
Abstract
Objective:
Adolescents and young adults (AYAs) with cancer face unique developmental, psychosocial, and care transition challenges between pediatric and adult oncology systems. Multidisciplinary team (MDT) approaches are promoted to address these complex needs; however, collaboration, implementation, and impact on AYA care remain inconsistently described in the literature. This systematic review synthesizes evidence on how MDTs are organized, enacted, and experienced in AYA oncology care and examines implications for patient-centered, developmentally appropriate care.
Methods:
Following Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines, a search of CINAHL, PsycINFO, and PubMed was conducted for studies published between January 2000 and March 2025. Eligible studies were peer-reviewed articles in English involving participants aged 15–39 years with cancer who addressed survivorship and multidisciplinary teamwork. Of 1048 screened records, 15 studies met the inclusion criteria and were included in the synthesis.
Results:
Four overarching themes were identified: (1) core elements of effective MDT collaboration, including flexible professional roles, MDT communication, and shared decision-making with AYAs; (2) addressing the unique psychosocial and developmental needs of AYAs, supporting care coordination, and psychosocial support; (3) implementation and functions of MDTs across the AYA cancer care continuum, facilitating smoother transitions between pediatric and adult services; and (4) the impact of MDT care on patient outcomes, including improved adherence to follow-up care and enhanced psychosocial well-being.
Conclusion:
Evidence shows MDTs function as relational processes shaping AYA cancer care quality, not just organizational structures. Effective MDTs emphasize patient-centered collaboration and multidisciplinary trust across the cancer trajectory. Future research should evaluate how MDT processes influence clinical, psychosocial, and survivorship outcomes for AYA.
Introduction
In the United States, approximately 89,000 adolescents and young adults (AYA) are diagnosed with cancer annually, and approximately 9270 AYA cancer-related deaths were reported nationwide. 1 AYA patients are 15–39 years old at the time of cancer diagnosis, 2 which poses unique health care considerations because of their physical and psychological developmental stages. Cancer treatment during this period can disrupt the developmental milestones of some participants.3,4 AYA patients have reported concerns about infertility and financial burdens.5,6 Additionally, 50% of AYA cancer patients experience significant psychological distress, which can hinder coping with cancer. 7 In particular, AYA patients undergoing treatment require care in several domains, including psychological, physical, daily living, and sexual. 8 Addressing the symptoms and needs of AYA patients requires a multidisciplinary effort because of their unique needs.
Following Tannenbaum and Salas, a team can be defined as “two or more people who interact with one another in situations where at least some members rely on other team members, share a common or overlapping sense of purpose or goals, and are viewed as a unit by others and/or themselves” (p. 5). 9 Similarly, in clinical settings, teamwork requires decision-making, the performance of interdependent tasks, and a common goal. 10 Multidisciplinary teams (MDT) may include physicians, nurses, social workers, psychologists, and other specialists. 11 AYA patients are at the center of the cancer care team, and the quality of care depends on interprofessional care aligned with their needs, values, and preferences. 12 This is particularly important because AYA patients desire treatment decisions that consider their developmental goals, such as education, family planning, career development, and employment. 13 Furthermore, multidisciplinary models emphasize patient-centered care by positioning patients at the center of care, with health care professionals coordinating their needs. 14 Accordingly, MDT team members must not only coordinate internally but also collaborate with patients and their other care providers, including primary care providers, to ensure continuity and coherence of care. 15 Therefore, MDT team members must coordinate with each other and the patient’s other care providers, such as primary care providers. 15
Some cancer centers have adopted MDT for AYA cancer care because of its benefits. In particular, collaborative, team-based care models have been shown to improve follow-up engagement and care coordination among cancer survivors. These approaches may also enhance trust in health care providers and support patient-centered education, which is particularly relevant for AYA patients. 16 Integrating a program within the existing team fosters collaboration and communication between pediatric and adult oncology teams, leading to enhancements in supportive care, psychological consultations, reproductive endocrinology, and fertility preservation. 17 Concurrently, a study involving AYA cancer patients from multiple hospitals highlighted the importance of emotional and social resources, nutrition, and exercise in augmenting current oncology team services. 18
Although MDT has been shown to improve outcomes for cancer patients in general, existing care models do not always adequately address the complex and multifaceted needs of AYA patients, which require a more comprehensive and coordinated multidisciplinary approach. 8 Therefore, a systematic examination of how MDTs are utilized in AYA cancer care is needed to identify current gaps and areas for improvement in the care provided. Accordingly, this systematic review aimed to investigate the use of MDTs in providing care for AYA with cancer.
Materials and Methods
Design
Search strategy
The search for relevant literature followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 19 The first author (H.S.) conducted a search using three electronic databases, the Cumulative Index to Nursing and Allied Health Literature, PsycINFO, and PubMed, from January 1, 2000, to March 31, 2025. Additional articles were identified through a library search. The search terms used individually or in combination were teamwork, cancer patients, adolescents, teenagers, young adults, cancer survivors, and MDTs.
The inclusion criteria for articles were as follows: Original empirical studies published in peer-reviewed journals in English; studies including participants aged 15–39 years with a diagnosis of cancer based on the National Cancer Institute’s definition of AYA with cancer 2 ; studies in which participants met a broad definition of survivorship from diagnosis to completion of cancer treatment; and studies that documented any aspect of MDT by health care professionals in outpatient, inpatient, or community settings. Studies were excluded if they were pilot studies, review papers, or publications focused on topics other than MDT, such as a concept paper on MDT or the development of a teamwork program without reporting teamwork outcomes.
A PRISMA flowchart 19 depicting the search strategy used to identify the articles for this review is presented in Figure 1. The search yielded 1048 articles: 171 from CINAHL, 737 from PubMed, 138 from PsycINFO, and 2 from ProQuest. After removing duplicate articles (n = 134), we reviewed the titles of 914 articles to ensure that they met the inclusion criteria. For titles that required clarification, we examined their abstracts, resulting in the exclusion of an additional 153 articles. We also reviewed the papers that were excluded to ensure that no pertinent study was overlooked. The remaining 46 articles underwent full examination, and 31 were excluded for several reasons, including not focusing on MDT (n = 24), not involving AYA patients (n = 3), being review papers (n = 3), or being pilot studies (n = 1). Ultimately, 15 articles were selected for this review. The first author (H.S.) conducted a thorough search of articles in various databases. The identified articles were thoroughly reviewed to ensure that there were no duplicates. A.K. and H.S. independently assessed the relevance of the articles based on the specified exclusion or inclusion criteria by screening the titles and abstracts. In the event of a disagreement, H.S. facilitated discussions to reach a final decision. All authors independently conducted a comprehensive examination of the full texts of the selected articles. Any disagreements among the authors were openly discussed to ensure a thorough and unbiased screening process.
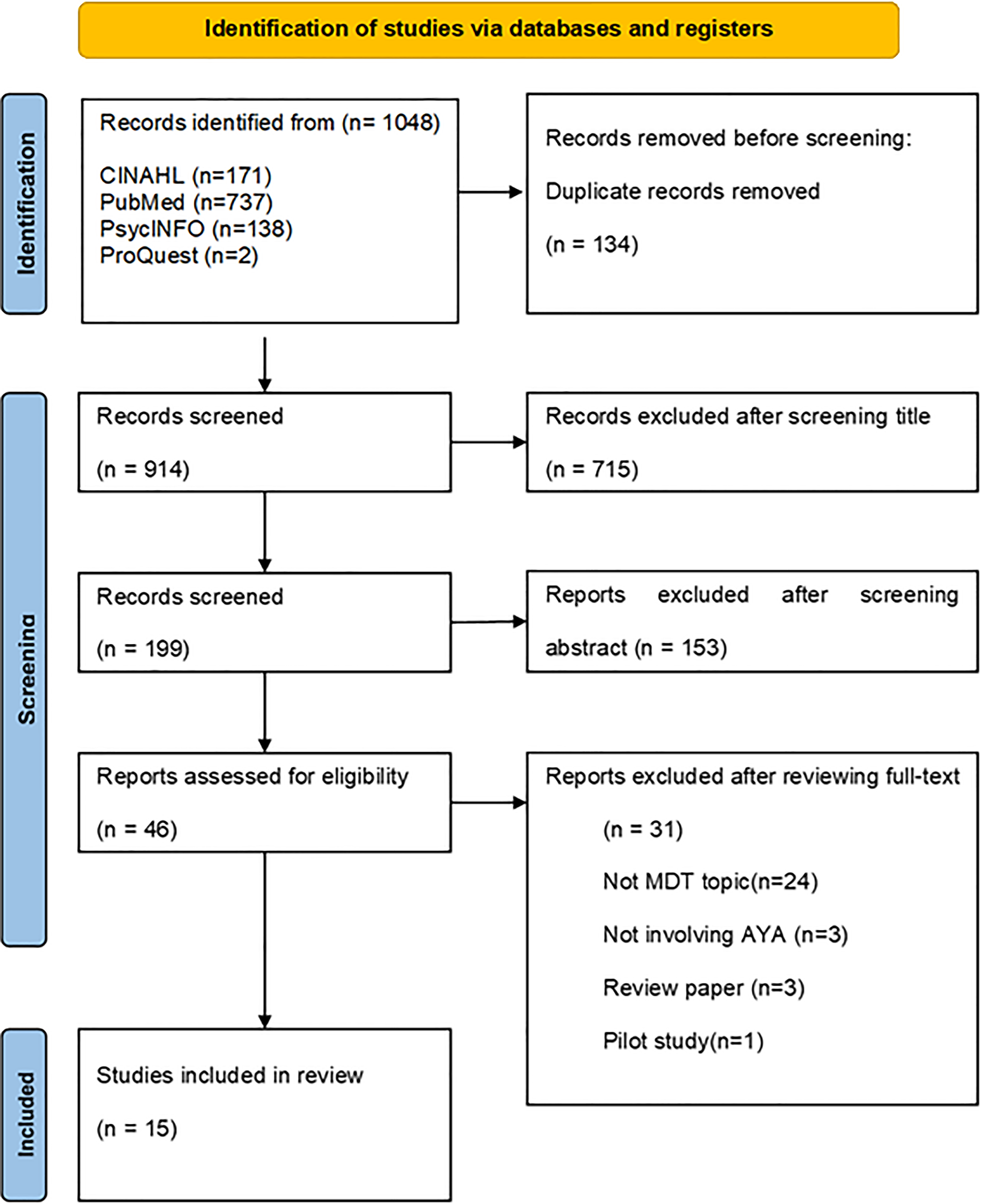
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 flow diagram for systematic reviews.
Quality appraisal
The selected articles were critically appraised individually by two authors (H.S. and A.K.) using the Mixed Methods Appraisal Tool (MMAT). 20 This tool is designed to assess the methodological quality of systematic reviews containing various research types, including qualitative, quantitative, and mixed-methods studies. The MMAT rated the quality of the methodology, including whether the research approach was appropriate to answer the research question, the adequacy of the findings derived from the data, the correctness of the interpretation of the results, the representativeness of the target population, and the appropriateness of the measurements and statistical analysis. Each article was scored 0%, 25%, 50%, 75%, or 100% based on the number of assessment items it addressed. Table 1 presents the quality scores for each study. The two authors compared the results (H.S. and A.K.), and the rate of agreement was 92% (four items out of 50 items had disagreements). Any discrepancies were discussed by the three authors (H.S., A.K., and J.C.G.) to resolve them. No articles were excluded due to poor quality based on the MMAT guidelines, which helped reduce bias and random and systematic errors. 31 The risk-of-bias assessment, as summarized in Table 1, revealed that 10 articles had a perfect score of 100%. Additionally, four articles scored 75%, and one article scored 50%. Despite not achieving perfect scores, these five articles were included because of the significance of their findings.
Summary of Evidence of Teamwork (n = 14)
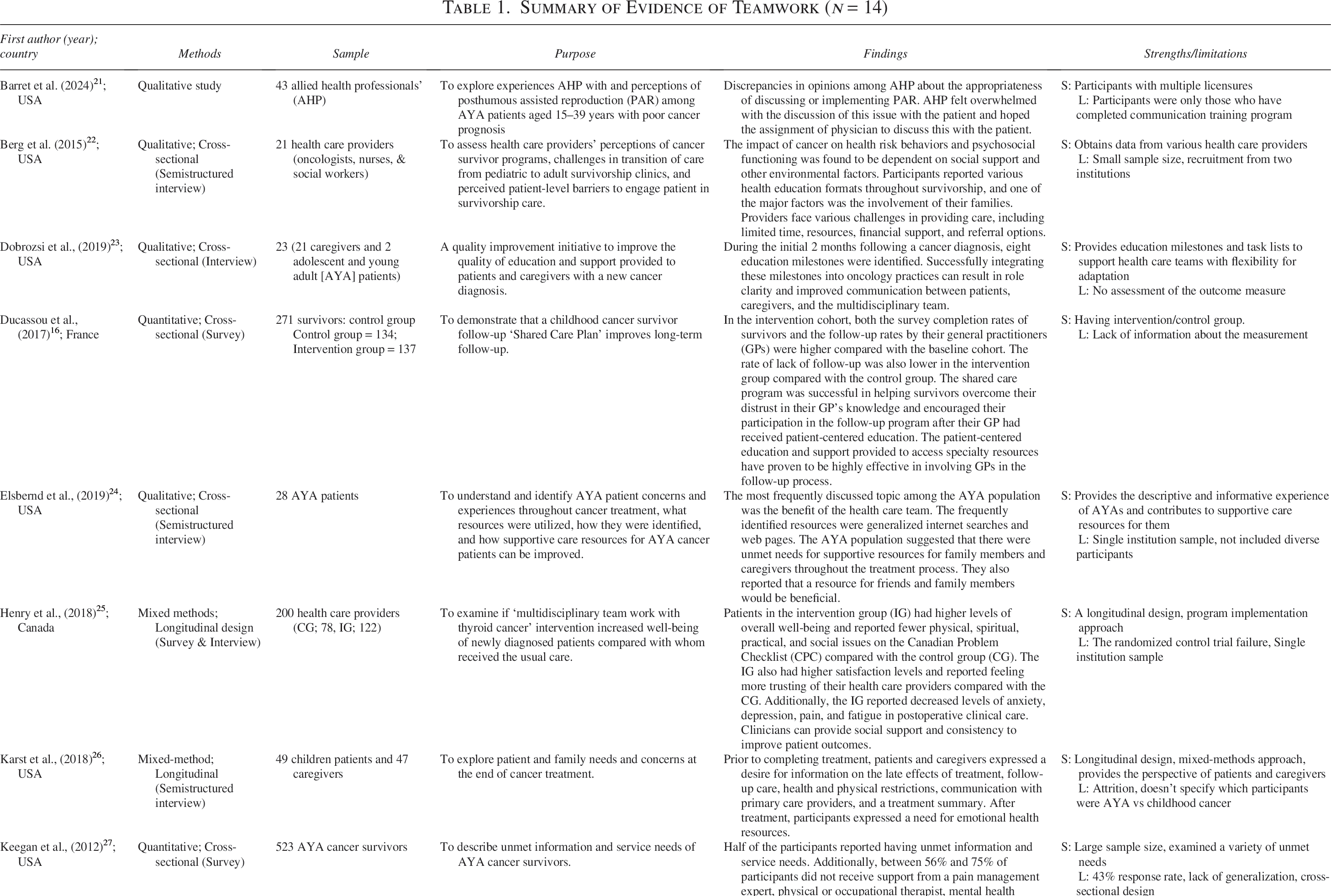
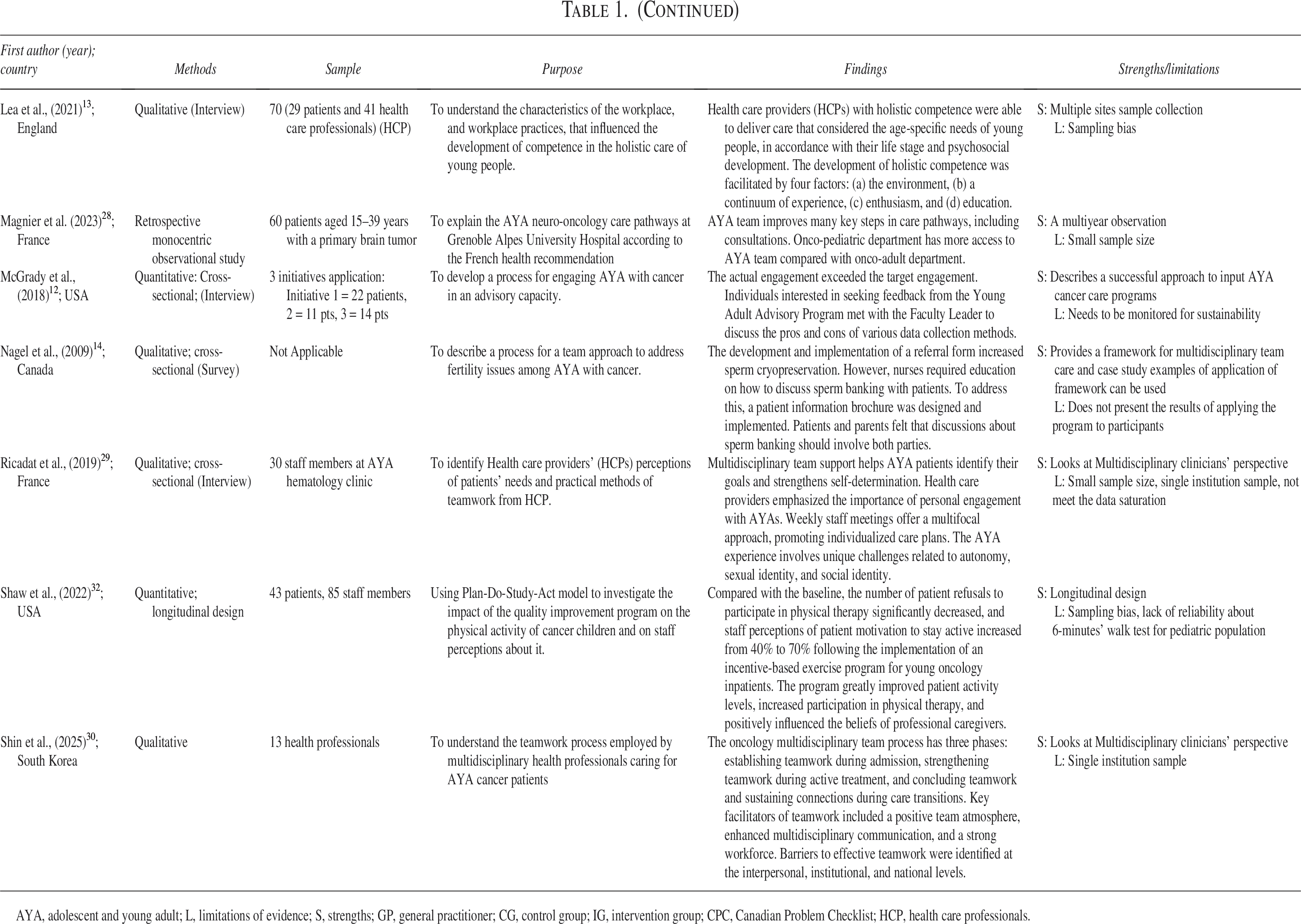
AYA, adolescent and young adult; L, limitations of evidence; S, strengths; GP, general practitioner; CG, control group; IG, intervention group; CPC, Canadian Problem Checklist; HCP, health care professionals.
Data extraction
Data extraction was conducted in parallel with the quality assessment. A comprehensive data extraction process was undertaken, encompassing quantitative and qualitative findings that were compiled into an Excel file. To ensure accuracy and consistency, the data extraction protocol was initially piloted with two articles, allowing for adjustments to achieve the most suitable format. The form recorded important study characteristics such as author, year, method, purpose, sampling, findings, strengths, and limitations. Table 1 presents the data extraction details.
Data synthesis
The findings from the qualitative, quantitative, and mixed-methods studies were synthesized using a structured data extraction table (Table 1). To facilitate integrated analysis, quantitative findings were transformed into narrative forms to ensure coherence and conceptual comparability with qualitative results. Rather than reproducing all original participant quotations verbatim, the qualitative findings were synthesized across the studies into integrated analytic summaries.
The synthesized data were examined iteratively to identify patterns of shared meaning and develop higher-order themes. Theme development was refined through ongoing discussions between the two researchers, with interpretive differences resolved through consensus, consistent with the principles of reflexive thematic analysis. 7 Detailed analytic notes and preliminary themes were subsequently reviewed and discussed with a third author, leading to an agreement on the final thematic structure.
Results
Characteristics of selected studies
Table 1 summarizes the 15 articles included in this systematic review. All articles were published between 2009 and 2025. The studies were conducted in different countries; eight were conducted in the United States,12,21–24,26,27,32 three were conducted in France,16,28,29 two were conducted in Canada,14,25 one was conducted in England, 13 and one was conducted in Korea. 30 The research approaches used varied; nine studies used a qualitative approach,13,14,21–24,29,31 four used a quantitative approach,12,16,27,32 and two used a mixed-methods approach.25,26 The sample sizes of the selected articles ranged from 21 to 523. The participants included health care providers for AYA with cancer,14,21,22,29,30,32 AYA with cancer undergoing treatment, survivors of AYA or childhood cancer,12,13,16,23,25,27,32 and AYA with cancer and caregivers.14,23,26,28
We assessed the risk of bias in each study using the MMAT; full details are presented in Table 2. The strengths and limitations of each study are presented in Table 1. Four considerations relevant to this review emerged: (1) effective MDTs rely on clear roles, communication, and shared decision-making; (2) the unique needs of AYA with cancer are addressed by MDTs; (3) MDT care improves coordination and psychosocial support; and (4) a single MDT is insufficient across the cancer continuum.
Risk-of-Bias Assessment Using MMAT

Y: yes; N: no; ?: Can’t tell.
MMAT, Mixed Methods Appraisal Tool.
Core elements of effective MDT
In this review, the core elements of MDT consist of the approach to care and personnel within the MDT. Seven of the 15 reviewed articles described MDT activities,12–14,16,23,25,30 whereas the remaining eight referenced team-based care without providing details of team endeavors.21,22,24,26–29,32 Three articles reported unique care delivery processes for patients with AYA. One approach involved a nurse coordinator who liaised between two separate cancer care teams, one consisting of physicians (surgery, endocrinology, and nuclear medicine), and the other consisting of other health care providers (dieticians, pharmacists, social workers, psychologists, and volunteer community support). 25 Another approach involves the adult and pediatric oncology ward in collaboration with an AYA team. 28
The specialties of MDT members who participated in AYA care or were deemed important varied between articles, with teams consisting of 2–13 different specialties. One article did not specify the disciplines included in the MDT, beyond noting that nurses played a central role in AYA care. 13 The most cited team members in relation to AYA care were physicians, with specialties such as oncology, endocrinology, reproductive endocrinology, surgery, nuclear medicine, general practice, palliative care, pain management, integrative medicine, and psychiatry included on MDT.12,14,16,22,23,25,27–30,32 Nurses and social workers are also important members of the MDT.13,14,16,22,23,25,27,29,30,32 Nutrition/dietetics12,22,23,25,27,32 and psychology12,22,23,25,27,32 were included in six MDTs each. Other specialties were included in three MDTs (physical therapy, occupational therapy, and community workers), two MDTs (pharmacy, spiritual care, child life specialists, and AYA patients), or one MDT (caregivers, nurse practitioners, kinesiologists, and ward aides) in the articles reviewed.12,21,23,25,27,29,32
In AYA care, physicians are frequently identified as key team members because they play a central role in determining treatment direction. Previous studies have consistently shown that physicians are responsible for clinical decision-making and often lead MDTs in oncology care. 33 However, physician-led team leadership may have limitations. Clinical decision-making may be overly focused on the biomedical aspects of care, with comparatively less attention to patients’ psychosocial needs. 33 In addition, when physicians assume responsibility for team coordination, collaboration, and resolution of technical or organizational issues, the time available for direct patient care may be reduced. 33
Therefore, to support patient-centered treatment decision-making, the involvement of a core professional who can complement the physician’s role is essential. Nurses are well positioned to fulfill this function by coordinating team members, facilitating role clarification, and ensuring that treatment and nursing care plans are consistently implemented in daily practice. Through their continuous presence in clinical settings, nurses can provide ongoing support to AYA patients and help integrate the medical and psychosocial aspects of care. 13 The findings of this study suggest that while the composition of a MDT is important, effective team functioning also requires a professional who actively guides and supports the team’s processes and day-to-day operations.
This multidisciplinary partnership consisted of a dedicated pediatric oncologist and an oncology nurse at a cancer center, and general practitioners in the community, in a model of shared follow-up care. 16 The role of each member of the MDTs varied among articles, with some emphasizing clearly defined roles, 23 while others focused on flexibility to achieve MDT goals. 29 Additionally, team organization varied, with some MDTs led by psychologists or oncologists, 16 depending on the team’s specific focus. 12
The unique psychosocial and developmental needs of AYAs addressed by MDTs
AYAs with cancer have unique psychosocial needs due to their developmental stage.13,22,29 Although most of the reviewed articles recognized these needs, only one MDT provided specific examples of how they addressed them. This team focused on balancing AYA’s need for independence with the family’s need to be involved in care, taking an individualized approach for each patient. 29 For instance, they did not automatically provide an extra bed for a family member to stay with the patient in the hospital room, as is common in pediatric wards. They also allowed AYA patients to make decisions about elective treatments, giving them a sense of control and independence while still considering the role of the family in care decisions. 29
Another issue related to the developmental stage is fertility preservation, as highlighted in four studies. One MDT recognized the AYA’s developmental stage related to body image and sexual identity and matched the gender of the team member involved in fertility preservation to the AYA’s preference. 29 Another MDT developed a comprehensive program for fertility preservation in AYA males with cancer, 14 while a third provided education on the impact of cancer treatment on fertility and options for fertility preservation for patients and caregivers. 23 The fourth is a personalized support program for AYA patients that may include fertility preservation, if indicated. 28
MDT members also acknowledged the need for social connections among AYA with cancer. Social workers on the team facilitated the maintenance of professional activities at work24,29 and social and academic ties with schools. 24 The MDT facilitated group activities for those currently in the hospital, extended hospital visiting hours to accommodate AYA preferences for later nights, and had the team nurse facilitate discharge when the team identified a patient who struggled with social isolation. 29 MDT members emphasized the need for AYA patients with cancer to receive specialized and holistic care in units dedicated to the AYA population during the treatment phase of their illness. If such units are unavailable, health care providers should receive regular training on the unique needs of AYA, and a “nurse champion” should be embedded in these units to advocate for AYA patients’ holistic care and raise awareness of their unique developmental, psychosocial, and supportive care needs. 13
Implementation and functions of MDTs
The care continuum for AYA cancer patients includes various phases, such as prediagnosis examination and testing, diagnosis, treatment, transition off treatment, and survivorship or palliation. However, the focus of the MDT varied among the teams in different studies, and some teams worked toward more than one purpose.
Most articles emphasized the treatment period,12–14,21,23–25,28–30,32 while four articles focused on survival.12,16,22,27 The diagnosis period was addressed in only two articles,23,25 and the transition to survivorship was mentioned in only one. 26 The diagnosis period was addressed in only two articles,23,25 and the transition to survivorship was mentioned in only one article. 26 None of the studies focused on the prediagnosis or palliation periods. Among the reviewed articles, two reported need assessments. One study conducted a needs assessment with AYA cancer patients to identify their needs during and after treatment at a children’s hospital. 12 Another article discussed an MDT that assessed oncology nurses’ knowledge of fertility preservation options for AYA patients. 14 Additionally, one MDT concentrated on enhancing AYA patient involvement in developing clinical projects related to their care and successfully implemented online strategies to create an AYA advisory board for the hospital. 12
Three MDTs focused on education, developing a coordinated and structured patient education program for the first 2 months after cancer diagnosis, 23 an educational video for patients, 12 educational materials, and a standardized dissemination process related to fertility preservation for male AYA with cancer, along with training for oncology staff members on the materials and process. 14 Another MDT focused on long-term survivorship follow-up among childhood and adolescent cancer survivors. 16 Finally, MDT activities focused on meeting the unique developmental and psychosocial needs of AYA with cancer.13,30
The MDT process in providing continuum care for AYA populations includes key components, such as effective communication and cooperation among health care team members to maintain a working relationship,24,30 open-mindedness, flexibility, trust among team members, 29 and regular scheduled meetings,16,23,25,29,30 which allowed for the development of flexible, individualized care plans for patients. 29 AYA patients and survivors valued clear, developmentally appropriate communication from MDTs and found miscommunication among team members confusing and burdensome. 24
Impact of MDT care on patient outcomes
Among the studies reviewed, MDT was found to be effective in improving patient adherence to follow-up care, 25 addressing concerns regarding care, supporting individual identity formation and self-determination of care plans,29,30 and promoting physical activity among cancer inpatients.16,32 The personalized and comprehensive guide provided by MDT improved survivors’ adherence to follow-up care and led to higher levels of overall well-being and care satisfaction scores and lower levels of psychological distress, fatigue, and pain compared with usual care. 25 Effective communication between oncology care providers and patients leads to decreased distress in AYA patients and their caregivers. 26 MDT was also effective in addressing fertility preservation, 21 although its impact has not been reported. 14 The collaboration of the oncology team in the ward and AYA team also improved supportive care and increased access to consultations for fertility.28,30
Critique of selected studies
The articles included in this review employed various methodologies, ranging from longitudinal to cross-sectional designs. Longitudinal studies have captured changes in AYA patients as they progress through different developmental stages,25,26 whereas cross-sectional studies have provided a snapshot of the data at a single point in time.12,27 The studies also included a diverse range of participants, including health care providers, AYA cancer patients, and their caregivers, which allowed for a comprehensive examination of the topic from multiple perspectives.22,26,29,30 However, a limitation of these studies was the small sample size and lack of diversity in some samples.14,22,24,25,30 In addition, several studies have examined only health care provider perspectives,8,14,23,29,30,32 while fewer have included the perspectives of AYA patients themselves or their caregivers, which limits the extent to which the findings reflect the patient experience of MDT care. In addition, some of the included studies may not fully align with the defined AYA cancer population. For example, one study focused on survivors who were diagnosed with cancer during childhood, 27 and another reported a mean age of 9 years (SD = 6), 21 indicating that a substantial proportion of participants were diagnosed with cancer at an age younger than the AYA age range. This variation in the study population may limit the comparability of the findings across studies. However,although the MMAT provided a structured appraisal of methodological quality, it may not fully capture other important aspects of the studies, such as the depth with which the research questions were addressed or the reporting of ethical considerations.
Discussion
This systematic review examines the use of multidisciplinary teamwork among health care providers in caring for AYA patients with cancer. The review included 15 articles, of which seven described the activities of the MDT, and the remaining eight did not provide details of team endeavors. Studies that reported the outcomes of MDT care demonstrated positive impacts on AYA cancer care and improved outcomes, similar to the findings in a previous systematic review 34 and a retrospective cohort study of MDT in adult cancer patients. 35 Four main themes were identified: first, the core elements of effective MDT collaboration; second, the specific psychosocial and developmental needs of AYAs that MDTs address; third, the implementation and functions of MDTs; and last, the effect of MDT care on patient outcomes.
Each MDT varied in its purpose and activities, or the recommended team activities. Few studies have focused on meeting the specific complex psychosocial needs of AYA patients with cancer, such as fertility preservation, exploring independence from their family of origin, and the need for social support from their peers.23,29 Best AYA cancer care practices suggest that AYA programs should be patient-centered 36 and personalized, 28 acknowledge each patient’s level of autonomy and maturity, 37 promote normalcy, 3 and empower them to achieve typical developmental milestones. 6 The National Academy of Medicine, 38 known as the Institute of Medicine until 2015, and the American Society of Clinical Oncology 39 both advocate for team-based cancer care throughout the cancer trajectory, from asymptomatic screening or symptomatic testing through to survivorship or end-of-life care. A holistic approach includes improved coordination of care among the multidisciplinary workforce caring for patients with cancer. Effective survivorship care to improve the quality of care and reduce care costs requires collaboration and coordination of care between primary care clinicians and specialists. 38
Although some studies have noted internal team processes contributing to MDT success, no studies have comprehensively covered all components of successful teamwork, and no studies have reviewed the use of a team framework in MDT implementation. However, one study proposed a health pathway with consideration of medico-psychosocial factors for AYA with brain tumors, 28 and this still needs to be examined. Therefore, frameworks such as the Cancer Care Team framework proposed by the Institute of Medicine, 38 the care coordination framework for facilitating teamwork in AYA oncology discussed in Johnson et al., 5 and the principles of teamwork specified by the NCI-ASCO teams in cancer care initiative 39 should be employed when designing MDT for the care of AYA with cancer. Future reports on MDT for AYA with cancer should include details on team processes.
The disciplines comprising MDT varied; however, they typically included physicians, social workers, and nurses. Additional specialists, such as fertility, psychologists, and child life specialists, should be included in teams for AYA with cancer to address both medical and psychosocial needs. The new ASCO clinical practice guideline for oncology care highlights the importance of noncancer care providers and caregivers as integral members of cancer care teams, 39 but only two reviewed articles included primary care physicians on the MDT,16,30 and none included caregivers as members of the MDT.
Owing to the length of cancer care and the diverse needs of AYA patients in different phases of care, it is challenging for a single MDT to address all the procedures during assessment, diagnosis, treatment, transition, and palliative care, while also considering their developmental stage. The European Society for Medical Oncology and the European Society for Pediatric Oncology recommend a coordinated, multidisciplinary approach to care led by a professional from a nonmedical discipline, such as psychology, allied health, social work, or education. 40 One study reviewed the implementation of such an approach by placing a nurse as a liaison between two separate teams, one comprising physicians and the other comprising allied health professionals. 25 Another potential approach is to utilize oncology nurse navigators who could act as team leaders or liaisons between each MDT for each phase of care. 30 The Oncology Nursing Society advocates for the involvement of nurse navigators in all phases of cancer care. 36 A careful handoff between nurse navigators for each phase of care could ensure smooth coordination of care without overburdening team members. These innovative approaches could be implemented in a coordinated manner to provide efficient and effective care across the cancer continuum.
Table 3 presents the key takeaways and future directions derived from the cross-study synthesis. Overall, the reviewed articles demonstrated the positive impact of MDT care for AYAs with cancer; however, MDT efforts remained fragmented across different phases of the cancer care continuum. Beyond the absence of a standardized MDT framework, such fragmentation may partly reflect the decentralized and patchwork nature of the health care system in the United States, which consists of a mix of for-profit and nonprofit, public, and private organizations. 41 Therefore, limited structural incentives may exist to support sustained investment of time and resources for implementing MDT-based care for AYAs with cancer in the United States. 38 Interestingly, the two reviewed studies that examined novel MDT care delivery models for cancer care16,25 were both conducted in countries with universal health care systems, suggesting that broader system-level support may facilitate more integrated MDT implementation. 41
Cross-Study Key Findings by Major Themes in MDT Care for AYAs
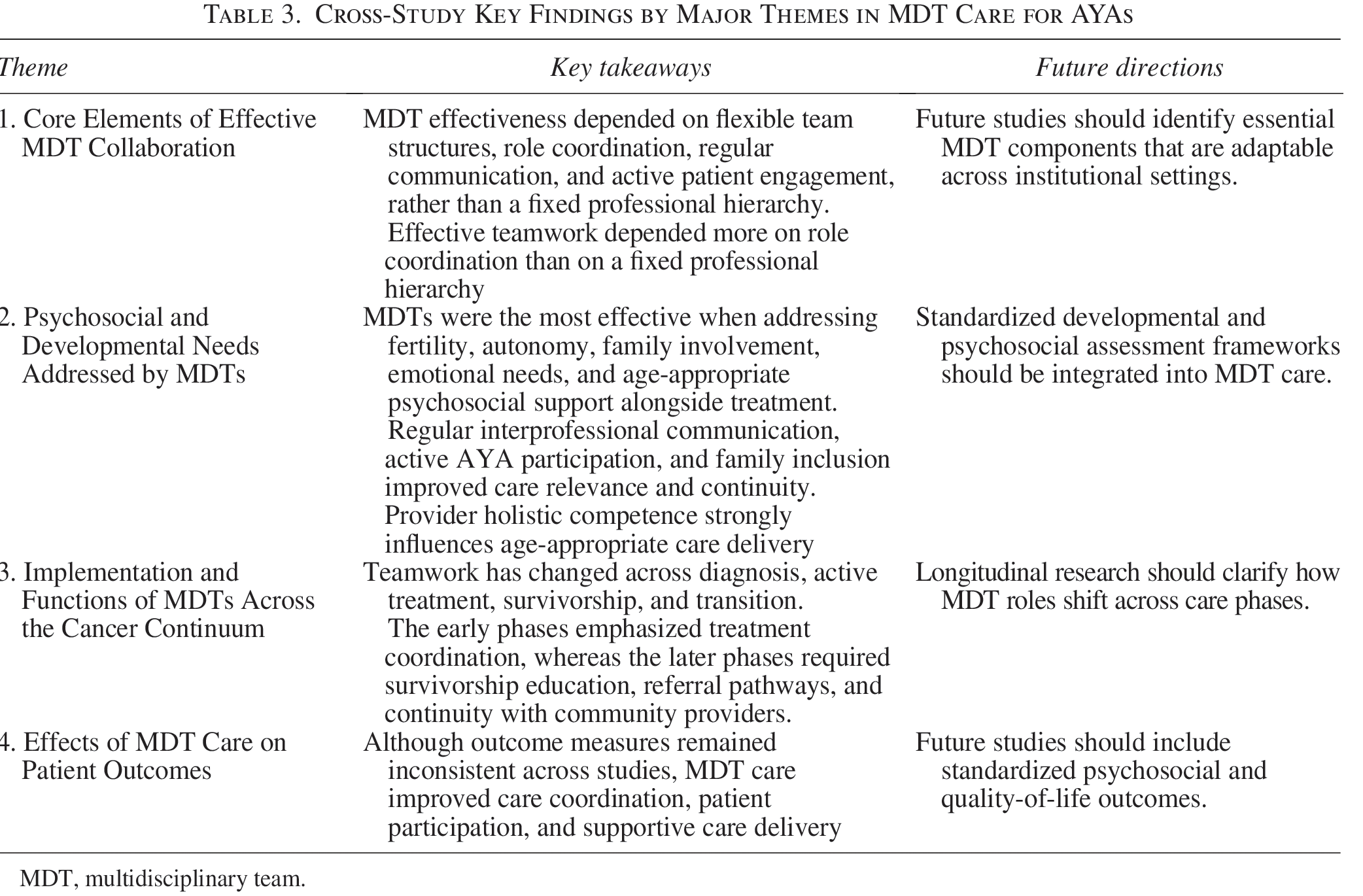
MDT, multidisciplinary team.
Nursing implications
The results of this systematic review highlight the benefits of team-based care for AYA patients with cancer, with nurses playing a critical role. To ensure coordinated care across the continuum, oncology nurse navigators can serve as team leaders or liaisons between each MDT. Nurses should understand the unique needs of AYA patients with cancer and work collaboratively with other disciplines on the MDT to optimize their care. Standardized approaches to education can also aid in the transition between phases of care.12,14,23 Nurses should consider involving or developing MDTs when providing discharge planning and education for AYA patients and their families. When implementing an MDT, nurses need to employ a framework that can serve as a comprehensive approach to deliver care for AYA patients with cancer. Nurses can act as mediators to enhance communication between patients and health care providers during both active and postcancer treatment phases. 30
Strengths and limitations
A key strength of this systematic review is the methodological rigor of the review process, particularly the use of the MMAT to critically assess the methodological quality of the included studies, which enhances the credibility and trustworthiness of the synthesized findings. However, one limitation is that the age of AYA samples varied across studies, which may limit the comparability of the results. Additionally, there is a lack of studies that directly demonstrate the outcomes of MDT implementation. Another limitation is the geographic and linguistic focus of the studies, as all selected studies were from Western countries and published in English, which may limit the generalizability of the findings to other regions and languages.
Conclusions
The provision of comprehensive care for AYA with cancer requires consideration of their developmental and social needs by the MDT. Our review of the available evidence for MDT in AYA cancer care examined the essential core elements of effective MDT collaboration, the specific psychosocial and developmental needs of AYA with cancer addressed by MDT, the implementation and functions of MDT, and the effect of MDT care on patient outcomes. All studies that implemented MDT efforts demonstrated positive impacts on AYA cancer care, indicating that institutions should consider implementing MDT for AYA cancer care. Future efforts should continue to measure the outcomes of MDT for AYA cancer patients and consider implementing comprehensive programs that encompass the phases of cancer care from diagnosis to survivorship. Further research is needed to evaluate AYA care over the cancer care continuum, particularly with respect to the impact of MDT programs for AYA populations. Such studies would provide valuable insights into which MDT components and strategies are impactful for this population.
Authors’ Contributions
Study design: H.S. and A.K. Data collection and analysis: H.S. and A.K. Data interpretation: H.S., A.K., and J.C.G. First draft article writing: H.S. and A.K. Article revision: H.S., A.K., and J.C.G.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.