
Abstract
Background:
Investigation of the neural substrates of post-traumatic stress disorder (PTSD) in military personnel using whole-brain approaches remains scarce, hindering the development of circuit-based neuromodulatory interventions.
Objectives:
This study aimed to identify potential associations between clinical symptoms and whole-brain resting-state functional connectivity with magnetic resonance imaging in military personnel with adulthood-onset war-related PTSD.
Methods:
Thirty-seven soldiers from the Canadian Armed Forces with moderate to severe treatment-resistant PTSD participated in this study. We assessed PTSD, anxiety and depressive symptoms, quality of life, and time since trauma. We characterized the whole-brain functional connectome using independent component analysis and regions of interest (ROI)-to-ROI connectivity, as well as its topology using graph theory.
Results:
Greater severity of PTSD and anxiety symptoms was associated with lower connectivity (r < 0) between the default mode network (DMN) and frontoparietal network. Greater severity of PTSD symptoms was also associated with a higher nodal clustering coefficient of the inferior parietal lobule from the DMN. Greater severity of anxiety symptoms and longer time since trauma was the only clinical variables that correlated with higher connectivity patterns, all involving the visual networks (the frontoparietal-visual, the visual-DMN, and within-visual networks).
Conclusions:
This work contributes to identifying brain targets for the development of personalized neuromodulatory interventions. In particular, the DMN may be a promising target to alleviate PTSD symptoms, and the visual network may be a target to treat comorbid anxiety symptoms.
Impact Statement
This work aimed to identify clinical correlates of resting-state functional connectivity in military personnel with post-traumatic stress disorder (PTSD) refractory to psychotherapy and pharmacotherapy (N = 37). Our findings indicate that increasing connectivity between the default mode and frontoparietal networks may be a promising therapeutic target to alleviate PTSD symptoms with personalized neuromodulatory interventions, whereas reducing connectivity within the visual network may constitute a target to treat comorbid anxiety. They also emphasize the importance of investigating clinical correlates using whole-brain methods to uncover new target engagement for therapeutic brain circuitry candidates.
Introduction
Military personnel has an estimated lifetime prevalence of post-traumatic stress disorder (PTSD) of up to 30.5% (Fulton et al., 2015; Thomas et al., 2010), as well as more severe symptoms (Naifeh et al., 2008) and worse pharmacotherapy and psychotherapy treatment outcomes than civilians (Bradley et al., 2005; Watts et al., 2013). Neuromodulatory treatments such as repetitive transcranial magnetic stimulation hold promises to treat PTSD. However, there is a need to understand the neural substrates of military PTSD related to symptom severity to develop such brain circuit-based treatments. Resting-state functional connectivity from fMRI (rs-fcMRI) analyzed with independent component analysis (ICA) provides valuable insights by identifying spatiotemporally consistent intrinsic connectivity networks (Damoiseaux et al., 2006; Laird et al., 2011). Graph theoretical approaches complement ICA by characterizing the brain’s global connectivity in regard to strength and modularity of the structural and functional topology (Bullmore and Sporns, 2009; see also Menon, 2011, for a review on the importance of large-scale brain network in psychiatric disorders).
Overall, rs-fcMRI studies in PTSD reported global patterns of weaker functional connectivity (see Bao et al., 2021 and Ross and Cisler, 2020 for reviews). This pattern of weaker connectivity frequently involves the default mode network (DMN), either in whole or in part (Akiki et al., 2017,2018; Tursich et al., 2015; Shang et al., 2014; Zhang et al., 2015; Sripada et al., 2012; DiGangi et al., 2016). However, only a few studies investigated the clinical correlates of these rs-fcMRI patterns in military personnel. It has been observed that greater PTSD symptom severity correlated with weaker connectivity between the ventromedial prefrontal cortex (vmPFC) and the middle frontal gyrus (MFG) and between the parahippocampal gyrus and the anterior insula (Misaki et al., 2018), as well as with higher DMN clustering coefficient (Akiki et al., 2018).
This study aimed to investigate the association between clinical symptoms and rs-fcMRI in military personnel with adulthood-onset war-related PTSD. We hypothesized that greater severity of PTSD symptoms correlates with lower connectivity implicating the DMN (Bao et al., 2021). We used group-level brain parcellations derived from ICA components to test this and further explored subnetwork-level nodal implications with a region of interest (ROI)-to-ROI approach. We also hypothesized that greater severity of PTSD symptoms would correlate with greater clustering coefficient in DMN regions (Akiki et al., 2018). We tested this with a dimensional data-driven network-based graph theory approach. Finally, we explored if severity of depression or anxiety symptoms, quality of life, and time since trauma correlate with rs-fcMRI measures.
Methods
Participants
Thirty-seven military personnel (active-duty or veterans) from the Canadian Armed Forces diagnosed with PTSD according to the DSM-IV-TR criteria (American Psychiatric Association, 2000) by psychiatrists in tertiary practice at a clinic dedicated to operational stress in military personnel participated in this study. Main inclusion criteria included adulthood-onset war-related PTSD within the past 25 years, a PTSD Checklist-Military (Weathers et al., 1994) score greater than 50 during the initial clinical evaluation and greater than 35 at the study screening visit, absence of neurological or psychiatric conditions aside from PTSD, anxiety, depression, and tobacco use disorders. We obtained written informed consent from participants before inclusion in the study. Participants’ characteristics are outlined in Table 1. The Research Ethics of the Canadian National Defense approved this study protocol.
Participants’ Characteristics
Clinical assessment
We measured PTSD symptoms with the Modified PTSD Symptom Scale–Self-Report (MPSS-SR) (Falsetti et al., 1993), depressive symptoms with the Beck Depression Inventory (BDI) (Beck et al., 1988), anxiety symptoms with the Beck Anxiety Inventory (BAI) (Fydrich, 1992), and quality of life in terms of general symptoms distress, interpersonal relations, and social role with the Outcome Questionnaire-45 (OQ-45.2) (Boswell et al., 2013). These questionnaires present good validity and reliability (MPSS-SR (Falsetti et al., 1993), BAI (Fydrich et al., 1992), BDI (Beck et al., 1988), and OQ-45.2 (Boswell et al., 2013)).
Functional MRI acquisition
We obtained MRI data with a standard 8-channel SENSE Head coil 3 Tesla Achieva scanner (Philips Healthcare, Best, The Netherlands). We first acquired T1-weighted images with a magnetization prepared rapid acquisition gradient-echo sequence: repetition time (TR) = 8.2 ms, echo time (TE) = 3.7 ms, field of view (FoV) = 250 mm, flip angle = 8°, 256 × 256 matrix, 180 slices/volume, slice thickness = 1 mm, no gap. We then acquired 5-min eyes open resting-state BOLD images (TR = 3000 ms, TE = 30 ms, FoV = 224 × 224 × 140 mm, flip angle = 70°, dynamic scans = 100, no gap).
Preprocessing
Rs-fcMRI analyses were performed using CONN Toolbox v21.a with the default preprocessing pipeline (Whitfield-Gabrieli and Nieto-Castanon, 2012). Functional data were first realigned and slice-timing corrected. We rejected outlier timepoints with the Artifact Removal Toolbox: scan-to-scan subject’s motion greater than 0.9 mm and BOLD signal changes above 5 standard deviations (Lumaca et al., 2019; Ramsay et al., 2023; Tung et al., 2021; Xu et al., 2023). No subjects were excluded based on excessive motion. Structural and functional data were then segmented into gray matter, white matter, and cerebrospinal fluid and no-linearly normalized to MNI space. The resulting volumes were parcellated using the 400 parcels local–global cortical atlas (Schaefer et al., 2018) implementing the 17 intrinsic networks variant as described by Yeo and colleagues (Yeo et al., 2011) labeled as follows: central visual (cVisN), peripheral visual (pVisN), somatomotor A and B, dorsal attention (DAN) A and B, salience (SN) A and B, limbic A and B, frontoparietal (FPN) A, B, and C, DMN A, B and C, as well as temporoparietal. Parcels were masked by individual subjects segmented gray matter to ensure spatial specificity. Functional data were resampled to 2 mm isotropic voxels and smoothed using an 8 mm full-width half-max Gaussian kernel. They were then denoised using linear regression of first-order covariates of confounding effect in the BOLD signal and dummy-coded outlier scans. Sources of noise in the BOLD signal were identified using the CompCor method (Behzadi et al., 2007) for white matter and cerebrospinal fluid contributions, as well as the six subject-motion parameters. Lastly, the signal was bandpassed filtered to 0.008–0.1 Hz.
Connectivity with ICA
To test for potential correlations between clinical symptoms and group-level intrinsic networks connectivity, we employed a data-driven approach using ICA (Calhoun et al., 2001) as implemented in CONN. We applied subject-level dimensionality reduction by retaining 64 components from a singular value decomposition characterizing each subject’s voxel-to-voxel correlation matrix. Then, we used the FastICA algorithm (Hyvärinen, 1999) with the G1/tanh nonlinear contrast function, followed by GICA3 backprojection, and kept the first 10 of the resulting group-ICA components. We calculated the Dice coefficient to quantify the spatial match to the 17-network parcellation for each component for labeling. For second-level analyses, we conducted linear regressions with the clinical scores and time since trauma in a general linear model framework while controlling for age. Statistical significance was determined using cluster-level inferences based on Gaussian Random Field theory with a voxel height threshold of p < 0.001 (uncorrected) and a cluster-level threshold of p < 0.05 (FDR corrected).
ROI-to-ROI connectivity
To test for potential correlations between clinical symptoms and the canonical 17 intrinsic networks (Yeo et al., 2011) and further explore subnetwork-level nodal implications, we computed ROI-to-ROI connectivity with the ROIs from the atlas by constructing spatial maps of Fisher-transformed Pearson correlation coefficients between the average BOLD timeseries of all 400 ROIs. We performed second-level analyses as described in the ICA section. We determined statistical significance using ROI-level inferences based on parametric multivariate statistics with a connection threshold of p < 0.01 (uncorrected) and a cluster-level threshold of p < 0.05 (FDR corrected) in an omnibus fashion (Nieto-Castanon, 2020). Of note, the ROI-to-ROI and ICA approaches differ in terms of how their spatial characteristics are developed. The ROI-to-ROI approach enables the results to be transposed into a public atlas of significance (Schaeffer’s atlas decimated into 400 parcels; Schaefer et al., 2018). The ICA approach is an intrinsically network-based measure driven by data specific to the sample under study. It allows for the mapping of intrinsic brain networks in an emergent manner specific to the group of participants.
Connectivity with graph theory
To test for potential correlations between clinical symptoms and the functional topological properties of the brain at both the network and nodal levels, we employed a graph theory approach. We computed the adjacency matrix for each participant by thresholding the individual ROI-to-ROI connectivity matrix using wiring cost (K). We extracted graph measures of degree, path length, clustering coefficient, local and global efficiency, as well as betweenness centrality (see Rubinov and Sporns, 2010, for a review) as implemented by CONN (Nieto-Castanon, 2020). We determined the cost threshold as the value of K that maximizes the small-world property of the network when compared with similarly sized random and lattice networks (Achard and Bullmore, 2007). Hence, we chose a cost threshold of K = 0.05 by virtue of its greatest joint difference in global efficiency against a lattice network and in local efficiency compared with a random network. Finally, we tested for correlations between the clinical scores and the resulting measures at both the ROI and network (average of all ROIs) levels while controlling for age and correcting the ROI-level graph measures for false discovery rate (Benjamini and Hochberg, 1995) as implemented in CONN. Given the use of cost for thresholding, we did not test for correlations between clinical scores and network-level degree.
We performed data analysis in MATLAB (version 2023b, MathWorks Inc.).
Results
Clinical assessment
The mean (s.d.) clinical scores were as follows: MPSS-SR = 74.70 (19.82), BDI = 26.43 (10.51), BAI = 24.57 (13.48), OQ-45.2 = 96.32 (23.67). The average (s.d.) time since trauma was 139.62 (82.62) months. Bivariate correlation statistics between these variables, as well as age, indicate that clinical scores are strongly correlated together (0.662 ≤ r ≤ 0.844) and that age and time since trauma are moderately correlated (r = 0.427; Supplementary Fig. S1).
Associations between clinical measures and ICA components
All clusters of significant association between clinical scores and connectivity with ICA components are shown in Table 2, and the ICA parcellations are illustrated in Supplementary Figure S2. Results from Table 2 are summarized in Supplementary Figure S3.
Statistically Significant Associations Between Clinical Scores and ICA Components
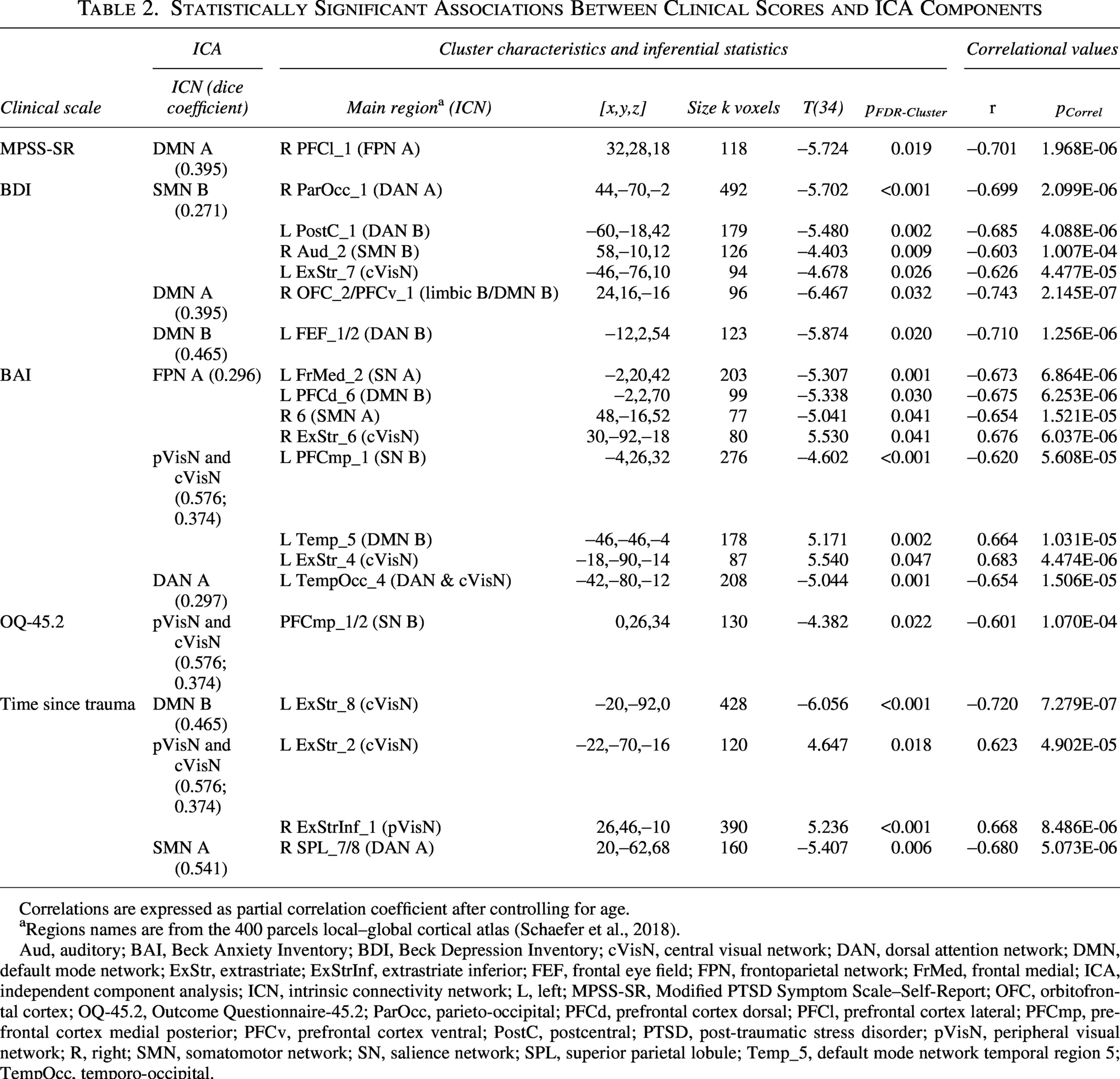
Correlations are expressed as partial correlation coefficient after controlling for age.
Regions names are from the 400 parcels local–global cortical atlas (Schaefer et al., 2018).
Aud, auditory; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; cVisN, central visual network; DAN, dorsal attention network; DMN, default mode network; ExStr, extrastriate; ExStrInf, extrastriate inferior; FEF, frontal eye field; FPN, frontoparietal network; FrMed, frontal medial; ICA, independent component analysis; ICN, intrinsic connectivity network; L, left; MPSS-SR, Modified PTSD Symptom Scale–Self-Report; OFC, orbitofrontal cortex; OQ-45.2, Outcome Questionnaire-45.2; ParOcc, parieto-occipital; PFCd, prefrontal cortex dorsal; PFCl, prefrontal cortex lateral; PFCmp, prefrontal cortex medial posterior; PFCv, prefrontal cortex ventral; PostC, postcentral; PTSD, post-traumatic stress disorder; pVisN, peripheral visual network; R, right; SMN, somatomotor network; SN, salience network; SPL, superior parietal lobule; Temp_5, default mode network temporal region 5; TempOcc, temporo-occipital.
Associations between PTSD symptoms and ICA components
Higher MPSS-SR scores, indicating greater severity of PTSD symptoms, were associated with lower connectivity between the DMN A (2nd ICA component) and the right FPN A (PFCl_1 area), corresponding to a region of the right MFG (Fig. 1).
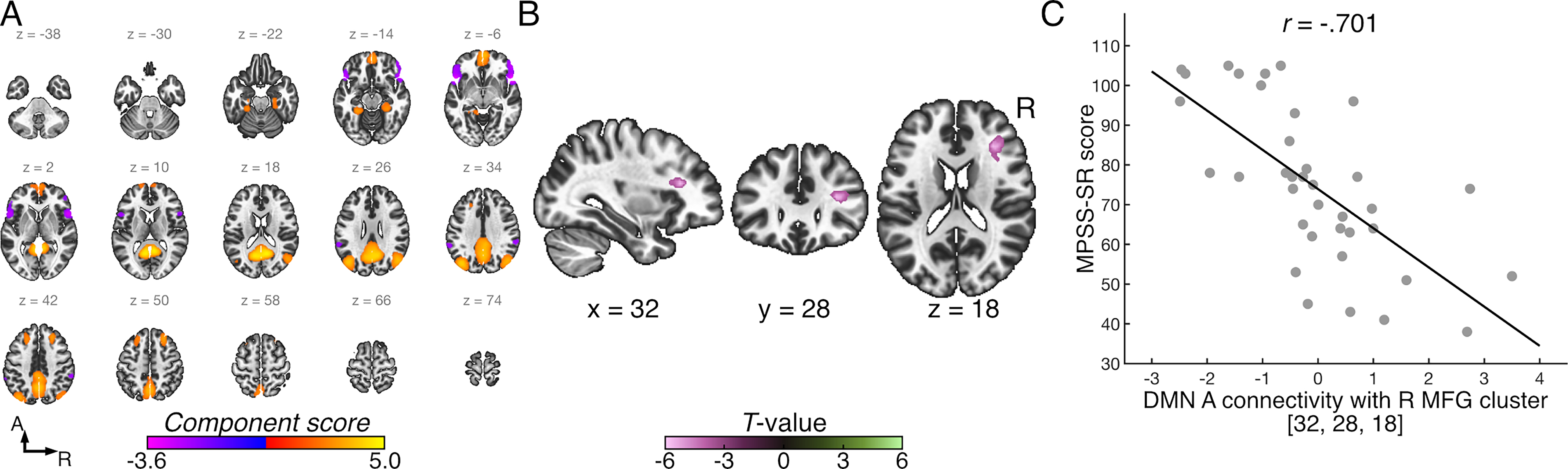
Significant associations between MPSS-SR scores and intrinsic network connectivity.
Associations between depressive symptoms and ICA components
Higher BDI scores, indicating greater severity of depressive symptoms, were associated with lower connectivity between the somatomotor B (1st ICA component) and the right DAN A (ParOcc_1), left DAN B (PostC_1), right somatomotor B (Aud_2), and left cVisN (ExStr_7) areas. Higher BDI scores were also related to lower connectivity between the DMN A and a cluster shared between the right limbic B (OFC_2) and right DMN B (PFCv_1). Finally, higher BDI scores were associated with lower connectivity between the DMN B (4th ICA component) and the left DAN B (FEF_1/2).
Associations between anxiety symptoms and ICA components
Higher BAI scores, indicating greater severity of anxiety symptoms, were related to lower connectivity between the FPN A (5th ICA component) and the left SN A (FrMed_2), the left DMN B (PFCd_6), and the right somatomotor A (precentral area 6), as well as higher connectivity with the right cVisN (ExStr_6). Higher BAI scores were also associated with lower connectivity between the pVisN & cVisN (7th ICA component) and the left SN B (PFCmp_1), as well as higher connectivity with the DMN B (left Temp_5) and left cVisN (ExStr_4). Finally, higher BAI scores were associated with lower connectivity between the DAN A (8th ICA component) and a cluster extending between the DAN A and cVisN, centered on the left TempOcc_4 area.
Associations between quality of life and ICA components
Greater OQ-45.2 scores, indicating poorer quality of life, were associated with lower connectivity between the pVisN & cVisN (7th ICA component) and the SN B (PFCmp_1/2).
Associations between time since trauma and ICA components
Greater time since trauma (in months) was associated with lower connectivity between the DMN B (4th ICA component) and the left cVisN (ExStr_8), as well as between the somatomotor A (10th ICA component) and the right DAN A (SPL_7/8). Greater time since trauma was also associated with higher connectivity between the pVisN & cVisN (7th ICA component) and the left cVisN (ExStr_2) and right pVisN (ExStrInf_1).
Associations between clinical scores and ROI-to-ROI connectivity
Quality of life was associated with connectivity in a network cluster anchored in the left ventral prefrontal cortex (DMN B; PFCv_1/3/4/5) and connecting the bilateral SPL (DAN A; left SPL_4/5/6/7 and right SPL_2/4). Poorer quality of life was associated with higher connectivity with the right SPL and lower connectivity with the left SPL. ROI-level correlations are detailed in Table 3 and shown in Supplementary Figures S4 and S5. There were no significant associations for the MPSS-SR, BDI, BAI scores, or time since trauma.
Association Between OQ 45.2 Score and ROI-to-ROI Connectivity

Correlations are expressed as partial correlation coefficient after controlling for age.
L, left; OQ-45.2, Outcome Questionnaire-45.2; PFCv, prefrontal cortex ventral; R, right, ROI, region of interest; SPL, superior parietal lobule.
Associations between clinical measures and graph theory metrics
Greater MPSS-SR scores were associated with higher nodal clustering coefficient of the left FPN B (IPL_2; Fig. 2A). Greater BAI scores were associated with higher nodal path length in the left FPN A (Cingm_1), the right cVisN (ExStr_9), and the left DMN B (pCunPCC_5); Figure 2B–D). There were no significant associations between BDI score, OQ-45.2 score, or time since trauma with nodal graph theory metrics or between the clinical variables and the network-level graph theory metrics.
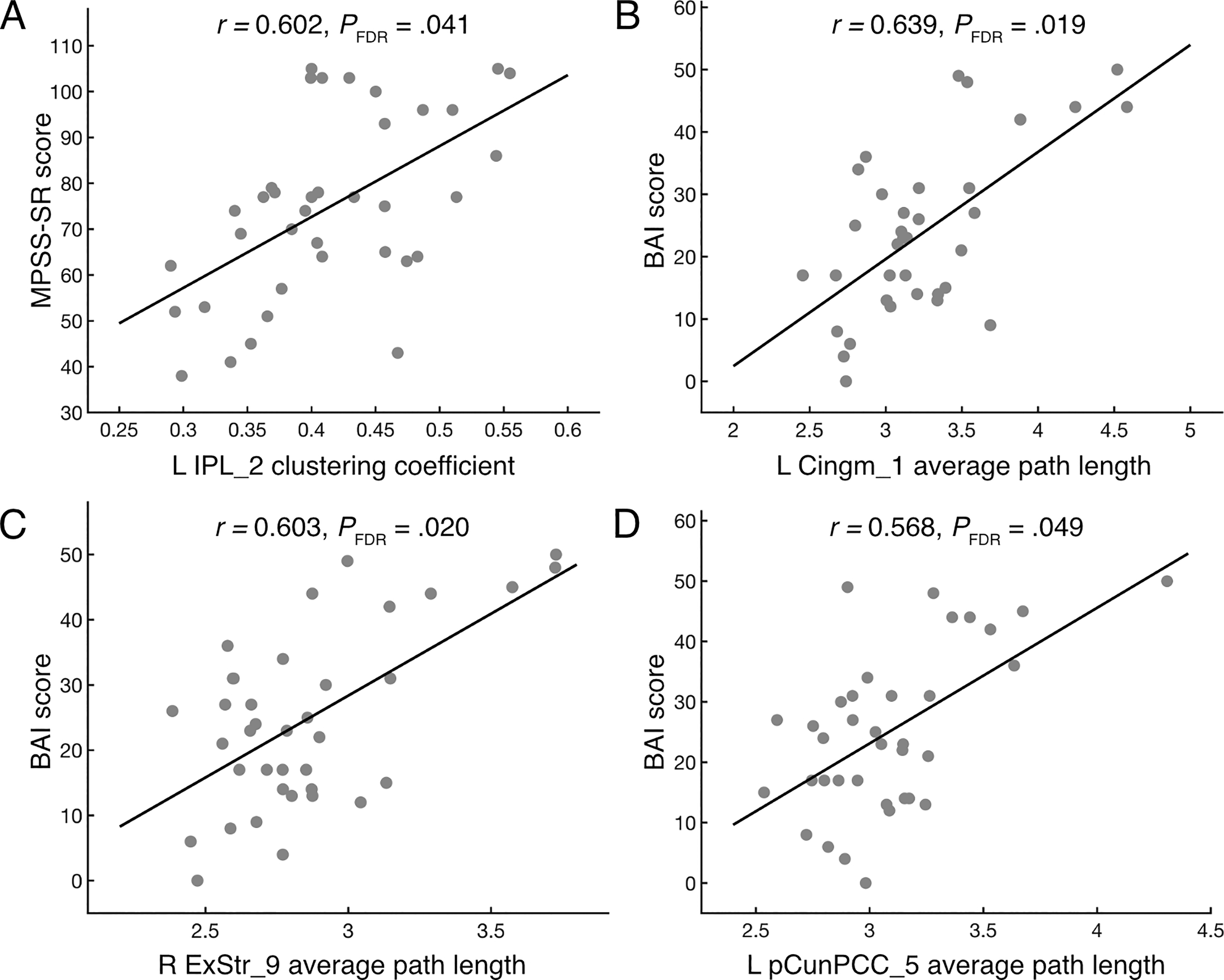
Scatter plots showing significant associations between graph theory metrics and
Discussion
This study investigated the association between clinical symptoms and functional connectivity with resting-state fMRI in military personnel with adulthood-onset war-related PTSD. Overall, greater symptom severity, longer time since trauma, and poorer quality of life were related to patterns of lower connectivity, particularly involving the DMN. The only clinical measures linked to higher connectivity patterns, which were exclusively observed in the visual networks, were greater anxiety and longer time since trauma.
We found that greater severity of PTSD symptoms is linked to lower connectivity between the DMN and FPN (MFG), as well as higher clustering coefficient of the FPN (IPL). This supports prior work observing that PTSD severity negatively correlated with lower connectivity between the DMN and the MFG (Olson et al., 2019). Interestingly, alleviation of PTSD symptoms after mindfulness-based exposure therapy has been related to increased DMN-FPN connectivity (King et al., 2016), further suggesting that this connectivity may constitute a therapeutic target. Also, patients with PTSD display higher clustering coefficient at the network and subnetwork levels, as compared with healthy controls (Akiki et al., 2018; Lei et al., 2015; Suo et al., 2015; Zhu et al., 2019), whereas adults with partial PTSD show lower clustering coefficient (Jung et al., 2016). Altogether, these studies and our findings support that greater PTSD symptom severity reflects greater segregation of the DMN (Akiki et al., 2018). Furthermore, higher whole-network clustering coefficient correlated with lower sustained attention in patients with PTSD (Zhu et al., 2019). Higher clustering coefficient of the IPL, a region involved in attentional processing (Clower et al., 2001), might thus contribute to attentional deficits or hypervigilance in PTSD (Ely et al., 2023; Punski-Hoogervorst et al., 2023; Vasterling et al., 1998). Overall, the DMN-FPN hypoconnectivity and FPN functional topology, correlating with PTSD symptom severity, might represent therapeutic candidates to target with neuromodulatory interventions. Given the observed DMN-FPN hypoconnectivity and higher IPL clustering, mainly in the right hemisphere, the use of neuromodulation targeting the right DLPFC, MFG, and/or IPL to modulate these metrics may lead to clinical benefits. These targets should also indicate the choice of neuromodulatory approaches. For instance, if multiple brain regions should be targeted, rTMS with a multilocus coil (e.g., Sinisalo et al., 2025) or transcranial current stimulation with a multiple electrodes montage (e.g., Weise et al., 2025) could be used. If deeper brain regions should be targeted, transcranial ultrasound stimulation (e.g., Tsunoda et al., 2026) or temporal interference (e.g., Weise et al., 2025) could be used. Such network-guided targeting approaches will contribute to personalizing target engagement associated with symptom severity with precision.
We observed that greater severity of depressive symptoms in military personnel with PTSD is related to lower connectivity in mostly somatosensory, default mode, and attentional networks. This is in line with previous work reporting that patients with depression displayed lower connectivity between the somatomotor and both the DAN and visual network, as compared with healthy controls (Hu et al., 2024; Yan et al., 2019). It has also been suggested that lower somatomotor-DAN/visual network connectivity is related to affective alterations and attentional biases observed in PTSD and depression (Martino and Magioncalda, 2024). We also found that greater depressive symptom severity is related to lower within-somatomotor connectivity, which aligns with previous findings in depression (Yan et al., 2019). Our results also suggest that greater depressive symptoms are related to lower DMN-DAN connectivity, which is in line with findings of lower DMN-DAN connectivity in patients with PTSD and/or depression (Siddiqi et al., 2023; Tse et al., 2024). Finally, greater overgeneralization of autobiographical memory in patients with depression has been linked to lower within-DMN connectivity (Zhu et al., 2012). Thus, our finding indicating that more severe depression is related to lower within-DMN connectivity might reflect trauma-related memory in PTSD, as suggested previously (Brewin and Vasterling, 2021).
Our findings indicate that greater severity of anxiety symptoms in military personnel with PTSD is related to patterns of lower, as well as higher connectivity. Lower connectivity involved the FPN-SN, FPN-DMN, FPN-somatomotor, visual-SN, and DAN-DAN/cVisN networks. Lower connectivity involving these networks has been observed in various clinical populations with anxiety symptoms, including generalized anxiety disorder (Kolesar et al., 2019), panic disorder (Pannekoek et al., 2013), social anxiety disorder (Zhang et al., 2023), as well as in patients with transdiagnostic anxiety (Xu et al., 2019). The observed higher connectivity related to greater anxiety in our patients with PTSD implicated the FPN-visual, the visual-DMN, and the within-visual networks. Similar higher connectivity has been reported in patients with social anxiety disorder (Ergül et al., 2019), in healthy individuals with high test anxiety (Hou et al., 2022), as well as in healthy individuals during emotional reappraisal (Sripada et al., 2014). Thus, higher connectivity within these networks may reflect anxiety-related hypervigilance and intrusive phenomena and/or a compensatory attempt to reappraise emotions in patients with PTSD and severe anxiety (Abdallah et al., 2017; Akiki et al., 2017). Finally, we found that greater anxiety severity was linked to longer nodal average path length in regions of the left FPN (midcingulate), the DMN (posterior cingulate/precuneus), and the right cVisN (lateral occipital cortex). Lower integration of a network encompassing the midcingulate gyrus was previously linked to harm avoidance in healthy individuals (Markett et al., 2016) and similarly observed in the posterior cingulate cortex of patients with social anxiety disorder (Zhu et al., 2017). Some evidence implicates the lateral occipital cortex in anxiety (Wang et al., 2018), but we are not aware of previous work in anxiety reporting altered functional topology of this region.
Poorer quality of life in our patients with PTSD was related to lower visual-SN connectivity, lower connectivity between the left ventrolateral prefrontal DMN and the left-sided parietal DAN, but higher connectivity between the left ventrolateral prefrontal DMN and the right-sided parietal DAN. The lower visual-SN connectivity observed for quality of life was similar to the one we found for anxiety involving the anterior midcingulate cortex, which may be related to the correlation between quality of life and anxiety in our patients. Interestingly, the observed lower left DMN-left DAN connectivity and higher left DMN-right DAN connectivity echoes prior work linking anger-aggression to asymmetrical connectivity within a principal component encompassing elements of the DAN, FPN, and DMN (Weathersby et al., 2019). This association is thought to rely on variations in emotional regulation abilities partly mediated by the ventrolateral/orbitofrontal cortex (Davidson et al., 2000), which is relevant for PTSD (Liberzon and Abelson, 2016). This also supports previous findings of increased DMN-DAN connectivity (vmPFC and right SPL) in veterans with PTSD compared with trauma‐exposed veterans without PTSD (Sheynin et al., 2020). Connectivity lateralization in PTSD might warrant examination, especially considering that clinical benefits from neuromodulation in this clinical population may vary on the targeted hemisphere (Boggio et al., 2010; Harris and Reece, 2021).
Longer time since the traumatic war event in our military personnel with PTSD was related to lower DMN-visual networks and somatomotor-DAN connectivity, as well as higher connectivity within the visual networks. As we observed that weaker somatomotor-DAN connectivity and stronger connectivity within the visual networks were associated with greater depressive and anxiety symptoms, respectively, this indicates a decrease in the contribution of these mechanisms in maintaining these symptoms over time since the trauma. From a therapeutic perspective, this suggests that the efficacy of circuit-based interventions likely differs depending on trauma recency. To our knowledge, no study has yet tested for potential correlations between time since trauma and whole-brain connectivity in PTSD, and as such, the variation in clinical relevance of circuits over time remains largely unknown. Future longitudinal studies are needed to capture how brain connectivity evolves across the fluctuating course of PTSD. Interestingly, we previously found that longer time since trauma correlated with greater gray matter volume in subregions of the occipital visual networks (Roy et al., 2022). Taken together, time since trauma might impact the structured and functional integration of visuo-attentional network. This indicates that brain circuits vary over time, highlighting the need for adapting brain therapeutic targets according to patients’ clinical profile.
This study has noteworthy limitations. Our ultimate goal is to identify the brain networks that are associated with symptom severity to develop a circuit-based neuromodulation intervention in military personnel with PTSD who have been refractory to psychotherapy and pharmacotherapy. Thus, our results may not be generalizable to civilian PTSD, early PTSD onset, or female military personnel, given our male-dominant sample (N = 34/37). Our participants displayed severe PTSD (33 out of 37 patients), which might have constrained the correlational analyses. Also, their clinical scores correlated together, which is expected given that PTSD symptoms overlap with depression (Gros et al., 2012,2010) and other anxiety disorders (Przeworski and Dunbeck, 2016), but our results should then be interpreted with caution due to multicollinearity. We also assessed symptoms with self-reported standardized questionnaires, not with semistructured interviews, which can be considered as a limitation. Furthermore, most patients were treated with medication. We cannot rule out that medications influenced our connectivity measures. We are not aware of studies in patients who were refractory to pharmacotherapy and asked to withdraw from medication in order to conduct a resting-state fMRI study. Future investigations should focus on connectivity correlates of patients with PTSD according to their comorbidity profile and medication blood levels. Finally, a 5-min resting-state fMRI acquisition appears sufficient to quantify the emergence of ICNs with group-ICA (Duda et al., 2023), but such short acquisition may have reduced the reliability of our edge-level connectivity estimates (Noble et al., 2019). Accordingly, our ROI-to-ROI results warrant replication using lengthier acquisitions. We partially mitigated this limitation during graph formation by retaining the 5% strongest edges in the adjacency matrix, which likely increased the stability of derived graph metrics.
Conclusion
In sum, this study delineates associations between clinical features of adulthood-onset war-related PTSD and patterns of functional connectivity in military personnel. Among those patterns, low DMN-FPN connectivity may be a potential target to explore for neuromodulatory interventions.
Authors’ Contributions
O.R.: Formal analysis, visualization, writing—original draft, and writing—review and editing. J.L.-.M.: Investigation, methodology, and writing—review and editing. E.R.: Methodology and writing—review and editing. M.M.: Investigation, methodology, and writing—review and editing. L.J.H.: Writing—review and editing. J.-.M.B.: Writing—review and editing. M.B.: Conceptualization, funding acquisition, investigation, methodology, resources, and writing—review and editing. S.F.: Conceptualization, funding acquisition, investigation, methodology, project administration, resources, supervision, and writing—review and editing.
Footnotes
Data Availability
Data will be made available on request.
Acknowledgments
The authors would like to express their highest gratitude for the significant contribution of Jean Leblond to this work. They also thank the military personnel for their participation, Julie Goulet-Kennedy for her help with data collection, and Sylvie Rivard for her administrative help.
Funding Information
This work was supported by the
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.