
Abstract
Purpose:
Adolescent and young adult (AYA) patients with cancer face complex decisions about family building, often compounded by misconceptions about hereditary cancer risk. Although guidelines recommend early discussion of fertility- and genetics-related risks, these topics are inconsistently integrated into routine care. To address this gap, we developed Reproductive Education and Fertility Links for Cancer Treatment (REFLECT), a digital health application designed to provide education and decision support related to fertility, genetic risk, and future family building for AYAs with cancer. This study developed and pilot-tested REFLECT to support informed decision-making.
Methods:
REFLECT was developed using evidence-based content and implemented on a web-based platform integrating multimedia education and decision support. Two iterative rounds of user testing were conducted with AYA survivors (ages 18–39) using a Learner Verification framework to assess comprehension, usability, relevance, and acceptability. Participant feedback informed iterative refinements.
Results:
Participants (N = 16) reported that REFLECT was engaging, easy to navigate, and relevant to fertility, genetics, and future family-building concerns. Iterative testing identified opportunities to improve navigation, accessibility, and content organization, which were addressed through refinement. Participants reported increased confidence in discussing fertility preservation and genetic risk with providers and emphasized the value of an integrated patient-centered tool, particularly at the time of diagnosis.
Conclusion:
This pilot demonstrates that REFLECT is feasible, acceptable, and usable among AYAs. By integrating fertility and genetic risk education with decision support in an accessible digital format, REFLECT addresses a critical gap in AYA oncology care. These findings support further evaluation in clinical settings.
Keywords
Introduction
Adolescent and young adult (AYA) patients with cancer face complex decisions related to future family-building options, often compounded by concerns of hereditary cancer risk and long-term effects of cancer treatment. Although approximately 10% of AYA cancers are hereditary,1–3 many perceive their cancer as hereditary regardless of clinical confirmation. 4 Notably, 65% of female AYA cancer survivors reported concerns about transmitting cancer risk to future offspring, regardless of mutation status. 4 Such misconceptions can influence reproductive decision-making, highlighting the need for accurate, developmentally appropriate education early in the cancer care continuum.5–11
Recognizing these challenges, professional societies (American Society for Reproductive Medicine, 12 American Society of Clinical Oncology, 13 National Comprehensive Cancer Network 14 ) recommend early counseling regarding fertility risks, reproductive options, and referral to genetic services for patients undergoing gonadotoxic therapies. Despite these guidelines, the majority of AYA patients report not engaging in discussions regarding fertility preservation (FP) or genetic risks at diagnosis.15–25
Consultations with reproductive and genetic specialists can clarify hereditary risk and inform decisions related to genetic counseling (GC), genetic testing (GT), and reproductive planning.26,27 Yet, these services are not uniformly integrated into standard AYA oncology care.17,28–31 AYA patients express strong preferences for receiving this information before or during treatment planning rather than after treatment completion.27,32 However, access to reproductive and genetic specialists is often limited, and referral practices are inconsistent across clinicians and institutions.17,27–31,33 Furthermore, patients who decline genetic services often report a desire for better education about genetic risk,34–37 while others outside typical referral criteria still seek information to guide family-building decisions. 27
Psychosocial barriers further complicate addressing AYAs’ genetic risk and future family-building concerns. 38 Uptake of GC/GT among eligible patients remains low (14%–36%), with even lower rates among racial and ethnic minority populations.39–41 Common reasons for declining GC/GT include limited knowledge of genetic risk, cost-related concerns, and fears of discrimination.34–37 Awareness of reproductive technologies such as preimplantation GT is also limited. 26 Despite substantial fertility-related distress and preferences for earlier communication, discussions about fertility and genetic risk are often delayed or absent.27,38,42 Thus, interventions must address psychosocial barriers while optimizing the timing, format, and accessibility of education and decision support.
Psychoeducational interventions have demonstrated efficacy in bridging knowledge gaps, addressing psychosocial barriers, and facilitating behavior change.43–47 Digital health applications are increasingly utilized in oncology to deliver education and support decision-making.48–50 AYA patients demonstrate a strong preference for digital formats over traditional paper-based education and show enhanced engagement with mobile and web-based technologies.51,52 Use of mobile health (mHealth) applications has been associated with improvements in AYA patients’ cancer knowledge, treatment adherence, and communication with clinicians. 53
However, although digital tools have been developed to address genetic risk in hereditary cancer populations (e.g., Rosa chatbot for BRCA-related cancers 54 and NEST CRC, an educational platform for early-onset colorectal cancer 55 ) and fertility-related concerns among AYAs (e.g., the Fex-Can Fertility program 56 ), existing interventions typically focus on either genetics or fertility, rather than the intersection of both. Moreover, many tools are tailored to adult populations or address single domains such as distress management or self-help.52,57 Currently, there is no integrated digital intervention designed to support both genetic risk communication and fertility in AYA oncology.
In response to these gaps, this study presents the development and preliminary evaluation of the Reproductive Education and Fertility Links for Cancer Treatment (REFLECT) digital health application, a theory-informed digital health tool designed to deliver integrated education and decision support for AYA patients with cancer. The overarching objective was to develop and iteratively refine the REFLECT application through successive rounds of user testing and to present preliminary findings on its feasibility and potential to enhance informed family-building decision-making among AYA patients with cancer.
Methods
Intervention description
REFLECT is a web-based digital health application that provides integrated education and decision support related to FP, genetic risk, and future family building for AYA patients with cancer. The educational framework was informed by prior formative research with AYA survivors and providers examining the intersection of these domains. 27
Developed in partnership with Nest Genomics, REFLECT adopts their customizable, HIPAA-compliant, cloud-based platform. The Nest Platform 55 functions as a “genetic companion,” supporting patient engagement through delivery of educational content and care-related tasks. The platform incorporates accessibility features (e.g., adjustable font size, audio content, inclusive imagery) and delivers developmentally appropriate content for clinical settings and home use.
REFLECT adapts the Nest platform to deliver multimedia education to AYAs with cancer. The adapted application includes core sections addressing fertility and genetics in cancer and future family building. Specifically: (1) “Learn Library”: self-paced educational resources; (2) “Understanding how cancer impacts fertility”: effects of cancer and treatment on reproductive health; (3) “Reviewing FP options”: pathways for future family building; (4) “Paying for fertility treatment”: financial considerations and resources; (5) “The importance of genetic testing”: hereditary cancer risk, GC/GT, and reproductive implications; and (6) “Decision-Making”: a values-based decision support tool 58 to clarify priorities, assess readiness for services, and support question generation for clinical encounters (Figs. 1 and 2). The content is modular, allowing flexible engagement based on individual needs.
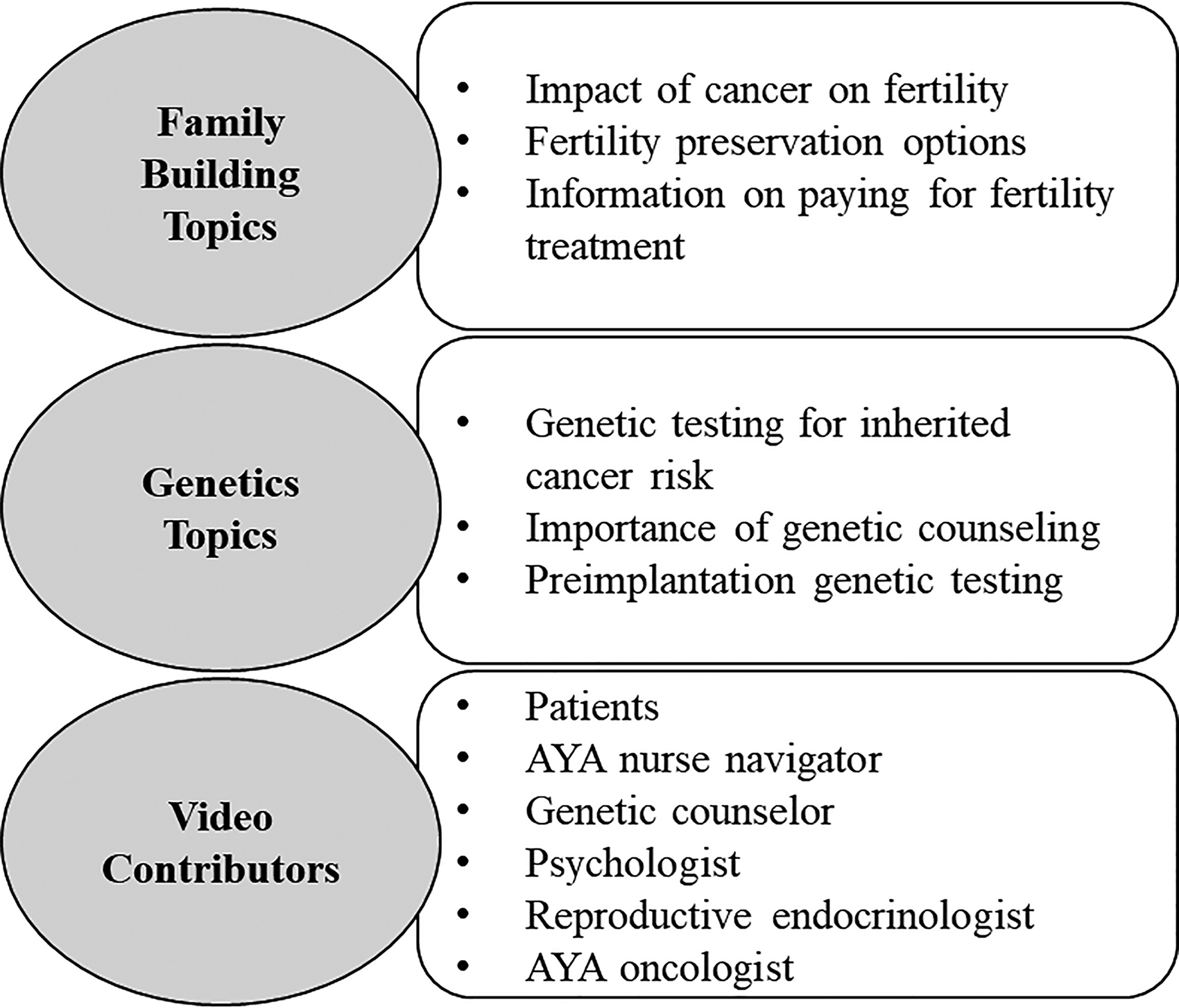
Topics included in REFLECT. REFLECT, Reproductive Education and Fertility Links for Cancer Treatment.
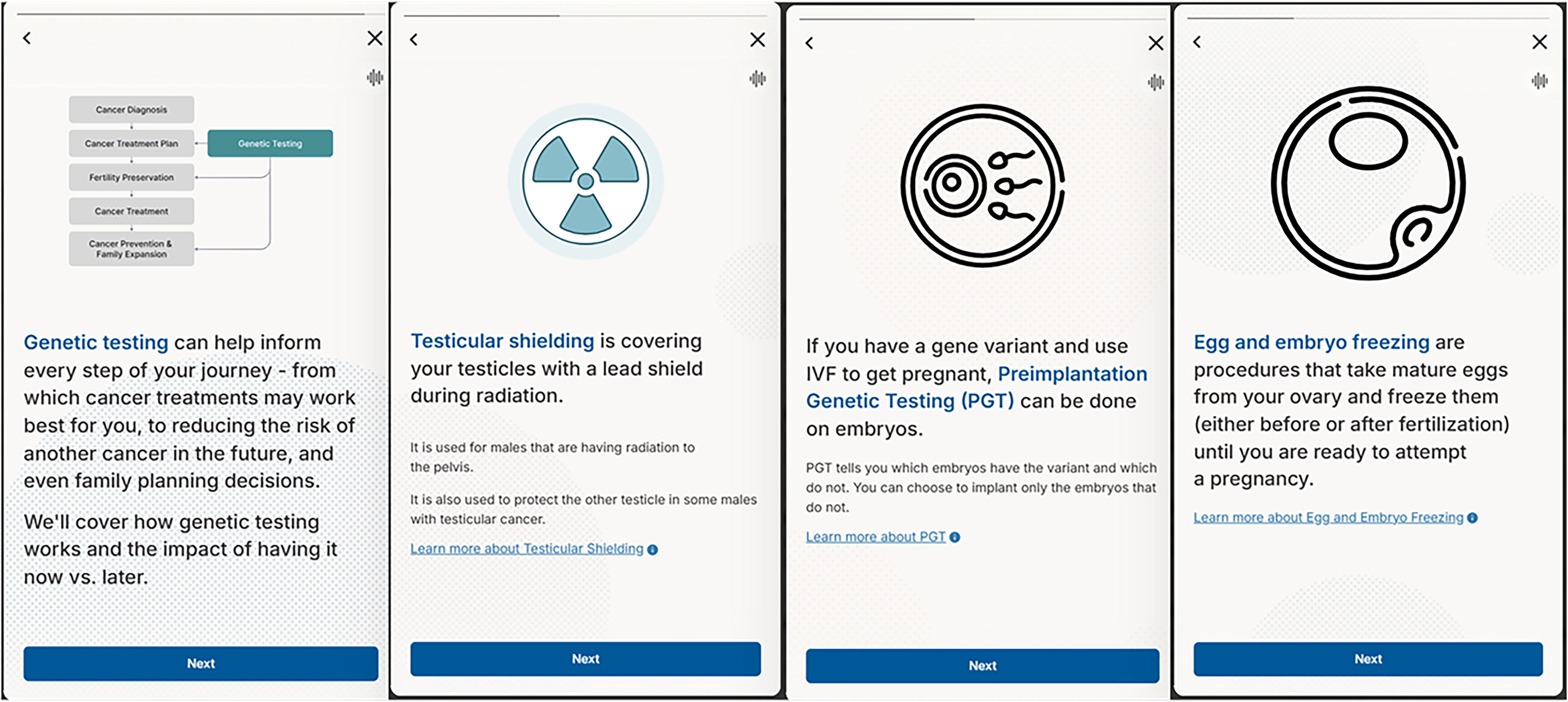
Example REFLECT screenshots depicting educational and interactive features.
Prior to piloting, the prototype underwent expert review by clinicians and researchers in oncology, oncofertility, and cancer genetics, with feedback informing refinements to clinical accuracy, clarity, terminology, and educational flow.
Participant recruitment
Participants were AYA cancer survivors aged 18–39 who had received care at an NCI-designated comprehensive cancer center. Eligibility criteria included (1) history of cancer diagnosis, (2) ability to speak and read English, (3) consideration of having children in the future, and (4) access to an internet-enabled device. All participants had completed primary cancer treatment at the time of participation and reflected on their experiences with fertility- and genetics-related decision-making. Participants were recruited through institutional referral networks, AYA program listservs, and targeted outreach. All participants provided verbal informed consent. The study was approved by the Moffitt Cancer Center Scientific Review Committee and Advarra Institutional Review Board (MCC #22569).
Learner Verification interviews
User testing was conducted using a two-round iterative design. In each round, participants interacted with REFLECT during individual semistructured interviews conducted via Zoom. Interviews were guided by a Learner Verification (LV) framework59,60 and incorporated a Concurrent Think-Aloud 61 approach, in which participants were asked to verbalize their thoughts, reactions, and interpretations while navigating the tool in real time. Semistructured interview guides assessed key domains central to application development, including (1) comprehension and ability to process information, (2) usability and navigation, (3) relevance to personal decision-making needs, (4) accessibility and design features, and (5) overall acceptability and cultural appropriateness.59,60
Participants were additionally encouraged to identify areas of confusion and recommendations for improvement. Round 1 participant feedback was synthesized to identify usability challenges and guide refinements in collaboration with Nest Genomics. A second group of participants then evaluated the revised version of REFLECT in Round 2 using identical procedures. This iterative process ensured that participant feedback directly informed successive refinements of the tool.59,60
Usability was assessed using five items adapted from the System Usability Scale (SUS)62,63 at the conclusion of each interview. Participants rated each item on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with negatively worded items reverse-coded. Items assessed perceived ease of use, complexity, confidence using the tool, integration of features, and likelihood of future use.
Data analysis
Qualitative data were analyzed leveraging a thematic analysis approach 64 integrating both deductive and inductive coding. Domains were guided by LV constructs59,60 with additional emergent domains identified inductively. A preliminary codebook was developed through independent coding of two transcripts by two coders (S.P.D., P.W.L.), followed by consensus meetings. All transcripts thereafter were double-coded, and discrepancies were resolved through discussion. Inductive themes were developed through pattern recognition across transcripts. Saturation was defined as no emergence of new themes during interim analysis. 65 Findings were synthesized after each round to inform iterative refinement of REFLECT.
Qualitative analyses were conducted in MAXQDA 66 and reported in accordance with the Consolidated Criteria for Reporting Qualitative Research guidelines. 67 Quantitative data were analyzed descriptively. Given the adapted version of the SUS, usability data were summarized using item-level descriptives rather than a summed score.
Results
Participant characteristics
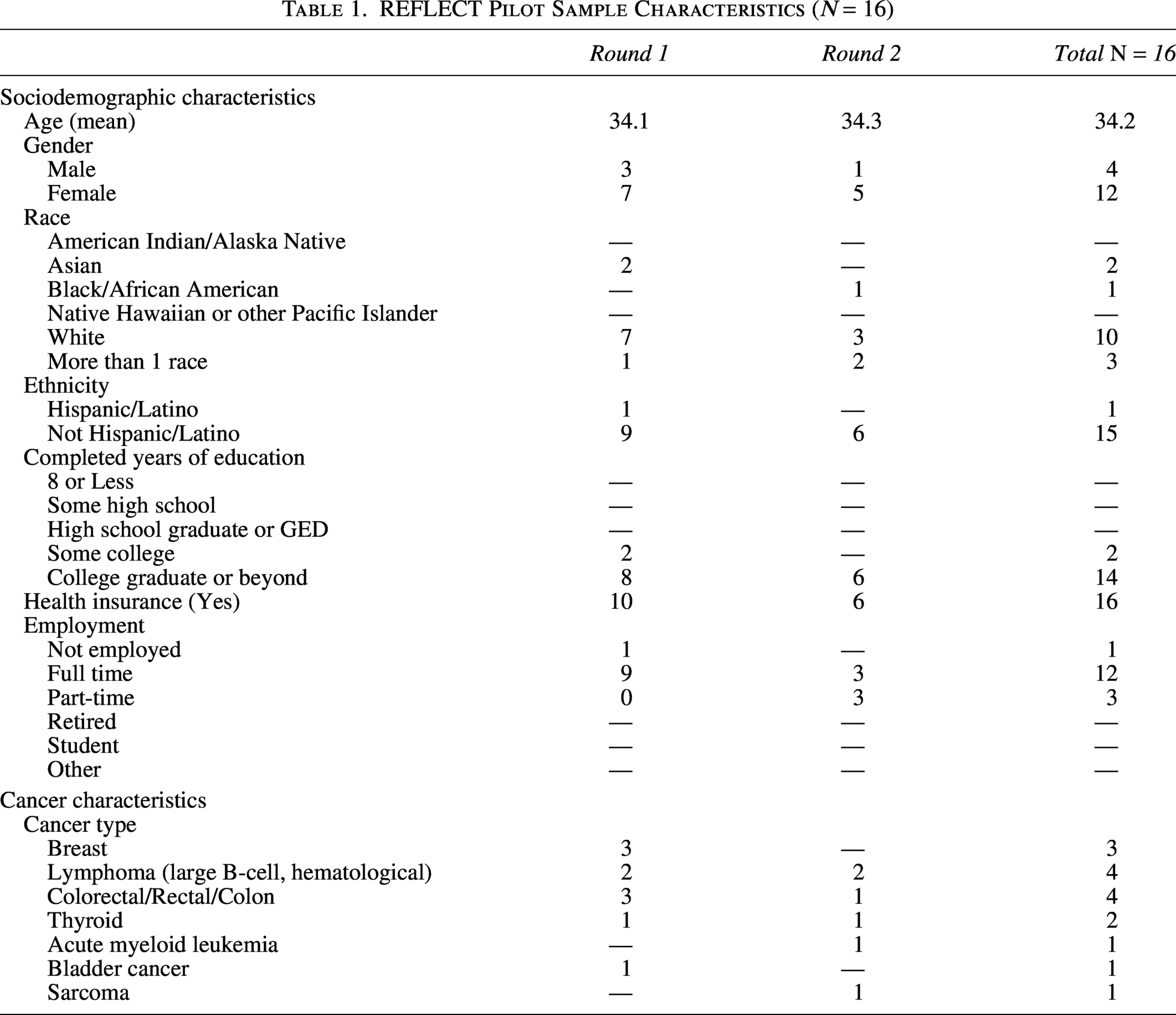
Two independent samples participated in two rounds of user testing (Round 1, N = 10; Round 2, N = 6), for a total sample of 16 participants. Participants had a mean age of 34 years (range 26.9–39.7); were primarily female (75%), White (62.5%), and non-Hispanic (93.8%); and had completed a college degree or higher (87.5%). Cancer diagnoses included breast cancer (18.8%), lymphoma (18.8%), colorectal/rectal cancer (18.8%), thyroid cancer (12.5%), and other malignancies (Table 1).
REFLECT Pilot Sample Characteristics (N = 16)
LV-guided qualitative findings
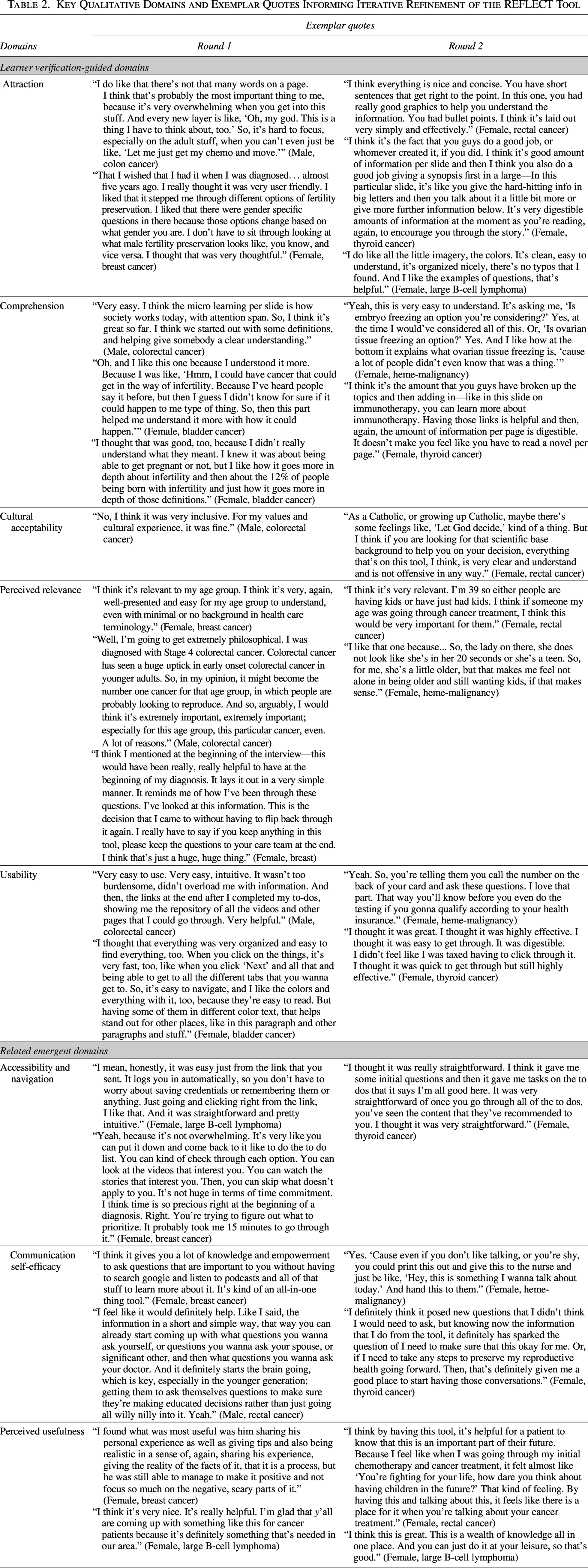
Findings were consistent across rounds, with no substantively new domains emerging in Round 2. LV-guided domains and emergent themes are summarized in Table 2 by interview round.
Key Qualitative Domains and Exemplar Quotes Informing Iterative Refinement of the REFLECT Tool
Attraction
Participants across both rounds described REFLECT as engaging, visually appealing, and easy to approach. Concise text, structured layout, and visual design were perceived to reduce information overload, particularly when engaging with fertility- and genetics-related content.
Comprehension
AYAs demonstrated strong comprehension of the REFLECT content. Across rounds, participants reported that the information presented was clear and understandable, with several highlighting the benefit of the multimedia format and opportunity for self-directed learning. Participants described content as digestible and appropriately paced, with one noting, “the micro learning per slide is how society works today, with attention span…” (male, colorectal cancer). Specific to the genetics content, one participant noted, “I think genetics can be very overwhelming. And that broke it down to be easy to read, or easy to understand, not too overwhelming, too stressful” (female, AML). Others noted that breaking topics into smaller sections and embedding links enhanced comprehension.
Cultural acceptability
Participants consistently reported that REFLECT was culturally acceptable and respectful of personal values. Content was perceived as inclusive and nonoffensive across both rounds.
Perceived relevance
Participants described the tool as highly relevant to their needs related to fertility, genetics, and future family building. Several participants highlighted the value of having FP and genetic risk information integrated within a single, patient-centered digital platform, noting that this addressed gaps in prior care experiences. One participant stated, “My overall impression was that it was very helpful, and especially with my past experience, because with my past experience, to be honest, I was just given a couple pieces of paper, like a pamphlet…” (female, breast cancer).
Usability
Across both rounds, REFLECT was described as user-friendly, intuitive, and easy to navigate. The organization and pacing of content were viewed as facilitating efficient engagement without contributing to cognitive overload. One participant noted, “Very easy to use. Very easy, intuitive. It wasn’t too burdensome, didn’t overload me with information… I thought it was quick to get through but still highly effective” (male, colorectal cancer). Clear navigation and visual design further supported usability.
Related emergent domains
Accessibility and navigation
Participants noted that the application was accessible, describing the layout as intuitive and the content as easy to locate and navigate. Audio features and visual organization supported accessibility, particularly for alternative learning preferences.
Communication self-efficacy
Participants reported that REFLECT supported communication self-efficacy by clarifying priorities, reducing pressure around sensitive treatment decisions, and preparing them for conversations with providers. One participant explained, “I like that it’s very clear that there’s no right or wrong choice… Decisions can feel like there’s a lot of pressure. Having that statement feels very low pressure… I liked being able to go within a rating system… especially if this is a tool that gets shared with a provider. I think that allows you to communicate your desires with your provider more clearly” (male, colon cancer). Participants attributed these effects to the values-based decision support component, which helped structure thinking, articulate preferences, and build confidence navigating clinical interactions. As one participant noted, “You’re giving us guidance on how to go into our appointments… you don’t know what to ask. You don’t even know what that doctor is called” (female, heme-malignancy).
Perceived usefulness
REFLECT was found highly useful due to its ability to consolidate fertility and genetic information that had previously been fragmented or difficult to access. Several participants noted that having integrated, patient-centered content in a single digital tool made information easier to engage with and apply to their own care. One participant reflected, “I think that it helps give people the confidence that they need to talk to their oncologist… I spent a lot of time during my cancer journey trying to get this information and I felt like a lot of it was in that tool” (female, rectal cancer).
Iterative refinement of REFLECT
Despite overall positive perceptions, participants identified minor usability and accessibility challenges during Round 1 testing. Areas for improvement included difficulty locating resources, clearer “Learn Library” navigation, requests for audio features, and streamlined content organization. One participant requested, “Is there any way that we could maybe change the organization of it or anything like that to make it more useful or intuitive?” (female, thyroid cancer). Another emphasized the importance of making the “Learn Library” more visible, stating, “I don’t really have much other than maybe put the learn section in the dashboard or homepage, because I definitely didn’t look all into that. Because sometimes, with these new apps, you don’t really go to look at the little page thing” (female, large B-cell lymphoma).
In response to this feedback, the study team collaborated with Nest Genomics to update the platform. Revisions included restructuring the “Learn Library” to improve content discoverability, enhancing navigational cues, adding audio functionality, and refining the visual layout and flow of the decisional support component. Subsequent user testing indicated improved ease of navigation and clarity.
Systems usability scale across both rounds
Patterns of responses to the adapted SUS items were consistent across both rounds of user testing. Item-level descriptives demonstrated high agreement with ease of use (M = 3.83), confidence using the tool (M = 3.50), and likelihood of future use (M = 3.25) on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Participants reported low agreement on items assessing unnecessary complexity (M = 2.00) and inconsistency (M = 2.00), indicating minimal perceived usability barriers.
Discussion
This pilot study demonstrates that REFLECT is a feasible and acceptable digital health application for AYAs seeking information about FP, genetic risk, and future family building after a cancer diagnosis. Across two iterative rounds of user testing, participants described the application as engaging, easy to navigate, and relevant to their needs. Participants also reported increased confidence in discussing FP and genetic services with providers and emphasized the value of integrating both domains within a single, patient-centered, digital platform. Collectively, these findings suggest that REFLECT addresses a critical gap in AYA oncology care27–29,38,68 by providing structured, accessible education and decision support during a period of high informational and emotional burden.
The strong acceptability and perceived usefulness of REFLECT highlight unmet needs in timely, integrated fertility and GC among AYAs with cancer. Despite guidelines recommending early discussion of fertility risks, FP options, and appropriate referral to genetics services, many AYAs report these conversations as delayed, inconsistent, or absent.12–15,69 Prior research indicates that insufficient knowledge about fertility risks, preservation options, and hereditary cancer contributes to decisional conflict, distress, and missed opportunities for intervention.4,5,32,38,70
Digital health applications are increasingly recognized as tools to support patient education and decision-making in oncology, particularly when time, emotional burden, and access to specialists are constrained.48–52,71 While previous tools in cancer genetics and fertility care have improved understanding and supported shared decision-making, they have largely addressed these domains separately.54–57,72–75 In contrast, REFLECT integrates FP, genetic risk, and future family-building considerations within a single, interactive platform. Participants emphasized the value of this combined approach, noting that it aligned with how they conceptualize reproductive decisions after cancer and addressed gaps they encountered during care. These findings extend prior work suggesting that integrating genetic and fertility content within a single platform is a critical design feature for improving patient knowledge and ensuring that AYAs feel informed about reproductive and hereditary risk options.27,31,57
Beyond education, participants responded positively to REFLECT’s values-based decision support component, which helped clarify priorities, assess readiness for genetic and fertility-related services, and prepare questions for providers. This aligns with evidence that decision aids can reduce decisional conflict and promote informed, patient-centered care by incorporating individual values into clinical decision-making.43–47,58,71 In AYA oncology, where decisions about FP, GT, and family building often occur under time pressure and emotional distress, such tools may be particularly valuable for supporting communication and decision-making.38,42,68 This pilot additionally offers preliminary insight into the implementation potential of REFLECT, as iterative user-informed refinement of navigation, accessibility, and content organization highlights the importance of designing digital interventions adaptable to diverse learning preferences and real-world use contexts.51–53
Some limitations warrant consideration. While the sample size was consistent with qualitative user-testing approaches and sufficient to achieve thematic saturation, the sample was small and drawn from a single NCI-designated comprehensive cancer center, which may limit generalizability. Participants were predominantly White, highly educated, and had reliable access to internet-enabled devices, potentially underrepresenting individuals of underserved populations with lower digital literacy or limited technology access and limiting evaluation of the tool across varying levels of education and health literacy. The sample also included relatively older AYAs, and findings may not fully reflect the information needs, developmental considerations, or baseline genetics knowledge of younger AYA patients. Further, this pilot was conducted with AYA cancer survivors rather than patients at diagnosis, which may limit the interpretation of decision-making under conditions of heightened urgency and emotional distress, and the tool was not evaluated in contexts where fertility decision-making often occurs in the care trajectory (e.g., remission for cancers that require immediate treatment). In addition, the study focused on individual patient perspectives and did not assess the role of parents or other support persons within the context of shared decision-making. Finally, clinical and behavioral outcomes such as uptake of GC, FP referrals, or changes in decisional conflict or distress were not assessed.
Future research should extend these findings by evaluating REFLECT’s effectiveness, implementation, and impact in larger and more diverse samples, including use at the time of diagnosis. REFLECT may also be relevant for AYAs who have completed family building but seek information about hereditary cancer risk or implications for existing children. Future studies should evaluate timing and clinical integration of REFLECT across different points in the cancer trajectory. Implementation in community and non-NCI settings remains to be evaluated, where access to FP and genetic services may be more limited. Future work should assess integration into diverse oncology care settings to support scalability. Larger trials are needed to assess feasibility, acceptability, usability, and fidelity at scale, as well as effects on outcomes such as knowledge, self-efficacy, distress, and informed decision-making. In addition, examining how REFLECT can be integrated into routine clinical workflows, through mechanisms such as electronic medical record prompts, referral pathways, or multidisciplinary care models, will be important for understanding its scalability and sustainability across oncology settings. Finally, the current version of REFLECT is available in English only. However, the platform supports future multilingual adaptation. The long-term goal is to make the application broadly accessible to patients.
Conclusion
This pilot provides early evidence that REFLECT is a feasible and acceptable digital health application for delivering integrated fertility and genetic education to AYA patients with cancer. By addressing gaps in knowledge and values-based decisional support, REFLECT may enable informed, patient-centered reproductive decision-making and guideline-concordant care.
Author's Contributions
S.P.D.: Contributed to study conceptualization and design, conducted data collection, data analysis/interpretation, and led manuscript writing. L.F. and P.W.L.: Contributed to study conceptualization and design, data collection, data analysis/interpretation, and critical revision of the manuscript. M.S., E.S., and T.S.: Representing NEST Genomics, collaborated to develop and refine the REFLECT platform and contributed to manuscript revision. J.M.: Contributed to clinical interpretation and critical revision. G.P.Q. and S.T.V.: Co-led this pilot and contributed to study conceptualization and design, interpretation of findings, and critical revision of the manuscript. All authors reviewed and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.
Footnotes
Funding Information
No funding was received for the study.