
Abstract
Purpose:
Young adult cancer survivors (YACS; 18–39 years old) face ongoing physical and psychosocial sequelae. The REDEFINE study tested the feasibility of mindfulness-based stress reduction (MBSR) using a randomized design. This secondary mixed-methods analysis examined whether qualitative mindfulness reflections were associated with meaningful changes in Patient Reported Outcomes Measurement Information System (PROMIS) depression, anxiety, fatigue, and pain interference scores.
Methods:
Participants were randomized to either an 8-week MBSR course or a waitlist control group. Waitlist participants began MBSR after 16 weeks. PROMIS measures were collected at baseline and at 8, 16, 24, and 32 weeks. For these analyses, data from both groups were combined. Participants submitted written mid-course and weekly homework reflections on their mindfulness experiences. Change scores were calculated between PROMIS T-scores at the start and end of MBSR and were assessed for meaningful change. Reflections were coded using grounded theory, and a concurrent triangulation mixed-methods design integrated qualitative and quantitative data.
Results:
Among 31 participants (mean age, 32.6 ± 5.8 years; 83.9% female, White, and non-Hispanic), nearly half reported meaningful improvement in pain interference (48.3%) and fatigue (48.3%), while more than half improved in depression (51.7%) and anxiety (58.6%). Mixed-methods analysis linked improvements in pain, depression, and anxiety with reflections describing increased bodily awareness, a more positive relationship with the body, and learning mindfulness skills.
Conclusions:
MBSR-related mind-body reflections align with meaningful improvements in psychosocial and physical symptoms among YACS. Reports of bodily relaxation and emotional regulation suggest the value of combining structured and unstructured patient-reported outcomes to capture the benefits of mindfulness interventions.
Introduction
Mind-body interventions have demonstrated efficacy to support the long-term physical and emotional well-being of cancer survivors. 1 Mindfulness-based programs (MBPs), such as Mindfulness-Based Stress Reduction (MBSR), have been effective in reducing symptoms of anxiety, depression, fatigue, and sleep disturbance across cancer populations.2–4 These outcomes are often evaluated through validated patient-reported outcomes (PROs),5–7 which enable patients to share subjective feedback on the effects of mindfulness on their emotional health, quality of life, and functioning. 8
One subgroup at comparatively higher risk for chronic mental and physical health outcomes is young adult cancer survivors (YACS). 9 The disruption caused by cancer during young adulthood can lead to lasting consequences on physical, emotional, and social development.10–13 As such, stress management is critical for YACS, who often face persistent post-treatment challenges. In fact, mind-body interventions such as mindfulness have already shown great promise in addressing stress and related psychosocial and physical sequelae among this population.16–19
The Patient-Reported Outcomes Measurement Information System (PROMIS) offers measures to evaluate varying domains of physical, mental, and social health across patient populations. PROMIS measures are scored using the T-score, where a mean of 50 and a standard deviation of 10 is representative of a reference population. Published score cut points are available to characterize PROMIS scores into clinically interpretable categories (e.g., normal to severe, low risk to high risk).20,21 Several PROMIS measures also provide minimally clinically important difference score criteria to provide insight into whether a patient has experienced a meaningful change in their PRO scores over time or following an intervention. PRO measures such as PROMIS offer patients and clinicians a shared method of tracking and understanding clinical symptoms over time.
MBPs have demonstrated clinical efficacy across a wide range of outcomes in mindfulness research studies. However, in more real-world settings, validated PRO like PROMIS are not routinely used. Instead, qualitative reflections are frequently collected during weekly or mid-course journaling. To fully understand changes in PROs, it is critical to examine not only whether change occurs, but also how patients’ experiences may change in their day-to-day life. Qualitative reflections offer a rich source of patient insight that may help contextualize or offer a more nuanced clinical understanding of observed PRO changes.
The present study utilized mixed methods to link qualitative mindfulness reflections to meaningful change in PROMIS scores to better understand whether and how lived experiences of mindfulness practice reflect meaningful clinical improvement in PROs. Although not a formal mediation analysis, this study examined whether qualitatively measured changes in mindfulness-related processes may help explain observed changes in quantitative PROs. As such, we adopted a quasi-mediation or mechanism-focused framework to explore potential pathways of change. This approach not only addresses a critical gap in understanding mindfulness mechanisms but also helps pave the way for more pragmatic, scalable, and patient-centered evaluation strategies in both research and clinical practice.
Methods
Present study
Data were collected through the institutional board review (IRB)-approved study, “Reducing Emotional Distress, Enhancing Function and Improving Network Engagement in Adolescent and Young Adult Oncology” (Northwestern University IRB# STU00093614; REDEFINE-AYAO), 19 which examined the feasibility and acceptability of a waitlist-controlled MBSR intervention among a sample of YACS. Participants were recruited from an adult medical center and a children’s hospital within a large Midwestern metropolitan city. Individuals were eligible to participate if they had received a cancer diagnosis between the ages of 18 and 39 years old, were still between 18 and 39 years old, and were cognitively and physically capable of participating in an in-person MBSR program.
MBSR intervention
MBSR is a structured, 8-week training program that teaches foundational skills in mindfulness meditation practice14,22 and has been applied extensively in cancer survivor populations.2,15,23–25 MBSR is a group-based, developmentally sequenced intervention that engages participants in a 2.5-hour skill-based class each week for 8 weeks. Each weekly session incorporates a combination of mindfulness meditation practice, group discussions (e.g., mindful inquiry), and gentle Hatha yoga. Participants also attend a half-day retreat of extended practice near the end of the course to reinforce concepts learned throughout the program. In this current study, participants were also asked to submit written weekly reflections and a mid-course reflection on things they were noticing and observing about their experience learning and practicing mindfulness meditation (see Supplementary Data for example reflection prompts). The overall goal of the intervention curriculum was to foster long-term mindfulness practices and strengthen stress-management skills.
Measures
The present study is a secondary analysis of data collected at baseline and at 8 and 16 weeks postintervention from participants in both the intervention and waitlist control groups. Participants completed sociodemographic, clinical forms, and standardized PRO measures prior to randomization. PRO measures were readministered after completion of the intervention at 8, 16, 24, and 36 weeks postbaseline assessment. PROMIS short forms of Depression, Anxiety, Fatigue, and Pain Interference were analyzed in the present study because each has established interpretive cut scores for meaningful score change. Previous applications of these measures have demonstrated strong reliability and validity.26,27
Participants were also asked to complete written reflections following their assigned home practices each week. Reflection prompts were intended to help participants gain insight into their experiences, challenges, and progress throughout the MBSR intervention. A daily “Home Practice Log” prompted participants to note the date, duration, and type of practice they completed (e.g., meditation, body scan, mindful eating). Last, participants were also asked to document “what they noticed” during their home practice. Midway through the course, after a day-long retreat, participants received three take-home reflection prompts asking: (1) what stood out to them, (2) what was challenging, and (3) what was surprising about the retreat.
Data analysis
Descriptive statistics were used to summarize participants’ sociodemographic and clinical data. Prior to combining the treatment and waitlist control groups, we used independent samples t-tests to learn more about possible baseline PRO score differences. Within-person changes in PRO T-scores were calculated between baseline and immediately after completion of the MBSR course (8 weeks). Previously established meaningful change estimates were utilized to determine whether individual participants’ scores remained the same, improved, or worsened: ±2.1 T-score points for pain, ±1.9 T-score points for fatigue, ±1.8 T-score points for depression, and ±1.6 T-score points for anxiety. 28 Quantitative data analysis was conducted through IBM SPSS (Version 28; IBM Corp.).
Qualitative data collected via participants’ written homework reflections were coded using a grounded theory approach. 29 A three-person coding process (C.M., C.S., and S.P.) was used to ensure rigor and reliability. First, two coders conducted initial coding by independently reviewing a subset of transcripts. This first round of line-by-line coding resulted in a set of descriptive codes that best described participants’ experiences. This was followed by a round of focused coding to identify the most common codes and develop broader themes describing patterns within the data. Discrepancies were discussed and resolved through an iterative process of revisions. Overall, the goal of this approach was to identify patterns and themes within the data relevant to the study’s research questions. Through multiple rounds of constant comparison, coders collectively agreed upon a framework of codes and larger themes. Intercoder reliability was assessed via an Interrater Reliability Test within the Dedoose program to ensure consistency in code application. Qualitative data were analyzed using Dedoose (Version 9; SocioCultural Research Consultants, LLC), a cloud-based qualitative analysis software program.
Analyses were conceptualized as exploratory examinations of mechanisms of change rather than formal mediation models, given the study design and sample size constraints. A concurrent triangulation mixed-methods design was employed in which quantitative and qualitative data were analyzed simultaneously and independently, and then integrated during the interpretation stage. 30 This design provides an opportunity to corroborate and converge two sets of study findings, such as the relationship between changes in participants’ PRO scores and themes identified in written reflections. A code was considered “meaningful” if it was identified in the reflections of at least 10 participants who exhibited improvements in physical or mental health, as evidenced by positive changes in their PRO scores. This threshold indicates both relevance and salience of the code within the context of improved health outcomes. The threshold was specified a priori and informed by both the available sample size and the qualitative characteristics of the data.
Results
Quantitative results
Data were collected from 31 participants with a mean age of 32.6 years. The majority of participants were female (83.9%, n = 26). Most participants identified as White or Caucasian (83.9%, n = 26) and non-Hispanic or Latino (83.9%, n = 26). Approximately half of the participants were diagnosed with breast cancer (51.6%, n = 16). On average, participants were 25.4 months from their cancer diagnosis. More than half of the participants (54.8%, n = 17) received radiation treatment for their cancer, and ∼38.7% (n = 12) underwent surgery. Sample demographics are further described in Table 1.
Sample Demographics
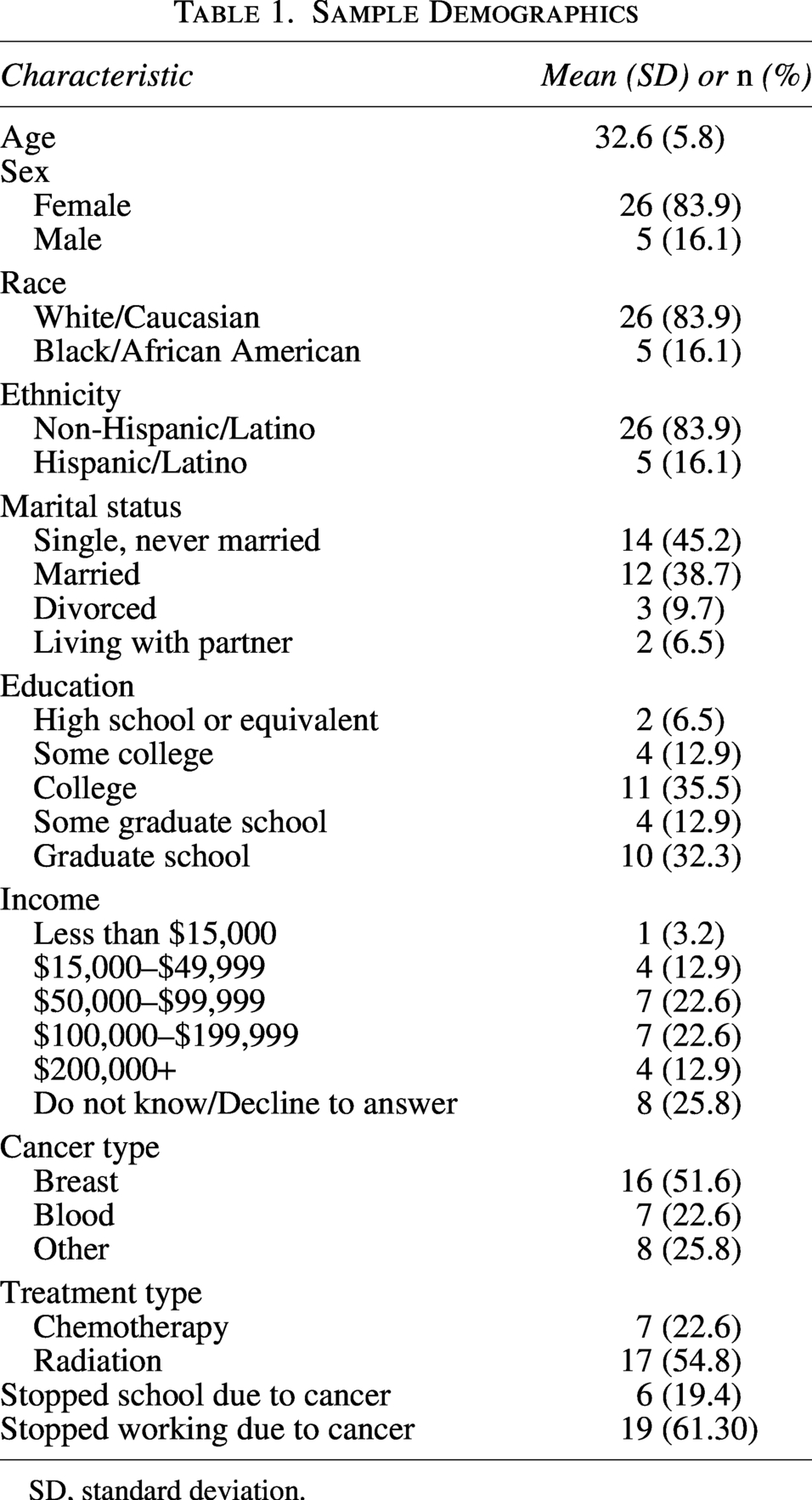
SD, standard deviation.
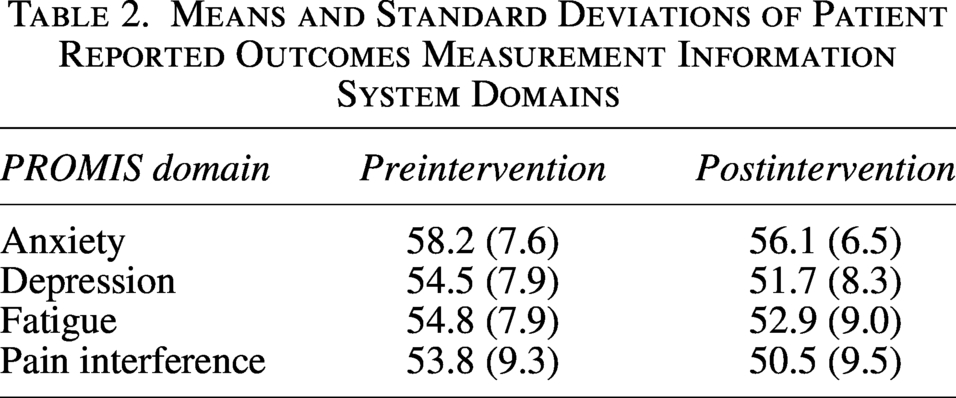
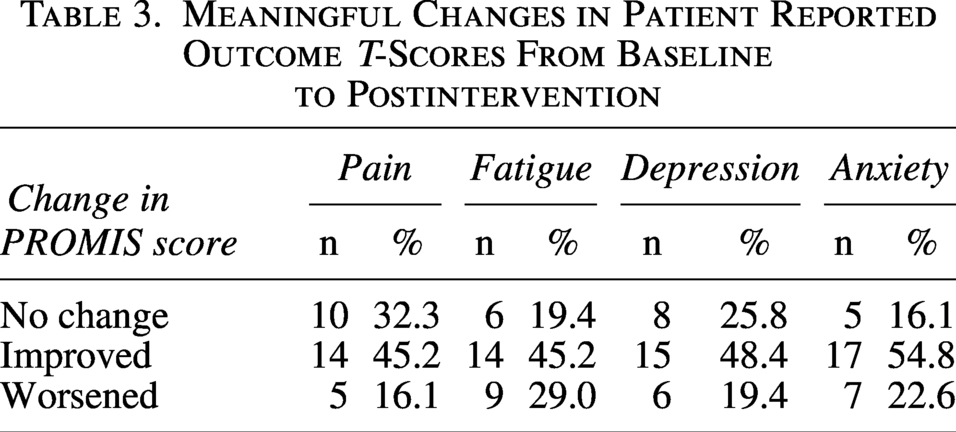
On average, participants reported decreases in all PROs after participating in the intervention (see Table 2). Based on the pre-determined meaningful change criteria, 28 we observed meaningful improvements in nearly half of the study sample across all four domains, as summarized in Table 3.
Means and Standard Deviations of Patient Reported Outcomes Measurement Information System Domains
Meaningful Changes in Patient Reported Outcome T-Scores From Baseline to Postintervention
Qualitative results
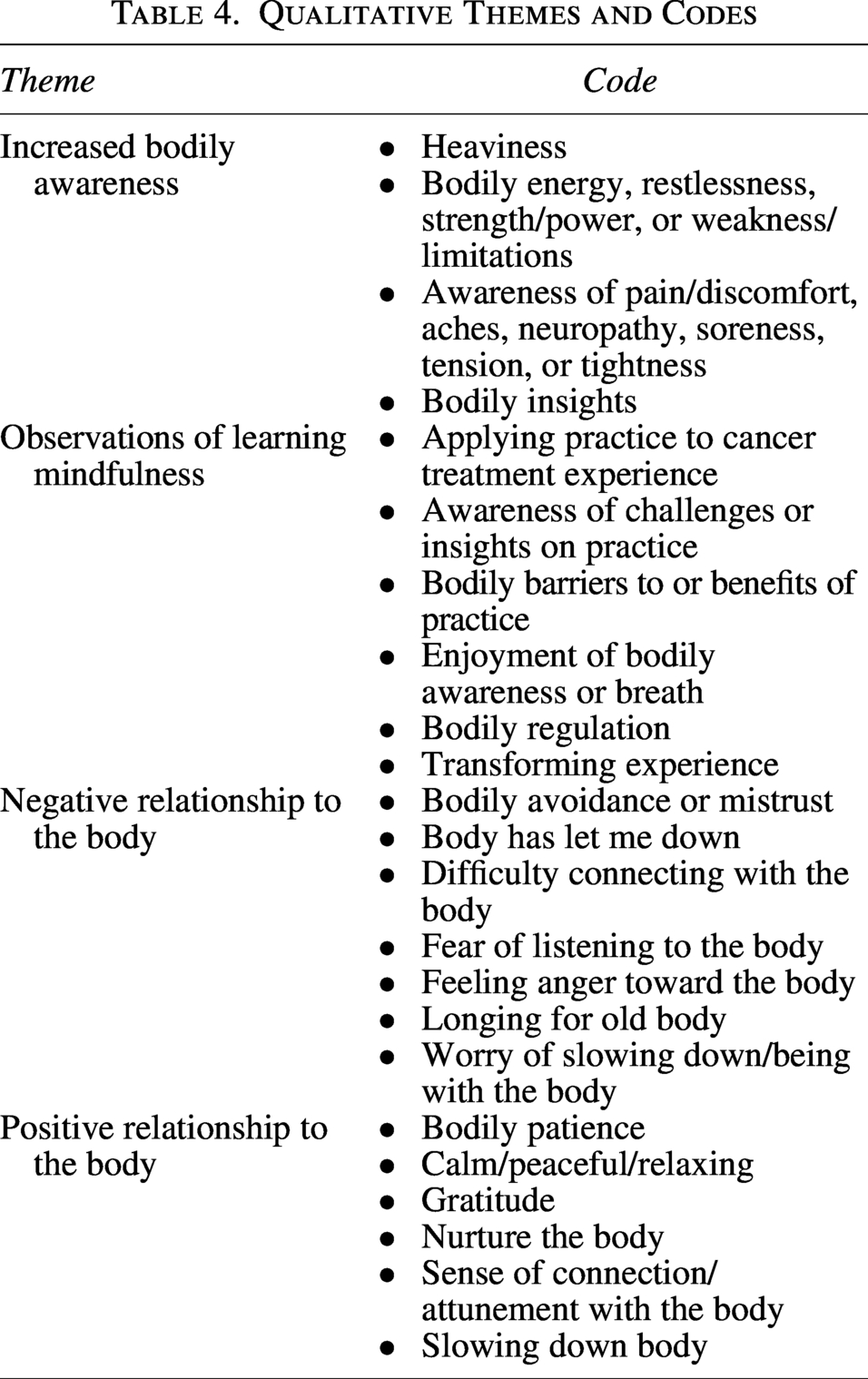
We identified 49 codes during the qualitative analyses, which were summarized into the following four themes: increased bodily awareness, negative relationship with the body, observations of learning mindfulness, and positive relationship with the body.
The theme of increased bodily awareness summarized participants’ descriptions of physical sensations they became aware of during mindfulness practice, such as heaviness, level of energy, and discomfort. For example, one participant shared that their “chest hurt during [an] exercise. Focusing on it helped [them] recognize it, not freak out, and it eventually went away.” Another participant shared they were “very focused on the lower half of [their] body. It felt like the lights turning on.”
Observations of learning mindfulness characterized participants’ acute awareness of their mindfulness practice. This includes barriers and challenges faced during mindfulness practice as well as applying practice to their cancer treatment experience. For example, a participant shared they “noticed that [their] mind wandered a lot today to thinking of other ways to help reduce stress and cancer thoughts” and “gently scolding [themself] to stay present & think about those later.”
Negative relationship to the body captured participants’ negative reflections on their own body. Excerpts within this theme included instances of bodily avoidance and mistrust, along with feelings of anger, disappointment, and worry about the current state of the body. For example, one participant shared that “it is difficult to want to know what [their body] is feeling/doing because [they are] so upset that it has let [them] down.”
Conversely, positive relationships to the body summarized participants’ positive interactions with their bodies. In one instance, a participant shared that they “feel [they are] becoming more aware of [their] body and allowing [their] self to relax.” Additional examples of codes that comprise these themes are summarized in Table 4.
Qualitative Themes and Codes
Mixed methods integration
See Table 5 for code-by-meaningful PRO improvement information. Of the 49 codes identified through qualitative analysis, seven codes met the threshold of being applied to at least 10 participants who demonstrated positive, meaningful changes in one of the four PROs—pain, fatigue, depression, or anxiety. These meaningful codes spanned three of our four qualitative themes. Within the “Increased Bodily Awareness” theme, the following codes met the threshold: different sensations, feeling tired or fatigued, and pain or discomfort. In the “Observations of Learning Mindfulness” theme, challenges in the practice, bodily benefits of practice, and transforming experience codes were found to be meaningful. Lastly, in the “Positive Relationship to the Body” theme, the calm, peaceful, or relaxing code met the meaningful threshold.
Number of Improved Participants by Qualitative Code and Patient Reported Outcomes Measurement Information System Domain
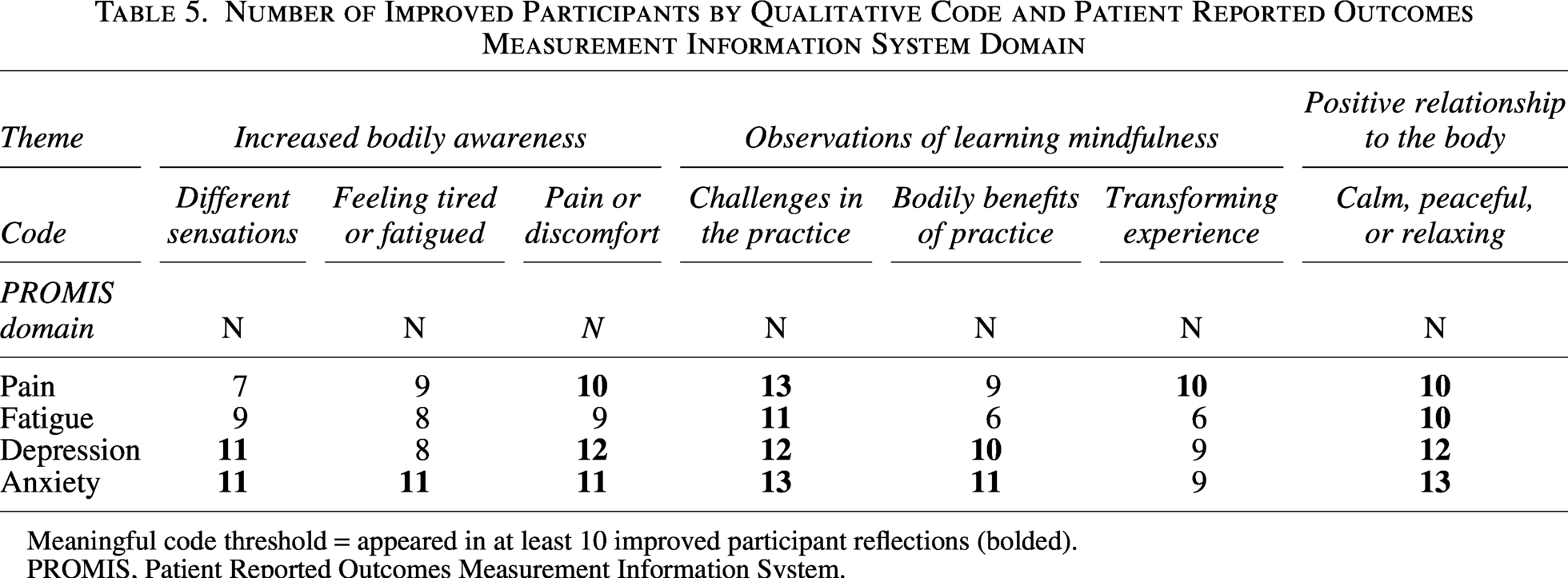
Meaningful code threshold = appeared in at least 10 improved participant reflections (bolded).
PROMIS, Patient Reported Outcomes Measurement Information System.
Reflections related to increased bodily awareness and body-based observations were meaningfully associated with multiple PROMIS domains. This can be observed by one participant who was not only aware of the physical pain they were experiencing but also used this awareness as a signal to change course. In the following quote, they share how their mindfulness practice has helped shift their anger to acceptance:
My muscles and joints really hurt today so instead of doing my planned yoga, I’m listening to my body and doing the body scan. Again, I feel peaceful, not angry at my body for hurting, more accepting that it just is.
Participant reflections also highlighted how mindfulness practice contributed to improvements in pain, fatigue, anxiety, and depression. One participant who demonstrated quantitative improvements in their pain score shared how mindfulness practice has altered their perception of pain and how they respond to it:
I’ve grown to love the body scan at the end of the day. Through it I’ve learned that not everything always hurts which was HUGE for me. I’ve also learned to recognize when things do hurt and to be okay with it instead of being pissed about it. I feel more and as a result feel less. Does that make sense?
Another participant who reported improvements in their fatigue shared how their stretching practice affected their energy levels:
The stretching felt really good. My body felt pretty good—didn’t notice any pangs. My thoughts were scattered. This relieved a lot of stress for me after work before going home. I was much more relaxed on the drive and had energy.
One participant who demonstrated improvements in depressive symptoms shared how the STOP activity helped address their emotions:
During the walk I very intentional used STOP, released negative emotions both literally and metaphorically.
The writing samples also offer insight into meaningful improvements even when such changes were not evident in quantitative measures. For example, one participant who demonstrated no change in their anxiety scores shared how their practice eased their anxious thoughts:
I found this helpful tonight as my right armpit has been sore all day, which I’m sure is nothing but I couldn’t help but worry and I felt angry. I wanted the feeling to just go away and the sitting meditation helped me get out of my head especially during the part of watching thoughts pass by. It provided relief.
Across the seven codes meeting the meaningful threshold, anxiety consistently emerged as a prominently improved domain. Each code was applied to at least 11 participants who demonstrated meaningful reductions in anxiety symptoms, except for the transforming experience code, which was applied to nine participants, nearly meeting the meaningful threshold. Meaningful codes were less frequent among participants demonstrating improvements in fatigue, with only two codes meeting the threshold. These findings suggest that meaningful improvements in anxiety appear to be more tangible in participants’ lived experiences, whereas improvements in fatigue are less so.
Two codes—challenges in the practice and calm, peaceful, or relaxing—appeared meaningful for participants across all PRO domains. Several participants described challenges encountered during mindfulness practice, yet many ultimately reported a sense of improvement despite these difficulties. For example, one participant who demonstrated improvements in both their anxiety and pain scores shared:
I feel so anxious & stressed I can’t concentrate. Breathing makes me feel less panicked. I have no energy, but I can breathe—so things can’t be that bad.
The frequency of these meaningful codes suggests that challenges during practice and the eventual calmness are common experiences among those engaging in mindfulness practice. More importantly, these experiences appear to be associated with improvements in health outcomes.
Discussion
In this study, we used a mixed methods approach to explore associations between qualitative reflections during an MBSR intervention and meaningful changes in PROMIS measures of depression, anxiety, pain interference, and fatigue.
Changes in PROMIS scores indicated that nearly half of the participants experienced clinically meaningful improvements across all four domains. Furthermore, qualitative analysis of written reflections resulted in 49 codes across four themes: increased bodily awareness, negative relationship to the body, observations of learning mindfulness, and positive relationship to the body. Mixed methods analysis revealed that several of these qualitative themes were associated with meaningful improvements in PROs. Anxiety was the most consistent PROMIS domain that was associated with meaningful qualitative codes, suggesting that mindfulness practices that cultivate awareness and acceptance of different physical sensations may be particularly helpful in reducing anxiety in this population. In contrast, fatigue was less apparent in participants’ lived experiences, suggesting that this domain may be less easily observed or articulated via narrative reflection alone. Our study sheds light on the lived experiences of YACS mindfulness learners and how their reflections aligned with meaningful PRO improvements in key outcomes of importance. Specifically, the significance of bodily-oriented themes reinforces our understanding of mindfulness’s role in repairing or reframing disrupted relationships with one’s body as a young adult survivor. This corresponds with existing qualitative evidence that YACS bodily perspectives shift as a result of the cancer experience. 31
YACS often experience mistrust, disappointment, or even a sense of disconnection from their bodies following cancer treatment. 32 Our findings suggest that mindfulness practices, such as body awareness practices and mindful movement, may provide a pathway toward greater bodily acceptance, regulation, and self-compassion—key ingredients of recovery and well-being. This dimension of mindfulness has been underexplored in YACS populations and presents an opportunity for exploration of more targeted, body-focused adaptations of MBPs in future research and clinical care.
This study also addresses a notable methodological gap. While the collection and analysis of qualitative data in mindfulness-based intervention trials has historically been considered resource-intensive and time-consuming, in real-world MBPs, participants often share weekly narrative reflections using structured and unstructured journal prompts. Through triangulating these reflections with validated PRO data, we demonstrate the value of integrated qualitative insights to help explain, deepen, and personalize quantitative findings. This integration provides a model for patient-centered, pragmatic evaluation strategies that could be scaled in both research and clinical settings.
Our study had some limitations. Firstly, change scores have known psychometric limitations, including reduced reliability relative to measurements obtained at individual time points. 33 As a result, the observed changes may have been partially influenced by measurement error rather than true change, which could inflate estimates and limit generalizability. Furthermore, this was a secondary analysis of a small, geographically homogenous sample of mostly White, non-Hispanic female participants, with a high preponderance of breast cancer patients. Although our coding process was rigorous with high intercoder reliability, the interpretive nature of qualitative and mixed methods analyses can only provide a subjective starting point from which to continue to explore these patterns and associations versus causal explanations.
Our findings suggest that certain MBSR-influenced written reflections may represent key mechanisms through which meaningful improvements in PROs occur. Although we did not conduct a formal mediation analysis, the observed patterns are consistent with a quasi-mediation framework in which engagement with mindfulness practices contributes to downstream changes in psychosocial and physical outcomes. However, given the observational nature of these analyses, we cannot establish causal directionality. Future studies using longitudinal or experimental mediation designs are needed to more rigorously test these mechanisms. Nonetheless, our study demonstrates the utility of unstructured qualitative reflections in providing context and deeper insight into the patient experiences underlying observed statistical trends.
While mechanistic evidence suggests that interoception and embodied awareness may represent important pathways through which mindfulness exerts its distress-reducing effects, 34 to our knowledge, specific body-focused components of MBIs (e.g., body scan, mindful movement) have not been studied in isolation in cancer-specific trials despite their centrality to these programs.15,25,35 Our findings suggest that bodily awareness may be a particularly salient mechanism, especially for anxiety and pain, through its role in enhancing self-regulation and reshaping patients’ relationships with their bodies. While unlikely to function as a singular “active ingredient,” this dimension of mindfulness may represent a tractable therapeutic target. Future research should test these pathways using longitudinal or experimental designs, and the integration of brief qualitative reflections alongside PROs may offer a pragmatic strategy for capturing these processes in real-world care. Our findings highlight how qualitative reflections offer a window into the lived processes of change during mindfulness practice and point toward bodily awareness and self-regulation as promising therapeutic targets. With the rise of artificial intelligence technologies, such as natural language processing, the examination of unstructured PROs has become more accessible than in the past. As such, opportunities to examine meaningful changes in qualitative PROs are ripe for investigation.
As patient-centered care moves toward integrating both structured and unstructured data, approaches such as ours may offer scalable strategies for tailoring mindfulness interventions to meet the needs of diverse survivor populations. The present study illustrates the potential of qualitative insights into routine care, which may provide clinicians with a deeper understanding of patients’ needs and offer opportunities for more individualized and responsive care plans for YACS.
Authors’ Contributions
K.L.: Writing—original draft and review and editing and visualization. C.S.: Formal analysis, writing—original draft, and data curation. S.P.: Formal analysis, writing—original draft, and data curation. C.M.: Writing—review and editing. B.H.: Project administration and writing—review and editing. S.S.: Funding acquisition and writing—review and editing. D.V.: Conceptualization, methodology, writing—original draft and review and editing, and funding acquisition.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
K.L. was supported by the National Cancer Institute (grant no. T32CA193193). This work was supported by the
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.