
Abstract
This study aims to develop and validate generic measures of perceived, internalized and enacted stigma for use with adolescents who have a diverse range of chronic illnesses. The findings of a qualitative study aimed at capturing commonalities in lived experience of the forms of stigma among adolescents with diverse illnesses were used to create the measures. Think-aloud interviews were conducted to ensure the measures were clearly understood by adolescents with an illness. The psychometric properties of the measures were then examined using a convenience sample of 189 adolescents with various illnesses. Principal component analyses of the measures identified four components for internalized stigma, two components for perceived stigma, and three components for enacted stigma. The internal consistency and test-retest reliability of the measures were acceptable. As expected, each measure correlated moderately with the self-esteem, and depression and anxiety measures but did not correlate substantially with the social desirability measures, providing support for predictive and discriminant validity. The three generic measures have sufficient reliability and validity to assess individual-level stigma among adolescents with chronic illnesses.
Plain Language Summary
This study was focused on creating reliable and valid generic measures of perceived, internalized, and enacted stigma for use with adolescents with different chronic illnesses. The measures were developed based on a previous study examining commonalities in adolescents’ lived experience of the stigmas, and were checked for clarity using ‘think-aloud’ interviews. Psychometric testing of the measures with 189 adolescents showed the measures had a clear structure (internalized stigma had 4 parts; perceived, 2; enacted, 3) and were consistent. Importantly, the scores correlated moderately with low self-esteem and anxiety, confirming they accurately measure the forms of stigma. These three measures are now validated tools for assessing individual-level stigma.
Stigma is defined as a social process in which an individual possessing a characteristic or attribute considered different from the social norm is excluded by others and treated disparagingly, both by others and themselves (Goffman, 1963; Link & Phelan, 2001). This social process also includes self- and other-emotional reactions and status loss, all of which occur in situations of differential power (Link et al., 2004; Link & Phelan, 2001). Having an illness inherently carries a social stigma (Goffman, 1963; Scambler, 2009). This occurs because those who possess the illness represent a deviation from what society expects health to look like or values as being healthy (Earnshaw et al., 2013; Fife & Wright, 2000; Stuenkel & Wong, 2009). Furthermore, people living with an illness often present with deviations in behavior or appearance from what is the norm in society or social interaction (Idemudia et al., 2018; Maffoni et al., 2017; Rodrigues et al., 2025). As a direct result of these deviations, they become vulnerable to being negatively treated and, consequently, stigmatized.
Adolescence represents a particularly difficult point in development as young people experience substantial physical, psychological, and social changes, all of which significantly impact their experience of illness-related stigma. Socially, adolescents move from a focus on their families and parents to their peers (Berk, 2004; Deacon & Stephney, 2007; Faulkner, 2003; Petersen et al., 2005; Sanders, 2013). The implication of this developmental shift is that social comparisons become more salient and important for adolescents, making the experience of stigma more pronounced for those living with a chronic illness (see review in Berk, 2004; Piaget & Inhelder, 1969). In addition to social changes, adolescents also expand their cognitive abilities, gaining the capacity to reason and understand their world in a more abstract manner (see review in Berk, 2004; Piaget & Inhelder, 1969). This cognitive growth means that adolescents begin to understand the health conditions they may have in greater detail, as well as possibly questioning how an illness is managed (Berk, 2004; Piaget & Inhelder, 1969). Furthermore, the environment adolescents encounter differs substantially from that experienced by adults (Berk, 2004; Faulkner, 2003; Petersen et al., 2005). For instance, adolescents typically attend schools where they experience less autonomy and control over themselves at a time when they begin to question why and how things are done (Berk, 2004; Faulkner, 2003; Petersen et al., 2005). These developmental and environmental differences may collectively lead adolescents to experience a different social reality than adults, especially when they are managing a chronic illness.
Literature Review
Problems with Measurement
Many health conditions associated with stigma in adults, such as asthma, sickle cell disease, epilepsy, and cystic fibrosis, have their origin during adolescence (Sawyer et al., 2007). However, much of the existing research on the experience of illness stigma in adolescents has been framed in terms of adult perspectives and experiences (Austin et al., 2004; MacLeod & Austin, 2003). This practice has been called into question by others and, consequently, limits the conclusions that can be confidently drawn from the research. One key problematic practice observed is that the measures used to quantify the experience of illness stigma were often not developed from the perspectives of adolescents. Instead, researchers often imposed their conceptualization of stigma by modifying the language in existing measures created for adults, or they used the perspectives of other adults, such as health professionals, parents (e.g., Arda Sürücü et al., 2020; Counts et al., 2025; C. A. Johnson et al., 2024; Paller et al., 2024; Pantelic et al., 2020; Soufi et al., 2024; Wiklander et al., 2013; Wright et al., 2007). The practice is problematic because the areas covered in such measures may not totally capture or readily overlap with the unique social experiences and contexts of adolescents (Austin et al., 2004; MacLeod & Austin, 2003).
A related issue observed in a number of other studies is the reliance on proxy ratings, where informants other than adolescents, such as their parents, are used to determine the adolescents’ experience of illness stigma (e.g., see review in Austin et al., 2004; Geoffroy et al., 2024; see review in MacLeod and Austin (2003), Liu et al. (2017), Meltzer et al. (2011); HIV—Surkan et al., 2010). The literature suggests that this practice may have affected the accuracy of the findings of these studies, as proxy ratings have been shown to differ significantly from self-reports (see reviews in Austin et al., 2004). It is strongly argued that the experience of stigma is largely subjective. As such, the use of adults’ experiences and perspectives to study the experiences of adolescents is not appropriate, as their experiences are different from those of adults, both in terms of their understanding of their illnesses and how they believe they are affected by them (Austin et al., 2004; Deacon & Stephney, 2007; MacLeod & Austin, 2003). Furthermore, unlike adults, adolescents are still developing cognitively, emotionally, and socially (Austin et al., 2004; Deacon & Stephney, 2007). Therefore, attempts to measure their experience with illness stigma should be specific to their developmental level, with the items reflecting their lived experiences, which are best achieved through qualitative assessments (Austin et al., 2004; MacLeod & Austin, 2003). While some researchers recognize the value of lived experience and have partially incorporated the qualitative perspectives of adolescents into quantitative measurement of their stigma experience (e.g., Austin et al., 2004; Kaushik et al., 2017; Moses, 2009; Ortiz-Domenech & Cumba-Avilés, 2021), these works typically focus on specific illnesses.
Need for Generic Measures Assessing Illness Stigma in Adolescents
Previous research examining the personal experience of stigma related to various illnesses, which has included studies with adolescents and adults, has indicated that there are similarities in the ways stigma is experienced across different conditions and suggested that generic measures should also be developed for use with multiple illnesses (van brakel, 2006; van Brakel et al., 2019). Indeed, a number of generic measures have been developed for use across illnesses in adults (e.g., Earnshaw et al., 2013—Chronic Illness Anticipated Stigma Scale; Rao et al., 2009—Stigma Scale for Chronic Illness). However, as reviewed earlier, the use of these adult measures with adolescents may be limited as they are likely to be inadequate in reflecting their unique experiences. Furthermore, existing stigma measures for adolescents, in addition to being illness-specific and only partially reflecting lived experiences, only focus on one of the three forms of stigma. Consequently, there remains a critical need for the development of generic measures that can be used across illnesses in adolescents.
This research is original in that it makes an empirical contribution by creating generic illness stigma scales for use with adolescents, which incorporate their lived experiences. Such developmentally appropriate measures would be useful for consistently exploring the complexities of and variations in adolescents’ experiences of stigma due to their illness over time, and for accurately assessing the effectiveness of programs designed to improve their health and well-being.
Theoretical Framework
The current research is guided by an expanded Modified Labeling Theory (MLT), which explains how individuals experience stigma at the individual level. The Modified Labeling Theory MLT (Link et al., 1989), which is based on work with adults, centers on perceived stigma, where individuals with a characteristic that differentiates them from others internalize negative societal stereotypes about their characteristic, leading to an awareness of these stereotypes and the expectation of devaluation and discrimination (known as enacted stigma). In response, the individuals engage in protective behaviors (e.g., secrecy, limiting social interaction, educating others, etc.) to avoid discrimination, which ultimately results in negative social and psychological consequences for them. Corrigan and colleagues (Corrigan & Watson, 2002a, 2002b; Corrigan et al., 2006; Watson et al., 2007) expanded this by proposing self-stigma, which occurs when the individuals also agree that the negative stereotypes are true and accept them as true of themselves, leading to a reduction in their self-esteem or self-efficacy. Self-stigma has also been called internalized stigma in the literature (Rao et al., 2009), and may manifest in individuals as various negative beliefs, thoughts, feelings, and behaviors (Brohan et al., 2010; van brakel, 2006).
Thomas and Lipps (2025) have further extended this conceptualization by incorporating a developmental perspective, suggesting that the experience of the three forms of stigma is fundamentally altered by adolescents’ social and cognitive development. This alteration moves the experience of stigma from a focus on specific actions to a more abstract conceptualization that grows with cognitive development. Socially, the experience of stigma shifts for adolescents toward issues of social inclusion or exclusion within their peer group. Importantly, the influence on perceived stigma is nuanced in adolescents as their experience of stigma centers on the anticipation of negative treatments rather than an awareness of negative societal stereotypes, which is enabled by the growth in abstract reasoning and social comparison processes characteristic of this developmental period.
Relationship of Stigma to Psychosocial Outcomes
Several previous studies have examined the experience of stigma due to having a chronic health condition and have found multiple negative consequences for individuals with the health condition. One of the most common consequences of experiencing stigma due to an illness is the negative effect it has on the self-concept of individuals (e.g., see review in Bonfine, 2013; Livingston & Boyd, 2010); experiencing stigma due to an illness has been negatively associated with self-esteem or self-efficacy. Mental health problems are also commonly reported as a result of experiencing stigma, with several studies finding a clear link between experiencing stigma and symptoms of depression and anxiety among individuals with various health conditions (Jenerette et al., 2012; Taft et al., 2009).
Furthermore, numerous studies have identified a negative effect of experiencing stigma on individuals’ social relationships and interactions with others (Earnshaw et al., 2013; Puhl & Heuer, 2009, 2010). In response to feeling stigmatized, individuals often engage in protective behaviors—such as social withdrawal, avoiding contact with others, self-isolation, selective disclosure, secrecy, concealment, or non-disclosure—in an effort to manage information about themselves or others’ impressions of them (Emlet, 2006; Papathanaious et al., 2001). These behaviors, in turn, result in strain on their social interactions due to poor interpersonal relationships (Badlan, 2006; Puhl & Heuer, 2009, 2010) and decreased perceived social support (Fukunaga et al., 2011; Puhl & Heuer, 2009).
Experiencing illness-related stigma has also been found to have a negative effect on how individuals manage their health conditions. Research has shown this to be a barrier to whether individuals sought healthcare for their conditions (Bediako et al., 2016), accessed treatment and adhered to treatment regimens (Rüsch et al., 2009), and adhered to the lifestyle recommendations (J. L. Johnson et al., 2007; Thomas & Nair, 2011).
The Present Study
The current study reports on the next steps of a multi-phase research effort focused on the development of generic measures of individual-level stigma for use with adolescents with a chronic illness. The primary aim is to develop psychometrically sound measures of perceived, internalized, and enacted stigma that can be used across various illnesses in adolescents. This research is specifically designed to overcome the limitations and inadequate practices highlighted in the literature review by deriving the contents for the measures from a direct exploration of adolescents’ experiences and perspectives through the use of qualitative methods.
Research Hypotheses
Methods
Participants
One hundred eighty-nine adolescents with various health conditions participated in this study. Their ages ranged from 12 to 19 years of age (mean age = 16.3 years, s.d. = 2.0 years). One hundred and thirteen of them (approximately 60%) were females. They were grouped according to their illnesses as follows: sickle cell disease (n = 37, 26.9%), endocrine condition (diabetes, thyroid and weight issues; n = 35, 18.5%), mental illness (depression, schizophrenia, ADHD, panic disorder, and conduct disorder; n = 30, 15.9%), HIV (n = 32, 16.9%), neurological condition (epilepsy/seizures, migraine/headaches, Bell’s palsy, myasthenia gravis, transverse myelitis, and paroxysmal-kinesigenic choreoathetosis; n = 32, 16.9%), and pulmonary condition (asthma, other restrictive conditions; n = 23, 12.2%). They were recruited through specialist clinics at two large general hospitals, and a public and private clinic in Kingston and St. Andrew, Jamaica. Table 1 provides an overview of the demographic and health characteristics of the adolescents who participated.
Demographic and Health Characteristics of Adolescents Participating in Study.
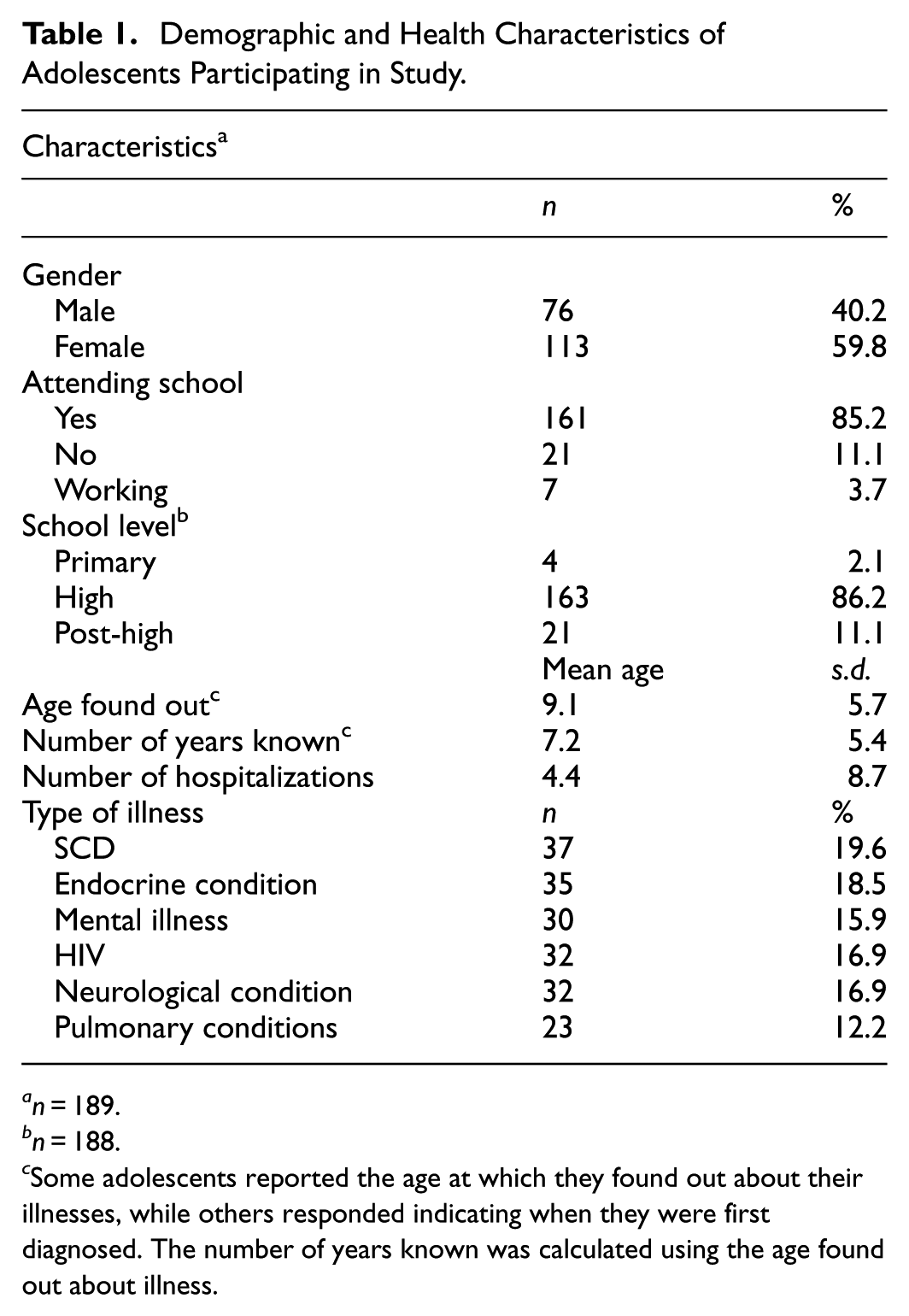
n = 189.
n = 188.
Some adolescents reported the age at which they found out about their illnesses, while others responded indicating when they were first diagnosed. The number of years known was calculated using the age found out about illness.
Development of the Generic Measures of Individual-level Stigma for Adolescents with a Chronic Illness
A three-stage approach, which combines both qualitative and quantitative techniques, was used to create the three generic measures of stigma. The stages moved from an initial qualitative phase (stage 1), through a quantitative item generation phase (stage 2), and concluded with a final qualitative refinement phase (stage 3).
Stage 1—Conceptualizing the Three Forms of Stigma from Adolescents’ Experience
A qualitative study was conducted previously by means of in-depth interviews with adolescents with various illnesses to conceptualize, in a generic way, the three forms of stigma (perceived, internalized, and enacted) based on their lived experiences. The findings of this study are reported elsewhere (Thomas & Lipps, 2025); nevertheless, a summary of the findings would be helpful here. The experiences of the adolescents with the three forms of stigma varied over the course of their illnesses due to their developmental level, cognitive maturity, and changes in their peer groups. Figure 1 provides a visual representation of the different forms of stigma along with the subthemes that came out of the qualitative study of how the adolescents experienced them.
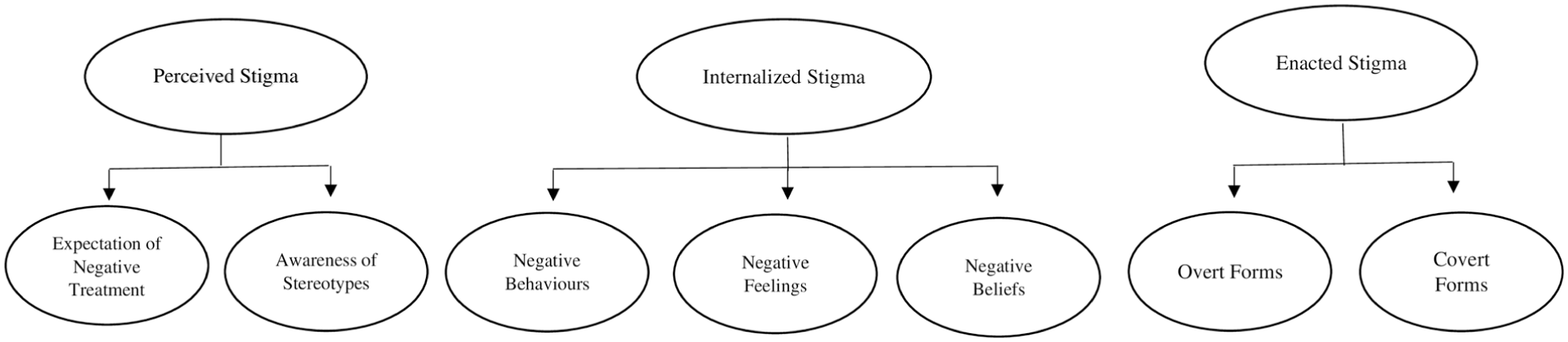
Conceptual model of the three forms of stigma from the viewpoint of adolescents with various illnesses.
Perceived stigma consisted of two subthemes: expectation of negative treatment and awareness of negative stereotypes. The experience of the adolescents with this form of stigma was centered more on various negative reactions or treatments they feared receiving if others found out or knew about their illnesses than on having an awareness of negative stereotypes related to their illnesses. Their expectation of negative treatment consisted of fearing what others would say or do to them or think about them if they knew about their conditions. Some of the negative treatments they feared experiencing included those who knew about their conditions telling others who would then treat them badly; being called names; being laughed at or made fun of; being teased; being treated as if they were different or abnormal; scorned; pitied; their condition being used against them; and being seen as sick and unable to do certain things. They also feared that their illness could be used against them and that talking about their illness could result in them being rejected by peers and important adults. Their awareness of stereotypes regarding their specific illnesses was limited and based on personal experiences or witnessing how others were treated.
Internalized stigma consisted of the subthemes: negative behaviors, negative feelings and negative beliefs. The adolescents internalized their expectation of various negative treatments, which resulted in various negative behaviors that included keeping their illness a secret from others and avoiding social interactions with those who treated them negatively in the past or whom they feared would do so in the future. Negative feelings they experienced due to their illnesses included, for example, feeling different from others, not feeling normal, feeling left out and feeling embarrassed. Negative beliefs consisted of the adolescents internalizing stereotypical beliefs about people with their illnesses, for example, believing that people with their condition looked different or would die early, which manifested as negative feelings and beliefs about themselves.
The adolescents experienced enacted stigma (negative treatments) mainly in their interpersonal relationships, through the overt and subtle actions of others. Overt actions included, for example, being called names, scorned, or laughed at. Covert actions included, for example, being treated differently, rumors being spread about adolescents, and the illness being used against adolescents.
Stage 2—Generation of Items for Generic Stigma Measures
Using the results of the qualitative study (Thomas & Lipps, 2025), items were written to measure the three forms of individual-level stigma, that is, perceived, internalized and enacted stigma. As much as possible, the actual words and expressions used by the adolescents in the qualitative study were incorporated into the items. This approach enhanced the face and content validity of the measures as well as their relevance to adolescents with different illnesses (Haynes et al., 1995; Moffat et al., 2009; Vogt et al., 2004). A pool of 72 items was developed with 33 items assessing the experience of internalized stigma, 10 items assessing perceived stigma, and 29 items assessing enacted stigma. As the adolescents’ experience with the different forms of stigma varied over the course of their illnesses, the four-point, frequency response option, 1 – not at all, 2– a little, 3 –to some extent, and 4 –a lot was chosen for responding to the items.
Stage 3—Qualitative Refinement of Generic Stigma Measure using Think-Aloud Interviews
Following the development of quantitative measures in stage 2, the final stage (stage 3) then used think-aloud interviews (a qualitative method; Collins, 2003; Hagen et al., 2008) to refine the pool of items. The think-aloud (cognitive) interviews were conducted with 12 adolescents (5 males and 7 females) with various health conditions to assess the relevance of the items as well as the clarity and appropriateness of their wordings. As each adolescent responded to an item, they were asked to explain their answer or say what they were thinking when they decided on their answer. Based on this, several items were revised to include translations into the Jamaican dialect or explanations added for clarity. The response options were also slightly modified in that ‘to some extent’ was changed to ‘some of the times’ and the period chosen for responding to the measures was specified as ‘their experience since they have had the illness’. Scores on the measures were obtained by summing numerical values for the responses to the items on each measure after reverse coding any negatively worded items. The three scales do not have specific cut scores to group participants into stigmatized and non-stigmatized groups. Instead, scores on the measures should be interpreted in terms of the magnitude of adolescents’ experienced stigma.
Measures Used to Assess Predictive and Discriminant Validity
Given the absence of a known, similar generic stigma measure for adolescents with chronic illnesses that could be used to establish concurrent validity (Cronbach & Meehl, 1955), the validation of the new measures was focused on establishing construct validity via a nomological network. Therefore, adolescents participating in the study were asked to respond to the three newly created generic stigma measures in addition to selected outcome measures for self-esteem, self-efficacy, and symptoms of depression and anxiety. These concepts were chosen because they have been consistently associated with the experience of illness-related stigma in the literature (e.g., Earnshaw et al., 2022; O’Donnell & Foran, 2024). Including these measures was necessary to establish the predictive validity of the new stigma scales. Additionally, adolescents also responded to measures of social desirability to support the establishment of the discriminant validity of the new stigma scales. The various measures included in the study are described below.
Rosenberg’s Self-Esteem Scale (RSES)
Self-esteem was measured using a revised version of the Rosenberg Self-Esteem Scale (RSES, Rosenberg, 1965). Scores on the RSES were expected to be moderately and negatively correlated with scores on the generic stigma measures if the stigma measures have predictive validity. The RSES is a 10-item scale that assesses global feelings of self-acceptance and self-worth using five positively and five negatively worded items. The items are rated using the four-point Likert scale: 1 –strongly disagree, 2 –agree, 3 –disagree, and 4 –strongly disagree. In the revised version, alternative wording or explanations of words were included for six of the items for clarity based on the outcome of the think-aloud interviews. Scores on the scale were obtained by summing numerical values for the responses to the items after reverse coding of negatively worded items. Higher scores indicated greater self-esteem. The scale has been used in research with samples of a variety of ages and is known to have acceptable reliability ranging from 0.77 to 0.88 (Fife & Wright, 2000). The internal consistency reliability of the scale in this study was 0.85.
Generalized Self-Efficacy Scale (GSE)
Self-efficacy was measured using a modified version of the Generalized Self-Efficacy Scale (GSE; Schwarzer & Jerusalem, 1995). Scores on the GSE were expected to relate moderately and negatively with scores on the generic stigma measures if the stigma measures have predictive validity. The GSE is a 10-item scale designed for individuals 12 years and older that assesses one’s belief in their ability to cope and adapt to daily activities and stressful events. The scale is rated using the four-point Likert scale: 1 –not at all true, 2 –hardly true, 3 –moderately true, and 4 –definitely true. Modifications to the scale were made following the think-aloud interviews. The modifications included adding alternate wording for each item and using a slightly modified response format. The response options were now 1 –not at all true, 2 –a little true, 3 –somewhat true, and 4 –definitely true. Scores were obtained by summing numerical values for the responses to the items. Higher scores indicated greater self-efficacy. The scale has been used in research with samples from a variety of countries and has internal consistency reliabilities ranging from 0.76 to 0.90 (Schwarzer & Jerusalem, 1995). The internal consistency reliability of the scale in this study was 0.81.
Revised Children’s Anxiety and Depression Scale (RCADS)
The major depressive disorder (MDD) and generalized anxiety disorder (GAD) subscales of the Revised Children’s Anxiety and Depression Scale (RCADS; Chorpita et al., 2000) were also administered to the adolescents to measure their levels of depression and anxiety symptoms. Scores on the sub-scales were expected to relate moderately and positively with scores on the generic stigma measures if the stigma measures have predictive validity. The Revised Children’s Anxiety and Depression Scale (RCADS) is a 47-item measure of depression and anxiety symptoms for children and adolescents (6–18 years old) with six subscales, including separation anxiety disorder (SAD), social phobia (SP), generalized anxiety disorder (GAD), panic disorder (PD), obsessive compulsive disorder (OCD), and major depressive disorder (MDD). The major depressive disorder (MDD) and generalized anxiety disorder (GAD) subscales consist of 10 and 6 items, respectively. Respondents rated how often each item on the subscales applied to them using the four-point Likert scale corresponding to: 1 –never, 2 –sometimes, 3 –often, and 4 –always. Scores on the subscales were obtained by summing the numerical values for the responses to the items for each subscale. Higher scores signified greater depressive and anxiety symptomatology. The RCADS has been found to have acceptable reliability and validity when used with various types of samples (Chorpita et al., 2005; Esbjørn et al., 2012). The scale has been used in research with samples from a variety of countries and has internal consistency reliabilities ranging from 0.86 to 0.97 for the generalized anxiety disorder (GAD) subscale and 0.77 to 0.98 for the major depressive disorder (MDD) subscale (Piqueras et al., 2017). The internal consistency reliabilities of the MDD and GAD subscales for this study were 0.83 and 0.84, respectively.
Pediatric Quality of Life in Neurological Disorders (Pediatric Neuro-Qol)
The levels of depressive and anxiety symptoms of the study participants were also measured using the short forms of the depressive and anxiety scales of the Pediatric Quality of Life in Neurological Disorders measurement system (Pediatric Neuro-Qol; Lai et al., 2012). Like the Revised Children’s Anxiety and Depression Scale (RCADS), scores on these subscales were expected to be moderately and positively related to scores on the generic stigma measures if the stigma measures have predictive validity. The Pediatric Neuro-Qol measurement system is an item bank that was developed for children with neurological disorders. It comprises both generic and targeted scales. The generic scales include brief scales for anxiety symptoms, depression symptoms, anger, interaction with peers, fatigue, pain, applied cognition, and stigma. The short forms of the depression and anxiety scales consist of eight items each. Respondents rated how often they experienced each item in the past 7 days using the five-point Likert scale corresponding to 1 –never, 2 –almost never, 3 –sometimes, 4 –often, and 5 –almost always. The response option ‘almost never’ was changed to ‘hardly’ for the current study after think-aloud interviews. Scores on the scales were obtained by summing the numerical values for the responses to each scale’s items. Higher scores signified greater depression and anxiety symptoms. The Pediatric Neuro-Qol measurement system has been used in studies with various samples and has been found to have acceptable internal consistency reliabilities ranging from 0.85 to 0.94 for the depression scale, and from 0.76 to 0.91 for the anxiety scale (Beckmann et al., 2018; Lai et al., 2015). The internal consistency reliabilities of the scales for this study were 0.86 for the depression scale and 0.81 for the anxiety scale.
Short Form Children’s Social Desirability Scale (S-CSDS)
Social desirability was assessed using the Short Form Children’s Social Desirability Scale (S-CSDS; Miller et al., 2014). Measurement of social desirability was intended to help establish discriminant validity of the generic stigma measures. For discriminant validity, it was expected that the correlation sizes between scores on the S-CSDS and the generic stigma measures should be much lower than the correlation sizes between scores on the predictive scales and those on the generic stigma measures. The S-CSDS is a 14-item scale that assesses an individual’s tendency to present themselves in favorable ways. Individuals respond to the items as ‘yes’ or ‘no’. Items with statements indicating a greater tendency for a socially desirable response are each rated 1 and items with statements indicating less of a tendency for a socially desirable response are each rated 0 (Miller et al., 2014; Vogel et al., 2006). Scores on the scale are obtained by summing numerical values for the responses to the items and range from 0 to 10. Higher scores on the scale indicate greater social desirability in the participants’ responses. The scale has been used in research with samples of a variety of ages and is known to have acceptable internal consistency reliability ranging from 0.82 to 0.85 (Miller et al., 2014). The internal consistency reliability of the scale for this study sample was 0.77.
The Revised Child Manifest Anxiety (RCMAS) – Lie Subscale 1
Social desirability was also assessed using the Lie subscale 1 of the Revised Children’s Manifest Anxiety Scale (Reynolds & Richmond, 1978). Like the S-CSDS, this scale was also administered to the study participants to support establishing the discriminant validity of the generic stigma measures, and the sizes of the correlations between scores on the RCMAS Lie Scale 1 and the generic stigma measures were expected to be weaker than that between the predictive scales and the generic stigma measures if the stigma scales have discriminant validity. The Revised Children’s Manifest Anxiety Scale (RCMAS) is a 37-item measure of anxiety for children and adolescents 6 to 19 years old (Reynolds & Richmond, 1978). The scale comprises 4 subscales: a 28-item total anxiety index across 3 subscales and a nine-item Lie scale. Respondents indicate yes (1) or no (0) to each item on the scale. The RCMAS Lie subscale 1 comprises six of the nine items. The subscale is scored by summing the numerical values of the responses. The internal consistency reliability of the entire nine-item scale was found to be 0.77 in previous research (Statistics Solutions, 2019). The internal consistency reliability of the six-item scale for the current study was 0.68.
Procedure
Ethical approval was obtained for the multi-phase research for the development of the generic stigma measures from The University of the West Indies, Mona Campus Research Ethics Committee (MCREC) (#ECP 200, 13/14) and the Southeast Regional Health Authority (SERHA) Institutional Ethics Committee of the Ministry of Health & Wellness, Jamaica (Approval obtained on February 12, 2015). In addition, approvals were obtained from the relevant authorities in the hospitals and clinics where study participants were recruited.
Eligible adolescents and their parents were identified during their visits to their various clinics or from service records or client databases with the help of the care staff working with the various institutions. All potential adolescents or their parents were informed about the study and asked if they would like to take part. If they agreed, the adolescents’ awareness of their diagnoses and other inclusion criteria was confirmed. Parental informed consent and youth informed assent were obtained for participants under 18 years old and youth informed consent was obtained for those participants 18 years and older. Adolescents were interviewed in the clinics where they were recruited (110 interviews), at other locations (4 interviews), via telephone (55 interviews) or using the video or voice conversation features of various social networking platforms (i.e., WhatsApp, Facebook Messenger or Skype; 20 interviews). To facilitate the establishment of the test-retest reliability of the generic stigma measures, 30 adolescents were invited to respond to the measures 2 weeks later. The duration of the interviews ranged from 30 min to 1 hr.
Data Analysis
The data collected were entered into and analyzed using Statistical Package for the Social Sciences (SPSS) version 22. The data were cleaned using SPSS Frequencies. Problems with univariate outliers, implausible values, and missing values were also checked for each variable and addressed as necessary. The missing values for each item on each scale were replaced using mean substitution.
Assessment of the psychometric properties of the new stigma measures was done in several steps. First, a series of exploratory principal component analyses using orthogonal (varimax) and oblique rotations were conducted separately for each new measure. A series of criteria were used to determine the best solution for a new scale (Tabachnick & Fidell, 2013). These criteria included scree plots, eigenvalues greater than one, the total percentage of the variance accounted for, simple structure, and the meaningfulness of the components resulting from the analysis process. Once the structure of each new measure was identified, the internal consistency reliability of each measure and its subscales was estimated. Pearson’s product-moment correlations were then calculated to estimate the concurrent and discriminant validity of each stigma scale and each subscale.
Results
Preliminary Analysis
The results of the descriptive analysis for the items making up the 3 generic measures revealed that only 7 of the 72 items making up the 3 measures had missing data. The missing data existed for one or two cases per item, so this was substituted with the item’s mean value, since the missing data was below 10% of the sample (Tabachnick & Fidell, 2013). Additionally, none of the items required transformation or removal.
Assessment of the Psychometric Properties of the New Stigma Measures: Principal Components Analyses
Internalized Stigma Measure
The initial principal component analysis using orthogonal (varimax) rotation for the 33 items included in this measure produced eight components with eigenvalues greater than one. However, a review of the scree plot of eigenvalues suggested that four components should be kept. A four-component principal component analysis using orthogonal rotation was conducted. An inspection of the rotated component loading matrix revealed that several items were loaded on more than one component, suggesting that the components may be correlated. A four-component principal component analysis using oblique rotation was then conducted. The results of this analysis found that some of the items did not load on only one component in the rotated structure and the pattern matrices. Consequently, the four-component solution using oblique rotation was repeated, removing items that did not load clearly on one component in an iterative process until four distinct components resulted. Of the 33 items that comprise the Internalized Stigma Scale, 7 items were removed. The final four components explained 49.4% of the total variance and are shown in Table 2. The first component, which was labeled as Feeling of or Desire for normalcy, accounted for 25% of the variance and consisted of eight items. An example of an item from this component was ‘You felt sorry that you have condition’. The second component, which was related to Secrecy, accounted for 10.4% of the variance and consisted of eight items. An example of an item from this component was ‘You kept it a secret from someone that you have condition’. The third component, which represented Reactions to negative treatment from others, accounted for 8.4% of the variance and consisted of five items. An example item from this component was ‘You stopped talking to someone because of how they reacted’. The fourth component, which represented Feeling isolated or ostracized, accounted for 5.7% of the variance and consisted of five items. An example item from this component was ‘You felt left out because of your condition’. Supplemental Table A in the Supplemental Appendix presents the components or sub-scales derived from the Principal Component Analysis, the number of items loading onto each component/sub-scale, an example item that measures each component or sub-scale, and illustrative quotes across illness from the qualitative study that influenced the development of the specific item, thereby clearly establishing the empirical basis for the item’s content.
Rotated Pattern Component Loading Matrix from Principal Component Analysis of Items Comprising the Internalized Stigma Measure.
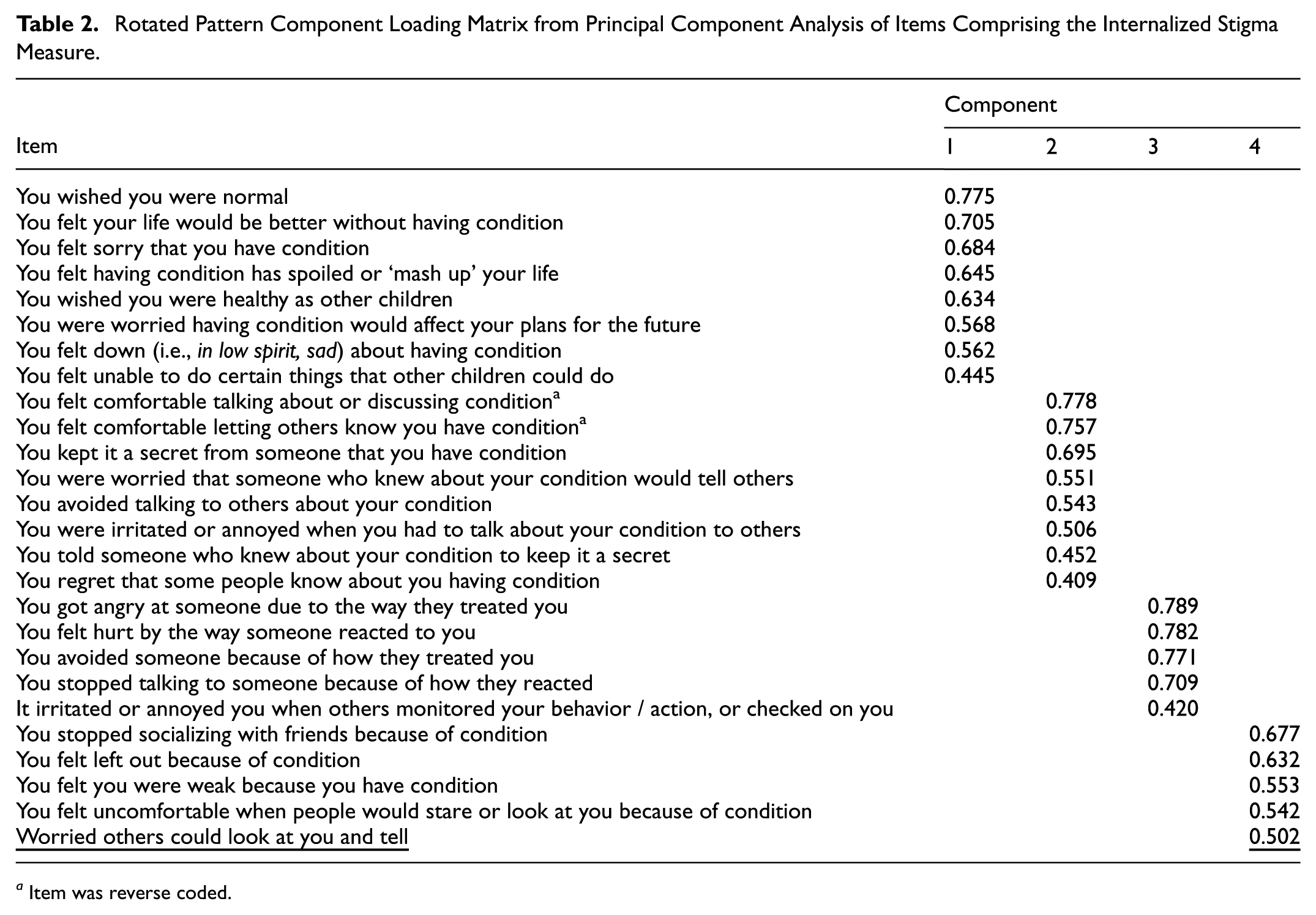
Item was reverse coded.
Perceived Stigma Measure
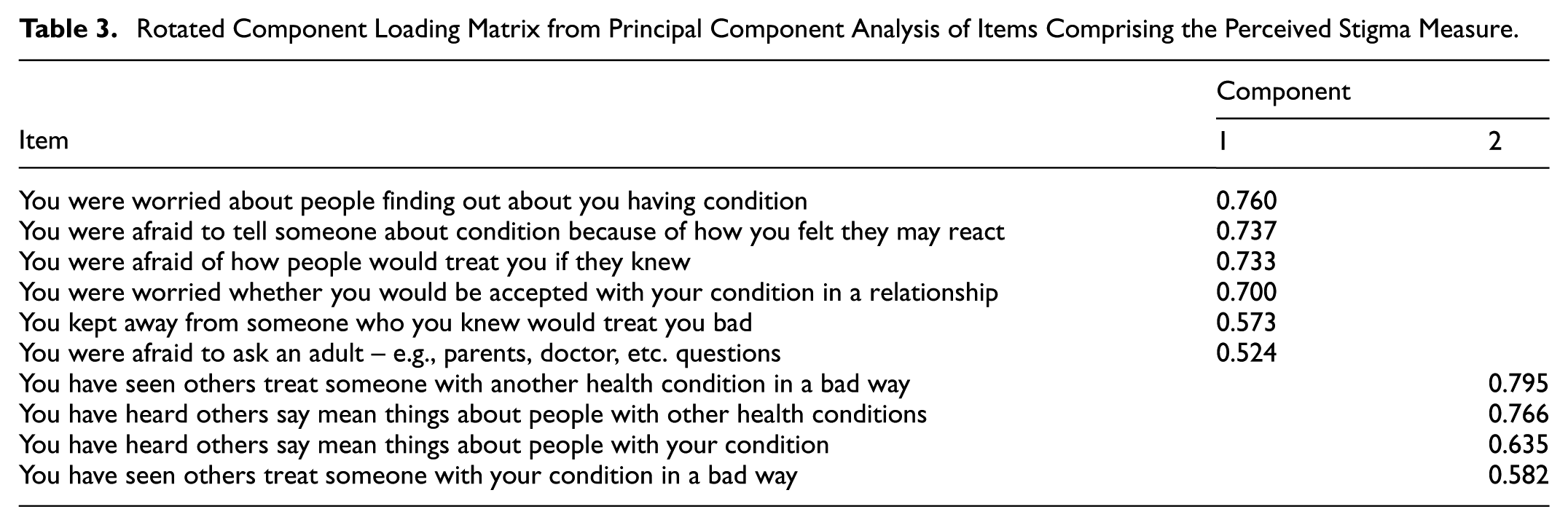
The initial principal component analysis using varimax rotation for the 10 items that make up the measure revealed three components. However, a number of the items on component one were cross-loaded on component two, suggesting a possible correlation of components. Consequently, a principal component analysis using oblique rotation was then performed and revealed that the components were not substantially correlated. Furthermore, components two and three had two items each, with the loading values for component two being positive and that for component three being negative, suggesting that components two and three were assessing the same construct. Therefore, a two-component principal component analysis was performed using varimax rotation. The two components fit the data well, accounting for 53.1% of the total variance (Table 3). The first component accounted for 37.9% of the variance and consisted of six items that was labeled Expectation of negative treatment. An example item from this component was, ‘You were afraid to tell someone about your condition because of how you felt they may react’. The second component accounted for 15.2% of the variance, consisted of four items, and was named, witnessed negative treatment of others. An example item from this component was, ‘You have heard others say mean things about people with your condition’. Supplemental Table B in the Supplemental Appendix presents the components or sub-scales derived from the Principal Component Analysis, the number of items loading onto each component/sub-scale, an example item that measures each component or sub-scale, and illustrative quotes across illness from the qualitative study that influenced the development of the specific item, thereby clearly establishing the empirical basis for the item’s content.
Rotated Component Loading Matrix from Principal Component Analysis of Items Comprising the Perceived Stigma Measure.
Enacted Stigma Measure
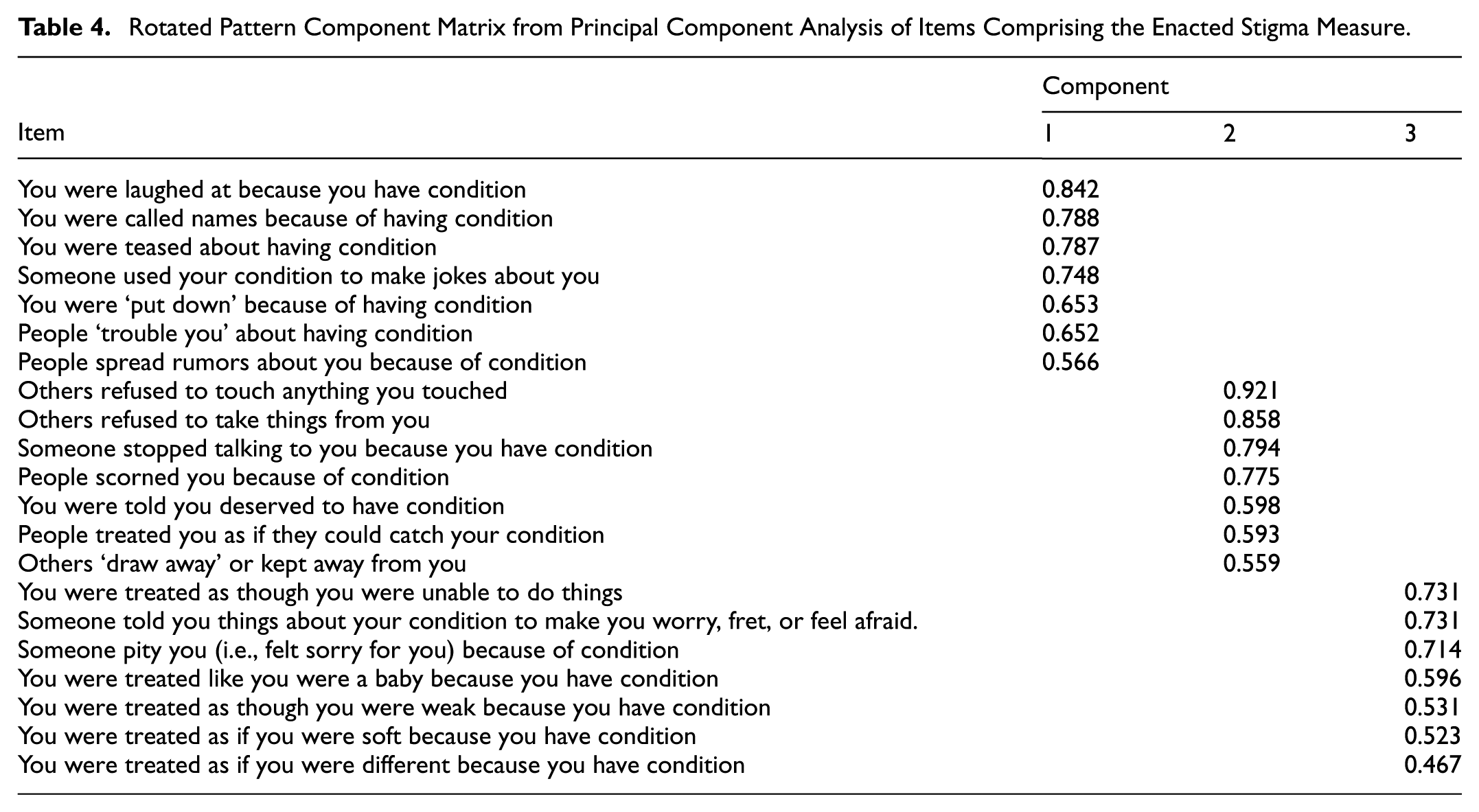
The initial principal component analysis using varimax rotation for the 29 items that make up the measure revealed six components; however, a review of the scree plot and the eigenvalues revealed that the number of components could be less. Consequently, three, four and five-component solutions using both varimax and oblique rotations were explored. These revealed that the four-component solution using oblique rotation had the best combination of the criteria for a solution. However, several of the items did not clearly load on only one component in both the rotated structure and the pattern matrices. So, the four-component solution using oblique rotation was repeated, removing items that did not clearly load onto one component in an iterative process until four distinct components resulted. However, while four clear components were generated, only three could be clearly interpreted. As such, the items for the fourth component were dropped in a further analysis. This refined analysis resulted in three clear components. Of the 29 items that comprise the enacted stigma scale, 8 items were removed. The three components accounted for 58.0% of the total variance and are shown in Table 4. The first component accounted for 38.4% of the variance and consisted of seven items that was labeled Mock. Included in this component were items, such as ‘You were teased about having condition’, and ‘You were called names because of having condition’. The second component accounted for 13.2% of the variance and consisted of seven items that pertained to being scorned. Examples of the items included in this component were ‘People scorned you because of condition’ and ‘You were told you deserved to have condition’. The third component accounted for 6.4% of the variance and consisted of seven items that represented being Treated as weak. An example item from this component was ‘You were treated as though you were unable to do things’. Supplemental Table C in the Supplemental Appendix presents the components or sub-scales derived from the Principal Component Analysis, the number of items loading onto each component/sub-scale, an example item that measures each component or sub-scale, and illustrative quotes across illness from the qualitative study that influenced the development of the specific item, thereby clearly establishing the empirical basis for the item’s content.
Rotated Pattern Component Matrix from Principal Component Analysis of Items Comprising the Enacted Stigma Measure.
Reliability
The internal consistency of the items making up each stigma measure overall as well as for the components underlying each scale are shown in Table 5. All the values were above 0.70, the value considered acceptable for a measure to be used in research (Nunnally, 1975). The test-retest reliability of the measures and their subscales was acceptable with test-retest coefficients ranging from r = 0.74 to 96 (Table 5).
Internal Consistency and Test-Retest Reliability Coefficients of Stigma Measures and their Components.
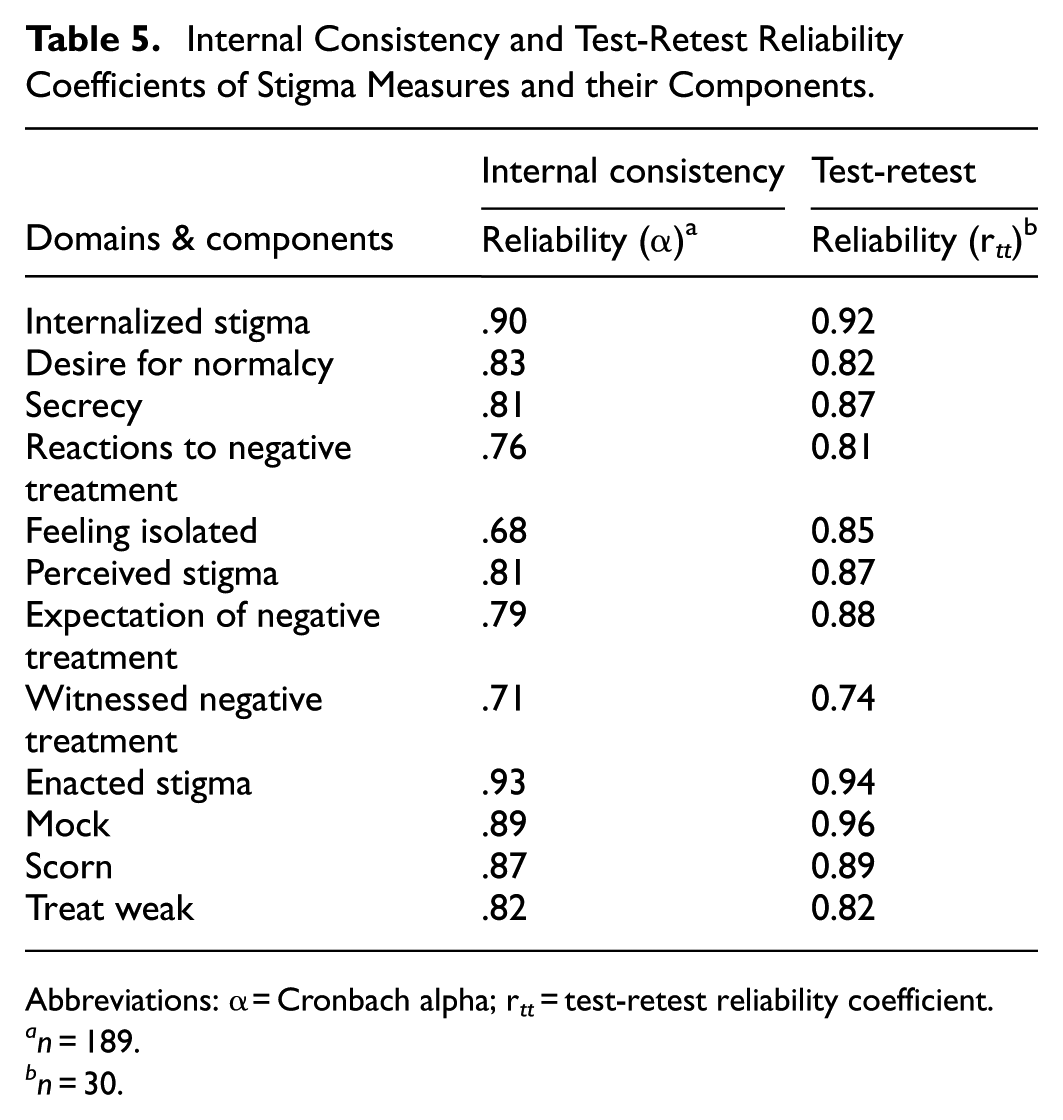
Abbreviations: α = Cronbach alpha; r tt = test-retest reliability coefficient.
n = 189.
n = 30.
Construct Validity
The evidence for the construct validity was based on the predictive and discriminant validity of the measures. For predictive validity, it was expected that adolescents’ scores on the generic measures of stigma should correlate with their scores on the measures of self-esteem, self-efficacy and symptoms of depression and anxiety, while for discriminant validity, it was expected that adolescents’ scores on the generic measures would have weaker correlations with their scores on the measures of social desirability.
As expected and supporting predictive validity, with some small exceptions, the adolescents’ scores on the stigma measures and their components were negatively and moderately correlated with their scores on the self-esteem scale, and positively and moderately correlated with their scores on the symptoms of depression and anxiety scales (Table 6). The exceptions to this pattern of scores occurred for the Witnessed negative treatment component of the Perceived stigma measure, where the sizes of the predicted relationships were smaller than expected. Contrary to the predictions as well, only some of the adolescents’ stigma scores correlated negatively with their scores for self-efficacy. The discriminant validity of the stigma measures and their components was supported through weaker correlations of the adolescents’ scores on these measures with their scores on the two measures of social desirability.
Predictive and Discriminant Validity for the Generic Stigma Measures and Components.
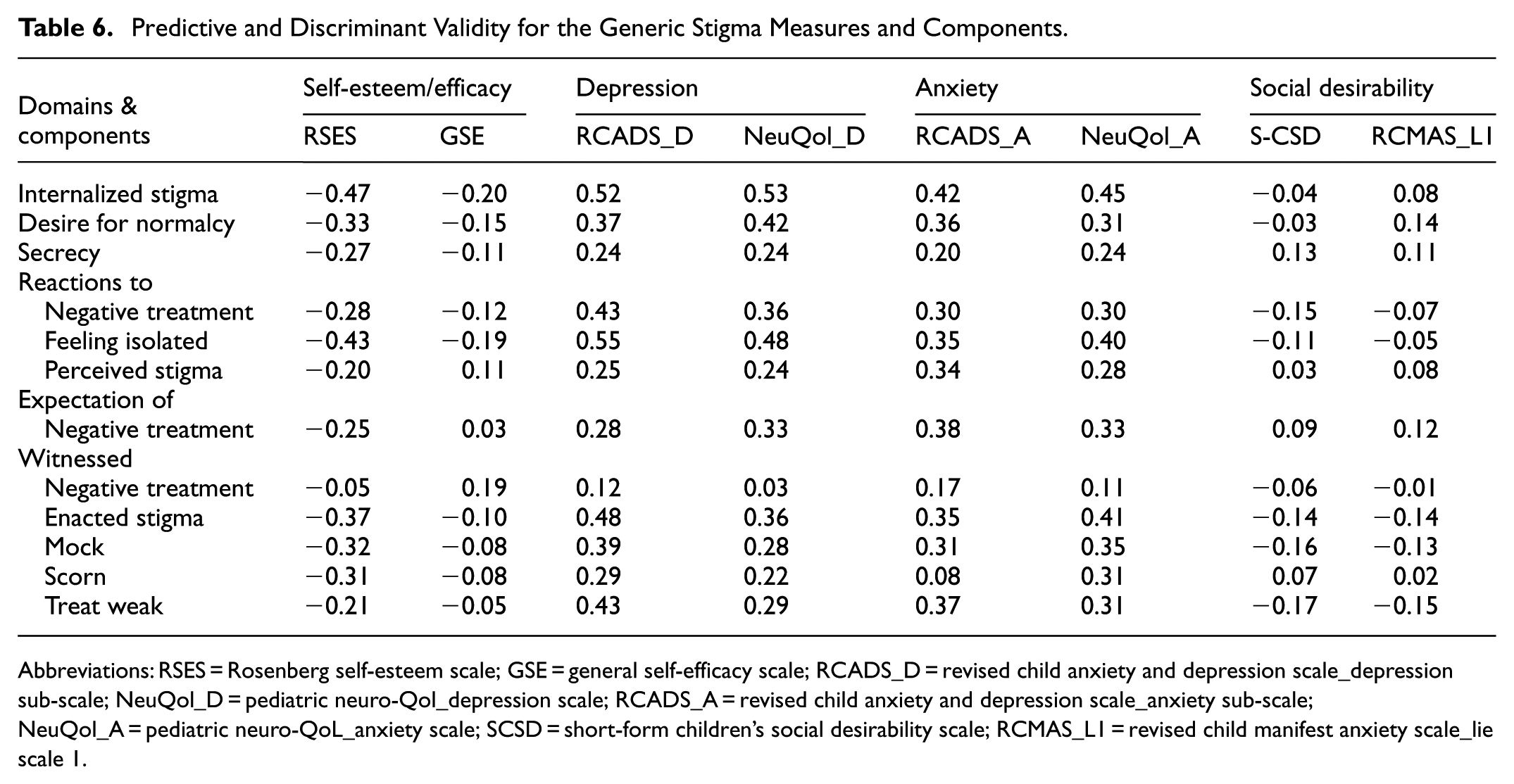
Abbreviations: RSES = Rosenberg self-esteem scale; GSE = general self-efficacy scale; RCADS_D = revised child anxiety and depression scale_depression sub-scale; NeuQol_D = pediatric neuro-Qol_depression scale; RCADS_A = revised child anxiety and depression scale_anxiety sub-scale; NeuQol_A = pediatric neuro-QoL_anxiety scale; SCSD = short-form children’s social desirability scale; RCMAS_L1 = revised child manifest anxiety scale_lie scale 1.
Discussion
This study sought to assess the psychometric properties of generic measures of internalized, perceived and enacted stigma that were developed from commonalities in adolescents with various illnesses lived experiences. As indicated in the literature review, past research has indicated that commonalities exist across illnesses and hence there is a need for generic measures (van brakel, 2006; van Brakel et al., 2019). While generic measures have been created for adults, no such measures have been developed for adolescents.
Principal component analyses identified several subscales that could be constructed within each measure. The subscales identified underlying the Internalized stigma measure included Desire for normalcy, Secrecy, Reactions to negative treatment, and Feeling isolated. Those identified underlying the Enacted stigma measure included being Mocked, Scorned, and Treated as weak; and those underlying the Perceived stigma measure included Expectation of negative treatment and Witnessed negative treatment. Many of these areas measured by the subscales identified within the different stigma measures represent important areas for the forms of stigma that have been noted in the literature and hence provide some evidence for the construct validity of the measures (Berger et al., 2001). A number of the areas are also relevant to adolescents’ social development, thus providing support for the construct validity of the scales (Berger et al., 2001). Adolescent social development includes striving for a sense of self-worth and independence, developing peer relationships, and wanting to be accepted by peers (Kroger, 2007; Sanders, 2013). Experiencing an illness, by its very nature, sets adolescents apart from their peers. Consequently, issues of normalcy, secrecy, isolation, and expectation of and reactions to negative treatment also become salient as adolescents’ management of their illness will be at odds with their normal developmental strivings (Holmbeck, 2002; Suris et al., 2004).
Further support for construct validity was found through evidence for the predictive and discriminant validity of each of the three stigma measures and their subscales. Evidence for predictive validity was found through the expected negative correlation of scores on the measures with scores for self-esteem, and positive correlation with scores for depression and anxiety symptoms. Evidence for the discriminant validity of the stigma measures was found through weaker correlations between scores on the stigma measures and the measures of social desirability than between scores on the stigma measures and the measures of self-esteem, and depression and anxiety symptoms.
Contrary to expectations, however, the analyses indicated that only some of the adolescents’ stigma scores correlated negatively with their scores for self-efficacy. This finding may have occurred for one of two reasons. First, there is a conceptual distinction between the constructs: the experience of stigma is primarily an emotional response rooted in social interaction, while self-efficacy represents a cognitive estimation of one’s ability to successfully carry out an action or achieve a goal. A relationship between the experience of stigma and the broad perception of agency may therefore not be as direct as expected. Second, the measure used in the study assessed generalized self-efficacy, which reflects a global perception of control rather than self-efficacy specific to illness management or social interaction. This suggests that the generalized perception of control may be more robust against the effects of social stigma than domain-specific efficacy. Furthermore, this finding may point to a complex relationship mediated by cultural protective factors. As parental support is prevalent in the Jamaican culture (Brown & Chevannes, 1998), it may help adolescents maintain a strong, generalized sense of personal agency despite experiencing stigma. This suggests that stigma may not penetrate and undermine the core generalized self-efficacy of these adolescents as severely as predicted by models developed in different cultural contexts, offering a valuable avenue for future cross-cultural research.
The reliability of the stigma measures was also supported. The internal consistency reliability of each measure overall as well as its components (subscales) was acceptable, with most values surpassing the 0.7 benchmark (Nunnally, 1975). The Feeling isolated component of the Internalized stigma measure was the exception, as its score was slightly below the benchmark. There was also high test-retest reliability of the stigma measures and their components, suggesting that the scores are stable over time.
The measures developed are the first known generic measures for the stigma of chronic illnesses in adolescents. Additionally, the three measures were designed using adolescents’ lived experiences of the stigma forms due to their illnesses rather than adapting measures designed for adults to use with adolescents. As adolescents experience different social environments as well as different developmental challenges from adults, it is likely their experience of internalized, perceived and enacted stigma will be different (Deacon & Stephney, 2007). As such, measures that have been adapted from adult measures may miss specific aspects or manifestations of the forms of stigma experienced by adolescents. The three measures developed in this study will enable researchers to better capture and compare the forms of stigma experienced by adolescents across different health conditions as well as across the different forms of stigma.
Implications for the Theoretical Framework
The results of this study confirm several central predictions of stigma theory regarding the impact of stigma on psychosocial health. Specifically, our data showed that the more adolescents reported experiencing the different forms of individual-level stigma, the lower their self-esteem and the higher their symptoms of depression and anxiety, aligning with established theoretical models. This finding provides strong evidence for the universality of the linkages between stigma exposure and negative self-perceptions and emotional states across different age groups and illnesses.
Furthermore, the structure of the measures themselves offers important theoretical contributions. The subscales identified within the measures (e.g., Desire for normalcy, Secrecy, Reactions to negative treatment in internalized stigma, and Expectation of negative treatment in perceived stigma) represent important manifestations of stigma that have been noted in the literature, as mentioned earlier. These factors, which are salient to adolescent social development (such as striving for self-worth, peer acceptance, and independence), confirm that stigma acts as a powerful barrier by putting their illness at odds with normal developmental strivings.
However, the limited relationship found between the adolescents’ stigma experience and generalized self-efficacy suggests a theoretical boundary condition. While the stigma theory predicts an erosion of personal agency, the data indicate that this effect may not penetrate the generalized perception of control in this population. This nuance suggests that future theoretical refinement should prioritize testing domain-specific self-efficacy (e.g., illness-management efficacy) over generalized measures and consider the role of strong familial support as a potential buffer that preserves a global sense of agency.
Originality and Contributions of the Research
This research is original and contributes significantly to the research of health-related stigma among adolescents in four primary ways. First, the scales are the first known generic chronic illness stigma scales specifically developed for adolescents. This directly answers the long-standing call in the literature for the development of generic scales (van Brakel, 2006; van Brakel et al., 2019). While such scales exist for adults, hardly any exist for adolescents, with the Child Attitude Toward Illness Scale (CATIS) being the only other relevant generic measure, which assesses attitudes rather than experienced stigma (see review in van Brakel, 2006).
Second, the research has developed three illness stigma scales based on adolescents’ lived experiences and viewpoints. Only a few existing studies have incorporated adolescents’ lived experience in this way (e.g., Austin et al., 2004).
Third, the scales developed in this study avoid the pitfalls of existing stigma research with adolescents, which mostly utilizes scales developed for adults and then adapted for youth. As adolescents face different social environments and developmental challenges from adults, measures adapted from adult tools may miss specific aspects or manifestations of stigma unique to this age group.
Fourth, the three measures will enable researchers to better capture and compare the forms of stigma experienced by adolescents across different health conditions (cross-illness utility) as well as across the different forms of stigma themselves (internalized, perceived, and enacted).
Limitations and Recommendations for the Future
Although the study has found evidence for the reliability and validity of the three stigma measures that were developed, there were limitations with the methodology that need to be highlighted. The scales have been developed using adolescents who were able to conceal their health conditions. As such, the measures may not be suitable for use with all types of health conditions, both those that are easily concealed and those that are not. Thus, the measures created may not contain all the possible common stigma experiences that adolescents with different health conditions may experience. It is recommended that future research explore whether the measures can be used with adolescents who have non-concealable illnesses.
The study responded to a call for generic measures, specifically in terms of cross-illness applicability—the ability to measure stigma commonly experienced across various chronic health conditions. While it demonstrated this cross-illness utility, it is critical to note that this does not imply cross-cultural universality. The study used a sample of adolescents from Jamaica, and as such, the measures may not be directly applicable or fully representative of adolescents with stigmatizing health conditions in other countries and cultures. How Jamaican adolescents experience and express stigma might be influenced by Jamaica’s unique cultural context (e.g., gender and gender roles and types of parental involvement; Brown & Chevannes, 1998; Green, 2017).
Gender and gender roles may have significantly influenced adolescents’ experiences and expression of stigma. In Jamaican culture, males and females are socialized to adopt more traditional gender roles. For example, males are socialized to be rough and tough, physically strong, sexually dominant and the breadwinner of the family. In contrast, females are taught to be ladylike, soft and gentle, and modest in their sexual behaviors as well as to love and care for the family (Green, 2017). These traditional expectations may amplify the feeling of internalized stigma for male adolescents whose illness conflicts with the ‘tough’ ideal, or for female adolescents who must balance social expectations with the vulnerability associated with their condition.
Parental involvement in adolescents’ lives may also have limited the generalizability of the findings. Unlike other societies, in Jamaica, parents tend to remain highly involved in their adolescents’ lives, up to and beyond adulthood. This is manifested by actions such as driving their adolescents to school, being highly involved in their education, meeting with teachers, and attempting to protect their adolescents from negative experiences, especially for female adolescents. (Brown & Chevannes, 1998). This high level of parental protection may provide a strong buffer against experiencing stigma or influence the way stigma is perceived, leading to a different profile of stigma than found in cultures where adolescents have greater autonomy or less protective familial support. Therefore, more research is needed using adolescents in other cultures who have stigmatizing health conditions to fully assess the cross-cultural applicability of these measures.
Additionally, the generic measures of stigma developed in this study are essentially designed for use with adolescents. As such, they may not be generalizable for use with pre-adolescents and younger children. Future research should examine whether these scales can be used with younger age groups or if scales specifically designed for children need to be developed.
Conclusions
The three generic measures of individual-level stigma that have been created using the experiences and viewpoints of adolescents with different illnesses were found to be reliable and valid measures and proved useful in differentiating the stigma experiences of adolescents with varying health conditions. The measures may be used in future studies to capture the experience of stigma at the individual level of adolescents with a variety of illnesses. The current research demonstrates that the combination of qualitative and quantitative research approaches can lead to the development of high-quality measures.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440261452310 – Supplemental material for Development and Validation of Generic Measures of Individual-Level Stigma for Adolescents With a Chronic Illness
Supplemental material, sj-docx-1-sgo-10.1177_21582440261452310 for Development and Validation of Generic Measures of Individual-Level Stigma for Adolescents With a Chronic Illness by Joan A. Thomas and Garth E. Lipps in SAGE Open
Footnotes
Acknowledgements
We wish to thank all the research participants and their parents. We are very grateful that they allowed us the opportunity to learn about their experiences with their various illnesses. We also wish to thank you also to the doctors and staff at the clinics and various other sites where the research was conducted for their kind support with accessing participants.
Ethical Considerations
Ethical approval was obtained from The University of the West Indies (UWI), Mona Campus Research Ethics Committee (#ECP 200, 13/14; approval obtained July 8, 2014) and the Southeast Regional Health Authority (SERHA) Ethics Committee of the Ministry of Health and Wellness in Jamaica (approval obtained February 12, 2015).
Consent to Participate
Parents provided written informed consent, and the youth provided written informed assent or consent prior to the data collection.
Author Contributions
All authors of the paper have seen, reviewed and approved this manuscript. Dr. Thomas and Professor Lipps were involved in the conception and planning of the research project. Dr Thomas collected the data. We both conducted the statistical analyses of the data and interpreted the findings, and wrote, reviewed and approved the paper for this submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data for this study are available in an anonymized format upon reasonable request from the corresponding author*.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.