
Abstract
A secondary analysis of a population-based study of cancer patients’ use of specialty palliative care (SPC), 2012–2015, was conducted, comparing a young adult (YA) cohort of those who died at age 21–39 years (n = 112); a cohort of those who died at 40–64 years old (n = 2957); and an older cohort that died at age 65 or older (n = 8949). The YA cohort had a higher rate of SPC use (44.6%) compared to the middle (34.3%, p = 0.0244) and older cohorts (21.1%, p < 0.0001). The cohorts did not differ significantly in the timing of SPC, which often occurred in the final days or weeks prior to death.
Introduction
About 80,000 young adults (YAs) aged 20–39 are diagnosed with cancer each year in the United States, representing approximately 4% of all newly diagnosed cancers. 1 Cancer in YAs differs in biology and treatment, and diagnosis occurs during significant life transitions, resulting in distinct supportive care needs compared to children and older adults.1,2
YAs with cancer often encounter access to care issues and health care challenges, including health insurance coverage gaps, high financial toxicity, lack of age-appropriate resources and programs, lack of access to cancer clinical trials, care coordination issues, and often fall between pediatric and adult care.3–6 They also experience significant physical, emotional, social, and spiritual distress that impacts their quality of life, making specialty palliative care (SPC) an important component of their care.1,2 In studies of YAs with cancer, SPC has been found to decrease pain, symptom scores, and the likelihood of high-intensity care at the end of life.7–10
Despite these benefits, studies have found that YAs with cancer are referred to palliative care at rates ranging from 9% to 85%, and additional studies have identified challenges related to delivering SPC to this population.3,4,7,11–14
Understanding how YAs compare to other age groups in their use of SPC is essential, yet the literature examining age and receipt of SPC remains limited. In our prior population-based study of SPC use in a mid-sized metropolitan area in the southeastern U.S., 15 we found younger age was associated with greater SPC use (adjusted odds ratio 0.78 [95% confidence interval: 0.75, 0.80], 10-year increments), but as with other studies, most of the patients were older than 65. This is a similar method to other studies in the United States and abroad that have found age-related differences in SPC use but do not specifically address YAs as a distinct group, often analyzing age as a continuous variable or using broad categories such as under 60 or over 80. This lack of focus on YAs, coupled with their underrepresentation in, and sometimes exclusion from, palliative care research, highlights a critical gap in understanding their access to and receipt of SPC. 16
The goal of the current study was to determine the use of SPC in YAs with cancer in a secondary analysis of the population-based data referenced above. The focus on YAs (diagnosed at age 21+ and died before 40) is due to constraints in the original study and does not include younger cancer patients.
Methods
The full methods of the original study are described in the prior article. 15 Briefly, this was a population-based decedent cohort study using secondary data from multiple sources. Data sources were the statewide cancer registry; statewide hospital discharge data; and medical groups’ SPC encounters.
The Virginia Cancer Registry (VCR) provided statewide data on adults who were diagnosed at ages ≥21 and whose deaths occurred 2012–2015. Virginia Health Information (VHI) provided statewide data on all hospitalizations from 2010 to 2015 for those cancer decedents. VCR data were linked to hospitalization data by VHI using hashed (encrypted) social security numbers. The three palliative care programs in the Richmond metropolitan statistical area (MSA) provided patient-level data on SPC services from 2010 to 2015. SPC services were inclusive of inpatient and community-based services, concurrent with cancer-directed therapies, not limited to end-of-life care. VCR data were linked by the researchers to SPC data using patient name and date of birth. The resulting VCR-VHI-SPC dataset was then linked to U.S. census data based on census tract identifiers at the time of diagnosis.
We included people that were living within the Richmond MSA at the time of cancer diagnosis and excluded cases that had additional cancers diagnosed when patients’ residence was outside the MSA. We excluded cases that had hospitalizations outside of the Richmond MSA (beyond the several small, rural hospitals just outside the MSA, none of which had SPC services) because we had palliative care data only from providers within the MSA.
For this secondary study, we created three cohorts of cancer decedents: those who died at age less than 40 (cohort 1; n = 112); those who died at ages 40–64 (cohort 2; n = 2,957), and those who died at ages 65 and above (cohort 3; n = 8,949).
Analyses were conducted to determine the use and timing of SPC in each cohort, with alpha set at 0.05 and no a priori hypotheses. Frequencies and percentages of sample characteristics were provided for categorical variables and means (standard deviations) and/or medians (interquartile range) for continuous variables. Logistic regression was used to simultaneously compare the distribution of sample characteristics for each of the two older cohorts with the youngest, unless expected frequencies were too small, when Fisher’s exact test was used in pairwise analysis. For ordinal sample characteristics, the proportional odds assumption of the logistic regression did not hold so the Wilcoxon rank-sum test was used for pairwise comparisons of each of the two older cohorts with the youngest. Odds ratio and confidence intervals comparing SPC use for each of the older cohorts to the youngest cohort were estimated using logistic regression. Adjusted models included sex, race, any hematological malignancy, multiple cancers, poor prognosis at time of diagnosis, year of death, and cancer site. Because of the possibility of differential misclassification of prognosis for hematological malignancies leading to incomplete adjustment, we also conducted a sensitivity analysis to determine whether hematological malignancy was an effect modifier for the relationship between age cohort and SPC by adding an interaction term to the multivariable logistic model. This was followed by separate analyses for those with and without ever having a hematological malignancy.
Analysis of time from SPC to death only included patients who received SPC. Median days from SPC to death were estimated using Kaplan–Meier survival methods and compared using a log-rank test. The distributions of the ordinal classification of days from first SPC to death were compared as described above for the full sample. Hazard ratios and confidence intervals were estimated using Cox Proportional Hazards regression. Models were similar to that for logistic regression.
Results
Characteristics of the cancer patients in the three cohorts are shown in Table 1. Compared to the other two cohorts, patients in cohort 1 (died age <40) were more likely to receive SPC; be female (vs. cohort 2); Black (vs. cohort 3); have a hematological malignancy; less likely to have a poor prognosis cancer (vs. cohort 2) or certain cancer diagnoses; and were more likely to be hospitalized (and at an SPC hospital) and were hospitalized more frequently.
Cohort Characteristics and Use of Specialty Palliative Care

The measure is a function of cohort definition so no statistical comparisons made.
STD, standard deviation; IQR, inter-quartile range; SES, socioeconomic status, derived from 7 data elements from the American Community Survey census data and converted to quintiles; SPC, specialty palliative care; poor prognosis = distant metastasis at diagnosis or nationally had 40% or fewer surviving for 5 years.
The timing of SPC is shown in Table 2. The timing of SPC was not statistically different among the three cohorts, but a trend toward earlier engagement with the younger cohorts is evident from the medians (50, 35, and 26 days in cohorts 1, 2, and 3). In all three cohorts, some patients first received SPC close to death: 14.0% of cohort 1, 13.5% of cohort 2, and 16.2% of cohort 3 received SPC in the last 3 days of life.
Age, Survival, and Time from Specialty Palliative Care to Death among SPC Recipients
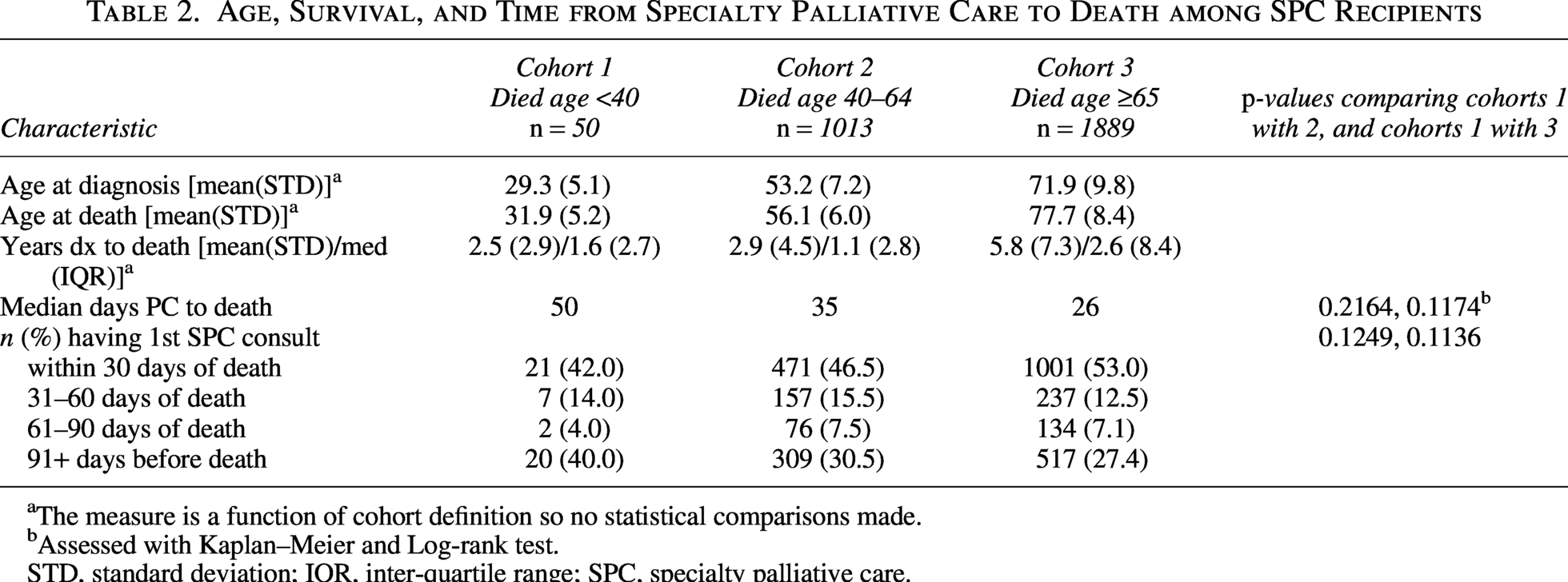
The measure is a function of cohort definition so no statistical comparisons made.
Assessed with Kaplan–Meier and Log-rank test.
STD, standard deviation; IQR, inter-quartile range; SPC, specialty palliative care.
The odds ratios for comparing the receipt of SPC and hazard ratios for timing of SPC are shown in Table 3. Adjusting for demographic and clinical characteristics, the odds of using SPC are 35% lower for cohort 2 and 65% lower for cohort 3 compared to the odds for cohort 1. The hazard ratios for the timing of SPC were not significant.
Odds Ratios and Hazard Ratios
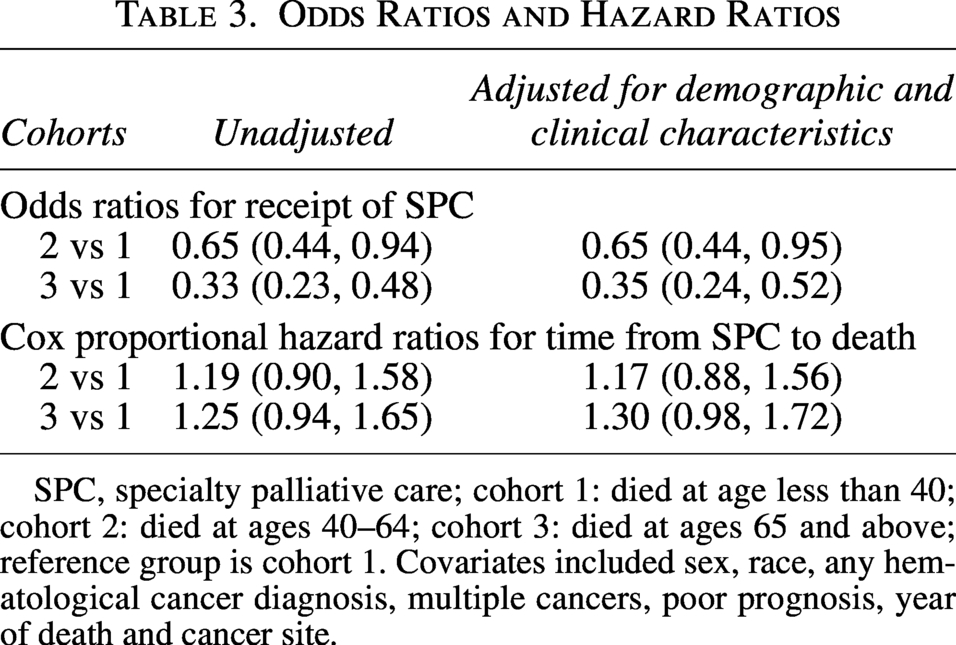
SPC, specialty palliative care; cohort 1: died at age less than 40; cohort 2: died at ages 40–64; cohort 3: died at ages 65 and above; reference group is cohort 1. Covariates included sex, race, any hematological cancer diagnosis, multiple cancers, poor prognosis, year of death and cancer site.
The sensitivity analysis to determine whether hematological malignancy was an effect modifier for the relationship between age cohort and use of SPC showed that the interaction term was not statistically significant (p = 0.74), indicating that hematological malignancy was not an effect modifier. However, the point estimates of the odds ratio for SPC for patients without hematological malignancies were similar to those for the entire cohort (0.70 [95% CI: 0.45, 1.09] for cohorts 2:1 and 0.39 [0.25, 0.60] for cohorts 3:1), while for patients with hematological malignancies, the odds ratios were more extreme (0.47 [0.21, 1.07] for cohorts 2:1; 0.24 [0.11, 0.54] for cohorts 3:1), favoring increased likelihood of SPC for the youngest cohort.
Discussion
This secondary analysis of a population-based dataset is the first to examine SPC use among YA cancer patients diagnosed at age 21 or older and deceased before age 40, compared to older cohorts (died 40–64 and ≥65 years). The findings indicate that YA cancer patients were more likely to receive SPC. It is unclear whether this pattern is due to distinct needs of YAs (e.g., a higher prevalence of symptom burden) or other factors (e.g., more frequent hospitalizations provided recurring opportunities for referrals to SPC).
While there were not statistically significant differences in the cohorts’ timing of SPC, the data indicate that the YA cohort had a slightly higher percentage of patients receiving SPC more than 90 days before death. This could be explored in further research—could younger adults with cancer receive more opportunities for SPC referral due to their more frequent hospitalizations?
It is worth noting that the YA cohort’s greater SPC use occurred despite their higher prevalence of hematological malignancies, which are generally negatively correlated with SPC use.15,17 Similarly, the YA cohort also had a higher prevalence of Black patients (than the oldest cohort), which some reviews have linked to a lower likelihood of SPC use, perhaps due to studies relying on low-validity data regarding SPC. 18
Methodologically robust studies of SPC prevalence in the United States are rare, and those including YA cohorts are rarer still. For example, six multi-site SPC studies from the past two decades reported only mean age, without detailing the number or percent of SPC users by age category, making it difficult to understand the specific needs of YAs.19–24 While over 130 studies of “palliative care” have utilized The Agency for Healthcare Research and Quality (AHRQ's) National Inpatient Sample and similar all-payer, all-age datasets, they rely on the Z51.5 “encounter for palliative care” ICD10 code, which captures a broad range of clinical scenarios not specific to SPC and is not mandatory for SPC encounters. 25 Validation studies have demonstrated poor sensitivity and positive predictive value for this code in adults (49.9%, 54.0%, respectively) 26 and in pediatric ICU patients (11.0%, 66.7%). 27
This study overcomes these limitations by using a population-based dataset with detailed SPC utilization data and offered a novel focus on YAs with cancer as a distinct group.
The SPC utilization among YAs underscores the need for age-appropriate SPC programs tailored to the developmental, emotional, and social challenges of a cancer diagnosis at a younger age. And despite YAs’ higher rate of SPC utilization, it is still only 45%. Furthermore, SPC comes late in the disease trajectory, often occurring close to end-of-life and within days or weeks of death: only 40% of the YA cohort in this study received SPC more than 90 days before death. The American Society of Clinical Oncology recommends early SPC integration for patients with advanced cancer, ideally at diagnosis or with uncontrolled symptoms, to optimize quality of life and symptom management. 28 Much work remains to be done to achieve the aspirational goal for cancer patients of all ages.
A limitation of this study was that it excluded patients diagnosed before the age of 21, whose cancer treatment and palliative care use could have occurred when they were 21+. Another limitation is that this study was of a particular geographic region, and the results are not necessarily generalizable to other areas of the U.S. or beyond. Other limitations related to this study’s reliance on secondary data include the lack of measurement of disease severity, physical function, or symptom burden at various time points.
Future research should explore the drivers of SPC use among YAs, including accessibility of SPC services, acceptability of services, characteristics of providers who do or do not refer YA patients to SPC services, and other factors. Future studies could help to explain the finding here that the YA cohort was more likely to use SPC than the older cohorts, despite relatively high hematological malignancy prevalence; this is in contrast to some prior research that has indicated lower SPC use in hematological malignancy patients. Studies using SPC data, rather than relying on imprecise codes like Z51.5, are needed to accurately capture utilization patterns.
Conclusion
In conclusion, this study contributes new insight into SPC utilization among YAs with cancer, a population often overlooked in SPC research. While findings show that YAs are more likely to receive SPC than older adults, it is still less than 50%. SPC was often initiated close to the end of life, as it was for the older adults as well. These findings underscore the need for earlier and more proactive integration of SPC for YAs, tailored to their distinct clinical and psychosocial needs. Prioritizing YAs as a distinct population in SPC research, policy, and practice is essential to developing care models that reflect their unique needs, values, and life circumstances.
Footnotes
Acknowledgment
The authors acknowledge the co-authors on the original study, which made this secondary analysis possible: David Buxton, Leanne Yanni, Seth Roberts, Nevena Skoro, Peter May, Egidio Del Fabbro, and Danielle Noreika (deceased).
Author Contributions
M.R., D.K.M., and J.B.C.: Designed the secondary analysis study. D.K.M.: Conducted the analyses. M.R., D.K.M., and J.B.C.: Interpreted findings. M.R., D.K.M., and J.B.C.: Drafted and revised manuscript.
Author Disclosure Statement
No competing financial interests exists.
Funding Information
The original study was supported by the American Cancer Society Pilot and Exploratory Projects Grant. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of this article.