
Abstract
Background:
Immersive virtual reality (IVR) is an emerging tool in neurorehabilitation, offering interactive, motivating experiences that promote motor and cognitive engagement. However, most IVR games are not designed for therapeutic use, and evidence on age- and gender-based responses remains limited.
Objective:
This study aimed to evaluate upper extremity movement patterns and cardiovascular responses elicited by commercially available IVR games in typically developing children and adults, with attention to age and gender differences.
Methods:
In Phase I, six Meta Quest 2 IVR games were analyzed for their therapeutic potential by physical therapy professionals. Five games (Fruit Ninja, Beat Saber, Bowling, Baseball, and Tennis) were selected for Phase II testing. Sixty-seven healthy participants (40 children aged 5–12, 27 adults aged 20–34) played each game for 3 minutes while seated. Arm movements were video-coded, and heart rate was continuously monitored. Participants completed usability and satisfaction questionnaires post-play.
Results:
Fruit Ninja and Beat Saber elicited the highest number of total, unilateral, bilateral, and multidirectional arm movements and produced the greatest cardiovascular responses. Adults demonstrated more total reaches, while children exhibited higher heart rate responses and more forward/backward reaches. Gender differences were observed in reach direction and heart rate. Boys reported higher simulator sickness scores, while males reported higher overall satisfaction.
Conclusion:
IVR games, particularly Fruit Ninja and Beat Saber, show promise for upper extremity rehabilitation by promoting motor and cardiovascular engagement. Age- and gender-related differences should inform individualized therapeutic applications. Future studies should explore these games in clinical populations.
Keywords
Introduction
Virtual reality (VR) has emerged as a promising tool in health and rehabilitation sciences, offering an engaging and interactive environment that promotes motor engagement and cognitive stimulation.1–3 Evidence supports VR’s effectiveness in improving upper extremity function in individuals with neurological conditions such as stroke and cerebral palsy (CP).4,5 Immersive virtual reality (IVR), in particular, offers real-time feedback and adaptable challenges that encourage users to perform targeted movements, making it a promising tool for upper extremity rehabilitation.3,6,7
The development of commercially available IVR platforms such as Meta Quest 2 (Meta Platforms, Inc.) has increased access to home-based rehabilitation. Compared with conventional therapy, IVR games can enhance motivation and adherence through enjoyable, game-based experiences.2,8 However, most IVR games are not specifically designed for therapeutic use and may feature complex controls that pose challenges for individuals with motor impairments. 9 Despite the growing interest in IVR applications for upper extremity rehabilitation, several challenges and gaps remain. These include physical discomfort from extended headset use and cybersickness (symptoms such as nausea, dizziness, and disorientation), which can limit participation and reduce intervention effectiveness.2,8,10–13
Furthermore, existing research on IVR rehabilitation tends to focus on a single age group, limiting the generalizability of findings.14–19 There is a need for studies comparing IVR’s effectiveness across both children and adults to optimize rehabilitation strategies for diverse populations. The success of IVR games in rehabilitation depends on various factors, including game design, user engagement, and physiological responses. 20 Elements such as game difficulty, enjoyment, and usability play a critical role in sustaining motivation and participation.7,17,18,21,22 In pediatric CP research, different IVR games have been shown to elicit varying movement intensities, underscoring the importance of game selection in clinical contexts.3,4 This study aimed to evaluate the immediate response of commercially available IVR games in eliciting upper extremity movements and cardiovascular responses in children and adults. We investigated how different games impact movement patterns and heart rate, with attention to age and gender differences. It was hypothesized that adults and children would perform differently due to developmental disparities in motor skills, with adults generally exhibiting greater coordination, strength, and cognitive processing abilities compared to children. Regarding heart rate differences, adults typically have a lower resting heart rate due to a more efficient cardiovascular system developed over time. 23 When engaging in physical activities, children experience a more significant heart rate increase relative to adults, as their hearts work harder to meet the activity demands. 24 Additionally, children’s cardiovascular systems are less efficient in responding to exercise, leading to a higher heart rate at a given level of exertion. 25
Performance differences between females and males were also expected, influenced by physiological factors such as muscle strength,26,27 hand dominance, and motor control strategies. 28 For example, males generally have greater muscle mass and cardiovascular endurance due to higher testosterone levels, which may result in lower heart rate responses during physical exertion.29–31 In contrast, females may exhibit different physiological responses due to differences in body composition, such as higher body fat percentages, which can affect endurance and heart rate responses.32,33 Ultimately, this study sought to evaluate the potential of IVR games as a tool for enhancing motor skills and improving rehabilitation outcomes, with consideration of age and gender-related factors in the process.
Materials and Methods
This study was conducted in two phases:
Phase I—game analysis: Six popular commercially available Meta Quest 2 IVR motion games were evaluated to identify movement and cognitive demands. Phase II—testing: The selected games were tested with typically developing children and adults to assess upper extremity movements and heart rate responses.
The study protocol was approved by the Georgia State University Institutional Review Board. Informed consent or parental consent was obtained for all participants.
Phase I: Game analysis
A licensed physical therapist and five Doctor of Physical Therapy (DPT) students evaluated six IVR games: Fruit Ninja, What the Bat?, Sports Scramble (Bowling, Tennis, Baseball), and Beat Saber.
Adapted from Chen et al. (2014), the Game Summary Table assessed each game’s movement and cognitive demands, including unilateral/bilateral reaching, movement speed, cognitive engagement, precision, endurance, eye–hand coordination, strength (inferred via movement velocity), feedback about the outcome, knowledge of results (KR) (e.g., score, success/failure), feedback about the quality of the movement, and knowledge of performance (KP) (e.g., trajectory, speed). Inclusion recommendations were based on these assessments (see Table 1).
Required Skills and Inclusion Recommendation for Meta Quest 2 Games
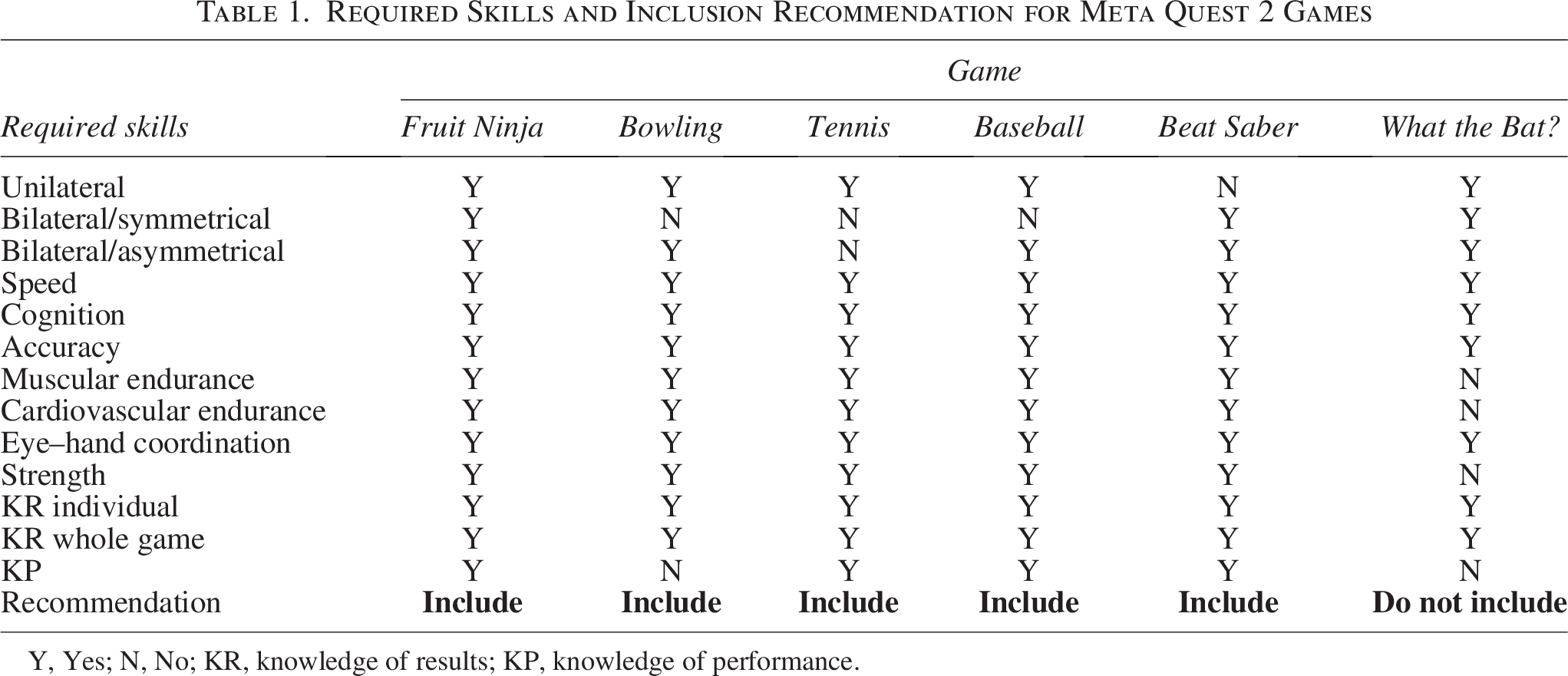
Y, Yes; N, No; KR, knowledge of results; KP, knowledge of performance.
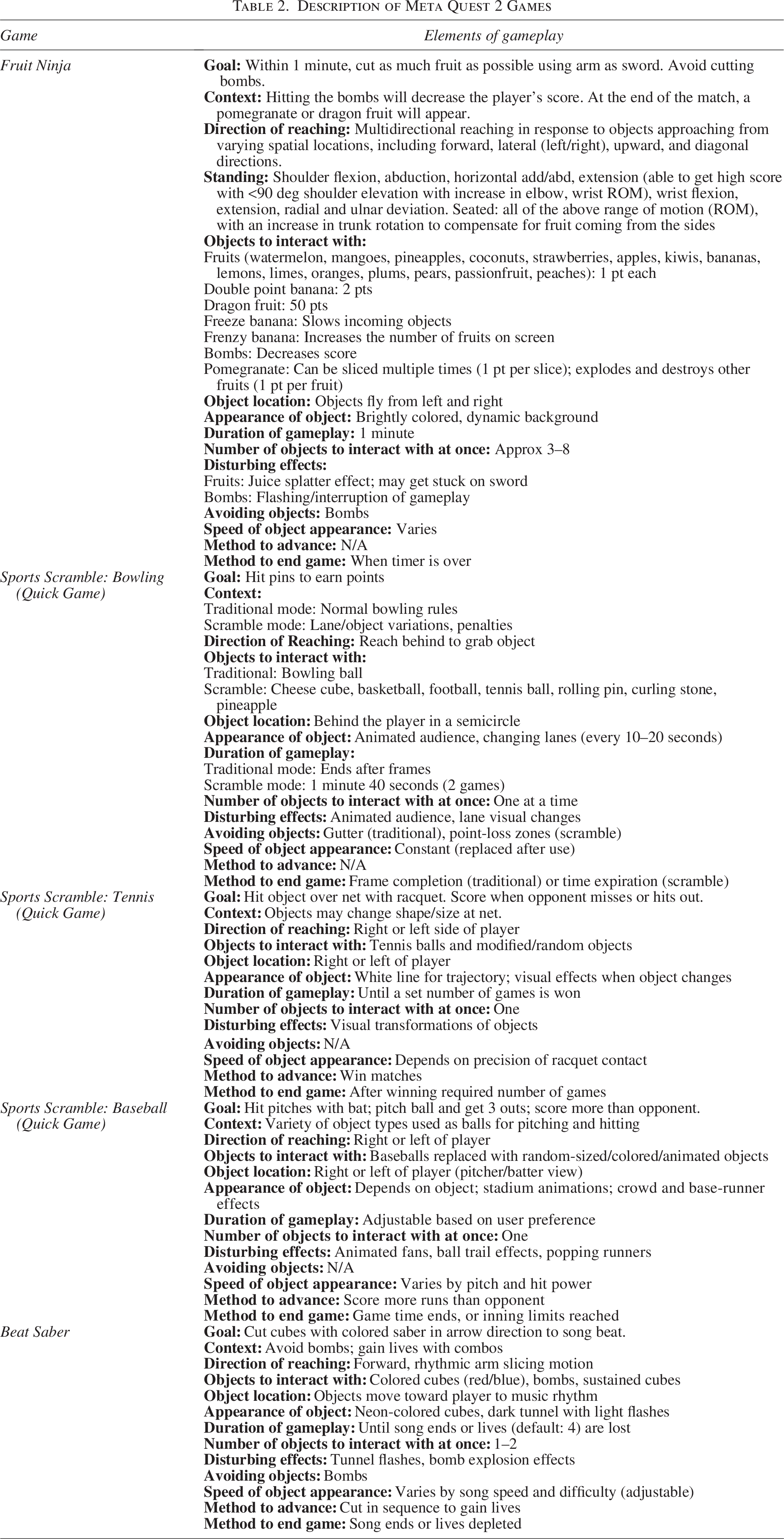
During a 1.5-hour lab session, evaluators played each game (5–8 times) while seated and observed others doing the same. They collaboratively completed descriptions and selected games for Phase II (see Table 2).
Description of Meta Quest 2 Games
Phase II: Testing with healthy participants
Participants
A total of 67 participants (27 adults aged 20-34; 40 children aged 5-12) were recruited via flyers, email, social media, and word of mouth. Inclusion criteria included ages 5-40, no neurological/orthopedic impairments, and proficiency in English or Portuguese.
Based on a power analysis with a desired power of 0.80 and a significance level of α = 0.05, assuming a large effect size (Cohen’s d = 0.8), a minimum of 25 participants per age group was estimated to be sufficient. This target sample size is consistent with previous exploratory VR rehabilitation studies.12–14 To ensure adequate statistical power, we recruited 27 adults and 40 children. A post hoc sensitivity analysis was also performed to estimate the smallest standardized effect size (Cohen’s d) detectable with 80% power at α = 0.05 (two-tailed). For the main between-group comparisons, the minimum detectable effect sizes were approximately d = 0.70 for adults (n = 27) versus children (n = 40) and d = 0.72 for females (n = 44) versus males (n = 23). Thus, the present sample was adequately powered to detect moderate-to-large effects (≈0.7) but underpowered to reliably detect small effects (d ≈ 0.2–0.4).
Apparatus
Participants used the Meta Quest 2 headset and controllers (Meta Platforms, Inc.). Gameplay was video recorded using an iPhone (Apple, Inc.), and heart rate was monitored using the Polar Beat system (Polar Electro, Inc.).
Procedures
After consent, participants completed a demographic questionnaire (included personal information such as age, gender, hand dominance, and VR experience) and rested for 5 minutes before baseline heart rate measurement. Each played five selected IVR games, seated (to ensure safety) for 3 minutes per game in randomized order. Heart rate was recorded at 1, 2, and 3 minutes during play. A 5-minute rest between games ensured heart rate recovery. Gameplay was video recorded for later movement coding.
After gameplay, participants completed the following assessments:
Custom survey: Game preferences, enjoyment, and fatigue. System Usability Scale (SUS):
31
10-item tool measuring ease of use and satisfaction. Simulator Sickness Questionnaire (SSQ):
32
16-item scale assessing nausea, oculomotor strain, and disorientation. User Satisfaction Evaluation Questionnaire (USEQ):
33
Measured usability, functionality, and overall satisfaction with the IVR experience.
These tools provided insights into usability, adverse effects, and user experience.
Data analysis: Movement and heart rate
Arm movements were operationalized in several ways: Unilateral and bilateral reaching were measured by counting the number of movements within a 3-minute period. Muscular endurance was operationalized as the total movement count in 3 minutes. Cardiovascular endurance was evaluated based on the maximal heart rate change. Video recordings were analyzed by five DPT students using Movie Maker, who underwent a 2-hour training session to standardize movement identification criteria. Movements were coded using a predefined operational manual specifying unilateral and bilateral reaching directions (forward, backward, left, right, diagonal, up, and down). To assess reliability, 20% of the video dataset was randomly selected and double-coded by the study coordinator. Interrater reliability was calculated using the intraclass correlation coefficient (ICC, two-way random model, absolute agreement). The resulting ICC values ranged from 0.86 to 0.94 across movement categories, indicating good reliability. Any discrepancies were discussed and resolved through consensus with the study coordinator, ensuring data accuracy and consistency.
Statistical analysis
Descriptive statistics summarized demographics, movement counts, heart rate changes, and questionnaire scores. Chi-square tests examined age and gender distributions. Linear mixed models analyzed differences in movement and physiological responses across games, age, and gender to account for fixed effects and random effects. Estimated marginal means were reported to represent model-adjusted means that control for other factors in the model, providing more accurate comparisons across conditions. Post hoc pairwise comparisons were reported using Bonferroni adjustments (P < 0.05). One-way analysis of variance (ANOVAs) assessed age and gender effects on SUS, SSQ, and USEQ scores. Analyses were performed using SPSS v29 (IBM Corp., Armonk, NY).
Results
Phase I
Six commercially available IVR games were assessed for their motor and cognitive demands. Table 1 summarizes each game’s features, targeted skills, feedback types, and inclusion recommendations. Interrater agreement supported Phase I assessments. Based on the evaluation, five games were selected for Phase II. What the Bat? was excluded due to its complex setup and unclear rules.
Among the selected games, Fruit Ninja, Bowling, Baseball, and Tennis primarily elicited unilateral reaching, while Beat Saber promoted symmetrical bilateral reaching. Four games facilitated asymmetrical bilateral movement. All five games addressed key rehabilitation goals, including speed, accuracy, endurance, and eye–hand coordination. All games provided KR, while all, except one, also included KP feedback. All games required cognitive engagement and targeted accuracy.
Table 2 presents detailed contextual elements relevant for clinical use, including object layout, game pacing, task complexity, and progression strategies. These data help clinicians tailor game selection to patient goals by matching game mechanics with motor and cognitive rehabilitation needs.
Phase II
Sixty-seven participants (27 adults, 40 children) completed Phase II, with 85.1% of participants being right-handed. Gender and hand dominance were not significantly associated with age group (all P > 0.05); a gender imbalance was observed. No significant differences were found in prior VR experience by gender or age. However, children were more likely to report fatigue (40.0% vs. 14.8%, P = 0.03) and prefer indoor play (62.5% vs. 18.5%, P = 0.001). Participant demographics are summarized in Table 3.
Demographics and Feeling about Playing IVR Games (N = 67)
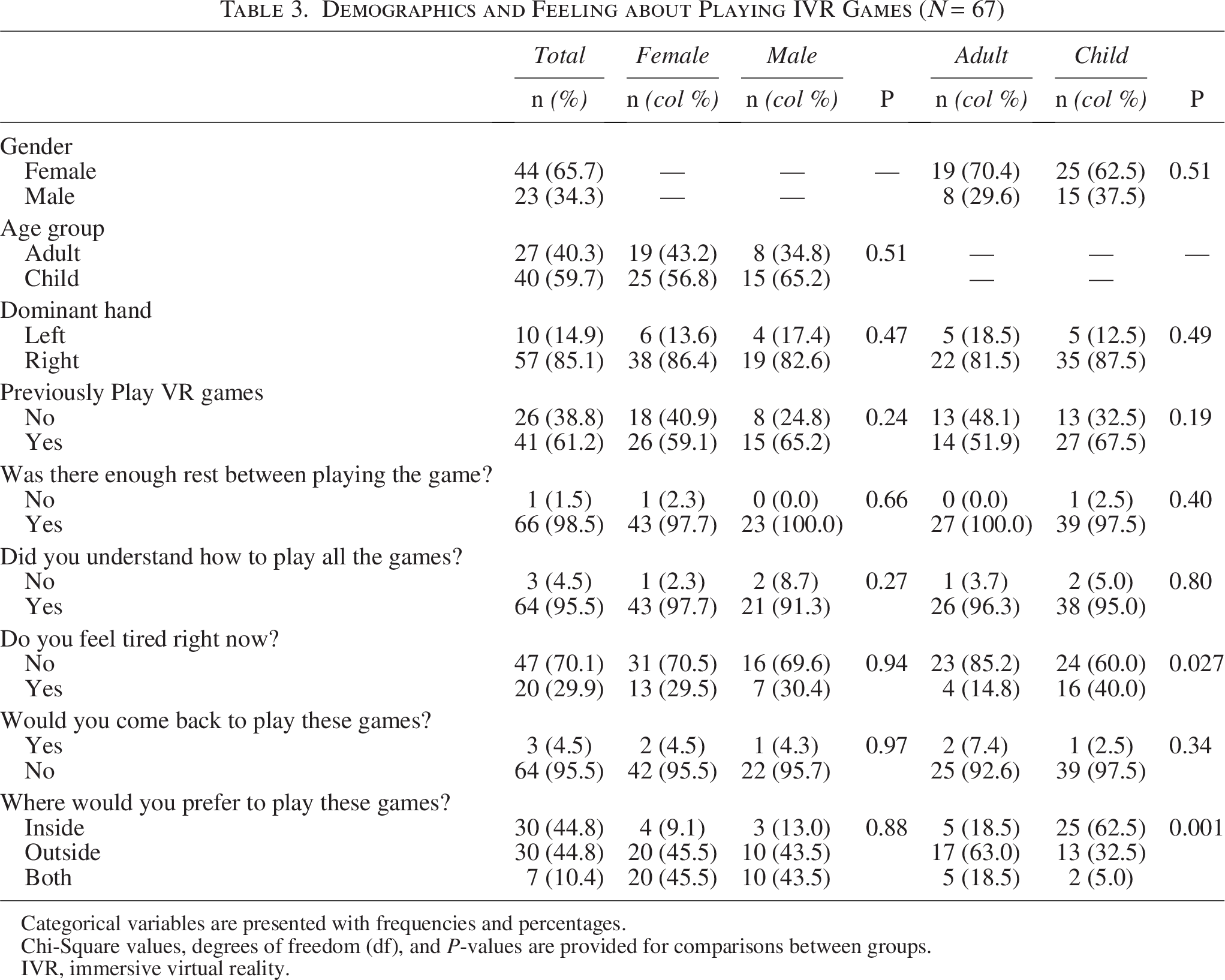
Categorical variables are presented with frequencies and percentages.
Chi-Square values, degrees of freedom (df), and P-values are provided for comparisons between groups.
IVR, immersive virtual reality.
Movement patterns across game types
Table 4 shows the mean and standard deviations of arm movements and heart rate data. Children displayed significantly higher heart rates at baseline and during gameplay (P < 0.05), indicating stronger cardiovascular responses compared to adults. Table 5 summarizes linear mixed model results. Beat Saber and Fruit Ninja elicited significantly more total reaches compared with Tennis (P < 0.001), while Bowling resulted in fewer (P = 0.005). Adults performed more total reaches than children (P = 0.008); gender had no significant effect.
Arm Movements and Heart Rate Across Groups (N = 67)
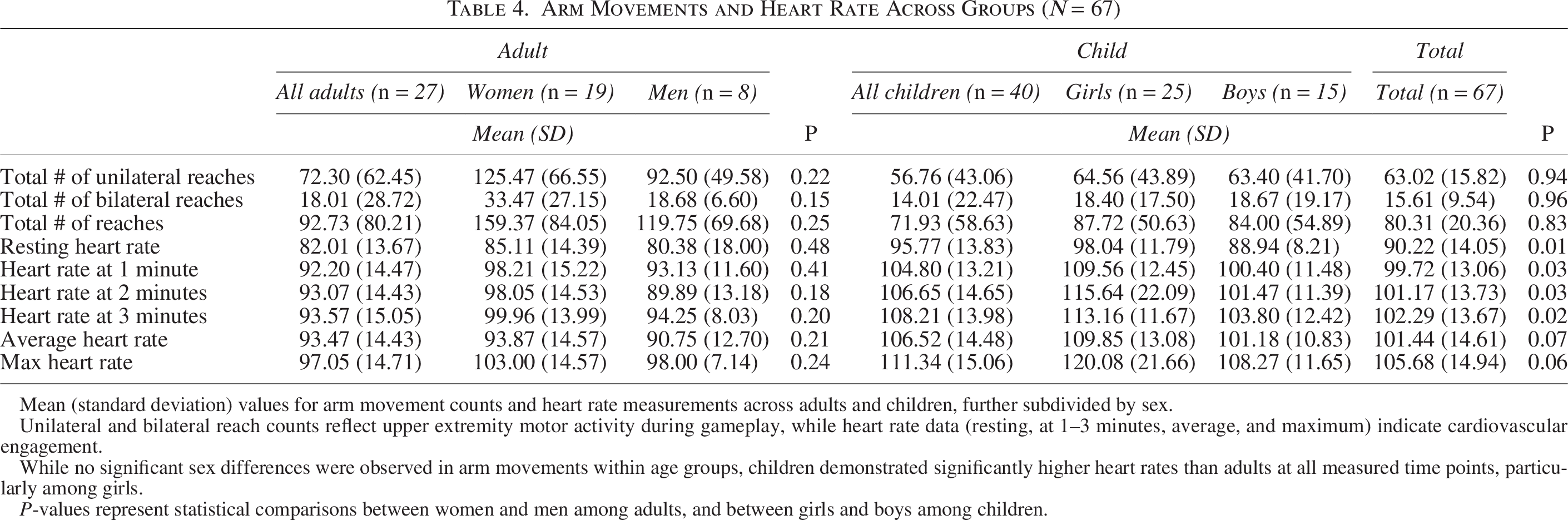
Mean (standard deviation) values for arm movement counts and heart rate measurements across adults and children, further subdivided by sex.
Unilateral and bilateral reach counts reflect upper extremity motor activity during gameplay, while heart rate data (resting, at 1–3 minutes, average, and maximum) indicate cardiovascular engagement.
While no significant sex differences were observed in arm movements within age groups, children demonstrated significantly higher heart rates than adults at all measured time points, particularly among girls.
P-values represent statistical comparisons between women and men among adults, and between girls and boys among children.
Movement Patterns Across Game Type and Groups (N = 67)
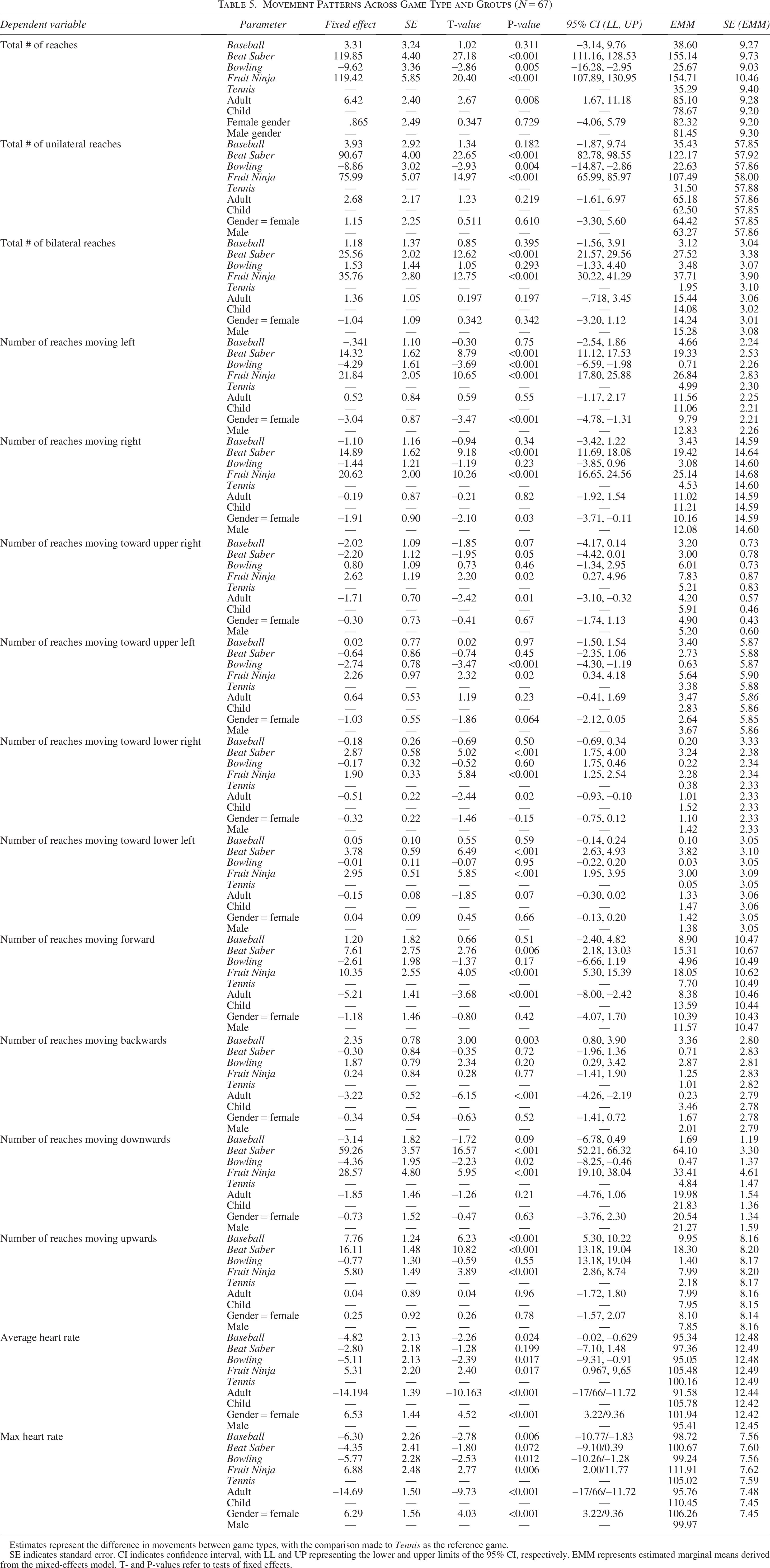
Estimates represent the difference in movements between game types, with the comparison made to Tennis as the reference game.
SE indicates standard error. CI indicates confidence interval, with LL and UP representing the lower and upper limits of the 95% CI, respectively. EMM represents estimated marginal means derived from the mixed-effects model. T- and P-values refer to tests of fixed effects.
Bonferroni Pairwise Comparisons Between Games Across Movement and Physiological Variables
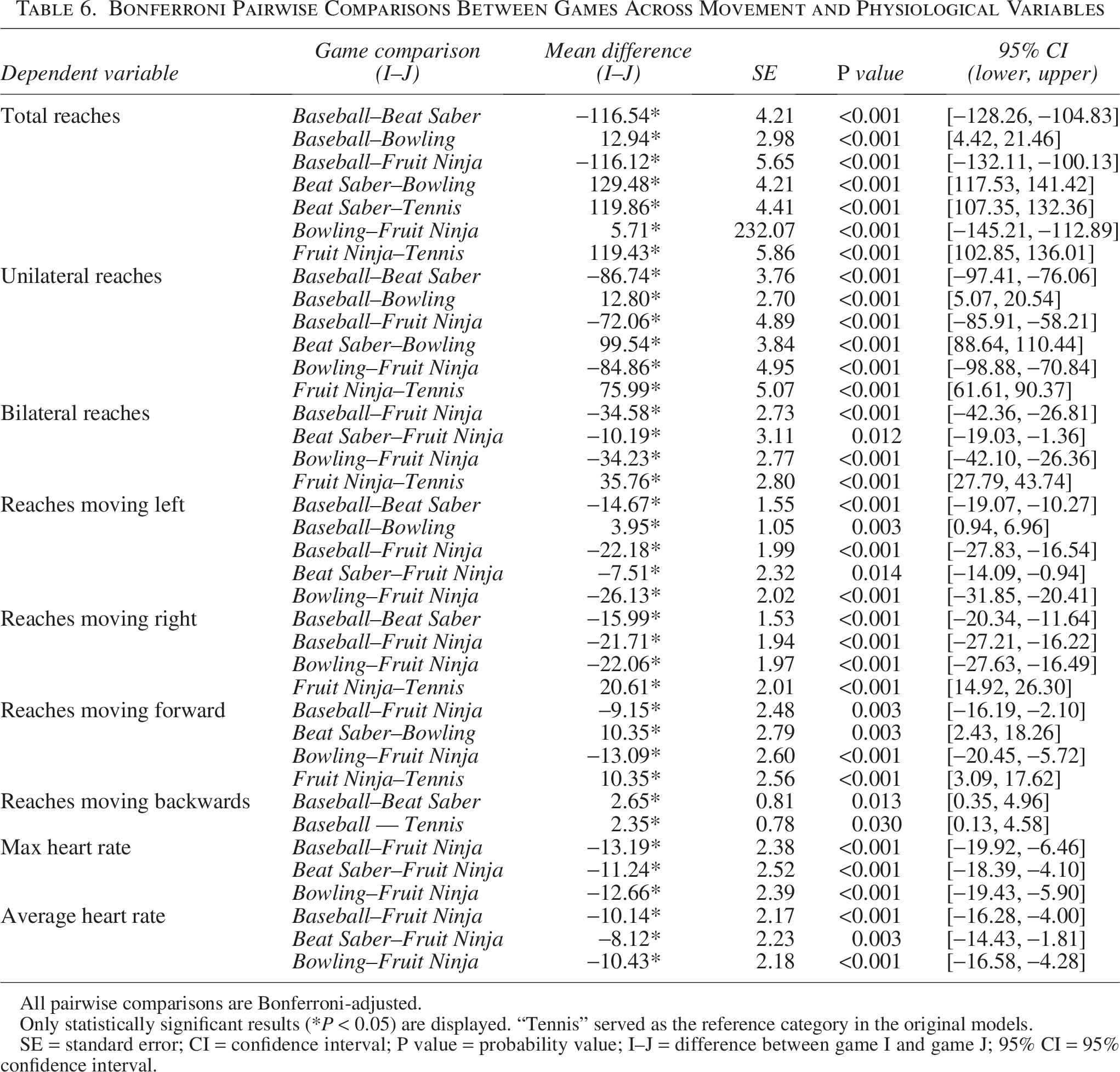
All pairwise comparisons are Bonferroni-adjusted.
Only statistically significant results (*P < 0.05) are displayed. “Tennis” served as the reference category in the original models.
SE = standard error; CI = confidence interval; P value = probability value; I–J = difference between game I and game J; 95% CI = 95% confidence interval.
Unilateral reaches were also higher in Beat Saber and Fruit Ninja (P < 0.001) and lower in Bowling (P = 0.004). No significant effects were observed for Baseball, age, or gender. Similar results were observed for bilateral movements, with both Beat Saber and Fruit Ninja outperforming Tennis (P < 0.001).
Directional reach analysis
Directional analysis revealed that Beat Saber and Fruit Ninja elicited more left, right, and forward movements than Tennis (P < 0.001). Bowling reduced leftward movements (P < 0.001). Males performed more directional movements than females (P < 0.05), and children performed more forward and backward reaches than adults (P < 0.001). Baseball increased backward movement (P = 0.003). Diagonal movement increases were especially evident in Fruit Ninja, which showed significant gains in multiple directions, including upper and lower diagonals and upward motions (P < 0.05). Beat Saber elicited the most number of downward movements (P < 0.001).
Cardiovascular response
Children showed significantly higher heart rates than adults at baseline and during gameplay (P < 0.05). Females had higher average and maximum heart rates than males (P < 0.001). Among games, Fruit Ninja elicited the highest cardiovascular response, with significantly greater average and maximum heart rates compared with Baseball, Bowling, and Tennis (all P < 0.05). Baseball and Bowling were associated with the lowest heart rates.
Post hoc comparisons between games
Bonferroni-adjusted pairwise comparisons (Table 6) confirmed that Fruit Ninja and Beat Saber were significantly more effective in promoting motor engagement than other games. For example, Beat Saber generated 129 more total reaches than Bowling (P < 0.001), and Fruit Ninja elicited 119 more total reaches than Tennis (P < 0.001). Both games also outperformed others in bilateral and directional movements. In terms of physiological engagement, Fruit Ninja produced significantly higher average and maximum heart rates than all other games, further highlighting its potential therapeutic value.
Gameplay preferences
Participant preferences (Supplementary Data S1) showed Fruit Ninja as most enjoyable (37.3%), followed by Beat Saber (28.4%). Bowling received the fewest “most fun” ratings (3.0%) and the highest “not very fun” ratings (55.2%). Beat Saber was rated easiest to play (46.3%), while Bowling and Tennis were most frequently rated as hardest.
Usability and acceptability
Supplementary Data S2 shows usability ratings. No significant group differences in SUS scores were observed (P = 0.054). However, simulator sickness scores differed significantly, with boys reporting the highest (P < 0.001). Satisfaction (USEQ) also differed (P = 0.011), with men and boys reporting higher satisfaction than women and girls.
Discussion
This study assessed the therapeutic potential and user acceptability of five IVR games played on the Meta Quest 2 headset. Using a two-phase design, we evaluated both gameplay mechanics and performance outcomes to understand the relevance of these games for cognitive and motor rehabilitation. The immersive and interactive nature of IVR environments positions them as promising tools for engaging users in rehabilitation tasks that simulate real-world activities.3,16,34
Phase I: Game analysis and inclusion
Game selection and therapeutic relevance
Through structured evaluation by six independent raters, What the Bat? was excluded due to ambiguous rules and complex setup. This highlights the importance of clarity and accessibility in therapeutic games. The remaining games (Fruit Ninja, Bowling, Baseball, Tennis, and Beat Saber) exhibited varied but meaningful therapeutic potential. Each of the five supported unilateral reaching, four allowed asymmetrical bilateral movement, and Beat Saber uniquely encouraged symmetrical bilateral actions. All of which are critical for restoring motor control, coordination, and functional symmetry.
These games targeted foundational rehabilitation domains, including speed, accuracy, strength, and eye–hand coordination, while also promoting muscular and cardiovascular endurance. All games provided KR, and most offered KP, enhancing motor learning by informing users about both outcomes and movement quality.
Core skill demands and feedback
All six games required cognitive and physical skills such as speed, accuracy, and coordination, making them broadly applicable to motor and cognitive rehabilitation. However, only four delivered KP feedback, with Bowling and What the Bat? lacking insights into movement quality, potentially limiting their use in motor-focused therapy.
Recommendations for therapeutic use
All games except What the Bat? are recommended for therapeutic use. These five balance cognitive and physical demands, deliver meaningful feedback, and foster motivation, key elements in effective rehabilitation. What the Bat?, while engaging, lacked muscular and cardiovascular engagement and actionable feedback, making it less suitable for structured therapy.
Phase II: Real-world performance outcomes
Motor engagement and movement patterns
Fruit Ninja and Beat Saber consistently elicited the highest number of total, unilateral, and bilateral reaches, promoting forward, lateral, and diagonal movements, essential for restoring upper-limb function and encouraging neuroplasticity.35,36 In contrast, Bowling resulted in fewer reaches but involved more complex coordination tasks (e.g., ball manipulation and release), which may support fine motor planning, beneficial for populations such as children with developmental coordination disorder.37,38
Physical and cardiovascular demands
Games differed in their physical intensity. Fruit Ninja and Beat Saber produced the most arm movement and cardiovascular activation, consistent with their rapid, dynamic gameplay.17,22 Bowling and Baseball elicited lower heart rate responses, possibly due to slower pace and precision-oriented tasks, making them more suitable for users requiring low-intensity engagement. 39
Age-related differences
Adults performed more total reaches, while children demonstrated higher heart rate responses, likely due to developmental differences in cardiovascular efficiency.25,40 Children also exhibited more forward and backward reaches, suggesting exploratory movement patterns, whereas adults engaged in more refined, efficient strategies.41–43 Notably, children reported significantly higher simulator sickness scores, consistent with literature linking younger age to increased VR-related motion sensitivity.44–46 These findings suggest that shorter sessions and simpler visuals may improve usability for younger users.
Gender-based differences
Males showed greater lateral reach activity, potentially reflecting more expansive gameplay styles or upper-limb strength differences.26,47,48 Females displayed higher peak and average heart rates, which may be due to physiological differences such as aerobic capacity and body composition.32,49 Despite these differences, overall engagement levels were similar between genders.
Subjective preferences versus objective performance
Interestingly, males reported higher satisfaction with IVR games despite also reporting more simulator sickness, contrasting with prior findings suggesting females are more sensitive to such symptoms.50,51 This may indicate greater tolerance among males due to higher gaming exposure or familiarity with immersive environments.
Enjoyment and difficulty ratings were consistent with objective data: Fruit Ninja and Beat Saber were the most enjoyable and least difficult, aligning with their high movement and exertion levels. This supports evidence that engaging games can enhance motivation and reduce perceived effort during physical activity,52,53 making IVR-based rehabilitation more appealing and sustainable.15,16,54
Clinical implications
These results support the integration of IVR into rehabilitation programs, with Fruit Ninja and Beat Saber particularly suited for multidirectional arm movement and cardiovascular conditioning. Children and users prone to motion sickness may benefit from shorter sessions and simplified visuals. 2 Clinicians can use game-specific profiles to tailor interventions according to participants’ age, gender, physical goals, neuromotor impairments, and individual tolerance levels.17,45,55 Gender- and condition-specific adaptations, such as customizable avatars, adjustable difficulty, and adaptive strategies, may further enhance user experience and accessibility.15,16,20
Limitations and future directions
This study has several limitations. First, using a healthy population limits generalizability, clinical groups such as individuals with CP or stroke. However, our study provides a base to understand the immediate responses of playing IVR games in adults and children. Future research should investigate the use of these games in target rehabilitation populations and explore adaptations based on individual needs, such as difficulty level, hand control options, and games that do not require button activation.
Second, the short gameplay duration may not reflect long-term engagement or functional gains. Longitudinal intervention studies are needed to assess therapeutic impact over time.
Third, the modest sample size and uneven gender distribution should be considered when interpreting subgroup comparisons. Our sample (N = 67) provided 80% power to detect only moderate-to-large effects (∼d ≥ 0.7) for the age and gender subgroup comparisons; smaller effects may have gone undetected.
Lastly, subjective reports of fatigue and enjoyment may be biased. Incorporating physiological fatigue measures and behavioral observations could provide more robust data. Future research should explore adaptive features (e.g., hand dominance, cognitive profile) and embed IVR into comprehensive rehabilitation protocols to maximize clinical impact.
Conclusion
This study demonstrated that IVR games effectively elicit diverse upper extremity movements in children and adults, with notable differences in reach patterns based on age. Each game produced varied movement profiles, emphasizing the importance of game mechanics in rehabilitation. The results highlight the clinical potential of IVR games that balance bilateral and targeted reaching. The observed engagement and feasibility support their use in therapeutic settings, including for individuals with neuromotor impairments such as CP. Future studies should explore clinical populations and how adjusting game features impacts movement quality, motivation, and rehabilitation outcomes over time.
Authors’ Contributions
B.S.S.: Writing—review and editing, writing—original draft, methodology, investigation, formal analysis, project administration, supervision, and visualization. H.R.: Formal analysis, writing—review and editing. Y.C.: Conceptualization, methodology, resources, supervision, writing—review and editing, and funding acquisition.
Footnotes
Acknowledgment
The authors thank the Doctor of Physical Therapy students, Andre Joseph Yousif, Bernard Turner, Eryn Render, Grayson Pareizs, Huy Chiem, Ivette Martinez, Kayla Owen, Maggie Abercrombie, Mansi Patel, and Rayley Ferrell, for their assistance with data collection and Dr. Ruiyan Luo for her suggestions on the statistical analysis method.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This work was supported by a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (90IFST0009).
Data Availability
Data will be made available on request.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.