
Abstract
Background:
Community-based organizations play an essential yet underrecognized role in addressing health inequities faced by adolescent and young adult (AYA) cancer survivors, particularly those from underrepresented communities. Elephants and Tea, a nonprofit organization, launched One Herd, a digital storytelling and health equity campaign designed to elevate lived experiences of underserved AYA survivors. This article describes the conception and development of that campaign and presents findings from its needs assessment.
Methods:
One Herd followed a five-phase process (1) assembling a multidisciplinary advisory team of underrepresented AYA survivors; (2) identifying campaign priorities and conducting a national needs assessment to inform content development; (3) analyzing survey findings and creating survivorship-centered content; (4) disseminating content through digital, print, webinar, and live storytelling platforms; and (5) evaluating campaign reach and perceived impact. A national needs assessment identified social and structural barriers to equitable survivorship care, guided by social determinants of health and community-engaged frameworks.
Results:
Eighty-one AYA cancer survivors completed the survey; 76 were included in the final analysis. Participants reported multilevel inequities, including limited access to fertility preservation resources, perceived bias and discrimination in health care, and unmet needs for peer connection and identity-affirming support. Findings informed the development of survivor-centered digital storytelling and educational materials for community and provider audiences. Dissemination formats included a print and digital magazine, webinars, and live storytelling events, with workforce education integrated into Elephants and Tea’s AYA Program for Oncology Workforce Education and Resources. Early feedback identified survivor stories as the most impactful campaign component.
Conclusions:
One Herd demonstrates how community-led, research-informed storytelling can operationalize narrative equity and bridge survivor experience with system-level education in AYA cancer care.
Introduction
More than 2.1 million adolescent and young adult (AYA; aged 15–39 at diagnosis) cancer survivors currently live in the United States, 1 and this number continues to grow. 2 AYAs represent an increasingly distinct population, 3 with specific and enduring health and psychosocial needs across the cancer continuum.4,5 Despite advances in survivorship care and overall cancer care delivery, persistent disparities remain both among and within AYA subgroups. These disparities are influenced not only by medical factors but also by the broader social determinants of health (SDOH), including the conditions in which individuals live, work, and access care that shape cancer outcomes and survivorship experiences.6–9
AYA survivors experience multiple inequities, including longer delays in diagnosis compared to other age groups,10,11 heightened psychosocial distress during a sensitive developmental period,12,13 financial hardship,14–16 and challenges related to fertility planning and family building.17,18 These inequities are compounded for AYAs with racial, ethnic, sexual, and gender minority backgrounds and low-income communities,19,20 who experience disparities in diagnosis, treatment access, survivorship, and cancer-specific survival.3,21,22
Because most AYAs receive their oncology care in community oncology settings rather than academic cancer centers, accessible community-based supportive care is critical.3,23 Nonprofit and other community organizations have sought to fill a major gap in addressing unmet needs and challenges, including efforts to mitigate disparities, but their efforts have been largely unstudied.24–26 Nonprofit and community-based organizations have increasingly sought to address these disparities by offering tailored support, peer connection, advocacy, and culturally responsive programming to some of the most marginalized AYA survivors.27,28 They also create opportunities for storytelling, a therapeutic practice shown to foster meaning-making, healing, and identity expression, in the wake of a traumatic experience such as cancer. 29
Through sharing of these meaningful stories, AYAs can communicate messages containing their identity, unique life experiences, and perceived meaning of the events. 30 In response to ongoing calls to advance antiracist and equity-centered approaches in AYA cancer care,31–33 this article describes the development and implementation of the One Herd content campaign, a community-led initiative designed to amplify lived experiences of underserved AYA survivors and translate those narratives into educational tools for health care providers and the broader oncology workforce.
Elephants and Tea
Elephants and Tea is a community-based organization that serves AYAs with cancer, caregivers, and health care professionals globally. 34 Founded in 2018, as the nonprofit media brand of the Steven G. Cancer Foundation, the organization’s mission is to ensure that AYAs facing cancer know they are not alone in their experience. They accomplish this mission through multiple initiatives including: (1) a free quarterly print and digital magazine featuring stories written by AYA cancer patients and survivors, (2) digital and in-person programs designed to connect AYAs and foster community, and (3) partnerships with health care institutions, researchers, and nonprofit organizations supporting AYA cancer care.
One Herd Content Campaign
In early 2021, leadership at Elephants and Tea identified an opportunity to leverage the organization’s storytelling platform and AYA cancer community trust to address persistent inequities in AYA survivorship. In partnership with This Exceptional Journey (TEJ) Media (https://thisexceptionaljourney.com/), the Elephants and Tea launched “The One Herd Content Campaign: The State of Underserved Communities Facing AYA Cancer” (hereafter, “One Herd”). 35 One Herd is a multiyear initiative designed to elevate the experiences of medically underserved and underrepresented AYAs while translating those narratives into educational content for health care professionals and community audiences. Launched in September 2022, One Herd employs an integrative model that combines qualitative storytelling with community-engaged data collection to identify structural gaps in care and disseminate findings across both survivor-facing and provider-facing platforms. The campaign is organized into five phases: (I) team construction; (II) research initiatives and goal setting; (III) data analysis and content creation; (IV) marketing and dissemination; and (V) evaluation (Table 1). Table 1 details each phase with a brief description of activities and the corresponding time of implementation.
One Herd Campaign
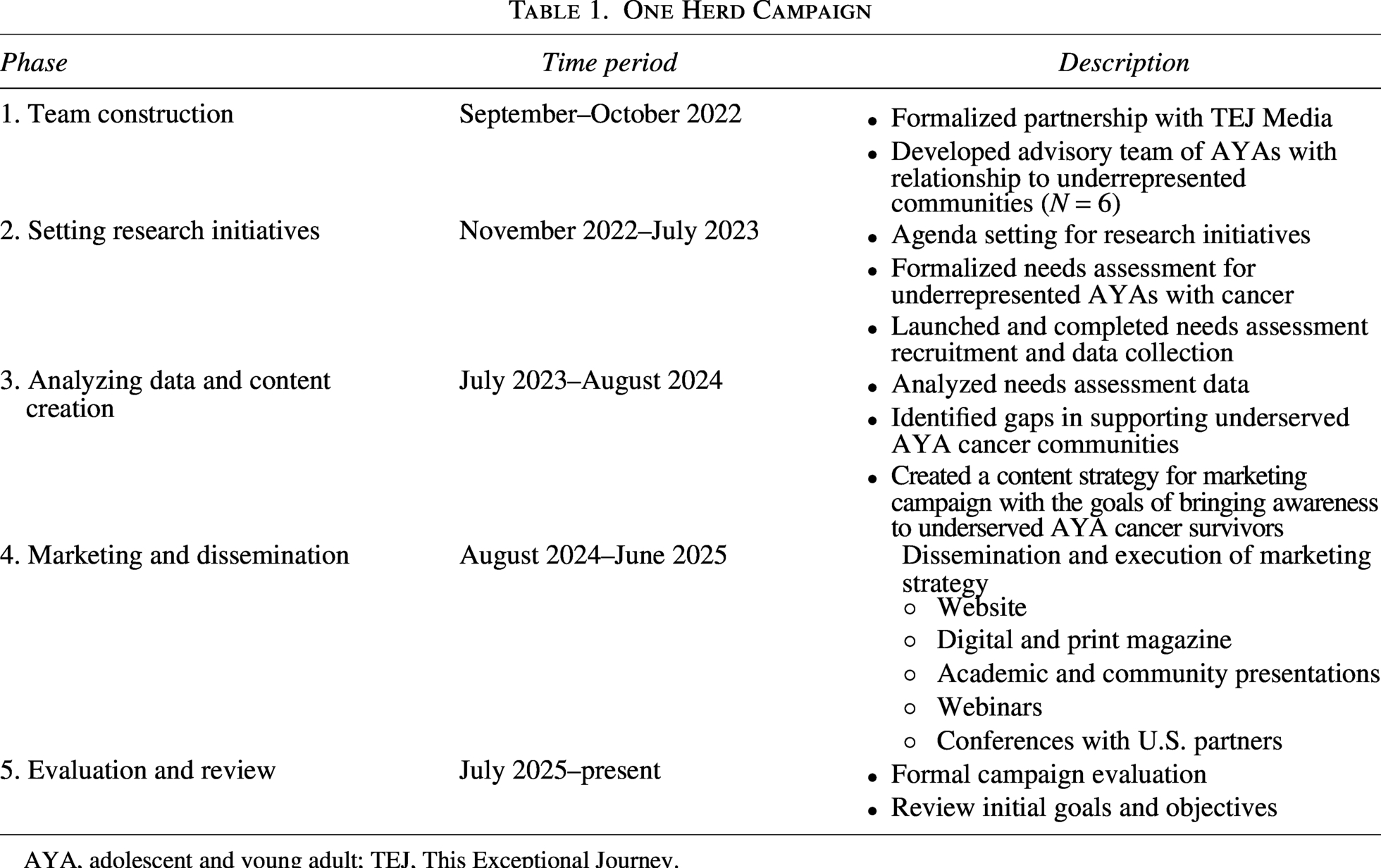
AYA, adolescent and young adult; TEJ, This Exceptional Journey.
Phase I: Team Construction
Campaign development
Phase 1 focused on assembling the One Herd advisory team. Elephants and Tea leadership (NG, KF, and RM) collaborated with TEJ Media (Y.M.) to recruit six community advisors who were themselves underrepresented AYA cancer survivors and recognized thought leaders in survivorship, health equity, mental health, health communication, epidemiology, and nursing. 36 Advisors contributed both lived expertise and professional insight in shaping the campaign’s direction. Responsibilities included participation in quarterly meetings, codevelopment of research questions (phase II), interpretation and refinement of preliminary findings (phase III), facilitating connections with aligned and allied organizations to expand campaign reach (phase IV), and contributing to program evaluation (phase V). Advisory members were offered either a $500 honorarium or the option to direct a $500 charitable contribution to an organization supporting underserved AYAs. This compensated, community-engaged advisory structure was intended to ensure accountability, representation, and power-sharing in the conception and deployment of the campaign. 37
Phase II: Research Initiatives and Goal Setting
Needs assessment design and recruitment
Phase II established the research priorities guiding the campaign. Through iterative discussion between January and February 2023, the One Herd advisory group identified a needs assessment as a foundational activity to inform equity-focused content development.38–40 Survey domains were selected based on (1) literature describing unmet supportive care needs and survivorship inequities among AYAs41–45 and (2) conceptual guidance from the World Health Organization’s SDOH Framework, 46 the National Institute on Minority Health and Health Disparities Research Framework,47,48 and Bronfenbrenner’s Social Ecological Model. 49 Survey content included sociodemographic characteristics, social needs, perceived experiences with the care team, social support, fertility-related care, mental health, spirituality, and storytelling.
The survey assessed domains associated with health-related social needs known to influence survivorship experiences, including transportation, financial toxicity, housing stability, social support, and community connection.9,23,41,44,50 These domains are reflective of SDOH mechanisms known to contribute to inequities in AYA cancer survivorship. A targeted national recruitment strategy was used, including outreach to hospitals with AYA programs, nonprofits, and industry partners who had accessed Elephants and Tea resources in the past (N = 10). The final instrument and domains are detailed in Supplementary Appendix and a recruitment flyer in Supplementary Appendix. The University of Rochester institutional review board (IRB) deemed this study exempt and not requiring of IRB oversight; data shared with researchers were not linked to identifiers and were not considered human subject research.
Phase III: Data Analysis and Results
Needs assessment findings
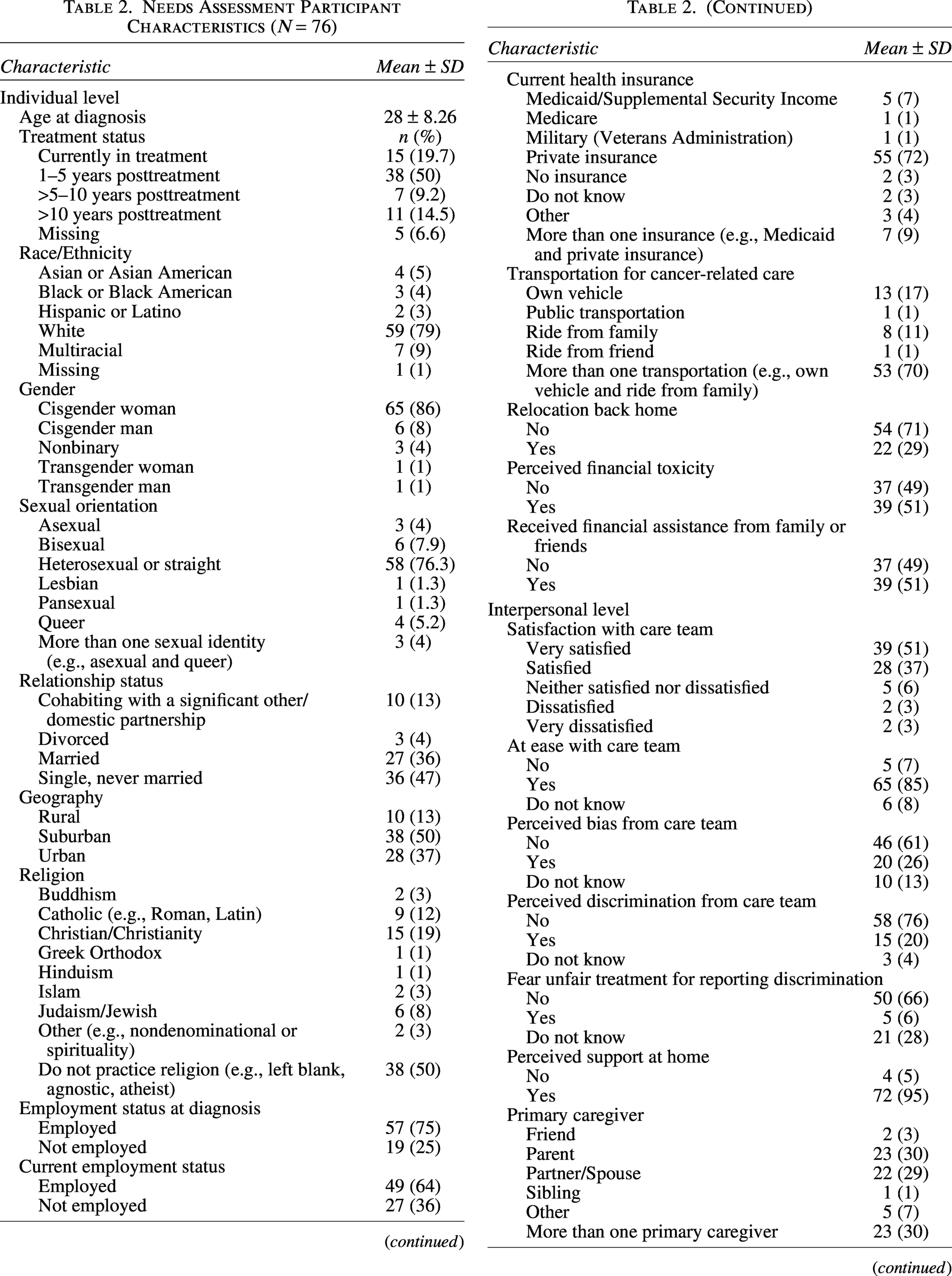
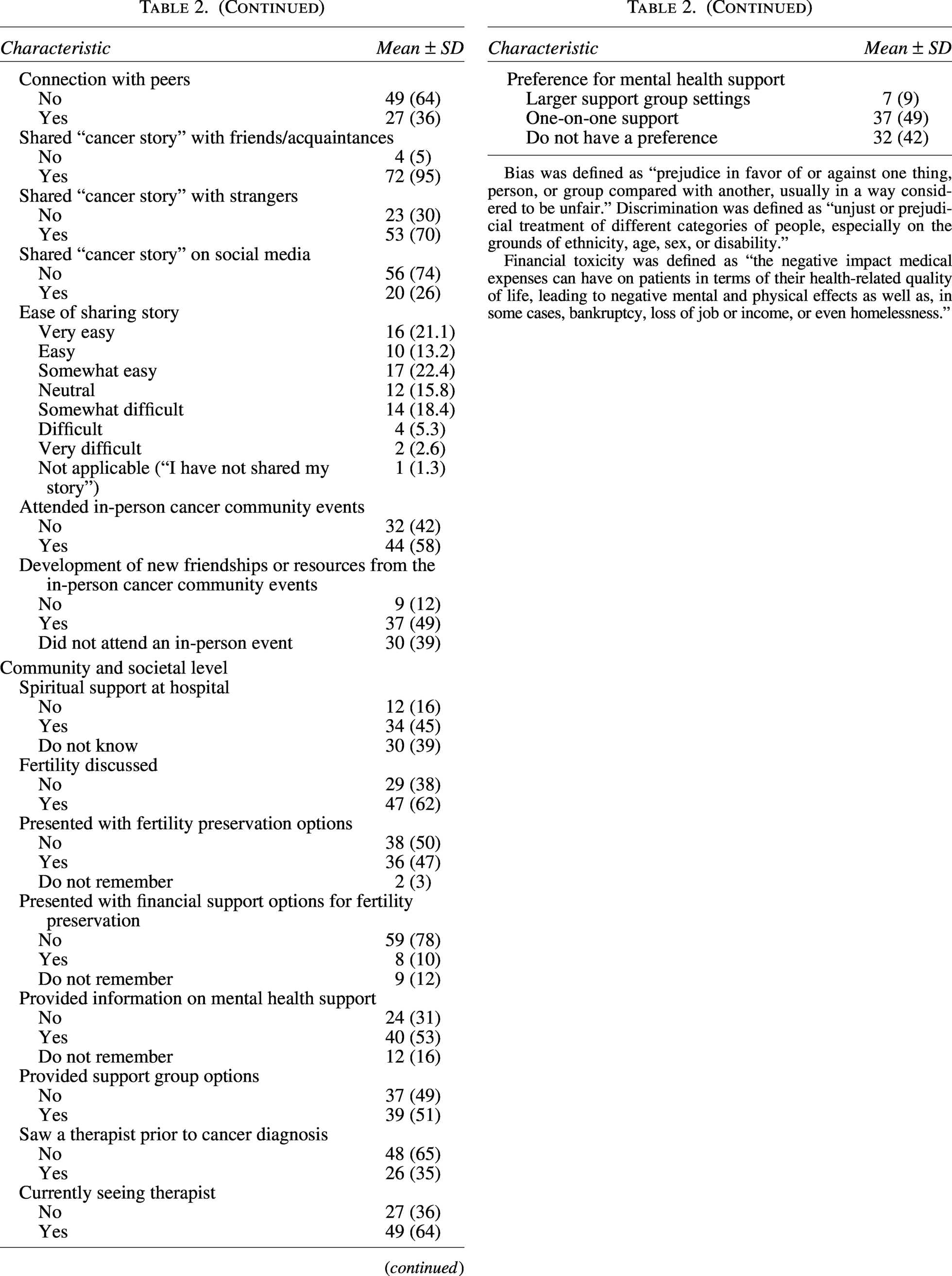
Phase III included data analysis and early content strategy development. A total of 81 respondents participated in the needs assessment; 76 were retained for analysis (Table 2). Survey data were analyzed using descriptive statistics, including means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Findings are summarized across three levels of influence (domains): 47 (1) individual (e.g., sociodemographic characteristics and social needs), (2) interpersonal (e.g., perceived interpersonal bias and discrimination and interpersonal support and communication), and (3) community and societal (e.g., institutional resources).
Needs Assessment Participant Characteristics (N = 76)
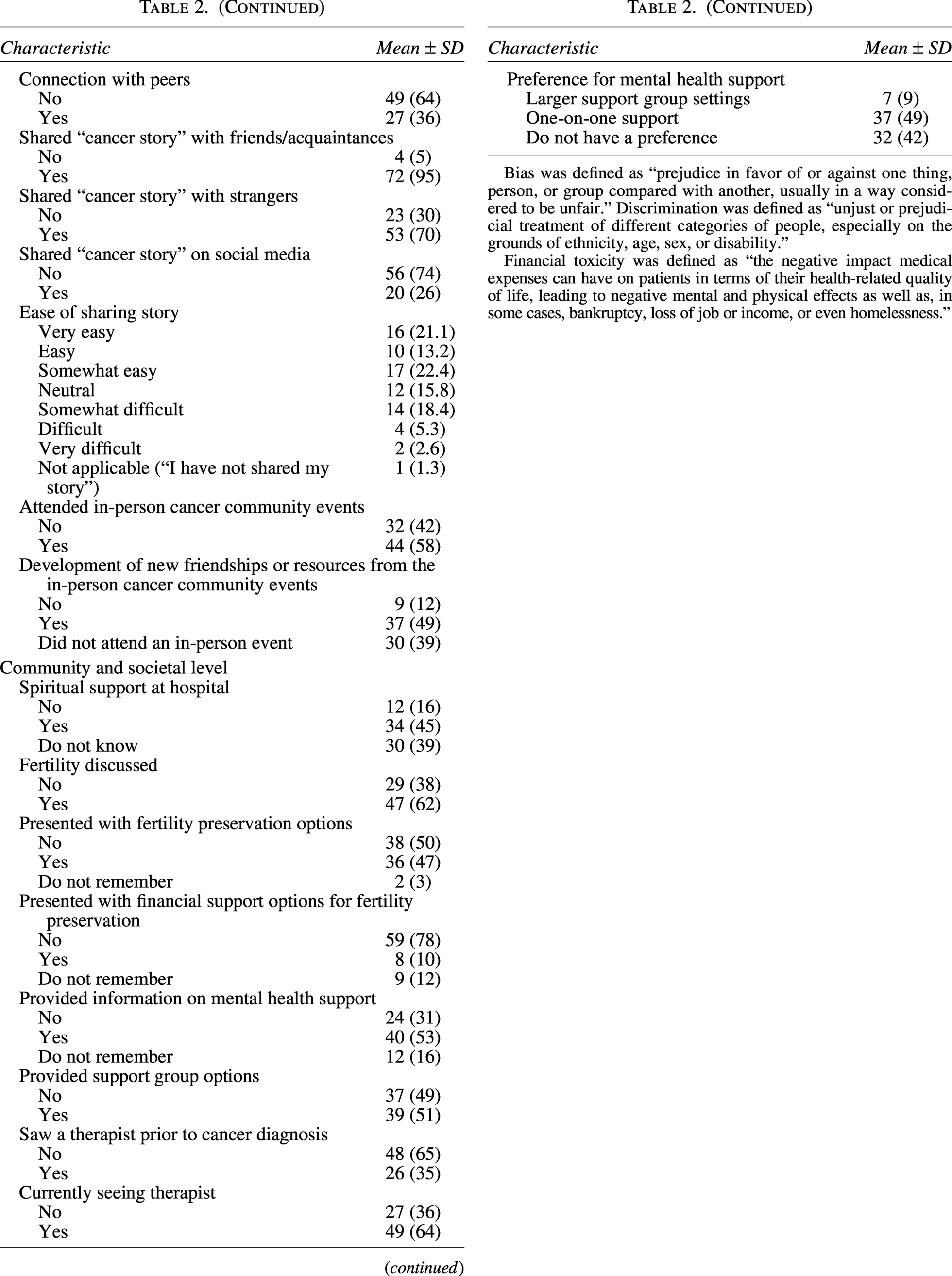
Bias was defined as “prejudice in favor of or against one thing, person, or group compared with another, usually in a way considered to be unfair.” Discrimination was defined as “unjust or prejudicial treatment of different categories of people, especially on the grounds of ethnicity, age, sex, or disability.”
Financial toxicity was defined as “the negative impact medical expenses can have on patients in terms of their health-related quality of life, leading to negative mental and physical effects as well as, in some cases, bankruptcy, loss of job or income, or even homelessness.”
Continued
Continued
Individual-level sociodemographic characteristics
Participants had an average age at diagnosis of 28 (±8.3) years. Twelve percent identified as Asian/Asian American, Black/African American, or Hispanic/Latino. The majority were cisgender women (86%), heterosexual (76%), employed (64%), and privately insured (72%). Approximately half were married or cohabiting with a significant other (49%), resided in suburban areas (50%), reported no religious affiliation (50%), and were <5 years posttreatment (50%).
Individual-level social needs
Seventy percent of AYA cancer survivors relied on multiple modes of transportation for cancer-related care, and 29% relocated to a parent’s home for treatment. Financial strain was common (51%), with many relying on financial support from family/friends.
Perceived interpersonal support and communication
Over one-quarter (26%) reported perceived bias from health care professionals during treatment, and 20% reported perceived discrimination from their care team during treatment. Most of the AYA respondents did not feel connected to peers during treatment (64%), although 95% reported feeling supported at home. Storytelling practices varied: the majority shared their story with strangers or friends and acquaintances (70%–95%), while fewer disclosed on social media (26%). One quarter (26%) expressed difficulty articulating their cancer story. Nearly half (49%) reported forming new connections or accessing cancer-specific resources through in-person community events.
Perceived institutional-level support services
Less than half (45%) of AYAs who responded reported access to spiritual or religious support through their treatment center. Fertility counseling and preservation support were particularly limited; 38% were not counseled on fertility, 50% were not offered preservation options, and 78% were unaware of financial assistance for fertility-related care. Half received information on mental health services (53%) or support groups (51%). One-on-one mental health care was strongly preferred (49%) over group-based support (9%). While 65% has not previously engaged with therapy before diagnosis, 64% reported currently seeing a therapist.
Within this formative sample, findings highlighted several multilevel gaps in supportive care relevant to the campaign’s equity-focused content development. Despite strong social support from family, AYA survivors lacked sustained peer connection during treatment, and some reported difficulties articulating their cancer story, suggesting unmet psychosocial and health communication needs. Structural barriers were also prominent: participants reported limited access to spiritual or religious services and a lack of or minimal awareness of fertility counseling, preservation resources, and financial assistance options for fertility preservation, which may underscore inequities in both information delivery and care navigation. Reports of perceived bias and discrimination within health care interactions further indicate that these gaps are not solely resource-based but also relational and systemic. Collectively, these findings illustrated how AYA cancer survivors continue to face concurrent social, financial, and institutional barriers that are insufficiently addressed through traditional survivorship models.
Phase IV: Marketing and Dissemination
Campaign implementation
Phase IV included dissemination of content created through the marketing campaign to both community and provider audiences. In response to the gaps identified through the needs assessment, the One Herd team developed a content strategy designed to translate findings into equity-focused storytelling and workforce education. In parallel with data analysis above, AYAs who expressed interest in sharing their lived experiences were invited to submit narrative pieces (N = 10). These narratives were integrated into the campaign using visual storytelling elements (e.g., photos and digital graphics) to reinforce representation, promote identity expression, and contextualize structural barriers within real-world survivorship experiences (Fig. 1). The strategy intentionally linked community voice with educational messaging to increase relevance for community health workers, patient navigators, and health care professionals serving underserved AYA populations.

Illustrative examples of digital storytelling from the One Herd community-based equity campaign.
Dissemination strategies included a dedicated landing page for the One Herd program (microsite), 35 a Digital and Print Magazine—One Herd: Giving a Voice to All, 36 academic and community presentations, 51 and webinars featuring panel discussions. See Supplementary Appendix for exemplars of these digital creative reports where needs assessment survey findings are complemented with personal stories from AYAs. In addition to virtual reach, the campaign was delivered across multiple in-person community events hosted in collaboration with partner hospitals and nonprofit organizations nationwide.
Additionally, we developed in-person and virtual events across the country with our partnering hospitals and organizations to disseminate the content campaign. One flagship event, a magazine launch in Buffalo, New York in September 2024, combined live storytelling with supportive care workshops (e.g., Healing Through Writing, Movement, and Creative Arts) to model narrative-based survivorship support in practice. Campaign findings were also integrated into Elephants and Tea’s AYA Program for Oncology Workforce Education and Resources (AYA POWER) in May 2025, 52 where One Herd advisory team members and two storytellers presented results from the needs assessment alongside their lived experiences.
Phase V: Evaluation and Review
Preliminary evaluation
Phase V is the final phase of One Herd and represents an ongoing evaluation period designed to assess the impact of the campaign as dissemination continues. Rather than a single endpoint assessment, evaluation is occurring iteratively and across multiple audiences. Health care professionals and AYAs are invited to provide feedback through post-event surveys. Initial evaluation surveys have already been distributed to participants of the AYA POWER session, and additional feedback will be collected from attendees of subsequent in-person and virtual events. The May 2025 POWER session had 40 virtual live attendees across multiple health disciplines. Eight attendees completed the post-session survey, and overwhelmingly respondents felt the first-person stories shared during the session were the most meaningful from the One Herd campaign.
This ongoing approach to evaluation allows the team to continuously assess changes in awareness, knowledge, attitudes, and survivor-centered communication practices, while also capturing the lived relevance of the campaign for AYA cancer survivors themselves. Findings from the evaluation will inform refinement of the content strategy and guide future directions for scaling this community-informed, equity-focused model of digital storytelling and workforce education.
Discussion
The One Herd content campaign represents an innovative and community-driven model for integrating research-informed digital storytelling into community-based AYA survivorship programming. By combining formative needs assessment data with narrative storytelling, the campaign demonstrates how lived experience can inform educational initiatives and workforce engagement.
Although the needs assessment sample was predominantly White, cisgender, and female, the broader campaign intentionally incorporated equity-centered approaches through multiple mechanisms. These included the formation of an advisory board composed of underrepresented AYA survivors and the integration of diverse lived-experience narratives through the storytelling component of the campaign. Accordingly, survey findings should be interpreted as formative insights used to guide campaign development rather than as a comprehensive representation of all underserved AYA cancer survivor populations.
Storytelling remains underutilized in oncology research and practice29,53,54 despite evidence that narrative approaches can enhance psychosocial well-being, identity formation, and social connection among AYAs.29,55,56 To our knowledge, One Herd represents the first to be systematically documented and evaluated. There have been novel approaches to engaging and partnering with AYAs to improve AYA cancer care and narrow outcome disparities, such as engaging with “social media influencers.” 57 This campaign is unique in its explicit design as a research-informed, community-led initiative that translates lived experience into equity-focused workforce education and system-level awareness.
Community-based organizations are uniquely positioned to facilitate these narratives because they operate outside traditional clinical structures and often have deeper trust among survivor communities. This campaign further supports storytelling as a meaningful equity strategy, particularly for AYAs from historically marginalized communities whose experiences are often absent from traditional oncology narratives and institutional datasets. Both community-based organizations and academic researchers who engage with AYAs should consider integrating digital stories into their programming and research studies. 56
An additional observation from the campaign was the emergence of other forms of marginalization, such as disability, neurodiversity, and weight-related stigma, that are rarely centered in the AYA cancer literature.58–60 These insights highlight the importance of intersectional approaches when addressing survivorship inequities.
The mean age at diagnosis of 28 years suggests that the needs assessment may reflect experiences more characteristic of young adulthood than adolescence. Developmental differences across the AYA age continuum may influence survivorship experiences, indicating the need for future research that explores age-specific survivorship needs.
Community-based organizations such as Elephants and Tea occupy a unique position in the AYA cancer care delivery landscape: they are embedded in the lived realities of AYA cancer survivors, trusted by historically excluded groups, and structurally nimble enough to surface narratives that clinical settings often overlook. In recognition of this role, Elephants and Tea has begun institutionalizing equity-oriented organizational practices by incorporating inclusive demographic and identity measures into registration systems to better reflect those served; intentionally curating and amplifying stories from AYAs across diverse racial, ethnic, disability, sexual orientation, gender identity, body size, and neurodiversity backgrounds; and partnering with media organizations such as TEJ Media to extend the reach of these narratives beyond oncology-specific spaces and into broader public discourse to influence cultural understanding and policy dialog.
These multilevel gaps illustrate not only unmet supportive care needs but also the importance of community-driven approaches that amplify lived experiences and translate survivor narratives into tools for education, advocacy, and system-level improvement. Storytelling in this context is not merely expressive; it functions as a mechanism of representation, accountability, and narrative justice for populations historically excluded from cancer discourse and survivorship research. By intentionally creating structured space for underrepresented voices, the campaign affirms the visibility of AYAs whose identities, needs, and experiences are often rendered peripheral or invisible within traditional care delivery models.
This work has several limitations. First, although the One Herd campaign was designed to center underserved and historically marginalized AYA survivors, the needs assessment sample was predominantly White, cisgender, heterosexual, and female, limiting generalizability to the broader diversity of marginalized AYA survivors. Second, the survey collected limited clinical variables and did not assess cancer type or treatment modality, which may influence survivorship needs. Third, the survey assessed perceived availability rather than participant preference for certain services, such as spiritual care. Finally, evaluation findings reflect early feedback from dissemination activities rather than long-term campaign impact.
The urgency of this work is heightened by current sociopolitical threats to equity infrastructure and data visibility in the United States.61,62 Federal actions aimed at restricting diversity, equity, and inclusion efforts, including Executive Orders targeting gender identity, the collection of sexual orientation and gender identity, and race data, represent not just administrative shifts but mechanisms of erasure.63–66 When demographic reporting and identity data are restricted, the communities most affected by disparities become statistically invisible, making inequities harder to document, resource, or remediate. In this landscape, community-based storytelling assumes an even more critical role as a countervailing force: it preserves visibility, affirms lived experience, and sustains truth-telling in spaces where policy threatens to narrow whose stories “count.”
Conclusion
The One Herd campaign demonstrates how community-based organizations can operationalize narrative equity by integrating storytelling, research, and workforce education. By amplifying survivor voices and translating lived experience into educational content, community-led storytelling initiatives offer a promising strategy for addressing structural inequities in AYA cancer survivorship.
Footnotes
Acknowledgment
The authors would like to thank the adolescent and young adult cancer survivors who participated in this campaign.
Ethics Approval Statement
The University of Rochester institutional review board (IRB) deemed this study exempt and not requiring of IRB oversight; data shared with researchers were not linked to identifiers and were not considered human subject research.
Patient Consent Statement
Patient consent was waived as all data were de-identified and collected in accordance with institutional ethical standards and the Declaration of Helsinki.
Permission to Reproduce Material from Other Sources
Elephants and Tea provided permission to reproduce images and graphics from their magazine.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
L.V.G. was supported by a Patient-Centered Outcomes Research Institute (PCORI) Eugene Washington PCORI Engagement Award (EACB-26540). Funding for the One Herd Content Campaign (secured by N.G. and K.F.) was provided by Eisai, Genentech, and Pfizer. N.R.B. was supported by the National Cancer Institute of the National Institutes of Health under Award Number K00CA253762 and the National Institutes of Health Extramural Loan Repayment Program for Health Disparities Research (L60CA284359).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.