
Abstract
Asset-Based Community Development (ABCD) is seen as a way of tackling the social determinants of health and reducing health inequalities. However, a better understanding of the mechanisms through which ABCD operates, and the environmental and relational conditions within which it is likely to be most effective, could increase its effectiveness at improving health and well-being and reducing inequalities. Interviews and focus groups were conducted with 25 people working in third sector and voluntary organizations to begin to improve understanding about ABCD approaches, how they are implemented, and how they are meeting the needs of disadvantaged populations. These individuals had local area knowledge of programs that follow an ABCD approach and which are currently running in the North West of England. The interviews were transcribed and thematically analyzed. Four overarching themes gave insight into the principles and practices of ABCD: Relationships and trust as mechanisms for change, Reciprocity and connectivity: “people not services,” Accountability and reducing dependency, and A socially sustainable model. ABCD focuses on identifying and developing individual capabilities, relationships, engagement within communities, and outcomes that are meaningful to people and consistent with relationships and support that are reciprocal and acceptable. ABCD is likely to be most effective in supporting vulnerable people where building trust is mirrored by an institutional and relational environment that is trustworthy and facilitative of developing people’s capabilities.
Background
Socioeconomically disadvantaged populations have shorter life expectancies than their more affluent counterparts and are more likely to suffer from a number of long-term and potentially life-limiting illnesses and associated risk factors (Marmot, 2010; Marmot & Wilkinson, 1999). Socioeconomic disparities also have the potential to affect upon the awareness, diagnosis, treatment, and control of these illnesses (Gupta et al., 2015; Steel et al., 2014; Yang, Qian, & Liu, 2017).
A recent evidence review found there are many community development and empowerment models where health needs are identified by the community members who then mobilize themselves into action (O’Mara-Eves et al., 2013). These models often aim to enhance mutual support and collective action and the review found there is evidence that they have a positive impact on outcomes, such as health behaviors and perceived social support (O’Mara-Eves et al., 2013). However, there is insufficient evidence to determine whether one particular model of community engagement is likely to be more effective than any other and there is insufficient evidence to test the effects on health inequalities (O’Mara-Eves et al., 2013).
There has been a resurgence of interest in asset-based community development (ABCD) in the context of global public health and particularly in the United Kingdom where it is seen as a way to address growing concerns over the widening of health inequalities (Brooks & Kendall, 2013; Bull, Mittelmark, & Kanyeka, 2013; Foot, 2012; Foot & Hopkins, 2010; Friedli, 2013; Morgan & Ziglio, 2007). ABCD has been described as a move from a disease prevention model to a more positive approach that aims to empower communities to tackle the social determinants of health by targeting general health and well-being (Bull et al., 2013; Foot, 2012; Foot & Hopkins, 2010; Morgan, Ziglio, & Davies, 2010). This approach aims to move away from top-down delivery with measureable targets that are put in place without consideration of the context in which they sit to a model that explores the links between individual health and social determinants and looks for ownership and accountability at an individual and community level. The Marmot Review (Marmot, 2010) encourages this new way of working and recognizes the need for the creation and development of healthy and sustainable communities who have suffered from the impact of social and economic inequality. It emphasizes the importance of utilizing local assets as key resources in tackling inequalities. As one of seven Marmot Cities, Coventry City Council, in partnership with public and voluntary sector organizations, worked to improve health inequalities through the facilitation of projects/programs and new ways of working (Faherty & Gaulton, 2017). This relationship between health care services, public health teams, and third sector and community groups has been encouraged by the 2013 transfer of public health services to local authority (Faherty & Gaulton, 2017). These actions were seen to result in a narrowing of the life expectancy gap between the most affluent and most deprived (Faherty & Gaulton, 2017). Other outcomes included educational development, health outcomes, improved life satisfaction and employment opportunities, and a reduction in crime in priority areas.
ABCD is seen as an important innovation in tackling health inequalities during a time of austerity and the changing landscape of localized health care. This is because it supports communities to set their own targets in terms of meeting their health and well-being needs (Foot, 2012; Foot & Hopkins, 2010; Hills, Carroll, & Desjardins, 2010). ABCD approaches to health and well-being identify and build on the strengths, or “assets” of individuals and communities (Kretzmann & McKnight, 1996), as well as valuing capacity, skills, knowledge, connections, and supportive potential in the community (Foot, 2012). ABCD adopts a partnership approach where services are coproduced and service users play a key role in the governance, design, and facilitation of services (Brooks & Kendall, 2013; Bull et al., 2013; Foot, 2012; Foot & Hopkins, 2010; Morgan & Ziglio, 2007; Morgan et al., 2010). ABCD may therefore be seen to offer the prospect of improving support for deprived/disadvantaged or neglected communities by adopting a collaborative approach (Foot, 2012; Foot & Hopkins, 2010).
The challenges of entrenched health inequalities in deprived and disadvantaged communities are long-standing (Marmot, 2010). The United Kingdom, along with many other countries, has in the years following the 2008 global financial crash adopted a policy of austerity. While austerity has been presented as a means of reducing deficits related to the financial crash, it is axiomatic that such a policy accords with wider neoliberal agendas. A primary strand of austerity policies has been an ongoing reduction in the resourcing of health services, local authorities, and in turn to funding difficulties for smaller local third sector (charitable) organizations that are key to improving health access for marginalized groups (Lamb et al., 2014). In the United Kingdom, the greatest burden of cuts has demonstrably been borne by the most deprived communities (Hastings, Bailey, Bramley, Gannon, & Watkins, 2015). It has been argued that this reduction in resource has occurred at a critical juncture, preventing potential efficiencies associated with improved intersectoral working being realized and has directly contributed to further fracturing of local service ecologies. Likewise, potential long-term efficiencies, through public health improvement and disease prevention strategies, have been sacrificed as services focus their limited resources on treatment, potentially increasing health inequalities and their impacts (Karanikolos et al., 2013). Within the context of politics of austerity, ABCD offers local authorities methodologies for optimizing the use of resources that are still available while also connecting positively with the individuals and communities who are carrying most of the socialized costs of corporate and market failure (Brooks & Kendall, 2013; Bull et al., 2013; Foot, 2012; Foot & Hopkins, 2010; Morgan & Ziglio, 2007). This can be realized by identifying and providing more appropriate and meaningful support to individuals and communities with the added benefit of improving health and reducing the need for accessing health services, thus potentially arresting the process of further socialization of the costs of the financial crash through cuts in the provision of public goods (such as health care).
The development and implementation of programs following an ABCD approach is promising in supporting such an agenda, and links with evidence that engagement with social networks and access to programs of work/enterprises that support such engagement play an important role in supporting health (mental and physical) of people with long-term conditions (Blakeman et al., 2014; Blickem et al., 2014; Reeves et al., 2014). However, there is currently limited evidence about the mechanisms underlying ABCD programs and the populations and contexts for which they are most suited. A realist synthesis by the authors (Blickem et al., 2018) provided some insights into possible key criteria for ABCD approaches, including how they work and what outcomes might be expected (Tables 1 and 2; Blickem et al., 2018).
Key Criteria of ABCD to Improve Health and LTCs.
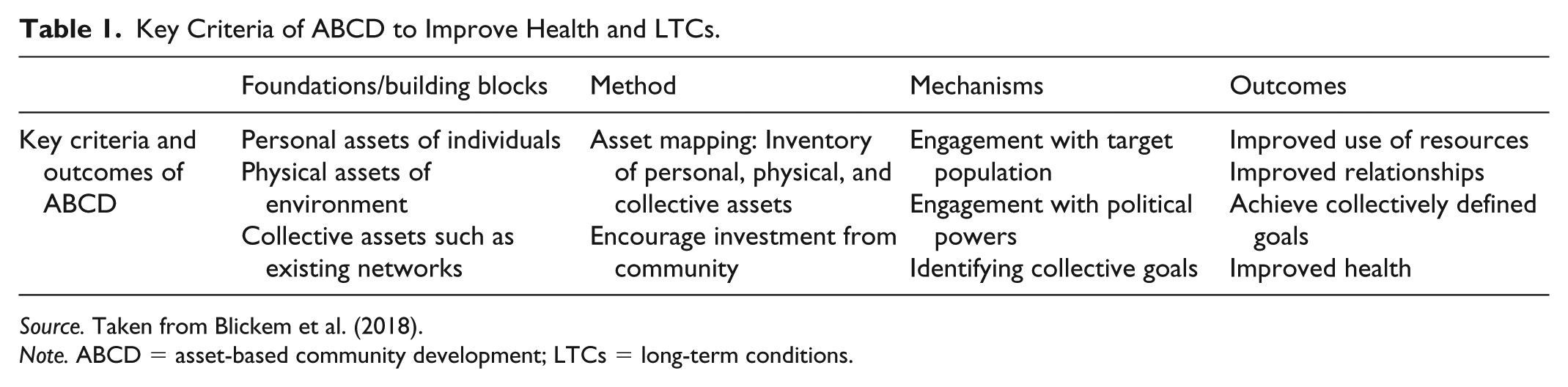
Source. Taken from Blickem et al. (2018).
Note. ABCD = asset-based community development; LTCs = long-term conditions.
Qualities of ABCD.
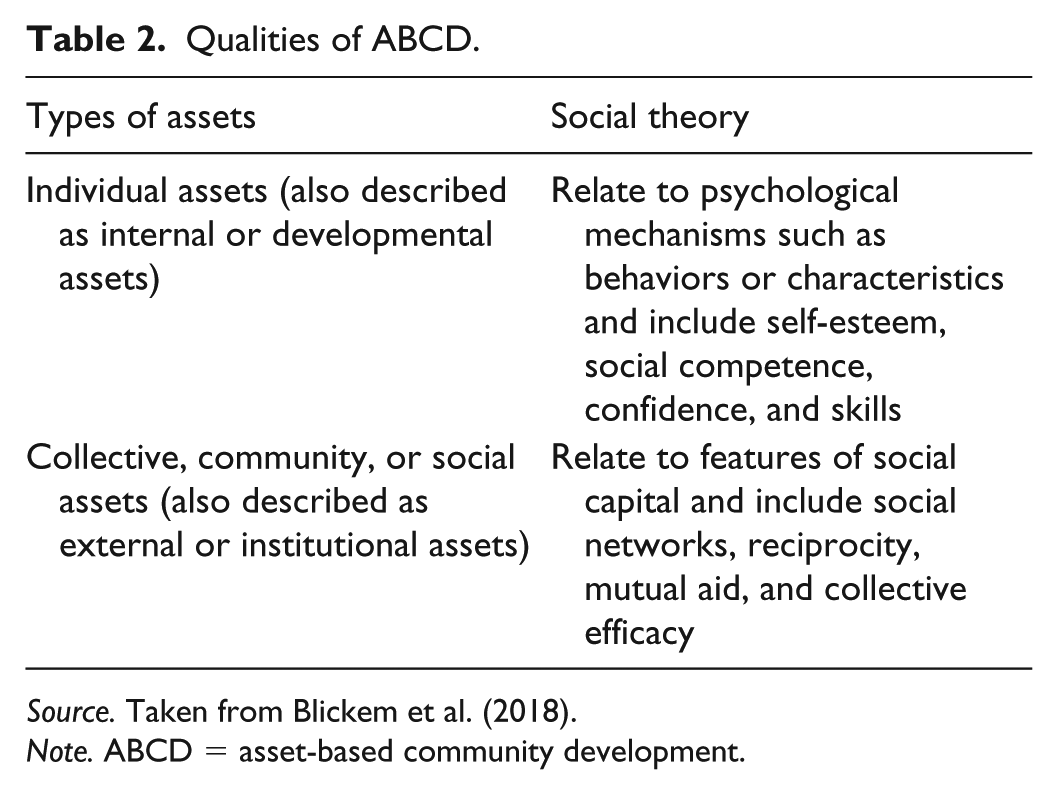
Source. Taken from Blickem et al. (2018).
Note. ABCD = asset-based community development.
This study intended to build on these findings to improve understanding about ABCD approaches, how they are implemented, and how they are meeting the needs of disadvantaged populations. Specifically the study aimed to
Provide an understanding about ABCD approaches from the perspective of community-based practitioners;
Examine ABCD in terms of who they work for and what benefits, if any, are achieved; and
Understand the underlying principles and processes of these approaches.
By understanding the ABCD approach from the perspective of practitioners, this study looked to explore and clarify some of the processes attributed to, and mechanisms or methods associated with, ABCD. With a fuller understanding of how ABCD operates in practice, this study aimed to provide some direction for how this approach can be more robustly applied and evidenced.
Method
Participants and Recruitment
Purposive sampling was adopted (Bowling, 2014), with participants of the study selected with the goal of being able to identify potentials for maximum variation and a range of perspectives from this sample to other actors and localities. Key individuals, who had local area knowledge of programs that claimed to follow an ABCD approach and which were currently running in the North West, were identified. Those contacted to participate in the study included regional community and voluntary sector organizations, community program managers, local public service leads, public health strategy and change leads, commissioners, public health specialists, and directors of public health. Between the months of January and May 2017, 92 individuals were contacted, with 25 agreeing to participate in the study. The final sample included community workers and local authority leaders whose organizations identified ABCD as one of their approaches. All of those who were contacted were sent a participant information sheet that provided more information about the project and its aims and objectives.
Interviews and focus groups were conducted with 25 people. This comprised of
Eight individual interviews;
One paired interview; and
Two focus groups (one with three people and one with 12 people).
Each interview lasted between 45 and 60 min. All of the interviews were conducted in person within the organizations where the individuals were based.
An interview guide was developed based upon the authors’ knowledge of the topic area and an article written by the authors (Blickem et al., 2018). The interview guide (see the appendix) focused on a number of key questions that aimed to elicit information about participants’ understanding of ABCD approaches, any examples of work that they have undertaken or knew about, how this approach may fit in with their organizational outcomes in the long-term, successes of this approach, and specific challenges/barriers.
Analysis
A grounded theory approach was used to guide data analysis (Charmaz, 2007). Open coding was initially used to analyze the transcripts (Coffey & Atkinson, 1996). Data were then analyzed thematically, using a constant comparison approach to develop themes (Miles & Huberman, 1994). This was carried out in the context of gaining a wider understanding of individuals’ knowledge and perceptions of ABCD and the impact this may have upon the development and facilitation of services; as well as potential challenges/barriers to this approach. Themes were developed independently by all authors and then agreed through discussion. Data collection continued until category saturation was achieved in that interviews continued until no new themes emerged from the data (Morse & Field, 1995).
Results
Topics raised in the interviews gave some insight into the principles and practices associated with ABCD. The analysis of the interviews identified four overarching themes in relation to ABCD. These were Relationships and trust as mechanisms for change, Reciprocity and connectivity: “People not services,” Accountability and reducing dependency, and A socially sustainable model. The following section will present these themes in relation to improving understanding about ABCD approaches and how they are reported to be meeting the needs of disadvantaged populations.
Relationships and Trust as Mechanisms for Change
ABCD was seen as being developed upon the premise of traditional community development but using a strengths-based rather than deficits-based approach to working with communities, that is, focusing on the positive features (assets) of a community rather than the problems associated with them. It was seen to be person-centered with an emphasis on relationships, which was usually articulated in opposition to bureaucratic approaches dominated by a drive toward formal accountability and detached from concrete needs and concerns: So we try and think about what’s the relationships that we’re trying to create here, rather than trying to create services. I think services as a concept gets in the way. If we try and create relationships, I think that’s what makes the most difference, because it helps people to get to the point where they don’t need us anymore. (P1)
Another participant highlighted the importance of person-centeredness to help create sustainability by building networks.
I think there’s a very clinical and medical model around health coaching and then there’s what we do as health coaching, which is more about a much more asset-based approach, looking at members of the community who may have experienced lifestyle changes themselves, training them up to be able to deliver that in their own community and creating a network, and kind of sustaining it that way. (P8)
Here the person-centered approach is contrasted with the medical model, aiding the process of translation of experiential knowledge into a communally available resource by building capacity for individuals to actually delivering it. This may evidence a shift/development of lay knowledge to lay teaching practice.
ABCD was seen to be distinct in its focus on identifying what would be seen as positive deviance.
Looking at a community or a population . . . . . . you’re looking for the outliers, if you like, the people who deviate away from standard behavior but do it in a very positive way, they’re doing better than their peers. (P1).
“Success” stories of resilience and survival were seen to be of particular value in areas with high levels of deprivation. Within a context of growing inequalities, where the external environments are hostile to facilitating individual health and well-being for a growing proportion of the population, ABCD offers inroads to identifying promising coping and resistance mechanisms building on human capacities, creativity, and labor as the resource that remains available. Specifically, they allow for community members to develop ownership and responsibility for their communities, make positive choices, and invest in relationships and their surroundings. There appeared to be less expectation of a shift in the availability of resource and environmental support, which translated into narratives focused more on building individual and community resilience and coping with such a context than on resistance and drive toward a political change. Thus, many of the interviewees talked about moving away from the traditional needs/deficit approach of public services and third-sector organizations toward an approach that focuses on the qualities of people, but saw such a shift in priorities as being within (rather than without) the status quo.
. . . people who are disadvantaged, where they are consistently defined by their deficits. And needs-based working, which is what most people are trained in, always defines people as a problem. And I don’t think people are a problem, I think they’re a solution most of the time. So for me, it just made sense to start looking at what people are good at, what their passions are, who they love. (P1)
This marks a broad gap between policy and implementation where, within the current climate, resources are only given under conditions of surveillance and accountability; this is usually in relation to narrowly defined outcomes and indicators that are usually not very meaningful in everyday contexts.
The sticking plaster approach doesn’t work, that whatever’s wrong, a person will keep presenting because it’s not healing the wound, it’s just putting a plaster over it. And asset-based approaches is about looking at the root cause and empowering people to find a solution for that root cause, with our support, themselves. And then that’s cost effective as well, so we’re seeing massive savings. (Participant from focus Group 2)
Reciprocity and Connectivity: “People Not Services”
Participants discussed the significant impact austerity has had upon the provision of services. However, this tended to translate more into questions about what can be done given the circumstances. It was seen as a vindication of an opportunity to normalize the use of ABCD as opposed to raising questions about the rationale and acceptability of such changes. Thus, the main emphasis in practitioner narratives was on ABCD as an asset-based approach, offering a practicable crisis management resource to soften the impact of the shrinking public sector and the reduction in access to services. For people in disadvantaged areas, this process was expected to need change in existing coping strategies, which respondents tended to see in positive terms: This needs-based, deficit-based approach, with humungous amounts of money being chucked at it, has made absolutely virtually no difference in terms of inequality whatsoever. I would say the evidence base is it doesn’t make much difference. . . . so in one sense, what have we got to lose by taking a strengths-based approach anyway? . . . . the austerity agenda, the cuts, etc., that have been happening in the last 5 years have been really helpful to a strengths- and asset-based working because many of the large agencies almost can’t avoid looking at where are the other resources that we can now use, because they don’t have the money to chuck at this stuff anymore. So that in a way is almost, perversely, helpful because they’re starting to become more and more open to what can communities and citizens do for themselves. (P1)
Reciprocity and connectivity were seen to lie at the heart of ABCD approaches, with people coming together around a common interest, albeit with varying degrees of success. ABCD was seen to be “citizen-led” and driven by the community thus acknowledging and building on what already exists and focusing more upon people and not services. These services were seen in most instances to be too inflexible to respond to need, possibly focused upon the wrong objectives and driven by narrowly defined outcomes. There was also a strong emphasis upon coproduction, that is, working with communities as well as within communities and the importance of connections or links to assets toward not only reducing a culture of dependency upon statutory services but also improving quality of life: I think part of the barrier is not just the deficit-based approach but the assumption that the solution to every problem is another service. And, as some of the (people) we work with fairly eloquently say, “We don’t need another bloody service, we’ve been through loads and loads and loads of services. Actually what we need is a decent quality of life.” And services can be a useful contribution to that, but they’re not the solution. (P1)
Communities were seen to be producing creative solutions to problems that worked to engage with others in their community. They were also seen to be more willing to take risks and innovate to make things work, which was seen as a contrast to a service-led approach. Once this sort of approach takes hold, then there is potentially a local and committed workforce to sustain positive change. This may be seen to illustrate a mixture of not only the need for trial and error element in adaptation to context but also the ideology of the wisdom of the community, the practical and the “hands-on”: Communities, I think, are a bit further, a bit more out there, more willing to take risks than organizations. And I think that’s important, that kind of ability or willingness to take risks or the willingness to innovate. . . . sustainable, long term, creative. There’s capacity an issue there as well. So it’s good because we have an army potentially, you know, we’ve kind of changed the world with an army, not with five quality improvement practitioners in a room at the CCG. (P2)
One example of this was a volunteer driver scheme run solely by members of the community to take patients suffering from cancer to their appointments. Not only was this scheme practically useful, but it was also seen to help develop relationships for the benefit of all parties. Another example was time banking, where skills were exchanged with other local people, for example, dog walking, shopping, knitting, lifting, and so forth; acknowledging that everyone’s skills are of equal value. These were not just seen as giving or exchanging help, according to one participant, but also these were ways to develop relationships with people who have a shared experience of life. If, for example, the volunteer drivers have experience of cancer or long-term health problems, then this is not their “problem” but rather their “asset”: So rather than seeing that experience as their problem, we’re seeing that as their asset in order to support other people because they’ve got an insight into managing that on a day-to-day basis. So it’s looking at, yeah, where that resides in an individual and their own strengths, rather than having an identity around a person who’s got anxiety or depression, saying, well, actually, you know, you’ve got really valuable experiences both of not only services but also negotiating your way through life with that, that you can bring to other people. (P6)
Practitioners of ABCD saw their role as tapping into these activities to facilitate and stimulate further action. One participant described his or her role as sharing his or her personal assets that people in more socially deprived circumstances may not have. This participant identified in addition to sharing his or her own resource that building resilience was also resource: And a key one within that realm is simply the people I know, the networks I’ve got that they don’t, and their parents don’t and their grandparents don’t, in many cases. And that’s an asset I can offer to them. They have 80% of what they need, they don’t need their aspiration building, they’ve already got aspiration. It’s how do we prevent them from having that aspiration knocked out of them that’s important, how do we build resilience. And then how do we provide them with the connections. . . . And then they can do their stuff. (P1)
Accountability and Reducing Dependency
Participants discussed the challenges of ABCD and in particular how services and organizations engage with community assets without changing them. Accountability and responsibility were seen as a concern for local services/organizations who felt the need to be in control of activities because of fears about repercussions if things go wrong: One of the big dilemmas in asset-based approaches is an understandable worry about if a GP or someone in a public service feels like recommending that someone starts and goes fishing next week or starts playing football, that your safe discharge of duty of care to something that might appear to be a bit unprofessionally or woolly, might come back to revisit you around some potential safeguarding thing. And then someone will ask, well, didn’t you do your risk assessments and didn’t you do your due diligence, and all those kind of things. (P3) So what we should be doing is trying to help those things to flourish, but mostly we should stop interfering. You know, for many occasions we need to be saying that to our staff, stop interfering, this is working, just let it work. But we’re a bit nervous of that. (P5)
This illustrates the tension between trust in rules and systems, and trust in people as alternative regulatory mechanisms and the current dominance of trust in systems in a highly bureaucratized public domain assumed to be inefficient and untrustworthy within the dominant neoliberal ideology. Thus, there is an underlying assumption that those responsible for the organization of community assets cannot be trusted to know what is right and do what is right. As an alternative, discussions focused around the principle of linking community assets with existing community services/public sector resources for a mutually beneficial relationship to enhance community assets. Participants questioned, however, whether it was possible to truly have or deliver an ABCD approach in this accountability and responsibility model, which requires specific method and process for it to work. This also speaks to the dangers or fears of professional/statutory service involvement because they bring with them their own values.
One example of this dilemma was a childminding scheme where parents/grandparents looked after each other’s children on an informal basis. This was seen as a great community asset, but the local health improvement programs were concerned about their duty of care in relation to safeguarding issues such as lack of Disclosure and Barring Service (DBS) checks and safety of play areas.
So, you know, in every community there’s always been groups of parents who set up a parent and toddler group in a local church, somebody brings along some toys, somebody else brings along a teapot and some teabags and whatever. Or groups of tenants. And, you know, they’re some of the classic examples of what happens in communities. And often, you know, that sort of community organization can go on for 15, 20 years and it doesn’t necessarily appear on anybody’s register or no organization is involved. (P7)
Similarly, this was shown to be evident with a breastfeeding support group where statutory services wanted to become involved: I’ve had a similar thing recently with the breastfeeding peer supporters. They’re volunteers who have done a really extensive training course around breastfeeding support. They’re more highly qualified on breastfeeding than health visitors would be. And a lot of them are, like, from nursing backgrounds or, you know, got professional backgrounds, or they haven’t got professional backgrounds but they’re mums and they’ve breastfed, and things like that. So a group of them wanted to set up a new breastfeeding support group. And that’s caused like a right palaver among some of the health visitors and children’s centers, you know, trying to almost like police it and saying, well, if they run it, they’ve got to have a health visitor going in, if they run it, it’s got to be called this and it’s got to run at this time in this building on this day. And it absolutely goes against what it’s supposed to be. . . . It’s there, it’s their energy that they’re giving to it and their time. (P4)
According to some participants, the problem with services getting involved in these informal activities is that they can create a culture of dependency and, when the money runs out and the support is no longer there, then communities have to start all over again. ABCD was viewed as a way of reducing this culture of dependency on services so that individuals/communities are able to be responsible for themselves and no longer need help from external organizations.
A Socially Sustainable Model in the Context of Austerity
ABCD was seen as a socially sustainable method for positive change in general, but the primary opportunity driving implementation of ABCD at the boundaries of traditional health services was neoliberal austerity. This is because individuals and communities are seen as being at the heart of solutions leading to self-reliance as something that is not only necessary at present, but also morally good. This sometimes extended into romanticizing a vision of a particular type of community—self-contained, self-sustaining, face-to-face, resilient—as a superior model of social organization and creativity that is best left alone and with little need for access to accumulated knowledge, evidence, experience, and expertise coming from outside.
The deficit approach logically leads you to a point where all the answers come from outside. So it’s an outsider, whether you’re an individual or a community . . . . . . If you start with an asset strengths based approach, the answer primarily comes from inside, which means it’s much more sustainable. (P1)
This strong commitment to the concrete and its many complexities made it difficult for the participants in this research to define what is or is not ABCD as they thought one of the most important principles of these approaches was having freedom, flexibility and to be responsive to very different sets of circumstances.
Because there’s never going to be a model, like you’re saying, if you are trying to measure something and it’s a clear model of doing it. If you are doing it an asset-based way, person X coming into [name of organization] and person Y, yes, you can just have the same training but actually those people are going to go on very, very different journeys and that model of working is never going to be the same. (P8)
ABCD has been difficult to evidence because they work at an individual level and so do not necessarily work with the same set of outcomes all the time. However, it was highlighted that being able to evidence this approach gives it credibility, for example, what is best practice, and how this might inform development of the approach going forward. From an organizational perspective, being able to evidence the effectiveness of coproduction with communities was important, but this should not stifle creativity: In my opinion, where the problem very often creeps in is that when people begin to see that a particular thing is effective, then they try and impose an evidence-based service model upon it. And in some respects that’s brilliant because it informs current, you know, customer practice and improves services, but done wrongly it stultifies the endeavors of the people who had the initial energy. (P3)
There were concerns that this focus on evidence could be used to try to impose evidence-based service models upon community organizations. Important outcomes, such as reducing social isolation and improving the life chances of young people, were identified, which can be difficult to track and measure: If you think about reducing social isolation, it’s really basic, isn’t it, it’s about saying that if somebody has no social connections and they’re sitting at home all day on their own, it’s not good. We’re social beings, aren’t we, to varying degrees, and by creating opportunities for people to come together, share common interests, have fun, do activities, whatever, it’s really obvious, isn’t it, that people’s sense of well-being is going to improve. But the challenge is, it’s tracking it, isn’t it, it’s measuring it. And most funders want to be able to measure things exactly . . . because what does it mean to say, well, actually here’s a case study, here’s somebody who says that by coming to the groups, whatever they may be, they’re connected to people, they feel better, whatever. It’s vague and sometimes it’s woolly. But actually, for me that’s the core of the human condition, isn’t it, it’s about the quality of people’s lives and just because you can’t measure it, it doesn’t mean it’s not valuable. (P7)
The need to focus on personally meaningful outcomes was seen as an important feature of ABCD approaches. A successful outcome for one person might be very modest, such as getting out of the house, but this might lead to further positive changes and it was recognized that when working with vulnerable people sometimes small steps are needed.
Discussion
In this study, practitioners described ABCD approaches as organic, innovative, natural processes with reciprocity and connectivity at their heart, with people coming together around a common interest, albeit to varying degrees of success. Linked with this were concepts such as skills, connectedness, collective assets, and knowledge, empowerment, and social capital. These concepts feature widely in the literature on ABCD (Blickem et al., 2018; Bull et al., 2013; Foot & Hopkins, 2010; Morgan et al., 2010; Rütten, Abu-Omar, Frahsa, & Morgan, 2009), but have been critiqued as vague ideas that do not produce a coherent approach to supporting disadvantaged communities (Friedli, 2013). However, this article and previous work by the authors (Blickem et al., 2018) have shown that ABCD has some conceptual clarity with methodologies associated with it. This study helps to illuminate some of the potential commonalities of approach between practitioners advocating/facilitating ABCD/an ABCD approach.
A key quality of ABCD practice is the strong emphasis on building and sustaining meaningful relationships within communities and developing networks of reciprocal exchange and acceptable support. While such approaches are likely to be consistent with the human condition generally, their application in areas of deprivation, within the context of growing inequalities and politics of austerity, is likely to benefit the most vulnerable people and communities (Blickem et al., 2018). This type of approach is in stark contrast to the way disadvantaged communities are often negatively defined as a set of problems, which leaves them feeling demoralized, disempowered, and isolated, in addition to being exposed to increasingly hostile, uncertain, and uninspiring environments (Blickem et al., 2018). The findings of this study suggest that on drawing on ABCD approaches such populations can start defining themselves differently, that is, what they are good at, what are their talents and skills, and so forth. Experiences, both positive and negative, are also seen as assets rather than deficits and further investigation is required into how individuals/communities talk about and develop their capabilities.
This places a focus upon relationality as a central tenet of ABCD not only in terms of building relationships and being inclusive to views, but also allowing space for considering the emergent properties of relationships. Optimizing use of resource may be seen as a primary objective with problems seen as resolvable through navigating around and making the “good” links, or just links. This focus upon capabilities and what matters to people moves away from actions that are based upon accountability and narrowly defined objectives. This was seen as important by participants because the previous “deficit” approach, reinforced by service models that are driven by apparent need, leads to a point where all solutions come from the outside. A model that identifies what services may already be available to fit individual/community needs, thus potentially compounds or encourages their problems. In addition, ABCD approaches are seen to provide solutions from the inside (rather than being externally defined), making the approach more meaningful to users and thus also more sustainable.
A major concern for practitioners was that externally defined need (and the resource made available to support need thus defined) has led to disadvantaged communities becoming heavily reliant upon health and social care services and developing coping strategies dependent on the availability of such resource. Reducing a culture of dependency and building a sense of agency was seen as an important objective to enable communities to identify their strengths so that they could begin to develop networks of support, embark on change, and make choices for themselves. Such a focus was justified through a combination of pragmatic (resource may be withdrawn at any moment) and normative (self-sufficiency and resilience as inherently morally good) arguments (MacLeod & Emejulu, 2014). In addition, as an ideology, ABCD appears consistent with, although not entirely reducible to, communitarian approaches to human development, with an emphasis on locality and building common purpose within localities as the best way to understanding and developing human capabilities (Bhattacharyya, 2004; Newman & De Zoysa, 1997; Reynolds, 2018).
Mobilizing social networks and focusing on community or population-based programs of work are seen as important approaches to supporting people with long-term health problems who are socially disadvantaged (Vassilev et al., 2011). There has been a move away from individually centered interventions to improving health, which have tended to hold individuals responsible for their poor health while ignoring micro and macrostructural influences (Vassilev et al., 2011). Collective efficacy, and its presence through social networks and communities, can be a protective factor for health, that is, being within a network that provides support, trust, and information on how this can help to achieve health goals (Lin, Fu, & Hsung, 2001). There is increasing evidence that focusing on social networks and community-based approaches to supporting disadvantaged communities can be very effective at improving health and well-being outcomes for people with long-term conditions (Blakeman et al., 2014; Blickem et al., 2018; Ennis & West, 2010). There is also a recognition that achieving positive outcomes is a collective process that requires the mobilization of a wide range of social, material, and environmental resources (Blickem et al., 2014; Carpiano, 2007; Stafford, De Silva, Stansfeld, & Marmot, 2008; Thoits, 2011). However, participants in this study discussed how vulnerable people may not have personal networks of support available to them and they may find it difficult to develop relationships. This may include people who feel let down by statutory services or who have had very difficult life experiences in environments that are untrustworthy, underresourced, or uninspiring, so building trust is a very important step toward supporting them to support themselves. Such a process would only be effective if building trust is mirrored by changing environments, institutions, and relationships into ones that are trustworthy. Thus, building capabilities is also about recognizing all that is current as a potentiality for development, so this also includes identifying where there may be gaps and insufficient capacity (Entwistle, Cribb, & Owens, 2018; Entwistle & Watt, 2013). Failing that, building trust may become meaningless or even irrational and earlier experiences of untrustworthiness maybe replicated.
One aspect of building relations of trust and trustworthiness is likely to require a move away from the dominance of a highly bureaucratized system of accountability and surveillance overseen by a neoliberal ideology with inherent distrust in regulatory mechanisms that are not market mediated.
Such a shift is likely to also open more space for regulating social relations through trust in people as opposed to trust in formal systems, rules, and regulations (Pilgrim, Tomasini, & Vassilev, 2010). ABCD approaches can help shift this balance through providing a platform for identifying meaningful relationships, developing capabilities, and building interpersonal trust.
Pilgrim, D., Tomasini, F. and Vassilev, I., 2010. Examining trust in healthcare: A multidisciplinary perspective. Palgrave Macmillan, London.
This study can help to modify and develop what is already known about ABCD approaches by revising a previous model proposed by the authors (Blickem et al., 2018). Trust, trustworthiness, and developing relationships can be considered to be the key mechanisms for an ABCD approach to work (Table 3). It is also important to stress that collective assets (Table 2) appear to be the fundamental building block for ABCD approaches because of the emphasis on social capital, social networks, and reciprocity.
Key Criteria of ABCD to Improve Health and LTCs—Newly Identified Mechanisms.
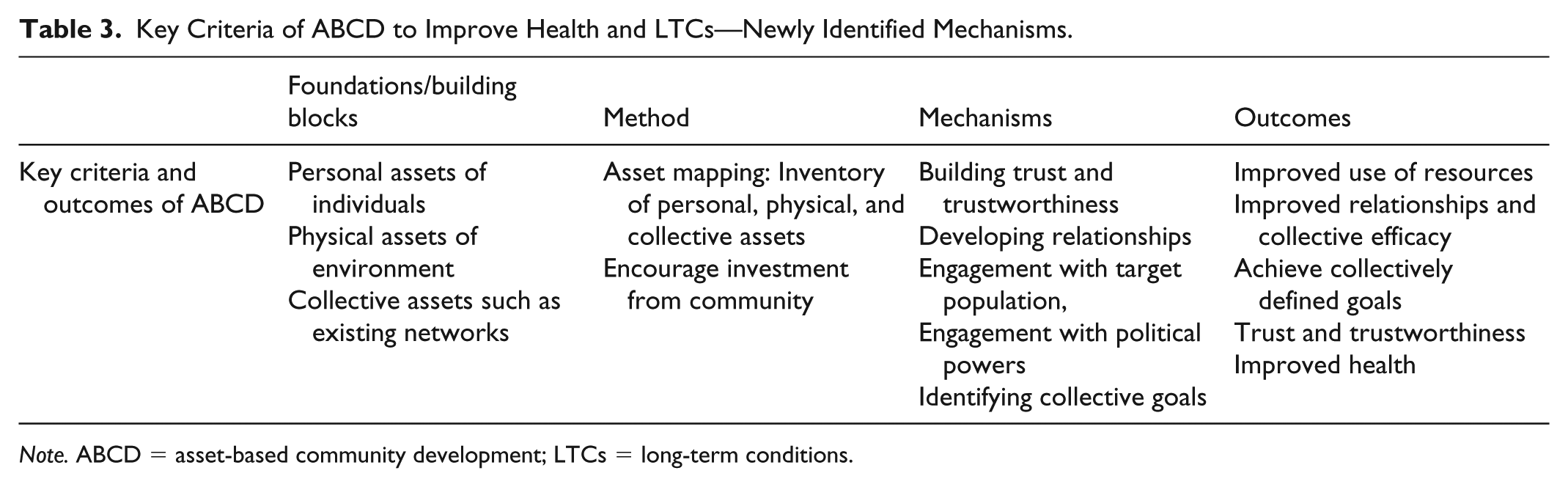
Note. ABCD = asset-based community development; LTCs = long-term conditions.
ABCD is seen by practitioners as a socially sustainable model to support disadvantaged communities because the austerity agenda may be seen to have created a favorable climate for promoting such approaches, for example, with large organizations that no longer have the level of investment they once had. On a personal level, this is clearly very important to practitioners, but this is only an indication rather than proof that their approach might be better. It is necessary to interrogate more closely how practitioners share their own resource and see building resilience as a resource. Although they provide a personalized, face-to-face support, it is not clear how much this differs from external support via services. However, as an ideology, it appears consistent with, although not entirely reducible to, communitarian approaches to human development, with an emphasis on locality, building common purpose within localities, and so forth, as the best way to understanding and developing human capabilities.
Strengths and Limitations of the Research
The coverage of this scoping project was limited to the North West region of England, including local authorities in the Liverpool City Region as well as Greater Manchester and Cumbria. However, the range of practitioners interviewed in this study suggests these findings may be generalizable across areas with similar demographics in the United Kingdom although further research is needed with members of communities whom these organization support.
Footnotes
Appendix
Authors’ Note
RH designed the study, conducted data collection and analysis, and wrote the article. CB designed the study, conducted data collection and analysis, and wrote the article. JL and IV contributed to the design of the study and wrote the article. SK wrote the article. With regard to ethics, before commencing, participants were verbally informed of the study and their confidentiality and arrangements for storage of data. They were then asked to sign a written consent form (if face-to-face). Ethical approval was granted by Liverpool John Moores University Ethics Committee (ethics reference: 16/PBH/015). The views expressed are those of the author(s) and not necessarily those of the National Health Service (NHS), the National Institute for Health Research (NIHR), or the Department of Health and Social Care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Liverpool Clinical Commissioning Group Research Capacity Funding. Ivaylo Vassilev’s contribution to this research was funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) Wessex.