
Abstract
Incidence rates of childhood overweight and obesity continue to grow in the United States, threatening children’s health and social development. The aim of this study was to explore how patient-centered care (PCC) at individual and system levels can influence children’s physical, mental, and social well-being. Using the National Survey on Children’s Health (NSCH), data were drawn from 4,045 parents of children aged 6 to 17 who were overweight or obese and had seen a doctor in the past year. Parents reported their child’s adverse childhood experiences (ACEs), difficulty paying medical bills, PCC, system of care, expression of weight concerns, physical activity, forgone mental healthcare, and ability to make friends. Structural equation modeling tested whether PCC mediated the effects of social determinants of health on physical, mental, and social outcomes. Unaffordable medical bills and ACEs significantly worsened children’s mental, physical, and social outcomes. Both system-level and interpersonal PCC mediated these effects. A well-functioning healthcare system predicted greater physical activity, while interpersonal PCC predicted increased use of mental healthcare, improved physical activity, and fewer difficulties making friends. However, provider expression of concern about overweight status was associated with reduced physical activity. PCC and system-level support enhance children’s well-being but cannot fully offset adverse environments. This shows the urgency of addressing broader social determinants. Providers should attend to children’s needs and avoid relying solely on weight-focused messaging, which may inadvertently harm physical activity and social adjustment.
Plain Language Summary
Study using parent reports from a national U.S. survey to better understand how patient-centered care and healthcare systems influence the well-being of children who are overweight or obese.
Keywords
Introduction
Incidence rates of overweight and obese individuals continue to grow in the United States. Children are no exception, with obesity rates growing from 5% in 1978 to 18.5% in 2016 (Anderson et al., 2019). Pre-pandemic data from the National Health and Nutrition Examination Survey in 2017 to 2020 indicated that obesity prevalence is 20.7% among 6 to 11 year olds and 22.2% among 12 to 19 year olds (Bryan et al., 2021). Current estimates are likely higher, as the upward trajectory of obesity rates was exacerbated by the COVID-19 pandemic (Hauerslev et al., 2022). Obesity has high health, social, economic, and personal costs (Swinburn et al., 2011). Adverse social circumstances, which are often captured through social drivers/determinants of health (SDH) or adverse childhood experiences (ACEs), demonstrate the depth of the problem by highlighting the systemic dynamics limiting advancement of improving health outcomes (Kumanyika, 2019, 2022). Consequently, overweight and obese children may often experience bullying and trouble making friends (Cheng et al., 2022; Ettekal et al., 2019; Haqq et al., 2021; Harrist et al., 2016). In the aftermath of COVID-19, where research shows increasing incidences of mental health issues among children and adolescents, these effects may be amplified (Oliveira et al., 2022).
Patient-centered communication (PCC) is shown to mitigate many health equity issues, with calls for improvements toward equitable care across multiple facets of the healthcare system including patient-centered medical homes (Wong et al., 2012). Family communication has also been found effective in improving the resilience and health outcomes of children (Downing, 2024; Wu & Brannon, 2024a). However, there is a lack of research examining how the social and clinical contexts interact to affect overweight and obese children’s health outcomes. Therefore, the aim of this study was to explore how PCC at individual and system levels can influence children’s physical and mental health outcomes, which are essential for individual child development, using nationally representative data. To do so, we utilize the theoretical lens of the ecological model of communication in medical interactions (“the ecological model” thereafter; Street, 2003).
Literature Review
Childhood obesity can increase risks of developing cardiovascular disease, type 2 diabetes, nonalcoholic fatty liver disease, polycystic ovarian syndrome, infertility, asthma, orthopedic complications, psychiatric disease, and increased rates of cancer (Kelsey et al., 2014), as well as reduced academic performance. Research shows that overweight or obese children face higher levels of social exclusion, leading to poorer mental and physical health consequences, which have long-term implications particularly for those who report weight stigma over long (>1 year) periods of time (Haqq et al., 2021; Q. Zhang & Deng, 2024). Causes of obesity are often linked to childhood environments, which are outside of the child’s control (Singh et al., 2010; Vrijheid et al., 2020). Obesity levels may go hand in hand with ACEs, such as parental divorce, incarceration, and domestic violence (Elsenburg et al., 2017).
Yet, SDH, such as inability to afford medical bills, contribute to the increasing childhood obesity rates (Schroeder et al., 2021). Such conditions may influence children’s weight via reduced PA and increased stress response (Elsenburg et al., 2017), generating poorer mental, physical, and social outcomes for obese children (Coley et al., 2015; Crandall et al., 2019). Poor mental and physical health can increase social isolation (Christiansen et al., 2021), as overweight children and those experiencing more ACEs are less likely to make friends (Pierce et al., 2022).
For the well-being of overweight and obese children, early intervention is essential, as current predictions are that more than half of today’s children will be obese as adults (Deal et al., 2020). Considering that the SDHs and ACEs already experienced by children may be hard to change, the goal of this study is to explore how modifiable factors (e.g., clinical communication) may alleviate the negative health impact of SDHs and ACEs.
Theoretical Framework
To break the vicious cycle of detrimental environments to poor health outcomes, we use the ecological model that suggests pathways to better outcomes (Street, 2003). Based on this model, clinical environments may interact with other social environments to produce health outcomes (Street, 2003). Specifically, PCC (exemplified by patient-centered communication) has therapeutic effects in predicting favorable patient outcomes. In an analysis of nationally representative data, PCC played a key role in alleviating the inherent challenges faced by people with low health literacy and socioeconomic status (Wu et al., 2024; Figure 1).
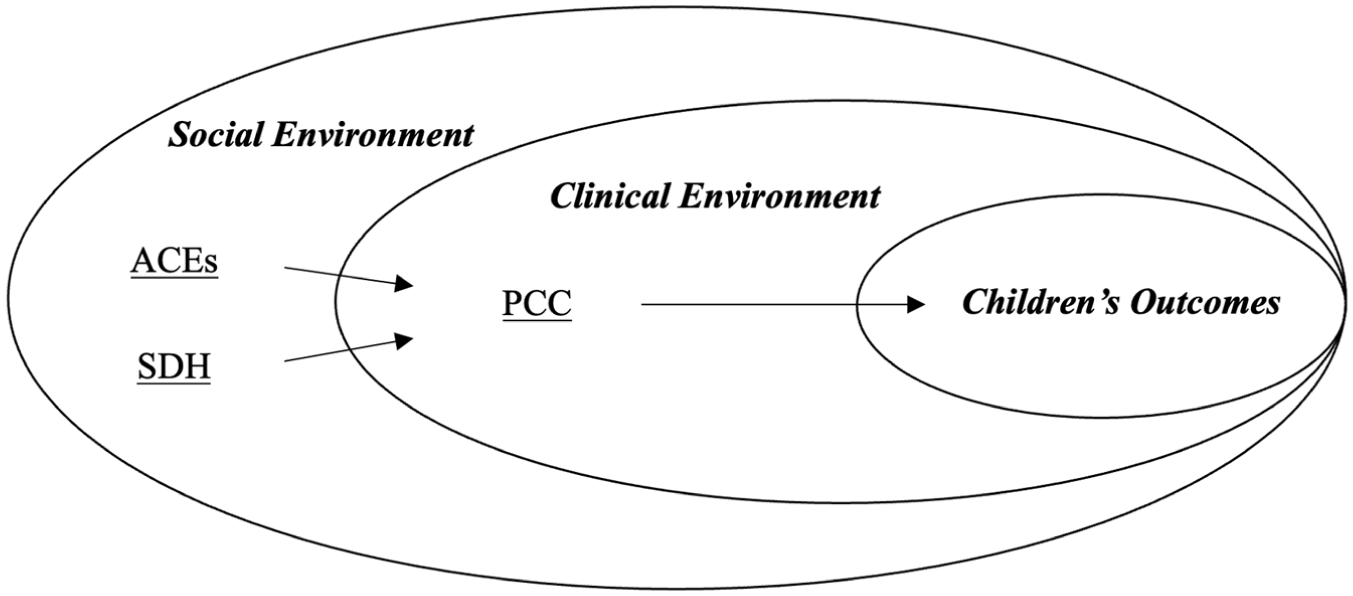
Theoretical framework.
At the individual level, PCC encompasses six functional dimensions: exchanging information, fostering healing relationships, making decisions, managing uncertainty, responding to emotions, and enabling patient self-management (Epstein & Street, 2007). When health care providers demonstrate PCC qualities, patient experiences (DeRosa et al., 2019), preventive service utilization (Kindratt et al., 2020), and treatment outcomes are improved (Hong et al., 2020). PCC is also shown to mitigate health disparities through increased access to affordable care (Langberg et al., 2019), effective information exchange (Mazor et al., 2013), and better self-management (Schlucter, 2014). Following the ecological model, this study examines how promotive factors like PCC may neutralize overweight children’s risk exposure to SDHs and ACEs in a counteractive fashion (Zimmerman, 2013). Patients (especially those with overweight and obesity) may see improvements in physical activity (PA; Wu & Brannon, 2022) and mental help-seeking (Wu & Street, 2025), essential for their social well-being (e.g., less social isolation):
Previous literature explored provider’s expression of overweight concerns in their interactions with overweight and obese (pediatric) patients. An interview study with overweight teenagers reported that teen patients expressed that their providers’ initiating a weight management conversation was important to them regarding weight control (Alexander et al., 2018). Nevertheless, how providers approach such conversations may make a difference. For example, whereas the British government recommended providers use “fat” to motivate patients’ weight control, a survey study with American adults suggested that patients preferred providers’ mentioning “(unhealthy) weight” to “fat/obese” (Puhl et al., 2013). The latter was perceived to convey weight-related stigma, being less motivating than the more neutral “weight” expressions (Puhl et al., 2013). Despite debates over terms providers should use when expressing concerns, research shows a positive association between physician weight discussion and weight loss (Pool et al., 2014). A scoping review of how healthcare professionals discuss more intensive weight management programs found that healthcare professionals working in children’s weight management services in the UK recommended social prescribing, or referring patients to community-based services like peer activities, crafts, and gaming to support pediatric patients who are overweight or obese and their families in efforts to improve physical and mental health outcomes (Garside et al., 2025). Researchers have not explored the impacts of discussing weight on other health outcomes. We probe the effects of such discussions as an example of PCC at the conversation level in the overweight and obese context:
Patient-Centered Care at the System Level
While PCC encompasses both the system- and individual-level, previous literature focused on interpersonal interactions to explore the effects of PCC, demonstrating the centrality of PCC to the patient care experience by examining outcomes such as improved patient satisfaction (Wu & Brannon, 2024a) and odds of receiving all PCC qualities (Kindratt et al., 2022). Expanding on the existing literature to approach equitable care more collaboratively, our study considers the role of a functioning care system as a higher-level component of PCC. A well-functioning pediatric care system includes several elements (Schlucter, 2014), including enhanced access and care continuity, managed care, community support, coordinated care, and the reception of medical and dental preventive care (Wong et al., 2012). For children, involving their family members (e.g., parents or guardians) is vital. The central role of family-centered communication (FCC) in a well-functioning healthcare system is important (Ilango et al., 2021). While there is an increased awareness that managing childhood obesity should involve peers and family members (Garside et al., 2025), evidence linking healthcare and family systems to obese children’s social outcomes (e.g., socializing with peers) remains scarce (Roberts et al., 2021). As it often takes a village to raise a child (Reupert et al., 2022), understanding how systems of care contribute to children’s health and social development is essential. FCC is usually indicated by whether a provider spends enough time with child, listens carefully, is sensitive to family values/customs, gives needed information, and helps the family to feel like a partner in care (Committee on Hospital Care and Institute for Patient- and Family-Centered Care, 2012). Reflecting the national guidelines of Healthy People 2030, (U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, n.d.) overweight and obese children should receive more family-centered, comprehensive, coordinated care to improve health and well-being.
Empirically, components of a well-functioning care system show improvements in pediatric patients’ health outcomes. A healthcare provider’s quality patient/family-centered communication can educate patients on the potential health risks of obesity (Durant et al., 2009). In the context of the NICU, partnership, communication, negotiation, and respect are key for alleviating parental stress and facilitating partnerships between provider and family members (Abukari & Schmollgruber, 2023). FCC is reported to improve patients’ health outcomes and reduce burnout among healthcare providers (Davidson et al., 2017). Continuous health insurance coverage predicted more access to needed care, reducing stress on families (Ilango et al., 2021).
Responding to the national call to provide holistic, 360-degree views on treating patients and collaborating with families (Institute of Medicine (US) Committee on Quality of Health Care in America, 2000, 2001), we consider the system of care as another way (along with PCC) to address the health equity experienced by overweight and obese children:
Social Environments of Patient-Centered Care
While PCC may theoretically and empirically mitigate the negative impacts of adverse environments characterized by SDH and ACEs, ironically, SDH and ACEs further limit the likelihood of receiving quality healthcare, as well. In the aftermath of COVID-19, where research shows increased rates of domestic violence yet lower rates of reporting (Kourti et al., 2023), children may be less likely to access healthcare. For another example, lower income is predictive of reporting lower PCC (Trivedi et al., 2021). Lacking access to affordable healthcare insurance in the United States may also limit children’s access to preventive care, particularly in the endemic COVID-19 era (Khanijahani et al., 2021). An analysis of nationally representative data of children’s health also showed that more ACEs experience predicted lower likelihood of experiencing the indicators of a good system of care (e.g., effective care coordination, having a medical home, shared decision-making; Schweer-Collins & Lanier, 2021). Consequently, children who need comprehensive care the most may not receive good quality of care, let alone that the clinical time constraints may have already restricted providers from engaging in ACEs-related conversations (Halfon et al., 2011), limiting their ability to understand the patient from a more holistic perspective (Branstetter et al., 2020). In turn, negative healthcare experiences can contribute to the increasing rates of overweight or obese individuals (Phelan et al., 2015).
Nevertheless, we consider the limiting effect of SDH and ACEs to explore how PCC at individual and system levels may help alleviate the risks of adverse childhood:

Conceptual model.
Methods
Data and Sampling
This study used nationally representative data from the 2022 National Survey of Children’s Health (NSCH), conducted by the U.S. Census Bureau Department of Commerce from July 8, 2022 through January 20, 2023 (United States Census Bureau, 2024). Using 360,000 address records, NSCH invited adults of US households with children age under 18 to answer questions regarding one of their children’s mental and physical well-being, as well as their healthcare and social needs. With a weighted response rate of 39.1%, 54,103 eligible questionnaires were collected. Our subsample included 4,045 children (aged between 6 and 17) who went to a doctor in the past year and reported being overweight (BMI at or above the 95th percentile of children of the same age and sex; CDC, 2022). As the data is secondary, we were not required to receive approval by the university’s Institutional Review Board.
Measures
The item unaffordable medical bills was measured by a dichotomous variable asking if the respondents’ families had problems paying for child’s medical or health care bills during the past 12 months (0 = No, 1 = Yes; M = .18, SD = .39; Cordova-Ramos et al., 2023).
Adverse childhood experience was measured by a composite of 11 dichotomies asking if the child has experienced the following hardships: (a) low family income; (b) divorce/separation of parents/guardians; (c) death of parents/guardians; (d) incarceration of parents/guardians; (e) witnessing domestic violence; (f) being a victim of domestic violence; (g) living with someone who has mental illness; (h) living with someone who has addiction; (i) racial/ethnical discrimination; (j) discrimination due to disability; (k) discrimination due to gender identity/sexual orientation. The 3-point composite was calculated to reflect the number of adverse childhood experiences, ranging from “0” (no adverse childhood experiences) to “2” (experienced 2 or more adverse childhood experiences; M = .87, SD = .86; Santos et al., 2023).
Patient-centered communication experiences with providers were measured by the mean of eight items reflecting the six functional dimensions of PCC (exchanging information, fostering healing relationships, making decisions, managing uncertainty, responding to emotions, and enabling patient self-management; Epstein & Street, 2007). Participants were asked how often their providers (a) spend enough time with them; (b) listen carefully; (c) show sensitivity; (d) provide specific information; (e) build partnerships; (f) discuss a range of options; (g) are easy to raise concerns or disagree with; (h) conduct shared decision making. Answers were measured on a 4-point scale (1 = Never, 4 = Always). Cronbach α among all items was .945, suggesting excellent scale reliability (M = 3.56, SD = .60; Epstein & Street, 2007; Wu & Brannon, 2024a).
System of care was measured by a dichotomous variable calculated by NSCH using 50 survey questions reflecting six areas of a well-functioning pediatric care system (United States Census Bureau, 2024), including (a) preparation for transition to adult healthcare; (b) having a medical home; (c) receiving medical and dental preventive care; (d) family’s partnership in the child’s care; (e) having adequate and continuous insurance; (f) having no unmet need or barriers to access services. The presence of at least one positive response indicated the child is likely receiving care in a well-functioning system (“1”). Otherwise, the child was considered not having a well-functioning system (“0”; M = .19, SD = .39; Kenney et al., 2022).
Provider’s expression of overweight concern was measured by a dummy item, “Has a doctor or other health care provider ever told you that this child is overweight?” (0 = No, 1 = Yes; M = .40, SD = .49; Limbers et al., 2025).
Forgone mental health care was measured by a dummy item asking if the child was able to receive needed mental health services during the past 12 months (0 = No, 1 = Yes; M = .03, SD = .17; Xu et al., 2025).
PA was measured by, “During the past week, on how many days did this child exercise, play a sport, or participate in PA for at least 60 minutes?” Answers included four levels, “0 days” (“0”), “1–3 days” (“1”), “4–6 days” (“2”), and “every day” (“4”; M = 2.39, SD = .91; Friel et al., 2024).
Difficulty making friends was measured by, “Compared to other children their age, how much difficulty does this child have making or keeping friends?” The answers were assessed by a 3-point scale, ranging from “No difficulty” (“1”) to “a lot of difficulty” (“3”; M = 1.44, SD = .651; Lanza et al., 2023).
Demographic background included sex and general health. Specifically, sex was measured as a dichotomous item (1 = male, 2 = female). General health was assessed by, “In general, how would you describe this child’s health?” The answers were measured on a 3-point scale (1 = fair/poor to 3 = excellent/very good).
Analysis
We tested the hypotheses using STATA 18, using structural equation modeling (SEM). Exogenous variables were unaffordable medical bills and adverse childhood. Endogenous variables were other study variables. All endogenous variables were regressed on the exogenous variables. The outcome variables (forgone mental health care, PA, and difficulty making friends) were also regressed on the PCC items (patient-centered communication, system of care, provider’s informing that the child was overweight). We added a non-directional path between forgone mental care and PA to explain the connection between physical and mental health (Ohrnberger et al., 2017). The model was controlled for sex and general health. Maximum likelihood method was used to estimate path parameters. Following recommendations from previous secondary data analyses, we listwise deleted missing values (Wu et al., 2024; Wu & Brannon, 2022). Kline’s (2015) cutoff indices were used to test the model’s goodness-of-fit. They included Chi-square value (p > .05), root mean square error of approximation (RMSEA < 0.08), comparative fit index (CFI ≥ 0.90), and standardized root mean square residual (SRMR < 0.08).
Results
Demographics
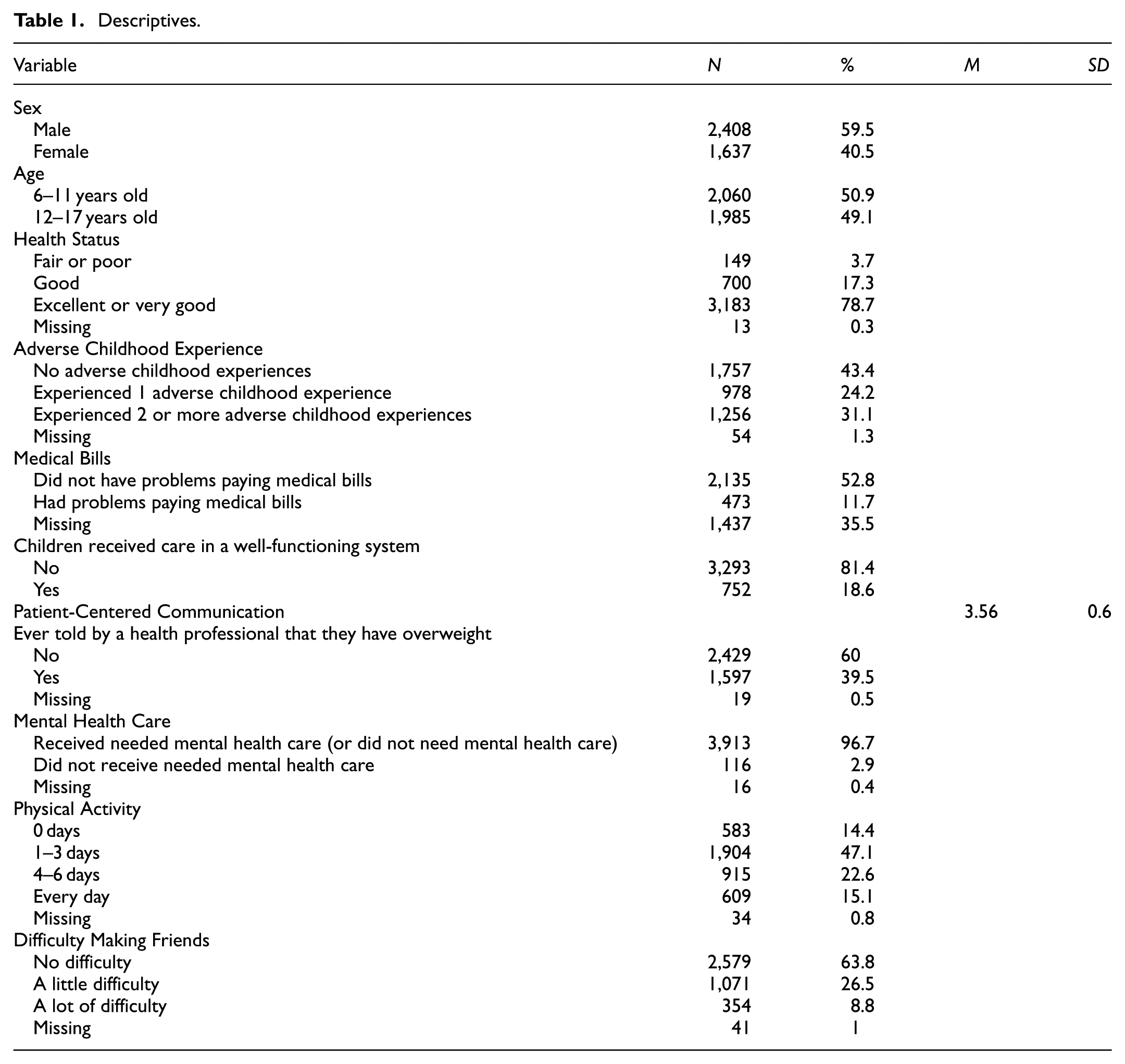
See Table 1 for demographics and descriptives and Table 2 for bivariate analysis. For health status, most children (N = 3,183, 78.7%) reported excellent general health. Notably, 55.3% of the children (N = 2,234) experienced at least one adverse event, and 11.7% reported having problems paying medical bills (N = 473). While the children’s PCC experience was mostly favorable (M = 3.56, SD = .60), only 18.6% reported having a well-functioning medical system (N = 752). Only 2.9% of the children did not receive needed mental health care (N = 116); 37.7% reported exercising at least 60 min a day > 4 days a week (N = 1,524). For social development, 1,425 children reported a little to a lot of difficulty making friends (35.3%).
Descriptives.
Bivariate Analysis.

Note. MB = medical bills; PCC = patient-centered communication; MH = mental health. *p < .05; **p < .01.
Structural Equation Modeling
Since the original SEM model did not generate good model fit (χ2(3) = 119.42, p < .01, RMSEA = 0.124, CFI = 0.923, SRMR = 0.028), we added a path from system of care to PCC to account for the organizational influence on healthcare delivery (Street, 2003). The new model generated an excellent fit (χ2(2) = 5.23, p = .07, RMSEA = 0.025, CFI = 0.998, SRMR = 0.005). Multicollinearity analysis showed that each predictor’s variance inflation factor (VIF) is under 1.3, suggesting very low multicollinearity (Alin, 2010; Figure 3).

Structural equation model.
H1 (Effects of PCC)
More PCC experience was associated with more frequent PA (β = .07, p < .01), less forgone mental care (β = −.09, p < .01), and less difficulty making friends (β = −.07, p < .01). H1 was accepted.
RQ1 (Effects of Provider Weight Discussion)
Provider’s expression of overweight concerns was associated with less frequent PA (β = −.15, p < .01) and more difficulty making friends (β = .08, p < .01). It did not significantly predict forgone mental care (β = −.02, p = .35).
H2 (Effects of a Well-Functioning System)
Patients’ experience with a well-functioning healthcare system was associated with more frequent PA (β = .06, p < .01). It did not predict forgone mental care (β = −.03, p = .12) or difficulty making friends (β = −.03, p = .08). H2 was partially accepted.
H3 (Effects of SDH and ACEs)
More experience with unaffordable medical bills was associated with poor perceived PCC experience (β = −.11, p < .01) and not having a well-functioning care system (β = −.14, p < .01). It did not predict having weight discussion initiated by providers (β = −.02, p = .44).
More ACEs experience was associated with poor perceived PCC (β = −.1, p < .01), not having a well-functioning care system (β = −.07, p < .01), and more likely to have weight discussion initiated by providers (β = .1, p < .01). H3 was partially accepted.
Direct predictors of forgone health care included unaffordable medical bills (β = .06, p < .01) and more ACEs experience (β = .09, p < .01). Direct predictors of difficulty making friends also included unaffordable medical bills (β = .04, p < .05) and more ACEs experience (β = .15, p < .01). A good system of care significantly predicted PCC experience (β = .21, p < .01).
Discussion
The aim of this study was to explore how PCC, experienced by overweight and obese pediatric patients living in adverse conditions, may alleviate the negative impact of the environment and enhance the mental, physical, and social well-being of the patients. Our findings showed the expected positive effects of PCC at individual and system levels. These findings generate theoretical and practical implications for research and clinical interactions. Our study expands on extant literature, considering patient-provider communication and the system of care as a whole to explore how equitable care can be approached in a collaborative way.
Theoretical Implementations
Extending previous research on how PCC may be associated with improved outcomes, this study applied the ecological model to the context of health inequity (Street et al., 2009; Wu & Street, 2022; Zimmerman, 2013). PCC has great potential to address health equity issues by attending to SDH, but scant literature has established PCC’s role (Street et al., 2009). While some recent studies showed association between PCC and increased access to in-person (Wu & Brannon, 2024a) and telehealth care (Wu & Brannon, 2024b), our study considered the detrimental impact of SDH and adverse childhood events on overweight pediatric patients and how PCC may help break the vicious cycle of structural disadvantages. Yet, despite the presence of the PCC factors (e.g., PCC at an interpersonal level, system of care), the negative connection between adverse environments and children’s health is still pronounced (Christiansen et al., 2021; Pierce et al., 2022). This highlights the severity of health disparities and inequities among overweight children experiencing childhood adversities, highlighting the urgency to address it. Outside of the clinical context, researchers recommended family-oriented strategies (e.g., family resilience) to tackle the accumulation of adverse events for overweight children. We approach health equity and disparity from a clinical perspective, suggesting changes at interpersonal and system levels for more favorable outcomes (Heerman et al., 2021).
Interpersonal- and System-Level Patient-Centered Care
At an interpersonal level, our findings align with abundant research linking PCC with improved health outcomes in overweight and general populations. An analysis of nationally representative data showed that higher levels of PCC indirectly predicted overweight and obese patients’ moderate exercise during COVID-19 through more frequent telehealth counseling and use of health-tracking devices (Wu & Brannon, 2022). Another secondary analysis also showed the direct effect of PCC on the general patients’ emotional well-being (Jiang, 2017). Our research confirms how essential it is for healthcare providers to prioritize their communication with patients. Based on the six aspects of PCC we mentioned earlier, providers may work on each aspect to optimize the health outcomes of the pediatric patients who are overweight and obese. This may differ depending on patient (and family), as some families may prefer information exchanges over managing uncertainty. Yet, providers should develop their skills to better facilitate communication with patients and their families.
Providers’ specific expressions of weight concerns for pediatric patients predicted less frequent PA and poorer social outcomes. Internalizing negative messages about weight can affect self-esteem (Fields et al., 2021), which can affect self-efficacy in engaging in specific behaviors (e.g., PA). If providers discuss weight with a negative frame, there could be an increase of weight stigma. Weight stigma is common, with many overweight or obese individuals ascribing negative ideals to themselves, resulting in internalized weight bias (Prunty et al., 2023). Higher levels of peer teasing and lower self-esteem are linked with internalized weight bias among children aged 9 to 18 years (Fields et al., 2021).
Internalizing this stigma can lead to heightened risks of physical health problems (Prunty et al., 2023). It is of importance for providers to learn how they might couch their expressions of weight concerns with appropriate strategies. Providers should learn about eating disorders more broadly to avoid planting seeds of disordered eating behaviors in efforts to help their overweight or obese patients (Nicula et al., 2022). Of importance, research indicates that healthcare professionals are often cautious to discuss weight status with overweight or obese children as they do not wish to provoke disordered eating behaviors (Lampe et al., 2020). Yet, there is little actionable research for healthcare professionals to implement examining the effects of caregivers and healthcare professionals speaking about weight with overweight and obese children.
Poor clinical outcomes and inattentive communication by providers are linked. Parents may perceive their pediatric visits “rushed” if the provider spent too much time discussing the children’s weight (instead of weight-managing strategies; Reyes, 2015). As adverse environments usually go hand-in-hand with childhood obesity (Elsenburg et al., 2017), children’s health conditions may be pronounced to the extent that their providers’ had to focus on the severity of the issue at hand. Even so, to improve the well-being of overweight children who live in adverse environments, healthcare providers can coordinate among colleagues to provide more collaborative care that addresses the children’s social needs beyond their health concerns, thereby integrating the system of care more collaboratively. Collaborative care can neutralize risk exposure of childhood events in a counteractive fashion (Zimmerman, 2013).
From a systematic perspective, our study examined and highlighted the important effects of a well-functioning system of care. Although little research has explored how the system of care may influence the quality of care and health outcomes, a healthcare system that collaborates with the local communities may reduce the disease burden of patients who are limited by SDH (Wong et al., 2012) Previous literature examined the role of isolated organizational factors (e.g., visit length, wait time) on patients’ health-related outcomes. For instance, long wait time at the clinic predicted patients’ dissatisfaction with their care, which is usually associated with poor health outcomes (Chen et al., 2019; Lee et al., 2020). Considering health care as an integrated system, our study suggests that a functioning system may not only enhance the performance of PCC but also offer sustained protection for pediatric health at a structural level (Elsenburg et al., 2017; Reyes, 2015; Zimmerman, 2013).
Practical Implications
For clinical conversations, our model observed negative effects of provider’s expression of overweight concern. This could reflect the problem’s severity, but providers should collaboratively address a child’s health and social needs beyond expressing their concerns. Healthcare practitioners could use techniques centered in PCC beliefs like motivational interviewing to delve into their patients’ obesity-related beliefs (Elwyn et al., 2014). Further, they can discuss collaborative, family-centered communication practices like attitude modeling and behavior modeling with parents and guardians (Lampe et al., 2020). Promoting collaborative physical activities for a family may improve a patient’s willingness to adopt increased levels of PA, as they might feel less singled out and targeted by the healthcare provider. mHealth may be another tool that can improve accessibility for patients of lower socioeconomic status, or those in geographically remote areas, as it provides a more innovative and flexible approach for many patients (Tate et al., 2013). Developing health promotion materials with different types of free or low-cost PA resources (e.g., YouTube channels) can provide patients with interesting and feasible options for maintaining or increasing their PA levels. Future research should focus on developing provider decision-making aids (e.g., a decision tree) to engage patients and their families in a non-stigmatizing, patient-and-family centered manner.
Systematically, in addition to attending to the components of an integrated and comprehensive system of care, the literature highlighted the role of child-centered care (CCC) in encounters with overweight and obese patients. It may allow children to have opportunities to ask questions, participate in shared decision-making, and engage in practices for better weight management. As recent research showed that PCC mediated the impact of media consumption on people’s adoption of healthy lifestyles, CCC may also help children better engage in healthy eating and PA. After all, for a well-functioning healthcare system, pediatric providers’ focusing on the family unit always is not enough. In analyzing the antecedents, attributes, and relationship between family-, person-, and child-centered care, respecting the individual child as having agency while still being dependent on the family may be more beneficial (Coyne et al., 2018).
Some limitations exist. Cross-sectional survey data may not have conclusions related to causality drawn. Experimental and longitudinal studies should explore the effective intervention strategies that may be implemented at interpersonal and systematic levels to address health disparities related to overweight and obese pediatric patients. Second, we only used “unaffordable medical bills” to represent children’s experience of SDH. Future research can include more SDH factors to explore how PCC may address each of them. Although the NSCH data are nationally representative, the 39.1% response rate may introduce potential selection bias. There may also be potential reporting bias (e.g., recall bias) from parents when assessing their children’s health outcomes and social development. Additionally, we did not account for ethnic or cross-national differences in our variables, which may limit generalizability of the findings. Future research can use larger samples and mixed methods to better understand the health outcomes and social development of underrepresented populations. We only studied the impact of clinical and family environments on the well-being of overweight children. Future research can explore the influence of other communication contexts, such as media, regarding how media messages may effectively convey the positive effects of healthy lifestyles on overweight and obese children. Also, because we did not compare PCC’s impact across different social contexts, future research could conduct systematic reviews to better understand variations in the influence of PCC.
Conclusion
Using a nationally representative sample, we studied the role of patient-centered care in alleviating the negative impact of adverse environments experienced by overweight and obese children. This population may benefit from targeted health interventions given the ever-increasing rise in overweight and obese children and adults in the US, particularly in the aftermath of the COVID-19 pandemic. As a result, unaffordable medical bills predicted parents’ reports of their children’s forgone mental health care and difficulty making friends; adverse childhood experiences predicted forgone mental health care, difficulty making friends, and provider expression of weight concerns. Patient-centered care, at interpersonal and systematic levels, predicted better physical, mental, and social outcomes. Our results showed that PCC had the potential to break the vicious cycle from adverse environments to poor health outcomes, enhancing the well-being of overweight and obese patients. Healthcare practitioners should collaboratively address the patients’ health and social needs beyond merely expressing their concern to improve health outcomes nationwide.
Footnotes
Ethical Considerations
Author Contributions
QLW and GEB contributed to the design and implementation of the present study, to the analysis of the results, and to the writing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.