
Abstract
Background:
Adolescents and young adults (AYAs; 15–39 years) with cancer face unique ethical challenges. Variations in ethics consultations (ECs) among different AYA age groups remain understudied, despite evolving developmental and psychosocial milestones.
Methods:
A 10-year retrospective review at an academic medical center examined EC cases in AYA oncology patients. Ethicists categorized ethical issues using an institutional 5 domains, 23-category classification schema Decisional Processes, Medical/Surgical Treatments, Patient/Family Behavior, Professional Issues, and Information/Communication. Categories included surrogate decision-making, informed consent, pain management, and resuscitation status/do-not-resuscitate (DNR) order. Multiple categories could be documented per EC. Primary outcomes were (1) the distribution of categories across domains and (2) the prevalence of specific categories among patients, compared across age groups (15–21, 22–29, and 30–39 years) using χ2 or Fisher’s exact tests (α = 0.05).
Results:
Among 59 ECs (mean patient age 26.4 ± 7.1 years; 52.5% female), Decisional Processes accounted for 41% of category applications, followed by Medical/Surgical Treatments (25%), Patient/Family Behavior (12%), Professional Issues (12%), and Information/Communication (9%). A total of 153 categories were recorded. The most common were surrogate decision-making (45%), quality-of-life (QoL) considerations (37%, including QoL deliberations [20%] and treatment-related QoL concerns [17%]), informed consent (20%), and DNR (18%). The distribution was consistent across age groups, except for pain control, observed only in 22–29-year-olds (3/16; p = 0.014).
Conclusion:
Decision-making primarily drove EC with consistent patterns across the AYA spectrum, except for pain control in 22–29-year-olds. Findings emphasize the need for structured decision-making approaches and age-specific pain management in AYA oncology.
Keywords
Introduction
Medical complexities in cancer care continue to grow as health care and technology advance, making decision-making more challenging and complicating treatment choices and quality of life (QoL). Ethics consultation (EC), established approximately 40 years ago, has expanded to many United States hospitals as a resource to support decision-making, address moral uncertainty, and resolve value conflicts. 1
Oncology care involves numerous ethical considerations—some common across all age groups and others specific to certain ages.2–5 Adolescents and young adults (AYAs; 15–39 years) face unique ethical challenges influenced by developmental changes, increased independence, family roles, and financial pressures.2–6 This population represents the largest uninsured age group.6–8 Although they are often grouped—possibly because they have experienced fewer mortality improvements than pediatric and older adult groups7,8—we hypothesize that ethical issues prompting consultations may differ across AYA subgroups. Addressing this gap could enhance anticipatory guidance, standardize documentation, and improve smooth transitions from pediatric to adult care—especially important given the high rates of disengagement.9,10 We aimed to understand the following:
What ethical concerns most often lead to AYA oncology EC? How consistent are consultation patterns throughout the AYA age range? What trends can help standardize documentation and proactive support during AYA oncology care?
Methods
Study design
We conducted a single-center, registry-based retrospective cohort study of ECs for AYAs with cancer at Cleveland Clinic from January 1, 2014, to December 31, 2023. Data were extracted from an Institutional Review Board (IRB)-approved registry maintained by the Center for Bioethics (IRB 6007; approved February 21, 2003). As a secondary analysis of de-identified registry data, additional IRB approval was not required.
EC service
The Cleveland Clinic Center for Bioethics employs 10 full- or part-time clinical ethicists and up to 4 fellows who staff an EC service covering all hospitals and outpatient clinics across Ohio, with additional support for other Cleveland Clinic markets in the United States and internationally. All consultations included in this analysis were conducted by clinical ethicists through the EC services (ECS), a hospital-based clinical service integrated into patient care and distinct from hospital ethics committees. Consultation requests may be initiated by patients, families, or care team members submitted through the electronic medical record, phone, or paging system. All consultations follow a standardized workflow and are documented in accordance with the American Society for Bioethics and Humanities Core Competencies. 1 Each consultation is logged in a centralized registry that supports patient care, quality improvement, education, and research (Supplementary Appendix SA1, Registry Variables).
Study population
We identified 59 unique patients aged 15–39 years with documented oncologic diagnoses who received EC during the study period. Nononcology cases and records lacking sufficient detail to classify ethical issues were excluded. When multiple consultations occurred within the same care episode, they were combined into a single instance per patient, resulting in 59 patients with 59 ECs.
Ethical issues classification
Ethical issues were classified using an institutional schema comprising 5 domains and 23 specific categories that were applied by clinical ethicists at the time of consultation within the EC registry (Fig. 1). The schema was developed iteratively by clinical ethicists within the ECS to capture recurrent mid-level ethical issues encountered in practice and to support service evaluation and education. Although conceptually aligned with prior pediatric EC typologies, it was not derived from a single externally standardized taxonomy and was designed for clinical coding. Previous pediatric EC studies have generally used related but methodologically distinct retrospective narrative or thematic approaches.11,12
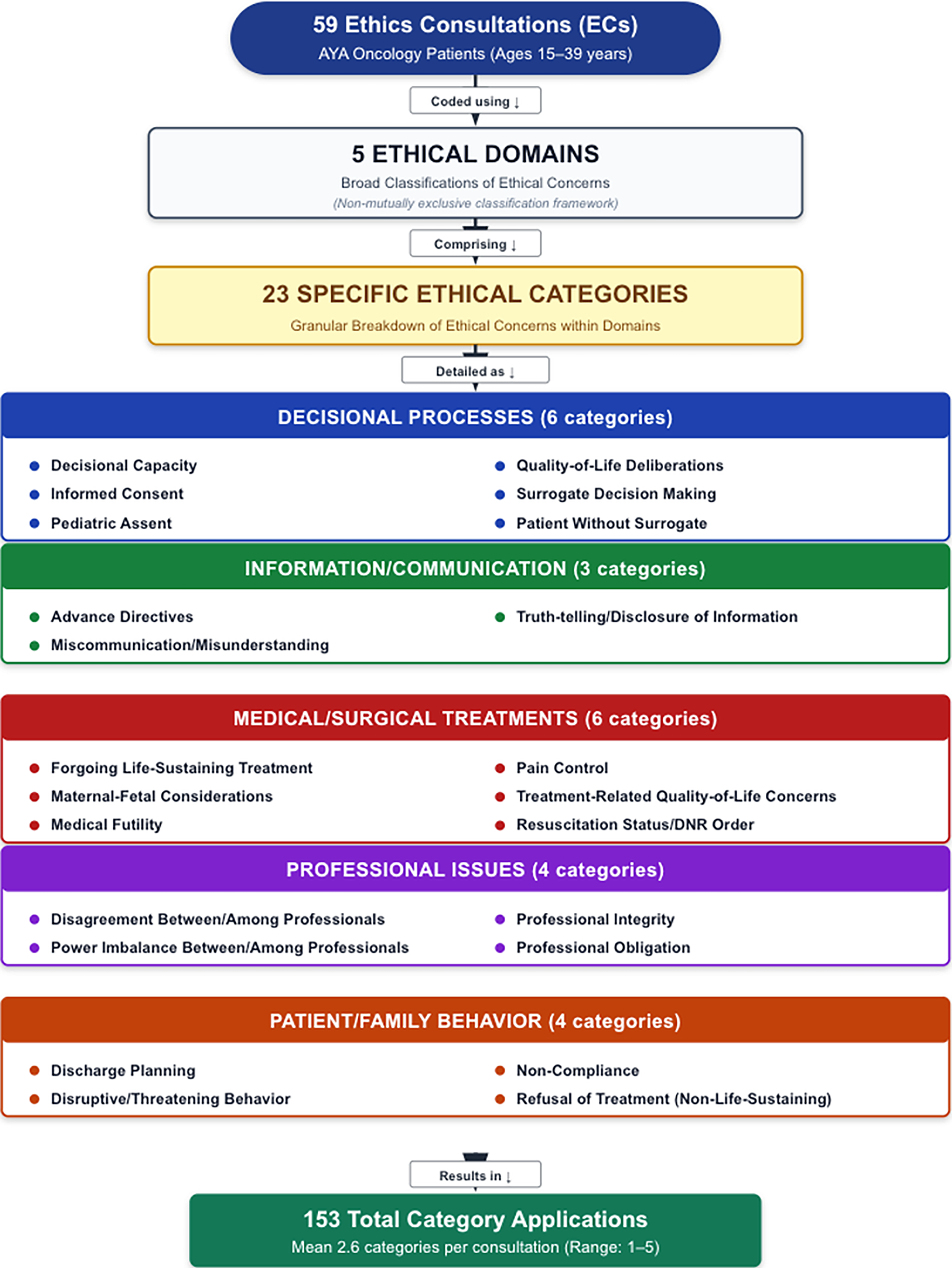
Ethics Consultation Classification Scheme. Cleveland Clinic’s institutional ethics consultation (EC) classification schema includes five ethical domains: Decisional Processes, Information/Communication, Medical/Surgical Treatments, Professional Issues, and Patient/Family Behavior. These domains are divided into 23 nonmutually exclusive categories. Each EC may be assigned multiple categories, reflecting the complexity of ethical challenges in adolescent and young adult oncology. This resulted in 153 category applications across 59 ECs, with an average of 2.6 categories per consultation (range: 1–5). Two QoL categories are identified: “QoL Deliberations” within Decisional Processes, considering QoL in decision-making, and “Treatment-Related QoL Concerns” within Medical/Surgical Treatments, addressing how therapies affect QoL. The category medical futility is retained as the original label used in the consultation registry and is interpreted here as disputes regarding nonbeneficial, disproportionate, or potentially medically inappropriate treatment, including cases in which an intervention was unlikely to achieve its intended physiological goal. AYA, adolescents and young adults; DNR, do-not-resuscitate; EC, ethics consultation; QoL, quality of life.
The five domains are Decisional Processes, Information/Communication, Medical/Surgical Treatments, Professional Issues, and Patient/Family Behavior. Within these domains, the 23 categories represent specific ethical concerns. Decisional processes included decisional capacity, informed consent or assent, surrogate decision-making, and patients without surrogates. Information/communication included advanced directives, misunderstanding or miscommunication, confidentiality, genetics, medical error, and truth-telling/disclosure. Medical/surgical treatments included forgoing life-sustaining treatment, treatment-related QoL concerns, pain control, maternal-fetal issues, and medical futility. In this study, the term medical futility denotes disputes regarding potentially inappropriate or nonbeneficial treatment, including intervention considered medically inappropriate or unlikely to achieve the intended physiological goal. Professional issues included disagreement among clinicians, power imbalances, professional integrity, and professional obligation. Patient/family behavior included disruptive or threatening behavior, nonadherence, refusal of nonlife-sustaining treatment, and discharge-planning challenges that complicated safe, coordinated care. Categories were binary, marked as either present or absent. They were not mutually exclusive and lacked hierarchical order; ethicists identified up to five categories per consultation to reflect overlapping ethical concerns. Across 59 consultations, this totaled 153 category applications, averaging 2.6 category assignments per EC. There were two distinct QoL categories within this framework, each associated with a different domain, which are neither mutually exclusive nor consistently overlapping. Inclusion of both QoL deliberations (within the decisional processes domain) and treatment-related QoL concerns (within the medical/surgical treatments domain) allowed for a more complete perspective on QoL-related ethical issues in decision-making and treatment contexts.
Statistical analysis
The unit of analysis was each EC for the 59 patients. Patients were divided into three age groups (15–21, 22–29, and 30–39 years), in line with international AYA oncology definitions.2,7,13 First, to assess domain workload, we examined the distribution of 153 category applications across the 5 domains. For each domain, we compared the proportion of applications within that domain to the combined proportions across all other domains, by age group, using Pearson χ2 tests on 3 × 2 contingency tables (age group × domain membership).
Second, to assess the prevalence of specific ethical concerns and evaluate pattern consistency across the AYA age range, we examined the proportion of patients (N = 59) experiencing at least one occurrence of each of the 23 categories and compared these proportions across age groups using Pearson χ2 tests or Fisher’s exact tests (when expected cell counts were <5) on 3 × 2 contingency tables (age group × category presence/absence).
Considering the exploratory nature of this analysis and the a priori hypothesis about age-related differences in ethical concerns, no adjustment for multiple comparisons was made. However, with 23 comparisons, the probability of Type I error increases, and any significant results should be viewed as hypothesis-generating. All statistical tests were two-tailed with α = 0.05. Analyses were performed using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
The average age was 26.4 ± 7.1 years: 16 (27.1%) were 15–21 years old, 16 (27.1%) were 22–29 years old, and 27 (45.8%) were 30–39 years old. Most patients were female (31/59; 52.5%), single (61.0%), and spoke English (96.6%). Approximately 40.7% identified as White, and 25.4% as Black or African American (Table 1).
Characteristics of Adolescents and Young Adults Oncology Patients Undergoing Ethics Consultations (N = 59) at the Cleveland Clinic from January 1, 2014, to December 31, 2023
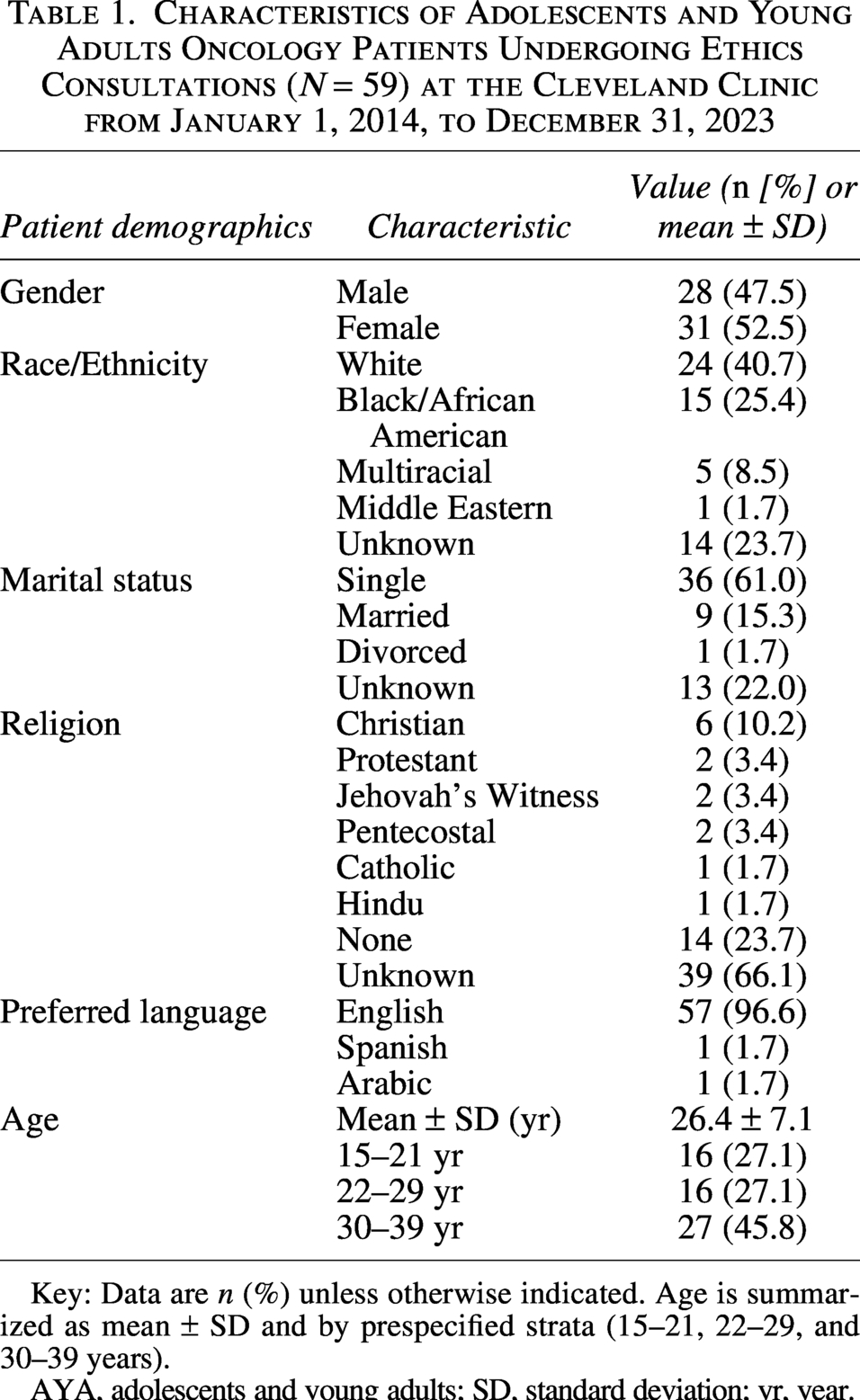
Key: Data are n (%) unless otherwise indicated. Age is summarized as mean ± SD and by prespecified strata (15–21, 22–29, and 30–39 years).
AYA, adolescents and young adults; SD, standard deviation; yr, year.
Distribution of ethical issues across domains
Out of 153 total category applications documented across all 59 consultations, Decisional Processes represented the largest share (64/153; 41.8%), followed by Medical/Surgical Treatments (38/153; 24.8%), Patient/Family Behavior (19/153; 12.4%), Professional Issues (18/153; 11.8%), and Information/Communication (14/153; 9.2%; Fig. 2A and Table 2). This domain-level distribution illustrates the composition of ethical issues driving consultation activity.
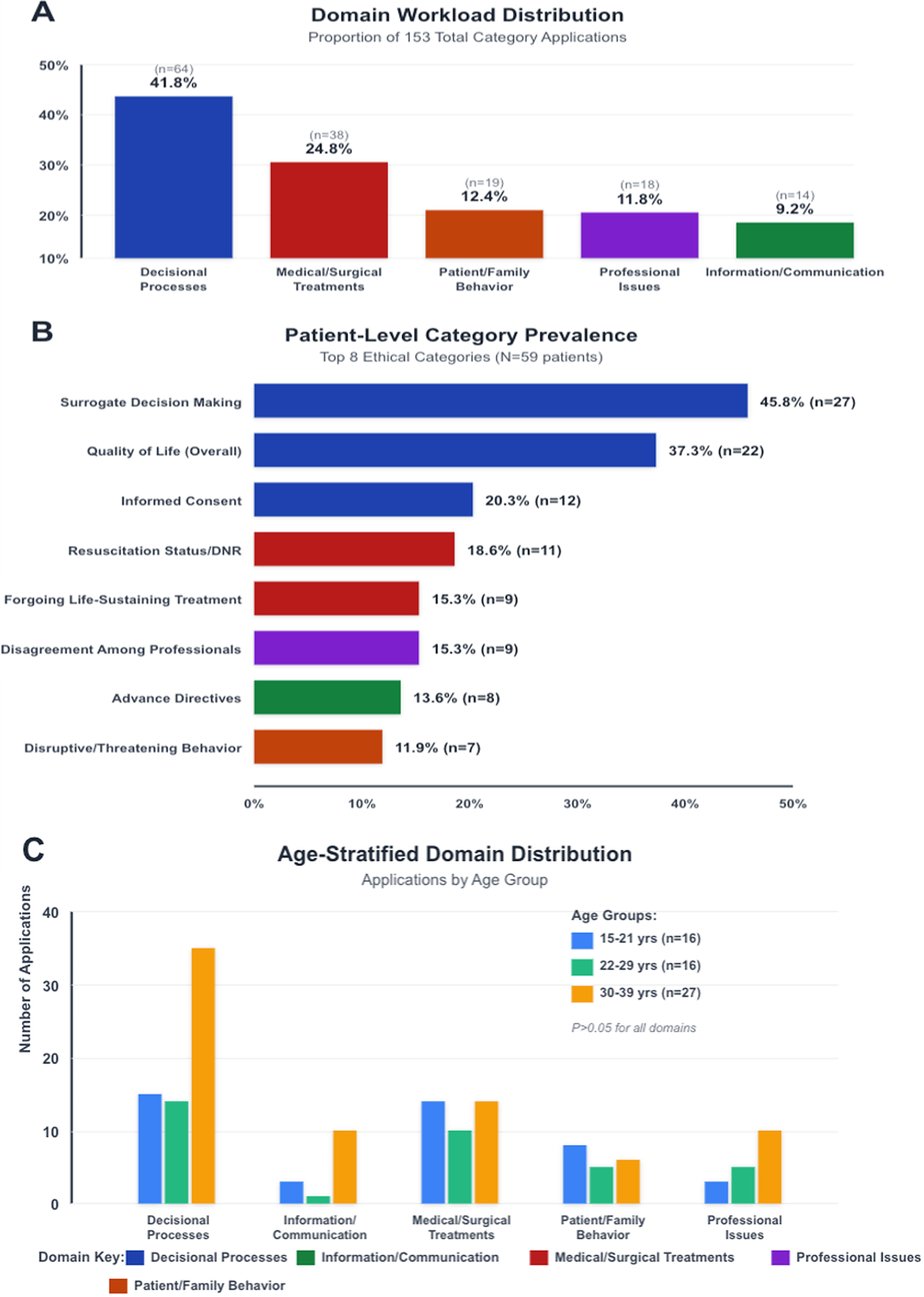
Ethics Consultation Patterns in AYA Oncology. Panel
Domain Workload Distribution by Age Group (Category Applications, N = 153)
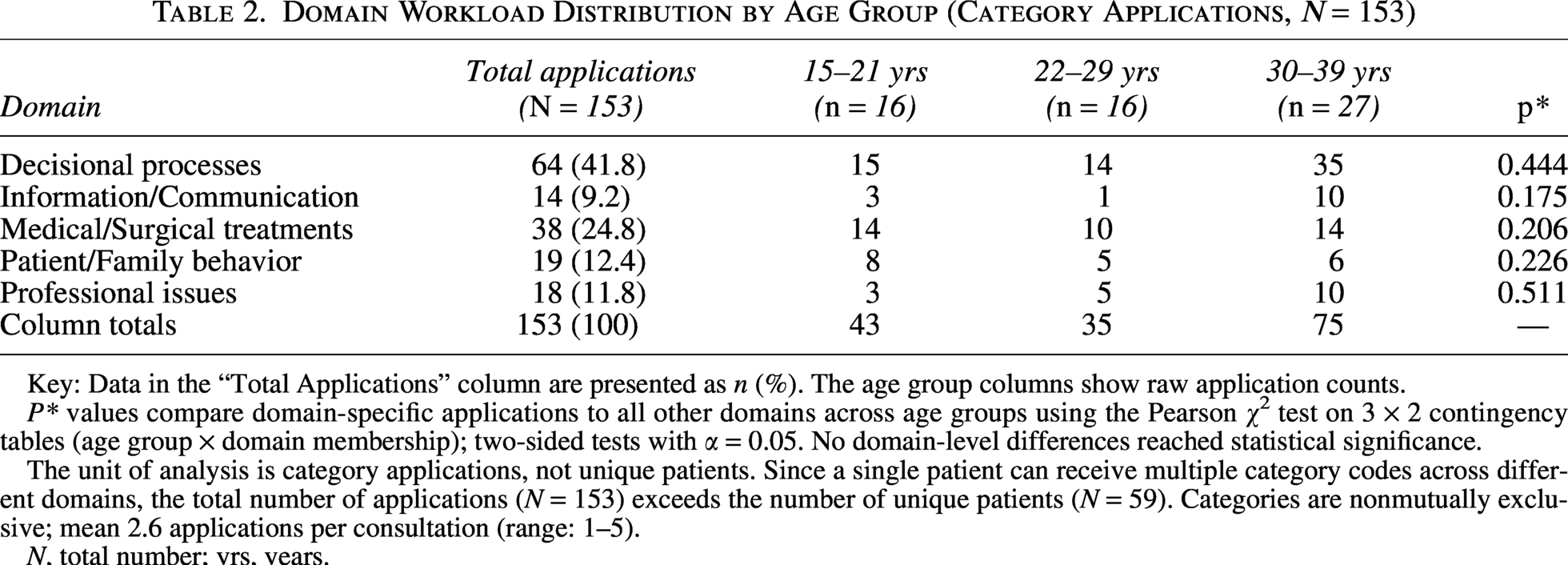
Key: Data in the “Total Applications” column are presented as n (%). The age group columns show raw application counts.
P* values compare domain-specific applications to all other domains across age groups using the Pearson χ2 test on 3 × 2 contingency tables (age group × domain membership); two-sided tests with α = 0.05. No domain-level differences reached statistical significance.
The unit of analysis is category applications, not unique patients. Since a single patient can receive multiple category codes across different domains, the total number of applications (N = 153) exceeds the number of unique patients (N = 59). Categories are nonmutually exclusive; mean 2.6 applications per consultation (range: 1–5).
N, total number; yrs, years.
Category prevalence among patients
At the patient level, surrogate decision-making was the most common ethical issue, affecting 27 of 59 patients (45.8%), followed by overall QoL considerations (22/59; 37.3%). When analyzed separately, QoL deliberations in decision-making appeared in 12/59 patients (20.3%), and treatment-related QoL concerns in 10/59 patients (16.9%). Other frequently documented categories included informed consent (12/59; 20.3%), resuscitation or do-not-resuscitate (DNR) orders (11/59; 18.6%), forgoing life-sustaining treatments (9/59; 15.3%), professional disagreement (9/59; 15.3%), advance directives (8/59; 13.6%), and disruptive or threatening behavior (7/59; 11.9%; Table 3 and Fig. 2B).
Patient-Level Prevalence of Categories Across Ethics Consultations by Age Group (Unique Patients, N = 59)
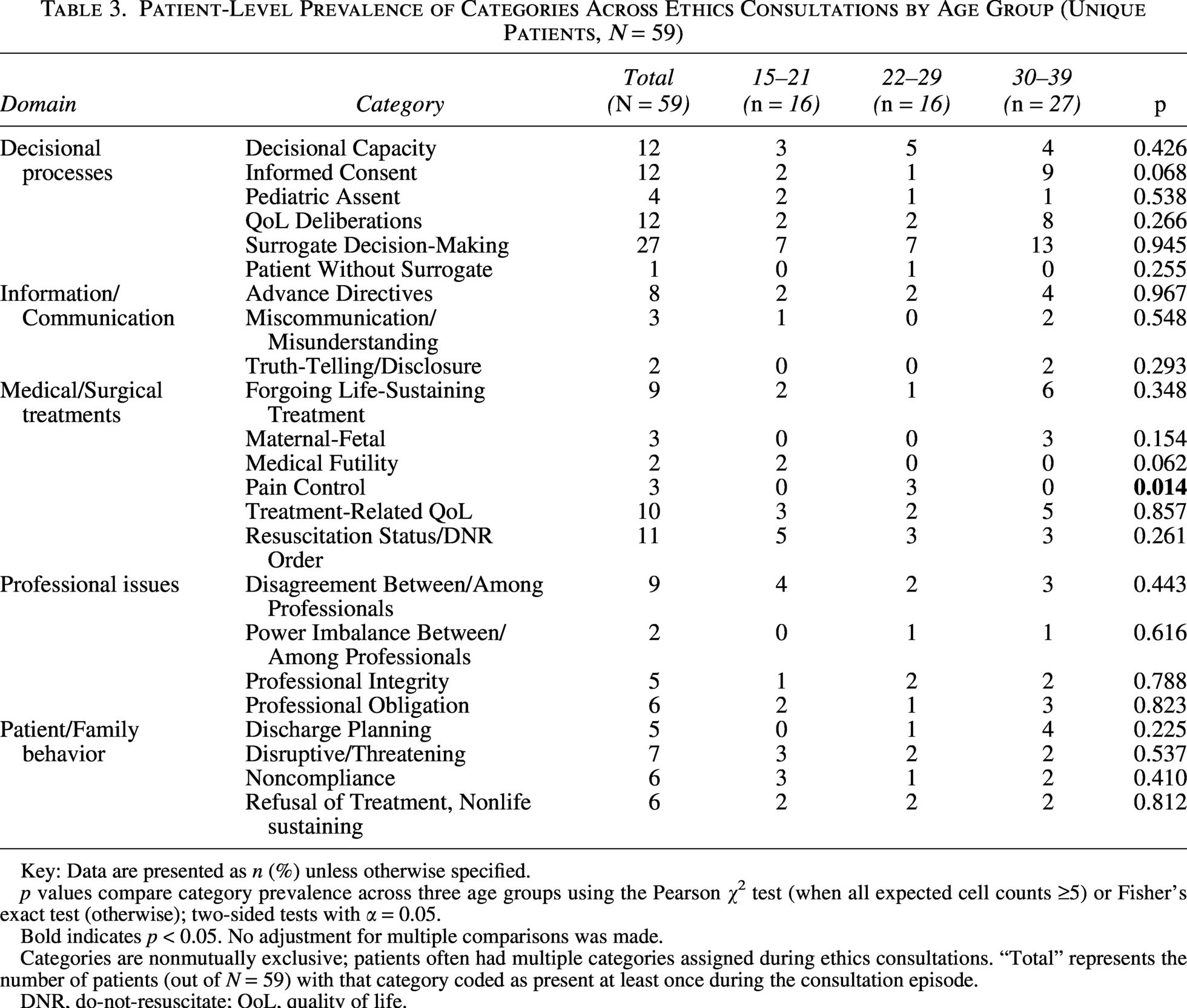
Key: Data are presented as n (%) unless otherwise specified.
p values compare category prevalence across three age groups using the Pearson χ2 test (when all expected cell counts ≥5) or Fisher’s exact test (otherwise); two-sided tests with α = 0.05.
Bold indicates p < 0.05. No adjustment for multiple comparisons was made.
Categories are nonmutually exclusive; patients often had multiple categories assigned during ethics consultations. “Total” represents the number of patients (out of N = 59) with that category coded as present at least once during the consultation episode.
DNR, do-not-resuscitate; QoL, quality of life.
Age group comparisons
When stratified by age group (15–21, 22–29, 30–39 years), the distribution of category applications across domains generally remained consistent (Fig. 2C and Table 2). At the category level, pain control was the only issue showing significant age variation, occurring exclusively in patients aged 22–29 years (3/16; p = 0.014) (Table 3). Less common categories included maternal-fetal considerations (n = 3), brain death (n = 2), and medical futility (n = 2), which typically co-occurred with decisional or communication concerns.
Discussion
Over more than 10 years, decision-making processes dominated ECs in AYA oncology, accounting for 41.8% of 153 category applications, with surrogate decision-making being the most common concern (45.8% of patients). Despite the developmental and psychosocial diversity within the AYA population, consultation patterns remained consistent across age groups, with pain control being the only age-specific concern that was statistically significant (p = 0.014).
Decisional complexity as the central challenge
The dominance of Decisional Processes and the high frequency of surrogate decision-making reflect ongoing family involvement and changing autonomy typical of AYA cancer care.14–17 This aligns with the NCCN 2024 AYA guideline, which emphasizes evaluating decisional capacity, obtaining informed consent, and designating proxies as ethical priorities, given neurocognitive effects and family dynamics. 13 The European Society for Medical Oncology/International Society of Pediatric Oncology Europe AYA position article similarly emphasizes surrogate conflicts as a major ethical challenge, especially when treatment preferences differ between patients and families. 2
The high prevalence of QoL-related ECs (37.3%)—including discussions of QoL in decision-making and treatment-related QoL concerns—along with resuscitation/DNR topics (18.6%) highlights ongoing gaps in advance care planning (ACP) and the importance of developing autonomy and identity formation at this stage of life. Structured ACP interventions and communication frameworks, such as the Serious Illness Care Program, improve clinician–patient alignment, documentation, and satisfaction with decision-making in serious illness. 18 Similarly, AYA-focused ACP tools like Voicing My Choices empower patient autonomy and encourage surrogate engagement across developmental stages. 19 The American Academy of Pediatrics now recommends starting goals-of-care conversations at diagnosis for high-risk cancers instead of waiting for disease progression.20–22
Age-related patterns: Developmental homogeneity
Although psychosocial maturity and independence vary among adolescents, emerging adults, and mature AYAs, our EC patterns remained notably consistent across these groups. This consistency across age groups supports survivorship and transition research, showing that decisional conflict and psychosocial needs are similar across the 15–39 years age range.7,9,23–25 Such evidence backs unified, AYA-focused ethics frameworks rather than strictly age-specific ones.
Pain as a transition-specific vulnerability
Pain control’s clustering among 22–29-year-olds may reflect vulnerabilities during the transition from pediatric-to-adult care, when patients take on self-management responsibilities and encounter adult providers who are less familiar with developmental nuances.26–30 Although pain control is often framed as a clinical or palliative care issue, it becomes an ethical issue when the obligation to relieve pain and alleviate pain-related suffering as expressed by the patient must be balanced against other goals and obligations, including preserving consciousness for communication, respecting AYA autonomy (including when it is emerging and evolving prior to the age of majority) and addressing patient, family, or clinician concerns that escalating analgesia may hasten death or signal abandonment. In AYAs, these tensions may be heightened during the transition to adult-oriented care and by the developmental importance of maintaining agency, relationships, and meaningful time.30,31 The World Health Organization Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents highlights that young adults face unique risks of undertreatment, requiring individualized, multimodal pain management strategies. 31 Early integration of palliative care improves symptom control and QoL, especially when standardized screening is incorporated.32,33 Validated AYA-specific tools such as the Symptom Screening in Pediatrics Tool (SSPedi) and its proxy versions reliably assess multidimensional symptom burden in cancer patients. 34
Behavioral and professional dynamics
Disruptive or threatening behavior (11.9%) and professional disagreement (15.3%) highlight the interaction of psychosocial stress, family conflict, and interdisciplinary challenges in AYA oncology. Systematic distress screening, early palliative involvement, and shared goals-of-care documentation may help prevent escalation and reduce reactive ECs.24,28,32–41 The NCCN Distress Management and AYA Oncology guidelines, together with American Society of Clinical Oncology guidance on screening, assessment, and care for anxiety and depressive symptoms in adults with cancer, recommend routine psychosocial screening at diagnosis and at key transition points, using validated tools integrated into standard workflows.42,43
Clinical implementation
Our findings support the goals of AYA stakeholders in translating:
Limitations
This single-center retrospective study limits its generalizability, especially to community settings that lack a comprehensive ethics infrastructure. The modest consultation volume (59 patients over 10 years) may reflect effective team-based problem-solving, selective use for complex cases, or access barriers, indicating the need for multicenter research. Categorization by individual ethicists without formal inter-rater reliability testing introduces potential variability in measurement. In addition, yes/no category coding may nuance representing AYA-specific concerns, such as identity formation, fertility, and future family-building, sexuality, peer relationships, educational disruption, and digital privacy than a qualitative narrative or mixed-method analysis could provide.11,12 The taxonomy’s different levels of detail—such as “QoL deliberations,” which encompass broader issues than “pain control” or “resuscitation/DNR”—make direct category comparisons more complicated. We did not evaluate consultation outcomes, stakeholder satisfaction, or impacts on long-term care quality—key areas for future research, especially to determine whether preventive interventions can reduce consultation needs while maintaining care quality.
Conclusion
ECs for AYAs with cancer, it involves complex, overlapping decision-making challenges across different developmental stages. Pain management often presents a unique vulnerability among emerging adults. The common use of surrogate decision-making, QoL considerations—including decisions and treatment concerns—and end-of-life planning, along with typical behavioral and professional conflicts, highlight areas for targeted preventive strategies. Evidence-based approaches such as structured decision documentation, systematic symptom screening with AYA-friendly tools, transition-readiness protocols, and integrated ethics support provide a framework to proactively address these issues while supporting AYAs throughout their cancer journey. Moving from reactive to preventive ECs offers a practical way to improve AYA cancer care and reduce ethical crises.
Authors’ Contributions
R.N.Z.: Writing—original draft (lead), writing—reviewing and editing (equal), investigation (lead), methodology (supporting), and data curation (equal). M.S.H.: Formal analysis (lead), writing—reviewing and editing (equal), investigation (supporting), methodology (lead), visualization (lead), and data curation (equal). K.E.: conceptualization (equal), writing—reviewing and editing (equal). A.K.: Data curation (equal) and writing—reviewing and editing (equal). K.B.: Writing—reviewing and editing (equal). J.S.C.: Conceptualization (equal), resources (lead), and writing—reviewing and editing (equal). S.M.T.: Conceptualization (lead), supervision (lead), and writing—reviewing and editing (equal).
Supplemental Material
sj-docx-1-jay-10.1177_21565333261464967 — Supplemental material for Ethical Consultation Utilization Patterns in Adolescent and Young Adult Oncology: A 10-Year Single-Center Study and Contemporary Ethics Framework
Supplemental material, sj-docx-1-jay-10.1177_21565333261464967 for Ethical Consultation Utilization Patterns in Adolescent and Young Adult Oncology: A 10-Year Single-Center Study and Contemporary Ethics Framework by Rachel N. Zeno, Miza Salim Hammoud, Kate Eshleman, Arjan Kalra, Kara Bendle, Joshua S. Crites, and Stefanie M. Thomas
Footnotes
IRB/Ethics Approval
This study involves a secondary analysis of de-identified registry data, for which no additional IRB approval is necessary.
Previous Presentation
The authors presented a poster at the 6th Global Adolescent and Young Adult Cancer Congress, December 2024. Poster at the American Society of Pediatric Hematology and Oncology 2026 Convention.
Author Disclosure Statement
The authors of this article have nothing to disclose.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.