
Abstract
Research on relative deprivation (RD) and health has focused primarily on adult populations. Using the National Longitudinal Study of Adolescent to Adult Health, this study examines the link between RD and adolescent depression and is the first to test the mechanisms that underlie this relationship. This study finds that controlling for school fixed effects, family income, and observed characteristics of students and their families, students with higher RD within schools exhibit more depressive symptoms. This study also considers how RD may influence adolescent depression. Sobel-Goodman mediation tests reveal that a combination of lowered self-esteem and future expectations (especially about educational attainment) explains nearly half of the association between RD and adolescent depression. Results of this study suggest that social inequality and stratification may implicate population health in the next generation through socioeconomic stratification within schools.
Introduction
Socioeconomic status (SES) is viewed as one of the most important determinants of health and well-being because it is associated with neighborhood context, health care access, material resources, and many other risk factors. Low SES, whether assessed by income, education, wealth, or occupation, is linked to increased risk of mortality, poor physical as well as mental health, and low levels of subjective well-being (Marmot 2002; Phelan et al. 2004; Reiss 2013). Yet since the early 1990s, studies have demonstrated that SES is important to health not only for those below the threshold poverty level but throughout the SES distribution (Adler, Boyce, and Chesney 1994; Hayward, Pienta, and McLaughlin 1997; Marmot and Wilkinson 2001; Wilkinson 1997). These findings have motivated researchers to consider an individual’s relative position in the SES distribution of a reference group as a potential risk factor of health above and beyond the effects of absolute SES (Deaton 2001; Marmot 2004; Subramanyam et al. 2009).
The theory of relative deprivation (RD) offers a way to study the SES-health link beyond the direct role of objective living conditions on one’s psychological health (Merton 1957; Runciman 1966). The concept of RD differs from other SES measures because RD explicitly involves a reference group with respect to the SES distribution to which individuals compare themselves. RD is an important measure of equitable distribution of resources at the individual level, reflecting conditions of widening economic disparities despite remarkable reductions in absolute poverty in our society. For example, RD captures the fact that in an unequal society, an individual who already has secured a fixed standard of the income required to meet basic subsistence needs can still feel deprived due to inability to maintain the same standard of living as others.
According to the theory of RD, people have a natural tendency to make upward rather than downward social comparisons (e.g., Merton 1957; Runciman 1966; Stouffer et al. 1949). In Runciman’s (1966:10) early descriptions of RD, he wrote that “the magnitude of a relative deprivation is the extent of the difference between the desired situation and that of the person desiring it.” The theory suggests that the standard of living of the person’s reference groups contextualizes how the person understands and experiences deprivation, which in turn shapes psychological health outcomes (Wilkinson 1996). That is, when individuals with higher levels of RD engage in upward comparisons, they are likely to experience worse psychological health and well-being, such as anger, depression, stress, and frustration (Wilkinson and Pickett 2006).
Despite compelling evidence that RD is consequential for an individual’s psychological health (e.g., Eibner and Evans 2005; Kondo et al. 2008; Subramanyam et al. 2009; Wildman 2003), most previous studies on this topic focus on adult populations. Relatively less is known about whether and how RD determines the psychological health of adolescents. Given that schools are a social context ripe for observation, interaction, and social comparison among adolescents, it is imperative to examine the effect of RD on adolescent mental health. Using data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) and computing students’ RD based on information about classmates’ household income, this study analyzes the link between RD and adolescent depressive symptoms.
This study’s contribution to the existing literature is threefold. First, this study builds on the few studies about the relationship between RD and youth outcomes. Previous studies document that RD is associated with the likelihood of engaging in delinquent and violent behavior (e.g., Balsa, French, and Regan 2014; Bernburg, Thorlindsson, and Sigfusdottir 2009). This research has improved our knowledge in this area and invites further empirical work that directly examines whether and how RD within schools shapes adolescent health. One of the few studies of a within-school analysis, by Elgar et al. (2013), documents the association between RD and self-reported psychosomatic symptoms among adolescents in Europe and North America. Despite this important finding, the use of cross-sectional data and lack of information about precise estimates of SES (besides material assets) limit our understanding about the relationship between RD and adolescent health.
Second, this study provides novel insights about underlying mechanisms through which RD influences adolescent mental health. Most previous studies focus almost exclusively on psychological distress or deficits (e.g., low self-esteem and lack of sense of control) resulting from upward social comparisons as the primary mechanism linking RD to mental health. In addition to this pathway, research about adolescence reveals indirect channels through which RD may influence psychological health among adolescents. This study investigates an additional potential mechanism: expectations about one’s future. Student perceptions about their relative status compared with peers may determine how they perceive their own future possibilities (Jamieson and Romer 2008), which may in turn affect adolescent psychological health (e.g., Webber 2007).
Third, this study offers a unique methodological contribution to this area of research. Addressing nonrandom sorting into reference groups is a key challenge in estimating social and contextual effects. Peer groups, including schoolmates and best friends, are not randomly assigned to individuals. Adolescents select into schools and friendships, and this selection is systematic and may be unobservable to researchers. To account for self-selection, this study adopts a quasi-experimental research design, wherein I control for school fixed effects to leverage quasi-experimental across-cohort variation in students’ parental income distribution (e.g., Balsa et al. 2014).
Background
RD and Adolescent Health
Schools are a critical context because youth spend most of their time in a given day at school and develop most of their current friendships, mentorships, and other relationships in schools (Coleman 1961). In particular, school peers provide a social context ripe for observation, interaction, and social comparison, serving as the most sensible and salient reference group for adolescents (Abrutyn and Mueller 2014; Crosnoe 2011; Mangyo and Park 2011). Students compare their own characteristics with those of their peers to make assessments about themselves, and they internalize these social comparisons if they have less resources relative to their peers (e.g., Mueller 2015; Mueller et al. 2010).
A number of previous studies have documented that, after adjusting for objective SES measures, subjective perceptions of family SES at the community or society level are associated with adolescents’ physical, mental, and behavioral health outcomes (Goodman et al. 2001; Goodman et al. 2003; Goodman et al. 2007; Gruenewald, Kemeny, and Aziz 2006; Ritterman et al. 2009). Although these findings highlight the importance of defining family SES in relative terms to better understand the effect of family SES on adolescent health, they are limited in that (1) subjective perceptions of family SES are endogenous (with respect to the health outcomes being studied) and (2) the role of peers and schools are largely ignored. More recent studies have addressed these limitations by using RD within schools as a key explanatory variable. A few studies show that RD (measured by the Yitzhaki Index), net of absolute family affluence, is associated with higher levels of obesity risk factors (such as unhealthy eating behavior and physical inactivity) (Elgar et al. 2016), psychosomatic symptoms (Elgar et al. 2013), and substance use (Balsa et al. 2014).
While these studies suggest potentially important relationships between RD within schools and adolescent health, gaps in the literature invite further investigation. Their ability to draw causal inferences is limited because previous studies rely solely on cross-sectional study designs unable to address the endogeneity of RD. In addition, few existing studies have utilized parental income, the SES measure upon which the theory and measurement of RD are based. Due largely to data limitations, a majority of previous studies use alternative SES measures such as material assets and parental education (Elgar et al. 2016). Using Add Health, a large-scale, school-based longitudinal survey, this study aims to establish whether RD within schools is associated with adolescent depressive symptoms. Based on information about classmates’ household income, RD is computed in various ways, including the Yitzhaki Index, Deaton’s formulation, and inverse percentile rank.
Mechanisms Linking RD to Adolescent Mental Health
The theory of RD and the existing literature on adolescence suggest that RD may shape psychological health via two mechanisms: (1) psychological resources and (2) future expectations. Although these mechanisms are not necessarily mutually exclusive and may operate in parallel, conceptually differentiating them as distinct mechanisms clarifies the multiple dimensions that may shape adolescent psychological health and well-being. Each pathway is explained below.
Psychological resources
The theory of RD argues that people tend to make upward social comparisons (e.g., Merton 1957; Runciman 1966; Stouffer et al. 1949). Runciman (1966:10) wrote that “the magnitude of a relative deprivation is the extent of the difference between the desired situation and that of the person desiring it.” Therefore, RD can affect individual health through psychosocial stress generated by upward social comparisons (e.g., anxiety, shame, frustration, and injustice) (Wilkinson 1996).
RD may arise in the lives of adolescents when they compare their own standard of living to that of their peers. Schools are an important venue in which adolescents learn about the standard of living of peers and their families (Coleman 1961; Crosnoe 2011). Adolescents who grow up in a family that is relatively worse off than their school peers realize their lower social position in the school-based hierarchy (Bourdieu 1984). Those with lower SES positions in the peer hierarchy may have worse mental health because they may feel relatively deprived of access to material resources and unable to imitate the lifestyle of their better-off peers (Pettigrew 2016; Wilkinson 1996). Children identify peers living in larger houses, driving more expensive cars, or going on lengthy vacations as rich (Weinger 1998) and use these high-wealth cues to guide their evaluations of others and themselves (Shutts et al. 2016). The negative effect of RD on adolescents’ psychological health and well-being may thus occur through their psychological deficits: low self-esteem, lack of sense of control, and feelings of inferiority and shame (Marmot et al. 1997).
Future expectations
RD influences other dimensions of psychological resources associated with health outcomes. Adolescence is a period in which youth begin to anticipate their lives as adults and figure out how they will relate to the broader society (Wilson 1987). For adolescents, feelings of RD (or perceptions of affluence of peers, the assumed reference group) may shape future expectations and aspirations (Jamieson and Romer 2008). Adolescents internalize feelings of RD if their peers are better off compared to them, which may create a sense of injustice, marginalization, and disbelief in equality because they feel deprived of the opportunities to fulfill their potential and to control life circumstances (Blau and Blau 1982; Runciman 1966).
Social comparisons that arise from RD may breed sentiments of fatalism and hopelessness about the future. RD may foster adolescents’ skepticism about the returns of their personal investments in education as they perceive that others possess more resources than they do to achieve desired goals (Wilson 1987). This, in turn, may produce a sense of powerlessness, fatalism, and helplessness toward their life chances such as their future income, education, housing status, health, and life itself. Therefore, adolescents who experience higher levels of RD may perceive goal blockage and have lowered future expectations, which may cause psychological strain and distress (Webber 2007).
In support of this proposition, existing evidence suggests that an increased likelihood of engagement in delinquent behavior among adolescents with higher RD can be explained by their feelings of injustice and unfairness as well as diminished future expectations (Harris, Duncan, and Boisjoly 2002; Napoletano et al. 2015). These negative psychological processes triggered by RD may be relevant for adolescent psychological health because during this period, youth develop lifestyle expectations and educational as well as occupational goals that will shape their adult lives. Taken together, RD may influence adolescent psychological health through not only dissatisfaction with current family SES position but also declines in future expectations about one’s educational attainment and life chances.
Data and Methods
Data
This study uses data from the restricted version of Add Health. Add Health is a school-based, longitudinal study of the health-related behaviors of adolescents and their outcomes in young adulthood. Beginning with an in-school questionnaire administered to a nationally representative sample of students in grades 7 through 12 in 1994–1995, the study follows up with participants via a series of in-home interviews approximately 1 year (wave 2), 6 years (wave 3), 13 years (wave 4), and 22 years later (wave 5). Other sources of data include questionnaires for parents, siblings, fellow students, and school administrators. By design, Add Health included a sample stratified by region, urbanicity, school type, ethnic mix, and size.
An unusual feature of Add Health is that the survey covers multiple cohorts within the same school. This feature is essential for this study’s identification strategy because it allows for comparison of students in different cohorts within the same school while accounting for selection into schools. Of the 14,736 respondents who completed both wave 1 and wave 2, 13,281 have cross-sectional weights and valid school identification codes. I dropped 254 respondents who have missing values on the dependent variable as well as proposed mechanism variables, leaving 13,027 students.
Dependent Variable
The dependent variable of this study is depressive symptoms measured by a 19-item self-report measure of the Center for Epidemiological Studies Depression Scale (CES-D) at wave 2 (Meier 2007). CES-D assesses respondents’ feelings, thoughts, and physical conditions during the past week. Each question had four response categories: 0 = never or rarely, 1 = sometimes, 2 = a lot of the time, and 3 = most of the time or all of the time. The final scale is the standardized average of the 19 item responses (Cronbach’s alpha = .87). A detailed description about the dependent variable is in Table S1 in the supplementary file.
Independent Variable
RD
The key independent variable is an individual-specific measure of RD in wave 1. I compute different measures of RD, including the Yitzhaki Index, Deaton measure, and inverse percentile rank. RD is commonly measured by the Yitzhaki Index, which combines information about the rank of an individual within a reference group and the extent of the inequality between the individual and better-off members in that group (Adjaye-Gbewonyo and Kawachi 2012). The Yitzhaki Index is a mathematical expression of Runciman’s (1966) theory. Runciman defines the conditions under which an individual feels relatively deprived: We can roughly say that a person is relatively deprived of X when (1) he does not have X; (2) he sees some other person or persons who have X, which may include himself at some previous or expected time, as having X; (3) he wants X; and (4) he sees it as feasible that he should have X. (P. 10)
Therefore, drawing on Runciman’s theory, the Yitzhaki Index can be expressed as follows:

where
Intuitively, student i feels deprived whenever he or she meets peers whose parents have a higher income, and the amount of i’s deprivation is proportional to the difference between
A limitation of the Yitzhaki Index is that it may be sensitive to changes in the scale of SES measures. For example, doubling the incomes of everyone in a reference group will double every individual’s RD. To circumvent this shortcoming, I use an alternative measure of RD. Deaton (2001) improves the Yitzhaki Index by normalizing it using the average income in the reference group,

In addition to the Yitzhaki Index and Deaton measures, I use ordinal rank (i.e., inverse percentile rank in terms of parental income), which parsimoniously captures students’ relative positions and ignores the distance between their affluence and all the affluence scores above them. To make the ordinal rank comparable across school cohorts of different sizes, I standardize the absolute ordinal rank by dividing it by the number of students in each school cohort. Percentile ranks can be calculated as follows:
I show main results using all three measures to test the robustness of the results. For mediation analyses, I present only results using Deaton’s version of the Yitzhaki Index since models using different indices of relative measures produce substantively similar results. To compute the measures of RD, I use parent’s self-reported family income. Parents were asked the following question: “How much total income, before taxes, did your family receive in 1994? Include your own income, the income of everyone else in your household, and income from welfare benefits, dividends, and all other sources.”
Figure 1 describes the extent to which the Deaton measure varies for a given decile in own family income. There are large differences between the two measures. The variation in the Deaton measure is strongest at the lower ends of the global distribution and smaller at the upper ends. Students at the upper end of the global distribution of family income are more likely to be at the bottom of the distribution of any school cohort in terms of the Deaton measure. By contrast, students at the lower end of the global distribution (especially from the second to fifth decile) are in a wider range of the distribution of the Deaton measure, depending on their peers’ family incomes.
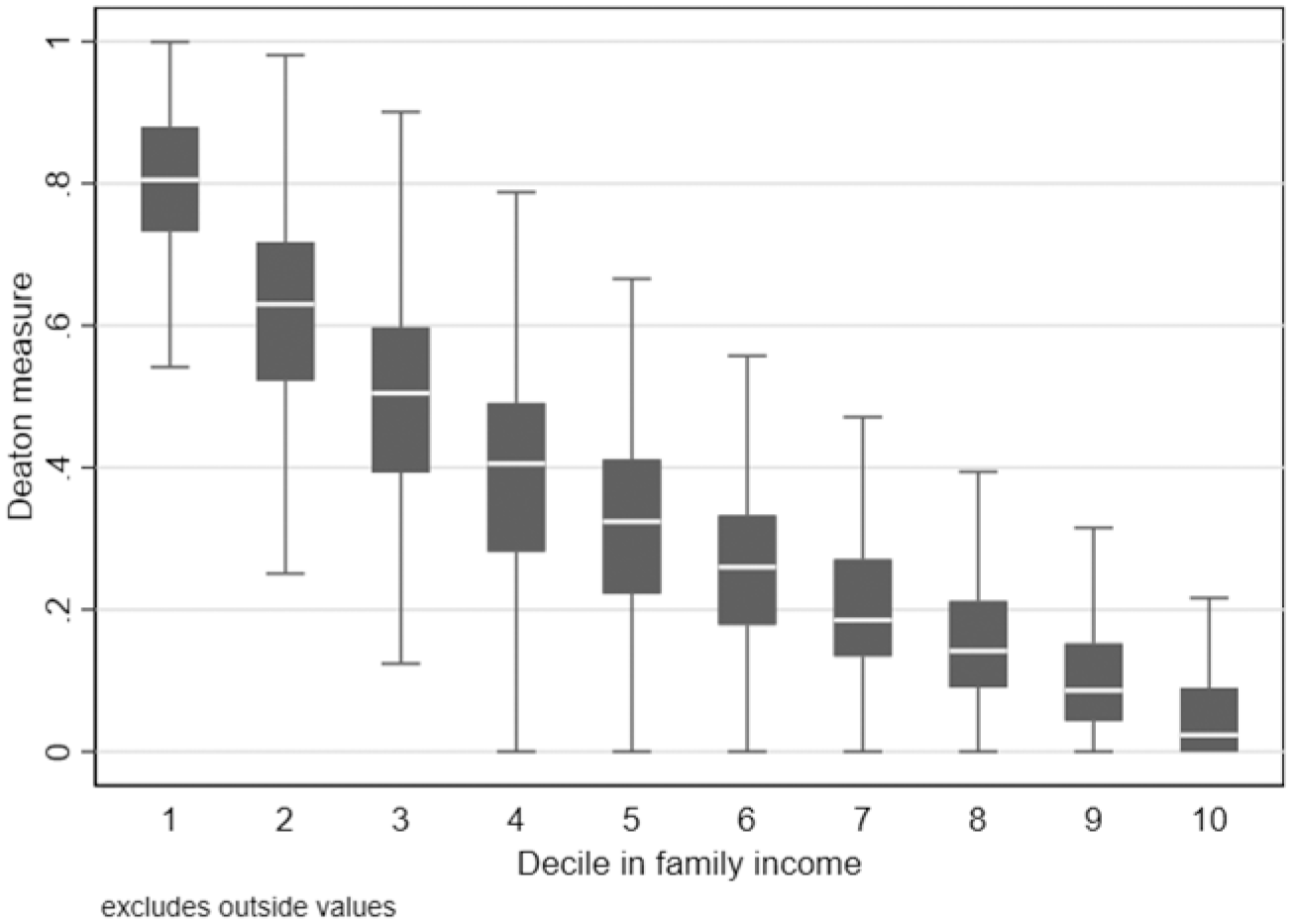
Family income versus Deaton measure.
In fact, the identification strategy of this study relies on a relatively smaller within-school/across-cohort variation. This strategy compares students in different cohorts who attend the same school and have the same level of family income but different relative SES positions due to an exposure to differential family income distribution of a school cohort. To further quantify the magnitude of this variation, I compute the within-school variance of the Deaton measure, conditional on student’s own family income, school, and cohort dummies. I find that it has a standard deviation of 0.19. Given that the Deaton measure is bounded between 0 and 1, this is a substantial variation within a school across cohorts. This suggests that the same family income can lead to very different relative SES positions depending on the cohort composition.
Mediating variables
A large set of potential mechanism variables is used in the analysis. All mechanism variables are measured in wave 1 to establish the temporal ordering between the outcomes and mechanism variables. First, psychological resources consist of two measures of psychological deficits including self-esteem and locus of control. Second, the measure of future expectations includes educational expectations and life chances expectations. Due to space limitations, a detailed description about mechanism variables is shown in Table S1 in the supplementary file.
Control variables
The following control variables are included in all regression models: gender, age, race/ethnicity (white, black, Hispanic, other race/ethnicity), standardized Peabody Picture Vocabulary Test (PVT) score, an indicator of first-born child status, grade level (grades 7–12), mother’s education, family income, and rural status. I also use depressive symptoms measured at wave 1 as a control variable. As a robustness test, I include the following set of grade-level characteristics: mean family income, percentage white, percentage black, percentage female, mean standardized PVT score, and mean maternal education. Summary statistics of the variables used in this study are presented in Table 1.
Summary Statistics, National Longitudinal Study of Adolescent to Adult Health (N = 13,027).
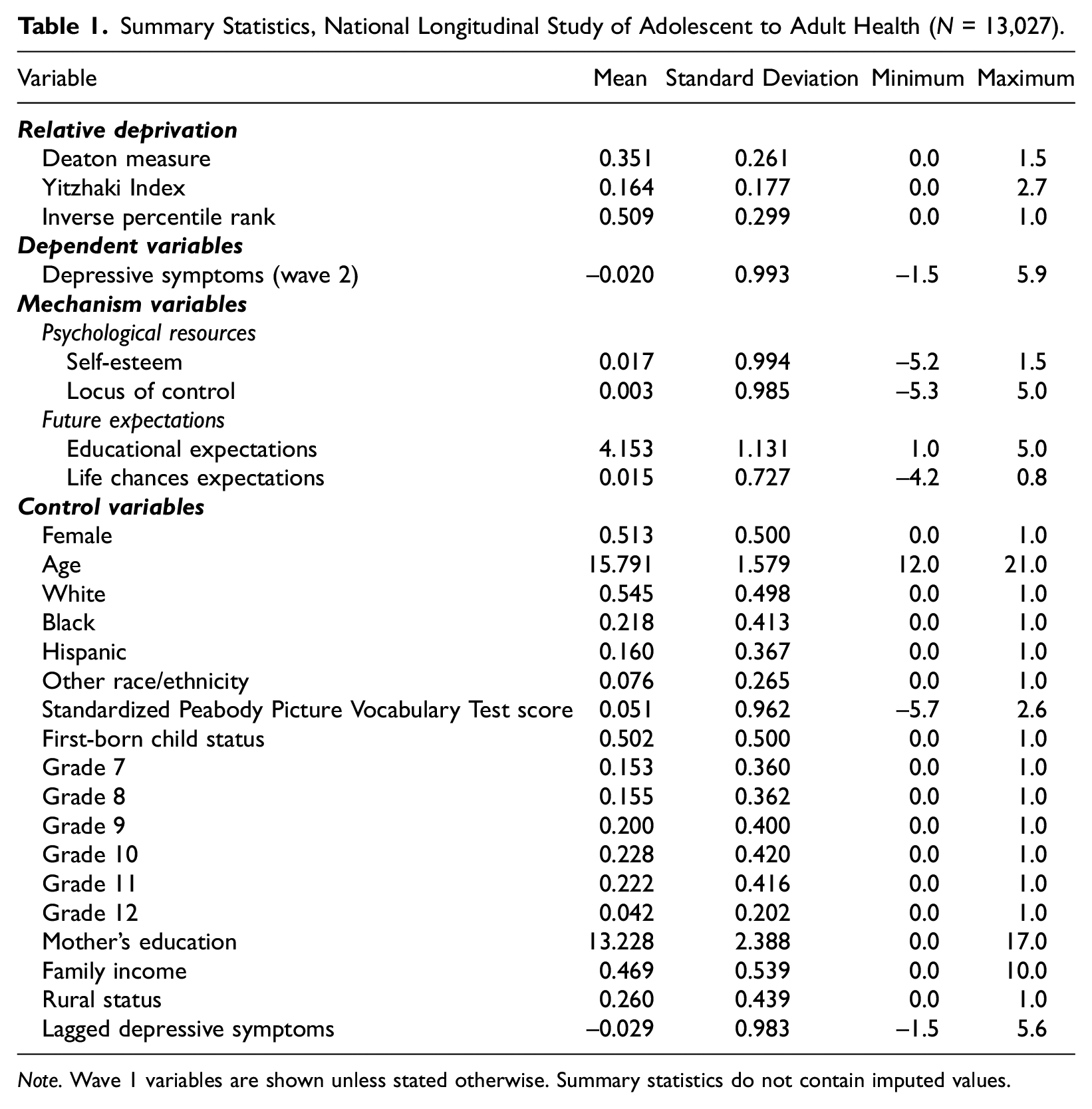
Note. Wave 1 variables are shown unless stated otherwise. Summary statistics do not contain imputed values.
Analytic approach
Similar in spirit to Balsa et al. (2014), this study leverages idiosyncratic variation in the cohort composition within the same school over time, which provides the basis for a quasi-experimental design. This strategy allows us to compare students in different cohorts in the same school who have the same level of family income but different relative SES positions due to exposure to a differential family income distribution of a school cohort. A key assumption of this research design is that parents purposely choose schools for their children but do not choose their children’s school cohorts. In a later section, I present evidence consistent with this key assumption, showing that school cohort composition (i.e., family income distribution) is exogenous to a host of student and family characteristics conditional on attending a given school. The primary empirical specification of this paper is as follows:

where the subscript g references the student’s grade and s represents her school. Y is wave 2 depressive symptoms for student i in grade g in school s. I estimate the equation using ordinary least squares (OLS) regression. FAM_INC is a student’s own family income. It is worth noting that, in this specification, the coefficient for family income,
A set of covariates includes a vector of student characteristics measured at the individual level (
To further address concerns about selection, this study estimates a lagged dependent variable (LDV) model. By directly modeling prior depressive symptoms (at wave 1), the LDV model adjusts for factors that are unobserved but that influence depressive symptoms and thereby influence current depressive symptoms (at wave 2). Thus, the LDV model improves upon equation 1 by reducing biases associated with unmeasured characteristics (i.e., controlling for selection into RD that is correlated with the outcome). However, the LDV model is unable to adjust for factors that differentially affect prior and current depressive symptoms. A more important shortcoming of the LDV model is that if residual autocorrelation is present, the LDV model causes coefficient estimates to be biased downward (Keele and Kelly 2006). With these points in mind, the current study presents results from both LDV models and OLS models without controls for depression at wave 1.
To investigate the potential mechanisms linking RD to depressive symptoms, this study conducts univariate and multivariate Sobel-Goodman mediation tests (Sobel 1982). Sobel tests indicate the proportion of the association between RD and depressive symptoms that can be attributed to a mediating variable as well as the significance of the indirect mediating effect.
Missing values for the income measures and the covariates were imputed using the chain equations (ICE) procedure in STATA 15.1 (Allison 2002). They were imputed with prediction equations that included all other variables in the analysis. While the dependent variable was not imputed, it was included in the imputation procedure (von Hippel 2007). I performed 10 imputations to predict missing values (Royston 2004). I estimate equation 1 within each imputed data set, and combined estimates were computed based on the 10 imputed data sets. Given the possibility that data are missing not at random in Add Health (especially on parental income), I investigated whether listwise deletion changes the results of this study (Allison 2002; Johnson and Young 2011). I also examined whether results are similar when omitting adolescents not living with either parent whose parental income is more likely to be missing. I found that the findings are substantially robust to the use of listwise deletion and restricting the sample to those living with at least one biological parent (see Tables S2 and S3 in the supplementary file).
Associations between Relative Deprivation and Wave 2 Depressive Symptoms.

Note. Robust standard errors are clustered at the school level in all models. All models include school fixed effects. Cross-sectional weights are used.
p < .10. *p < .05. **p < .01. ***p < .001.
Results
Before presenting the empirical results of the association between RD and adolescent depression, I show evidence of whether, conditional on attending a given school, parental income composition of cohorts is quasi-exogenous. I conduct an empirical test that mimics analyses often conducted in the randomized control trials. I first examine whether the cohort mean parental income is correlated with predetermined student characteristics by running regressions of several important student characteristics on cohort mean parental income. Then, I examine whether controlling for school fixed effects removes statistically significant correlations. Disappearance of the associations after fixed effects are applied is evidence that within-school cohort-to-cohort variation in parental income distribution is plausibly exogenous.
Figure 2 plots correlations between school cohort mean income and individual-level characteristics (full regression results are presented in Table S4 in the supplementary file). Each dot is a coefficient from a separate regression and is labeled with the name of the dependent variable. Coefficients with school fixed effects are in the right panel of Figure 2. As shown in the left panel of Figure 2, cohort mean parental income is significantly correlated with each individual characteristic. However, when school fixed effects are controlled (the right panel of Figure 2), these associations disappear (i.e., small and statistically insignificant coefficients). This indicates that while there is strong systematic selection into schools, conditional on attending a given school, cohort-to-cohort variation in parental income distribution is plausibly exogenous (or quasi-random).
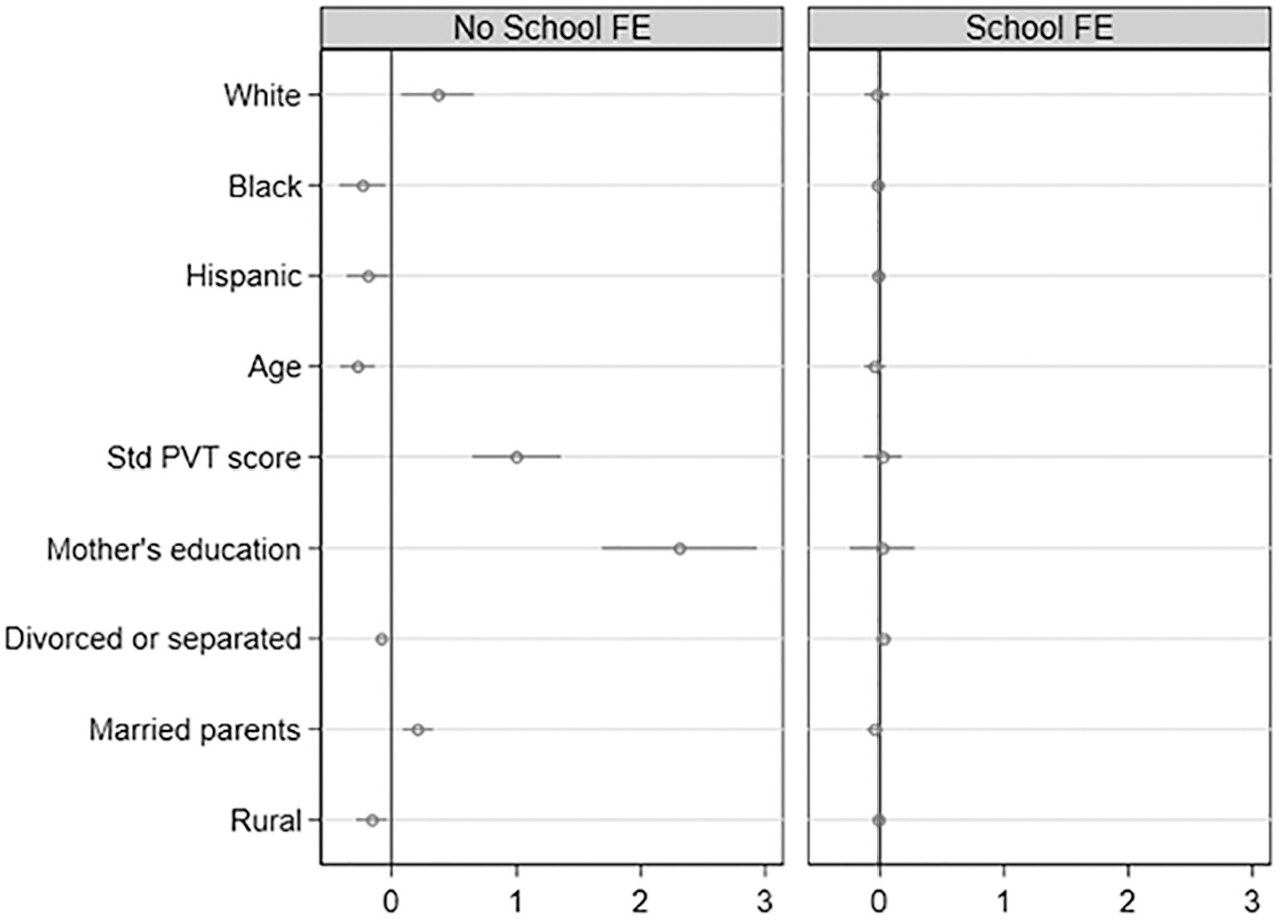
Balancing tests of grade-level mean parental income.
Table 2 presents OLS estimates of the association between RD and adolescent depressive symptoms. All models include individual-level demographic controls, family-level controls, student’s own parental income, and grade as well as school fixed effects. The odd-numbered columns present the main OLS results, and the even-numbered columns control for wave 1 depressive symptoms. Column 1 demonstrates that a higher score on the Deaton measure is associated with an increase in depressive symptoms (b = .179). To interpret, a one-standard-deviation increase in the Deaton measure of RD increases approximately 5 percent of a standard deviation in depressive symptoms ([.179 × .261] / .993). This is equivalent to the change in depressive symptoms associated with a 2.5-year decrease in mother’s years of schooling ([.179 × .261] / –.019).
Column 2 presents the results from the LDV model. In column 2, the coefficient of the Deaton measure represents the marginal impact of an increase in the Deaton measure on depressive symptoms at wave 2, conditional on earlier depressive symptoms, which is why the magnitude is not directly comparable to the one in column 1. Results show that the inclusion of LDV reduces the coefficient of the Deaton measure by about 47 percent. However, it is important to note that, even after controlling for LDV, the association of the Deaton measure and depressive symptoms remains statistically significant. These results provide evidence of the robustness of the OLS results to potential omitted variable bias. Moreover, as shown in columns 3 through 6, results are consistent and robust across other measures of RD (i.e., the Yitzhaki Index and inverse percentile rank). To interpret, a one-standard-deviation increase in the Yitzhaki Index and inverse percentile rank increases about 4 and 6 percent of a standard deviation in depressive symptoms, respectively.
To confirm the internal validity of the findings of this study, I discuss results from a series of robustness checks. I provide results of sensitivity checks with respect to alternative methods of controlling for own parental income (see Table S5 in the supplementary file). By allowing for a flexible functional form of income (i.e., natural logarithm, quadratic and cubic polynomials), I confirm that the coefficient of RD is not an artifact of a highly nonlinear relationship between parental income and depressive symptoms (Jones and Wildman 2008). Throughout the rest of the article, I control for parental income for the linear term because despite some attenuation (about 12–29 percent) results are robust to different methods of controlling for parental income. The goodness-of-fit statistics (including Akaike information criterion and Bayesian information criterion) show that allowing for nonlinearities does not improve model fit. This suggests that the linear controls for parental income are preferable and parsimonious (results not shown).
I address the possibility of contextual-level confounders. In the main model, I included separate fixed effects for schools and cohorts, allowing for comparisons of students with the same absolute parental income who belong to different cohorts in the same school. The school fixed effects control for observed and unobserved factors that affect selection into schools. However, school-cohort-specific confounding factors cannot be captured by these separate school and cohort fixed effects. An alternative specification might be to control for a vector that captures the average demographic characteristics of the student’s classmates or to replace separate school and grade fixed effects with school-by-grade fixed effects. I show that results of this study are robust to controls for several important grade-level characteristics as well as school-by-grade fixed effects (see Table S6 in the supplementary file).
To shed light on potential mechanisms through which RD shapes adolescents’ depressive symptoms, I estimate several auxiliary regression models. I begin by examining the links between RD and a set of proposed mechanism variables that represent two broad pathways. I then conduct Sobel-Goodman mediation tests to investigate whether the association between RD and depressive symptoms is explained by proposed mechanism variables.
Table 3 presents results for regressions of potential mechanism variables on the Deaton measure of RD. In Table 3, mechanism variables are listed in the first column, and only the coefficients of the Deaton measure are presented. Panel A of Table 3 demonstrates that RD predicts lower levels of self-esteem and locus of control. Panel B of Table 3 shows that students with higher RD tend to report lower educational expectations and tend to be more pessimistic about their life chances.
Associations between Relative Deprivation and Wave 1 Mechanism Variables (N = 13,027).
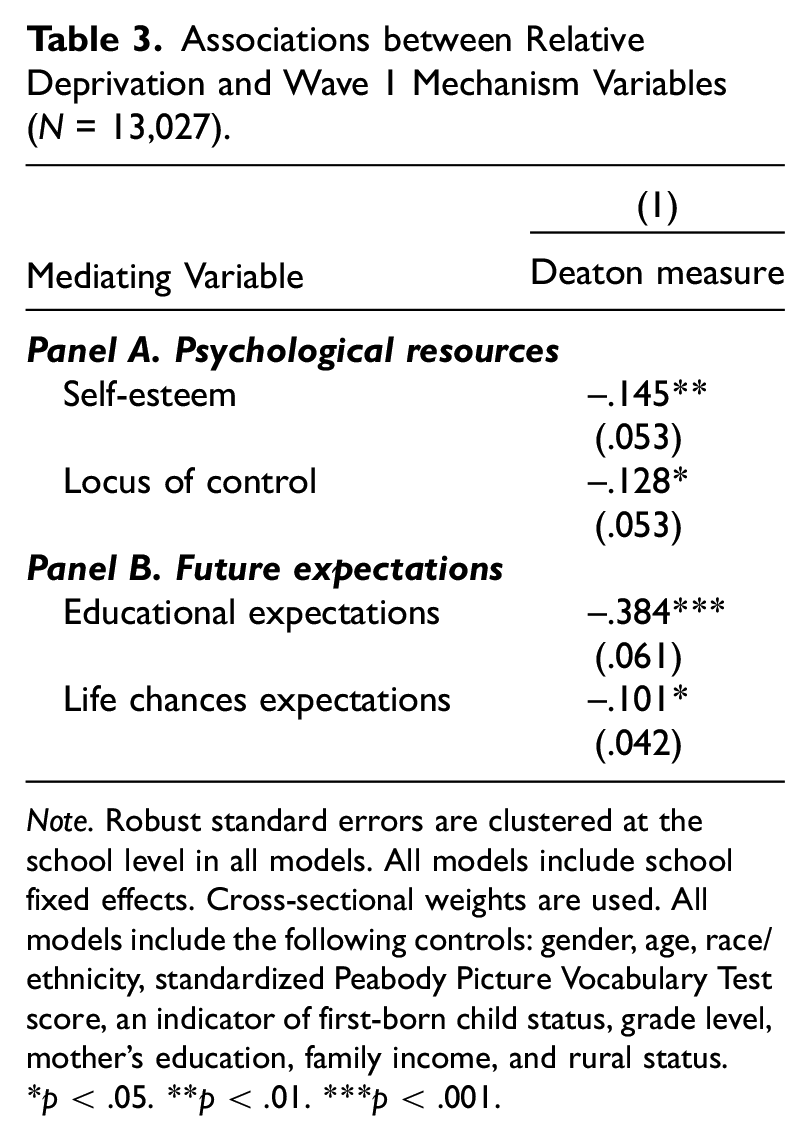
Note. Robust standard errors are clustered at the school level in all models. All models include school fixed effects. Cross-sectional weights are used. All models include the following controls: gender, age, race/ethnicity, standardized Peabody Picture Vocabulary Test score, an indicator of first-born child status, grade level, mother’s education, family income, and rural status.
p < .05. **p < .01. ***p < .001.
In Table 4, I investigate whether proposed mechanism variables mediate the relationship between RD and depressive symptoms. Columns 1 and 2 present results for univariate Sobel-Goodman mediation tests. Results show that both psychological resources and future expectations partially attenuate the observed association between RD and depressive symptoms. Panel A demonstrates that self-esteem and locus of control explain about 23 and 7 percent of the association, respectively, though the indirect effect of locus of control is statistically insignificant. In panel B, educational expectations and life chances expectations mediate about 33 and 15 percent of the relationship between RD and depressive symptoms, respectively.
Sobel-Goodman Mediation Tests.
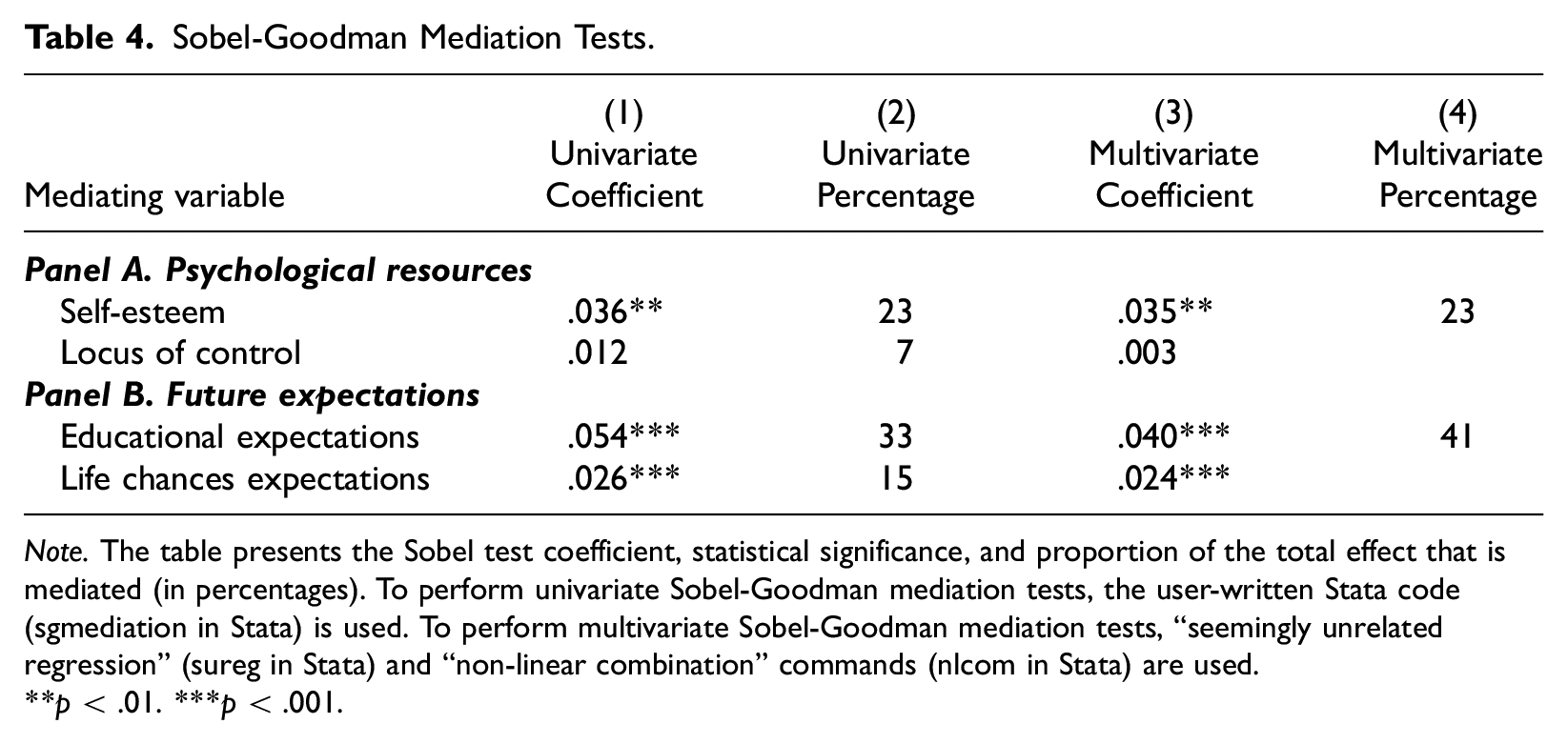
Note. The table presents the Sobel test coefficient, statistical significance, and proportion of the total effect that is mediated (in percentages). To perform univariate Sobel-Goodman mediation tests, the user-written Stata code (sgmediation in Stata) is used. To perform multivariate Sobel-Goodman mediation tests, “seemingly unrelated regression” (sureg in Stata) and “non-linear combination” commands (nlcom in Stata) are used.
p < .01. ***p < .001.
In columns 3 and 4, results from multivariate mediation analyses show that the total mediated effects for psychological resources and future expectations are estimated to be about 23 and 41 percent, respectively. These results suggest that the contribution of reduction in future expectations to a high level of depressive symptoms is larger than that of psychological deficits. Results from a multivariate mediation analysis to consider all proposed mechanism variables jointly indicate that the total mediated effect is estimated to be about 46 percent (results not shown). In sum, a combination of psychological resources and future expectations is an important mediating pathway running from RD to depressive symptoms.
In supplementary analyses, I conduct mediation analyses based on the LDV results (see Table S7 in the supplementary file). Results suggest that the mediating effects of psychological resources are reduced from 23 percent to 7 percent. By contrast, despite some attenuation (from 41 percent to 30 percent), the mediating effects of future expectations, especially educational expectations, remain quite robust. In fact, a large reduction in the mediating effect of psychological resources in the LDV model is not surprising given that wave 1 depressive symptoms are correlated with wave 1 self-esteem and locus of control (r = –.48 and –.30, respectively). Therefore, these results should be interpreted cautiously since controlling for wave 1 depressive symptoms may have removed the mediating effects for which psychological pathways may be responsible. Nonetheless, these supplementary results offer additional support for the important role of future expectations in mediating the association between RD and adolescent depression.
Discussion and Conclusion
Although numerous studies document the link between RD and health outcomes, substantial gaps in the literature remain. There is limited evidence about the psychological health implications of RD among adolescents. This study investigates whether and how RD within schools shapes adolescents’ depressive symptoms. Using Deaton’s measure of RD, an improved measure of the Yitzhaki Index (Adjaye-Gbewonyo and Kawachi 2012), this study shows that even after controlling for own family income, RD harms adolescent mental health: A higher score on the Deaton measure is associated with higher levels of depressive symptoms among adolescents. Findings are robust to alternative measures of RD (such as the Yitzhaki Index and inverse percentile rank), motivated by different theoretical and empirical concerns, lending strong support to the theory of RD.
This study offers several novel insights that help unpack the “black box” of the effects of RD on adolescent mental health. This study underscores relatively understudied potential psychological mechanisms of the effect of RD—that is, future expectations. My findings suggest that declines in future expectations are remarkable at explaining the links between RD and adolescent depressive symptoms. This finding indicates that lower psychological well-being or distress is not the only negative consequence of upward comparison’s affecting adolescent psychological health. Adolescents who are relatively deprived tend to use their own experience of relatively lower social status to form future expectations, especially about educational attainment (e.g., Wilson 1987, 1996). Students are more likely to develop deep feelings of fatalism and hopelessness about their educational attainment and life chances when they perceive that they are relatively deprived. These lowered expectations thereby lead to higher levels of depressive symptoms. By contrast, those with higher relative SES positions may be able to maintain and reinforce mainstream cultural values (e.g., high SES attainment) and remain optimistic about the future.
This study is not without limitations. First, this study captures students’ RD at one point in time, leaving open the possibility that RD may be a dynamic and changing variable: Some students’ families may gain income or wealth as the students develop, which increases their relative SES positions. The stability or instability of RD also may be important for adolescent mental health. For instance, if a student experiences more changes in relative SES status throughout childhood and adolescence, he or she may have more uncertainty about life overall and report higher levels of psychological distress. Relatedly, family income may not be a perfect measure for students’ SES because they may not have a precise understanding of own parental income as well as peers’ parental income. Other than income, parental education may be an alternative source of RD among adolescents (e.g., Balsa et al. 2014). Because parental education is available in Add Health, I have examined whether using parental education as a source of RD yields similar results. I found that the association between RD (based on years of schooling completed by mothers) and depressive symptoms was in the expected directions, though this association was statistically insignificant (results not shown). This may be due to substantially reduced variation in parental education and subsequent lower statistical power. Future research is required to determine which factor is a more salient basis for social comparisons among adolescents and how it creates social and cultural environments that harm psychological health and well-being among relatively deprived adolescents.
Second, there may be error in the RD measure. By design, Add Health contains randomly sampled students within schools rather than the population of schools (Harris 2013). Although a robustness test using a subset of “saturated” schools in Add Health that surveyed all students provides strong evidence of the validity and reliability of the measure of RD with statistically negligible error (see Figure S1 in the supplementary file), potential measurement error may lead to attenuation bias. Third, although this study uses two waves of data to explicitly establish temporal ordering of RD and depression in the main model, it is unable to address the issue of reciprocity and temporal ordering in the mediation model. This is particularly a concern when examining self-esteem as a mediator because of the endogeneity of depression and self-esteem at wave 1. Future analyses should attempt to resolve this issue, ideally using panels with more than three waves of data. Fourth, the data are somewhat outdated when considering adolescents’ school life today compared to in the mid-1990s. Upward comparisons may have worse health effects than those captured here because of the widespread use of social media and social networking sites in recent decades (Vogel et al. 2014).
Last, while school fixed-effects models remove all stable school characteristics and nonrandom selection of students into schools, this framework captures only effects of RD that operate through mechanisms that vary across cohorts within schools. If schoolwide RD affects students’ psychological health differently, this impact will be absorbed by the school fixed effects and thus will be missed. Moreover, limiting the deprivation reference group to classmates within the same school may be a source of measurement error because students may use the whole school as a reference group against which they compare themselves. While future research is warranted to disentangle potentially differential effects of class- and school-level RD, it might be empirically difficult to tease them out due to strong correlations between the measures. For example, in this study, cohort-level and school-level measures of RD are highly correlated: Deaton measure = .86, Yitzhaki Index = .82, and inverse percentile rank = .96. Although school fixed effects are believed to eliminate a large part of neighborhood-level confounders, there may be remaining neighborhood-level characteristics that are not removed by school fixed effects but may confound the relationship between RD and adolescent depression.
Despite these limitations, this study makes notable theoretical contributions. First, this study broadens our understanding of how SES might have an impact on adolescent health. Analyzing RD, rather than absolute family SES, clarifies contradictions in the literature about the link between socioeconomic factors and health—that is, the inconsistency of the SES-health gradient in youth (West 1997; West and Sweeting 2004). This study suggests that a part of SES effects on adolescent health may operate through disadvantages in SES position within schools. Moreover, this study considers additional mechanisms that undergird the effect of RD, namely, future expectations about SES attainment. The development of future expectations needs to be considered when examining health implications of RD among adolescents because adolescence is a unique developmental stage for identity formation and future expectations and the link between future expectations and adolescent health is well-established (e.g., McDade et al. 2011).
Second, this study suggests that social inequality and stratification may implicate the next generation’s population health vis-à-vis socioeconomic stratification within schools. In adolescence, emerging school-based social hierarchies and ranking systems may heighten RD to deteriorate physical and mental health especially among those at the lower end of the SES distribution, thereby contributing to health inequalities. In the longer term, RD in school settings may reinforce intergenerational transmission of social disadvantages (Haas 2006). The finding that RD is linked with declines in future expectations about educational attainment provides evidence for the claim that RD hampers social mobility (Wegener 1991).
Findings of this study may inform adolescent health policy. Monitoring RD, rather than exclusively poverty levels, may help schools identify at-risk adolescents and take effective measures to improve their psychological health and well-being. Psychological support and counseling services are a possible intervention to reduce the negative consequences of RD. It also may be important for teachers to help relatively impoverished adolescents feel hopeful about their future, particularly about their future educational trajectories (e.g., college expectations).
This study holds implications for parental school choice and educational policy. Attending schools with higher-SES students has long been believed to benefit adolescent health and educational outcomes. A popular policy response to this claim is to mix rich and poor kids in schools and classrooms (e.g., social or neighborhood mixing). The often-cited argument is that poor kids benefit from interacting with higher-SES students and their families (e.g., Coleman et al. 1966). However, this study documents a possible trade-off between school SES composition and relative SES position—that is, low-SES students attending a school with higher-SES composition should experience higher RD. Therefore, moving to a wealthier neighborhood or school may have distinct health consequences for students, depending on their own SES levels. Since the net effects for an individual student should depend on the extent to which benefits of attending schools with higher SES composition (e.g., average peer quality, teacher quality, and school resources) are offset by drawbacks of having lower relative SES position (as is found in this study), more research is required to better gauge the trade-offs between contextual SES effects and RD effects.
Supplemental Material
RR3_04_RD_depression_supplementary_file_FINAL – Supplemental material for Does Relative Deprivation within Schools Influence Adolescent Depression?
Supplemental material, RR3_04_RD_depression_supplementary_file_FINAL for Does Relative Deprivation within Schools Influence Adolescent Depression? by Jinho Kim in Society and Mental Health
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Korea University (K2008821). This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information about how to obtain the Add Health data files is available on the Add Health website (![]() ). No direct support was received from grant P01-HD31921 for this analysis.
). No direct support was received from grant P01-HD31921 for this analysis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.