
Abstract
Purpose:
Child, adolescent, young adult survivors of cancer (CAYAs) experience social and psychological hardships after treatment completion. As CAYAs transition to adult contexts, their cancer identity and its associated public perceptions may shape how they are treated in these settings. It is critical to understand the content of these beliefs in same-aged peers to help CAYAs navigate them. To explore the associations and drivers that underlie childhood cancer stereotype formation and stigma for CAYA survivors, college students listed their associations with this concept and completed measures of familiarity and stigma.
Methods:
We used freelisting to explore cultural models of childhood cancer. College students (N = 125) wrote down up to 15 words that they associated with childhood cancer. Participants also completed the Level of Contact Report and the Family Questionnaire, adapted for CAYA cancer, to assess stereotype differences based on established contributors to cancer-related stigma.
Results:
Participants (mean age = 20.77 years, standard deviation = 5.15 years) listed the most common diagnoses and treatments. Those with lower familiarity (no personal contact; n = 79) more frequently mentioned organizations. Those with greater familiarity (personal contact, n = 46) more frequently listed symptoms. Participant lists also differed based on family stigma toward CAYA cancer (mean[SD] = 24.11 [6.91], range = 12–73). Participants with higher stigmatization scores (median split at ≥ 24) listed more media-driven, warrior-focused imagery, while participants with lower stigma scores (<24) listed empathetic terms more frequently.
Conclusion:
These findings illustrate the influence of media and cancer-focused organizations in shaping cultural domains of CAYA cancer in a population that has low personal familiarity with the disease.
Background
Advances in treatment and early diagnosis have led to a growing number of childhood cancer survivors, many of whom are adolescents and young adults. 1 Throughout this article, we refer to this group of survivors up to 39 years of age as children, adolescents, and young adults (CAYAs). Despite improved survival, CAYAs continue to face lifelong physical and psychosocial challenges after treatment completion. These challenges include difficulties forming and maintaining social relationships,2–6 psychological distress,7–10 and barriers to educational attainment and employment.4,7,11,12 While a multitude of factors contribute to these social and psychological difficulties, the role of public perceptions, specifically stereotypes about cancer survivorship, is often overlooked. In CAYAs, stigma has been demonstrated to have a social impact (e.g., un- or underemployment, psychological distress, social exclusion), as well as physical effects.13,14
As CAYAs, in particular adolescents, navigate emerging adulthood, public perceptions and stereotypes about their cancer may shape how they are treated in social, academic, and professional settings, making it critical to understand the content of these beliefs. 15 In each of these contexts, CAYAs decide whether to disclose their often concealable cancer history.16–18 Disclosure can be associated with negative stereotypes or discrimination, leading to hurdles in the workplace and in their romantic relationships.18–21 Current evidence suggests that fear of poor reactions based on stereotypes leads CAYAs to conceal their cancer in new relationships, hampering their social life and generating psychological strain.16–18,22–24 Similarly, parents of CAYAs experience stereotyping, referred to as caregiver stigma. Parents of children with cancer experience socioeconomic strain as well as changes in their peer relationships, leading to isolation and greater psychological distress.25–28
The transition to adulthood poses a significant challenge for CAYAs and an opportunity to redefine or disclose their identity.16,17,29 To examine stereotypes that may shape these experiences, we recruited emerging adult college students, with whom CAYAs interact in academic, social, and early professional settings, to list associations with childhood cancer. By focusing on childhood cancer, we aimed to elicit spontaneous, culturally shared beliefs about cancer conceptualized as a past experience rather than an active illness. As stereotypes form the cognitive basis of stigma, identifying the beliefs peers hold about cancer survivorship is a critical first step in understanding how stigma develops and affects CAYAs.
Given the limited literature on CAYA stereotypes, we used freelisting to assess culturally shared knowledge and examine the content and structure of stereotypes. 30 As stigma can be reduced and stereotypes altered by contact with someone from the stigmatized group, 31 we examined differences between those that did and did not have personal contact with childhood cancer. Given the familial nature of childhood cancer and the effect of stigma on caregivers of CAYAs, we also explored differences in associations based on caregiver stigma.
Methods
Design
Data for this study were collected as part of a larger randomized trial examining the influence of media portrayals on CAYA stigma, the results of which are published elsewhere. 32 Due to the specificity of the topic and the comparative nature of the analyses (i.e., familiar vs. unfamiliar, greater vs. smaller caregiver stigma), we aimed to recruit 125 participants, consistent with sample size recommendations for freelists. 33 Participants were recruited through undergraduate and graduate courses in behavioral health at a public university in the Southeast USA. They received extra credit for their participation. The freelist was on a digital platform and available to students at any time. All participants viewed a digital informed consent form and agreed to participation using a radial button in the survey. The project was approved by the University of South Florida Institutional Review Board (STUDY3320) and deemed exempt.
Measures
Freelisting
To understand stereotypes and current associations of college students with CAYA cancer, we used the freelisting method grounded in cognitive anthropological theory.34,35 Participants were instructed to “Please list what you associate with childhood cancer in the fields below. List as many associations as you can think of.” Participants were provided with 15 slots into which they could enter responses; however, it was not mandatory to fill all slots.
CAYA cancer familiarity
We assessed familiarity with CAYA cancer using the Level of Contact Report, 36 which is a single-item scale asking participants to check all applicable of 12 different statements describing degrees of contact with people with mental illness. This measure was adapted by changing “severe mental illness” to “children or adolescents with cancer” (e.g., “My job involves providing services/treatment for children or adolescents with cancer”).
Caregiver stigma
We assessed CAYA caregiver stigma by adapting the Family Questionnaire. 37 Caregiver stigma is the stigma associated with an individual who is closely related to someone with the stigmatized identity.38,39 The original Family Questionnaire (FQ) is a 12-item questionnaire asking participants to respond to a vignette about the father of a 30-year-old woman with mental illness. Participants then complete 12 items representing different stereotypes of mental illness (e.g., “I would think that Beth’s condition is John’s fault.”) on a 9-point scale from “not at all” to “very much.” The vignette was adapted to change “schizophrenia” to “cancer” and change the age of the character from 30 years to 15 years old to indicate CAYA cancer. Cronbach’s alpha for the adapted FQ’s 12 items was 0.61 (95% confidence interval 0.52–0.70) in this study.
Data analysis plan
Attention questions were interspersed throughout the survey to ensure active participant engagement. All participants completed the questions correctly.
Our methodology and examination of results were guided by Bernard and colleagues’ (2016) book Analyzing Qualitative Data. Data were cleaned by collapsing similar items into one category (e.g., “hospital” included “hospitals,” “hospital stays,” etc.). This process, conducted by the primary author of this article, is subject to interpretation. A complete list of which variations were subsumed under a larger category is provided in Supplementary Appendix.
Data were analyzed using Visual Anthropac—Freelists 1.0 (Analytic Technologies), which is a free, open-source program for analyzing freelists (www.analytictech.com/anthropac/anthropac.htm). Following guidelines by Bernard and colleagues (2016), data were analyzed for (1) frequency, which assumes that more frequently mentioned items have higher cultural value, (2) average rank, which examines the average position of words within a list, with more common terms in the cultural domain being mentioned earlier, and (3) saliency, which divides the percentile rank by the total number of lists to calculate overall prominence in the cultural domain.30,40 Additionally, we identified an inflection point. The inflection point in a freelist reflects the point after which responses become too diffuse to be interpreted. Following established freelist analytic convention, we determined the natural inflection point visually as the point after which there were too many responses for a specific frequency to be meaningfully interpreted.
After an analysis of all data, differences based on familiarity and caregiver stigma were examined. Participants were split into those who had personal experiences with childhood cancer and those who did not have personal experiences with CAYA cancer, using the Level of Contact Report. Using SPSS Version 28 (IBM Corp., 2021), we identified the median on the FQ and assigned all participants to be either above or below the median for further analyses. Additionally, a t-test was conducted to identify differences between groups in terms of age and caregiver stigma (for the groups split based on familiarity).
Results
Demographics
Our freelist sample consisted of 125 total participants (mean age = 20.77 years, standard deviation = 5.15 years); however, some participants did not complete demographic information. We included all participants who had complete data on the freelist, regardless of their completion of the remainder of the surveys. Our sample consisted of predominantly female-identifying participants (n = 73), with some male-identifying (n = 9), and non-binary (n = 3) participants. Most participants (n = 46) identified as White/Caucasian, with some Asian (n = 11), African American/Black (n = 8), Native American/Pacific Islander (n = 1), mixed race (n = 9), or other (n = 9). Of our sample, 26 participants identified as Hispanic/Latino, and 57 did not.
Freelist
Participants listed between 1 and 15 words with an average of 6.21 (standard deviation = 4.29) words listed.
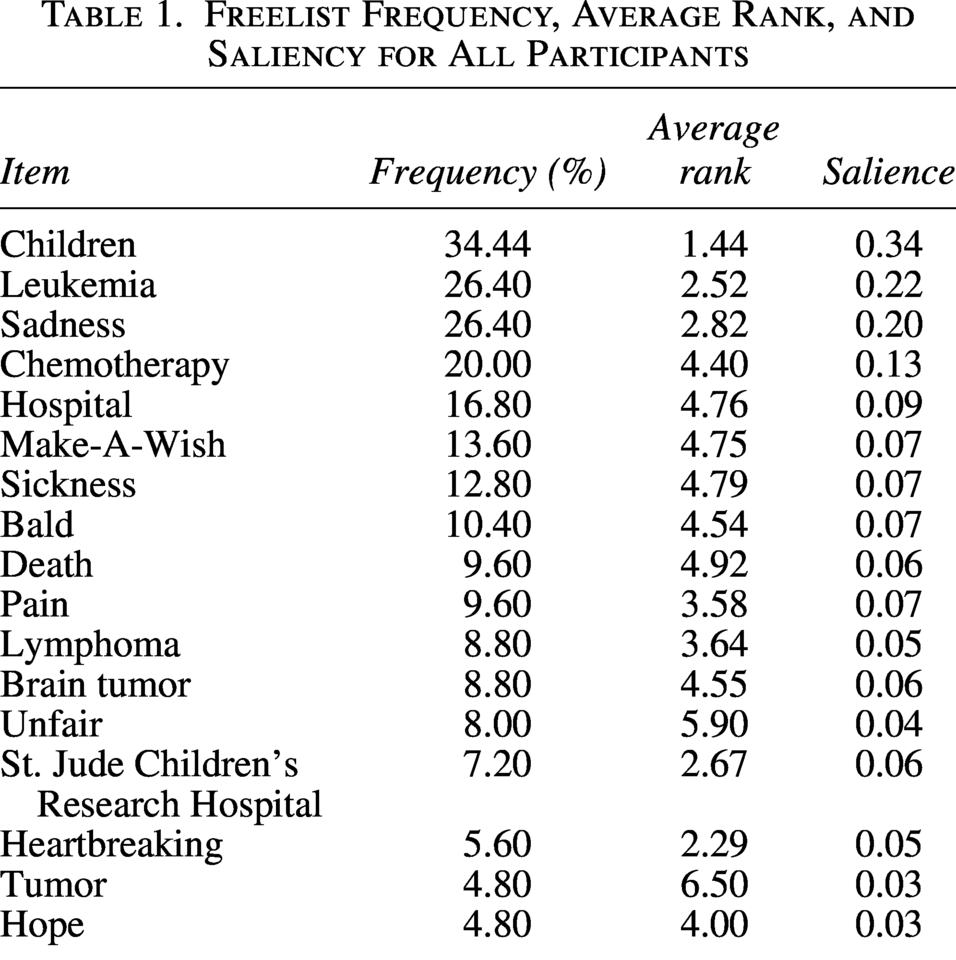
Overall, “children” was listed most frequently (35.8%), followed by “leukemia” and “sadness” (both 27.5%), and “chemotherapy” (20.8%). Other cancer types were also listed above the inflection point in the list, including “lymphoma” (9.2%), “brain tumor” (9.2%), and “tumor” (5.0%). Childhood cancer-related organizations featured rather prominently, too, with “Make-A-Wish” (13.3%) ranking above “St. Jude Children’s Research Hospital” (7.5%). “Death” was listed by 10.0% of participants and ranked within the top 10 most frequently listed words. Table 1 displays the complete list of words, frequencies, average ranks, and saliency.
Freelist Frequency, Average Rank, and Saliency for All Participants
Familiarity with CAYA cancer
Familiarity with CAYA cancer ranged across the entire spectrum of possible responses. Notably, almost all participants (n = 112, 90.3%) reported that they consumed media about CAYA cancer, and a majority of participants (n = 63, 50.8%) reported that a movie, television show, or documentary was their closest level of contact (see Table 2). Of those with closer contact, most had a family friend (n = 38, 79.2%) or relative (n = 25, 52.1%) who had experienced CAYA cancer. Only one participant (0.8%) in our sample was a survivor of CAYA cancer.
Level of Familiarity Across Personal Contact and Non-Personal Contact Groups
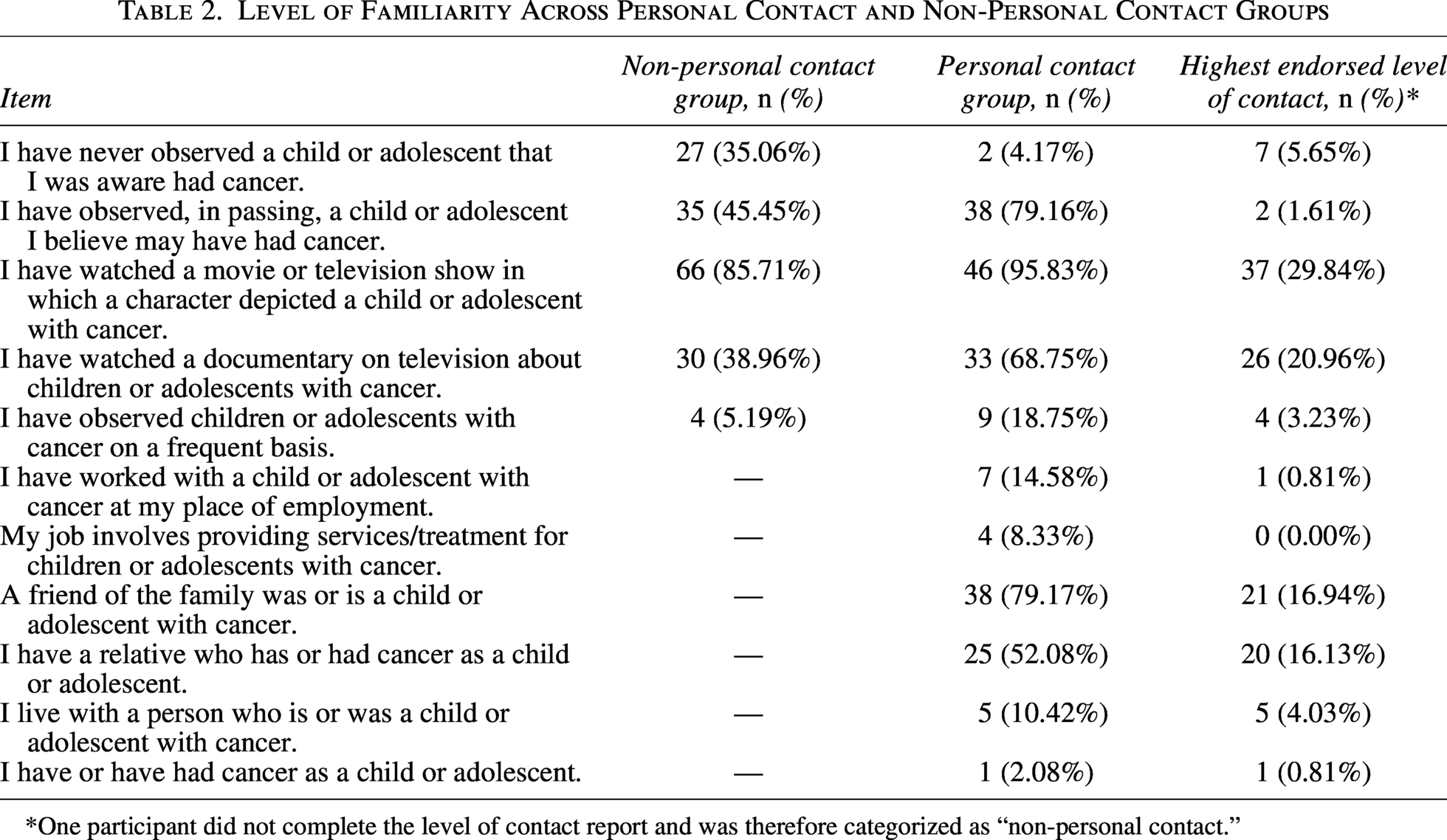
One participant did not complete the level of contact report and was therefore categorized as “non-personal contact.”
Based on the level of familiarity, we divided our sample into a personal contact (PCG; n = 48, 38.4%) and a non-personal contact group (NPCG; n = 77, 61.6%). The groups did not significantly differ in terms of age or caregiver stigma scores (p > 0.05).
We determined that an inflection point for the freelist would be near the 10% mark (9.2% for PCG and 8.9% for NPCG). Tables 3 and 4 display the frequencies, average rank, and salience for the PCG and NPCG.
Freelist Frequency, Average Rank, and Saliency for Non-Personal Contact Group
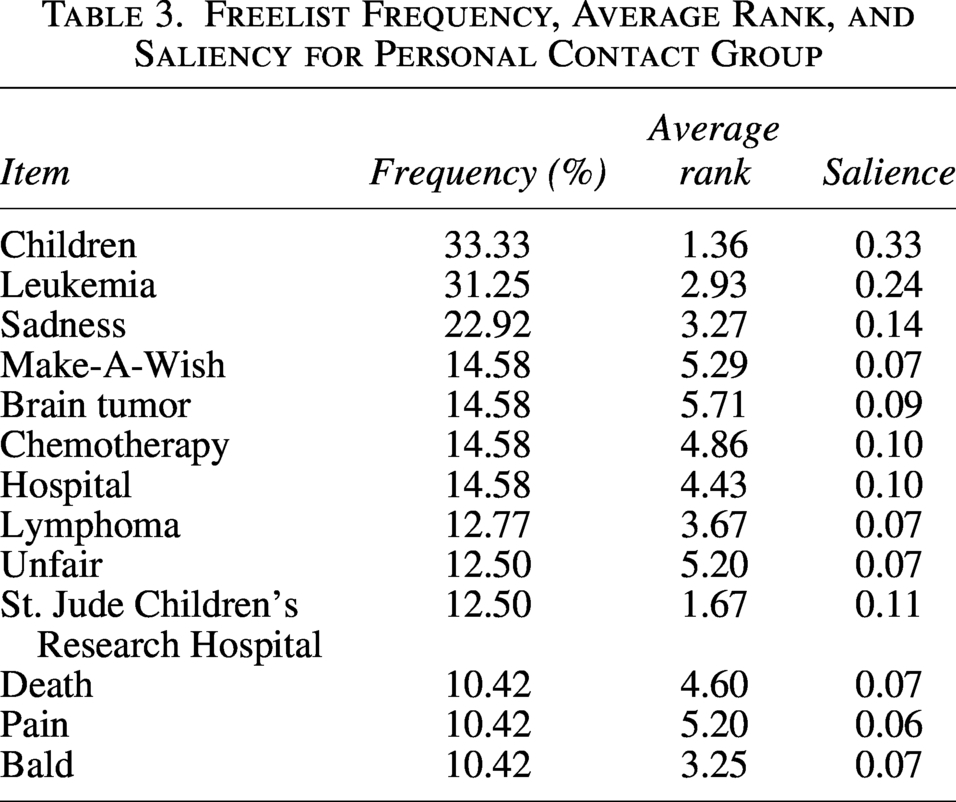
Freelist Frequency, Average Rank, and Saliency for Personal Contact Group
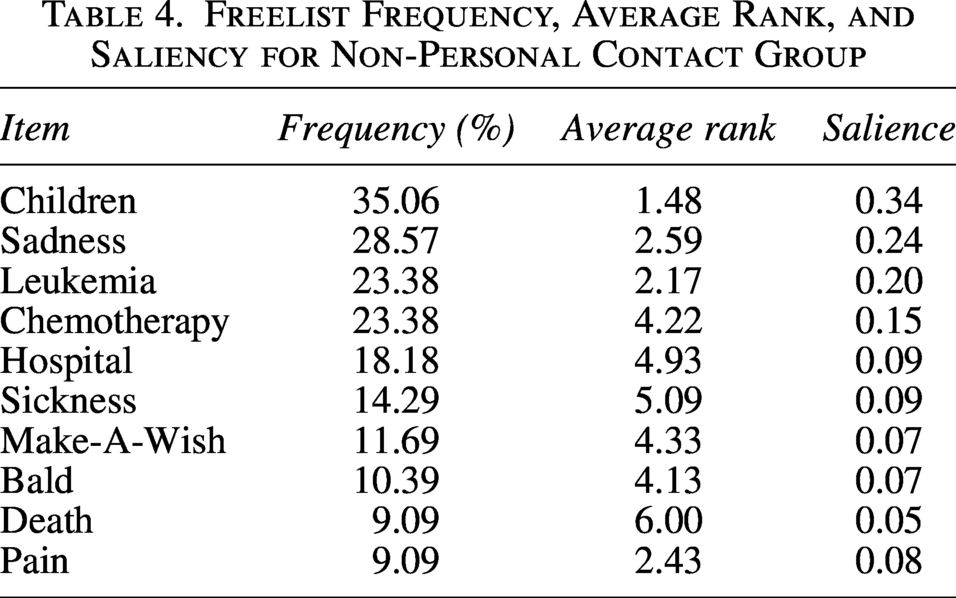
“Children” was the most frequently listed item for both the PCG and NPCG (34.1% and 36.7%, respectively). “Sadness” (29.3% PCG, 26.6% NPCG) and “leukemia” (29.1% and 24.4%, respectively) were second and third most frequently listed for both groups, in reversed order. Those in PCG listed specific cancers, such as “brain tumor” (17.1%) and “lymphoma” (14.6%), whereas the NPCG listed “chemotherapy” (25.3%) and “hospital” (19.0%), items that appeared less frequently and with lower average rank than in the PCG.
Organizations featured more prominently in the NPCG, with both “St. Jude Children’s Research Hospital” and “Make-A-Wish” appearing with a slightly higher frequency, average rank, and saliency than in the PCG, indicating higher familiarity with constructs associated with cancer. The PCG listed “death” at a very similar frequency, rank, and salience compared with the NPCG. “Unfair” appeared only in the PCG.
“Baldness” and “pain” were the only symptoms mentioned in both lists, with the PCG listing “bald” higher than the NPCG and listing “pain” with slightly higher frequency but lower average rank than the NPCG.
Family stigma
We used the FQ to determine whether our participants had high or low caregiver stigma. The FQ scores ranged from 12 to 73, with a mean of 24.11 and a standard deviation of 6.91. We conducted a median split at a sum score of 24 and compared the freelists of these two groups. Groups did not differ significantly on demographic variables.
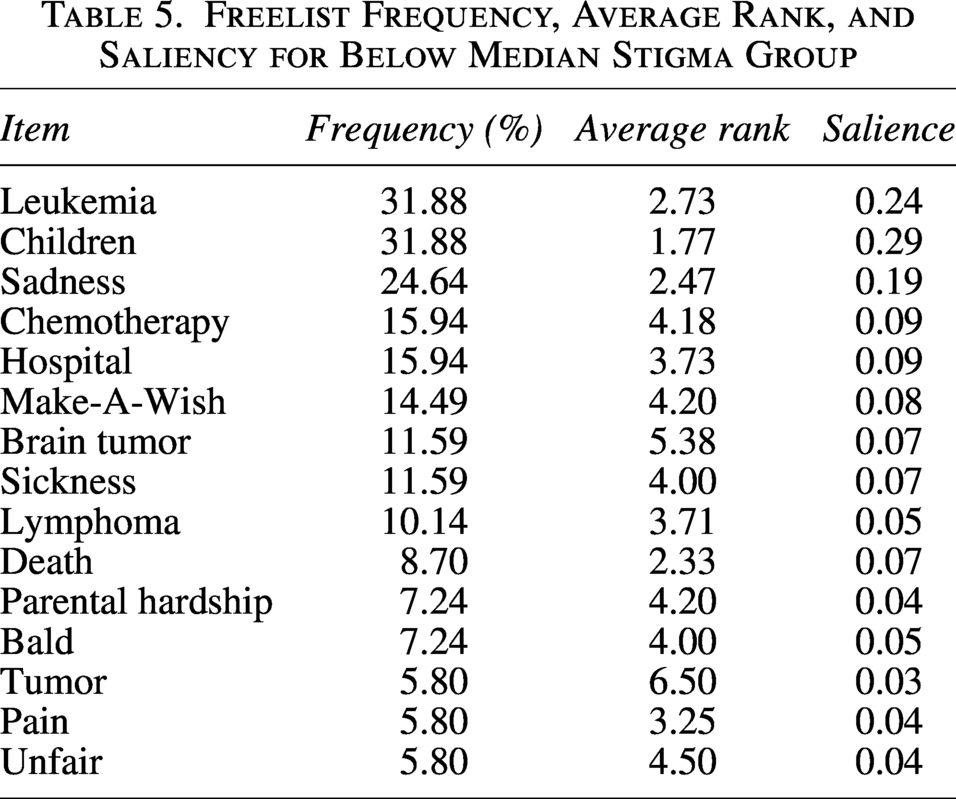
Those in the below median split stigma group (BMSG, n = 69; see Table 5) listed the same top three associations as the aforementioned groups. Those in the above median split stigma group (AMSG, n = 53; see Table 6) listed “children” (41.2%), “sadness” (31.4%), and “chemotherapy” (27.5%) as the top three responses.
Freelist Frequency, Average Rank, and Saliency for below Median Stigma Group
Freelist Frequency, Average Rank, and Saliency for above Median Stigma Group
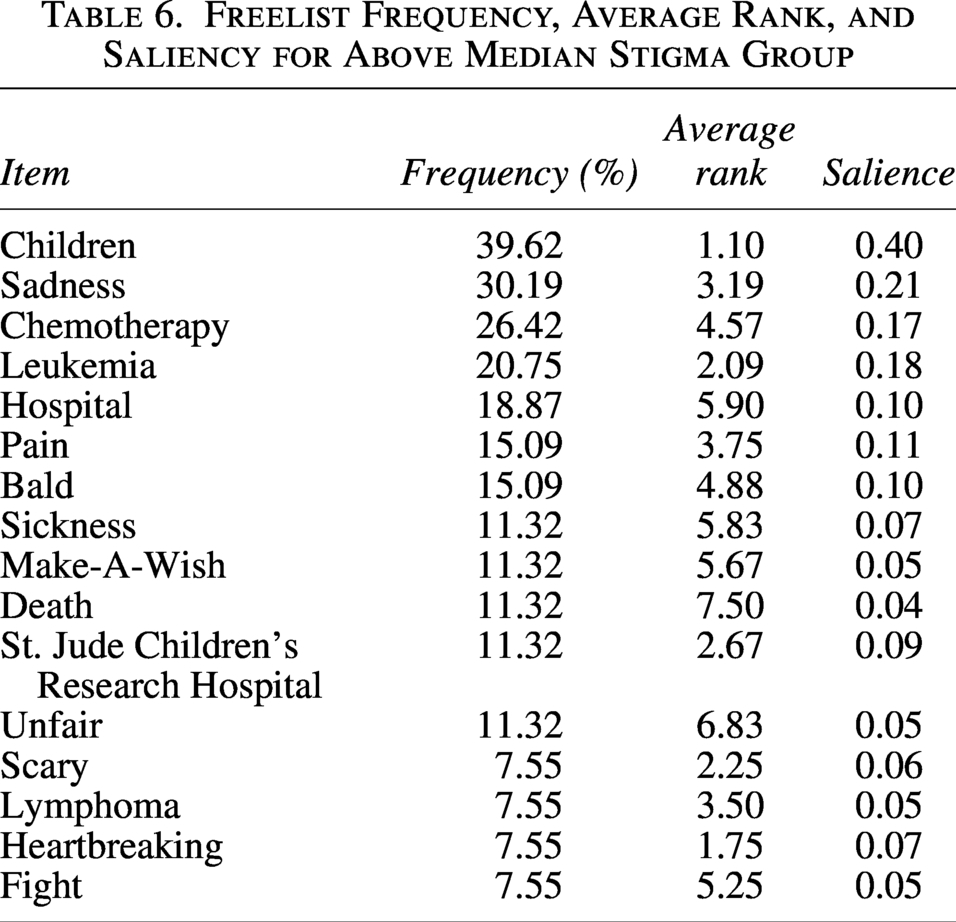
Other notable distinctions between the lists included that “brain tumor” (11.6%) and “tumor” (5.8%) were mentioned only in the BMSG. Additionally, the BMSG mentioned “parental hardship” (7.2%). “Pain” (15.7%) and “bald” (15.7%) were mentioned more frequently in the AMSG than in the low stigma group (5.8% and 7.2%, respectively). Additionally, the AMSG mentioned “heartbreaking,” “scary,” and “fight” at 7.8%, while these were not mentioned in the BMSG. “Death” was mentioned slightly more in the AMSG (11.8%) than BMSG (8.7%). However, it was ranked higher and had higher saliency in the AMSG.
Discussion
Findings from this study demonstrated that while there was a largely common cultural domain among college students, associations and stereotypes varied depending on the level of personal contact the participant had with CAYA cancer and the level of caregiver stigma. NPCG listed organizations more prominently, while those with personal experience listed emotional words more frequently. The AMSG more frequently listed media-driven battle imagery than those with lower stigma scores, suggesting that such images may contribute to CAYA stigma. Notably, the most common associations were diseases and treatments, indicating general awareness of CAYA cancer.
Aligning with research from the mental illness field, our findings differed based on the level of personal experience with the stigmatized identity.41,42 The PCG listed more emotional language than those without personal contact. For example, “unfair” appeared only in PCG, emphasizing the emotional aspect of a personal connection with cancer. Meanwhile, organizations were mentioned with higher frequency in the NPCG, as those without personal contact are more likely to draw on organizations and media for the representations of cancer in the absence of personal experience. This finding emphasizes the importance of these organizations in shaping the image of cancer survivors.
Participants in the AMSG were more likely to refer to stereotypical language, such as “heartbreaking,” “scary,” and “fight.” This pattern is consistent with battle imagery, portrayed in many movies and magazines do.19,43 Evidence from other stigmatized identities suggests that media depictions often underlie stigma development.44,45 Given the high prevalence of media consumption in this sample, it is likely that media significantly contributed to the cultural domain. While such depictions in relation to CAYAS may appear to be positive, praising CAYAs for their bravery and using battle imagery to amplify this praise, this media deemphasizes the psychological needs of parents and patients, creating an unattainable ideal.19,43
The BMSG referred to parental hardship more frequently. The FQ assesses family stigma; thus, a consideration of parental hardship is likely to yield more empathy for the parents and therefore a lower score on the FQ. Importantly, this indicates an awareness of the family dynamics involved in CAYA cancer that did not appear across other groups. Parents of child and adolescent patients experience psychosocial and financial hardship during their child’s treatment;25–28 however, narratives of CAYA cancer often deprioritize parents and their mental health needs.19,43 Our finding suggests that greater awareness and understanding of the caregiving burden involved in CAYA cancer occurred more frequently in those with lower stigma. Additionally, those in the BMSG referred more frequently to specific diseases, indicating greater knowledge of the CAYA cancer domain, aligning with stigma research indicating that greater knowledge of a disease reduces stigma. 46
Across groups, “leukemia” and “chemotherapy” were mentioned frequently, reflecting an accurate perception of adolescent cancers and their treatment, though knowledge was not directly measured. 47 These are also the most common diseases and treatments depicted in movies, perhaps indicating the power of media to influence public perceptions or educate about childhood cancer. 43 Given that 90.3% of this sample reported media consumption and for half of this sample, this was the closest level of contact, media was likely the primary influence on our participant’s responses, emphasizing this as a second primary source for participants to draw information from.
Cancer stigma is theorized to be driven by its strong stereotypical association with death and the desire to avoid those associated with death.48,49 CAYAs themselves have reported fears that their peers associate them with death and being contagious.50,51 Media often overemphasizes the extent to which CAYA cancer is associated with death, representing a higher mortality rate than reality, which may lead to fatalism in cancer patients and a strong association between cancer and death in the general public.19,43 Though death is theorized to be a driver of the stigma around cancer, 49 it was mentioned only by 10.0% of all participants. Additionally, the frequency of listing “death” differed little across stigma groups, indicating that perhaps this is not as common of an association as theorized.
Understanding what the perceptions of CAYA cancer are, is an important first step in developing treatments to address these stereotypes. Patients may explicitly have to address some of these stereotypes as they navigate the contexts outside of a medical environment. Not endorsing stereotypes is an important aspect of stigma resistance, thus discussing and debunking stereotypes can help patients resist stigma they may face.52–54 Simultaneously, patients may already be aware of and internalizing these stereotypes when they receive a diagnosis. An explicit discussion of stereotypes by providers with their patients (especially those with less familiarity with childhood cancer) and challenging those stereotypes through cognitive rehabilitation techniques may improve psychological well-being. This approach has been found to be effective for addressing other types of stigma, such as mental illness stigma. 55
While associations overall were frequently neutral or positive, these stereotypes may still have negative effects on the stigmatized. A study investigating the impact of stereotypes on identity formation in childhood cancer survivors found that they internalize both positive and negative stereotypes. 56 The fear of these stereotypes can lead to CAYAs not disclosing or discussing their cancer identity to avoid workplace discrimination or strains in their personal relationships, increasing loneliness and complicating social connection.17,21 Thus, a complete understanding of the stereotypes CAYAs are aware of and responding to is an important step in supporting survivors in their social interactions.
Limitations
This study recruited a large number of participants, enabling a comparison of several smaller subgroups; however, participants were college students, who were predominantly female and white/Caucasian, limiting the study’s generalizability to other populations. Furthermore, the responses indicate that the freelist prompt may have required more specificity. Several responses, such as “children,” indicated that the prompt was too broad, and thus, responses were non-specific. Even the most frequently appearing words had rather low frequencies, indicating that childhood cancer is not a well-defined cultural domain and that many of our participants were unfamiliar with it. Nonetheless, this study is an important first step in identifying the stereotypes that are in the cultural domain of CAYA cancer in college students.
Future studies should endeavor to garner a patient perspective, both to understand patients’ own associations with their disease and their perceptions of stereotypes they are anticipating, navigating, and confronting. Furthermore, this study focused on survivors at a specific age (15 years old), but cancer-related stigma may vary across different stages of the CAYA trajectory. Therefore, future studies should explore how survivor age influences stigma perceptions.
Conclusion
This study yielded two key findings. First, CAYA cancer represents a diverse but largely accurate cultural domain in college students that varies according to personal familiarity and family stigma. Lower familiarity was associated with more frequent references to organizations, whereas personal experience was associated with greater emotional content. Higher family stigma scores were associated with more frequent listing of media-driven battle imagery.
Second, these findings underscore that for individuals with limited personal exposure to CAYA cancer, associations are shaped predominantly by media portrayals and cancer-focused organizations. Consistent with stigma research from other health contexts, media-driven imagery appears to contribute to stigmatizing representations. As such, both media outlets and cancer-focused organizations carry significant responsibility in shaping public perceptions of CAYA cancer for a populace with limited personal exposure.
Authors’ Contributions
K.K. was involved in conceptualization, methodology, project administration, supervision, and reviewing and editing. D.M.T. aided in the conceptualization, supervision, analysis, and reviewing and editing. R.T.W. aided in supervision and editing. N.L. was responsible for all aspects of this project.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding for this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.