
Abstract
Purpose:
To examine longitudinal changes in trunk muscle mass during chemotherapy in children and adolescents with lower-limb osteosarcoma and to compare these changes according to surgical procedure.
Methods:
Medical records of 11 patients admitted to a university hospital in Japan between 2010 and 2023 were analyzed. Trunk muscle mass was assessed using computed tomography scans of the L3 vertebral body using the VINCENT® abdominal analysis system. Changes in trunk muscle mass from admission to discharge were categorized as increase (≥5%), maintenance (±5%), or decrease (≤−5%). Rehabilitation-related variables and surgical procedures were examined in relation to muscle mass changes.
Results:
The mean age was 13.7 years (eight males and three females). Seven patients underwent limb-sparing surgery, and four underwent amputation. No significant associations were observed between rehabilitation-related variables (hospitalization duration, rehabilitation frequency, or session duration) and trunk muscle mass changes. However, a significant association was identified between surgical procedure and trunk muscle mass changes. All patients who underwent amputation maintained or increased muscle mass, whereas five of the seven patients who underwent limb-sparing surgery experienced a decrease.
Conclusion:
In this retrospective observational study, trunk muscle mass changes during chemotherapy were associated with the type of surgical procedure but not with rehabilitation-related variables. Further studies with larger sample sizes are warranted to better understand factors associated with muscle mass changes in this population.
Introduction
Osteosarcoma is the most common type of malignant bone tumor in children and adolescents. Recent advances in diagnostic imaging technologies, neoadjuvant chemotherapy, and extensive resection techniques have greatly improved the long-term prognosis of patients with osteosarcoma. 1 Therefore, the goals of rehabilitation in young patients with osteosarcoma include improving motor function and quality of life, including the ability to return to school or work. However, rehabilitation for young patients with osteosarcoma undergoing pre- and postoperative chemotherapy is often challenging in terms of improving muscle strength and increasing muscle mass. 2
One contributing factor is the adverse effects of chemotherapy. Standard pre- and postoperative chemotherapy typically involves a multiagent regimen comprising methotrexate, cisplatin, and doxorubicin (Adriamycin). During and after chemotherapy, patients often experience a decline in physical function, which adversely affects their activities of daily living.3,4 Following the administration of chemotherapeutic agents, side effects such as anorexia, fatigue, and myelosuppression frequently occur. Anorexia and fatigue can lead to reduced physical activity and malnutrition, thereby increasing the risk of developing disuse syndrome. 3 Furthermore, the occurrence of myelosuppression necessitates restrictions on the training environment and exercise intensity. Additionally, recent reports have highlighted the increasing occurrence of muscle function decline and atrophy induced by cancer cells and chemotherapeutic agents.5–10 Cytotoxic drugs such as doxorubicin are known to damage both cancerous and normal cells, thereby affecting muscle function.8,9 Additionally, synthetic glucocorticoids, which are often co-administered during chemotherapy, significantly impact muscle catabolic processes, leading to muscle atrophy and weakness.7,8 The reduction in muscle mass and strength caused by these factors can result in a temporary or prolonged decline in physical function. 9
For these reasons, rehabilitation during preoperative and postoperative chemotherapy for young patients with osteosarcoma must aim to improve muscle strength and increase muscle mass while adjusting the training load to accommodate expected fluctuations in physical condition due to the chemotherapy regimen.
Wide resection prioritizes limb-sparing surgery; if this is not feasible, amputation is selected. Following wide resection, reconstruction with prosthetic joint replacement or the use of autografts is performed as part of limb-sparing surgery. If amputation is selected, the patient will require a prosthesis and must achieve a prosthetic gait. 11
In postoperative rehabilitation, it is essential to consider not only the effects of chemotherapy but also the resected and remaining muscles following wide resection and the reconstruction method used. Additionally, muscle strength and mass must be improved while carefully considering the rest required for the affected limb.
As outlined previously, children and adolescents with osteosarcoma undergo intensive treatment that may influence muscle mass during chemotherapy and surgery. However, longitudinal changes in trunk muscle mass during treatment, particularly according to surgical procedure, remain unclear. Therefore, the aim of this study was to examine longitudinal changes in trunk muscle mass during chemotherapy in children and adolescents with lower-limb osteosarcoma and to compare these changes according to surgical procedure.
Materials and Methods
Study design
This was a retrospective, observational, single-center case-control study. Data were obtained from medical records, and no experimental procedures were conducted as part of this study. All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board (IRB) of Sapporo Medical University Hospital (IRB No 352-49). Informed consent was obtained using an opt-out method. The authors declare that no funds, grants, or other support were received during the preparation of this article.
Patients and eligibility
Patients eligible for inclusion in this study were those admitted to a university hospital in Japan between April 1, 2010, and March 31, 2023. The study focused exclusively on individuals younger than 30 years at the time of admission and who had a confirmed diagnosis of primary osteosarcoma of the lower extremities. To ensure a consistent treatment framework, only patients who underwent the standard treatment protocol for osteosarcoma were included. This protocol consisted of preoperative chemotherapy, wide-resection surgery, and postoperative chemotherapy. At our institution, treatment was generally conducted during extended hospitalizations that encompassed preoperative chemotherapy, surgery, and postoperative chemotherapy. However, depending on the individual treatment schedule and the patient’s clinical condition, some patients were temporarily discharged or allowed short home stays between chemotherapy cycles. Therefore, the reported hospitalization period reflects the cumulative duration of inpatient care during the overall treatment course. Additionally, all patients included in the study participated in a rehabilitation program during the course of their treatment.
Patients were excluded if the required computed tomography (CT) images at the L3 vertebral level were not available for muscle mass evaluation. During the study period, 12 patients met the inclusion criteria. One patient was excluded due to the absence of CT imaging at discharge, resulting in a final sample of 11 patients.
Participant characteristics
Data for this study were extracted from the electronic medical records of the hospital. To minimize recall bias, objective medical records were used instead of self-reported data where possible.
The collected information included patient demographics, such as age and sex, along with clinical history detailing the date of diagnosis, tumor location, and histopathological findings. Treatment information was also collected, including details of the chemotherapy regimens administered, surgical procedures performed, and rehabilitation interventions undertaken. All data were anonymized prior to the analysis to ensure patient confidentiality.
Patient-reported outcome measures
Patient-reported outcomes included factors such as age at onset, sex, primary tumor site, and length of hospital stay. Surgical approaches for wide resection were classified as either limb-sparing surgery or amputation. Additionally, the rehabilitation process was evaluated, including the total number of rehabilitation days, the frequency of rehabilitation sessions, and the duration of training in each session. In the preoperative rehabilitation protocol, physical therapy was conducted with a focus on improving overall body strength, including areas outside the affected limb, while considering the patient’s condition owing to the side effects of chemotherapy. For postoperative rehabilitation, the protocol differed between the groups. In the limb-sparing surgery group, range of motion (ROM) exercises for the affected area were initiated as early as possible, and weight-bearing was gradually increased to full weight-bearing as directed by the surgeon. In the amputation group, training to improve strength and ROM of the residual limb was initiated postoperatively. Once the wound at the amputation site had healed, a prosthesis was fabricated, and the patient began a phased program of prosthesis fitting and gait training. In both groups, physical therapy aimed at enhancing overall body strength, including areas outside the affected limb, was continued postoperatively.
Measurement of trunk muscle mass
In this study, trunk muscle mass was assessed using plain CT scans obtained at admission, before and after wide resection, and at discharge. These scans were analyzed using the VINCENT® abdominal analysis system (Fujifilm Medical Co., Ltd.), which automatically quantifies body composition at the upper edge of the L3 vertebral body, focusing on skeletal muscle, as well as subcutaneous and visceral fat mass (Fig. 1).

Computed tomography scans analyzed using the VINCENT® abdominal analysis system.
VINCENT® is a medical image analysis software widely used in both clinical practice and research, particularly in the evaluation of sarcopenia and nutritional status. Compared with manual methods, muscle mass measurement using automated analysis software such as VINCENT has been reported to have higher reproducibility and lower intra- and inter-observer variability.12,13
Data analysis
Trunk muscle mass was measured as cross-sectional area using CT scans, and changes from admission to discharge were analyzed. In evaluating changes in trunk muscle mass during treatment, particular attention was paid to the measurement accuracy of skeletal muscle area (SMA) obtained from abdominal CT images at the level of L3. Automated image analysis software, such as VINCENT, is known to provide high reproducibility in SMA measurements. Previous studies have reported intra-observer variability of approximately 1%–2% and inter-observer variability of 2%–5% in such measurements.12,13
Based on these findings, a change in SMA within ±5% was considered to fall within the range of measurement error and was therefore interpreted as muscle mass maintenance. Patients were classified into three groups according to the changes observed at discharge: those with an increase in trunk muscle mass of ≥ 5%, those with changes within ±5% (maintenance group), and those with a decrease of ≥ 5% (i.e., ≤ −5%).
To examine factors associated with changes in trunk muscle mass, an independent t-test was conducted to compare rehabilitation-related variables, including hospitalization duration, number of rehabilitation days, frequency of rehabilitation sessions, and session duration, between the maintenance or increase group and the decrease group. Additionally, the chi-square test was used to evaluate the association between changes in trunk muscle mass (maintenance, increase, or decrease) and the extent of surgical resection. A p value of < 0.05 was considered statistically significant.
Results
Twelve patients met the inclusion criteria during the study period. One patient was excluded due to the absence of a high-resolution CT scan, resulting in a final cohort of 11 patients.
The mean age of the patients was 13.7 years, including eight males and three females. The average height was 159.5 cm, and the average weight was 50.7 kg. The primary tumor sites were the distal femur in six cases and the proximal tibia in five cases. Seven patients underwent limb-sparing surgery, while four underwent amputation. The mean duration of hospitalization was 318.1 days. On average, rehabilitation sessions were conducted three days a week, with each session lasting an average of 40.0 minutes (Table 1). All patients were initially treated according to the standard institutional protocol for osteosarcoma, which included multiagent chemotherapy consisting of high-dose methotrexate, doxorubicin, and cisplatin (MAP regimen) administered both preoperatively and postoperatively.
Patient Characteristics

Baseline characteristics of the study participants (n = 11).
F, female; Lt, left; M, male; Rt, right; WR, wide resection.
The outcomes for trunk muscle and fat mass (cross-sectional area at the upper edge of the L3 vertebral body, cm2) are presented in Table 2. Missing data were noted in one case preoperatively and in two cases postoperatively.
Trunk Muscle Mass (Cross-Sectional Area at the Upper Edge of the L3 Vertebral Body)
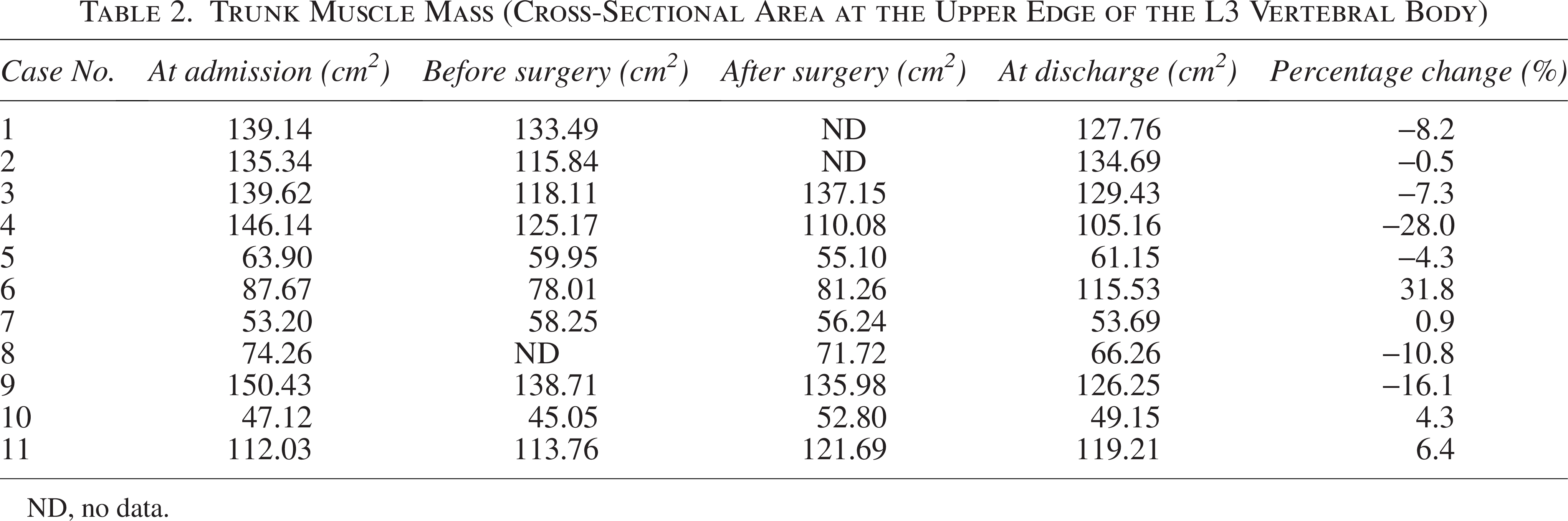
ND, no data.
Two patients had an increase of ≥ 5% in trunk muscle mass at discharge compared with admission. Four patients maintained their muscle mass within a ±5% range from admission to discharge. However, five patients experienced a decrease of ≥ 5% during the same period. These results indicate substantial individual variation in trunk muscle mass changes from admission to discharge.
Associations between trunk muscle mass changes and clinical factors
We investigated the relationship between trunk muscle mass changes, rehabilitation implementation status, and surgical procedures.
Patients were divided into two groups: those with maintained or increased muscle mass (maintenance/increase group, n = 6) and those with decreased muscle mass (decrease group, n = 5). An independent t-test was used to compare the length of hospital stays, number of rehabilitation days, rehabilitation frequency, and rehabilitation session duration between the two groups. However, no statistically significant differences were observed in any of these variables (Table 3).
Relationship Between Trunk Muscle Mass Changes and Rehabilitation-Related Variables
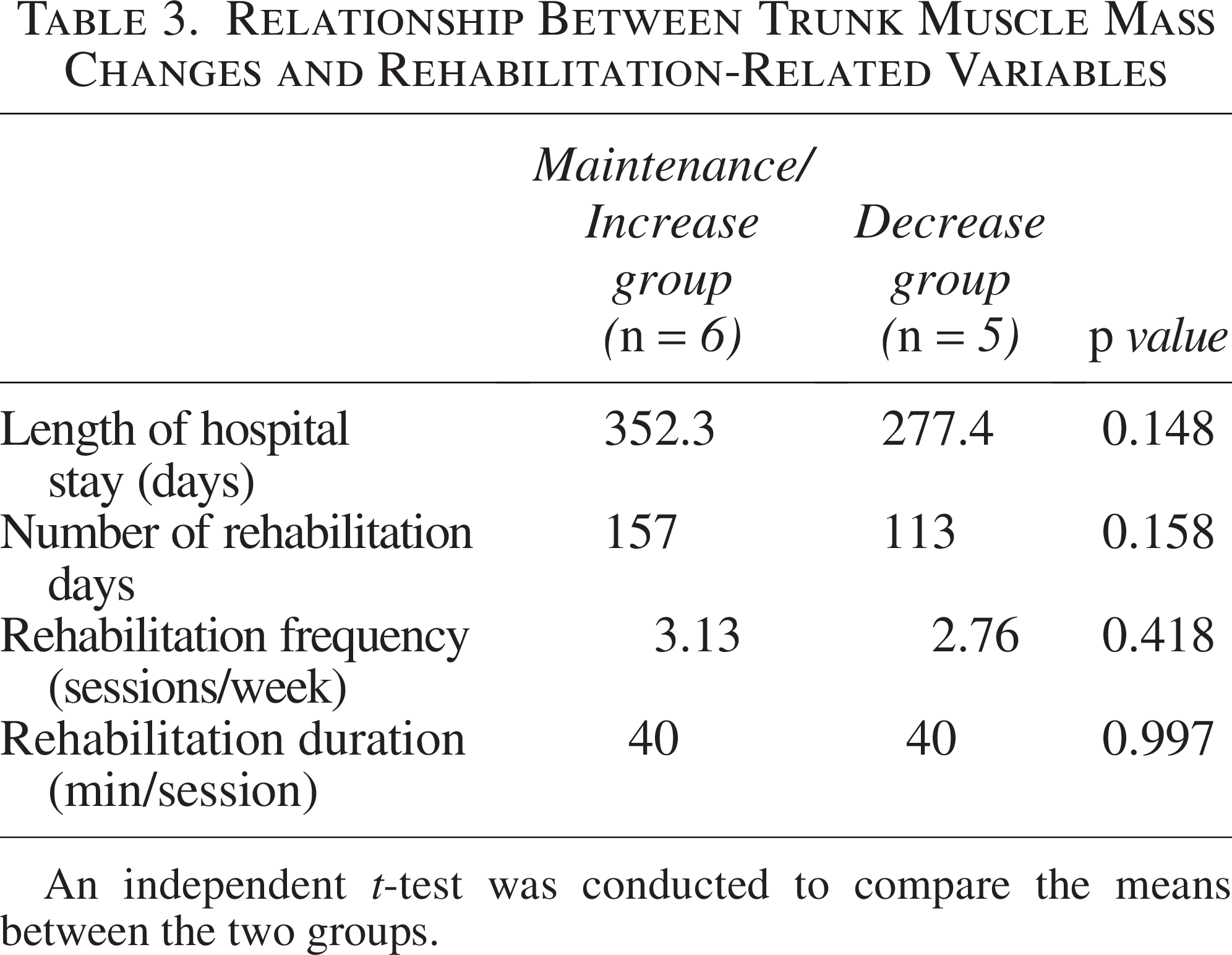
An independent t-test was conducted to compare the means between the two groups.
Next, we examined the relationship between trunk muscle mass and the type of surgical procedure. Among the 11 patients, four underwent amputation, and all of them maintained or increased their muscle mass, whereas five of the seven patients who underwent limb-sparing surgery showed a decrease in muscle mass. A chi-square test revealed a statistically significant association between surgical procedure and changes in trunk muscle mass (p = 0.022; Table 4).
Relationship between Trunk Muscle Mass Changes and Surgical Procedures
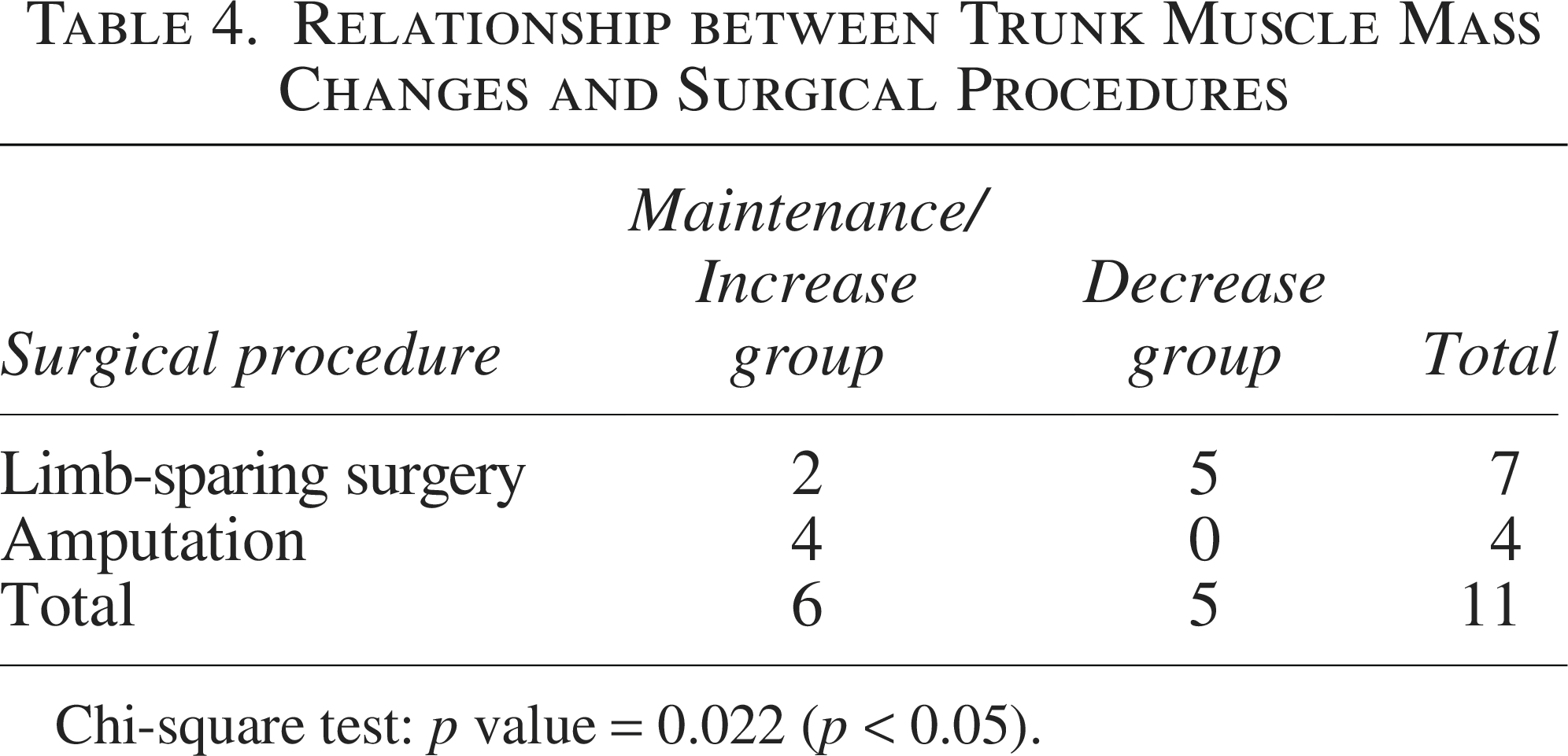
Chi-square test: p value = 0.022 (p < 0.05).
Discussion
Although several studies2,14 have focused on muscle strength of the affected lower limb after extensive resection, no studies have examined trunk muscle mass, as in the present study, or investigated the relationship between rehabilitation practices and surgical procedures. Thus, this study provides a novel perspective.
In pediatric osteosarcoma rehabilitation, it is crucial to understand the chemotherapy regimen and adjust the training load based on anticipated fluctuations in the physical condition to enhance muscle strength and mass. Particularly after extensive resection, it is important to understand the condition of the resected and remaining muscles, as well as the reconstruction method, and to work to improve muscle strength and mass while considering the necessary rest for the affected limb.
To date, it remains unclear whether rehabilitation therapy contributes to improvements in muscle strength and mass in young patients with osteosarcoma under such challenging conditions. Johansen et al. evaluated knee extensor strength in patients who underwent extensive resection and reconstruction with tumor prostheses for osteosarcoma. 2 Their findings revealed that strength on the surgical side was significantly lower than that on the nonsurgical side and in the control group. Specifically, knee extension torque was only 20% of that in the control group, whereas knee flexion torque was approximately 58%, and it took twice as long to generate the force.
In this study, no statistically significant differences were observed in rehabilitation conditions—such as length of hospitalization, number of rehabilitation days, frequency of rehabilitation sessions, or rehabilitation session duration—between the group that maintained or increased trunk muscle mass and the group that experienced muscle loss. These findings indicate that no significant association was observed between rehabilitation-related variables and changes in trunk muscle mass in this cohort.
Next, we examined the relationship between trunk muscle mass and the type of surgical procedure. Among the 11 patients included in this analysis, all four patients who underwent amputation either maintained or increased their trunk muscle mass, whereas five out of the seven patients who underwent limb-sparing surgery showed a decrease in trunk muscle mass. The chi-square test indicated a statistically significant association between surgical procedure and changes in trunk muscle mass. The observed differences may reflect a combination of surgical invasiveness, postoperative immobilization, and rehabilitation characteristics; however, causality cannot be determined in this observational study.
When directly comparing the percentage change in trunk muscle mass between the two groups, the limb-sparing group showed a mean change of –9.0%, whereas the amputation group demonstrated a mean change of +7.8%. Although the sample size was small and the group sizes were unequal, precluding the detection of statistically significant differences, the observed trend should be interpreted with caution. These findings suggest that postoperative recovery constraints may differ between surgical procedures and could be associated with reduced trunk muscle mass; however, the specific mechanisms remain unclear.
Reconstruction following limb-sparing surgery involves the use of tumor prostheses or autografts. Both methods require the affected area to remain immobilized during the perioperative period to facilitate tissue repair. For tumor prostheses, load-bearing and gait training must be conducted carefully to prevent prosthetic damage or loosening. Autografts often require prolonged non-weight-bearing until bone union is achieved. Owing to these factors, maintaining rest in the affected limb during chemotherapy after limb-sparing surgery is crucial, making it difficult to increase muscle mass through rehabilitation.
Conversely, after amputation, once the wound at the stump has healed, a prosthesis can be fitted and gait training with the prosthesis can begin early. As there is no need to consider wound rest or weight-bearing restrictions, active efforts to improve muscle strength and mass can be pursued even during postoperative chemotherapy and may be associated with the observed maintenance or increase in trunk muscle mass in this group.
One limitation of this study is the small sample size. Osteosarcoma is a rare malignancy, which limited the number of eligible cases during the study period. Therefore, this study should be considered exploratory and hypothesis-generating rather than confirmatory. Furthermore, neither did we evaluate the physical activity levels and nutritional status of patients during hospitalization, nor did we investigate the specific rehabilitation exercises they performed in detail. Another limitation is that the trunk muscle mass was assessed using a single CT slice, meaning that volumetric and qualitative evaluations of the muscles were not performed. Rehabilitation protocols differed between surgical procedures, making it difficult to distinguish the effects of surgery from those of rehabilitation. As this was a single-center study including only patients who met specific imaging criteria, the generalizability of the findings may be limited. Furthermore, potential confounding factors—such as variations in chemotherapy dose intensity, treatment-related symptoms (e.g., pain and fatigue), and disease progression status, including metastasis—were not evaluated and may have influenced changes in muscle mass.
Trunk muscle mass reflects overall muscle mass and contributes to stability during standing and walking. Particularly during transfemoral prosthetic gait following amputation, the trunk muscles, along with the muscles around the hip joints, significantly influence walking speed and gait performance. 15 Based on the findings of this study, further research with a larger number of cases is necessary to directly compare changes in trunk muscle mass between the limb-sparing and amputation groups. Such research may help inform the development of rehabilitation programs aimed at improving muscle strength and mass in young patients with osteosarcoma after limb-sparing surgery. Additionally, future studies should consider measuring trunk muscle mass volumetrically and focus on the qualitative evaluation of muscles rather than solely on their quantity.
Conclusion
This study highlights the challenges of maintaining trunk muscle mass during preoperative and postoperative chemotherapy in pediatric patients with osteosarcoma. Our findings indicate that the type of surgical procedure is associated with differences in rehabilitation outcomes. Amputation may allow more active postoperative rehabilitation and may facilitate maintenance or increases in muscle mass, whereas limb-sparing surgery may involve prolonged restrictions that hinder muscle development. These findings support the need for tailored rehabilitation protocols that consider the surgical approach and emphasize strategies to better support muscle mass recovery in patients undergoing limb-sparing surgery. Future research should include larger sample sizes and incorporate volumetric and qualitative muscle assessments to provide a more comprehensive evaluation.
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of Sapporo Medical University Hospital (IRB No 352-49) was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to Participate
Informed consent was obtained as an opt-out method.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Presentations
This study was presented at the 61st Annual Meeting of the Japanese Association of Rehabilitation Medicine, held from June 13 to June 16, 2024.
Authors’ Contributions
M.A.: Data curation, formal analysis, writing—original draft. M.T.: Conceptualization, methodology, writing—original draft. T.M.: Conceptualization, methodology, writing—original draft. M.E.: Writing—original draft, writing—review & editing. All the authors have reviewed and approved the final version of the article.
Footnotes
Acknowledgment
The authors sincerely thank the physical therapists at the Department of Rehabilitation, Sapporo Medical University Hospital, for conducting the training sessions during the treatment period. Their dedicated support was instrumental to the success of this study. The authors also thank the radiologists at the Department of Radiology, Sapporo Medical University Hospital, for performing the CT scans and providing their expertise in the analysis. Finally, the authors thank Editage (![]() ) for English language editing.
) for English language editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors declare that no funds, grants, or other support were received during the preparation of this article.