
Abstract
Background:
We analyzed the predictors of marriage and parenthood in our cohort of adult survivors of childhood cancer.
Methods:
We conducted a retrospective cohort analysis of adult survivors of childhood cancer aged > 25 years at a tertiary cancer center in India, evaluating marital status, parenthood, and associated predictors using multivariable logistic regression.
Results:
Among 844 survivors, 36.4% of males and 37.6% of females were ever married. On multivariable analysis, male sex (odds ratio [OR] 0.58, 95% confidence interval [CI] 0.41–0.83, p = 0.003) and diagnosis of central nervous system (CNS) tumor/retinoblastoma (OR 0.42, 95% CI 0.22–0.81, p = 0.009) were associated with lower likelihood of marriage, while employment was strongly associated with higher likelihood (OR 3.75, 95% CI 2.62–5.37, p < 0.001).
Among married survivors, treatment before 2000 was associated with a higher likelihood of parenthood (OR 3.94, 95% CI 2.20–7.06, p < 0.001), while other treatment-related factors were not significantly associated. Highly gonadotoxic treatment (OR 2.19, 95% CI 1.22–3.93, p = 0.01) was associated with use of assisted reproductive technology.
Conclusions:
Sociodemographic and temporal factors, particularly employment and treatment era, were the primary determinants of marriage and parenthood in this cohort.
Introduction
Advances in the diagnosis and treatment of childhood cancer have led to improved survival world-wide; 80% of children treated in high-resource settings are expected to be long-term survivors.1,2 Certain treatment exposures in children and adolescents with cancer may lead to gonadal insufficiency, suboptimal fertility outcomes, and sexual dysfunction.3–12
Survivors of childhood cancer may also be less likely to marry and have children compared to normal/sibling comparator cohorts, although the likelihood varies by diagnosis, other clinical factors, and treatment exposures.13,14 Predictors of not being married have included male sex, history of central nervous system tumors, receipt of cranial radiotherapy, mental disability, poor physical functioning, blindness, or low social functioning scores.13–16 Divorce patterns in survivors are reported to be similar to peers. 13 While several treatment factors are known to affect fertility in survivors of childhood cancer, there is no increased incidence of congenital anomalies in children born to survivors of childhood cancer.17–19
Most literature regarding fertility, marital and reproductive outcomes use data from cohorts in North America and Europe; with limited data from India and other low-middle income countries (LMICs).13–21 We analyzed the marital status and reproductive outcomes in our cohort of adult survivors of childhood cancer.
Methods
The After Completion of Treatment Clinic at the Tata Memorial Centre serves 5-year survivors of childhood cancer (age <18 years at diagnosis) who are currently at least 2 years in remission. 22 Survivors undergo risk-based, exposure-related surveillance for long-term effects of cancer and its treatment using a modified version of the Children’s Oncology Group guidelines. 23
This was a retrospective cohort analysis of adult survivors of childhood cancer, current age >25 years, treated at a single tertiary cancer center.
Data regarding demographics, treatment exposures, pubertal status, menstrual history, marital status, sexual dysfunction, and parenthood were extracted from the clinic database, electronic medical records, and patient files. History of any health problems attributable to cancer diagnosis and treatment or other causes was noted. Specific treatment details included cumulative cyclophosphamide equivalent dose (CED), which was calculated using a standard definition, 10 surgeries involving the HP-axis, pelvis, and gonads and site, dose and field of radiation.
Highly gonadotoxic treatment was defined as either CED >8 g/m2, hematopoetic stem cell transplant involving an alkylator +/- total body irradiation, myeloablative and reduced intensity conditioning, hypothalamic radiation >30 Gy, any testicular, ovarian radiation, or surgery involving bilateral gonad removal or within the HP region.6–9 The primary objectives were to evaluate (i) ever-married status and (ii) reproductive outcomes (parenthood and infertility) among adult survivors of childhood cancer >25 years of age and to identify demographic and treatment-related predictors associated with these outcomes. 24 Survivors aged >25 years were included to ensure adequate opportunity for marriage and reproductive outcomes within the sociocultural context where these events typically occur in early adulthood.
Impaired spermatogenesis was defined as either azoospermia or oligospermia (less than 15 million sperms per mL of semen). 10 Primary gonadal failure in males was defined as decreased testosterone concentrations along with elevated luteinizing hormone and serum follicular-stimulating hormone (FSH) levels or failure to develop signs of puberty by age 14. 11 Diminished ovarian reserve was defined as low values for serum anti-mullerian hormone and/or antral follicular count for age. Premature ovarian insufficiency (POI) was defined as amenorrhea for >4 months and 2 elevated levels of FSH in the menopausal range in any adult female <40 years of age. 9 “Ever-married” was defined as individuals who had been married at any point (including currently married, divorced, or widowed). Parenthood was defined as having biological offspring. Information on assisted reproductive technologies was not systematically captured in the earlier years and therefore not separately analyzed. Documented infertility was defined as a clinical diagnosis recorded in medical records OR failure to conceive after ≥12 months of unprotected intercourse. 24
Statistical analysis
Results for continuous variables are expressed as median with range or mean (±standard deviation), and categorical variables are expressed using frequencies and percentages. For comparison of trends in cumulative incidence of late effects, a p value < 0.05 was considered significant, and all p values were two-sided. Multivariable logistic regression models were constructed to identify predictors of (i) ever-married status and (ii) reproductive outcomes. Covariates included age, sex, diagnosis, treatment exposures (including cranial radiation), and socioeconomic indicators where available. Variables were selected based on clinical relevance and univariable p < 0.1. Multivariable analyses were performed adjusting for potential confounders. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Analyses were conducted using IBM SPSS version 24. A two-sided p value < 0.05 was considered statistically significant. Model diagnostics, including assessment for multicollinearity and overall goodness-of-fit, were evaluated to ensure the stability and validity of the regression models. Missing data were handled using complete-case analysis.
This study was approved by the Institutional Ethics Committee at the Tata Memorial Centre, and a waiver of informed patient consent was granted due to the retrospective nature of the study and use of de-identified data.
Results
The analysis included 844 survivors aged >25 years—210 female and 634 male. Table 1 shows the clinical and demographic profile of this cohort. The median age at cancer diagnosis was 9 years, with a current median age of 29 years (range 25–60 years). The most common diagnosis was acute lymphoblastic leukemia (29%), followed by Hodgkin lymphoma (19.8%), Ewing sarcoma (9.1%), and non-Hodgkin lymphoma (8.8%). About one-third (34.9%) of survivors had treatment exposures placing them at high risk of gonadotoxicity.
Demographics and Outcome of Adult Survivors >25 Years (n = 844)
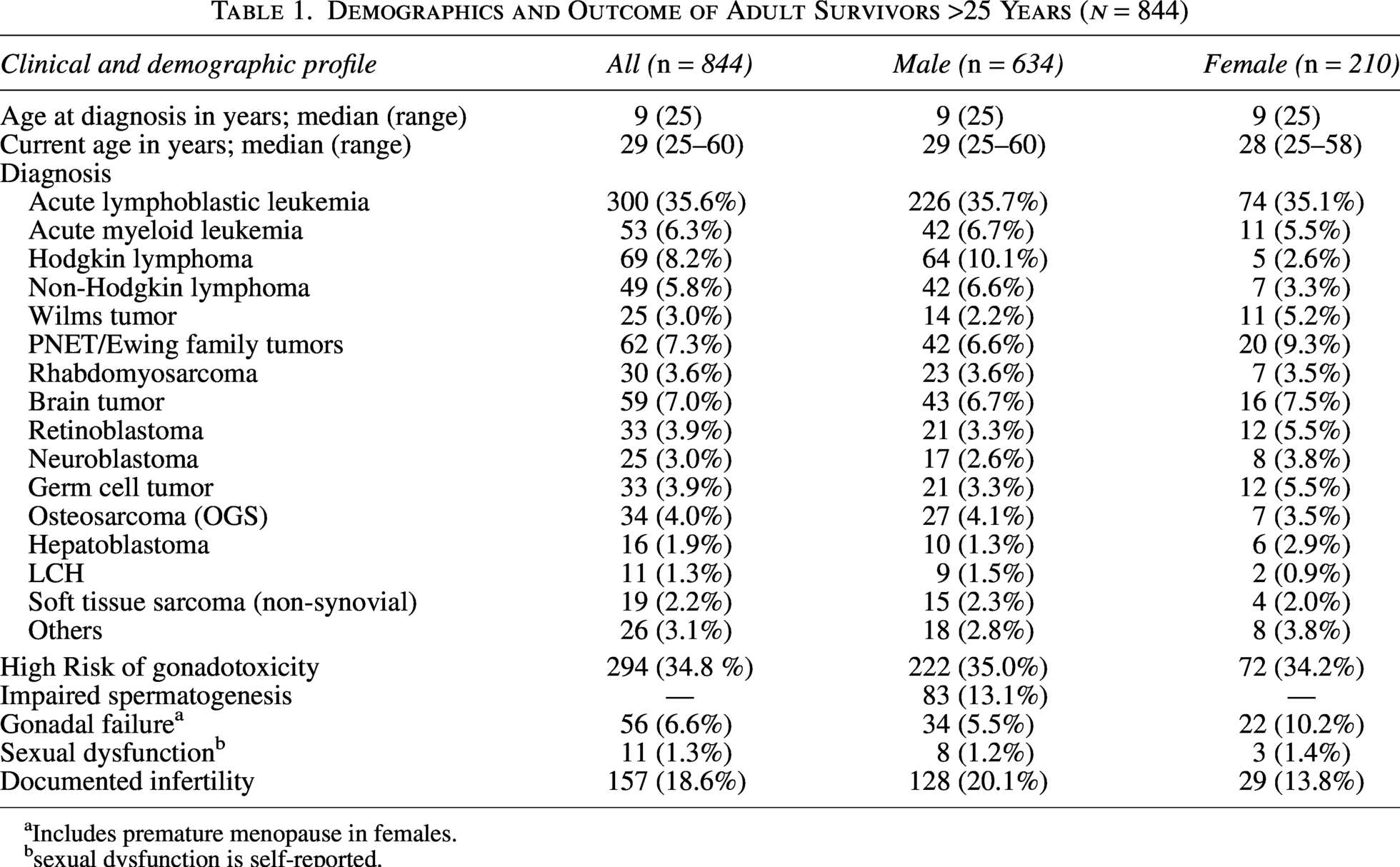
Includes premature menopause in females.
sexual dysfunction is self-reported.
Marital status and predictors of marriage
Of the 634 male survivors aged >25 years, 231 (36.4%) were ever married. At last follow-up, 224 (35.3%) were married, 7 (1.1%) divorced and 2 widowed. The spouse was aware of the cancer diagnosis in 44 (19%) marriages (Table 2).
Marital Status and Parenthood in Survivors Aged 25 Years (n = 844)
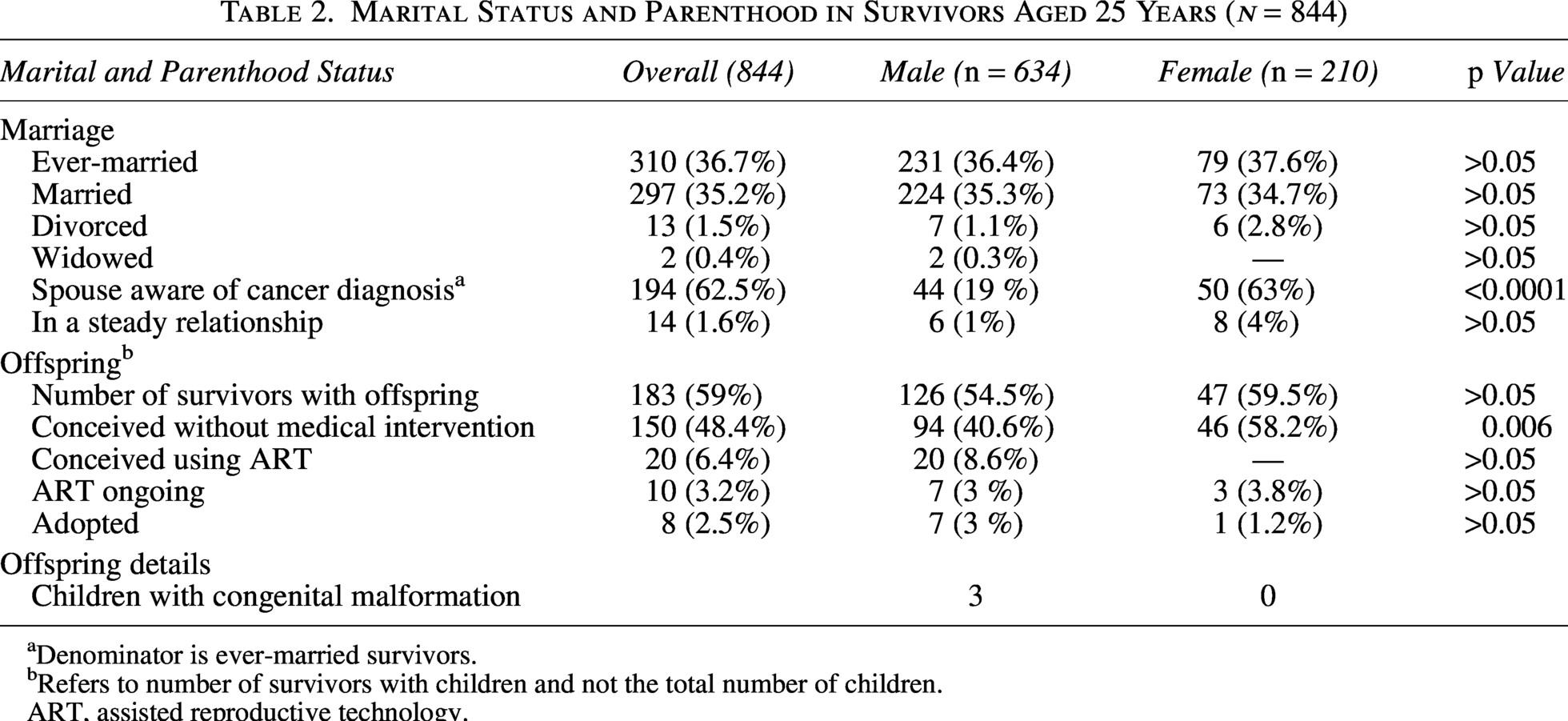
Denominator is ever-married survivors.
Refers to number of survivors with children and not the total number of children.
ART, assisted reproductive technology.
Of the 210 female survivors aged >25 years, 79 (37.6%) were ever married. At last follow-up, 73 (34.7%) were married, and 6 (2.8%) divorced. The spouse was aware of the cancer diagnosis in 50 (63%) marriages, which was higher than in male survivors (Table 2).
There are only four marriages among cancer survivors, one of which ended in a divorce. No same-sex relationships have been reported.
On multivariable analysis, male sex (OR 0.58, 95% CI 0.41–0.83, p = 0.003) and diagnosis of CNS tumor/retinoblastoma (OR 0.42, 95% CI 0.22–0.81, p = 0.009) were associated with a lower likelihood of being ever married. Employment was strongly associated with a higher likelihood of marriage (OR 3.75, 95% CI 2.62–5.37, p < 0.001). Cranial radiation and pelvic/gonadal radiation were not significantly associated with marital status (Table 4).
Predictors of Ever Being Married, Parenthood and Assisted Reproductive Technology Use
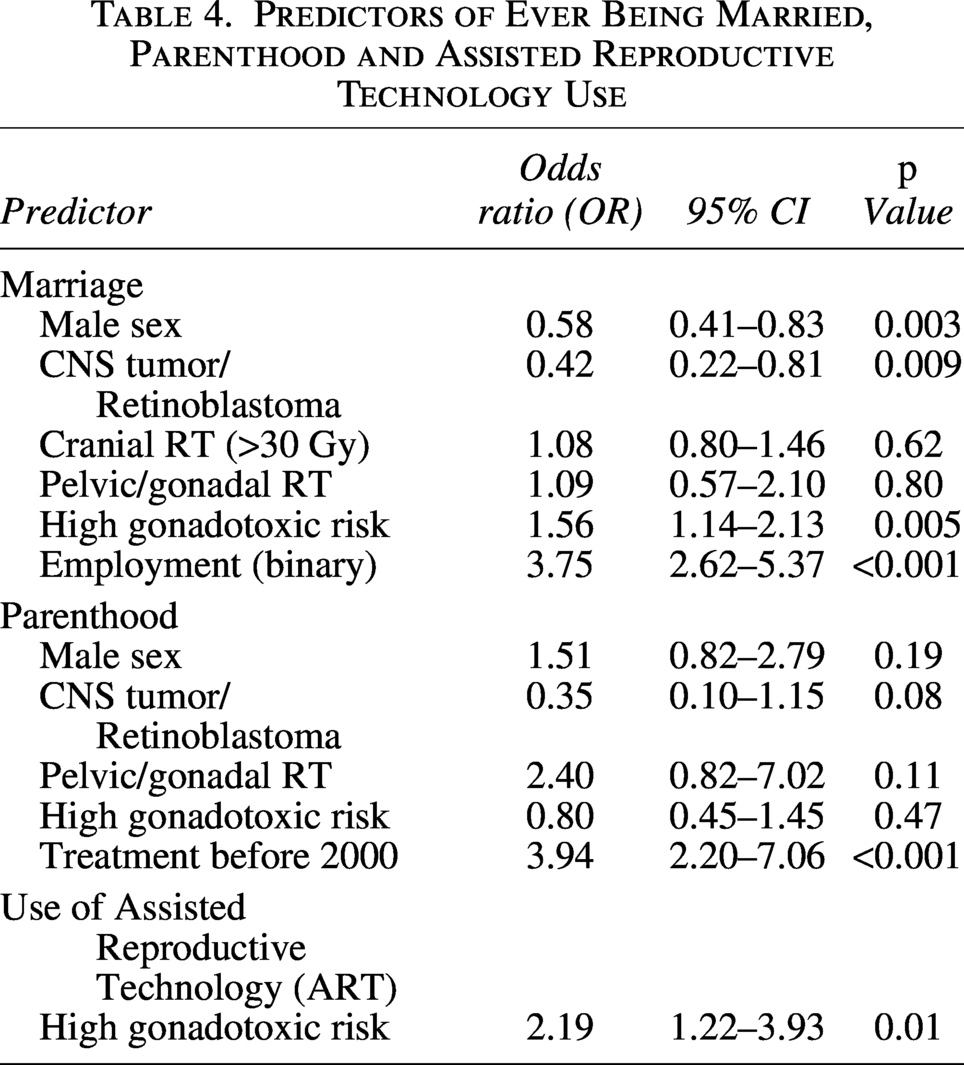
The proportion of married survivors was similar between sexes (males OR 0.95, 95% CI 0.87–1.03, p = 0.11). The presence of neurocognitive impairment (OR 0.82, 95% CI 0.41–1.65, p = 0.36), psychiatric issues OR 1.10, 95% CI 0.65–1.87, p = 0.4), hypogonadism (OR 1.16, 95% CI 0.69–1.95, p = 0.33) and receipt of pelvic/gonadal radiation (OR 1.175, 95% CI 0.67–2.06, p = 0.338) were not predictors of being married (Table 4).
Reproductive outcomes and parenthood
Documented infertility was present in 18.7% overall (20.2% in males, 13.5% in females). Impaired spermatogenesis was identified in 13% of males, while gonadal failure (including POI in females) was reported in 6.6% overall: 34 (5.5%) males and 22 (10.2%) females. Among married survivors, 59% had children. Among married males, over half—126 (54.5%)—were documented to have offspring, conceived without medical intervention in 94 (40.6%) and conceived after assisted reproduction (ART) in 20 (8.6%). Seven male survivors adopted children. Thirty survivors were documented to have tried ART without success (Table 3). Sexual dysfunction was documented in only 11 survivors.
Marital Status by Decade of Treatment
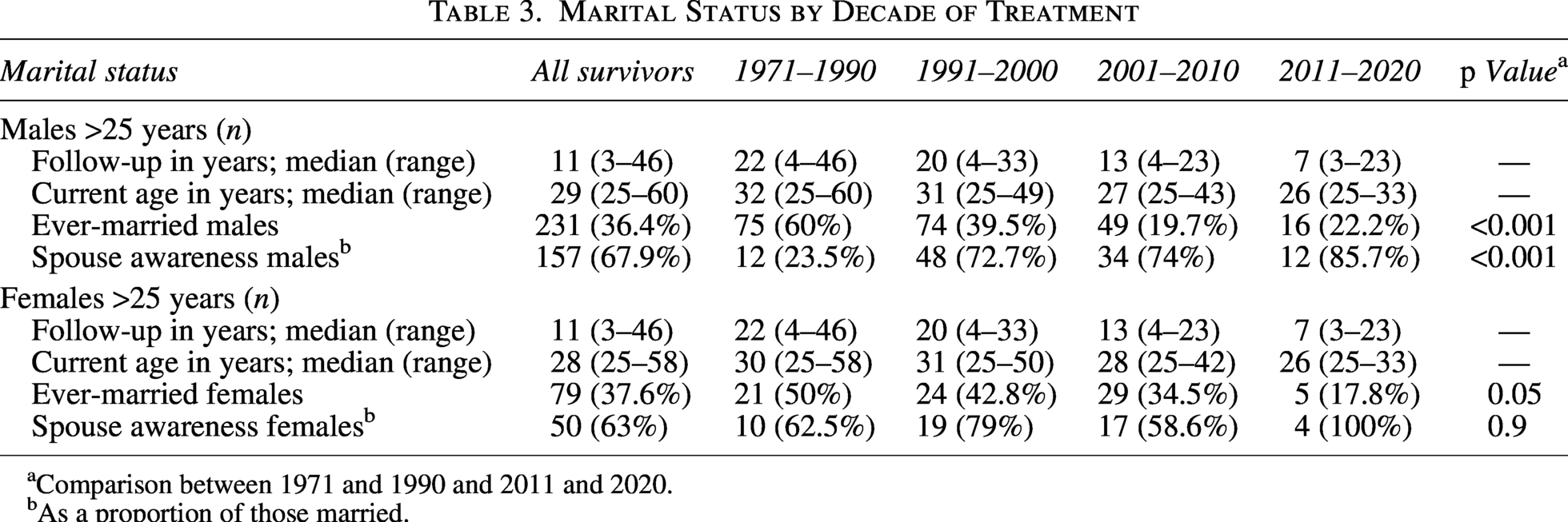
Comparison between 1971 and 1990 and 2011 and 2020.
As a proportion of those married.
Forty-seven (59.5% of) married women were documented to have offspring, conceived without medical intervention in all except one, where the child was adopted due to fear of genetic transmission. Three survivors are pursuing donor-assisted reproduction. Two female survivors (one has connective tissue disorder) had multiple miscarriages (Table 3).
In multivariable analysis (n = 308), treatment before 2000 was significantly associated with a higher likelihood of parenthood (OR 3.94, 95% CI 2.20–7.06, p < 0.001). Other variables including sex, gonadotoxic risk, pelvic/gonadal radiotherapy, and diagnosis were not significantly associated with parenthood (Table 4). ART use was higher in those at high risk of gonadotoxicity (OR 2.191, 95% CI 1.22–3.93 p = 0.01).
Offspring
All offspring of female survivors are documented to be normal. Three male survivors had children with congenital anomalies—meningomyelocele, suspected Marfan syndrome, and imperforate anus. All babies were conceived without medical intervention and >20 years after the father’s cancer treatment.
Trends over successive decades
The proportion of ever-married men declined across decade of treatment—from 60% (1971–1990) to 40% (1991–2000), 20% (2001–2010), and 22% (2011–2020) (p < 0.001). Spousal awareness improved over time: only 24% of spouses were aware of the survivor’s cancer diagnosis in the earliest era, compared to 73%–86% in later decades. The proportion of ever-married women decreased from 50% (1971–1990) to 43% (1991–2000), 35% (2001–2010), and 18% (2011–2020) (p = 0.05). Unlike males, spousal awareness in women remained consistently higher (60%–100%) across decades, without a clear trend (Table 3).
Discussion
While reports from North America and Europe describe suboptimal fertility, marital and reproductive outcomes in cohorts of childhood cancer survivors,3–5,13–21 there is limited data from other parts of the world. In our cohort, about one-third were ever married (36.7%), with no significant sex difference (36.4% males vs. 37.6% females) and divorce reported in <2%.
A substantial proportion—around two-thirds—of survivors aged >25 years in our cohort (median age 29 years in male, and 28 years in females) remained unmarried. While the median age at marriage in India is approximately 22 years for women and 25 years for men, the absence of a comparator population limits direct conclusions regarding differences from the general population. Employment emerged as the strongest predictor of marriage, highlighting the potential importance of financial independence and socioeconomic stability during the transition to adult roles among AYA cancer survivors. Survivors exposed to highly gonadotoxic therapies were not less likely to marry in our cohort; this may reflect residual confounding or sociocultural factors and warrants further exploration. Literature suggests that survivors of child, adolescent and young adult cancers, especially CNS tumors and retinoblastoma, are less likely to marry than siblings, and non-marriage is associated with cranial radiation, worse task efficiency, short stature, and poor physical function.13–16,25
Importantly, a subset of male and female survivors in our cohort did not disclose the history of cancer diagnosis and treatment to their prospective partners or spouses. A cancer diagnosis may carry social stigma in some settings, which may influence survivors or families in decisions regarding disclosure of medical history to prospective partners.26,27 Only 19% of male survivors’ spouses were aware of their cancer history, compared to 63% of female survivors’ spouses. Cancer-related stigma has been reported to affect women disproportionately in India and other LMICs, 28 and further qualitative analysis will help elucidate the contradictory findings in our study. Fortunately, spousal awareness increased over the decades in both males and females.
A substantial proportion of survivors had fertility-related late effects, especially males, with one in five facing infertility. Female survivors, while fewer, showed higher rates of gonadal failure than males. Less than half (40.6%) of males are documented to have offspring without medical intervention, with at least 50 (7.9%) having tried ART. Given the relatively young median age of the cohort, longer follow-up will be required to fully characterize reproductive outcomes. Reproductive outcomes seem to be higher in females, with only three survivors pursuing donor-assisted reproduction. A higher proportion of survivors treated in earlier decades, especially prior to 2000, were married. This observation may partly reflect differences in age distribution and duration of follow-up between treatment eras, as well as possible changes in societal patterns of marriage over time.
None of the babies born to our survivors is reported to have cancer. Three male survivors had children with congenital anomalies, which appear unrelated to the father’s cancer diagnosis or treatment; data from larger cohorts document no increase in congenital anomalies as a result of cancer treatment received by parents.17–19
Limitations of the study
While this article has shortcomings inherent to retrospective data collection over several decades with significant under-reporting of certain outcomes and lack of comparator cohort, this is a real-world report of the marital status and reproductive outcomes from India. Additionally, the absence of a comparator group and restricting reproductive outcomes to married survivors may limit direct inference regarding relative risks compared to the general population. Sexual health concerns may also be underreported in survivorship settings, particularly in sociocultural contexts where discussions regarding sexual health may be limited.
Implications for India and other resource-limited settings
The results of our study also highlight the large proportion of newly diagnosed and relapsed patients who receive highly gonadotoxic treatment but did not undergo fertility preservation. Oncofertility in adolescents and children remains an underserved area in India, and current initiatives seek to improve reproductive outcomes in survivors of childhood cancer.29,30
Conclusions
Gonadotoxicity and reproductive dysfunction remain a real concern in survivors of childhood cancer. Despite the reduction of gonadotoxic exposures in contemporary protocols, a substantial proportion of children being treated in the current era remain at high risk of gonadotoxicity. There is an urgent need to recognize patients on treatment and survivors who would benefit from fertility preservation and gonadotoxicity surveillance. The findings of this study underscore the importance of addressing fertility, relationships, and psychosocial well-being as integral components of long-term survivorship care for adolescents and young adults treated for childhood cancer.
Authors’ Contributions
MP conceptualized and designed the study, performed data collection and analysis, interpreted the data, drafted the initial manuscript, revised the manuscript critically for important intellectual content, and served as the corresponding author. VRMG contributed to clinical management of patients, assisted with data interpretation, and critically reviewed and revised the manuscript. SG contributed to clinical care and study implementation and critically reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript and agree to be accountable for all aspects of the work.
Ethics Approval and Consent to Participate
Approved by Institutional Ethics Committee.
Availability of Data
Available on request.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.