
Abstract
Purpose:
Theoretical models on fear of cancer recurrence (FCR) have been developed and validated for adult cancer survivors, despite high levels of FCR being found in adolescents and young adults (AYAs). This study intended to empirically validate a model of FCR for AYAs based on the theoretical models of Lee-Jones and Lebel.
Methods:
One hundred AYAs diagnosed with cancer between the ages of 15 and 25 were included (59% female). Data were collected online and in-person from four hospitals and one association for young cancer patients in Portugal using the Quality of Life (QoL) Questionnaire Core-30, the FCR7 scale, the Emotion Regulation Questionnaire, the 15-item Systematic Clinical Outcome and Routine Evaluation scale, the Satisfaction with Social Support Scale, and the Hospital Anxiety and Depression Scale.
Results:
A path analysis showed an excellent model fit: χ2(28) = 30, p = 0.363; Bentler comparative fit index (CFI) = 0.99; Tucker–Lewis index = 0.98; root-mean-square error of approximation = 0.03; standardized root-mean-square residual = 0.08. Significant paths were found from FCR to depressive symptoms and QoL, with friends’ support moderating the path between FCR and depressive symptoms. Depressive symptoms and QoL were also related to emotion suppression and friends’ support.
Conclusion:
Being satisfied with their friends’ support seems to be protective for AYAs with high FCR levels, while satisfaction with family support does not seem to have an influence. This diverges from previous models, supporting the need for a distinct AYA model. Additionally, emotion suppression was related to depression and QoL, but not FCR.
Introduction
Cancer diagnoses are increasing, particularly in younger people. Among adolescents and young adults (AYAs), individuals between the ages of 15 and 39, 1 over 1.3 million have been diagnosed with cancer worldwide in 2022. 2 Data have shown an ascending trend in incidence and cancer burden globally among AYAs, together with a decline in mortality.2,3 With this increasing prevalence, it is important to enhance our understanding of how cancer impacts these young survivors.
Adolescence and young adulthood are challenging developmental periods focused on exploration and change (e.g., biological, physiological, psychological, developmental, and societal).1,4 When confronted with cancer, these normative tasks can be disrupted. AYAs with a cancer diagnosis typically face a premature confrontation with their mortality, may become increasingly dependent on their parents, experience changes in their social life and education/career, among other challenges.1,5 Consequently, AYAs tend to face unique psychosocial and developmental issues when diagnosed with cancer.1,5 In recent years, AYAs with cancer have gained international recognition, evidenced by the increasing number of published articles, allowing a better understanding of the impact of cancer.
Research indicates that one of the main causes of distress for AYAs with cancer is fear of cancer recurrence (FCR), 6 which is defined as “fear, worry, or concern about cancer returning or progressing.” 7 In fact, studies with participants over 18 years old have shown that younger age is a risk factor for high FCR. 8 A systematic review focused on FCR in AYAs with cancer found that 31%–41.9% experience moderate levels of FCR and 13%–62% high levels. 9 This broad range could be due to the diverse ways FCR was measured in the included studies (e.g., FCR instruments, single question, and study-specific questions). Additionally, the currently accepted FCR definition was published in 2016, 8 while the studies included in this review were published between 1997 and 2018, 10 which could also have influenced it. Nonetheless, more recent studies have found similar prevalences ranging from 20% to 93.3%,10–16 further supporting the high prevalence of FCR among AYAs with cancer. When it comes to FCR evolution over time, a longitudinal study with young breast cancer survivors 13 found that FCR seems to diminish for most survivors. However, for 34% of them, FCR increased or remained high for up to 5 years post-diagnosis. 13
Up to a certain point, FCR can be adaptive, leading to behavioral changes focused on normative checking and physical alertness. However, when FCR leads to high preoccupation/worries that persist for over 3 months along with an excess of vigilance and sensitivity to bodily symptoms, 17 it becomes a problem. Research shows that high FCR affects the mental health of AYAs with cancer, with studies finding associations with low quality of life (QoL) and high anxiety, depression, and post-traumatic stress symptoms.9–11 Furthermore, experiencing high FCR was related to high fatigue symptoms and physical comorbidities.9,11 Considering the negative impact FCR can have on AYAs with cancer, the development of interventions for this group is crucial, requiring a clearer picture of the mechanisms that influence FCR.
Models of FCR in adult survivors
Over the years, several models have been proposed to help understand FCR in adults.18–24 These models usually suggest that (1) some internal or external trigger to FCR exists, (2) the way this trigger is interpreted can influence FCR, and (3) FCR can lead to a behavioral or emotional response. Some of these models also focused on cognitive processes and contents, such as metacognitive beliefs about worry,22,23 and cognitive bias, 24 or explored the role of social variables in predicting FCR. 21 Below, two widely used FCR models will be further explored as they set the foundation for this study.
The first model to conceptualize FCR was the Self-Regulation Model of Illness by Lee-Jones and colleagues. 19 Considering that FCR is based on a person’s illness representation, it was suggested that internal and external cues are antecedents that activate cognitions, beliefs, and emotions related to FCR, depending on how they are interpreted. This can lead to behavioral and psychological consequences that can further influence the cognition and interpretation of the cues. This model has been empirically validated, with findings indicating that FCR mediates the relationship between internal (e.g., feeling sick and attention to internal bodily sensations) and external cues (e.g., contact with health professionals, media, and social context), and limited planning for the future and body checking. 25
More recently, Lebel and colleagues 20 proposed a blended model of FCR. This model stated that internal and external cues increase the perceived risk of recurrence, which, in turn, increases FCR. The coping strategies used by survivors are hypothesized to have a bidirectional relationship with FCR, meaning that while maladaptive coping strategies (i.e., avoidance, body checking, etc.) may give an immediate reassurance that cancer has not come back and temporary relief, in the long-term, they increase FCR. Furthermore, uncertainty in illness moderates the relationship between triggers and the perceived risk of recurrence. Survivors’ intolerance of uncertainty and their metacognitions are considered important vulnerability factors that maintain worry. This blended model of FCR was empirically validated, that is, triggers, perceived risk of recurrence, and uncertainty about illness predicted FCR, with the latter being associated with maladaptive coping strategies. Positive beliefs about worrying and intolerance to uncertainty led to even more maladaptive coping but did not predict FCR. 20
Why existing FCR models may not be the best fit for AYAs
Despite these models’ important contribution to FCR understanding, their validation studies only included adult cancer survivors as participants, which limits our understanding of FCR in AYAs with cancer. Additionally, there are developmental factors that are important during adolescence and young adulthood but are not being considered in these models. As mentioned above, adolescence and young adulthood are challenging periods where several important developmental tasks occur.1,4 Through the interaction with their social environment, including their peers, AYAs develop their personal and sexual identity, establish long-term relationships, or gain independence from their parents, for example. However, a cancer diagnosis can disrupt their social interactions. 5 AYAs with cancer report feeling isolated and alienated from peers while missing out on typical activities their peers are experiencing. Social support can help AYAs with cancer cope with their illness and help them feel less alone. 5 Considering the significant impact that FCR has on AYAs’ lives and the lack of an age-specific model, we propose a model to better understand FCR in AYAs with cancer based on existing, validated models of FCR for adults.19,20
FCR-AYA model
Like the two previous models,19,20 we hypothesize that when AYAs with cancer experience internal and external triggers, it can be interpreted as a possibility that cancer has returned, leading to an increase in FCR levels. The severity of the FCR experienced will depend on the uncertainty of illness, in line with the findings by Lebel and colleagues. 20
Additionally, experiencing high FCR could lead to behavioral responses by the AYA with cancer (such as visiting the doctor) and/or have psychosocial consequences (such as experiencing high anxiety, high depression, or low QoL), as suggested by Lee-Jones. 19 The coping and/or emotion regulation strategies used are expected to influence the AYAs’ FCR levels. For those who resort to maladaptive coping and/or emotion regulation strategies, it is possible that when experiencing FCR, these may lead to increased behavioral responses and/or psychosocial consequences. In the model by Lebel, 20 coping strategies such as avoidance and reassurance-seeking were related to high FCR in adults. As for emotion regulation strategies, one type that has been previously investigated is emotional suppression (i.e., when a person suppresses the external expression of emotion, like putting on a smile when they are sad), 26 with a recent meta-analysis finding that emotional suppression was related to worse psychosocial outcomes in adult cancer patients. 27
Furthermore, it is hypothesized that some factors could strengthen (i.e., risk factors) and/or weaken (i.e., protective factors) the relationship between FCR and behavioral responses/psychosocial consequences. During adolescence and young adulthood, family, peers, and intimate relationships are essential for healthy development.4,28 However, cancer can disrupt their social life and increase dependence on parents or other caregivers. 5 The literature on adults with cancer has also found that good family communication 29 and social support 30 were associated with low FCR, making them potentially important factors in FCR. These factors may play a role in maintaining or mitigating AYAs’ FCR levels. A schematic representation of the proposed FCR-AYA theoretical model is shown in Figure 1.
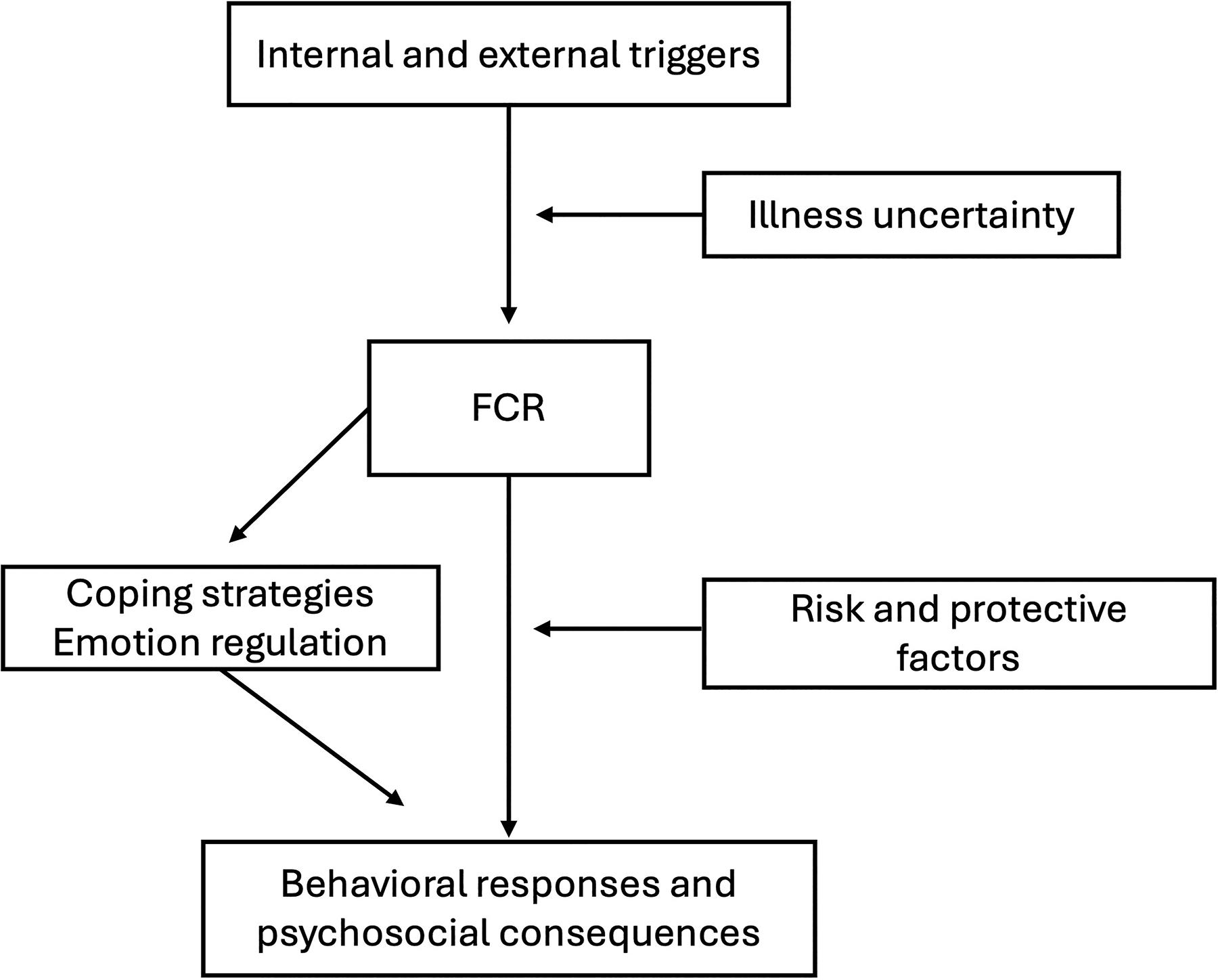
Proposed theoretical model of FCR in AYAs. AYAs, adolescents and young adults; FCR, fear of cancer recurrence.
In summary, although AYAs with cancer have a high prevalence of FCR, which impacts their mental health and QoL, no validated model exists to explain the mechanisms that trigger and sustain FCR in AYAs. The FCR-AYA model builds upon previous FCR models for adults by incorporating the potential role of emotional regulation strategies in the behavioral responses and psychosocial consequences of FCR, and by considering risk/protective factors that are important to the psychosocial development of AYAs based on theories of human development. Validating and refining the FCR-AYA theoretical model is essential and could assist in developing or adapting interventions to reduce FCR levels in AYAs with cancer. Thus, this study aims to empirically validate part of the FCR-AYA model.
We hypothesized that (1) internal triggers, such as high pain and fatigue, will be related to high FCR; (2) suppressing one’s emotions will be associated with high FCR and psychosocial consequences (high depression and low QoL); (3) FCR will be related to high depression and low QoL as well; and (4) that family communication and satisfaction with support from family and friends will moderate the relationship between FCR and psychosocial consequences.
Method
Participants
Since AYAs with cancer are a heterogeneous group, we adjusted the age range according to the study’s objectives. 31 For this cross-sectional study, we considered AYAs diagnosed with cancer between 15 and 25, whose developmental stages are more alike in this age range, aligned with previous studies. 32 Nonetheless, it is important to note that these similarities may not extend to all developmental domains nor to non-WEIRD (i.e., western, educated, industrialized, rich, and democratic) populations. The literature on FCR consistently shows no significant association between FCR and time since diagnosis and survivorship stage, 9 so no limits were imposed.
One hundred AYAs (59% female, 41% male), between 15 and 38 years old at recruitment (M = 23.17, SD = 5.45), participated in this study (Table 1). Most were single (86%), either students (43%) or full-time employees (33%), and almost half had already finished high school (44%). As for their clinical characteristics, most AYAs were diagnosed with hematological cancer (Hodgkin’s lymphoma = 49%; leukemia = 16%; non-Hodgkin lymphoma = 8%). The average age at diagnosis was 19 (SD = 3.24). Most AYAs were diagnosed up to 5 years prior (83%) and were no longer under treatment (70%), had not had a recurrence (77%), and did not report having additional health problems (78%).
Sociodemographic and Clinical Characteristics of the Participants
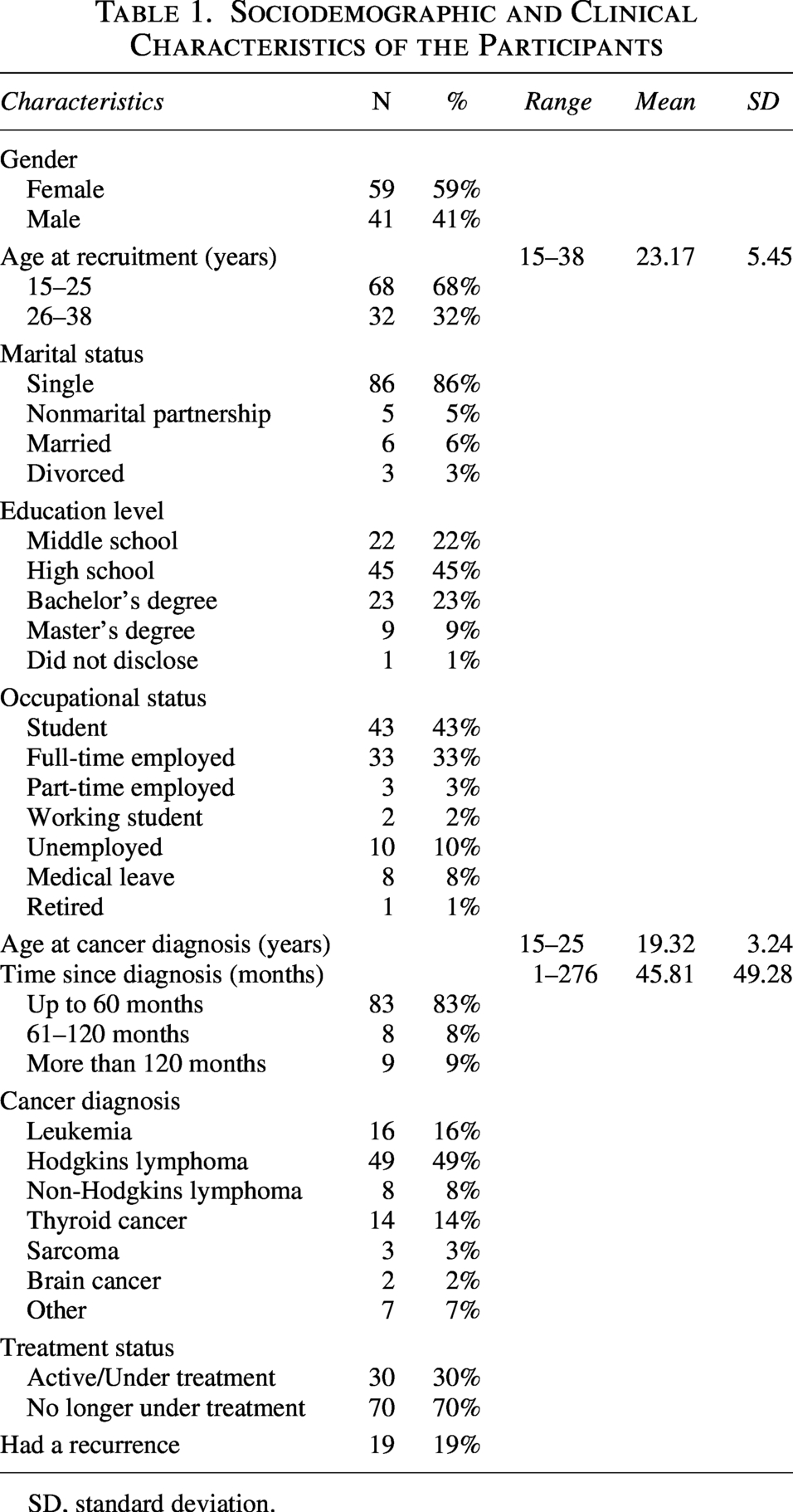
SD, standard deviation.
Measures
Internal triggers
Bodily sensations
Pain and fatigue were assessed using the symptoms subscales of the European Organization for Research and Treatment of Cancer (EORTC) QoL Questionnaire Core-30 (QLQ-C30).33,34 The pain subscale included two items, and the fatigue subscale three items. These were scored on a 4-point Likert scale, with higher scores indicating higher symptoms. In the Portuguese validation of this questionnaire, 34 these subscales showed good internal consistency (α = 0.81 for pain and α = 0.84 for fatigue). Similar results were found in our sample (α = 0.85 for both).
FCR
The Fear of Cancer Recurrence 7 scale35,36 was used to assess FCR levels. This unidimensional scale included six items on a 5-point Likert scale and one item on an 11-point scale. A higher score indicates greater FCR levels, with a score of 20 or higher indicating clinically relevant levels. Regarding internal consistency, the Portuguese validation 36 showed good results (α = 0.89), corroborated in our sample (α = 0.92).
Emotion regulation
Emotion suppression
A subscale of the Emotion Regulation Questionnaire37,38 assessed emotion suppression. The four items were scored on a 7-point Likert scale, with higher scores representing greater use of emotion suppression. Both the Portuguese validation for cancer patients 38 and our sample showed good internal consistency (α = 0.72 and 0.8, respectively).
Risk and protective factors
Difficulties in family communication
The 15-item Systemic Clinical Outcome and Routine Evaluation scale39,40 assesses family function and contains one subscale for difficulties in family communication. With five items, this subscale is scored on a 5-point Likert scale. Higher scores correspond to higher levels of difficulty regarding family communication. A Cronbach’s α of 0.73 was found in the Portuguese validation 39 and of 0.82 in our sample.
Satisfaction with social support
Two subscales from the Satisfaction with Social Support Scale 41 assessed perceived satisfaction with social support from friends and family. Each subscale had five items rated on a 5-point Likert scale, with higher scores representing greater perceived social support. The original validation of the scale in Portugal found α = 0.83 for the subscale on satisfaction with support from friends and α = 0.74 for the family one. In our sample, similar results were found (α = 0.79 and 0.74, respectively).
Psychosocial consequences
Depression
The Hospital Anxiety and Depression Scale42,43 was used to assess depressive symptoms. The subscale Depression has seven items on a 4-point Likert scale, with higher values indicating higher depressive symptoms. Internal consistency was 0.81 in the Portuguese version 43 and 0.78 in our sample.
QoL
The summary score of the QLQ-C30 was used to assess QoL, as recommended by the EORTC. 44 This includes the physical, emotional, social, role, and cognitive functioning subscales, as well as the symptom subscales (i.e., fatigue, pain, and nausea and vomiting) and single items (i.e., dyspnea, sleep disturbances, appetite loss, constipation, and diarrhea). Higher results represent higher QoL. The original article does not indicate a reliability analysis; however, in our sample, an α of 0.93 was found.
Procedure
Data collection took place between June 2023 and February 2025, both in person at two hospitals in Porto and online at two additional hospitals (one in Coimbra and one in Lisbon), as well as at one patient association in Portugal. The study was presented to potential participants by the researcher on-site or by a health professional from the collaborating institution. The patient’s association for young people with cancer disseminated the study to its members. AYAs with cancer could participate online or in person, with informed consent being obtained before participation for all participants, as well as parental consent for minors (15–17 years old at recruitment). Ethics committees and data protection authorizations were obtained from the four hospitals where data collection occurred and from the first author’s institution.
Data analysis
Data were analyzed using SPSS version 29 and R software, with a significance level of p = 0.05 (two-tailed). Univariate outliers were initially assessed using Z-scores, with values beyond ±3 considered potential outliers. Missing values were assessed with Little’s MCAR test, indicating that our missing values were completely at random, χ2(923) = 929.385, p = 0.435. Thus, the expectation–maximization method was used to handle missing values. 45 This method is part of the group of maximum likelihood methods and is considered robust and unbiased when dealing with missing data that are missing at random. 46 Next, multivariate outliers were assessed using Mahalanobis distance. Normality was evaluated by examining skewness and kurtosis, with values between ±1 indicating acceptable normality. No multivariate outliers were found, and all variables were normally distributed.
Descriptive analyses were performed, followed by Pearson correlations between participants’ characteristics and psychosocial variables to identify variables that might need to be controlled for in the model. Correlations between the psychosocial variables were also performed. Finally, a path analysis was performed using the lavaan 47 package in R to test our hypothesis after centering all variables. To ensure sufficient statistical power, we performed sensitivity analyses by modifying initial parameters to assess whether the conclusions changed. More specifically, separated models were tested for depression and QoL, followed by testing the full model. Since results were similar, only those of the full model analysis are presented in the “Results” section. Additional details and results for the separated model can be found in Supplementary Material. Model fit was assessed using the chi-square test, Bentler comparative fit index (CFI), Tucker–Lewis index (TLI), root-mean-square error of approximation (RMSEA), and standardized root-mean-square residuals (SRMR). Nonsignificant chi-square test, CFI and TLI ≥0.80, and RMSEA and SRMR <0.10 indicated acceptable fit. 48
Results
Correlations between participants’ characteristics and psychosocial variables
Age at diagnosis was positively associated with FCR, and treatment status was negatively related to depression, pain, fatigue, and emotion suppression, and positively to QoL. Emotion suppression was also negatively associated with age at recruitment. No other significant associations were found (Table 2).
Correlations Among Sociodemographic, Clinical, and Psychosocial Variables
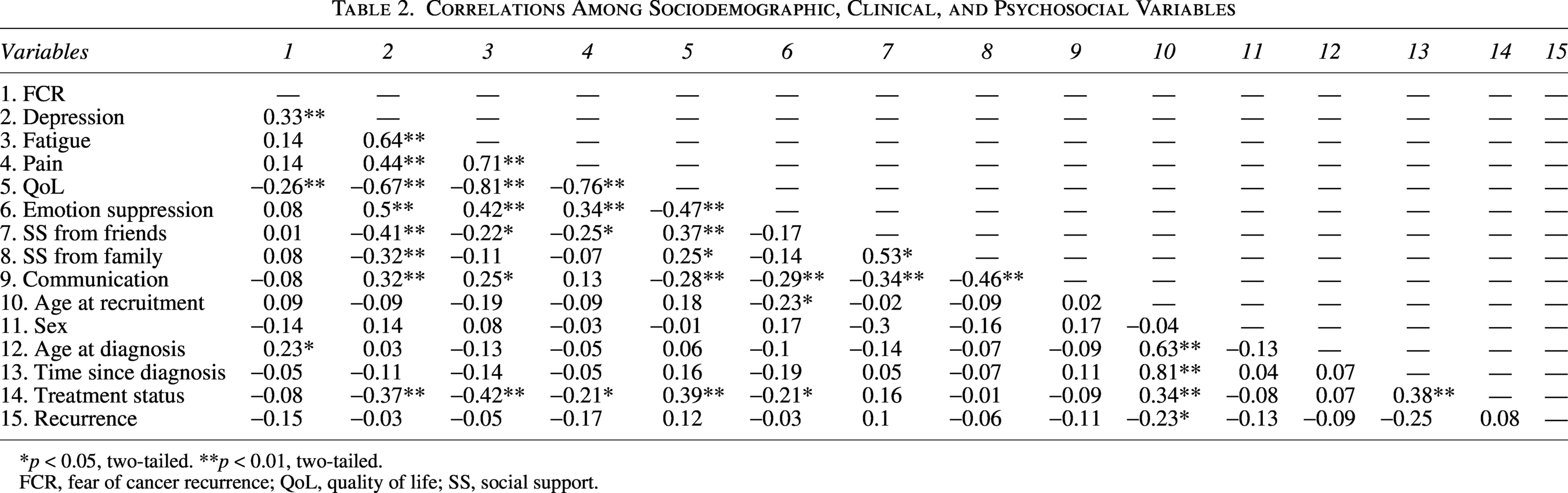
*p < 0.05, two-tailed. **p < 0.01, two-tailed.
FCR, fear of cancer recurrence; QoL, quality of life; SS, social support.
Correlation between psychosocial variables
In contrast to our hypotheses, high FCR was only significantly related to high depression and low QoL. High depressive symptoms and low QoL were associated with each other and with every other psychosocial variable in the model (pain, fatigue, emotion suppression, difficulties in family communication, and support from friends and from family). High pain and fatigue were also associated with each other, as well as high emotion suppression and low social support from friends. Additionally, high difficulties in family communication were related to high emotion suppression, high fatigue, and low satisfaction with social support from family and friends. The latter were also positively associated with each other (Table 2).
Testing the FCR-AYA model
A path analysis was used to examine the validity of the FCR-AYA model by assessing the paths from FCR to depression and QoL, and whether these were moderated by family functioning and satisfaction with friends and family support. The paths between emotion suppression, depression, and QoL were also assessed. Due to the lack of statistical power and complexity of the model, and considering the preliminary results, the paths between FCR and pain, fatigue, and emotion suppression were not included. The model was controlled for age at diagnosis and treatment status, since these variables were related to FCR, depression, and QoL.
In the first phase, without moderation interactions, the full model results indicated an excellent model fit: χ2(7) = 10.69, p = 0.153; CFI = 0.98; TLI = 0.91; RMSEA = 0.07; SRMR = 0.06. Ten paths were close to zero and statistically nonsignificant and thus were set to zero (family support with QoL; communication with depression and QoL; age at diagnosis with depression, emotion suppression, communication, and family support; treatment status with FCR, communication, and family support). The model was then tested with these paths set to zero, and results continued to show an excellent fit: χ2(17) = 18.23, p = 0.372; CFI = 0.99; TLI = 0.99; RMSEA = 0.03; SRMR = 0.08. Both models were compared, and no significant differences were found, χ2(10) = 18.27, p = 0.670. Therefore, the more parsimonious model was retained (i.e., the second model with trimming effects). Finally, the interaction terms of the moderation variables were added. Results of this model show an excellent fit: χ2(28) = 30, p = 0.363; CFI = 0.99; TLI = 0.98; RMSEA = 0.03; SRMR = 0.08.
Figure 2 illustrates the standardized coefficients of the significant paths found. Consistent with our hypotheses, FCR was positively associated with depression (β = 0.30, p < 0.001) and QoL (β = −0.24, p = 0.002). Additionally, emotion suppression was positively associated with depression (β = 0.34, p < 0.001) and negatively with QoL (β = −0.32, p < 0.001), partially confirming our hypothesis. Being satisfied with the support from friends (β = −0.23, p = 0.006) and from family (β = −0.15, p = 0.047) were both negatively linked to lower depression. Only friends’ support moderated the relationship between FCR and depression (β = −0.21, p = 0.007), partially supporting our hypotheses. Figure 3 illustrates that the positive link between FCR and depression is stronger in AYAs when the support from friends is lower. Moreover, high levels of friends’ support mitigate this association, revealing a moderation effect. This means that support from friends seems to play a protective role against the impact of FCR on depression. As for QoL, no moderation effect was found. However, friends’ support was close to reaching significance (β = 0.15, p = 0.056). QoL levels were only positively associated with support from friends (β = 0.29, p < 0.001). Considering our control variable, treatment status was positively related to QoL (β = 0.28, p < 0.001) and negatively related to depression (β = −0.28, p < 0.001), emotion suppression (β = −0.21, p = 0.033), and support from friends (β = 0.16, p = 0.047). Age at diagnosis was only positively related to FCR (β = 0.23, p = 0.02).

Path model tested of the FCR-AYA model. Note: * p < 0.05; ** p < 0.01; *** p < 0.001.
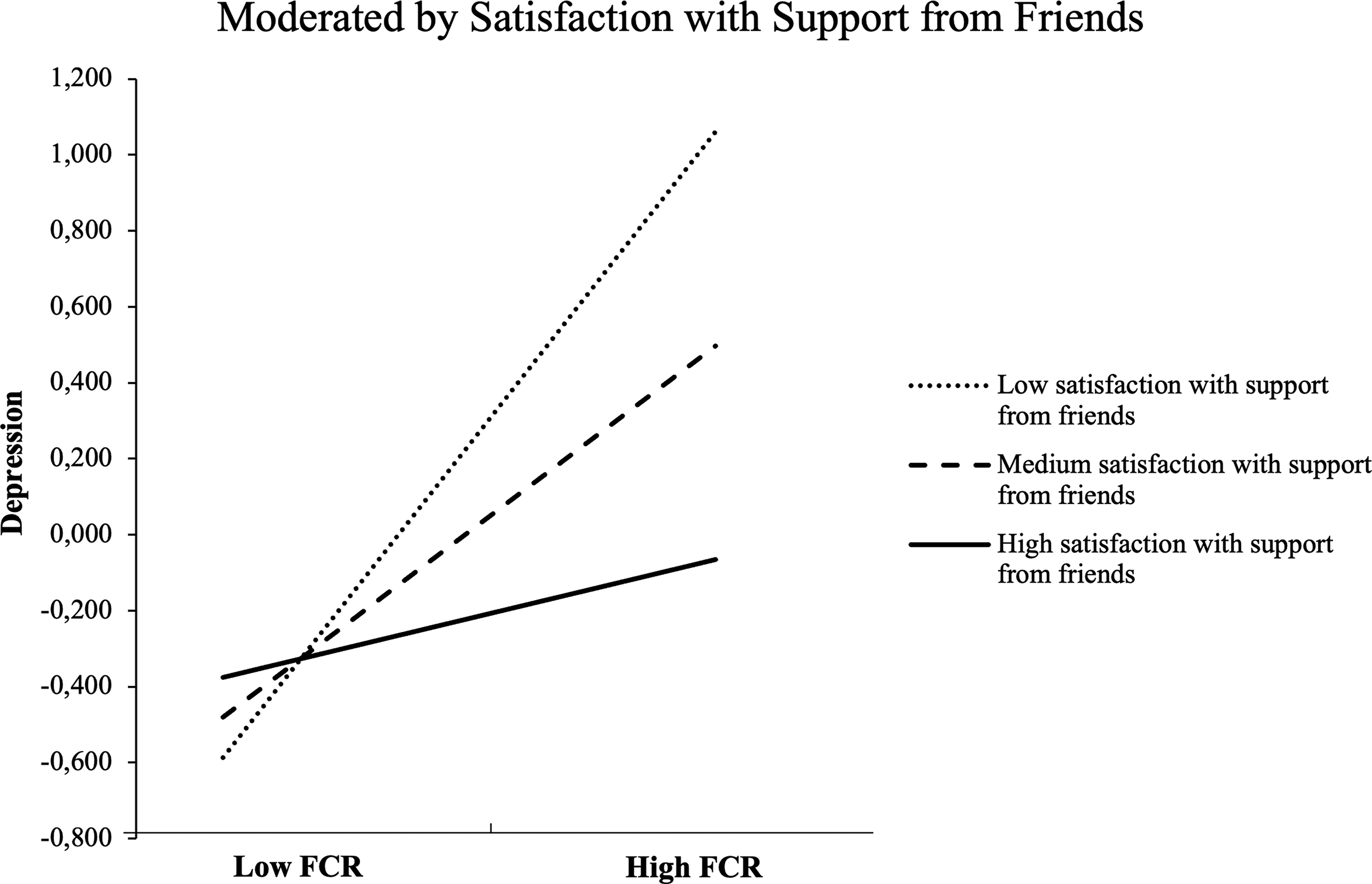
The moderating effect of satisfaction with support from friends on the relationship between FCR and depression.
Discussion
To the best of our knowledge, this study represents the first attempt to validate a model to better understand FCR in AYAs with cancer. Results partially support the proposed model based on the models by Lee-Jones 19 and Lebel 20 for adults. It indicates that FCR leads to higher depression and lower QoL, with AYAs’ satisfaction with their friends’ support moderating the relationship between FCR and depression levels. Nevertheless, replication with a larger sample is encouraged not just to confirm our findings but also to test other components of the proposed model that were not assessed in this study.
As hypothesized, high FCR was related to high depression and lower QoL in our sample, which is in line with previous research. 9 Emotion suppression was also associated with depression and QoL, but not with FCR. This result was quite surprising, considering that adults with cancer reported in interviews trying not to think, talk, or hear about FCR, by putting it aside, forgetting about it, or distracting themselves from it. 49 One possible explanation is that emotion suppression may not have a direct effect on FCR as hypothesized, but rather an indirect effect that warrants further investigation.
One interesting finding of this study is that being satisfied with the support provided by their friends seems to be protective for AYAs with cancer, weakening the relationship between FCR and depression. However, the same was not found for family communication and satisfaction with their support. During adolescence and young adulthood, relationships with peers and friends are important for healthy development,4,28 especially for individuals facing cancer. 5 AYAs with cancer may see their social lives affected by being away from school/work and missing out on experiences typical of this life phase, which could lead to isolation and feelings of alienation from their peers.1,5 Our results suggest that maintaining friendships that provide satisfactory support is important during the cancer journey to support psychosocial adjustment, making peer support a potentially helpful intervention for AYAs. Care interventions focused on reducing FCR levels and improving psychosocial adjustment in AYAs with cancer should include components not only on retaining and returning to friendships but also on developing and maintaining meaningful and supportive friendships. School-based literacy on how to deal with a peer who is diagnosed with a chronic disease like cancer is also recommended. Family also plays a crucial role during the AYAs’ cancer journey, 1 as evident by our results: Being more satisfied with their family’s support relates to lower depression levels. Nevertheless, despite these associations, family support did not moderate the relationship between FCR and depression. Therefore, interventions aiming to improve AYAs’ adjustment to cancer should target family support. However, interventions targeting FCR in AYAs should focus on friends’ support.
Contrary to our hypothesis, pain and fatigue were not related to FCR in our preliminary analysis. This contrasts with the literature, where FCR has been previously related to higher pain and fatigue in adults 50 and higher fatigue in AYAs with cancer. 9 In a qualitative systematic review, noticing something in the body (either pain or other physical symptoms) was also the most common trigger reported by adults with cancer, 49 giving strength to the important role of these symptoms as triggers. One possible explanation for our results may be the subscales used. These had only two to three general items (e.g., “Did you need to rest?”) and may not have been comprehensive enough to capture the complexity of the pain and fatigue experience. Future studies could use more comprehensive scales to assess this assumption, specifically designed to evaluate these symptoms. It is also possible that the inability to test the effect of illness uncertainty in this study, as hypothesized in our FCR-AYA model, is influencing this result. Perhaps it is not exclusively the presence of pain and fatigue that is related to FCR but rather how they are interpreted through illness uncertainty. Thus, it is important that future research test the potential role of other factors, such as illness uncertainty, in this relationship.
A positive correlation between age at diagnosis and FCR was also found, meaning that, among AYAs diagnosed between the ages of 15 and 25, those who were older at diagnosis experience higher FCR. In the AYA with cancer literature, results from previous studies are inconsistent, with some showing a negative association and others showing no association.9,10 However, it is important to note that these studies’ samples differed from our study, having focused on AYAs diagnosed with cancer between the ages of 18 and 39. Could it be that those going through emerging adulthood (18–25) at the time of cancer diagnosis experience higher FCR than adolescents (15–17) or young adults (26–39)? Exploring FCR differences among AYAs’ subgroups could provide more clues. There is also the possibility that this association results from cultural or contextual differences. For example, in Portugal, there is no health care unit specifically for AYAs with cancer. So, those diagnosed before age 18 are usually followed in pediatric clinics, while those diagnosed at age 18 or older are followed in adult clinics, which could have contributed to different experiences.
Study limitations and future directions
This article presents the first attempt to validate a theoretical model for better understanding FCR in AYAs with cancer. However, some limitations must be acknowledged. First, the sample was mainly composed of single AYAs, with more than half having been diagnosed with hematologic cancer in the last 5 years and who were no longer under treatment. Additionally, there is a wide range of time since diagnosis in our sample. This overrepresentation of specific tumor types may be a consequence of the hospitals and services where data collection occurred. Therefore, results may not be generalizable to the entire population of AYAs with cancer. Second, the measures used to assess pain and fatigue may not have been comprehensive enough to capture their complexity. Third, despite its important findings, this study cannot indicate the direction of these relationships due to its cross-sectional design. Therefore, longitudinal studies are necessary to complement the model’s validation. The FCR-AYA model tested in this article remains partial, as not all proposed variables were included. Future studies seeking to further validate it could benefit from testing the influence of these variables. Some examples are coping strategies (such as avoidance), other emotion regulation strategies, illness uncertainty, external cues (such as medical appointments or exams/medical procedures), and behavioral responses (such as planning for the future), but also other internal cues, psychosocial responses, and the potential indirect effect of emotion suppression. These variables have been included in some FCR interventions for adults that showed improvements,51–56 with one of these interventions currently under adaptation for AYAs. 57
Clinical implications
This study’s findings can have implications for our understanding of the mechanisms that sustain FCR and its impact on psychosocial adjustment, and inform future interventions aimed at improving AYAs’ mental health. For health care professionals, these results support the importance of assessing not only family support but also that of their friends. In addition to these promising results, further research is needed to confirm them and investigate other components that may play an important role in AYAs’ FCR. It is essential that further efforts be made to continually test and refine this model. This could lead to a better understanding of the mechanisms underlying high FCR in AYAs and, consequently, to the development and/or adaptation of interventions aiming at reducing FCR and its impact on AYAs with cancer.
Conclusion
This study is a first step in empirically validating a model to better understand FCR among AYAs with cancer. Our results suggest that high FCR is related to low QoL and high depression, with high satisfaction with friends’ support having a protective role against the impact of FCR on depression in AYAs. However, more investigation on FCR triggers for AYAs is warranted.
Ethics Approval
The study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the following Ethics Committee: Faculty of Psychology and Education Sciences of the University of Porto (reference number 2023/02-13), Portuguese Institute of Oncology in Porto (reference number CES. 196/023), Portuguese Institute of Oncology in Lisbon (reference number UIC/1580), University Hospital Center of São João (reference number CE-102-23), and University Hospital Center of Coimbra (reference number OBS.SF.085-2023).
Consent to Participate
Informed consent was obtained from all participants involved in the study.
Authors’ Contributions
M.C.N., J.A.E.C., and J.B.P. conceptualized the study. The work was supervised by C.S., S.M., and J.B.P. M.C.N. conducted the literature review. Dissemination of the study and data collection was conducted by M.C.N. M.C.N. analyzed the data and wrote the original draft, and F.N. assisted in the data analysis and the writing of the results section. All authors have reviewed the article, suggested improvements, and read and agreed to the submitted version of the article.
Footnotes
Acknowledgments
The authors would like to express their deep gratitude to all AYAs who participated in this study.
Author Disclosure Statement
The authors have no relevant financial and nonfinancial interests to disclose.
Funding Information
This article was supported by national funding from the Portuguese Foundation for Science and Technology, within a PhD scholarship to M.C.N. (
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.