
Abstract
Reciprocity, a core component of social capital, is rarely theorized or measured leaving the relationship between reciprocity and health ambiguous. Historically, reciprocity measures have not been used in the context they were designed causing measurement error. This multi-phased study was designed to develop and validate a reciprocity measure for formal and informal groups within communities and congregations as part of a more comprehensive social capital measure. In-depth interviews (n = 72), cognitive interviews (n = 40), and an expert review panel guided item development and selection for content validity. South Carolina residents (n = 500) completed the 10-item Reciprocity of Social Support (RSS) Scale during 2008-2010. Construct validity was supported through an exploratory factor analysis (EFA) that confirmed a two-factor model for the scale for community- and congregation-based groups. Cronbach’s α values indicated items were highly correlated for community groups and church groups. Psychometric analyses of the RSS Scale support convergent and divergent validity for the community- and congregation-based groups. Mean RSS Scale scores were not statistically different between community- and congregation-based groups. This scale has proven psychometric properties for utilization in future research investigating reciprocity of social support in community- and congregation-based groups and will be useful to examine whether reciprocity (by context and type of group) is associated with physical and/or mental health.
Keywords
Social capital has been defined as connections among individuals’ social networks, including group membership, characterized by trust between individuals and norms of reciprocity that facilitates collective action and cooperation for mutual benefit (Kawachi, Kennedy, & Glass, 1999; Putnam, 2000; Putnam, Leonardi, & Nanetti, 1993). Social capital is an established health determinant, independent of other social and behavioral determinants (Giordano, Ohlsson, & Lindström, 2011), and its dimensions at the individual and community levels are associated with individual and population health (Kawachi, Kennedy, Lochner, & Prothrow-Stith, 1997; Moore, Haines, Hawe, & Shiell, 2006; Viswanath, Randolph-Steele, & Finnegan, 2006; Yip et al., 2007). However, questions still surround the relevance of social capital for health outcomes, and researchers are seeking measures within specific social contexts to investigate its effects (Giordano et al., 2011).
To clarify the associations between social capital and health, a critical step is to differentiate between structural social capital and cognitive social capital (Harpham, 2008; Hurtado, Kawachi, & Sudarsky, 2011). Structural social capital refers to behaviors (e.g., participation in associations) that facilitate access and influence networks providing social support or other potentially beneficial resources (Harpham, 2008; Hurtado et al., 2011). Cognitive social capital (e.g., trust and reciprocity) refers to values, perceptions, and expectations regarding social behaviors that provide a sense of community belonging and safe and stable representation of reality (Harpham, 2008; Hurtado et al., 2011). In other words, structural social capital refers to what people do (e.g., participation in associations and networks), and cognitive social capital refers to what people think (e.g., values and perceptions) that influences individuals’ behaviors toward mutually beneficial collective action (Harpham, 2008; Krishna & Uphoff, 2002) and is therefore likely to precede the actions included in structural social capital. For the purposes of this article, reciprocity will be examined through the lens of cognitive social capital, that is, what people value or believe they or others in their network would do under certain circumstances.
Reciprocity has long been of theoretical interest in the social sciences. In Alvin Goulder’s (1960) seminal publication, he provided a theoretical explanation of reciprocity and clarified the concept as patterns of returning or responding to benefits received. He described reciprocity as “moral cement” that stabilizes social relationships by creating a sense of obligations to one another (Goulder, 1960). Harpham (2008) explained that reciprocity as a two-way behavioral relationship: when someone has helped someone there is an expectation that the favor will be returned when needed. Stone (2001) emphasized reciprocity as a core construct of social capital because it is an indicator of the quality of social relationships that impacts people’s abilities to solve common problems (Stewart-Weeks & Richardson, 1998).
Social Capital in Faith Groups and Community Groups
Social capital depends on context at individual and group levels (Kawachi & Berkman, 2000). Tangible and intangible resources are a function of specific social connections (Cattell, 2001). Community participation, through formal and informal groups, is thought to produce more social capital (Putnam, 2000) because it facilitates access to resources (Hurtado et al., 2011) and provides individuals with a sense that they can solve their problems through collective action (Hawe, 1994; Zakus & Lysack, 1998).
Putnam (2000) suggests that faith communities may be the single most important source of social capital in the United States. Faith communities commonly contribute to social services and community cohesion through social capital (Dinham, Furbey, & Lowndes, 2009). In the United States, Christianity, Judaism, and Islam all have commitments to peace, justice, honesty, service, personal responsibility, forgiveness, respect, and obligation to others that can contribute to the development of trusting relationships (Furbey, Dinham, Farnell, Finneron, & Wilkinson, 2006). Thus far, no studies have examined whether faith groups also contribute to reciprocity in relationships.
Wald and Calhoun-Brown (2007) estimated that between three fifths to three fourths of the American adult population were members of a Christian church. In 2009, 41.6% of Americans reported attending church at least once a week or almost every week (Newport, 2010). Church attendance levels varied across U.S. regions, with the highest levels in the South and Midwest (45%-63%; Newport, 2010). Furthermore, according to the Corporation for National and Community Service (CNCS, 2006), U.S. adults have been more likely to volunteer through religious organizations compared with civic, educational, political, professional, hospital, or recreational organizations with proportions volunteering varying by age from 36.5% among 45- to 54–year-olds to 45.5% among those 65 years and older. No other type of organization has comparable levels of involvement (CNCS, 2006). This high level of volunteerism helps account for the role of faith communities in fostering social capital.
Measuring Reciprocity
Reciprocity is a core part of cognitive social capital (Abbott & Freeth, 2008; Stone, 2001), and there is evidence that reciprocity of social support may impact health outcomes. For instance, a study by Moskowitz, Morris, and Schmidt (2010) examined reciprocity of social support in a low-income population and found a balanced proportion of giving and receiving may buffer the effect of stressors more than the absolute amount of received support.
However, in most social capital studies, scholars rarely or inadequately theorized or measured reciprocity (Abbott & Freeth, 2008; O’Brien, Burdsal, & Molgaard, 2004; Stone, 2001), leaving the relationship between reciprocity and health ambiguous (Abbott & Freeth, 2008). This may be in large part because social capital constructs are multi-dimensional, not entirely distinct from one another, and the same questions are often used to measure different constructs, particularly among the constructs of trust and reciprocity (Blaxter, 2004). The reciprocity measures that do exist are often used out of contexts for which they were designed (Abbott & Freeth, 2008). As a result, measures are often worded with underlying assumptions about relationships (e.g., “friends” and “neighbor”), which may not be meaningful to respondents, (Abbott, 2009; Harpham, 2008) if the terms are not further defined for the respondent. Common reciprocity measures that use the terms neighbors and friends include “Have you assisted neighbors or friends? Have your neighbors or friends assisted you?” (Ziersch, Baum, MacDougall, & Putland, 2005). In relation to the term friends, respondents may have various meanings ranging from friends that receive greeting cards to those called on during difficult times (Abbott, 2009). Therefore, inferences regarding the respondents’ relationship to his or her “friends” remain unclear, and may have varied impacts on health (Abbott, 2009). Common reciprocity measures that use the term neighbor or neighborhood include the ones mentioned previously, as well as “In my neighborhood, most people are willing to help others” (Pollack & von dem Knesebeck, 2004). The term neighbors can also be confusing to respondents because respondents may define neighbor differently (e.g., a neighbor who lives on the respondents’ street compared with a neighbor who lives in the respondents’ community). Such general terms (i.e., friends, neighbors, and neighborhoods) may be imprecise indicators of particularized social capital, that is social capital that occurs within specific groups of people; therefore, such general terms may not accurately depict the respondent’s relationship in a particular context. To address these contextual measurement issues, Dudwick, Kuehnast, Nyhan Jones, and Woolcock (2006) recommend that field researchers have a thorough understanding of the context in which the measures are developed, so the measures for different groups are relevant and understandable to the local population being studied. For example, researchers may rely on local cultural or ethnic idioms that more clearly convey the intended relationship to the respondent.
Other common measures for reciprocity solicit level of agreement with generalized statements such as “Most people try to be helpful” in the General Social Survey (Kawachi et al., 1999) or “People are helpful” and “People look after themselves” from the World Values Survey (Inglehart, Basáñez, Díez-Medrano, Halman, & Luijkx, 2004). Such generalized questions, though simple, do not capture the complexities of social relationships (Abbott, 2009) or the social context (Abbott & Freeth, 2008; Stone, 2001). Some social capital literature presents measures that conflate reciprocity and trust measures, even though they are two separate constructs. Letki and Evans (2005) use both in an effort to measure trust in a single scale. Newton (1997) advised that failure to conceptualize separate dimensions of social capital will confuse our understanding of how these dimensions empirically operate.
Furthermore, many studies have examined social capital based on outcomes (i.e., volunteerism and political participation), but do not examine mechanisms of social capital (Calhoun-Brown, 2005), such as reciprocity among community members, including faith communities. During a broad-based consultative workshop (Dinham & Shaw, 2012), reciprocity was identified as a valued aspect of faith communities by congregation-based groups. Members of congregation-based groups said that reciprocity should be measured to demonstrate contributions for faith communities and to assess the level of support generated within faith communities. However, few quantitative measures capture reciprocity in the context of communities, and no measures exist to assess reciprocity in the context of faith communities (Dinham & Shaw, 2012). Thus, these lack of reciprocity measures leave the relationship of reciprocity and health unknown in particular contexts; therefore, it is necessary to develop and refine measures of reciprocity in specific community settings using qualitative data (Dudwick et al., 2006), which will help determine whether different types of groups (i.e., community-based groups and congregation-based groups) differentially affect health outcomes (Morgan & Swann, 2004).
The purpose of this study was to develop and validate a measure of reciprocity for formal and informal groups within specific contexts (community and congregation) to determine whether levels of reciprocity differ by context. A scale that measures reciprocity will allow future studies to examine whether reciprocity (by context and type of groups) is associated with physical and/or mental health.
Method
Study Design
A multiphase study was conducted using scale development methods outlined by DeVellis (2003). The reciprocity scale development was part of a larger project to develop and test the Relationships in Community Groups (RCG) questionnaire, a multi-dimensional measure of social capital. The overview of study phases for the construction of the Reciprocity of Social Support (RSS) Scale is outlined in Table 1.
Overview of Study Phases for Construction of the Reciprocity of Social Support Scale.

Note. RSS = Reciprocity of Social Support; RCG = Relationships in Community Groups; LSNS-6 = Lubben Social Network Scale–6.
In Phase I, perceptions of norms of reciprocity in community- and congregation-based groups were assessed using in-depth interviews to support content validity. In Phase II, the qualitative data from Phase I were used to generate items and response categories, which were subsequently reviewed by an expert panel for content validity. In Phase III, the items and response categories were evaluated using cognitive interviews, which led to revisions of the items and response categories, further assessing content validity. In Phase IV, a variety of psychometric methods were utilized to evaluate reliability and validity of the scale, which included the assessments of construct validity (i.e., convergent and divergent validity). Mean comparisons were also performed for community- and congregation-based groups. These methods and results for each study phase are described in subsequent sections.
The study protocol was approved by the University of South Carolina’s Institutional Review Board. Written informed consent was obtained for all participants in Phase I and Phase IV. Oral consent was obtained from participants in Phase III. The development of the RSS Scale was part of a study that developed a more comprehensive multi-dimensional measure of social capital for community- and congregation-based groups. Participants in Phase I and III received US$20 for their time in the study (between 40 and 90 min) and participants in Phase IV received US$10 for their time in the study (between 20 and 60 min). The limitation to Christians was solely for the qualitative portion of the survey development: the structure and language of the scale reflected those of Christian faith because of the initial setting of preliminary work.
Study Setting
The setting for study phases was in South Carolina. In effort to include participants with varied racial, educational, and income levels, participants were recruited from eight counties across the state.
Phase I: Conceptual Framework and Qualitative Methods
The methods in which the reciprocity of social support items was developed contributed to content validity. Phase I was guided by a conceptual framework (see Figure 1). Trust has been shown to be inversely associated with common mental illnesses (De Silva, McKenzie, Harpham, & Huttly, 2005). Therefore, it would not be surprising for people with mental illness to score low on individual social capital scales (i.e., trust and/or reciprocity scales; De Silva et al., 2005). As Figure 1 illustrates, high levels of trust often lead to formal and informal group participation, and high levels of social participation often result in increased trust between group members (Lindström, 2004), although limitations of physical health may reduce social participation (Yong, 2012). The research team theorized that as members experience interpersonal trust with group members, they may also experience reciprocity of social support and a sense of belonging to the group that leads to future experiences of trust, reciprocity of social support, and a continued sense of belonging experienced between group members. Furthermore, individuals may experience enhanced positive mental health outcomes and have downstream effects of protective and improved physical health outcomes.

Conceptual framework linking trust, reciprocity of social support, and sense of belonging with physical and mental health.
From the theoretical framework, investigators developed an in-depth interview guide using open-ended questions to elucidate participants’ values, perceptions, attitudes, and opinions regarding social capital constructs, including reciprocity between group members (Krishna & Shrader, 1999). Interview items included (a) study participants’ group participation in the past year; (b) identification of the one group that was most important to them; (c) for the identified group, participants commented on the other group members’ interest in helping others (Krishna & Shrader, 1999), which investigated the cultural norm and values held about reciprocity within the group (Stone, 2001); and (d) the benefits received from the connections within the groups, which informed whether participation in social networks was due to a norm of reciprocity (e.g., act out of obligation or for the common good), which are indicators of quality of the social networks (Stone, 2001).
Phase I: In-Depth Interviews
Prior to the current project, several of the authors implemented a congregation-based holistic health intervention aimed at older adults meeting in small, interracial groups. Named Heart, Soul, Mind, and Strength (HSMS), groups met weekly for 2 hr over a 1-year period. Participants from that program were included in Phase I of the study because investigators thought there may be additional mechanisms related to social capital that resulted in broader health benefits.
In 2008, in-depth interviews were conducted (n = 72). Phase I inclusion criteria for participants were African American and White adults (ages 50 and above) who were residents of South Carolina. Phase I study groups were defined by three levels of religious participation: (a) HSMS participants (n = 24), (b) regular attendees of religious services who were not HSMS participants (i.e., attended religious services at least once a month; n = 24), and (c) infrequent/non-attendees of religious services (i.e., did not attend religious services more than twice a year; n = 24), each level stratified by race—African American and White—for a total of six study groups of n = 12 each. The HSMS participants were randomly selected to participate in the in-depth interviews. Regular attendees of religious services and infrequent/non-attendees of religious services were selected using a snowball sampling method from eight counties in South Carolina.
All interviews were audio recorded, transcribed, and researchers provided hand-written notes for each interview. Interviews were coded using QSR NVIVO7 software (QSR International, Burlington, Massachusetts, United States). Each transcript was independently reviewed and analyzed by two researchers (H.C.P. and M.C.M.) using an open coding process (Strauss & Corbin, 1990). Themes were identified across the six study groups based on supporting comments from at least two participants. Coders met on a frequent basis to discuss and compare the themes they identified independently and discussed coding issues until agreement was reached. The codebook contained a list of defined codes.
Phase I: Results
Seventy-six percent (n = 55) of the participants were women. All participants were 50 years or older (M = 66 years, SD = 10.90). Table 2 highlights Phase I participant demographic characteristics. Thematic analysis identified the types of groups to which participants belonged (i.e., community- and/or congregation-based groups); the most important groups in which they participated (i.e., community- and/or congregation-based groups); their group’s interest in helping others, whether within and/or outside their group; and reported benefits of group participation, usually described in terms of the social support participants provided and/or received in their group. Comments reflected the types of social support experienced: tangible, emotional, informational, positive social interaction, and spiritual (Krause, 2002; Sherbourne & Stewart, 1991).
Participants’ Socio-Demographic Information for Study Phases I and IV.

Note. HS = high school.
Age (Phase I)—Missing data (n = 6)
Race (Phase IV) —Missing data (n = 1)
Due to rounding, percentage total may not equal 100
Education (Phase I)—Missing data (n = 1)
Education (Phase IV)—Missing data (n = 1)
Marital Status (Phase I)—Missing data (n = 1)
Phase II: Item Development
The social capital literature and results of the thematic analysis guided the development of a large pool of items and served to support content validity of the measure. During the second study phase, investigators developed 63 items to measure reciprocity of social support. An expert review panel with relevant expertise in medicine, social work, social determinants of health, epidemiology, and health promotion, played an integral role by helping to guide the development of the questionnaire. The panel met twice a month for approximately 6 months to determine which questions to include in the social capital measures. Item inclusion was based on items that were theoretically congruent with the reciprocal nature of social support provided and received in a group setting, consistent with the literature or qualitative findings, and structurally appropriate (i.e., concise, not double barreled, without multiple negatives; DeVellis, 2003).
Phase II: Item Selection
The reciprocity scale development was part of a larger project to develop and test a comprehensive measure of social capital for community groups. Therefore, to reduce participant burden in this study and in future studies, 10 items were selected from the item pool based on the relevance to the study population from the original 63 items. Five items were selected to measure the likelihood the participant would provide social support to group members, and 5 items were selected to measure the likelihood the participant would receive social support from group members.
Items were informed primarily by the work of Sherbourne and Stewart (1991). The item on emotional support, that is, positive feeling from experience with group members was derived from participant comments about helping others or being helped during times of personal and emotional difficulties, producing the phrase following the stem “to get through a difficult time emotionally.” Positive social interaction, defined as the availability of sharing enjoyed activities, was reflected in the item “to do something enjoyable with.” Informational support, offering or receiving advice, information, guidance, or feedback, was assessed by the item “to share (your/their) experiences and knowledge.” Spiritual support (Krause, 2002), characterized as support in the realm of faith beliefs, was based on participant comments about feeling supported on their faith journey, finding spiritual guidance, and most frequently providing and receiving prayers, which led to the item, “to provide spiritual support, that is, pray for (you/them).” Sherbourne and Stewart (1991) define tangible support as provision of material aid and behavioral assistance. Participants commented on assisting others and/or being assisted usually during an illness, which led to the item “to take a meal if (they/you) were sick.”
Phase III: Cognitive Interviews
The items and question formats for the social capital measures, including the RSS Scale items, were examined using cognitive interviews (n = 40) to support content validity. Cognitive interview participants’ demographic characteristics were similar to participants who completed the survey in Phase IV (see Table 2). Participants were asked to discuss their reactions to the 10 reciprocity items to identify issues related to order, comprehension, wording, clarity, and response categories (Willis, 2005). Field researchers (HP and MM) and expert review panel iteratively reviewed field notes and made subsequent changes to the scale based on participant feedback.
Phase III: Results
The cognitive interviews led to modifications to the page format, directions, item wording, and response categories. The sample size was expanded until no new instrumentation issues emerged; ultimately, cognitive interviews were used to examine nine versions of the RSS Scale. See Table 3 for the final RSS Scale items.
Reciprocity of Social Support Scale items.
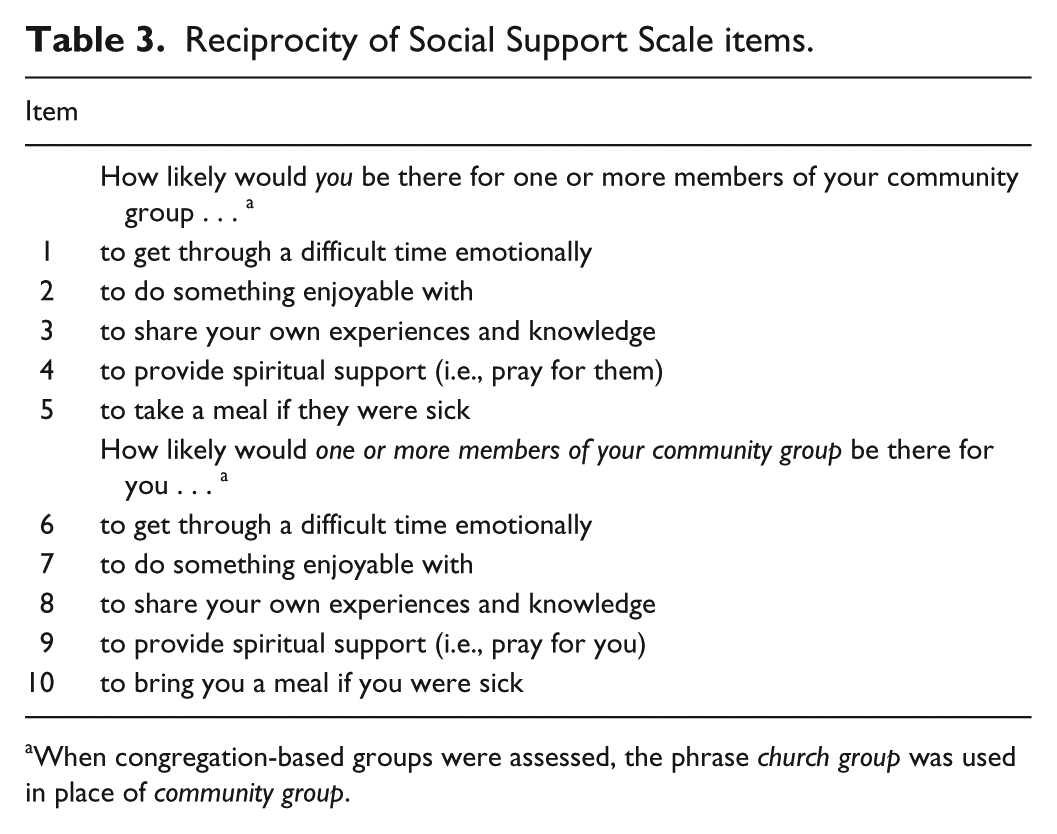
When congregation-based groups were assessed, the phrase church group was used in place of community group.
Phase IV: Procedures Used for Testing Psychometric Properties
Following content validation from the in-depth interviews, expert panel review of scale items, and cognitive interviews, a variety of psychometric methods were utilized in Phase IV to evaluate reliability and validity of the RSS Scale, and separate analyses were run for the community- and congregation-based groups.
Participants for Phase IV were a convenience sample of 500 adults. Researchers (H.C.P. and M.C.M.) recruited individuals from various community settings (e.g., parks, workplaces, laundromats, flea markets, convenience stores, recreational centers, fund raising events, civic clubs, and churches) to achieve a diverse sample that varied by age, race, and education.
Phase IV: Study Measures
In addition to the RSS Scale, other measures developed for the larger project to assess social capital in community groups were administered at the same time and included an 11-item RCG Trust Scale and a 2-item RCG Sense of Belonging Scale, developed by the authors using the same rigorous procedures as the RSS Scale and will be reported in separate manuscripts.
RSS Scale
The 10-item scale assessed the social support provided and received within each participant’s community- and/or congregation-based group. The RSS Scale is displayed in Table 3. A Likert-type 5-item response scale was used for all items (1 = not at all to 5 = very likely), which was scored by taking mean scores of the responses for the 10 items. Higher scores indicated higher levels of reciprocity of social support in the group.
RCG Trust Scale
An 11-item scale was developed to assess trust in community- and/or congregation-based groups. The scale measured four components of trust: openness, benevolence, honesty, and dependability (Hoy & Tschannen-Moran, 1999).
RCG Sense of Belonging Scale
A two-item scale was developed to assess an individual’s sense of belonging in a community- and/or congregation-based group.
Lubben Social Network Scale–6 (LSNS-6)
The six-item self-reported scale measured active network size of friends and family, potential instrumental support, and perceived confidents (Levy-Storms & Lubben, 2006; Lubben, 1988). This scale demonstrated high levels of internal consistency, stable factor structures, and high correlations with criterion variables (Lubben et al., 2006).
Socio-demographic characteristics
Items elicited key socio-demographic characteristics: gender, level of education, marital status, race/ethnicity, age, length of residency in current community, and length of membership and frequency of participation in selected group.
Phase IV: Analysis
Data were scanned into Excel© spreadsheets using Teleform© software, and imported into SAS© version 9.2 for data management and analysis, including descriptive statistics of participants’ demographic characteristics and scores from the RSS Scale, RCG Trust Scale, RCG Sense of Belonging Scale, and the LSNS-6.
To assess construct validity, an exploratory factor analysis (EFA) was conducted separately using promax rotation for community- and congregation-based groups to determine whether the survey items assessed the same latent dimensions and whether all items loaded similarly for each group type. According to Hatcher (1994), the minimal number of subjects for EFA should be greater than 100, or 5 times the number of variables being analyzed; therefore, the study groups were an adequate sample size for the analysis.
Convergent validity, a form of construct validity, was tested by Pearson correlation analyses between the RSS Scale and the RCG Trust Scale in community- and congregation-based groups. The theoretical framework predicted the two scales should have strong positive correlations. Convergent validity was also tested by Pearson correlation analyses between the RSS Scale and the RCG Sense of Belonging Scale. It was hypothesized that the scales should have strong positive correlations because they are theoretically related. Divergent validity, a form of construct validity, was tested by Pearson correlation between the RSS Scale and the LSNS-6. It was hypothesized that the RSS Scale and the LSNS-6 assess related although distinct constructs; therefore, it was predicted that there would be weak positive correlations between the RSS Scale and the LSNS- 6. Last, Cronbach’s α (Cronbach, 1951) assessed internal consistency of the 10-item RSS Scale in community- and congregation-based groups. A “high” value of α (≥.70) is considered desirable in most social science research studies (Nunnally & Bernstein, 1978).
Phase IV: Results
The average age of the participants (n = 500) was 45.95 (SD = 17.95), and 68% (n = 342) were female, 54% (n = 268) were white, 50% (n = 251) graduated from college or had completed any graduate study, 46% (n = 230) were married or living with a partner, and 34% (n = 172) had lived in their community 1 to 10 years. Socio-demographic variables were controlled for in all subsequent analyses. Phase IV participant socio-demographic characteristics are presented in Table 2.
The RSS Scale took a few minutes to complete, but was administered along with other measures of social capital, so the entire survey took on average 40 min to complete (ranging from 20 to 60 min).
A repeated-measures ANOVA was used to determine whether RSS Scale scores would vary for individuals who participated in a community-based group and a congregation-based group (n = 233). Results indicated that congregation-based groups had a slightly higher mean RSS Scale score (M = 4.45, SD = 0.58) compared with community-based groups (M = 4.36, SD = 0.73), though the difference was not statistically significant, F(1, 232) = 2.79, p = .0963.
EFA
The responses to the 10-item RSS Scale were subjected to an EFA using squared multiple correlations as prior communality estimates. The principle factor method was used to extract the factors. A rotation was not possible. A scree test suggested two meaningful factors. The results of the EFA are displayed in Table 4. A factor loading ≥0.40 is considered desirable in social science research (Costello & Osborne, 2005).
Reciprocity of Social Support Factor Loadings and Cronbach’s α Values If Item Was Removed for Community-Based Groups and Congregation-Based Groups.

Note. Bold items indicate high loadings (above 0.40).
Items 4 and 9 (spiritual support) and 5 and 10 (tangible support, that is, take a meal if they were sick) evidenced low-loadings (below .40) for both factors in the community group members. When the items with low loadings were dropped (Items 4, 5, 9, and 10), the two-factor model was run again with the six items that originally had high loadings (above .40).
Total number of participants exceed n = 500 because each participant could report they belonged to community- or congregation-based groups, or both.
EFA- and Community-Based Groups
For both types of groups, a two-factor model was used based on the hypothesis that social support is provided and received by members of a group. For members of community-based groups, Items 1, 2, and 3, all related to providing support to other group members, loaded strongly on the first factor (factor loadings from 0.64 to 0.85) and Items 6, 7, and 8 loaded strongly (range from 0.60 to 0.78) on the second factor, related to support received from members of the community group. Items 4 and 9 (spiritual support) and 5 and 10 (tangible support, that is, take a meal if they were sick) evidenced low-loadings (below 0.40) for both factors in the community group members. When the items with low loadings were dropped (Items 4, 5, 9, and 10), the two-factor model was run again with the six items that originally had high loadings (above 0.40). Results indicated a model fit for a two-factor model. From the original items, Items 1, 2, and 3 loaded strongly on the first factor, social support provided to members of a community group, now ranging from 0.68 to 0.74, and Items 6, 7, and 8 loaded strongly on the second factor, social support received from members of a community group, ranging from 0.69 to 0.77.
EFA- and Congregation-Based Groups
For congregation-based groups, a parallel two-factor model was tested. Items 1 to 5 loaded strongly on the first factor (0.51-0.82), for social support provided to members of a congregation-based group. Items 6 to 10 loaded strongly on the second factor (0.60-0.80), social support received from members of a congregation-based group.
Convergent Validity
The RSS Scale had a very strong positive association with the RCG Trust Scale for community- (r = .71) and congregation-based groups (r = .72; p ≤ .0001 for both). The RSS Scale had a strong positive association with the RCG Sense of Belonging Scale for community- (r = .60) and congregation-based groups (r = .625; p ≤ .0001 for both); therefore, convergent validity was established based on analyses.
Divergent Validity
The RSS Scale had a weak positive association with the LSNS-6 for community- (r = .26, p ≤ .0001) and congregation-based groups (r = .15, p = .0110), which established divergent validity.
Internal Reliability
Cronbach’s α values were high and consistent within the RSS Scale for both study groups. The raw α coefficient for the reciprocity scale was .92 for community-based groups and .93 for congregation-based groups, well above the acceptable level of .70 (Nunnally & Bernstein, 1978). In community-based groups, the raw α coefficient for the subscale social support provided was .87 and was .89 for the subscale social support received. In congregation-based groups, the raw α coefficient for the subscale social support provided was .87 and was .91 for the subscale social support received. Removal of any items did not dramatically alter the internal reliability of the scale. See Table 4 for the results of the EFA using a two-factor model and Cronbach’s α values if an item was removed for community-based groups and congregation-based groups.
Discussion
To our knowledge, this is the first scale developed to measure reciprocity of social support that is suitable for community- and congregation-based groups that has been created using a rigorous scale development process. Results indicated that the scale performed very well on tests of reliability and validity—content validity and different forms of construct validity, including convergent and divergent validity.
Norms of reciprocity were explored in community- and congregation-based groups using in-depth interviews. Through cognitive interviews and an expert review panel, items and response categories were assessed, strengthening the scale’s content validity (Knafl et al., 2007) and readability, allowing the scale to be self-administered.
The RSS Scale performed as expected in validity tests. Scree test findings suggested two meaningful factors. This procedure helped inform the decision to use a two-factor model, which reinforced the research team’s hypothesis of the conceptual nature of reciprocity of social support, specifically that social support is provided (Factor 1) and received (Factor 2). The EFA provided evidence that the items capture reciprocity of social support as two-factor models for both group types. It was hypothesized that there would be two factors of the reciprocity of social support—the first, social support provided to group members (Items 1-5), and the second, social support received from group members (Items 6-10). Results indicated that the norms for reciprocity of social support in community-based groups include providing and receiving emotional social support, positive social interaction, and informational social support, which has been found to have protective effects on mental health (Berkman & Glass, 2000; Gjerdingen, Froberg, & Fontaine, 1991; Janevic et al., 2004). Spiritual and tangible social support did not have adequate factor loadings in a two-factor model for community-based groups; therefore, these items (4, 5, 9, and 10) can be excluded when measuring reciprocity of social support in community-based groups.
However, the results of the EFA for norms of reciprocity in congregation-based groups included all 10 items. Therefore, the additive value of belonging to a congregation-based group compared with a community-based group may stem from providing and receiving spiritual and tangible social support. For future studies, the full scale may be used to explain the buffering effects of congregation-based groups on health outcomes compared with community-based groups.
As hypothesized, tests of convergent validity supported very strong positive correlations between the RSS Scale and the RCG Trust Scale for the community- and congregation-based groups (r = .71, .72; p ≤ .0001 for both study groups) and strong positive correlations for the RSS Scale and the RCG Sense of Belonging Scale for the community- and congregation-based groups (r = .60, .625; p ≤ .0001, for both study groups). Tests of divergent validity of the RSS Scale and the LSNS-6 demonstrated a weak positive association for the community- (r = .26, p ≤ .0001) and congregation-based groups (r = .15, p = .0110).
The Cronbach’s α values obtained in this study indicated that the items for community groups (α = .90-.91) and church groups (α = .92-.93) were highly correlated.
Results of this study provided evidence that community- and congregation-based groups contribute to reciprocal social support. Although results indicated that congregation-based groups contribute to higher levels of reciprocity of social support, levels were not significantly higher than community-based groups and thus do not confirm a difference in reciprocity of social support for these groups. However, the differences in item loadings for four factor suggest there are aspects of reciprocity that differ between the two types of groups. Currently, there is a lack of literature comparing reciprocity of social support in community- and congregation-based groups, so there is no empirical literature with which results can be compared. Further research is needed to explore whether significant differences in levels of reciprocity of social support exist within particular community- (e.g., volunteer groups) and congregation-based groups (e.g., faith-based support groups, prayer groups).
Although reciprocity is a core construct of social capital (Stone, 2001), little is known about it, as it is very rarely theorized, defined, or measured (Abbott & Freeth, 2008). Previous studies suggest that reciprocity is an indicator of the quality of social relationships (Stone, 2001), results in tangible and intangible resources (Cattell, 2001), facilitates access to resources (Hurtado et al., 2011), and impacts people’s abilities to solve common problems through collective action (Hawe, 1994; Stewart-Weeks & Richardson, 1998; Zakus & Lysack, 1998). Therefore, a valid and reliable measure of reciprocity is needed to determine if reciprocity of social support experienced in different types of groups (i.e., community-based groups and congregation-based groups) differentially affect health outcomes; Morgan & Swann, 2004).
To address this paucity, the RSS Scale will now allow for more sophisticated social capital theories to be examined and will assist in the advancement of understanding the relationship between reciprocity of social support in community- and congregation-based groups and the associations of protective health effects, particularly on mental health. If an association does exist, reciprocity of social support may be a targeted strategy for the prevention and management of chronic illnesses or the maintenance of healthy behaviors.
Kawachi and Berkman (2001) found that protective effects of social ties on mental health are not uniform across groups in society. Therefore, this measure may enable detection of variation in social support reciprocity among community- and congregation-based groups by demographic characteristics (i.e., age, gender, ethnicity, marital status, and socioeconomic status).
Limitations
The RSS Scale demonstrated reliability and validity in the sample in which it was developed; however, these findings should be interpreted in light of several limitations. This study used a convenience sample. Participants’ reciprocal behaviors related to social support may not have been representative of the larger population. Importantly, religious homogeneity of the qualitative work and validity sample limits the generalizability of the scale’s validity. The in-depth interviews were conducted with individuals belonging to a Christian Protestant denomination and the validity sample included only individuals of Christian faith. This is an indication where the scale is relevant for the Christian population, but may be less applicable in other faith traditions (e.g., Judaism or Eastern religious traditions).
In addition, the in-depth interviews that guided item formation were performed in a population of adults aged 50 and above; other aspects of reciprocity may not have been captured that are relevant to younger age groups. Moreover, women were overrepresented in the in-depth interviews and during administration of the instrument. However, reliability and validity testing indicated positive findings when administered to the study sample that ranged from ages 18 to 94 and to men, which indicates the scale is appropriate to use in various age groups and for men and women.
Finally, this scale may not be appropriate to use outside the Southern United States. The scales were developed in communities across South Carolina, which included high-income and very-low-income areas; however, further psychometric testing is needed for the scales if used in varied geographic and developing regions, so the items reflect the norms of reciprocity specific to the contexts of interest. For example, participants in this study did not identify self-esteem as an important dimension of social support, which refers to others’ communications indicating the person is valued (e.g., letting the person know they are competent at something or have an admired personal quality; Cohen & Wills, 1985). However, self-esteem has been found to be an important dimension of support among various populations in previous studies (Brookings & Bolton, 1988; Cohen & Wills, 1985).
Conclusion and Future Research
The RSS Scale for community- and congregation-based groups was developed over a 2-year process, which included qualitative work for item development and validity and reliability testing. To our knowledge, this scale is the first with proven psychometric properties that can be recommended for utilization in future research investigating reciprocity of social support in community- and congregation-based groups. An interesting finding from the study, as indicated by the EFA, was that the norms of reciprocity of social support for church groups include spiritual and tangible social support. Future research should focus on understanding the additive value of belonging to a congregation-based group compared with other community-based groups, and whether the additive value of a congregation-based group is associated with protective mental and physical health outcomes. Furthermore, our results showed small differences in mean RSS scores across different group settings (i.e., higher, but not significantly different scores in congregation-based groups compared with community-based groups). Further research is needed to investigate these differences and determine the implications of reciprocity in specific group settings. Recommendations of future research include adapting the scale for use in other faith communities and additional cultures, including developing countries and various ethnic and religious populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by a grant from the John Templeton Foundation.