
Abstract
Disordered eating behaviors pose significant health risks, yet evidence among young adult (YA) cancer survivors is limited. We examined the prevalence and associated factors of disordered eating attitudes and binge eating symptoms in YA survivors (18–39 years). Participants (n = 173) completed surveys assessing eating attitudes and behaviors, food security, and demographics. Briefly, 21.5% reported high concern for disordered eating attitudes, and 26.6% had moderate-severe binge eating risk. Both outcomes were significantly associated with weight-related concerns (β = 0.45 and β = 0.46) and socioeconomic advantage (β = 0.31 and β = 0.22). Food insecurity predicted higher binge eating (β = 0.22). Screening, education, and resource provision in survivorship care are needed.
Introduction
Cancer survivorship rates among young adults (YA), defined as individuals aged 18–39 years, have been increasingly improving, with 5-year survival rates ranging from 83% to 86%. 1 A cancer diagnosis and treatment are life-changing for most individuals; however, YAs face unique challenges during this developmental period as they navigate key milestones such as finishing school, starting college, building careers, forming relationships, and starting families. 2 Because of these challenges, this stage of life is characterized by increased vulnerability to stress, making YA more likely to have specific needs and psychosocial challenges that are unmet. 2 Studies targeting YA cancer survivors have been found to show poor mental health and reduced quality of life, along with impaired social functioning that significantly impacts their daily lives and long-term well-being. 2,3 Financial hardship and socioeconomic inequities worsen psychological health and overall functioning, with YAs being particularly vulnerable compared to older adults due to greater work limitations, fewer financial resources, and high out-of-pocket costs that often lead to medical debt and bankrupcy. 4
Disordered eating behaviors are a major public health issue due to their association with increased depressive symptoms over time, a higher risk of future suicidality, an elevated likelihood for a later eating disorder diagnosis, and excessive long-term weight gain. 5,6 Disordered eating behaviors encompass a broad spectrum of eating-related actions and attitudes toward food, weight, shape, and appearance that do not meet the frequency and severity criteria for a diagnosed eating disorder. These behaviors include binge eating and unhealthy weight-control practices such as self-induced vomiting, food restriction, dieting, and emotional eating. 7 Eating disturbances and body dissatisfaction are among the most common negative psychological effects from cancer diagnosis and treatment 8,9 and play a critical role in the onset and progression of eating disorders. 10 However, evidence on disordered eating behaviors among YA cancer survivors remains limited, with most research focusing on body image and consistently reporting high levels of body dissatisfaction in this population. 9 In addition, one study reported that mental health was significantly associated with eating beliefs, particularly those related to binge eating in YA survivors. Given the heightened vulnerability of this population to developing eating disorders due to psychological stress, further research is needed to characterize the prevalence and associated factors of eating disorders in YA survivors of cancer. Accordingly, this cross-sectional study aimed to examine the prevalence and associated factors of disordered eating attitudes and binge eating symptoms within this group of YAs to inform future hypothesis-driven research.
Methods
Study design, participants, and setting
This is a cross-sectional study with YA cancer survivors from a southeastern National Cancer Institute (NCI)-designated comprehensive cancer center, diagnosed between the ages of 18 and 39, who were able to read and speak English. Participants were recruited using a convenience sampling approach through the cancer center’s Adolescent Young Adult Program monthly newsletter, distributed via email between 2023 and 2024. The newsletter included a study flyer describing the study purpose and eligibility criteria, along with a QR code and link directing interested individuals to the REDCap survey. Upon accessing the link, potential participants first completed an eligibility screener. Those who met inclusion criteria were routed to the electronic informed consent form. After providing consent, participants proceeded to the online survey, which took approximately 35 minutes, and received a $30 gift card for participation in the study. All information collected from participants was in full Institutional Review Board (IRB) and Health Insurance Portability and Accountability Act compliance.
Data collection
The online self-administered survey contained general demographic questions (e.g., age, gender, race/ethnicity, and education), diagnosis-related questions (e.g., type of cancer and time since treatment ended), the Eating Attitudes Test (EAT-26), 11 the Binge Eating Scale (BES), 12 the 6-item US Household Food Security Survey, 13 and self-reported weight and height, which were used to calculate body mass index (BMI).
The EAT-26 is a widely used self-report measure of symptoms and concerns characteristic of eating disorders. 11 It consists of 26 items divided into three subscales: Dieting, which assesses restrictive eating and weight concerns; Bulimia and Food Preoccupation, which evaluates binge eating and purging tendencies; and Oral Control, which examines self-control overeating and external pressures to gain weight. Possible scores range from 0 to 78, and a total score of ≥20 indicates elevated eating and weight-related concerns with potential risk for an eating disorder and the need for further clinical evaluation.
The BES is a 16-item questionnaire assessing the presence of certain binge eating behaviors, which may be indicative of an eating disorder. 12 The scale consists of two components [eating behaviors (eight questions) and emotional cognition upon binge eating (eight questions)]. Each of the 16 items presents four response options, ranging from no binge eating symptoms (score = 0) to severe binge eating symptoms (score = 3). The total score can range from 0 to 46. Scores are categorized as follows: ≤17—no or minimal binge eating behavior, 18–26—moderate binge eating behavior, and ≥27—severe binge eating behavior. 12
The US Household Food Security Survey 13 is a validated, 6-item scale that assesses household food insecurity and hunger in the last 12 months. Increased affirmative responses to items (e.g., “The food that (I/we) bought just didn’t last, and (I/we) didn’t have money to get more.” Was that often, sometimes, or never true for (you/your household) in the last 12 months?) indicate higher food insecurity levels. Possible scores range from 0 to 6, with higher scores indicating lower levels of food security. Scores are categorized as 0–1 = marginal food security; 2–4 = low food security; and 5–6 = very-low food security. 13
Data analysis
Descriptive statistics were calculated to characterize the sample. For bivariate and multiple regression analysis, variables were recoded to ensure adequate cell counts and preserve statistical power given the sample size. Race/ethnicity was dichotomized as White or minority groups (including Black/African American, Hispanic/Latino, Asian American, Asian/Pacific Islander, and multiracial). Due to a small cell size (N = 3) and to protect participant confidentiality, individuals who identified as “Other” for gender were excluded from the final regression analysis. To capture the multidimensional nature of socioeconomic status (SES) while minimizing model degrees of freedom, a three-level composite SES variable was created by combining education (low education: ≤high school degree, high education: >high school degree) and income (cut point: $50,000) into three categories: low education/any income, high education/low income, and high education/high income. For cancer treatment types, surgical treatment was combined with immunotherapy and hormonal therapy, while chemo and radiation were kept as a distinct category. Weight concerns and food insecurity were entered as continuous variables. Bivariate analysis was performed using independent t tests, Analysis of Variance (ANOVA), or Pearson correlations, as appropriate. To examine factors associated with disordered eating behaviors, two separate hierarchical multiple linear regression analyses were conducted, one for each outcome: EAT-26 total score and BES total score. Both models used the same three sequential blocks of variables: (1) sociodemographic factors, (2) clinical factors, and (3) psychosocial factors. Model assumptions were verified for each analysis. Multicollinearity was assessed using variance inflation factors. Linearity and homoscedasticity were inspected visually using scatterplots of standardized residuals versus fitted values, and normality of residuals was verified using Q–Q plots. Statistical significance was set at p < 0.05 (two-tailed).
Results
Descriptive characteristics are summarized in Table 1. The mean age of participants was 33.7 ± 5.6 years, and 79.2% were female. Most participants were White (70.5%), 67.7% had a college degree or higher, and 43.4% had yearly incomes greater than $70,000. The most common cancer type was breast cancer (20.8%); patients were most frequently diagnosed with cancer stage II (25.4%); and chemotherapy (67.1%) and surgery (59.0%) were the most common types of treatments. One quarter of YA cancer survivors reported comorbidities, with the most frequent being obesity (15.0%). The mean BMI was 28.5 (8.4) kg/m2. Approximately one third of the participants were highly concerned about their weight (20.2% very and 12.7% extremely concerned). More than one quarter experienced some degree of food insecurity (28.3% low or very low food security), and the food insecurity score mean was 1.2 ± 1.7. Figure 1 illustrates the scores obtained from the EAT-26 and BES, revealing that 21.5% of the participants had high levels of concern about dieting, body weight, or problematic eating behavior, while 26.6% had moderate to severe risk for binge eating disorder. The mean EAT-26 score was 12.9 ± and the mean BES score was 12.6 ± 8.6.

Distribution of Eating Attitudes Test-26 (EAT-26) and Binge Eating Scale (BES) scores among young adult cancer survivors (n = 173).
Demographic and Clinical Characteristics of Adolescent and Young Adult Cancer Survivors (n = 173)
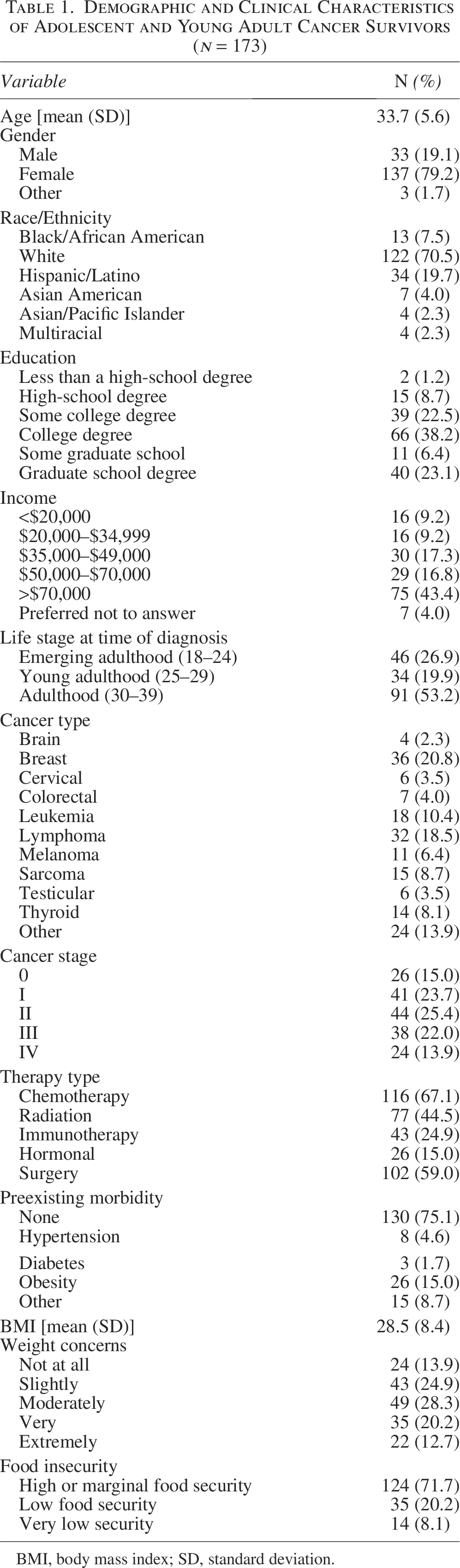
BMI, body mass index; SD, standard deviation.
In Table 2, the hierarchical multiple regression analysis demonstrated that the EAT-26 score was significantly positively associated with having “High Education/High Income” status (β = 0.31, p = 0.011) and with increasing weight concerns (β = 0.45, p < 0.001). In the BES score models, significantly positive association was found for “High education/High income” status (β = 0.22, p = 0.037), having a pre-existing comorbidity (β = 0.19, p = 0.004), increasing weight concerns (β = 0.44, p < 0.001), and increasing food insecurity (β = 0.22, p = 0.001). In contrast, radiation was negatively associated with the BES score (β = −0.16, p = 0.015).
Hierarchical Multiple Linear Regression Analyses of the Association Between the Eating Attitudes Test-26 Score and the Binge Eating Scale Score with Covariates Among Young Adult Cancer Survivors (n = 173)
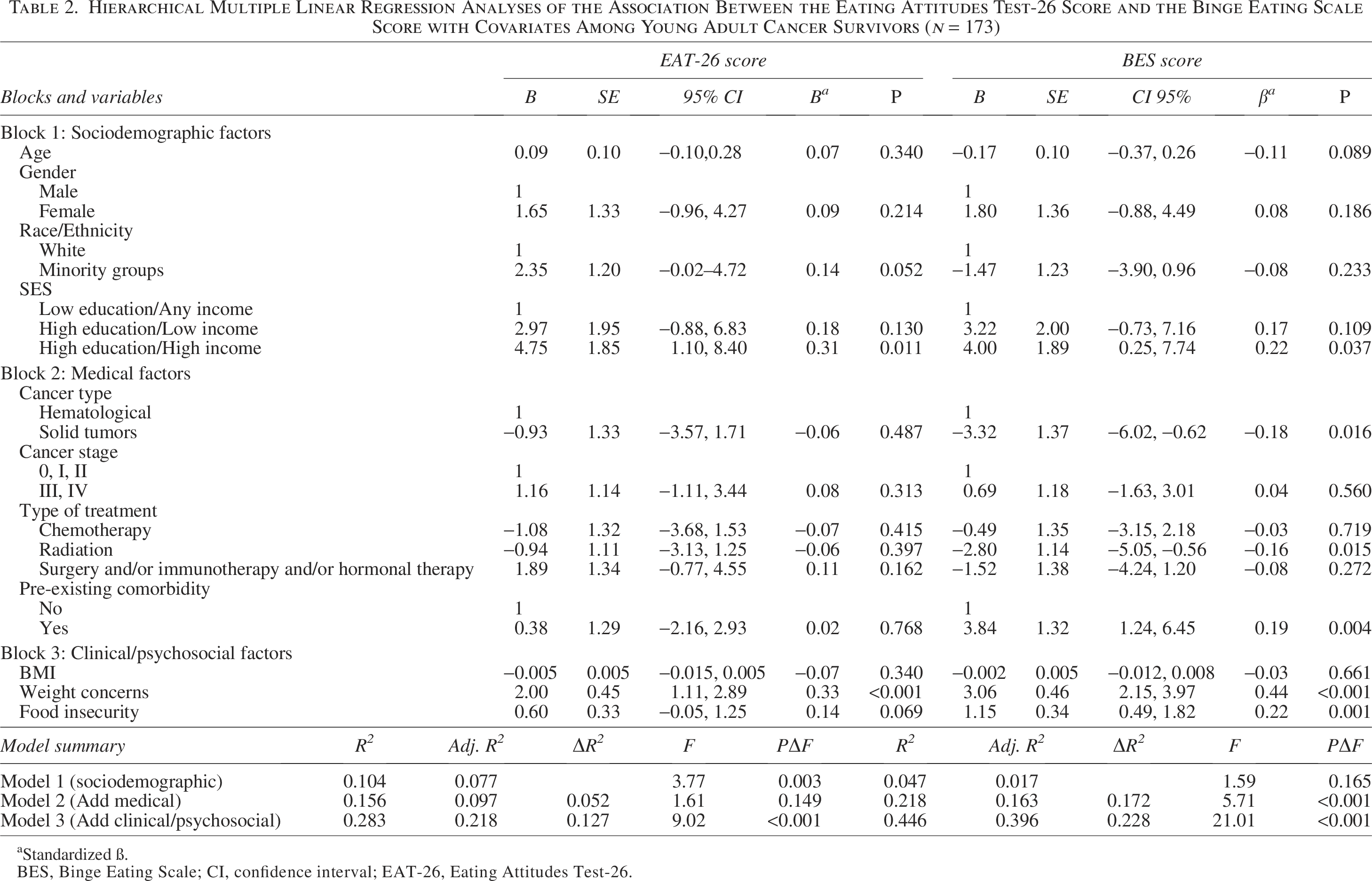
Standardized ß.
BES, Binge Eating Scale; CI, confidence interval; EAT-26, Eating Attitudes Test-26.
Discussion
Our findings revealed a high prevalence of binge eating symptoms among YA cancer survivors, while disordered eating attitudes were comparable to those reported in other studies. Weight-related concerns emerged as the strongest predictor for both outcomes (β = 0.33, p < 0.001, and β = 0.45, p < 0.001, respectively), underscoring the psychological burden associated with weight in this population. SES was identified as another substantial predictor, with the most socioeconomically advantaged group showing positive associations with disordered eating attitudes (β = 0.32, p = 0.009) and binge eating symptoms (β = 0.22, p = 0.036). We also found that YA experiencing food insecurity (β = 0.24, p < 0.001) reported significantly higher levels of binge eating symptoms.
Our study found that the prevalence of disordered eating attitudes in our sample (21.5%) was similar to that reported in the general U.S. population (16.7%–23.9%). 14,15 Importantly, the prevalence of binge eating symptoms among YA cancer survivors (26.6%) exceeded rates reported in previous studies of university students using the BES (12.9%–20%). 16,17 However, our sample was skewed toward older individuals within the YA age range. Research on this phenomenon among YA cancer survivors is limited, with reported prevalence of disordered eating behaviors varying greatly (6.5%–49.7%), 8,18 –20 which may be related to a lack of standardized, population-appropriate assessment tools. Evidence from longitudinal studies indicates that disordered eating behaviors contribute to psychological issues across all ages, leading to ongoing stress, anxiety, and abnormal weight fluctuations that impact daily life. 21,22 This is particularly critical for YA cancer survivors, who face heightened risks due to the long-term effects of cancer treatment and survivorship challenges.
Weight-related concerns were significantly positively associated with EAT-26 and BES scores. Core risk factors for eating disorders include weight/body shape concerns, overvaluation of weight/body shape, and drive for thinness disorders. 10 Although body image concerns have been examined among YA cancer survivors, 9 weight concerns remain relatively understudied. Our findings align with prior research on breast cancer survivors (mean age: 51 ± 6.3 years), which reported greater weight concern compared to matched controls (mean diff = 0.5, ES = 0.42, p < 0.001). 8 These findings underscore the need to deepen our understanding of weight concerns among YA cancer survivors in order to develop innovative strategies, such as interventions exploring emerging technology-based strategies to promote interoceptive awareness and body acceptance, 23 to effectively reduce the eating disorders risk.
The literature is inconsistent regarding the relationship between SES and disordered eating behaviors. 24 In our study, socioeconomic advantage was associated with disordered eating behaviors, while binge eating symptoms showed a significant positive association with food insecurity. Although these associations appear to emerge from opposite ends of the socioeconomic spectrum, they likely reflect distinct pathways that can each lead to elevated disordered eating symptoms. In the general population, a systematic review and meta-analysis found that food-insecure adults had 1.66 times higher odds of binge eating (95% CI: 1.42–1.93) and 2.70 times higher odds of binge eating disorder (95% CI: 1.47–4.96) compared to food-secure adults. 25 Among YA cancer survivors, a cohort study similarly reported that severe food insecurity was associated with a greater prevalence of binge eating. 26 Further research is needed to elucidate the mechanisms underlying the relationship between SES, food insecurity, and disordered eating behaviors in YA cancer survivors.
Our study has several limitations, including its cross-sectional design, small sample size, reliance on self-reported measures (e.g., screeners and short-form assessments), and the inability to comprehensively assess social determinants of health due to survey length constraints. Furthermore, as this was an exploratory study, we prioritized the use of brief screening tools rather than incorporating clinical diagnoses of eating disorders. These findings may also be less generalizable beyond an NCI-designated cancer center. Future research should include larger and more diverse samples, incorporating cancer survivors receiving care in varied settings, and more social determinants of health to better examine potential differences across gender, race, ethnicity, cancer type, resource availability, and environmental conditions.
Conclusion
The association between weight concerns, SES, and food insecurity with disordered eating behaviors suggests that both psychological and social determinants shape post-treatment outcomes, underscoring the complex interplay of financial and nutritional challenges in this population. Care initiatives could include screening and education on eating behaviors within routine health care, along with resources to support cancer treatment outcomes, while also exploring emerging technology-based strategies that offer promise despite recognized limitations. 23,27 However, further research is needed to evaluate their effectiveness.
IRB Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the IRB of Moffitt Cancer Center (protocol number: MCC#22488).
Authors’ Contributions
A.P.S.R.: Writing—review and editing, writing—original draft, visualization, and formal analysis. AW.B. and N.I.B.: Writing—review and editing, conceptualization, methodology, project administration, investigation, and data curation. T.L.C. and M.S.: Writing—review and editing, conceptualization, methodology, and funding acquisition.
Footnotes
Acknowledgment
The authors would like to thank the participants of this study for their valuable contributions.
Data Availability Statement
The data analyzed for the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This work was supported by the Moffitt Adolescent and Young Adult Survivorship Program.