
Abstract
Purpose:
This study aimed to evaluate the cardiovascular medical management of young adults who had viewed the massive open online course (MOOC) “Childhood Cancer, Living Well, After” four years earlier during the feasibility study (START-MOOC1), compared with those who had not.
Methods:
A retrospective, descriptive, French multicenter study was conducted involving 322 childhood cancer survivors (CCS) (range, 20–36 years) eligible to view the cardiovascular health module of the MOOC. Participants were divided into two groups those who had viewed the MOOC (MOOC+) four years earlier and those who had not (MOOC−). We collected data on medical follow-up, cardiovascular care, and lifestyle habits using a short questionnaire. We analyzed it using descriptive statistics and comparative tests.
Results:
Of the 322 eligible CCS, 95 completed the questionnaire (34 MOOC+ and 61 MOOC−). The participation rate was significantly higher in the MOOC+ group (55.7% vs. 23.4%, p < 0.0001). We found no significant difference between the groups regarding general medical care and cardiologist follow-up. However, 20% of MOOC+ participants began cardiological follow-up after the MOOC, 15% increased their physical activity, and 6% improved their diet. In addition, 25% of MOOC+ participants began complementary therapies.
Conclusion:
The MOOC “Childhood Cancer, Living Well, After” did not result in any significant difference in cardiovascular follow-up behaviors compared with patients who did not view the MOOC. However, the MOOC+ group promoted positive lifestyle changes. Further research with a larger cohort is necessary to assess the full impact of the MOOC on the long-term medical follow-up.
Keywords
Introduction
Over the last few decades, advances have significantly reduced cancer mortality rates among children and improved survival rates, which now stand at 85% overall. 1 However, this has also highlighted potential late side effects of cancer treatment due to the tumor itself or complications of surgery, radiotherapy, or chemotherapy. 2 The cardiovascular system is particularly vulnerable to cardiotoxic cancer therapies, such as anthracyclines and radiotherapy, which are frequently used to treat childhood cancers.3,4 The anticipated cancer-related cardiac toxicities are especially cardiac dysfunction, hypertension, and dyslipidemia.
Cardiovascular disease is one of the leading causes of mortality and late morbidity among childhood cancer survivors (CCS). It’s essential to screen and manage additional cardiometabolic risk factors (obesity, hypertension, diabetes, and dyslipidemia) and to detect early signs of cardiac dysfunction in order to improve long-term survival in these patients.3,5
The North American, Australian (Children’s Oncology Group), and European scientific societies have developed long-term follow-up guidelines, whose convergence in the International Guidelines Harmonization Group (IGHG) reflects a consensus to improve and standardize screening strategies.6–11
Despite published guidelines and recommendations, many patients are unaware of their initial diagnosis, treatment, or late effects secondary to therapy.12–14 In the United States, 40% of the CCS population did not obtain follow-up echocardiography, while 31.6% of French survivors did undergo follow-up echocardiography within the last 5 years post treatment. 15 A smaller number of survivors, predominantly female, continued with long-term follow-up echocardiography (15.2%). Males (compared with females) and patients aged 36 to 49 (compared with patients younger than 36) were less likely to have undergone an echocardiogram (performed by a cardiologist) in the previous five years 16 , even though the first major cardiac event in chronic coronary syndrome typically occurs at age 31. 4
Empowering CCS to understand their medical history and long-term risks is vital, as informed patients make better lifestyle and health choices, a concept known as health literacy.17,18 Few studies have evaluated cancer survivors’ knowledge in survivorship, and health literacy has been chiefly assessed subjectively, despite expectations of adequate patient understanding. 19
Systematic reviews of interventions to improve adherence to surveillance guidelines in former childhood cancer patients found that only few randomized controlled trials reported significant improvements in adherence after the intervention.20–22 These studies showed that adding telephone counseling to mailed health information improved surveillance with echocardiography and mammography. In 2021, a study showed that a “Survivor Healthcare Passport” (a portable card summarizing the patient’s treatment, potential late effects, recommended tests, and their frequency) improved former pediatric patients’ knowledge of diagnosis, treatment, risks, and follow-up care. 23
To empower CCS to understand the risks associated with previous treatments and assist them in their health care decisions, our French team developed a MOOC (Massive Open Online Course) titled “Childhood Cancer, Living Well, After.” We initially studied the feasibility of its use in the START-MOOC1 study, which further details the video modules provided to survivors and the decision-making algorithm used to guide their allocation. 24 The research hypothesis was that well-informed patients feel more involved in their medical management and make better lifestyle and health choices.
The main aim of this study, which expands on the original START-MOOC1 study, was to evaluate the self-reported cardiovascular management of young adult CCS who received personalized therapeutic education through the MOOC, with a 4-year follow-up, compared with those who did not.
Materials and Methods
This study, conducted in 2024, expands on the original START-MOOC 1 feasibility study 24 that involved, in 2020, young adult CCS who were diagnosed with a solid tumor or leukemia between 2000 and 2010, lived in mainland France, and were less than 15 years old at the time of diagnosis, identified from the French Childhood Cancer Observation Platform, 25 a cohort based on the French national registry of childhood cancer. 26 The original START-MOOC 1 study aimed to create a MOOC entitled “Childhood Cancer, Living Well, After” and assess its feasibility to educate young adult CCS in a personalized way based on the treatments they have received.
Population
The eligible population of this study consisted of young adult CCS (range, 20–36 years) who, due to the risk of cardiac side effects, were eligible to view module 5 (“Good heart and lung health”) of the MOOC. Some of these patients did view module 5 (MOOC+ group, n = 61) during the START-MOOC1 study, while others did not wish to do so (MOOC− group, n = 274; i.e., an eligible population of 335 patients) (Fig. 1).
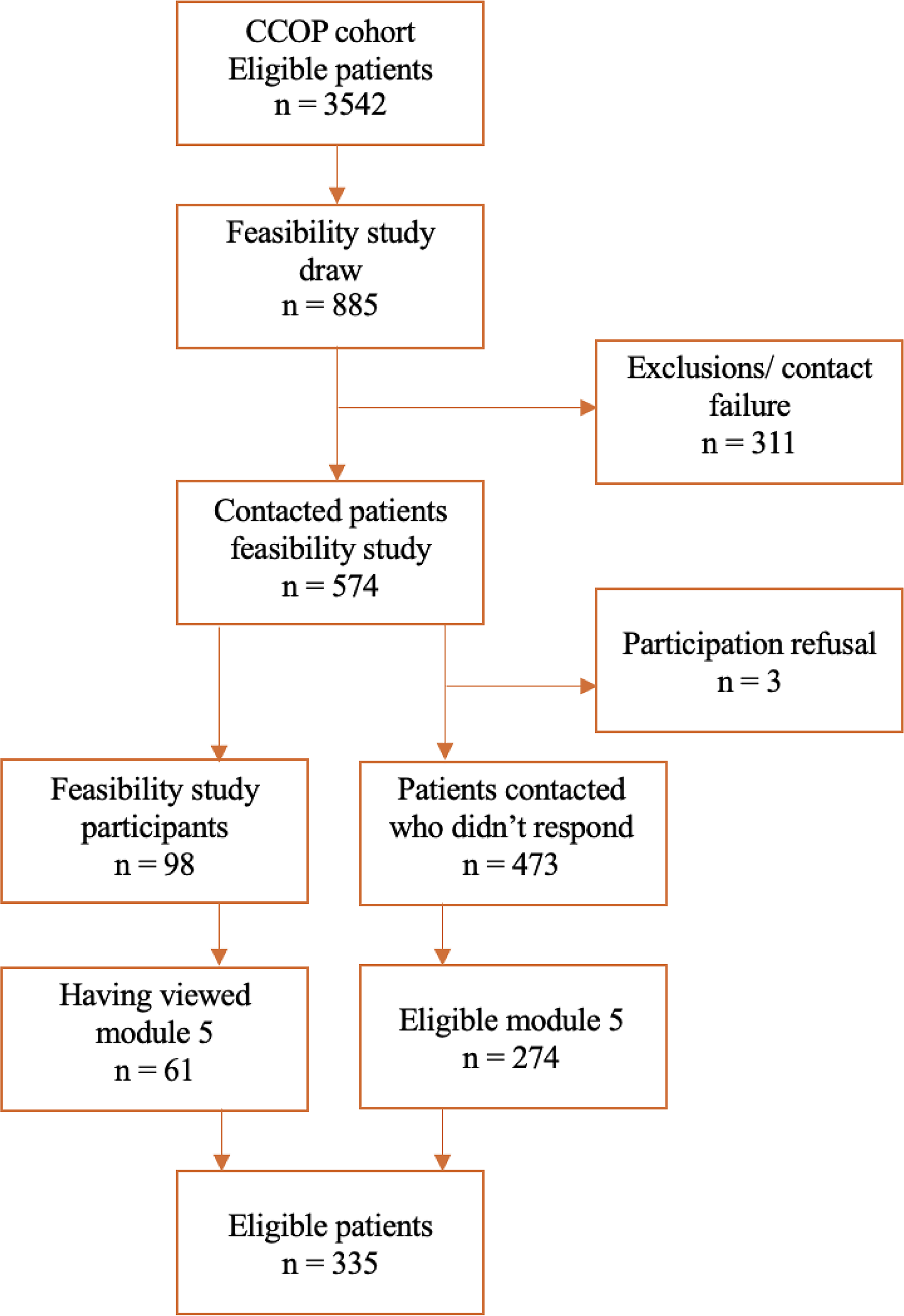
Flow chart of the eligible study population. CCOP, Childhood Cancer Observation Platform.
The risk of cardiac side effects, inducing eligibility for module 5, was determined using the algorithm presented in the feasibility study. 24 It was based on the cancer treatment received: chemotherapy (anthracyclines regardless of dose) and radiotherapy (chest-directed irradiation regardless of dose). No information regarding the prior cardiological follow-up of these patients was available.
MOOC modules
The total content of the MOOC “Childhood Cancer, Living Well, After” is described elsewhere. 24 Patients of the MOOC+ group viewed the three common modules: (1) “Taking care of yourself after cancer” (healthy lifestyle—nutrition/food portion size/Mediterranean diet—physical activity), (2) “Well in your head, well in your skin” (how to manage stress, anxiety), (3) “Let’s talk about fertility!” (information about fertility and Assisted Reproductive Technology). In addition, among the eight personalised modules, they also viewed at least the module No. 5, “Cardiac and Pulmonary Health.” So they have watched at least 4 of the 11 modules in the MOOC. Module 5 included six mini videos: testimonials, role of the heart or lungs, risks of cardiac or pulmonary complications, and individual prevention.
Method
This retrospective, descriptive, multicenter study expands on the original START-MOOC 1 study. 24 It gathered information on the medical follow-up, particularly cardiovascular follow-up, of CCS using a short questionnaire covering three main themes: follow-up by the general practitioner (GP); cardiovascular management; and general questions on diet, physical activity, and pregnancy in women. The questionnaire structure differed according to the group (Supplementary Appendix SA1, Supplementary Appendix SA2).
Some eligible patients may have undergone several treatments with potential cardiac side effects. An arbitrary choice was made to ensure exclusivity in the analysis of population characteristics. In this order of priority, we classified the participants into a single category: total body irradiation > chest radiation > anthracyclines.
Recruitment strategy
There were no exclusion criteria. The various eligible patients were contacted differently depending on whether they had been exposed to the MOOC (MOOC+ group or MOOC− group) four years earlier:
We contacted the 61 patients exposed to the MOOC (MOOC+ group) by email with a link to access the online questionnaire. The questionnaire was created using an online survey software (LimeSurvey), which allows restricted access by invitation only and with a personalized code. This software enabled data anonymization. Participants could complete the questionnaire in several stages, but the access code could not be reused once the questionnaire has been completed. The 274 patients not exposed to the MOOC (MOOC− group) were contacted by post, with the information leaflet and the relevant questionnaire. They could return the completed questionnaire in a prestamped, prefilled envelope or complete the online questionnaire appropriate to that group (link or QR code and personalized access code indicated in the letter).
Questionnaire
Each patient was informed that they had one month to complete the questionnaire. If the form was not completed, a reminder letter or email was sent 15 days after the initial contact.
Incomplete questionnaires that could not be properly analyzed were included in the nonresponse group. Some questions allowed multiple answers and were not exclusive (MOOC+: questions 6.3, 8, and 10; MOOC−: questions 4.3 and 7) (Supplementary Appendixes SA1 and SA2).
Ethics statement
The Ethics Committee of the University Hospital of Saint-Etienne approved this study on November 08, 2023. The initial global study START-MOOC1 received authorization from the French Expertise Committee for Research, Studies and Evaluations in the Field of Health on February 02, 2019, and from the French National Commission for Data Protection and Liberties (CNIL) (no. DR2019-215) on August 02, 2019.
Patients were informed in the letter they received that their response to the questionnaire was equivalent to consent to participate in the study.
Statistical analysis
Participant characteristics (age, sex, diagnosis, and reason for module eligibility) were collected, and descriptive statistics were obtained. Questionnaire data collected via the LimeSurvey online software are aggregated results, not allowing responses to questions related to participant characteristics. The two groups were compared using the Chi2 or Fisher’s exact test for qualitative data and a Student’s t-test for quantitative data. Results were considered significant at the 5% level.
Results
Participation and population characteristics
Of the 322 successfully contacted patients, 102 completed the questionnaire; however, 7 of them provided only partial responses and were therefore ultimately included in the non-response group (Fig. 2). There were 34 patients from the MOOC-exposed group (MOOC+) and 61 from the non-MOOC-exposed group (MOOC−). The participation rate was 29.5% of those contacted (Fig. 2), with a significantly higher rate in the MOOC+ group (55.7% vs. 23.4%, p < 0.0001) (Table 1). Most participants from the MOOC− group (58%) returned questionnaires by mail, with the remainder of participants answering online.
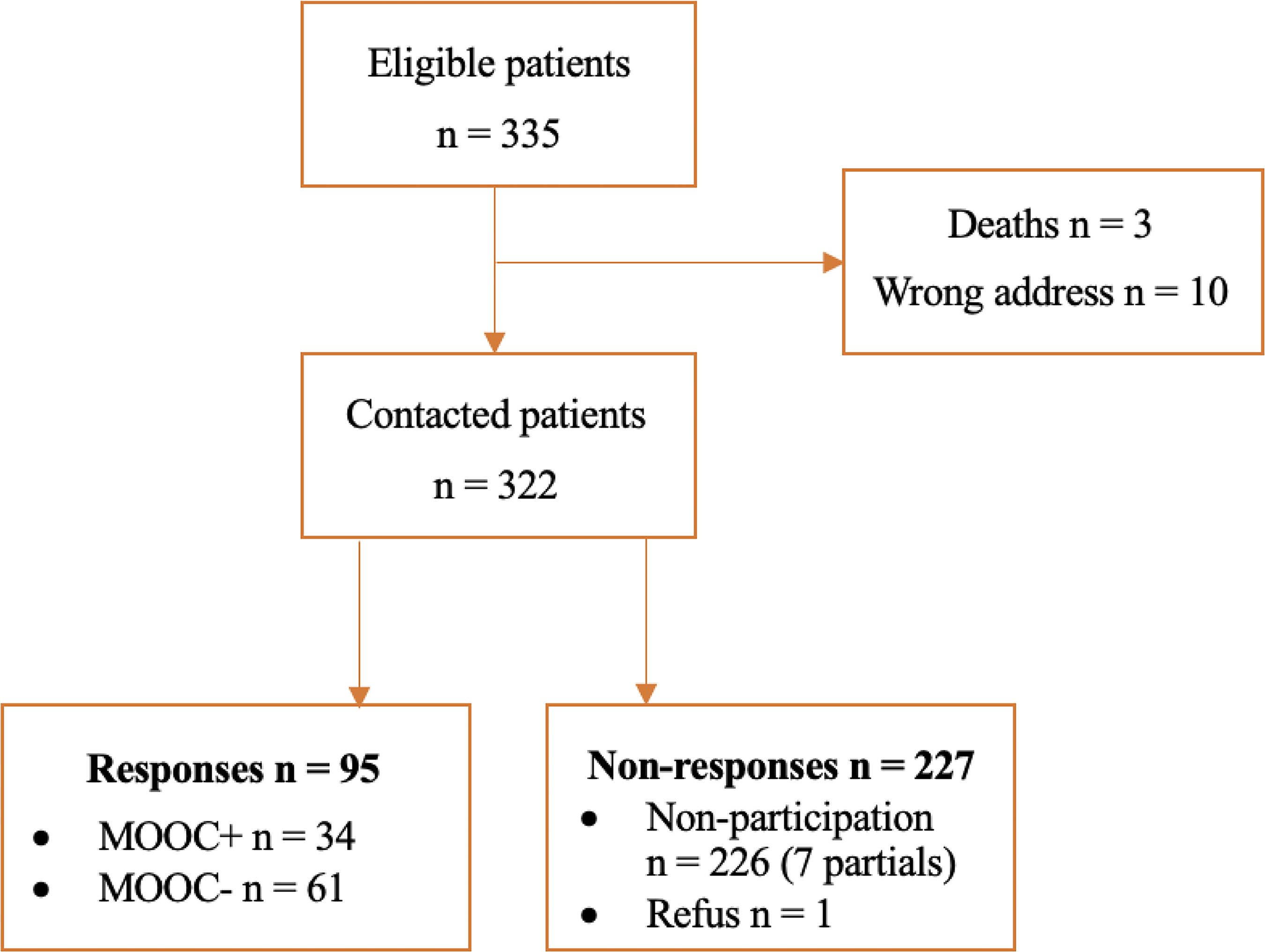
Flow chart of study population.
Characteristics of the MOOC+ and MOOC− Patients Eligible for the “Good Heart and Lung Health” Module According to Their Participation in the Study

Bold and italic values indicate statistically significant P-values (p < 0.05).
Including germ cell tumors, carcinomas, CNS and SNS tumors, and liver and kidney tumors.
CNS, central nervous system; MOOC, Massive Open Online Course; RT, radiotherapy; SNS, sympathetic nervous system; TBI, total body irradiation.
The characteristics of the study population showed no significant differences between the two groups (MOOC+ and MOOC−) except for sex, with the MOOC+ group being predominantly female (Table 1). In the MOOC− group, the type of cancer was a significant factor in participation (p = 0.04).
The average age at the time of the study was similar between the two groups: 27.6 years (±3.8) for MOOC+ and 27.4 years (±3.5) for MOOC−.
MOOC+ versus MOOC− results
General medical care
Although there was no difference between those exposed and not exposed to MOOC in terms of frequency in GP visits (p = 0.3), 59% (36/61) of survivors followed up with their GP at least once a year in the MOOC− group versus 53% (18/34) in the MOOC+ group (Table 2). Five MOOC+ and 17 MOOC− patients never saw their GP outside an acute episode, and two MOOC+ did not have one.
General Medical Care of the 34 MOOC+ and 61 MOOC− Patients Who Responded to the Questionnaire
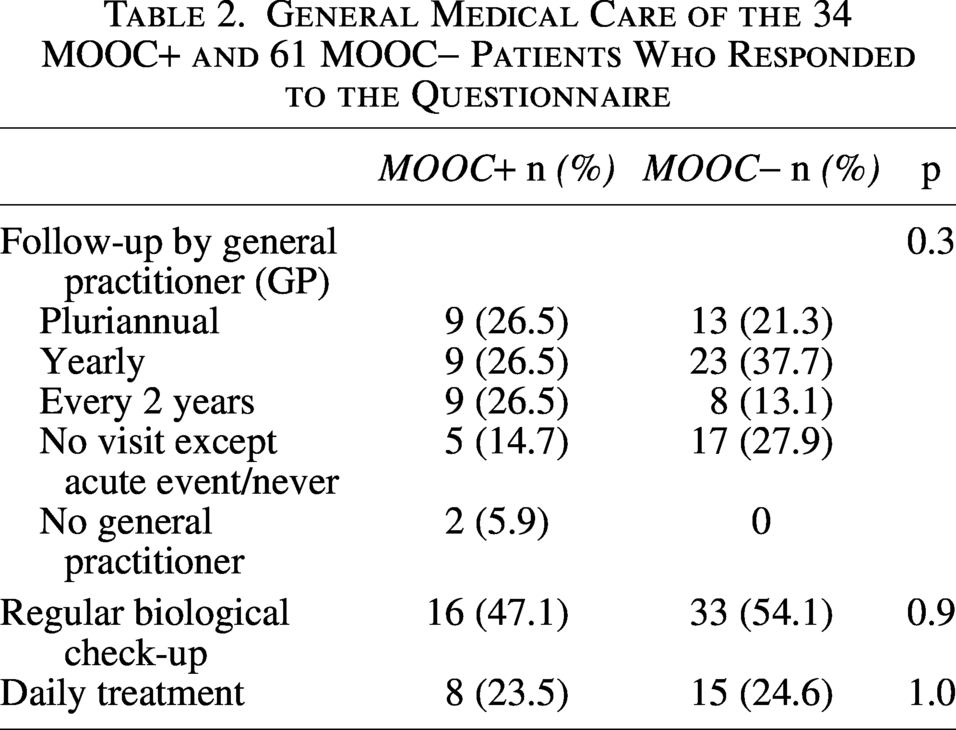
In both groups, a half the patients indicated that their GP prescribed biological check-ups for health monitoring, and 75% answered that they did not take any medications daily. In the MOOC+ group, among the eight patients who were taking regular medication, two were taking cardiovascular drugs (i.e., approximately 6% of patients in the MOOC+ group) (angiotensin receptor blockers – [ARB] 2 and lipid-lowering drugs). In the MOOC− group, 2 patients reported taking cardiovascular medication (ARB-2 and β-blockers, i.e., approximately 3% of patients in the MOOC− group).
Cardiovascular care
In each group, half of the patients reported receiving follow-up care from a cardiologist (p = 0.8) (Table 3).
Cardiovascular Care for MOOC+ and MOOC− Patients
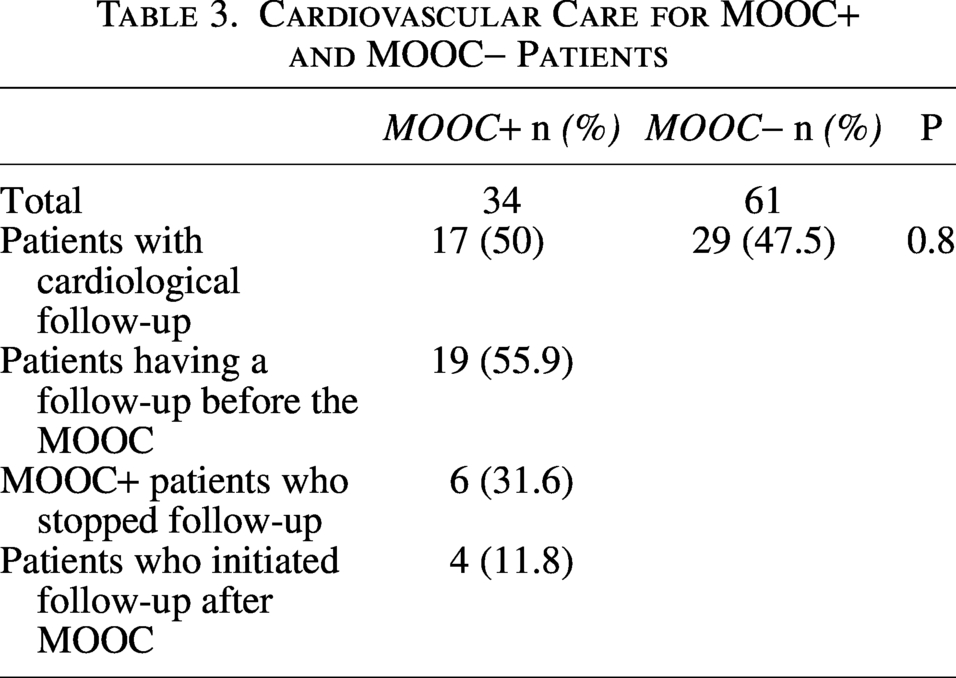
Four MOOC+ patients (11.8%) underwent cardiological follow-up after viewing the MOOC. More specifically, of the 13 patients who did not already have a cardiovascular follow-up, four patients started one (19%). However, six patients also answered that they had stopped their follow-up afterward, making it impossible to highlight a significant difference in follow-up between the two groups in conjunction with therapeutic education via the MOOC.
At the question “Who referred you to the cardiologist in the first place?”, in both groups, mainly oncologists advised initial referral (56% in the MOOC+ and 55% in the MOOC− group). GPs were also advisers initial referrals to cardiologists (13% MOOC+, 20% MOOC−).
Pregnancy
Twelve women reported having had a pregnancy, with no significant difference between the groups (24% MOOC+ and 27.3% MOOC−, p = 0.8).
In the MOOC+ group, of the six women who had had a pregnancy (including one who had suffered a spontaneous miscarriage), four had had a cardiac ultrasound before pregnancy (66.6%), and only 2/4 had had one during pregnancy.
In the MOOC− group, six women also reported having had a pregnancy (including two spontaneous miscarriages and one elective abortion), two had a cardiac ultrasound before pregnancy, and none during pregnancy. There was no statistically significant difference in the performance of these examinations between the two groups.
Other care or consultations
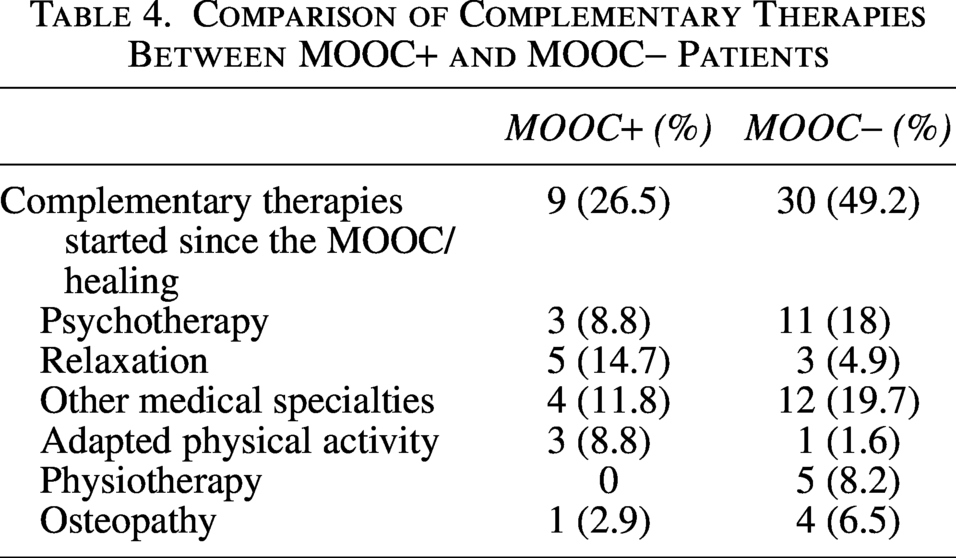
Complementary therapies reported were psychotherapy, relaxation, other medical specialties, adapted physical activity, physiotherapy/rehabilitation, and osteopathy. Nine patients in the MOOC+ group (26.5%) reported starting at least another care since viewing the MOOC. In the MOOC− group, 30 patients (49%) reported having had other care or consultations since their cancer was cured (Table 4).
Comparison of Complementary Therapies Between MOOC+ and MOOC− Patients
Current care for survivors
MOOC+ group
Only 53% of patients consulted their GP at least once a year as part of their long-term follow-up, as recommended by IGHG of late effects of childhood cancer. Ninety-one percent of the patients in this group did not change their follow-up with their GP after viewing the MOOC. Eighteen patients (53%) already had very regular follow-ups, while one reported that he preferred to see their oncologist and one had forgotten the information the MOOC provided 4 years ago. Only two patients (5.8%) discussed the information acquired through the MOOC with their GP.
Of the 20 patients who said they had a cardiologist follow-up before viewing the MOOC (58.8% of the group), 10 (50%) said they went for a consultation every 5 years, 8 (40%) every 2 years, and 2 (10%) every year.
Of all MOOC+ patients, 10 (29.4%) indicated that they had undergone other examinations as part of their cardiological follow-up (with cardiac echography), including advanced imaging (cardiac CT or MRI), Holter ECG, and cardiac stress tests.
Among patients with no cardiological follow-up, 12 patients (70%) believed that follow-up was unnecessary (opinion or affirmed by a health care professional). Other reasons include difficulty in accessing an appointment (two patients, 12%), geographical distance (two patients, 12%), the fact that it is time-consuming (two patients, 12%), or a source of stress (one patient, 6%).
Regarding lifestyle changes, two patients (6%) said that they had modified their eating habits, and five patients (15%) reported increased physical activity.
MOOC− group
Similarly, only 59% of MOOC− patients had at least annual follow-up by their GP, implying that 41% needed long-term follow-up in line with the latest recommendations.
Among the 61 patients, 29 patients (47.5%) underwent a cardiological follow-up. Sixteen patients (55%) went for a consultation every 5 years, 11 (38%) every 2 years, 1 said he went every year, and another every 10 years. Two patients (3%) had no follow-up, only a consultation at a distance from the cure.
Forty-nine patients (80%) in the MOOC− group felt that they had a healthy lifestyle, with a healthy diet and regular physical activity, and 24 (39.3%) said that they had modified their lifestyle after cancer recovery.
Forty-one patients (67%) expressed interest in informative videos about their childhood cancer and treatments.
Discussion
MOOCs are effective tools for educating and empowering patients, enabling them to participate actively in their own long-term care. Pediatric cancer survivors benefited from educational videos addressing both general topics (post-cancer follow-up, healthy lifestyle, psychological well-being, fertility) and cardiac-specific content, all developed on the foundation of the prior MOOC feasibility study. Previous research on pediatric cancer survivors focused on online and mobile educational interventions that focus on diet, physical activity, and weight.27–32 This study is the first to explore a method of improving pediatric cancer survivor adherence to surveillance through directed education with online video(s).24,33 Young adult survivors of pediatric cancer at potential risk for cardiomyopathy were assessed through questionnaires addressing medical habits, cardiology follow-up, and lifestyle habits. Participants were contacted in two groups: those who had viewed a lifestyle video promoting heart health and those who had not received this intervention.
This study found no statistically significant difference in improved adherence to surveillance screening in pediatric cancer survivors post-MOCC education intervention. Although only half of the population adhered to long-term follow-up recommendations, which aligns with the literature data, 34 some results remain encouraging.
Pediatric cancer survivors exposed to the education module clarify if they were already followed by cardiology or were lost to follow-up and were re-referred for cardiology follow-up (19%). Heart-healthy activity increased by 15% and diet improved in 6% of pediatric cancer survivors. The results of this intervention are encouraging, particularly in light of recent studies emphasizing the importance of cardiovascular risk management and lifestyle improvement, especially in this vulnerable population of survivors.5,35
While post-traumatic stress, generalized anxiety, depression, and fear of cancer recurrence were not specifically assessed, 26.5% of survivors reported engaging in complementary therapies—most commonly psychotherapy and relaxation techniques, as suggested in the MOOC modules. These observations underscore the need for systematic integration of mental health assessment and support within the long-term follow-up of CCS.
These results align with the recent 2024 study on CCS treated for Hodgkin’s lymphoma. 36 The results showed a higher awareness of the recommendations in the mobile app group than in the control group, but no significant difference was found in screening or intention to screen.
Another study reported similar results in a population of women with ovarian cancer for whom current guidelines recommend genetic risk assessment by a geneticist, but this is rarely carried out in practice. 37 The mobile application did not increase the number of consultations, but the patients were more knowledgeable about hereditary ovarian cancer and communicated more with their families.
In this study, from the survivors’ perspective, cardiology follow-up was often considered unnecessary, either because they perceived no further need for surveillance or trusted their current providers’ knowledge. Yet, evidence shows that many providers remain insufficiently confident in managing late cardiac effects.13,38–40 Digital tools, such as apps or survivorship passports, have been proposed to bridge this gap.41–43 Nevertheless, referral to cardio-oncology—now increasingly recognized as the standard of care for survivors exposed to cardiotoxic therapies—appears essential. 6
The MOOC was disseminated in 2020, coinciding with the COVID-19 pandemic. This temporal overlap may have constrained participants’ ability to implement recommended follow-up, as access to elective and nonurgent care was markedly limited during this period.
As some survivors reported forgetting the MOOC content they saw in 2020, regular, personalized reminder tools appear essential to sustain adherence to recommended long-term follow-up.
Limited screening may also reflect an “ostrich policy,” with patients avoiding potentially unfavorable results. 44 A related concept, akrasia—acting against one’s better judgment—has been described in a French study and could provide a useful framework to strengthen long-term CCS follow-up. 45
A strength of our study is that 67% of patients in the control group—that is, those who had not participated in the 2020 feasibility study and therefore had not been exposed to the MOOC—reported being interested in viewing educational videos providing information about their cured childhood cancer and the treatments they had received. This finding supports the potential value of broader dissemination of the MOOC in the future.
Limitations of the study
Our study had several limitations, and in the end, further research is needed. First, a key limitation of this study is its reliance on patient-reported information rather than objectively verified data from the National Health Data System, which may have introduced reporting bias and limited the precision of our findings. The questionnaire mainly consisted of yes/no items, with a few follow-up open questions. Some conditional questions were not always fully understood, highlighting how respondents may interpret questions clear to the author differently. No themes emerged from open-ended responses. For example, we asked about cardiac echocardiography before or during pregnancy but did not record whether pregnancies occurred before or after MOOC exposure, limiting assessment of the MOOC’s impact on adherence to recommended monitoring.
The study design used an online questionnaire, necessitating anonymization of data and aggregation of results, making it impossible to link the information collected to the corresponding patients. As a result, responses could not be analyzed according to the treatments received, although the recommended follow-up period varied according to the therapies administered during childhood. A differently designed study could enable a more detailed analysis of patients’ cardiovascular follow-up and fairer comparison with the recommendations of learned societies.
Another significant bias in the study was the difference in the sex distribution of the patients between the two groups. This result was expected, given the choice of the initial population, but it is a selection bias, which could lead to misinterpretation of the results. The observed differences could be due to biological or behavioral differences between the sexes. This bias could be avoided in future studies using randomization methods.
Conclusions
This study is a 4-year follow-up by the same research team to the initial START MOOC1 study conducted in 2020, aiming to assess whether patients changed their medical follow-up after viewing the MOOC. While no significant changes in medical management were observed, some results were promising. This work was conducted as an intermediate step pending approval from the French data protection authority (CNIL) for a larger-scale project, using a multiple randomized controlled cohort trial design. The forthcoming study is expected to provide a more accurate, reliable, and representative evaluation of the MOOC’s impact and to explore barriers to implementing long-term screening for late effects in this population.
Authors’ Contributions
Each person listed as an author was aware of the content of the article and participated in the study in a meaningful way. All authors contributed to the interpretation of the results, the editing of the article, and the approval of the final submitted version. All authors accept responsibility for the decision to submit this article for publication. L.F., C.B., and L.C. developed the study concept and drafted the article. C.B. and C.D.-G. developed the concept of the MOOC “Childhood Cancer, Living Well, After” and obtained funding. L.F. and L.C. contributed to study methodology, data preparation, and analysis. V.L., B.D.M., M.D.M., and C.P. contributed to the resources by managing the technical part of the MOOC. All other authors contributed to the resources by managing part of the MOOC conceptualization.
Footnotes
Acknowledgments
The authors sincerely thank all of the former patients and participants in this study. They also thank Laura Dang-Viet for her help with this study; Dr. Sylvie Martin-Beuzart, Ophthalmologist; Dr. Muriele Schneider, Physical Medicine and Rehabilitation; and Mr. Olivier Mounier and Mrs. Christèle Gouy from the Department of Informatics, University Jean Monnet, Saint-Etienne for their great investment in the creation of the MOOC.
Author Disclosure Statement
The authors declare no competing financial interests.
Funding Information
We thank the French National Institute of Cancer (INCa), the League Against Cancer, and the ARC Foundation for Research Against Cancer, which funded the START-MOOC1 study (
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.