
Abstract
Background:
Sarcomas are rare, heterogeneous malignancies that disproportionately affect adolescents and young adults (AYAs) aged 15–39 years. Despite representing less than 1% of new cancer diagnoses in the United States, sarcoma is a leading cause of mortality in individuals under 20 years old. Although age-specific challenges that may compromise long-term survivorship have been investigated, the specific experiences and perspectives of young adults navigating the sarcoma care continuum remain underexplored.
Methods:
We conducted a qualitative study using semistructured, web-based interviews with AYAs (18–39 years) who underwent surgical resection for extremity sarcoma at a single comprehensive cancer center, conducting interviews between August 2024 and January 2025. Participants were recruited from an orthopedic oncology clinic and consented electronically. Interviews explored experiences from diagnosis through recovery, including communication, support systems, and perioperative education. Transcripts were analyzed using inductive thematic analysis.
Results:
In total, 14 participants (64% female) with diverse sarcoma subtypes and treatment histories completed interviews. Themes included (1) diagnostic challenges, such as low clinical suspicion and delays in referral to sarcoma specialists; (2) the critical role of support systems during diagnosis and hospitalization; and (3) communication gaps regarding fertility, financial concerns, postoperative complications, and long-term recovery.
Conclusions:
AYAs with sarcoma face unique barriers across the care continuum, including delayed diagnosis, limited psychosocial support, and insufficient perioperative education. Interventions to improve early recognition, strengthen referral pathways, enhance communication, and deliver tailored resources are urgently needed. Larger, multicenter studies should validate these findings and inform strategies to optimize outcomes for this vulnerable population.
Keywords
Introduction
Sarcomas represent a heterogeneous group of malignancies that disproportionately affect adolescents and young adults (AYAs) aged 15–39 years. 1 Despite representing less than 1% of new cancer diagnoses in the United States, sarcoma is a leading cause of cancer-related mortality in individuals under 20 years old. 2 Unfortunately, variations in clinical presentation, sarcoma subtypes, and underlying biology complicate both diagnosis and treatment decisions. 3 Paradoxically, although sarcomas are prevalent among younger individuals, these challenges may be more pronounced in this demographic and are believed to contribute to the disparities in outcomes between age groups. As an example, given that cancer, in general, is rare in young adults, low clinical suspicion and misattribution of symptoms to benign causes can lead to delays in diagnosis. 4 In addition, delays in diagnosis compound other factors associated with poor clinical outcomes, including residential distance from a specialized sarcoma center with age-specific care pathways and access to clinical trials (i.e., distance decay). 5
In addition to impediments that young adults may face as part of diagnosis and prior to treatment, there are multiple barriers to receiving recommended treatments after the diagnosis has been established. Existing evidence shows that young adults who experience illness encounter systemic, interpersonal, and individual-level difficulties, including limited health literacy, inadequate insurance coverage, fragmented care coordination, and psychosocial stressors. 6 Few studies address these issues in the context of young adult sarcomas or explore how these might vary by treatment phase (i.e., active treatment versus survivorship). The latter is an important consideration as issues such as mood disorders and anxiety,7,8 which have been shown to peak during diagnosis and treatment for young sarcoma patients, 9 have also been associated with treatment nonadherence in other AYA cancer types. 10
Despite increasing awareness that these age-specific challenges may compromise long-term survivorship, 11 the specific experiences and perspectives of young adults navigating the sarcoma care continuum remain underexplored, particularly in the context of surgical decision-making, perioperative counseling, and recovery following limb-sparing or ablative procedures. Consequently, patient-driven and targeted solutions are lacking. As a first step in designing strategies that promote high-quality care for this population, we conducted a qualitative study using semistructured interviews anchored in questions that explored factors that shaped care trajectories for young adults who underwent surgical resection of their sarcomas.
Methods
Study setting and design
Young adults aged 18–39 years with extremity bone or soft tissue sarcoma who received their surgical treatment at The Ohio State University James Comprehensive Cancer Center were recruited between July 2024 and February 2025. Those who underwent their index surgery more than 5 years prior to study enrollment were excluded. Patients who received nonsurgical treatment modalities (i.e., chemotherapy and radiation) at external facilities were eligible. Fluency in written and spoken English was required.
A semistructured interview guide was developed through collaboration with the principal investigator (J.H.A.), an AYA social worker, and the research team (Supplementary Data). Open-ended questions were designed to elicit participants’ perspectives spanning the full care continuum but were intentionally anchored around the perioperative surgical experience, including preoperative counseling, hospitalization, postoperative complications, and recovery. Questions focused on patient experiences at specific time points, from consultation to final follow-up, and included topics such as communication with the surgical team, preparation for surgery, the perioperative experience, and long-term recovery. The interview guide was piloted with an AYA patient advocate and sarcoma survivor and revised prior to its use for data collection.
After receiving institutional review board approval (STUDY 2024C0045), patients were recruited by research team members in the orthopedic oncology clinic to participate in a 60-minute web-based interview. Electronic consent was obtained prior to conducting interviews. Participants were compensated with a $50 electronic gift card.
Procedures, coding, and analysis
A trained interviewer conducted all participant interviews (L.J.R.). Transcripts of interview audio recordings were transcribed verbatim with care taken to redact any information that might identify the patient, their familiars, or providers. A representative sample of interview transcripts was reviewed independently by three analysts to generate a preliminary coding rubric. Iterative review was used to develop a final coding rubric. One analyst then coded all transcripts using the finalized coding rubric. Following completion of coding, the research team met to refine, organize, and synthesize codes into final themes. NVivo version 14 (QSR International) was used to facilitate data management and analysis.
Results
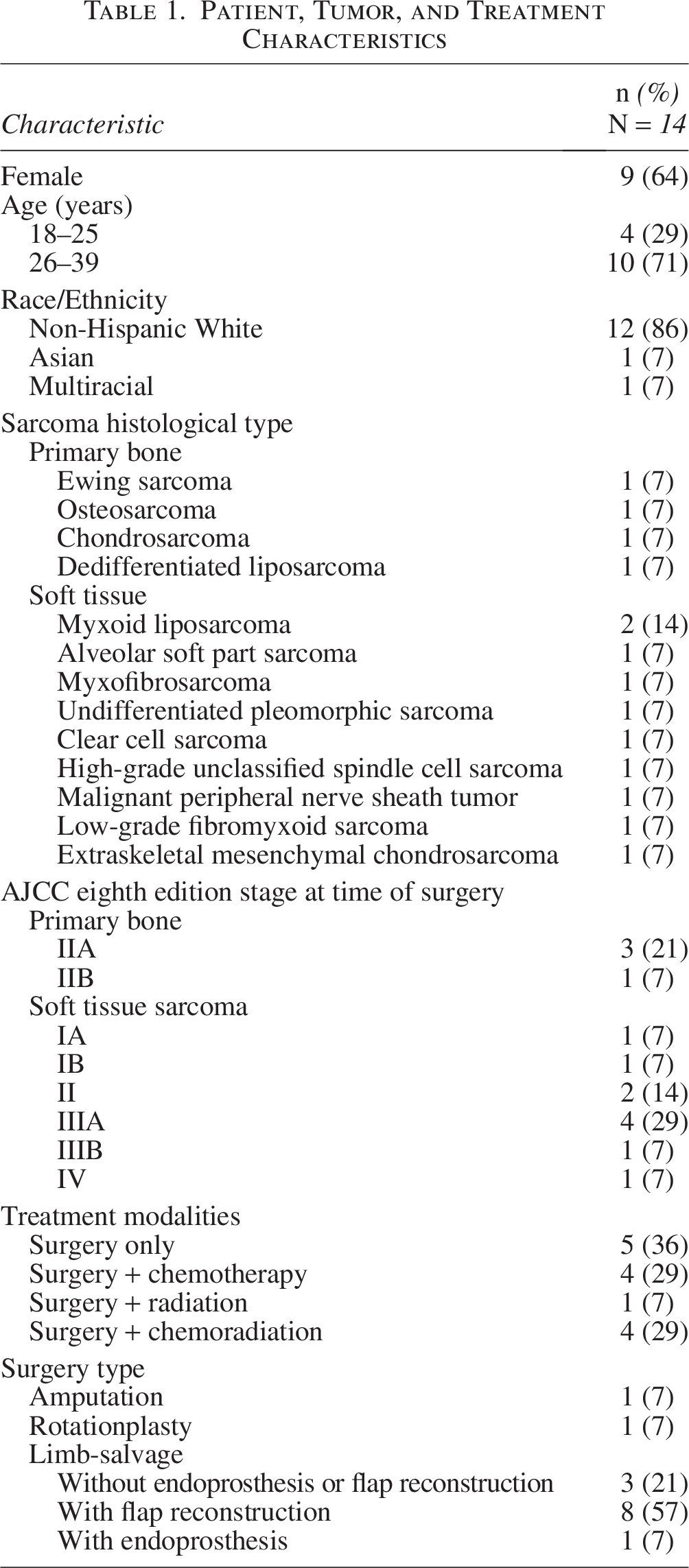
Of the 14 patients who participated, 9 (64%) identified as female. The majority of participants were between the ages of 26 and 39 at the time of their surgery, with only 4 (29%) being under 26 years of age. The sample included a heterogeneous representation of bone and soft tissue sarcomas (Table 1).
Patient, Tumor, and Treatment Characteristics
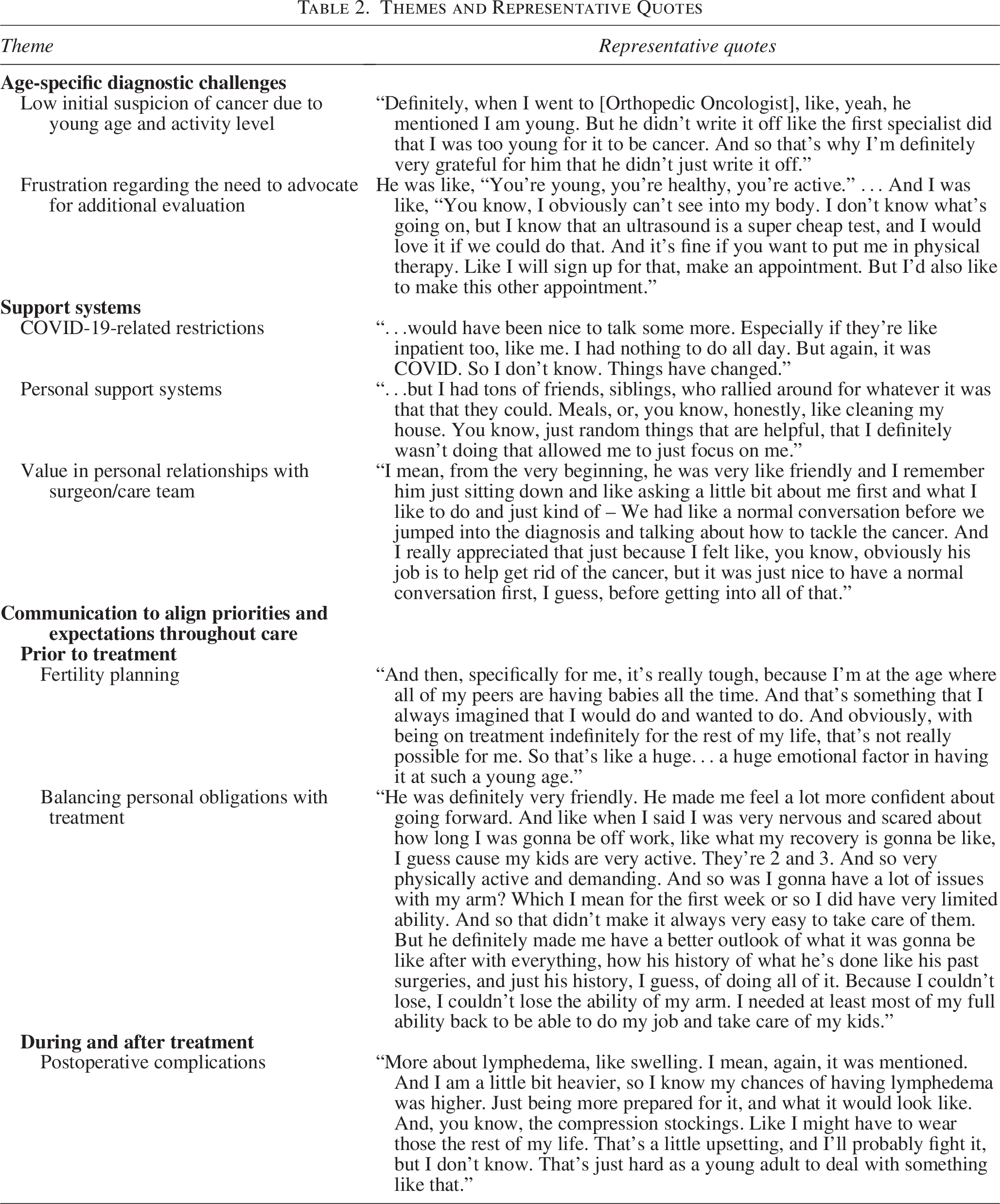
Dominant themes emerged pertaining to experiences with diagnosis, perioperative processes, and recovery. While the themes identified in this study span the sarcoma care continuum, they are fundamentally rooted in the surgical experience. Surgery represented the defining event around which diagnostic delays, treatment trade-offs, hospitalization experiences, and recovery expectations were interpreted. These themes are described below, with additional supportive quotations in Table 2.
Themes and Representative Quotes
Age-specific diagnostic challenges
Participants described circumstances that may have delayed their diagnosis. The majority of participants commented on their level of activity prior to diagnosis, suggesting that both they and their providers had a low clinical suspicion that their signs and symptoms represented cancer. One patient commented that although he had knee pain, “it took a while for [him] to look into it because [he] was so busy, and [he] just didn’t …think it could be anything that serious.” Even when cancer was suspected, referral to a comprehensive cancer center with sarcoma specialists was needed because of “people with sarcoma having issues of it being incorrectly diagnosed from the beginning, because it is so rare,” and nonsarcoma specialists having limited experience with “what treatment would be like.” If diagnostic evaluation was not completed prior to referral, patients experienced frustration about having to advocate for timely and additional work-up in advance of meeting with a sarcoma oncologist. One participant explained:
One thing that I don’t love…[the doctor] was trying to soften it…And this is one thing I would really like to see changed. One of the worst parts about having a cancer diagnosis is waiting to find out how bad it actually is….[T]here was like a 3-week waiting period to get in to see the doctor, and it wasn’t until I got in to see the [primary oncologist] that they then scheduled the MRI and PET scan. And I was just like, you know I’m going to need this…. You knew that before talking to me.
Support at diagnosis and during treatment
Participants emphasized the importance of being informed early that they would need their support networks present during pivotal conversations, such as diagnosis and treatment planning. A patient reported dismay that “the office never reached out and said, ‘Hey, can your spouse come with you?’… you might want to have that support at the appointment…. I would recommend if a doctor knows that he’s gonna give a patient bad news, [say] ‘hey, make sure you bring someone with you.’”
During treatment, support was also highlighted as a critical issue. Young adult sarcoma patients highlighted the critical role of support systems during their cancer journey, especially in the immediate perioperative period and inpatient stay and amid the challenges posed by COVID-19, which forced many to adapt creatively to maintain access to emotional and logistical support. One participant explained that:
Because of this COVID thing you know, they had limits on visitors… You could be there during your surgery, but then they were, was the craziest thing like they were gonna make [my wife] leave…. I reached out to one of these patient advocate type, you know, kind of deals, and I explained to them, I’m like, ‘Listen, you know my surgery was double the length it was supposed to be. I’m going to be here for the next 7 days by myself. You guys should really probably let her back in.’
While friends and family were the primary sources of support, participants emphasized the critical role of provider support. Specifically, patients expressed a strong desire to bond with their surgeons, valuing personal relationships that fostered trust and comfort throughout their care experience. One participant recounted that he was told by his surgeon, “We’re gonna be friends,” and that this elevated the “level of care.”
Communication to align priorities and expectations throughout surgical care and recovery
Participants identified several aspects of care that would have benefited from improved communication to align their expectations and priorities with those of their health care team. Individuals consistently described gaps in communication surrounding surgical planning, perioperative expectations, and recovery, particularly when personal priorities such as fertility, functional outcomes, and return to work were not explicitly addressed before surgery. Narratives explicitly indicated concerns and expectations for family planning, financial navigation, emotional support, education about postoperative complications and healing, and understanding surveillance and health maintenance during survivorship.
While participants generally were agreeable to recommended treatment plans, several noted that their desires with regard to family planning or fertility preservation were not sufficiently prioritized by their care teams. One patient expressed her frustration with her treatment timeline, stating, “I said my biggest concern was fertility. You’re telling me you want to start next week, and also that the chemo that you want to use is … very detrimental to my fertility. I was, at that point, furious.” This same participant highlighted how her financial concerns also related to her priorities for care: “It’s not like [reproductive endocrinology will] take you, and it’ll be a payment later. It’s like if you don’t show up, I think I had to make an $8000 down payment for them to even start ovarian stimulation. So, if you don’t just have like 8k hanging out, like you’re hosed.”
Young adult sarcoma patients described recovery as a period marked by emotional and informational gaps, often highlighting ineffective communication resulting in poor preparation for events that transpired during and after treatment. Although postoperative complications related to extremity sarcoma surgery were discussed during preoperative visits, participants reported not fully understanding the severity, likelihood, or functional impact of adverse events such as hematomas, lymphedema, infection, or prolonged pain (Table 2). Wound care, in particular, emerged not only as a physical concern but also as a deeply emotional one, with perceptions of scars differing and, for some, evolving over time—from a desire to hide them to acceptance and even empowerment.
The inner thigh incision, I think is you know, fine. Its good… . I know a lot of people say, ‘well, scars, you know, tell the story…remind you what you’ve been through.’ It’s just hard when you’re a young adult and you still wanna…kind of live like a young adult and feel like you can wear dresses or shorts and not worry about your cancer scar or your port…I don’t want people to see that I have that. I don’t wanna have to have that conversation. I know there’s people that will have that conversation and will share. That’s just not me.
For these and other postoperative/post-treatment issues, participants expressed a need for clear, accessible online resources that resonate with their experiences and help them navigate post-treatment realities. Patients found value in peer-to-peer support videos and seeing others’ scars, which helped normalize their own experiences and supported mental health recovery.
Participants also suggested that more robust mental health resources tailored to their age, experience, and stage of recovery might help with aligning expectations and facilitate communication. One participant shared:
[The] survivor’s guilt. I kind of wish I was helped a little more with that. I also kind of wish that some counselors would be open about hearing people vent maybe about their feelings. Because sometimes they can bring emotions completely unrelated to the surgery because you’re going through a rough time…. Sometimes I felt like I wasn’t really being listened to that often.
Even after completing treatment, the need for clear communication about expectations persisted. Participants discussed a pervasive sense of uncertainty about the future—regarding health, identity, and life plans—compounding their distress and underscoring the importance of anticipatory guidance and ongoing psychosocial support throughout survivorship. One young adult shared:
At the 3-year mark, I didn’t say, ‘What is my chance now of recurrence?’ I feel like sometimes it kind of weirds them out when I ask those questions. They’ll answer me but I can tell they don’t usually talk about that maybe. So, I never felt like I could ask those questions. But I do feel like maybe some of this in-depth information is a little frowned on. It’s not something they like to give out.
Discussion
In this interview study of young adults with sarcoma, participants shared experiences spanning from diagnosis through recovery, reporting both on aspects of their care that were effective and areas in which improvements could be made. Notably, patients reflected on the need for referral to a cancer center specializing in sarcoma treatment, processes that allowed their support systems to participate in their care, communication and alignment of physician and patient priorities, and educational materials to enhance their understanding of events in the perioperative period and during recovery. These narratives highlight opportunities for interventions to advance care for this demographic (Fig. 1).
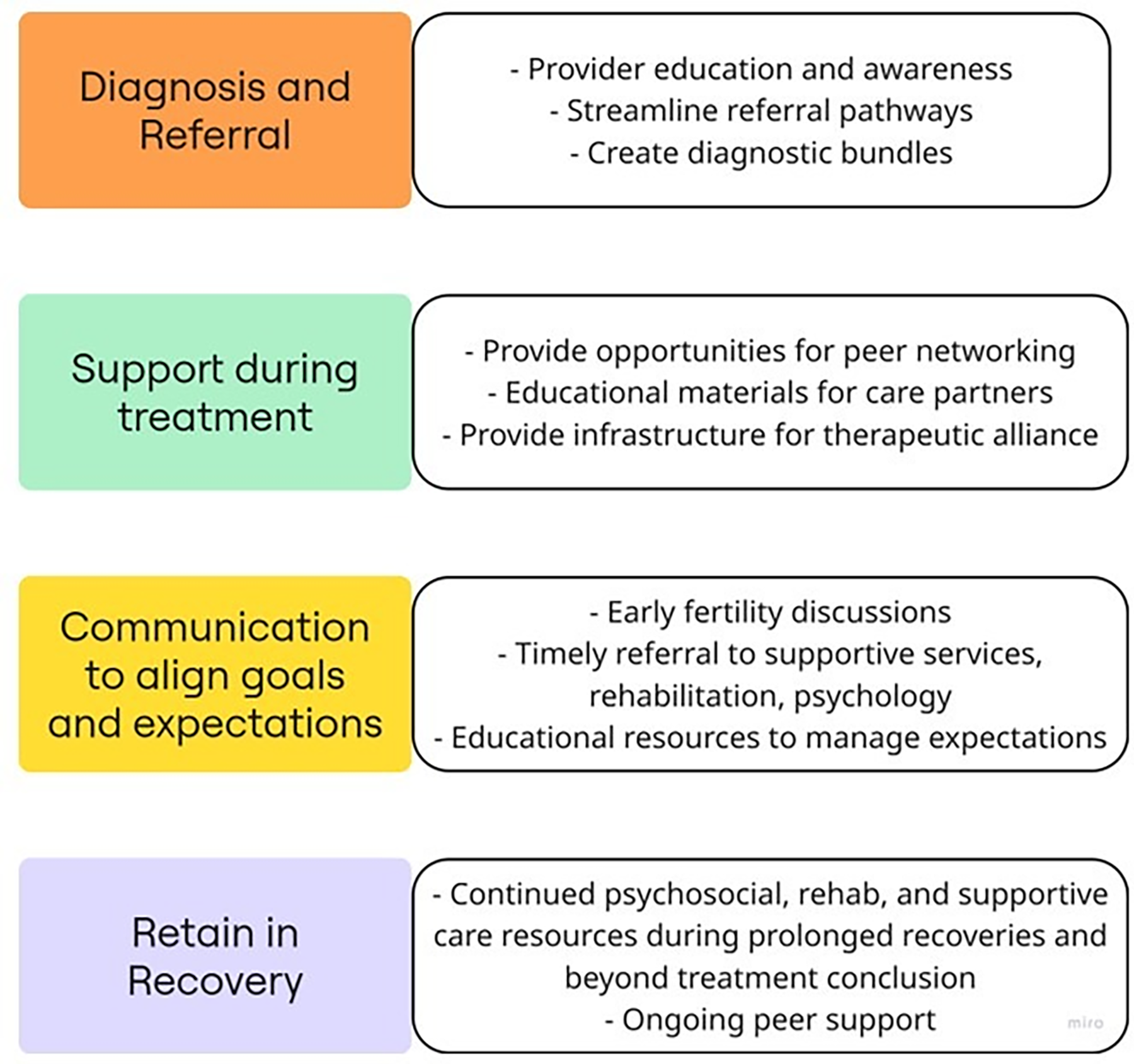
Opportunities for interventions to advance care for patients diagnosed with sarcoma as adolescents or young adults.
Themes related to difficulties or delays in diagnosis were nearly universal across interviews, consistent with this recurring theme in sarcoma-specific studies.11,12 While the National Comprehensive Cancer Network has published guidelines to assist in treatment once diagnosis is established, resources to guide practitioners in suspecting sarcoma are scarce. The American Society of Clinical Oncology has published a guide to diagnostic workflow that recommends providers consider soft tissue sarcoma on the differential diagnosis for deep, fixed, or firm masses that are larger than 4 cm and exhibit rapid growth (Fig. 2). Osseous sarcomas may also grow rapidly, present with pain at night or at rest, and/or be associated with a soft tissue mass. Magnetic resonance imaging is helpful and may prompt timely referral to a specialist, which in the case of suspected sarcoma should occur prior to performing a biopsy. Appropriate workup and a prompt, accurate diagnosis are paramount, especially since suboptimal resection leads to additional surgery and increases the complexity of surgical resections and reconstructions and may even necessitate amputation. 14
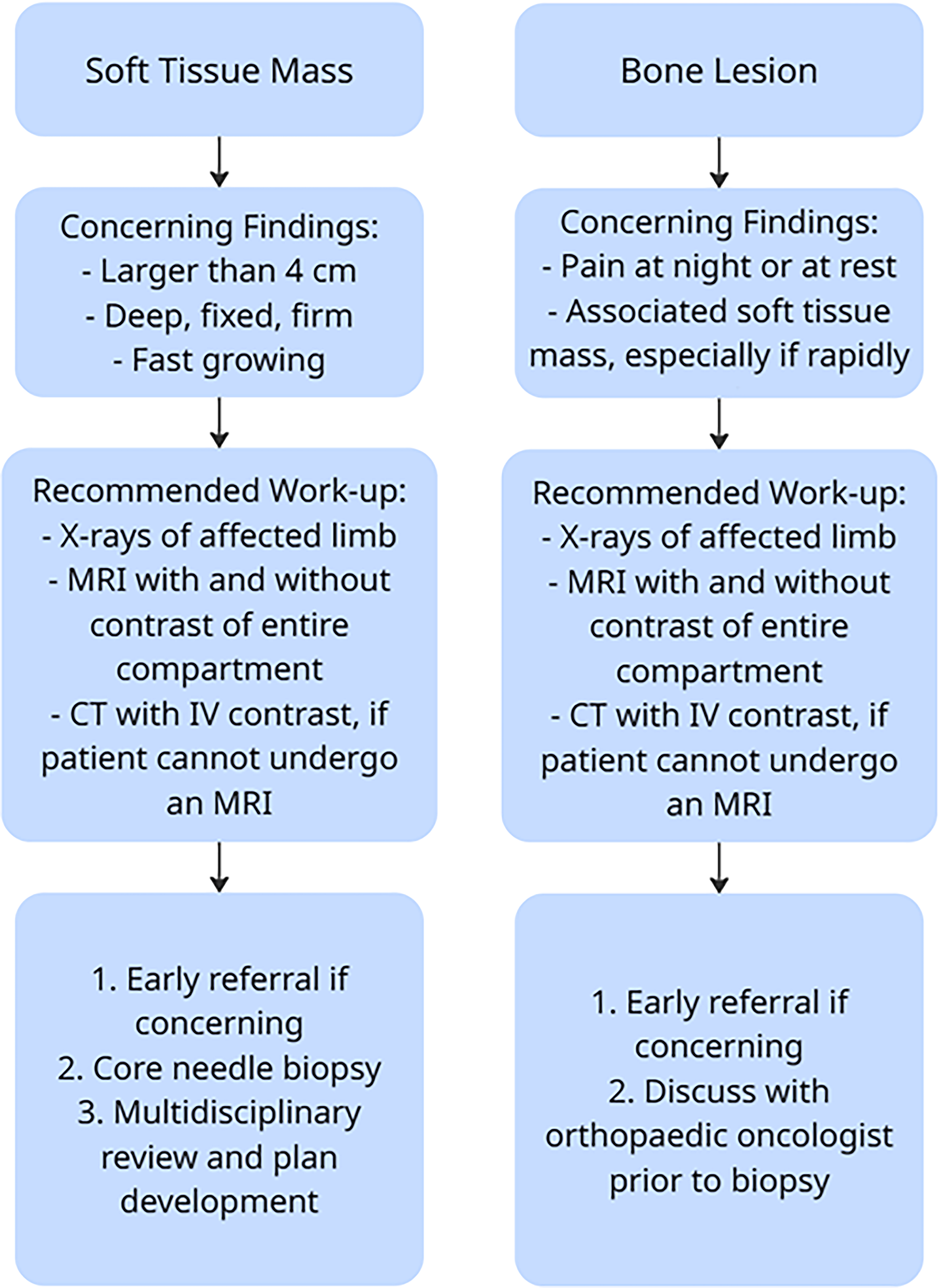
Considerations for the work-up of bone lesions and soft tissue masses in the adolescent and young adult patient. Adapted with the author’s permission from Sarcoma as a Model for Adolescent and Young Adult Care, Reed et al., J Oncol Pract 2019. 13
Once the correct diagnosis is made, treating AYA cancer patients at National Cancer Institute (NCI)-designated cancer centers is critical for optimizing outcomes and addressing the unique needs of this population. 15 In their population-based analysis of California Cancer Registry data for 1674 children and AYAs diagnosed with soft tissue sarcoma between 2000 and 2014, Alvarez et al. found that having treatments at specialized cancer centers was associated with better overall survival among AYAs. 16 AYAs often fall into a care gap between pediatric and adult oncology, facing distinct psychosocial, developmental, and survivorship challenges. Specialized programs at Children’s Oncology Group- or NCI-designated centers are designed to bridge this gap by offering age-appropriate support, clinical trial access, and multidisciplinary care tailored to AYAs’ medical and emotional needs.17,18 From the perspective of community providers, however, while there is often strong support for referring AYAs to specialized centers, barriers such as geographic distance, insurance limitations, and continuity of care concerns can complicate referrals. 19 Moreover, some community clinicians may feel confident managing AYA patients locally, especially when relationships with academic centers are not well established. 20 Interventions that align care delivery with best practices while respecting local provider roles and patient preferences are needed. Digital approaches, expanded telehealth, and outreach programs should be leveraged to strengthen partnerships between community practices and NCI-designated centers.21,22
Participants’ narratives also emphasized the importance of effective communication at the level of patients and their providers. Open, bidirectional dialogue, such as that which occurred for one of the participants in this study who praised the surgeon’s effort to get to know them and engage in a “normal conversation,” cultivates a mutual understanding of treatment goals, values, and life circumstances, which can significantly influence care decisions and adherence. 23 This understanding is especially critical in sarcoma, where treatment pathways may involve trade-offs between aggressive interventions and quality-of-life considerations. Darabos et al. found that young adult cancer patients who developed stronger therapeutic alliances with their providers, as measured by an adapted version of the validated Human Connection Scale, 24 had improved mental health outcomes. 25 Misalignment in priorities, which in our study occurred when providers emphasized clinical outcomes while patients prioritized fertility preservation, mental health, or return to work, can lead to dissatisfaction, reduced trust, and suboptimal care experiences. Therefore, integrating structured communication strategies, such as shared decision-making tools and regular goal-setting conversations, is vital to ensure that care plans reflect what matters most to patients. 26 As surgery was the central treatment event in many of the participants’ experiences, the surgical care team is uniquely positioned to address age-specific needs across the perioperative continuum by improving communication. This approach not only enhances patient satisfaction but may also improve clinical outcomes by promoting engagement and continuity in care. 27 Furthermore, the oncologic surgeon is frequently the physician making the initial diagnosis. This presents an opportunity for surgeons to play an active role in timely referrals to supportive care resources, including oncofertility, psychosocial oncology, and social workers. While surgeons may be less comfortable with these conversations, appropriately educated physicians can be empowered to advocate for their patients and ensure that time-sensitive referrals are placed.
Young adults recovering from cancer surgery often require distinct informational and emotional resources to fully understand their medical care and set realistic expectations for recovery. As an example, participants in this study who had experienced postoperative complications (e.g., infection and lymphedema) reported feeling inadequately prepared for these adverse events. AYA cancer patients may benefit from tailored educational materials that explain surgical procedures, potential complications, and recovery timelines in accessible, developmentally appropriate language. Innovative strategies such as the pilot study described by Masumoto et al., which employed a game-based educational program for childhood cancer survivors and demonstrated significant gains in health management awareness and knowledge compared to baseline among study participants, show promise and warrant further investigation. 28 Additionally, resources that address long-term functional outcomes, psychosocial impacts, and strategies for reintegration into daily life can help young adults form more accurate and empowering expectations. Incorporating peer support, digital tools, and age-specific counseling into postoperative care may further enhance understanding and engagement, ultimately supporting better recovery experiences and outcomes. 29
This study has several limitations worth noting. As a single-center, NCI-designated CCC investigation, the results may not be easily extended to other institutions or care settings. While thematic saturation was achieved with 14 interviews, the small sample impacts the breadth of perspectives captured. The majority of participants were treated by two surgeons, which may have limited the variability of participants’ perspectives with respect to surgical planning and perioperative experiences. Participants varied considerably in age and sarcoma subtype, and although all underwent surgery, their systemic and radiation treatments differed. While reflective of the variability in the presentation and treatment of sarcoma, this heterogeneity may influence experiences and perceptions. This study was intentionally restricted to those with resectable sarcoma, and future studies are needed to understand the experiences of those with unresectable disease to enable consideration of these findings in the context of the broader sarcoma population. Recall bias may also be present, as some participants underwent surgery several years prior to their interview. These factors collectively constrain the ability to draw definitive conclusions and highlight the need for larger, multicenter studies to validate and extend these insights.
Conclusion
This study underscores the complex and multifaceted needs of AYAs with sarcoma, spanning timely diagnosis, specialized referral, effective communication, and tailored educational resources. While participants highlighted areas of excellence in their care, their narratives also revealed persistent gaps that can impact outcomes and quality of life. Addressing these gaps will require coordinated efforts to strengthen diagnostic pathways, expand access to sarcoma-focused centers, and implement structured strategies for shared decision-making and perioperative education.
Authors’ Contributions
Data analysis, manuscript writing and review: S.M. Transcript coding, data analysis, manuscript review: A.A. Conceptualization, interviewing, data analysis, manuscript review: L.R. Transcript coding, data analysis, manuscript review: M.B. Conceptualization, manuscript review: R.H. Conceptualization, manuscript review: A.M. Conceptualization, manuscript writing and review: J.A.
Author Disclosure Statement
S.P.M.: American Society of Clinical Oncology Conquer Cancer Career Development Award, American College of Surgeons Faculty Research Fellowship. A.M.A., L.J.R., M.B., R.H., and A.S.M.: No interests to disclose. J.H.A.: NCCN Panel member.
Footnotes
Funding Information
The projected was funded by an internal Steps for Sarcoma Idea Award.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.