = 47; age 19–39), caregivers of adolescent patients (n = 55), and caregivers of young adult patients (n = 43). Basic demographics of both groups are presented in Tables 1 and 2. Patients were primarily diagnosed with either bone and soft-tissue tumor (40.4%) or leukemia and lymphoma (34.2%). The average time since diagnosis was approximately 3 years, and most patients had received chemotherapy (97.4%) (Table 3).
Demographics of Patients (N = 95)
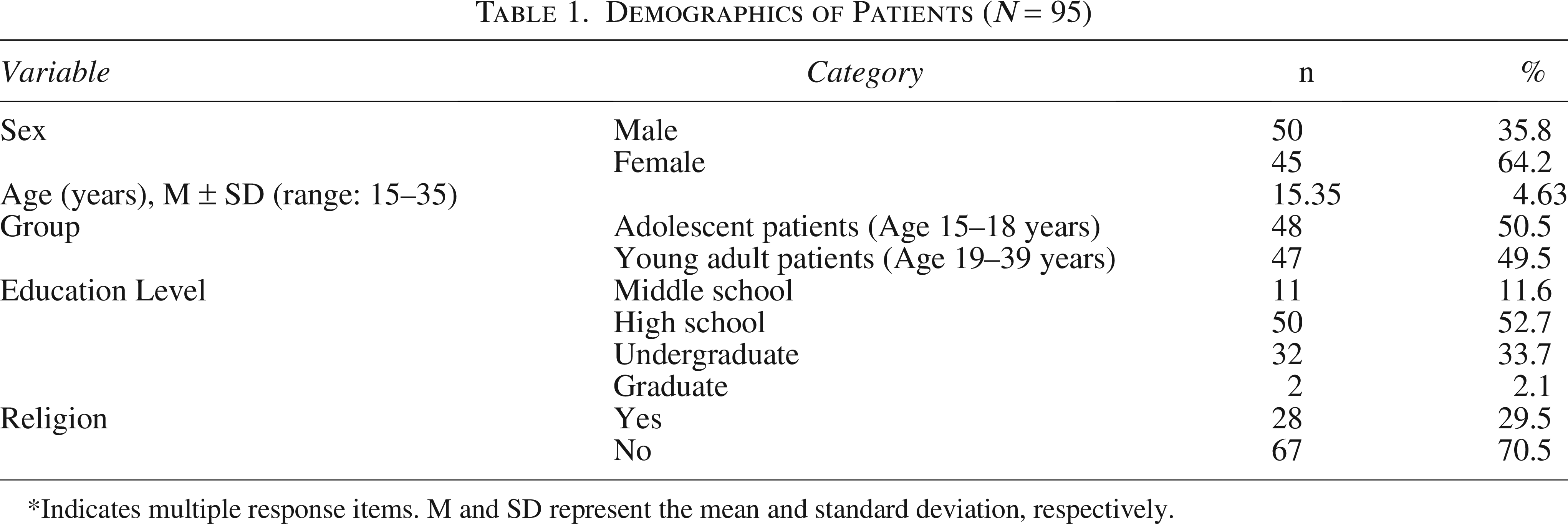
*Indicates multiple response items. M and SD represent the mean and standard deviation, respectively.
Demographics of Caregivers (N = 98)
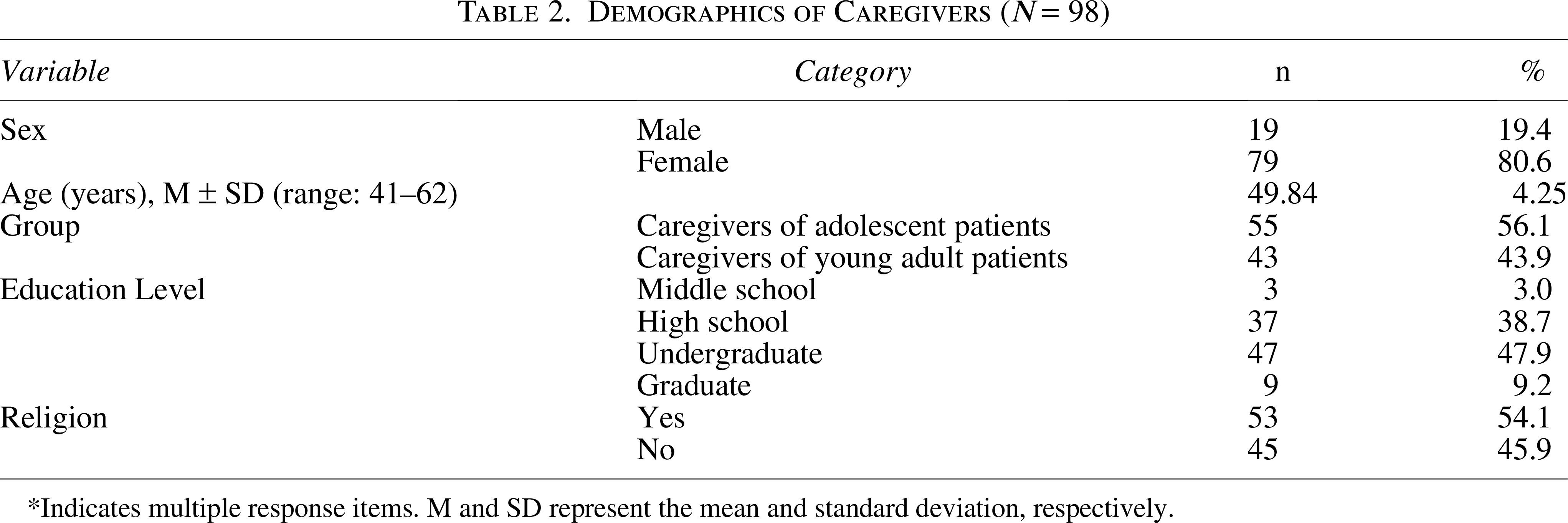
*Indicates multiple response items. M and SD represent the mean and standard deviation, respectively.
Reported Clinical Characteristics of Patients

*Indicates multiple response items. M and SD represent the mean and standard deviation, respectively.
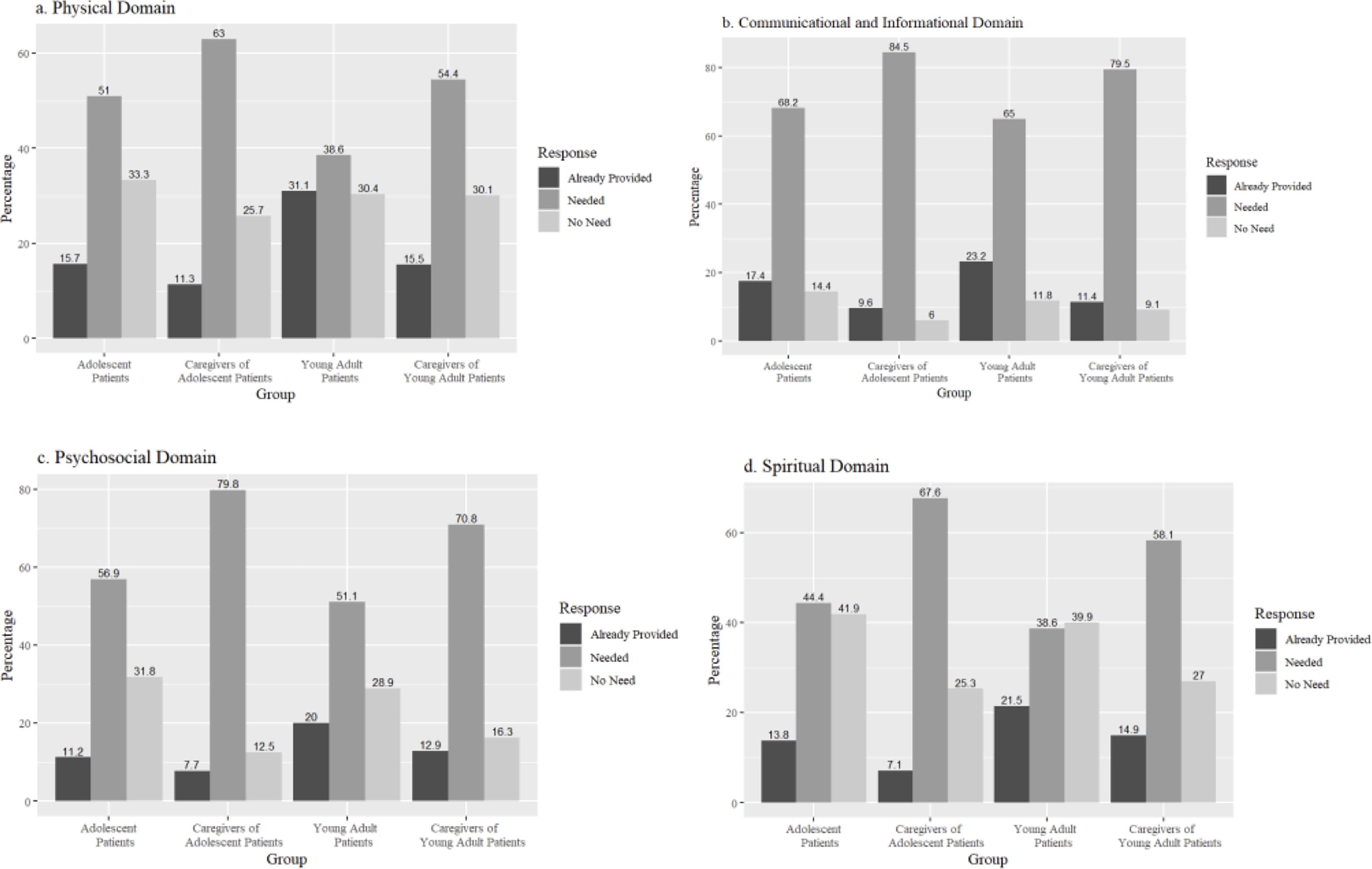
Responses in four domains of the patient-centered palliative care survey
Figure 1 shows the distribution of responses in each care domain in the patient-centered palliative care survey. Response scores were categorized as follows: 0 = service already provided; 1 = service not needed; and 2–4 = service needed. Significant differences in the distribution of responses for groups were confirmed by a chi-square goodness-of-fit test. In most cases, “Needed” was the most frequently chosen response. For example, the responses of adolescent patients’ caregivers differed significantly from all other groups in the physical domain, χ2(2, N = 824) = 358.58, p < 0.001. Standardized residuals indicated that caregivers of adolescent patients were significantly more likely to report “Needed” (z = 14.92) than “No Need” (z = −3.96) and “Already Provided” (z = −10.96). However, young adult patients showed a different pattern in the spiritual domain. Their responses differed significantly, χ2(2, N = 466) = 29.68, p < 0.001; however, the “No Need” (z = 2.46) response was reported similarly, while the “Needed” (z = 1.98) response was more frequent and the “Already Provided” response significantly less frequent (z = −4.44) than expected.
Group differences in the patient-centered palliative care survey
To compare differences in the total scores of the patient-centered palliative care needs survey among groups (Fig. 2), a one-way between-groups ANOVA was used. The results confirmed a significant difference in palliative care score based on group condition, F(3, 189) = 9.85, p = 0.001, n2 = 0.14. Post-hoc testing using Tukey’s procedure revealed significantly higher levels of palliative care need among adolescent caregivers (Mean = 128.24) than among adolescent patients (Mean = 98.13), t(189) = 3.65, p = 0.002, d = 0.72 and young adult patients (Mean = 86.17), t(189) = 5.07, p = 0.001, d = 1.01. Moreover, young adult caregivers (Mean = 114.91) reported significantly higher levels of palliative care need than young adult patients, t(189) = 3.26, p = 0.01, d = 0.69.
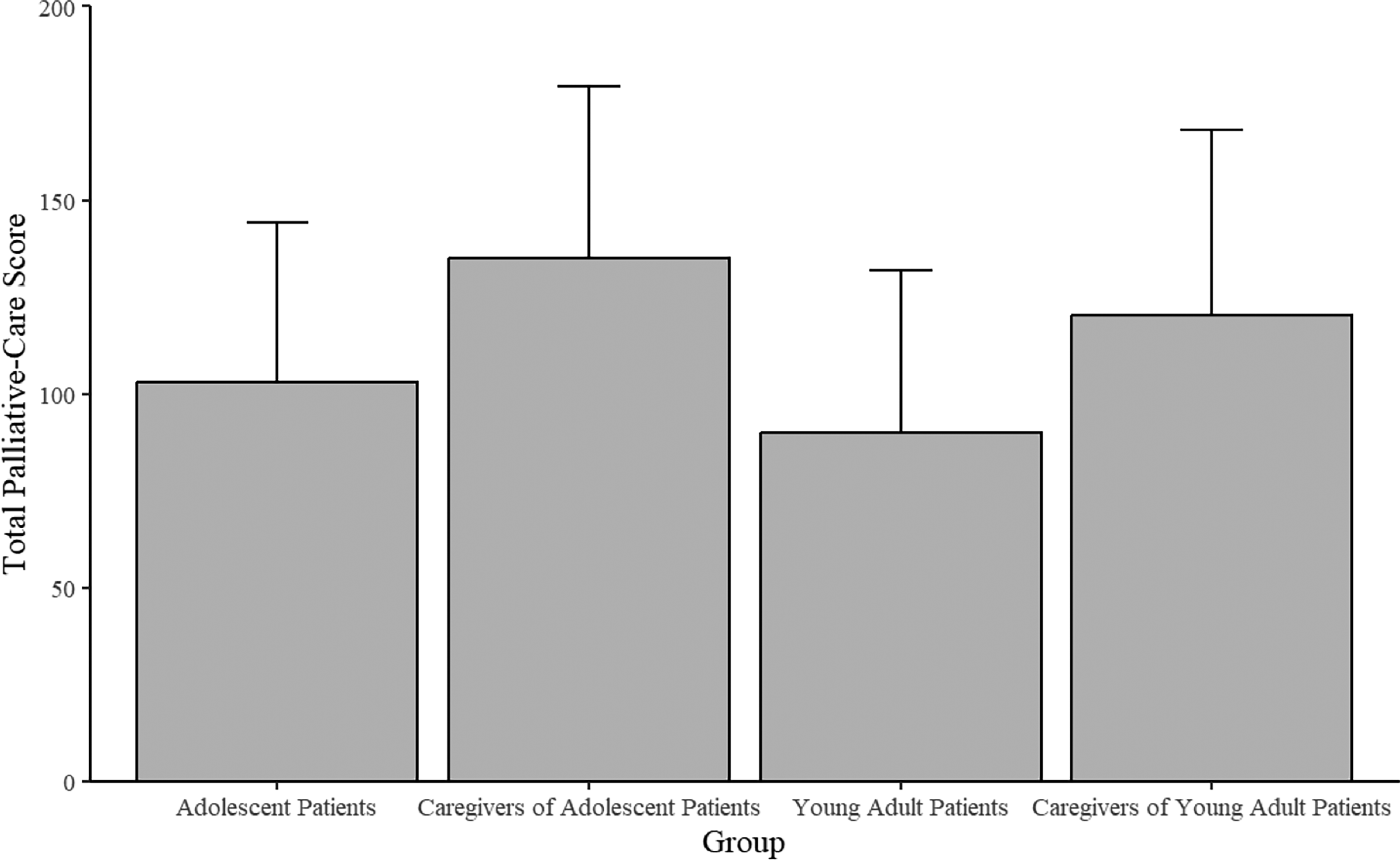
Differences in total patient-centered palliative care scores between groups.
Domain-level differences in the patient-centered care survey
Table 4 presents differences between patient-centered palliative care domains and three top-rated items within each domain. A one-way between-groups ANOVA confirmed a significant difference in mean scores among four palliative care domains, F(3,768) = 14.32, p = 0.001, n2 = 0.06. Post-hoc testing using Tukey’s procedure indicated significantly higher scores for the communication/information domain (Mean = 2.34) than the physical (Mean = 1.71), t(768) = 6.50, p = 0.001, d = 0.66, psychosocial (Mean = 2.05), t(768) = 3.01, p = 0.01, d = 0.31, and spiritual (Mean = 1.84), t(768) = 5.10, p = 0.001, d = 0.52 domains. Furthermore, psychosocial-care needs were rated significantly higher than physical-care needs, t(768) = 3.49, p = 0.003, d = 0.36. Across most of the top-rated items for each domain, adolescent patients’ caregivers perceived a higher need for palliative care services than other groups. By contrast, exceptions were observed for items 2 and 21: For item 2 (physical need), no significant group differences were found, F(3,189) = 1.63, p = 0.18. For item 21 (communication/information need), young adult patients’ caregivers reported significantly higher scores than other groups, F(3,189) = 6.80, p < 0.001.
Group Differences in Patient-Centered Palliative Care Domains and Their Highest-Rated Perceived Care Needs

M and SD represent the mean and standard deviation, respectively.
Differences in the caregiver-centered palliative care survey
Figure 3 shows the differences in total score in the caregiver-centered palliative care survey. Welch’s two-sample t-test was used to compare palliative care scores (score range 0–84) of caregivers of adolescent patients (M = 50.92) and those of young adult patients (M = 43.93). Although the plot suggests a higher perceived need by caregivers of adolescent patients, no statistically significant difference between the groups was found, t(80.04) = 1.71, p = 0.09, Hedge’s g = 0.36. Among the survey items, questions 10 (financial support), 14 (bereavement support), and 11 (support for loss of income source) received the highest average scores.
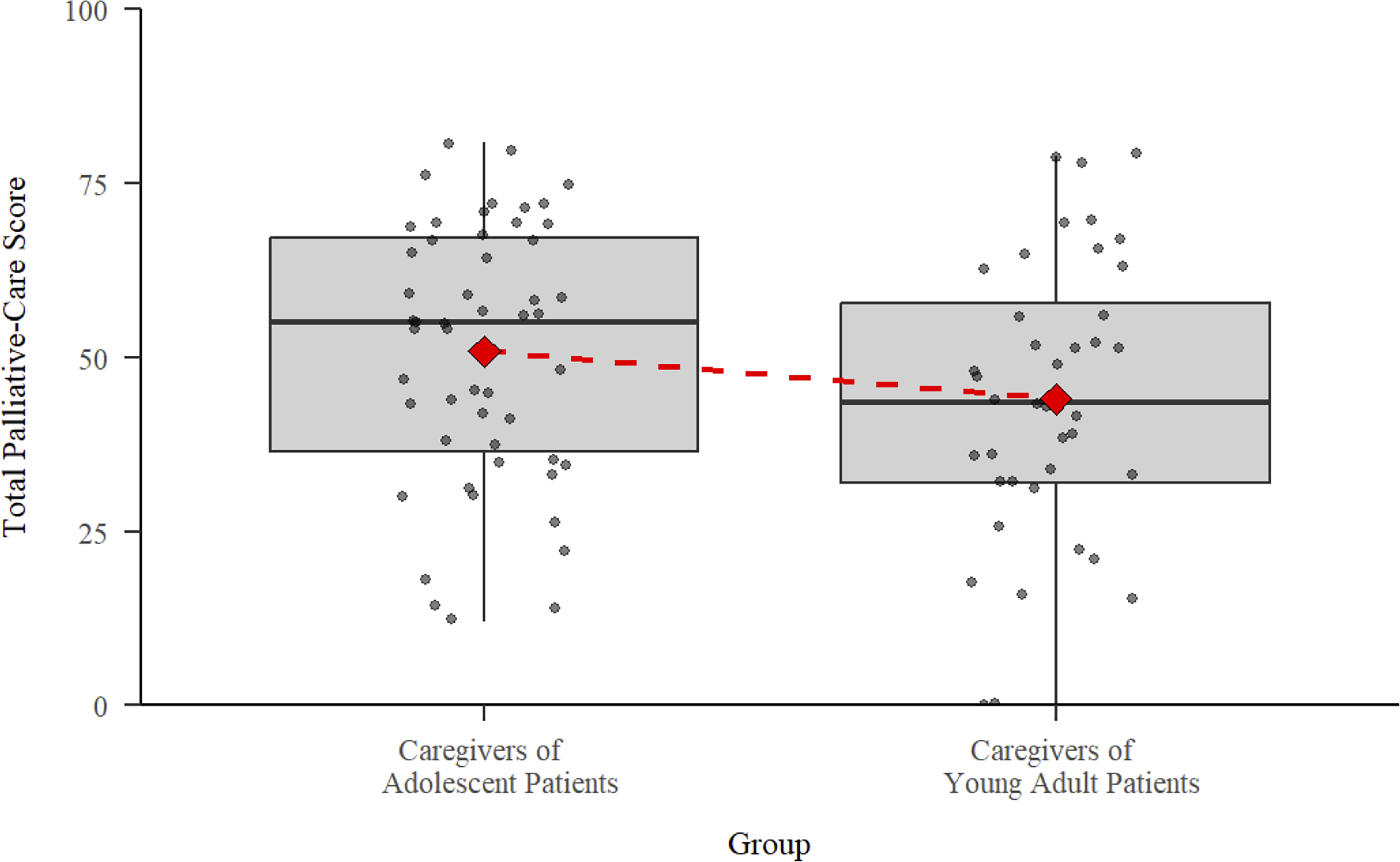
Differences in caregiver-centered palliative care scores.
Discussion
This study employed a cross-sectional survey to assess unmet palliative care needs among AYA patients with cancer and their caregivers in South Korea. The patient-centered survey revealed that both patients and caregivers consistently identified all domains of patient care as “needed,” suggesting an under-provision of essential services within the current palliative care model. Communication/information needs emerged as the most frequently unmet needs across all groups. This can be partially explained by the unique dynamics of South Korean AYAs, who, despite their dependence on caregivers during cancer care, may express independence and autonomy when responding to surveys. Moreover, there is an association between high levels of unmet cancer-related information needs and low perceived control over life, 40 suggesting that elevated communication/information needs may stem from a desire to regain a sense of stability and control. Although prior research has reported mixed findings regarding whether communication/information or psychosocial needs are the most unmet, this study emphasized a particular demand for enhanced communication/information support for AYA patients and their caregivers.41,42
Conversely, physical needs were frequently marked as “already provided” and had the lowest domain-specific score among all four domains, suggesting effective symptom and pain management within the current health care system. Early integration of physical care on referral is recommended by many palliative care guidelines and appears to be successfully implemented.43,44 As the present study suggests, successful integration of physical care offers a positive outlook for improvements in other care domains when palliative services are adapted to address diverse unmet needs.
Spiritual needs had the highest proportion of “no need” responses, which is unexpected given the existential challenges AYA patients face from illness and developmental tasks.45,46 Moreover, a previous study reported high levels of distress, including spiritual concerns, among AYA patients’ caregivers. 46 Although the majority of participants in the current study identified as having no religion, there were no significant differences in the level of spiritual care needs based on religious affiliation. Spirituality is recognized as a critical coping mechanism during serious illness. 46 However, its unclear definition among AYA patients hinders effective integration into AYA cancer care. Additionally, declining religiosity among younger South Koreans may contribute to a misunderstanding of spirituality.47,48 Consequently, the AYA patients and their caregivers may have prioritized immediate concerns over spiritual support. Given its importance, spiritual care should be delivered in a developmentally appropriate and context-specific manner for AYA populations. 49
Caregivers across all groups—especially of adolescent patients—reported higher palliative care needs than patients, consistent with prior research suggesting that caregivers perceive younger patients’ illnesses as more severe, which increases the demand for support. 50 Possible explanations for low need among patients include limited self-awareness and high levels of avoidance behavior.51,52 Furthermore, young adult patients reported the lowest palliative care need in all care domains, contrasting with previous studies conducted in the United States and Japan, wherein young adult patients expressed high levels of unmet care needs.53,54 These discrepancies suggest cultural or contextual factors may influence Korean young adult patients’ perceptions of need and engagement with palliative care services.
Although no statistical difference was found in caregiver-centered unmet care needs, visual trends revealed a higher perceived need among adolescent patients’ caregivers. In many Asian cultures where family harmony is prioritized, younger patients become increasingly dependent on their caregivers for decision-making, which in turn contributes to greater caregiver burden.20,55 Furthermore, AYA caregivers experience a greater burden than those caring for other age groups due to developmental complexities alongside severe illness.20,27 These compounded burdens may prevent caregivers from providing full support, thereby adversely impacting patients’ treatment course and outcomes. In this study, caregivers consistently prioritized financial support and bereavement services, which highlights the need to address their practical and emotional burdens and to improve their QoL and care experiences.
Although the study provides important insights into the unmet palliative care needs of AYA patients and their caregivers, it has several limitations. First, the survey research method may have constrained the interpretation of the findings; a mixed-methods approach with qualitative interviews could better capture complex unmet needs. Second, the small sample size of caregivers may have limited the statistical power to detect significant differences between caregiver groups, limiting confidence in interpreting group-level results. Finally, excluding health care providers restricts the ability to assess discrepancies between perceived needs and actual service provision. Future studies should include health care providers to achieve a more comprehensive understanding of unmet needs in palliative care services.
To build on these findings, future research should focus on developing targeted interventions that address the distinct needs of AYA patients and their caregivers. Parallelly, a standardized screening tool should be designed and validated for early identification of unmet care needs. Finally, further studies should examine how cultural, developmental, and systematic factors shape AYA patients’ and their caregivers’ needs and perceptions—particularly in non-Western contexts where family dynamics, autonomy, and care expectations differ from current models.
Conclusions
The number of AYA cancer patients in South Korea is increasing, along with the demand for palliative care services tailored to their unique needs; yet, efforts to provide a comprehensive understanding of the priorities and unmet palliative care needs of these patients and their caregivers have been limited. Accordingly, the present study offers a nuanced understanding of these needs across key palliative care domains as reported by both patients and caregivers. These insights can inform the development of tailored palliative care models that address previously unmet needs as well as lay the groundwork for diverse strategies—whether through research, practice, or policy—to enhance the QoL of AYA patients and caregivers. Furthermore, this study emphasizes the importance of inclusive approaches that recognize the interdependent nature of patient and caregiver well-being. Sustained efforts in research, practice, and policy are essential to ensure that palliative care systems evolve to equitably support the diverse needs of AYA populations.
Authors’ Contributions
Conceptualization: J.A.L. Investigation: S.O., M.P., H.J.C., H.J.K., H.J.H., and S.K. Data curation: S.O., H.J.H., and S.K. Methodology: J.A.L., S.O., M.K.P., and H.J.K. Writing—original draft: S.O. Writing—review and editing: J.A.L., S.O., S.Y.K., and H.J.B. Supervision: H.J.P. and M.R.P. Project administration: J.A.L. and S.O. Analysis: S.O. Validation: J.A.L., S.Y.K., and H.J.B. Funding acquisition: J.A.L.
Footnotes
Acknowledgment
The authors thank the participating hospitals and all participants who generously participated in this study.
Availability of Data and Materials
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This study was supported by the National Cancer Center (NCC2023-0215).