
Abstract
Background:
Adolescent and young adult (AYA) patients with cancer frequently experience psychosocial distress, yet age- and gender-related differences in distress in routine care are not fully understood.
Purpose:
To examine age- and gender-related differences in distress and specific psychosocial concerns among AYA patients with cancer using routine distress screening.
Methods:
This retrospective single-center study included AYA patients aged 15–39 years who completed distress screening with the Distress Thermometer (DT) and problem checklist prior to first-line cancer treatment. Clinically significant distress was defined as DT ≥ 4 based on NCCN guidelines and institutional practice. Distress levels and checklist items were compared across age groups (teens, 20s, 30s), gender, cancer stage, and time from diagnosis to screening.
Results:
Among 213 patients, clinically significant distress (DT ≥ 4) was more frequent among teenage males than among males in their 30s. Female patients reported more emotional concerns across all ages, while fertility-related concerns were reported by both males and females. Financial concerns, reflecting financial toxicity, were most common among patients in their 30s and those with advanced-stage disease. A shorter interval between diagnosis and screening was associated with higher distress levels.
Conclusions:
Using the standard DT cutoff of ≥4, distress among AYA patients with cancer varied significantly by age and gender. Teenage males represented a particularly vulnerable group with elevated distress at diagnosis, while financial toxicity was a major concern among patients in their 30s. These findings emphasize the need for early, age- and gender-tailored psychosocial screening and support in AYA oncology care.
Keywords
Background
Each year, approximately 1.19 million adolescents and young adults (AYAs) are diagnosed with cancer worldwide. 1 In Japan, about one million individuals are diagnosed with cancer annually, including approximately 20,000 AYAs aged 15–39 years, many of whom have rare cancers. 2 The 5-year survival rate for AYA patients with cancer has improved from 73.7% in the 1990s to 86.4% between 2010 and 2016. 3 However, outcomes remain poor for certain cancer types, such as soft tissue sarcomas, renal, colorectal, and melanoma, and the incidence of cancer in the AYA population continues to rise. 3 AYAs face a variety of developmental milestones—such as higher education, employment, marriage, and childbearing—while simultaneously coping with a cancer diagnosis. As a result, they experience unique and complex psychosocial challenges. It is estimated that up to 90% of AYAs with cancer experience some form of psychological distress, 4 which can significantly impair their quality of life. 5,6 Despite these challenges, the diverse physical, emotional, and social difficulties faced by AYAs—including academic, occupational, marital, sexual, and family-related issues—remain underrecognized in clinical practice.
To address these multidimensional issues, support from a multidisciplinary team is essential. In Japan, the Third Basic Plan to Promote Cancer Control Programs, released in 2017, specifically emphasized the need to support the AYA generation. At our hospital, National Cancer Center Hospital, an AYA Support Team has been active since 2015. 7 To identify psychosocial issues efficiently and facilitate timely multidisciplinary intervention, our institution developed a screening tool (ST) specifically designed for AYAs. 8 This tool is used to screen all patients with cancer aged 15–39 years, including inpatients from all departments and outpatients from hematology, oncology, and chemotherapy services. Screening is primarily administered by nurses, and if necessary, referrals are made to relevant professionals. Patients typically complete the screening via tablet, with nurses available to provide clarification as needed. Responses are recorded directly in the electronic medical record system. 9 Internationally, several AYA-specific screening tools have been validated, such as the Adolescent and Young Adult Psycho-Oncology Screening Tool (AYA-POST). 10 These tools have revealed age-related differences in distress; however, most studies have focused on adolescents and individuals in their 20s. Previous studies have also reported gender differences in distress among AYA patients with cancer. 11 However, limited research has explored the experiences of those in their 30s, and no studies to date have comprehensively examined the combined influence of both age and gender.
This study aimed to address that gap by exploring how distress and psychosocial concerns vary by gender and age among AYA patients with cancer.
Purpose
The objective of this study was to examine the relationship between age and gender and the Distress Thermometer (DT) score, the number and content of selected checklist items, the time from diagnosis to screening, and the time from diagnosis to treatment initiation.
Materials and Methods
Study design and participants
This was a retrospective, single-center study conducted at the National Cancer Center Hospital in Japan. The study included all AYA patients with cancer aged 15–39 years who visited our hospital between April 2021 and December 2022 and completed the AYA-specific ST prior to initiating their first cancer treatment.
Data collection
The following data were extracted from electronic medical records: age, gender, primary tumor site, clinical stage, date of diagnosis, date of screening response, date of treatment initiation, treatment details, time taken to complete the screening, and responses to the screening. Among these, we analyzed only the cases in which the ST was completed before the initiation of treatment.
Measurements
The primary outcome was the relationship between age and gender and DT score, as well as the content of the selected checklist items. Secondary outcomes included the associations between age or gender and: (1) the number of checklist items selected, (2) the interval from diagnosis to screening, and (3) the interval from diagnosis to treatment initiation. In addition, we evaluated the following: the proportion of patients with a DT score ≥4, the proportion of patients selecting each checklist item, the time from diagnosis to screening, and the time from diagnosis to treatment initiation. Higher DT scores indicate greater levels of distress. Although a DT cutoff score of 5 has been suggested in some studies involving recently diagnosed AYA patients, 11,12 we adopted a cutoff of ≥ 4 based on the National Comprehensive Cancer Network (NCCN) Guidelines for Distress Management, 13 a previous study 14 and institutional clinical practice. This threshold has been widely used in oncology settings to enable broader screening and identification of patients experiencing distress. However, the DT is a ST rather than a diagnostic instrument, and this cutoff should be interpreted as an indicator for further psychosocial assessment rather than a definitive diagnosis. In addition to the DT, we analyzed the problem checklist to further characterize patients’ psychosocial concerns. Specifically, the frequency of individual checklist items was used to identify the types of concerns, and the number of items endorsed was treated as a descriptive measure reflecting the breadth of concerns rather than the severity of distress. The ST used in this study consists of a validated 10-point DT scale and a 49-item problem checklist adapted from the NCCN Distress Thermometer and Problem List (DTPL). The Japanese version was developed through translation and cultural adaptation, with the addition of items specific to the AYA population in Japan. Its reliability and validity have been confirmed in Japanese patients with cancer. 9 To create the Japanese version, the DTPL was translated and linguistically adjusted to align with the cultural context, with additional items added as needed. 8 The DT, originally developed by the NCCN, is a widely used tool for assessing cancer-related distress. It uses a scale from 0 (no distress) to 10 (extreme distress) and has been validated for use in Japanese patients with cancer. 15
Statistical Analysis
The associations between gender and DT scores, as well as the content of selected checklist items across age groups (15–19: teens, 20–29: 20s, 30–39: 30s), were assessed using chi-square (χ2) tests. Checklist item responses were analyzed separately by gender using χ2 tests.
Differences across the three age groups were analyzed using analysis of variance. Subgroup analyses were conducted using independent t-tests to assess differences in DT scores and the number of checklist items selected by age and gender.
Spearman’s rank correlation was used to examine the relationships between the time from diagnosis to screening and both the DT score and the number of checklist items selected. A two-tailed p value of <0.05 was considered statistically significant.
Results
Patient characteristics
A total of 959 patients aged 15–39 years visited our hospital for the first time between April 2021 and December 2022. Of these, 498 patients initiated their first cancer treatment at our institution. Among them, 302 completed the ST. After excluding cases with missing data and those who completed the screening after starting treatment, the final sample comprised 213 patients (Fig. 1). The baseline characteristics of all patients are shown in Table 1. Among 213 eligible patients, 73 (34.2%) were males and 140 (65.7%) were females. The median age was 32 years. By age group, 25 patients (11.3%) were in their teens (15–19 years), 55 (25.8%) were in their 20s, and 133 (62.4%) were in their 30s, respectively. The most common primary cancer sites were breast (n = 44, 19.9%), bone and soft tissue (n = 36, 16.3%), genital (n = 33, 14.9%), gastrointestinal (n = 33, 14.9%), hematological (n = 17, 7.9%), lung (n = 13, 6.1%), and brain (n = 11, 5.2%). Advanced-stage disease was present in 23 patients (10.1%) with stage 3 and 32 patients (15.0%) with stage 4 disease.

Consolidated Standards of Reporting Trials (CONSORT) diagram of participant flow in the study. This diagram shows the number of eligible patients, exclusions, and final participants included in the analysis.
Patient Characteristics
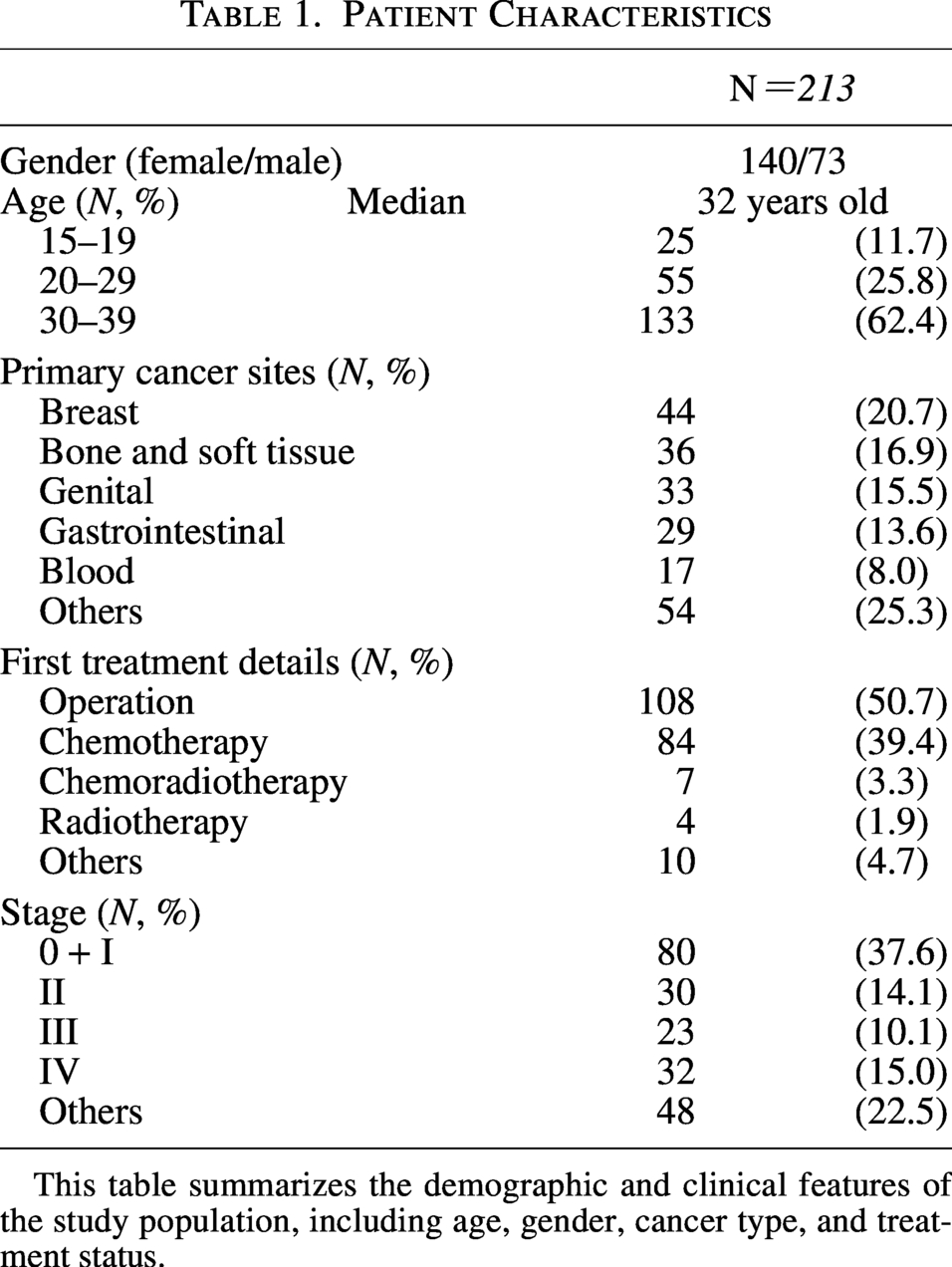
This table summarizes the demographic and clinical features of the study population, including age, gender, cancer type, and treatment status.
Relationship between gender/age and DT score
The mean DT scores were 4.1 (±3.0) for males and 4.2 (±2.9) for females (p = 0.73). By age group, the average DT scores were 4.5 for teens, 4.7 for those in their 20s, and 3.8 for those in their 30s (±2.5, ±3.3, ±2.8, respectively; p = 0.139). The proportions of patients with DT scores ≥4 were 68% for teens, 65% for those in their 20s, and 47% for those in their 30s (Table 2). Among males, a significantly higher proportion of teenagers had DT scores ≥4 compared to those in their 30s (82% vs. 43%, p = 0.025). Among females, there were no significant differences in DT scores across age groups (teens: 57%, 20s: 65%, 30s: 54%; p = 0.25) (Fig. 2).
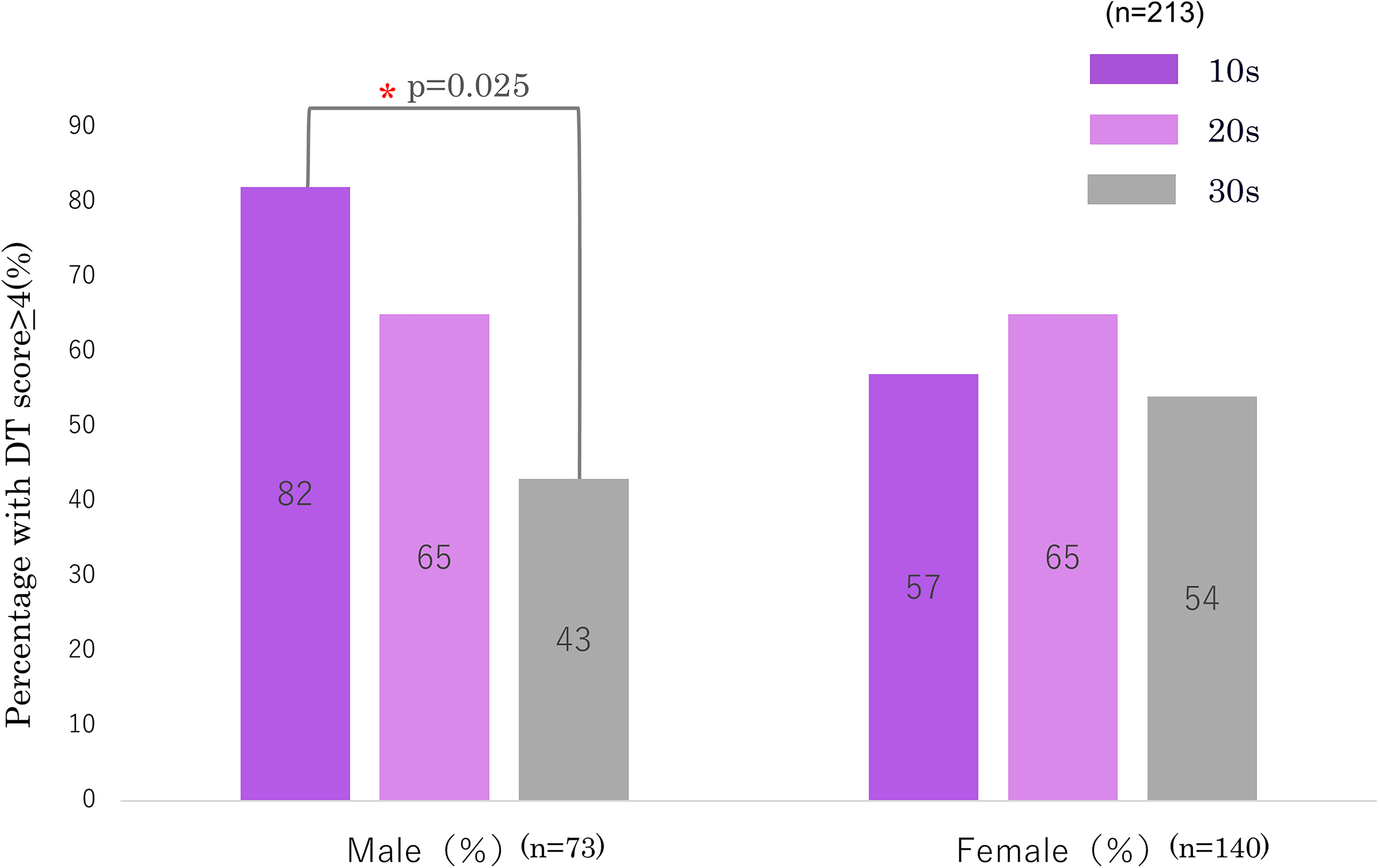
Proportion of patients with clinically significant distress (DT ≥ 4) by age group and gender. The figure displays the percentage of patients with DT ≥ 4 across three age groups (10s: 15–19, 20s: 20–29, 30s: 30–39), separately for males and females. Group comparisons were conducted using the χ2 test. A two-tailed p value < 0.05 was considered statistically significant. DT, Distress Thermometer.
Relationship Between Gender/Age and DT Score
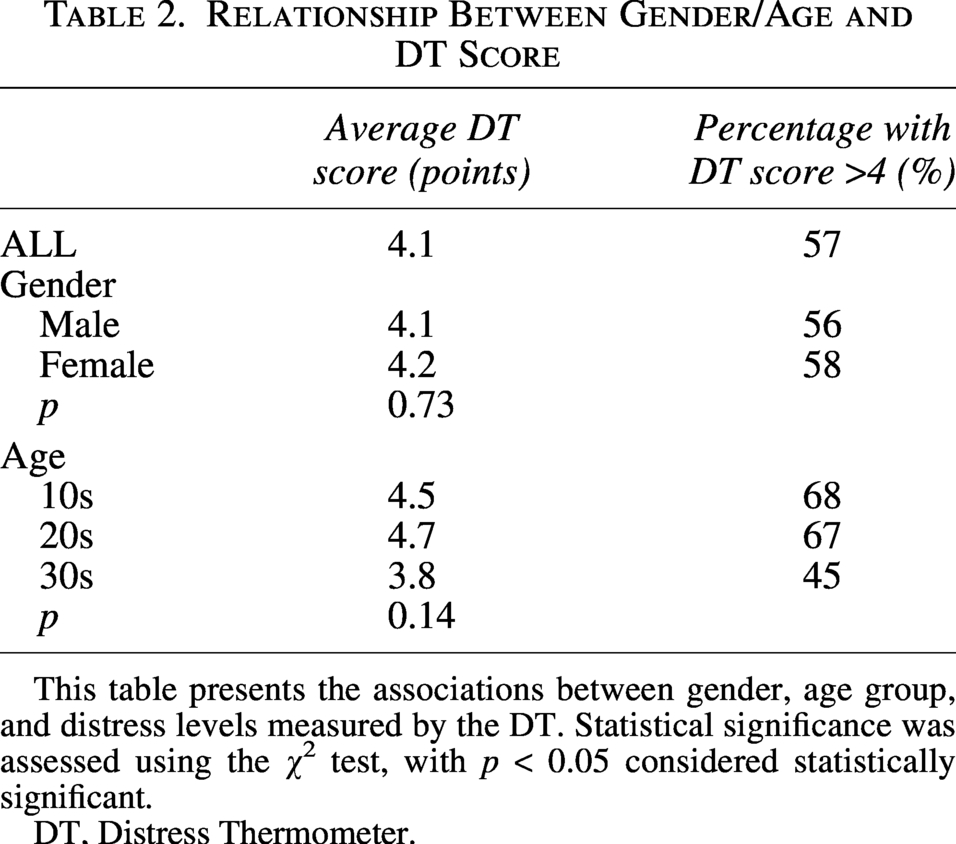
This table presents the associations between gender, age group, and distress levels measured by the DT. Statistical significance was assessed using the χ2 test, with p < 0.05 considered statistically significant.
DT, Distress Thermometer.
Relationship between gender/age and checklist items
The mean number of checklist items selected did not differ significantly by gender (males: 10.7, females: 11.5; p = 0.49) or age group (teens: 11.9, 20s: 11.7, 30s: 10.9; p = 0.14).
The distribution of selected checklist items among all patients is summarized in Figure 3A. The complete results for all checklist items are provided in Supplementary Figure S1. The most frequently reported concerns were “anxiety,” “worry,” and “money.” Anxiety was reported by 60% and worry by 59% of patients across all age groups. All patients with stage IV disease in their 20s (n = 8) and 30s (n = 22) reported financial concerns. Patients in their 30s were significantly more likely to report financial concerns than younger patients (teens: 32%, 20s: 24%, 30s: 74%; p < 0.001).
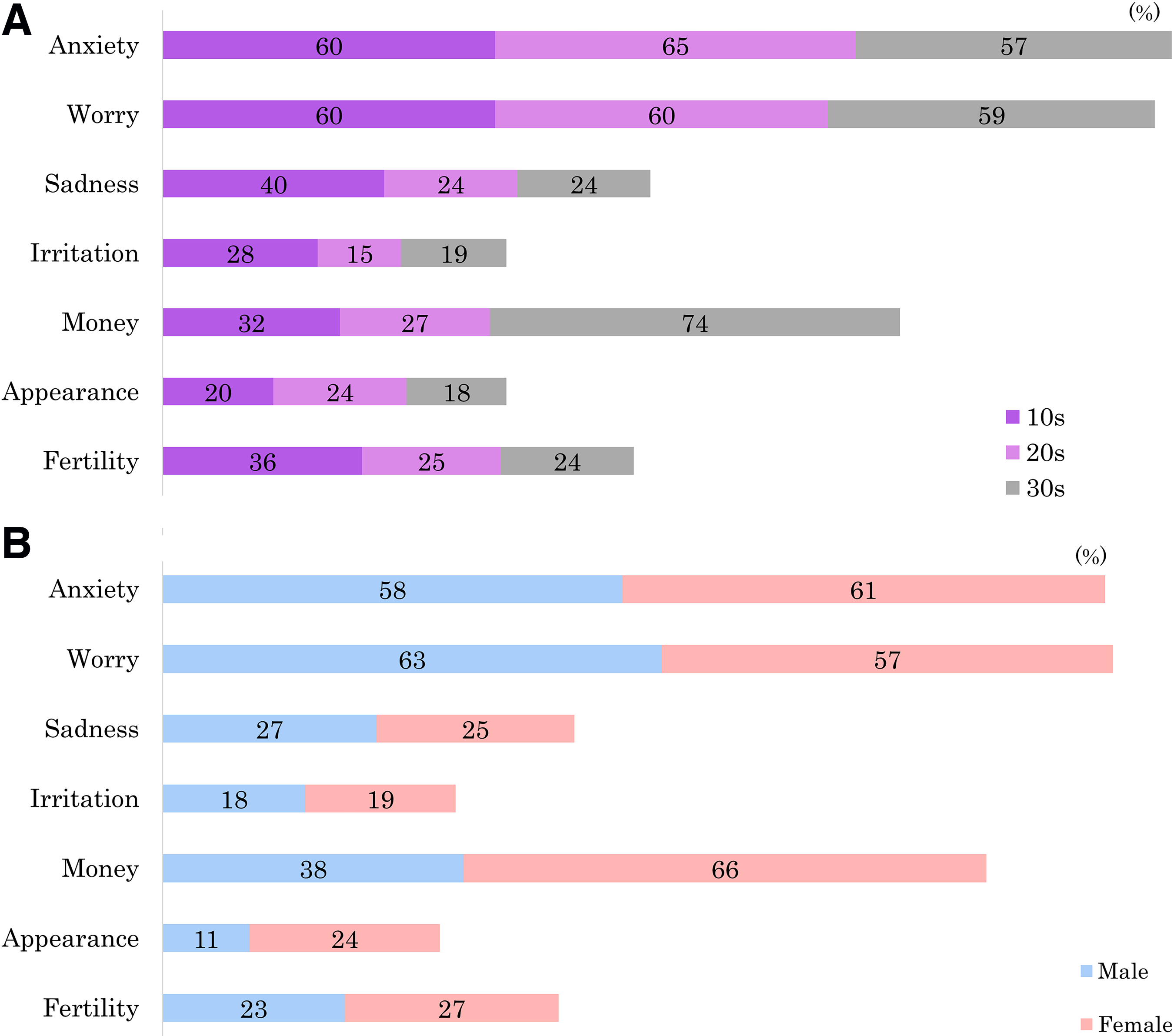
Gender differences in selected checklist items are shown in Figure 3B. Females were more likely than males to report concerns about appearance (11% vs. 24%, p = 0.02) and money (38% vs. 66%, p < 0.001). Fertility-related concerns were reported by 23% of males and 27% of females, with no significant gender difference (p = 0.54), suggesting that reproductive issues affect both sexes equally and should be addressed regardless of gender. Teenage females were more likely to report “sadness” (teens: 57%, 20s: 15%, 30s: 24%; p = 0.009) and “irritation” (teens: 42%, 20s: 12%, 30s: 18%; p = 0.04).
Relationship between time from diagnosis to treatment/screening and DT score or checklist items
The interval from diagnosis to the start of treatment was significantly shorter for males than for females (25.8 ± 29.0 days vs. 50.5 ± 45.5 days, p < 0.01). Similarly, the interval from diagnosis to screening was also shorter in males (11.6 ± 22.5 days) than in females (24.3 ± 36.2 days; p < 0.01). Correlation analysis revealed a negative association between the time from diagnosis to screening and DT score for both males (correlation coefficient = −0.30; p < 0.01; 95% confidence interval [CI]: −0.41 to −0.17) and females (correlation coefficient = −0.20; p < 0.01; 95% CI: −0.33 to −0.07). These findings indicate that a shorter interval from diagnosis to screening was associated with higher distress levels. In males, there was also a significant negative correlation between the time from diagnosis to screening and the number of checklist items selected (correlation coefficient = −0.27; p < 0.01; 95% CI: −0.39 to −0.15), suggesting that earlier screening was associated with a greater number of reported concerns.
Discussion
This study revealed age- and gender-specific patterns of distress among AYA patients with cancer, with teenage males showing higher distress, and patients in their 30s with advanced-stage disease reporting greater financial concerns. Screening conducted before treatment initiation facilitated an accurate assessment of patients’ needs, underscoring the importance of timely psychosocial support.
The majority of participants were female (65.7%), with a median age of 32. While overall DT scores did not significantly differ between genders, a higher proportion of teenage males had DT scores ≥ 4 compared to males in their 30s (82% vs. 43%, p = 0.025). The most commonly reported concerns were anxiety (60%), worry (59%), and financial issues (57%), with financial concerns being most prevalent among patients in their 30s (74%). All patients with stage IV disease reported financial distress.
Notably, approximately one-quarter of both male and female patients expressed concerns about fertility, with no significant gender differences. Earlier studies suggested greater fertility-related distress in females 15 ,16,17; however, recent research shows similar levels of concern among male AYA patients. 18,19 This finding supports the recommendation that fertility preservation should be routinely discussed with all AYA patients during pretreatment counseling.
Our results are consistent with previous studies highlighting psychological distress in the AYA cancer population. For instance, Justafré et al. (n = 103, aged 15–25) identified “psychological health” as the most unmet need among patients aged 15–25, citing anxiety, fear of relapse, and difficulty understanding treatment information. 20 Similarly, McCarthy et al. (n = 288, aged 15–29) reported high levels of concern for “missing normal activities with friends” (49.3%), “boredom” (46.1%), “appearance” (38.4%), “education” (34.7%), “anxiety or fear” (33.3%), “sleeping difficulties” (33.3%), and “mum and/or dad” (32.4%). In our study, comparable levels of concern were observed for “anxiety” (60%), “worry” (59%), “appearance,” “sleep,” and “daily life,” supporting the consistency of emotional distress across cohorts. However, several key differences emerged. In our cohort, 52% of patients endorsed concerns related to “work or school,” surpassing the 34.7% who selected “education” in McCarthy et al.’s study. 21 This likely reflects the broader age distribution in our sample, including a larger proportion of individuals in their 30s with work-related responsibilities.
Moreover, financial concerns were markedly more prevalent in our cohort—reported by 57% of all participants and 74% of those in their 30s—whereas neither Justafré et al. 19 nor McCarthy et al. 21 emphasized financial issues, likely due to the younger age range of their study populations. Last, “interaction with other family members” was selected by only 10% of our participants, significantly lower than the 32.4% reported in McCarthy et al., 21 suggesting possible age-related or cultural differences in perceived family-related distress.
Previous studies have not fully captured the financial concerns of AYA patients with cancer, likely because their study populations tended to be younger than those in the present study. In contrast, our findings highlight substantial financial needs among patients in their 20s and 30s, particularly those with stage 4 disease. Kelly et al. reported that patients raising children experience greater financial difficulties. 21,22 The elevated financial concerns observed in our cohort may be attributed to the high proportion of participants in their 20s and 30s who are likely in the child-rearing stage of life. These individuals face not only treatment-related expenses but also additional costs associated with daily living and childcare. Moreover, previous research has shown that patients with advanced-stage cancer often incur significantly higher expenses due to repeated treatments and hospitalizations. 23 –25 These findings reinforce our results, showing that financial concerns were especially common among patients with stage 4 cancer.
A negative correlation was observed between the DT score and the time from diagnosis to screening for both males and females, indicating that patients experienced higher levels of distress closer to the time of diagnosis. This pattern likely reflects the acute psychological impact of receiving a cancer diagnosis—a phenomenon well-documented in psycho-oncology as a period of heightened vulnerability. 26 As Holland has emphasized, the diagnostic phase often triggers intense emotional responses, which may subside over time as patients begin to process their diagnosis and engage with care. 26 These findings underscore the importance of the immediate postdiagnosis period as a critical window for psychosocial assessment and early intervention, especially among AYA patients.
Strengths of this study include the consistent timing of screening—conducted after diagnosis but before the initiation of treatment—which minimized the influence of treatment-related factors and allowed for a more accurate assessment of baseline psychosocial needs. The study employed a validated ST routinely used in daily clinical practice, enhancing both the external validity and the real-world applicability of the findings. In addition, the relatively large sample size (n = 213) enabled meaningful subgroup analyses by age and gender, providing nuanced insights into the distress profiles of AYA patients with cancer. Although conducted at a single institution, the study was carried out at a national comprehensive cancer center with an established AYA care system and multidisciplinary coordination. This ensured a high degree of standardization in the implementation of screening and data collection, thereby improving the consistency and reliability of the results.
This study has several limitations. First, it was a single-center, retrospective study conducted at a hospital that treats approximately 2000 AYA patients with cancer annually. Compared to other institutions in Japan, our hospital has a notably high volume of AYA patients and is characterized by a dedicated AYA Support Team and a more comprehensive AYA care system. As a result, there is a potential for selection bias, and the findings may not be generalizable to other settings or regions. Financial concerns may vary across countries depending on differences in health care systems, insurance coverage, and social welfare structures. Therefore, the financial distress observed in this study may not fully reflect the experiences of AYA patients in other health care contexts. Second, distress was assessed at a single time point prior to treatment initiation. Consequently, changes in psychosocial needs over the course of treatment were not captured. The relationship between overall distress and specific psychosocial concerns was also not fully explored. Data on patients who completed screening after treatment initiation were not available; therefore, differences between pre- and post-treatment assessments could not be evaluated. Third, the inclusion of a heterogeneous patient population with varying cancer types, stages, and treatment plans may have introduced confounding factors that limit the interpretation of the results. Finally, this study did not assess the effects of subsequent psychosocial interventions, making it difficult to determine how identified needs influenced treatment outcomes or quality of life. In addition, because multiple statistical comparisons were conducted in this exploratory study without formal adjustment for multiple testing, the possibility of type I error cannot be excluded. Therefore, the findings should be interpreted with caution. Future studies using multivariable analyses, such as logistic regression models that allow examination of interactions between age and gender while adjusting for potential confounders, may further clarify the complex relationships observed in this study. This study demonstrated that distress levels among AYA patients with cancer vary by both age and gender, highlighting the need for psychosocial support strategies tailored to demographic subgroups.
To further improve care, future research should explore how distress evolves across the cancer treatment trajectory and identify the optimal timing and content of interventions that address the specific needs of each patient subgroup.
Conclusions
This study identified distinct age- and gender-specific patterns of distress among AYA patients with cancer, with the highest levels observed shortly after diagnosis.
Psychological support is particularly needed for adolescents and patients in their 20s, among whom distress levels were highest, with adolescent males representing the most vulnerable subgroup. In addition, financial concerns were particularly prominent among patients in their 20s and 30s and those with advanced-stage disease.
Authors’ Contributions
T.I., H.I., and N.M. participated in the design of the study. T.I., H.I., N.M., and M.O., Takuma K., Takashi K., and Y.H. designed and performed the statistical analysis plan. All authors contributed to writing and revising the article critically, and all gave their final approval of the version to be published.
Ethics Approval
This study was approved by the National Cancer Center Hospital Certified Review Board (Approval No. 2019-215).
Informed Consent
The requirement for informed consent was waived by the Institutional Review Board due to the retrospective nature of the study.
Footnotes
Acknowledgment
The authors are grateful for the support from Japan Agency for Medical Research and Development (AMED). The authors thank in advance all the patients, investigators, patients and caregivers, representatives, and institutions involved in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Statement
This research was supported by AMED under grant number
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.