
Abstract
In this study, we examine the relationships among reflected appraisals, self-views, and well-being for individuals diagnosed with severe and persistent mental illness. We also test a perceptual control model of identity to determine whether discrepancies between stigmatized reflected appraisals and stigmatized self-views are associated with self-evaluation (self-esteem and self-efficacy) and psychological distress (depressive symptoms). We find that stigmatized self-views are significantly associated with lower self-esteem and self-efficacy and higher levels of depressive symptoms. Stigmatized reflected appraisals are also associated with lower self-efficacy and higher depressive symptoms but are not associated with self-esteem. As predicted, discrepancies between reflected appraisals and self-views are associated with lower levels of self-efficacy and higher levels of depressive symptoms; however, we do not find a relationship between identity discrepancy and self-esteem. We discuss the implications of our findings for identity and stigma research.
Keywords
Introduction
Stigma is negatively associated with well-being among individuals with severe and persistent mental illness (SPMI). According to Goffman (1963:3), stigma refers to an “attribute that is deeply discrediting” by society. As it relates to mental illness, stigma is conceptualized as a weakness of character, one that is based on societal reaction and results in a “spoiled identity.” For those with SPMI, stigma compounds the stress of mental illness and can further compromise well-being (e.g., Link et al. 1989; Marcussen and Ritter 2016; Rosenfield 1997). Drawing on symbolic interactionist assumptions regarding the relationship between self and society (Cooley 1902; Mead 1934), labeling and identity theories have identified mechanisms that explain the development and maintenance of stigmatized identities. In particular, these theories have emphasized the relationship between societal and self-views, and between public and self-stigma (Corrigan and Watson 2002).
Labeling scholars have long argued that the impact of deviant labels on well-being is conditional on the recognition and acceptance of societal views (Becker 1963; Lemert 1951; Scheff 1966; Tannenbaum 1938). When individuals perceive that they are devalued or likely to be discriminated against, these perceptions have negative consequences for how they view themselves, resulting in lower self-esteem (e.g., Link 1987; Link et al. 1989), mastery (e.g., Rosenfield 1997), and quality of life (Marcussen and Ritter 2016; Rosenfield 1997). Identity theorists similarly emphasize the importance of social interaction and perceptions of others in the development of self-views (e.g., Burke 1991, 1996; Stryker [1980] 2002; Stryker and Statham 1985). Burke’s perceptual control model in particular views identities as a process whereby individuals continuously compare self-meanings associated with an identity (self-views) to perceptions of how others see them in the context of that identity (reflected appraisals; Burke 1991, 1996). Burke’s theory assumes that individuals are motivated to confirm self-views. Failure to verify an identity, or identity discrepancy, is negatively associated with self-esteem and self-efficacy (Burke and Harrod 2005; Cast and Burke 2002; Marcussen 2006) and positively associated with psychological distress (Burke 1991; Burke and Harrod 2005; Burke and Stets 2009; Marcussen and Gallagher 2017; Marcussen and Large 2003).
The relationship between reflected appraisals and self-views has been examined in numerous studies of deviant identities (e.g., Asencio and Burke 2011; Granberg 2011; Kaufman and Johnson 2004; Kroska and Harkness 2006; Lee and Craft 2002; Marcussen and Asencio 2016; Markowitz, Angell, and Greenberg 2011). These studies show a relationship between reflected appraisals and self-views that is consistent with the basic tenants of labeling and identity theories, providing some insight into the development and maintenance of stigmatized identities. They also illustrate a negative effect of stigmatized reflected and self-appraisals on self-evaluation and distress. Many of these studies draw on identity theories, such as the perceptual control model; however, they do not directly test identity theory in the context of a stigmatized identity. Thus, while the perceptual control model has been successful in explaining the relationship between identity and well-being for normative identities, less is known about whether individuals benefit from verifying stigmatized self-views (Stets and Serpe 2013).
In this paper, we examine the relationship between stigmatized appraisals and well-being among individuals with SPMI. Drawing on Burke’s theory and building on research linking identity and stigma (Markowitz et al. 2011), we use meaning-based measures of reflected appraisals and self-views to examine the independent relationships among appraisals (from self and other), self-evaluation (self-esteem and self-efficacy), 1 and psychological distress (depressive symptoms). We also test a perceptual control model to examine whether discrepancies in identity meanings are associated with these outcomes. Previous research has demonstrated that the inability to verify self-views related to normative identities is detrimental to self-evaluation and well-being (Burke 1991, 1996). We examine whether these relationships hold for a stigmatized identity. Understanding identity verification within the context of mental illness may provide insight into the maintenance of stigmatized identities and consequently, advance our understanding of how identity and stigma processes shape well-being.
Background
An assumption of symbolic interactionism is that the self is reflexive (Cooley 1902; Mead 1934). We imagine how others view us in the context of social interactions or situations, imagine judgments associated with that appearance, and adjust our behavior accordingly (Cooley 1902). Importantly, it is our perceptions of how others see us that help to shape our self-views. According to Mead (1934), socialization processes further require that individuals learn to see themselves from the perspective of others, often starting with personal relationships such as family and friends (significant others) and extending to societal views more broadly (the generalized other). Understanding societal expectations associated with the roles we hold or the groups to which we belong is critical to the development and maintenance of identities (Mead 1934).
Developing a Stigmatized Identity
Stigma and labeling theories incorporate symbolic interactionist assumptions in their emphasis on social interaction in the development of a deviant self-concept (e.g., Goffman 1963; Lemert 1951; Tannenbaum 1938). According to Scheff (1966), individuals who are labeled mentally ill may engage in a self-fulfilling prophecy whereby stereotypes associated with the label become part of their self-definition. Acceptance of this new self-definition results in the formation of a mental illness identity. Therefore, social stigma becomes self-stigma through societal reaction and social interaction (Goffman 1963). Despite its contributions, Scheff’s labeling theory has had its share of critiques, including the emphasis placed on formal labeling processes and the suggestion that labels are the primary cause of mental illness. Extensions of labeling theory such as Thoits’s (1985) self-labeling theory and Link’s (1987; Link et al. 1989) modified labeling theory address these limitations.
Thoits (1985) argued that individuals are capable of self-labeling, omitting the necessity for overt or public labeling as suggested in earlier approaches (Scheff 1966). Self-labeling implies that individuals need not have direct interaction (or reaction) to form identities. Instead, Thoits (1985:222) emphasized the role of the “imagined perspective” in the self-labeling process. Link’s (1987; Link et al. 1989) modified labeling theory shifted the focus of labeling research from identifying labels as a causal element in the development of mental illness to the consequences of negative stereotypes perpetuated through labeling. These consequences, which result from the anticipation of negative social reactions surrounding the mental illness label, erode self-esteem and mastery (e.g., Link 1987; Link et al. 1989; Rosenfield 1997) as well as psychological well-being (Marcussen and Ritter 2016; Rosenfield 1997).
The arguments advanced by these theories have broadened our understanding of the causes and consequences of mental illness labels. In particular, modified labeling theory provides a model for examining how perceptions of public attitudes about mental illness impact self-evaluation and psychological well-being among individuals with mental illness (Link 1987; Link et al. 1989). Nonetheless, empirical work using this approach has produced modest results when linking perceived (or public) stigma to well-being (Thoits 2011; Thoits and Link 2016), particularly in light of psychological research that has consistently demonstrated relationships between internalized (or self) stigma and self-esteem, self-efficacy, and psychiatric symptoms (e.g., Corrigan, Watson, and Barr 2006; Drapalski et al. 2013; Ritsher and Phelan 2004; Watson et al. 2007). The perceptual control model of identity incorporates the perspective of the imagined other and self-views, providing a theoretical framework that bridges stigma and identity research.
Maintaining a Stigmatized Identity
Like labeling theories, identity theory builds on the assumption that self-views are developed and maintained through social interaction (Mead 1934; Stryker [1980] 2002). This assumption is articulated in identity theories that have emerged from structural symbolic interactionism (e.g., Burke 1980; Stryker [1980] 2002), and define identity in terms of the meanings that individuals attach to roles that they hold (e.g., a responsible student), groups to which they belong (e.g., compassionate women), and who they are as a person (e.g., an honest person; Stets and Serpe 2013). These meanings emerge through social interaction and role-taking.
Burke’s (1991, 1996) identity theory views identities as a perceptual control system, where social behavior is a consequence of comparisons made between how individuals view themselves in a given identity (self-view) and how they perceive others view them in that identity (reflected appraisals). In this model (Burke 1991, 1996), the self-view is conceptualized as an identity standard, or a set of personal meanings and expectations associated with each identity. Both self-views and reflected appraisals are measured along specific dimensions of meaning, typically captured with a series of semantic differential scales (e.g., responsible to irresponsible, compassionate to uncompassionate, honest to dishonest). While identity theory has largely been used to predict behavioral outcomes in the context of role-identities, the perceptual control model has been applied to other bases of identity, including group and person identities, as described above (Stets and Burke 2014b; Stets and Serpe 2013).
When individuals experience a discrepancy between reflected appraisals and self-views, they will typically engage in behavior meant to bring the two views back in line with one another. When discrepancies are persistent or when these behaviors are not effective in achieving consistency, they can have negative consequences for self-esteem (e.g., Asencio 2013; Cast and Burke 2002; Marcussen 2006), self-efficacy (Burke and Harrod 2005; Cast and Burke 2002), and psychological well-being (e.g., Burke 1991, 1996; Burke and Harrod 2005; Marcussen and Gallagher 2017; Marcussen and Large 2003). Consistent with self-verification theories (e.g., Higgins 1987; Swann 1983), identity theory suggests that individuals seek to confirm characteristics associated with identities regardless of whether they are positive or negative. In other words, the primary motivation for behavior is to verify, not enhance, one’s self-view (Burke 1991, 1996; Burke and Stets 2009). The question remains whether that pattern holds for stigmatized identities.
There is reason to believe that individuals may be motivated to verify stigmatized self-views. Stable self-views provide coherence and predictability in social interactions (Lecky 1945; Swann 1983). According to Swann (2012), individuals generally prefer being true to who they think they are. A better understanding of oneself along with the ability to predict reactions of others may result in smoother interactions and greater well-being (Goffman 1959). Swann (2012) further argues that the desire to seek stability in self-views is intimately connected to the initial source of these views, namely, feedback from others (Cooley 1902; Mead 1934). The same feedback that helps shape self-views eventually provides confirming evidence of those views. The confidence that comes from continuous feedback that matches self-views can supersede the motivation to seek feedback that exceeds them. Indeed, verification of self-views has been positively associated with both self-worth and self-efficacy (Swann, Chang-Schneider, and Larsen McClarty 2007).
Stigma and identity theories have laid the groundwork for conceptualizing stigmatized reflected appraisals and self-views (Goffman 1963; Markowitz et al. 2011; Martin, Pescosolido, and Tuch 2000; Phelan et al. 2000; Wahl 1995). Goffman (1963:4) described social identities as comprised of personal attributes (e.g., honesty) that are associated with a social category and stigma as “a special kind of relationship between attribute and stereotype.” Numerous researchers have shown that stereotypes depicting individuals with mental illness as dangerous, unpredictable, and unstable persist in the public eye despite changes in attributions of the perceived causes of mental illness (Corrigan and Watson 2002; Martin et al., 2000; Phelan et al. 2000; Wahl 1995). Stigmatized reflected appraisals, unlike general perceptions of public attitudes, assess the extent to which individuals perceive that others apply stereotypes to them personally. In other words, stigmatized reflected appraisals suggest a perception that is both imagined and self-relevant. When stigmatized attributes are internalized, they become normative expectations for individuals who occupy the identity (Goffman 1963; Scheff 1966) and subsequently part of the identity standard or self-view (Burke 1991, 1996).
Stigmatized Identities and Well-being
The relationship between reflected appraisals and self-views has been the focus of numerous studies across a range of deviant identities (e.g., Ascenio and Burke 2011; Carter and Mireles 2016; Granberg 2011; Kaufman and Johnson 2004; Kroska and Harkness 2006; Lee and Craft 2002; Marcussen and Asencio 2016; Markowitz et al. 2011). For some of these studies, reflected appraisals and self-views simply confirm that the individual is characterized or defined by a certain identity, such as a deaf person (Carter and Mireles 2016), a criminal/drug user (Asencio and Burke 2011), or a person with mental illness (Marcussen and Asencio 2016). Other studies have used qualitative data to explore the role of appraisals in the development and maintenance of deviant identities, such as gay and lesbian identities (Kaufman and Johnson 2004) and stigmatized health identities (Granberg 2011; Lee and Craft 2002). These studies suggest that identity processes operate similarly for deviant identities relative to normative identities. They also show that reflected appraisals and self-views may operate independently and/or differently across different identities (e.g., Asencio and Burke 2011).
A few studies have explicitly linked reflected appraisals and self-views to self-evaluation and psychological well-being for individuals with mental illness. For example, Marcussen and Asencio (2016) found that self-views (I see myself in terms of my mental illness) and reflected appraisals (others see me in terms of my mental illness) were independently associated with lower self-esteem among individuals who reported mental health problems. Kroska and Harkness (2006) showed that self-identity (myself as I really am) was negatively related to potency (or self-efficacy), whereas reflected appraisals (myself as others see me) were negatively associated with evaluation (or self-esteem) in a sample of psychiatric patients.
Markowitz et al. (2011) linked the reflected appraisal process to self-evaluation and recovery in a study of mothers and their adult children with schizophrenia. The authors assessed a series of attributes/stereotypes associated with the mental illness identity from the perspective of self (I am) and other (my mother thinks I am). In this study, the authors measure identity in line with Burke’s identity standard: as a set of semantic differential scales that capture attributes commonly associated with mental illness (e.g., competent to incompetent, friendly to unfriendly, safe to dangerous). The results of this study showed that reflected appraisals and self-appraisals were differentially associated with well-being. Reflected appraisals, while positively associated with self-views, were not directly associated with symptoms, self-efficacy, or life satisfaction. The mental illness self-view, however, was associated with decreases in self-efficacy and life satisfaction and increases in symptoms. The authors also found that the effects of self-view on well-being were not mediated by reflected appraisals. This study is notable for a couple of reasons. First, the authors used a multidimensional measure of the mental illness identity that included a set of meanings from the perspective of self and significant other. The adjectives used to reflect identity meaning and the semantic differential scales used to measure identity draw from stigma and identity literatures. Second, this study shows that reflected appraisals and self-views are not necessarily measuring the same thing or associated with the same outcomes.
The studies discussed above have used identity theories or concepts in an attempt to better understand stigmatized identities. In some cases, researchers have drawn explicitly from the perceptual control model to provide insight into the ways in which individuals perceive feedback from others to develop (and confirm) meanings associated with stigmatized identities (e.g., Granberg 2011; Kaufman and Johnson 2004; Lee and Craft 2002). While these studies have certainly contributed to research linking stigma and identity, they stop short of testing an identity model of mental illness. Given its success in predicting mental health and behavioral outcomes in the context of normative identities, an examination of mental illness using the perceptual control model has the potential to advance stigma and identity literatures.
Hypotheses
Identity theory and research has played an important role in understanding processes associated with the development and maintenance of stigmatized identities. We see a few directions identity theorists can take to move this research forward. First, we suggest there is value in measuring the independent effects of reflected appraisals and self-views on self and mental health outcomes. While theoretical models of deviant identities have focused on the relationship between reflected appraisals and self-views, recent studies have suggested they may be independently related to well-being. Establishing the relationship between identity meaning and well-being is an important first step in understanding these key components of a stigmatized identity. Drawing on the stigma and identity literatures (Burke 1991, 1996; Markowitz et al. 2011), we use measures of self-views and reflected appraisals that incorporate stigmatized attributes (or meanings) commonly associated with mental illness. We expect that stigmatized appraisals (from self and other) will be negatively related to self-evaluation and psychological distress. Specifically, we propose the following hypotheses:
Hypothesis 1: (a) Stigmatized reflected appraisals and (b) self-views will be negatively associated with self-esteem.
Hypothesis 2: (a) Stigmatized reflected appraisals and (b) self-views will be negatively associated with self-efficacy.
Hypothesis 3: (a) Stigmatized reflected appraisals and (b) self-views will be positively associated with depressive symptoms.
Second, our study extends identity theory by testing the perceptual control model in the context of a stigmatized identity. Specifically, we examine the extent to which a discrepancy between reflected appraisals and self-views related to the mental illness identity is associated with self-evaluation and depressive symptoms. Consistent with theory and research on verification processes in normative identities, we expect that a discrepancy in a stigmatized identity will be negatively associated with well-being.
Hypothesis 4: A discrepancy between stigmatized reflected appraisals and self-views will be negatively associated with self-esteem.
Hypothesis 5: A discrepancy between stigmatized reflected appraisals and self-views will be negatively associated with self-efficacy.
Hypothesis 6: A discrepancy between stigmatized reflected appraisals and self-views will be positively associated with depressive symptoms.
Data And Methods
Sample
The study sample is comprised of active adult clients of a community mental health center located in a Midwestern city. Active clients are those who received at least one unit of service within the previous 120 days. Research partners at the county mental health services board randomly selected 1,500 of the approximately 2,500 active clients to be contacted about the study between November 2011 and April 2012. Administrative support staff at the community mental health center addressed and mailed letters to each randomly selected client, which included information about the study and a form that they were asked to return to the research team if they were interested in being contacted by phone about potentially participating in the study.
Data were collected during face-to-face interviews that lasted approximately 90 minutes. Of the clients who were mailed letters about the study, 262 returned the form indicating that they were interested in being contacted by the research team, for a response rate of 17 percent. 2 Though the response rate was lower than expected, when sample characteristics (e.g., gender, Medicaid eligibility, age, ethnicity, units of mental health services) were compared to the full population of active clients, we found only two significant differences: gender and Medicaid eligibility. Our sample was 60 percent female (vs. 44 percent in the remaining population) and 88 percent Medicaid eligible (vs. 80 percent in the remaining population). Interviews were scheduled with 223 clients (85 percent of those who expressed interest in the study; 15 percent of those who were originally contacted). The study received approval from the Northeast Ohio Medical University institutional review board.
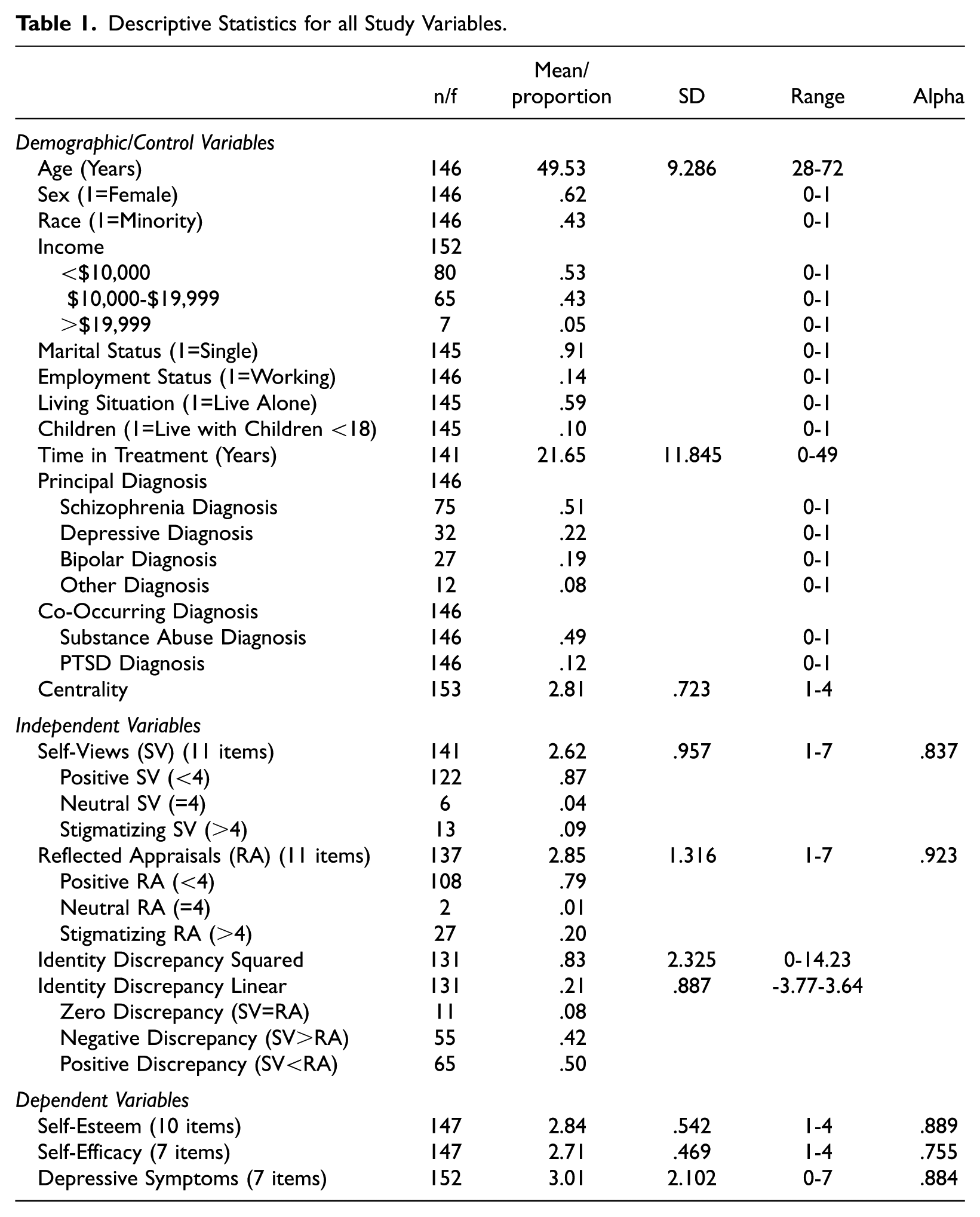
The analytic sample for the present study is comprised of 156 individuals who were re-interviewed during Wave 2 of the original study, approximately 18 months after Wave 1. Stigmatizing self-views and reflected appraisals were only included in the Wave 2 interview. 3 Demographic characteristics of the analytic sample are displayed in Table 1. On average, the sample is approximately 50 years old, 62 percent female, and 57 percent white. In terms of income, 53 percent of respondents receive less than $10,000, 43 percent receive between $10,000 and $19,999, and 5 percent receive more than $19,999 per year from all sources. Ninety-one percent of respondents are single, 14 percent are employed, 59 percent live alone, and 10 percent live with children under the age of 18. Respondents have been in mental health treatment for an average of about 22 years. Forty-nine percent of respondents have been diagnosed with a co-occuring substance abuse disorder, and 12 percent have been diagnosed with PTSD. In terms of principal diagnosis, schizophrenia (51 percent) is the most common, followed by depressive (22 percent), bipolar (19 percent), and other (8 percent) diagnoses.
Descriptive Statistics for all Study Variables.
Measures
Dependent Measures
Depressive symptoms are measured using an abbreviated seven-item version (Mirowsky and Ross 1992) of the Center for Epidemiological Studies-Depression (CES-D-19) scale (Radloff 1977). Respondents are asked, “On how many days in the past seven days have you . . . ?” Items include, “felt you could not get going,” “felt that you couldn’t shake the blues,” and “felt sad.” All items are summed and divided by the number of items in the scale, with higher scores indicating more depressive symptoms (Cronbach’s alpha = .884).
Self-esteem is measured using the 10-item Rosenberg Self-Esteem scale (Rosenberg 1965). Items include, “I feel that I am a person of worth, at least on an equal basis with others” and “I feel that I have a number of good qualities.” Self-efficacy is measured using the seven-item Pearlin Mastery scale (Pearlin and Schooler 1978). Items include, “I have little control over things that happen to me” and “Sometimes I feel like I am being pushed around in life.” Responses for self-esteem and self-efficacy items range from 1 (strongly agree) to 4 (strongly disagree). Higher scores indicate more self-esteem or self-efficacy, respectively. Cronbach’s alpha reliability is .889 for self-esteem and .755 for self-efficacy.
Independent Measures
The independent variables in the first set of analyses are self-views and reflected appraisals. Self-views and reflected appraisals are measured by asking respondents to fill out a handout containing 11 pairs of semantic differentials (adapted from Markowitz et al. 2011) that represent the positive and negative poles of stigmatizing characteristics associated with the mental illness identity. Respondents are given a handout showing a scale that ranges from 1 to 7, with negative characteristics on one pole and their positive equivalents on the other pole and instructed, “Mark on the scale where you think you best fit in your mind, saying before each item, ‘I am . . . ’” for self-views and “ . . . others think I am . . . ” for reflected appraisals. The semantic differentials include unfriendly-friendly, dangerous-safe, unintelligent-intelligent, incompetent-competent, disorganized-organized, unstable-stable, unpredictable-predictable, unreliable-reliable, irrational-rational, childlike-adult, and irresponsible-responsible. All items are summed and divided by the number of items in the scale, with higher scores representing more stigmatizing self-views or reflected appraisals, respectively. Cronbach’s alpha reliability is .837 for self-views and .932 for reflected appraisals.
In the second set of analyses, the independent variables are identity discrepancies. Identity discrepancies are calculated using the self-view and reflected appraisal measures described previously. Linear discrepancies are calculated by subtracting the self-view scale from the reflected appraisal scale; squared discrepancies are calculated by squaring the linear discrepancy value. As shown in Table 1, the average linear identity discrepancy is .21, and the average squared discrepancy is .83. Only 8 percent of respondents have no discrepancy. Among those respondents with a discrepancy, 42 percent have a negative discrepancy (i.e., self-views are more stigmatizing than reflected appraisals), and 50 percent have a positive discrepancy (i.e., self-views are less stigmatizing than reflected appraisals).
Both the squared and linear discrepancy terms are included in the analyses because the relationship between identity discrepancy and psychological distress is theoretically curvilinear, where zero discrepancy is expected to produce zero distress and increasing discrepancy in either a positive (i.e., the reflected appraisal is higher than the self-view) or negative (i.e., the reflected appraisal is lower than the self-view) direction should increase distress (Burke and Harrod 2005; Stets and Burke 2014a). Given that, most contemporary identity research examines the impact of squared discrepancies in models that control for linear discrepancies. If squared discrepancies significantly predict distress in models in which linear discrepancies are not statistically significant, identity theory is supported.
Control Variables
The analyses presented here include controls for principal diagnosis and mental illness identity centrality, or the extent to which respondents think that mental illness is a major part of who they are. Principal diagnoses are coded so that 1 = the presence of that respective disorder. Mental illness identity centrality is measured using an item that asks respondents to rate their level of agreement with the statement “My mental illness is a major part of who I am” on a scale ranging from 1 (strongly disagree) to 4 (strongly agree).
Analytic Strategy
We estimate two structural equation models (SEMs) to investigate (1) the relationships between stigmatizing self-views and reflected appraisals and outcomes related to self-evaluation and psychological distress and (2) the relationships between identity discrepancies and those same outcomes. SEM is ideal for concurrently estimating relationships among multiple correlated independent and outcome variables. The SEMs employ full information maximum likelihood estimation to retain as many cases as possible in the analyses. Robust standard errors are used to correct for the autocorrelation of errors.
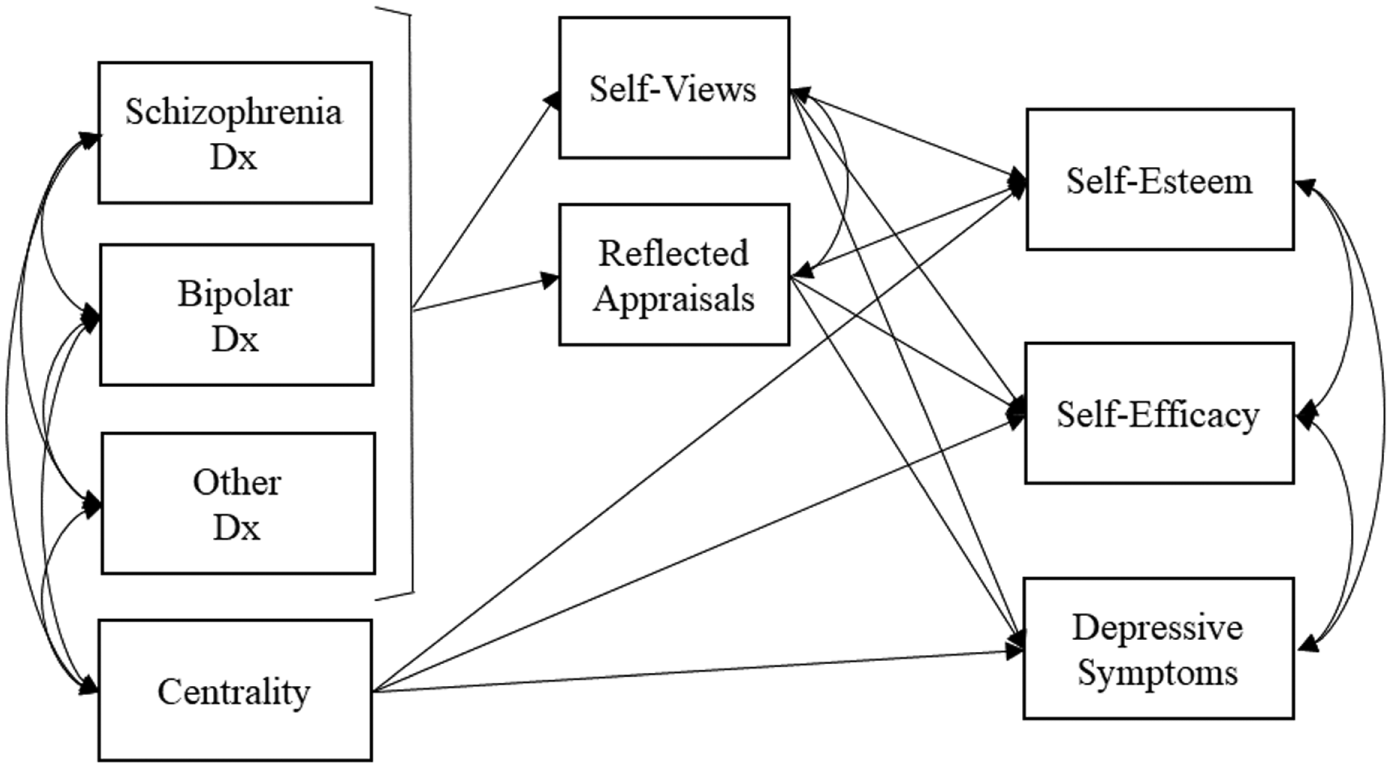
For both analyses, we estimated preliminary models in which we included controls for variables that are theoretically and empirically relevant to identity, mental illness, and recovery, including demographic characteristics, time in treatment, substance abuse diagnosis, PTSD diagnosis, principal diagnosis, and mental illness identity centrality. In the final models presented here, we omitted all control variables that were not significantly associated with any of the focal independent or dependent variables, leaving only mental illness identity centrality and principal diagnoses and their significant associations (structural pathways) with the focal independent and dependent variables. Figure 1 depicts the final structural equation model for self-views and reflected appraisals. Figure 2 depicts the final structural equation model for identity discrepancy.
Final structural equation model for reflected appraisals and self-views, self-evaluation, and depressive symptoms.

Final structural equation model for identity discrepancy, self-evaluation, and depressive symptoms.
Results
Bivariate correlations between all independent and dependent variables are displayed in in Table 2. Stigmatizing self-views are negatively associated with both self-esteem (r = −.508) and self-efficacy (r = −.406) and positively associated with depressive symptoms (r = .442). Stigmatizing reflected appraisals are also negatively associated with self-esteem (r = −.504) and self-efficacy (r = −.399) and positively associated with depressive symptoms (r = .399). The linear discrepancy terms are not significantly associated with self-evaluation or depressive symptoms, but the squared discrepancy term is significantly associated with both self-efficacy (r = −.221) and depressive symptoms (r = .191). Finally, self-esteem and self-efficacy are positively and significantly associated with one another (r = .676) and negatively associated with depressive symptoms (self-esteem r = −.546 and self-efficacy r = −.467).
Correlations between Study Variables.
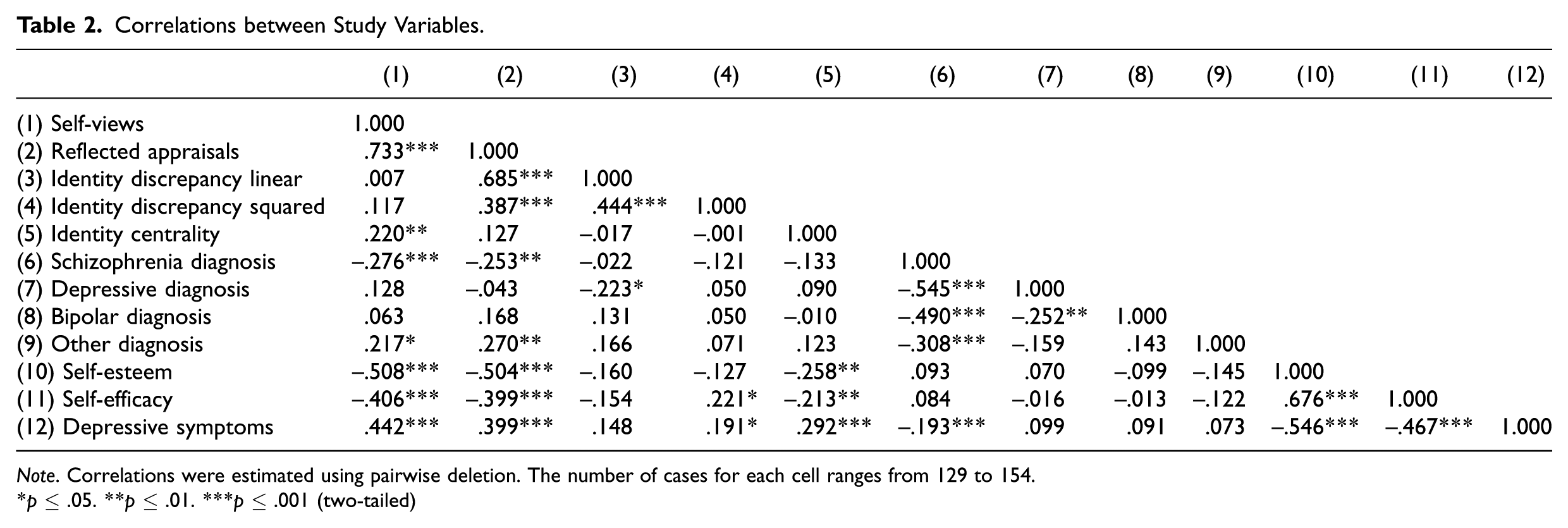
Note. Correlations were estimated using pairwise deletion. The number of cases for each cell ranges from 129 to 154.
p ≤ .05. **p ≤ .01. ***p ≤ .001 (two-tailed)
Stigmatizing Self-views and Reflected Appraisals
In the first structural equation model, we estimated associations between stigmatizing appraisals (self and other) and well-being (self-evaluation and depressive symptoms). The model fits the data well, χ2 = 10.620, 11 df, p = .475, Comparative Fit Index (CFI) = 1.000, root mean square error of approximation (RMSEA) = .000; and R2 values indicate that it explains approximately 13, 11, and 11 percent of the variance in depressive symptoms, self-esteem, and self-efficacy, respectively. Variance inflation factors (VIFs) indicate that multicollinearity is not an issue because all are at or below 2.16. Conventionally, VIFs at or above 10 are considered to indicate possible problems with multicollinearity, although some use a more conservative cutoff of 4 (O’Brien 2007).
As shown in Table 3, we find that stigmatizing reflected appraisals are not significantly associated with self-esteem, failing to support Hypothesis 1a, which predicted a negative association. Hypothesis 1b is supported in that stigmatizing self-views are significantly and negatively associated with self-esteem (b = −.163, p < .05). With respect to self-efficacy, we find support for Hypotheses 2a and 2b; stigmatizing reflected appraisals (b = −.084, p < .05) and stigmatizing self-views (b = −.107, p < .05) are significantly and negatively associated with self-efficacy. Finally, considering depressive symptoms, Hypotheses 3a and 3b are supported; stigmatizing reflected appraisals (b = .333, p < .05) and self-views (b = .555, p < .001) are significantly and positively associated with depressive symptoms. Wald tests comparing the associations between stigmatizing reflected appraisals and self-views and the outcomes with which they were both significantly associated were all nonsignificant, meaning that the null hypothesis that they are equal cannot be rejected. In other words, stigmatizing reflected appraisals and self-views have equal but independent associations with self-efficacy and depressive symptoms.
Standardized (Beta) and Unstandardized (b) Coefficients and Robust Standard Errors (SE) for Self-views and Reflected Appraisals Structural Equation Model (N = 155).

Note. The analytic sample is larger than the number of cases reported in Tables 1 and 2 because the structural equation model was estimated using full information maximum likelihood estimation. Empty cells represent structural paths that were not estimated. Correlations not shown: self-views and reflected appraisals r = .730; self-esteem and self-efficacy r = .576; diagnostic control variable correlations with each other and centrality. χ2 = 10.620, 11 df, p = .475, Comparative Fit Index = 1.000, root mean square error of approximation = .000.
p ≤ .05. **p ≤ .01. ***p ≤ .001 (two-tailed)
In sum, we find that respondents who report more stigmatizing self-views also report less self-esteem and self-efficacy and more depressive symptoms and that respondents who report more stigmatizing reflected appraisals also report less self-efficacy and more depressive symptoms. The fact that stigmatizing self-views but not stigmatizing reflected appraisals are associated with self-esteem suggests that one’s sense of worth is only affected by stigma that is internalized.
We also find that mental illness identity centrality is independently associated with two of the three outcomes. Specifically, mental illness identity centrality is negatively associated with self-esteem (b = −.129, p < .05) and positively associated with depressive symptoms (b = .615, p < .001). In other words, the more respondents view their mental illness as an important part of who they are, the less self-esteem and more depressive symptoms they report.
Mental Illness Identity Discrepancies
In the second structural equation model, we estimated associations between mental illness identity discrepancy and self-evaluation and depressive symptoms. The model fits the data well (χ2 = 7.850, 11 df, p = .726, CFI = 1.000, RMSEA = .000), and R2 values indicate that it explains approximately 25, 31, and 21 percent of the variance in depressive symptoms, self-esteem, and self-efficacy, respectively. Like the previous model, VIFs indicate that multicollinearity is not an issue as all are at or below 2.16.
Table 4 shows the results of our second structural equation model. We find support for identity theory’s verification assumption in that only the squared discrepancy term (hereafter referred to as mental illness identity discrepancy) but not the linear discrepancy term is significantly associated with outcomes. Concerning self-evaluation, mental illness identity discrepancy is not significantly associated with self-esteem, failing to support Hypothesis 4, which predicted a negative association. Hypothesis 5 is supported as mental illness identity discrepancy is significantly and negatively associated with self-efficacy (b = −.036, p < .05). Mental illness identity discrepancy is also significantly and positively associated with depressive symptoms (b = .141, p < .05), supporting Hypothesis 6. Similar to the analysis involving stigmatizing self-views and reflected appraisals, we find that mental illness identity discrepancy is most consistently associated with self-efficacy and depressive symptoms.
Standardized (Beta) and Unstandardized (b) Coefficients and Robust Standard Errors (SE) for Identity Discrepancy Structural Equation Model (N = 155).
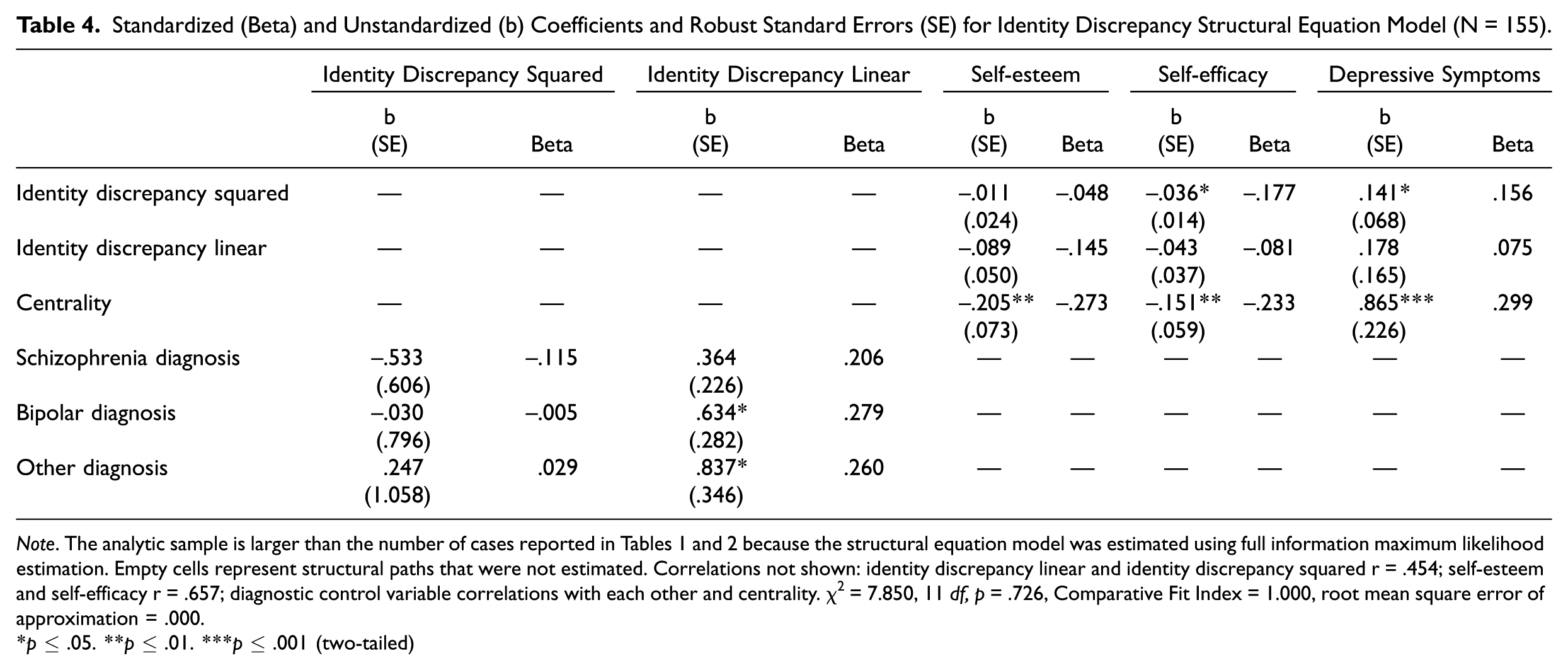
Note. The analytic sample is larger than the number of cases reported in Tables 1 and 2 because the structural equation model was estimated using full information maximum likelihood estimation. Empty cells represent structural paths that were not estimated. Correlations not shown: identity discrepancy linear and identity discrepancy squared r = .454; self-esteem and self-efficacy r = .657; diagnostic control variable correlations with each other and centrality. χ2 = 7.850, 11 df, p = .726, Comparative Fit Index = 1.000, root mean square error of approximation = .000.
p ≤ .05. **p ≤ .01. ***p ≤ .001 (two-tailed)
We find that mental illness identity centrality is associated with all three outcomes. Specifically, mental illness identity centrality is negatively associated with self-esteem (b = −.205, p < .01) and self-efficacy (b = −.151, p < .01) and positively associated with depressive symptoms (b = .865, p < .001). In other words, the more respondents view their mental illness as an important part of who they are, the lower their self-evaluation and greater their depressive symptoms.
Discussion
Identity theory has been successful in explaining the relationships among self-views, reflected appraisals, and well-being for normative identities (Stets and Serpe 2013). In this study, we examined whether identity processes are similar in reference to the mental illness identity among individuals with SPMI. Drawing on identity theory (Burke 1991, 1996) and stigma research (Markowitz et al. 2011), we measured identity meanings as a series of attributes that represent common negative stereotypes of individuals with mental illness. We focused on the perspective of the generalized other in this study because it is closely connected to public views about mental illness (what most people believe) but at the same time connects those views directly to the individual (what most people believe about me).
We found that while stigmatized reflected appraisals and self-views are strongly associated with one another, they are independently related to depressive symptoms as predicted. Individuals who believe others think of them in terms of these stigmatized attributes and individuals who apply these stereotypes to themselves report a greater amount of depressive symptoms. The pattern for self-evaluation is mixed. Stigmatized self-views are associated with both lower self-esteem and self-efficacy, whereas stigmatized reflected appraisals are associated with lower self-efficacy only. This finding is contrary to our predictions; however, it is supported by research that suggests the relationship between perceived stigma and self-esteem is generally modest (e.g., Crocker and Major 1989; Thoits 2011), whereas the relationship between internalized (or self) stigma and self-esteem is stronger (e.g., Livingston and Boyd 2010). It is worth noting that while individuals in our study did not report substantially high levels of either stigmatized self-views or reflected appraisals, individuals were more likely to report stigmatized reflected appraisals than self-views. Consistent with labeling and identity theories, endorsement of these negative attributes was generally associated with poor well-being.
We also found that a discrepancy between stigmatized reflected appraisals and self-views was associated with lower self-efficacy and higher levels of depressive symptoms. Our findings support our hypotheses (with the exception of self-esteem) and are theoretically consistent with identity theory (Burke 1991, 1996). Although our findings did not show that identity discrepancy was significantly associated with self-esteem, it is important to note that there was no model in which the linear discrepancy term was significant, indicating that self-enhancement was not supported in our data. In general, our findings support the notion that individuals benefit from consistency between reflected appraisals and self-views even when those appraisals and views are stigmatizing.
Taken together, our findings have implications for identity and stigma literatures. First, this study contributes to identity theory and research by extending the perceptual control model to examine mental illness as a stigmatized identity. Previous research has studied stigmatized identities drawing on identity theory and principles of identity verification (Asencio and Burke 2011; Granberg 2011; Kaufman and Johnson 2004; Lee and Craft 2002; Marcussen and Asencio 2016; Markowitz et al. 2011). This research tests these theoretical claims and finds that the associations between discrepancy and well-being that have been well documented for normative identities hold for the stigmatized identity of mental illness. Second, our findings add to stigma research by examining the ways in which identity processes may contribute to the maintenance of a stigmatized identity. We find that while societal views (or reflected appraisals) regarding mental illness are important, self-views are associated with well-being above and beyond the effects of reflected appraisals. This finding is also supported by previous research (Markowitz et al. 2011). Our results further suggest that stigmatized self-views represent stable meanings that individuals may be motivated to verify. According to Burke (1991, 1996), self-views are not merely a reflection of societal views but also serve as a motive for future action. Through meaningful behavior, individuals have the capacity to change or shape subsequent reflected appraisals. Thus, while perceptions of what others think are important for recovery (Markowitz et al. 2011), self-views also play an integral role in both identity and recovery processes.
Limitations and Future Directions
While this research makes contributions to stigma and identity research, it also has limitations that should be considered. First, our study uses cross-sectional data, which limits our ability to make causal assertions. With respect to the relationship between stigmatized reflected appraisals and self-views, this excludes us from determining whether one influences the other or more likely, whether the relationship between the two is reciprocal. Similarly, in our test of the perceptual control model, we are unable to determine whether discrepancies have a causal impact on self-evaluation and well-being or if individuals with low self-efficacy and high depressive symptoms are more likely to seek verification of their stigmatized identities. Identity theories rooted in structural symbolic interactionism assert that identities develop over time but become fairly stable (Kuhn 1964). This assertion underlies the assumption that individuals are motivated to confirm self-views (Burke 1991). As a result, assessing the dynamic aspects of identity formation can be challenging even with multiple waves of data. Nonetheless, truly longitudinal data, ideally data that assess a transitional period, might allow us to better observe the synergistic process between reflected and self-appraisals for individuals who are in the process of recovery.
The nature of the sample should also be considered when interpreting our findings. The sample includes individuals who have been formally diagnosed with SPMI and are receiving community mental health services. These individuals may differ from individuals who self-label or who are diagnosed but not seeking services or treatment. Although theoretically individuals in our sample are equally likely to be responsive to reflected appraisals and to be motivated to verify self-views, having received mental health services may result in their being psychologically healthier than individuals who have an undiagnosed or untreated mental illness (Marcussen and Ritter 2016; Rosenfield 1997). Again, it would be instructive to examine identity processes across various stages of mental illness, including before entering treatment.
Our findings related to self-esteem also deserve further attention. We found that stigmatized self-views were significantly associated with poorer self-esteem; however, stigmatized reflected appraisals and identity discrepancies were not. It is not uncommon for self-esteem, particularly global self-esteem, to show small or weak effect sizes in social psychological research, including identity research (e.g., Cast and Burke 2002). There are a number of explanations for these modest effects, ranging from conceptual to methodological (see MacKinnon 2015 for a review). We focus on two explanations that target the source of stigmatized appraisals (self or other) and the management of a stigmatized identity.
According to identity scholars, different bases of identity (role, group/social, person) are associated with different components of self-esteem (Burke and Stets 2009; Stets and Burke 2014b). Group or social identities, which relate to social integration, are most strongly related to feelings of self-worth. Importantly, for group or social identities, the comparison point is often other members of the group. To the extent that mental illness functions as a group or social identity, it is possible that reflected appraisals from peers would be more closely associated with self-worth than reflected appraisals from the generalized other, as measured in this study. Along these lines, Crocker and Major (1989) suggest that individuals cope with stigmatized statuses by comparing themselves to members of their “in-group” (e.g., others with mental illness) and devaluing characteristics of the “out-group” (e.g., others without mental illness). According to these authors, these strategies might explain a weak empirical relationship between stigma and self-esteem. An important direction for future research examining identity theories of mental illness may be to explore the extent to which one’s mental health status reflects one or all of the bases of identity as defined by Stets and colleagues (Stets and Burke 2014b; Stets and Serpe 2013), keeping in mind that different interactional environments may draw out different characteristics of the identity.
The modest relationship that exists between stigma and self-esteem may also be a result of stigma resistance strategies used by individuals who perceive devaluation and discrimination (Thoits 2011). Resistance can take the form of deflection strategies (cognitive strategies that distance individuals from the mental illness identity) or challenging strategies (behavioral strategies that aim to change others’ views of mental illness). In the present study, we found identity centrality (i.e., my mental illness is a major part of who I am) was associated with poorer self-evaluation and greater distress. This finding is consistent with Thoits’s research, which shows that deflection strategies (reflecting the opposite of centrality) are associated with lower levels of distress and higher positive affect (Thoits 2016; Thoits and Link 2016). Moving forward, examining stigma resistance in the context of the perceptual control model would be particularly useful. On the one hand, deflection strategies may temper the effects of stigmatized reflected appraisals on self-views as individuals assume that perceptions about mental illness do not apply to them (Marcussen and Asencio 2016). On the other hand, challenging others’ perceptions of mental illness represents a more active strategy that constitutes meaningful behavior (Burke 1991) designed to change perceptions of how others see mental illness. These strategies have the potential to promote positive self-evaluation and psychological well-being, as well as highlight the role of personal agency in identity processes and mental health recovery.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Northeast Ohio University Office of Research and Sponsored Programs (Christian Ritter, PI) to establish a Research Focus Area in Community-based Mental Health Research.