
Abstract
Objective:
To determine the effect of training children with familial Mediterranean fever (FMF) using a mobile game (MG) or training booklet (TB) on self-efficacy, symptom management, and quality of life (HRQoL) compared with a control group.
Materials and Methods:
The sample of the randomized controlled experimental study consisted of children with FMF. Children in the experimental groups received training with TB (n = 14) or MG (n = 14). The control group (n = 15) received no intervention and continued their routines. The Pediatric Rating of Chronic Illness Self-Efficacy Scale (PRCISE), and Juvenile Autoinflammatory Disease Multidimensional Assessment Report (JAIMAR) were used to collect data. Data were collected in pre-test, post-test-1, and post-test-2.
Results:
The MG group’s PRCISE (P < 0.001, P < 0.001), HRQoL (P = 0.001, P = 0.001), therapeutic compliance (P = 0.002, P = 0.004), increased and the mean pain scores (P = 0.044, P = 0.010), the number of symptoms decreased (P < 0.001, P < 0.001) in both measurements after the intervention. The mean PRCISE score of the TB group increased only in post-test 1 (P = 0.008), and the mean HRQoL total score did not change significantly in either post-test measurement (P > 0.05). The TB group’s symptom management indicators were similar at all measurements (P > 0.05). The control group’s PRCISE and HRQoL scores and symptom management indicators were similar at the three measurement times (P > 0.05).
Conclusion:
The MG increased illness self-efficacy, symptom management and HRQoL in children with FMF and its effect lasted longer than the TB. It is recommended to use and disseminate technology-based and interactive education methods such as MG in the management of chronic diseases in children.
Introduction
Familial Mediterranean Fever (FMF) is the most common monogenetic autoinflammatory disease.1,2 FMF negatively affects the daily life of children due to lifelong acute exacerbations.3,4 Lack of information about the disease and uncertainty about when an attack will occur are sources of stress for children. 5 Moreover, emergency room visits due to attacks, school absences, the need for regular medication use throughout life, and emotional stress negatively affect the health-related quality of life (HRQoL).6–8 Therefore, to increase the HRQoL, children need to adopt and maintain the necessary health behavior changes. 9 A child’s ability to manage their disease is important to increase the HRQoL. 6 For good disease management, the child’s education and disease self-efficacy must be ensured. However, health professionals often focus on the medical dimension of the disease and show less interest in the child’s adaptation to the treatment process and in managing the effects that arise due to the disease. Education programs that meet children’s need for information, support them in coping with their disease, and aim to monitor them during the process should be organized. 10 In this context, there is a need for research to evaluate children’s knowledge, skills, and disease management to facilitate early recognition of recurrent symptoms and to minimize attack episodes. 11
Today, with the increased accessibility of technological tools, the use of mobile technologies by children, adolescents, and health professionals, is becoming increasingly common. 12 These technologies, which are readily accepted by children and adolescents, will be useful in positively changing behaviors that affect the disease process, especially in chronic diseases. 13 Video games developed for health can provide health-related behavioral changes by encouraging children’s disease self-efficacy and self-management. 14 The use of video games in education allows children to feel that they are in control of their own lives at an earlier age. Thus, video games can make a difference in patient education and the management of chronic diseases. 15 When the literature is examined, it has been shown that video games can be used effectively in many areas, especially in the management of chronic diseases such as diabetes,16,17 cancer,12,14 and asthma.18,19 However, as far as we know, there is only one study on disease education and management for FMF, in which a traditional education booklet was used. 10 We believe that by increasing children’s disease self-efficacy and self-management, HRQoL will increase, symptom control will be provided, and future complications can be prevented. This study aimed to determine the effect of educating children aged 8–14 years with FMF using a mobile game (MG) or training booklet (TB) on disease self-efficacy, symptom management, and HRQoL. In this regard, our hypotheses were that FMF training given with MG would increase disease self-efficacy, symptom management, and HRQoL compared with the TB group and the control group.
Materials and Methods
Study design and setting
This study was a randomized controlled pre-test post-test study. Data were collected in the Child Health and Diseases Outpatient Clinics of a Training and Research Hospital in Kastamonu between August 2023 and April 2024. The study population consisted of children who were diagnosed as having FMF and admitted to the hospital for routine tests, and the sample consisted of children who met the inclusion criteria. The inclusion criteria were as follows: having an FMF diagnosis for at least 1 year, using colchicine, having at least one attack per year, being aged 8–14 years, volunteering to participate in the study, being literate, having parental permission to participate in the study, and the child or parent having an Android phone/tablet. Children with any identified mental disabilities, communication difficulties, or other chronic diseases, or any newly diagnosed chronic disease during the follow-up period, were not included in the study.
Sample size
The sample size was calculated using the G*Power 3.1.9.7 software. Because no similar study had been conducted previously, it was determined that a total of 36 children should be included in the calculation, with a medium effect size of f: 0.25, 0.80 power, β: 0.95, α: 0.05 for the two-way mixed analysis of variance (ANOVA), with at least 12 children in each group.20,21 A total of 45 children were included in the study because the length of the follow-up period could cause case losses, with a 20% increase in each group resulting in 15 children in each group. Randomization of the groups was achieved using an online program. 22 During the follow-up, one child from the MG group did not complete the scales and one child from the TB group did not read the booklet regularly, so two children were removed from the follow-up. Accordingly, the data of 43 children were included in the final analysis (Fig. 1). After the data were collected, a retrospective post hoc power analysis was performed to determine the adequacy of the sample size. The power of the test was determined as 0.98 and the sample size was found to be sufficient.
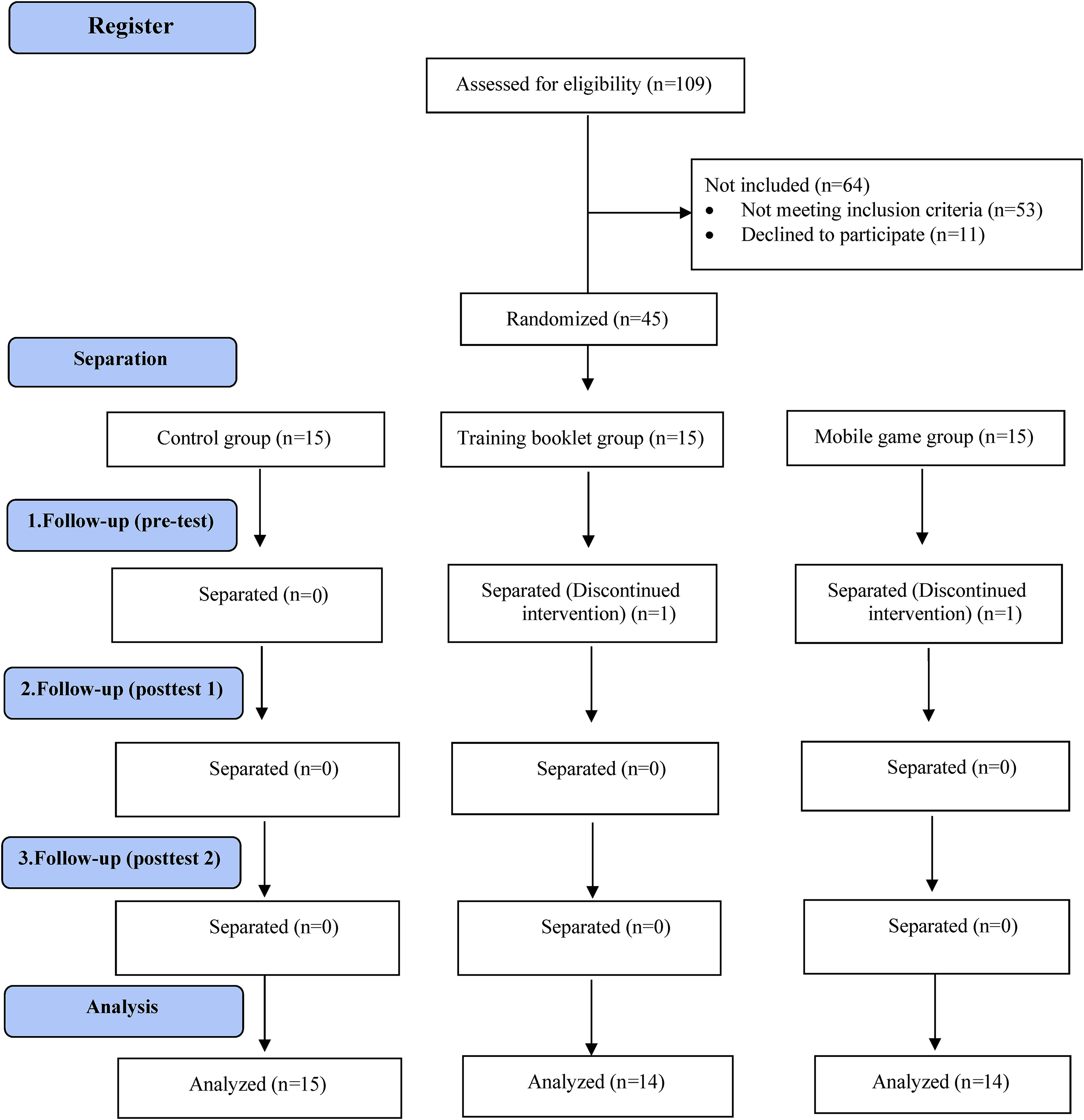
CONSORT flow chart.
Outcome measurements
Self-efficacy
Pediatric rating of chronic illness self-efficacy scale (PRCISE) was developed to assess the disease self-efficacy of children aged 10–17 with chronic illnesses. 23 The scale is an 11-point Likert-type scale consisting of 15 items, all positive, and the score of each item varies between 0 and 10. The total scores that can be obtained from PRCISE range from 0–150, and self-efficacy increases as the score increases. 24 The Cronbach’s alpha value of PRCISE was 0.703. PRCISE was applied to children in pre-test, post-test-1, and post-test-2. In our study, the Cronbach’s alpha value of the scale in post-test-2 was calculated as 0.921.
Symptom management and HRQoL
Juvenile Autoinflammatory Disease Multidimensional Assessment Report (JAIMAR) was developed for the multidimensional assessment of children aged 8–18 years with autoinflammatory diseases. 25 The scale has parent and child versions and measures four dimensions: Functional ability, pain, therapeutic compliance, and HRQoL. The child version of JAIMAR was used in our study. The functional abilities sub-dimension is scored on a 4-point Likert scale, and therapeutic compliance and HRQoL sub-dimensions are scored on a 5-point Likert scale. Scoring in functional abilities and HRQoL sub-dimensions is from 1 to 5, and the items in the therapeutic compliance sub-dimension are scored in reverse. A visual analog scale (VAS) is scored between 0 and 10 to measure pain. As the score decreases in the functional abilities, pain, and HRQoL sub-dimensions, and increases in the therapeutic compliance sub-dimension, it shows that the individual’s situation is more positive. There is no single total score or cut-off point obtained from the scale. Each criterion has its own scoring. The Cronbach alpha value of JAIMAR was found to be between 0.507 and 0.998. 25 JAIMAR was applied to children in pre-test, post-test-1, and post-test-2. In our study, the post-test-2 Cronbach alpha value was calculated as 0.638–0.911.
Mobile game and training booklet
A number of studies have suggested that infections, trauma, emotional stress, exposure to cold, fatigue, insomnia, long-term travel, excessive physical activity, prolonged standing, a high-fat diet, prolonged fasting, excessive food consumption, and non-compliance with colchicine treatment trigger attacks in FMF.10,26–30 MG and TB, in line with this literature information, and opinions received from 11 experts (a pediatric rheumatology professor, pediatric nursing faculty members, pediatric rheumatology nurses, a dietician, and a physiotherapist). The TB and MG provided information about the disease (e.g., what FMF is, how it is treated), self-management of factors that triggered attacks (e.g., exercise and activity, nutrition, sleep, stress management, infection prevention, medication use) and self-management of attack symptoms (e.g., fever, abdominal pain, joint pain, intestinal problems).
The TB was created with cartoon-like drawings and short narratives. To make the TB eye-catching, a nurse and a child with FMF were created. The TB consisted of a dialogue and question-and-answer format (Fig. 2). TB and MG had the same educational content. In TB, the information in plain text was presented as audio narration in the informative videos section of MG, and then the child played the game related to the relevant section. For example, in TB, the child had the opportunity to learn what to do for joint pain during flare-ups by reading, while in MG, the child first learned from the video narration and then played the game related to that section, earning points for correct answers. Support was received from the Computer Engineering Department of Istanbul University-Cerrahpaşa Faculty of Engineering in the preparation of the MG software, and from the Graphic Design Department of Kastamonu University Faculty of Fine Arts for the drawing of the visual characters used. The MG was developed using the Unity game engine, the most preferred game development platform for mobile devices and 2-dimensional games. The final product was an educational game that could provide positive or negative feedback on children’s performances based on their choices. Each stage of the game begins with a short educational video about the disease (Fig. 2). The educational videos voiced by the first researcher were enriched with visual presentations. Then, the child was given the opportunity to play the game and make choices that were appropriate to those presented in the educational video. For example, in the section on nutrition, the aim was to collect the appropriate foods at the ends of the balloons moving on the screen within a certain period. The child received negative points when they chose foods that were not appropriate for their nutrition, such as French fries, and positive points when they made appropriate choices, such as carrots (Fig. 2). To pass each stage and reach the next stage, it was necessary to obtain a certain number of positive points over time.

Training booklet
Procedure
Data were collected in an average of 30 minutes before and after the application by the first researcher through face-to-face interviews.
Pilot study
A preliminary application was conducted with four children because the game was newly developed and it was the first application to be performed. During the pilot study, children aged 15 years and over said that the game was not interesting for their age group. The age group determined as 10–15 years was updated to 8–14 years. These children were not included in the study.
Pre-test
Before the application, PRCISE, and JAIMAR were applied to the children in the MG, TB, and control groups. The MG link was loaded onto the phones of the children/parents in the MG group and the stages were introduced. The first stage of the game was played under the supervision of the researcher. The booklet was introduced to the children in the TB group, and they were made to read it once under the supervision of the researcher. The literature includes one-time or multi-session MG and TB applications. Based on the findings of these studies and the importance of reinforcement training, children were asked to play/read MG/TB at home once per week 4 weeks.10,12,18,31,32 When a child entered the game, the information was sent to the researcher via e-mail. The contact information of the mothers in both groups was collected, and reminder messages were sent once per week. The mothers were asked to remind their children to read the booklet/play the game. Children who did not play the game the desired number of times or did not read the booklet during this period were excluded from the study. The control group received no intervention and continued their routines (nutrition, medication use, movement and exercise, stress, sleep, pain management, etc.).
Post-test 1
PRCISE and JAIMAR were administered to children in the control and experimental groups at the end of week 4, on the last day they played the game/read the booklet. Because the end date of the intervention was calculated at the time the children were enrolled in the study, their hospital arrival times were planned. After the 4-week intervention, the MG group’s access to the game was restricted. The TB group was asked to bring their educational booklets with them when they arrived at the hospital for post-test 1, and the booklets were then taken back. This practice was crucial for monitoring the continuity of the results in post-test 2 without any intervention.
Post-test 2
PRCISE and JAIMAR were re-administered face-to-face to all groups at the end of the 8th week. After the study data were collected, the children in the control group were informed about TB and MG and trained using their preferred method. Providing post-study training to the control group ensured their access to information, thus protecting their ethical rights and benefits.
Analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) for Windows 25.0 (IBM, Armonk, NY, USA) package program. Descriptive statistics and internal consistency analysis was used in the evaluation of the data. The Kolmogorov–Smirnov test and skewness and kurtosis values were examined to determine whether the data showed a normal distribution. One-way analysis of variance (ANOVA) was used for independent groups. Bonferroni correction was applied for post hoc analyses. Changes in measurements within the group were analyzed using repeated measures ANOVA. If there was a significant difference between the periods, the dependent group t-test was used to compare the two periods between which the difference occurred. The Chi-square test and Fisher’s exact test was used for categorical data analysis. Significance was evaluated at a level of P < 0.05.
Ethics
This study was approved by the Kastamonu University University Institutional Review Board (IRB# 023-KAEK-7) in 08.02.2023, and permission for the use of scales was obtained via email. Children and their parents gave verbal and written consent before the application. In addition, a clinical trial number was obtained before starting the study (ClinicalTrials.gov ID: NCT05980780).
Results
Participants
The mean age of the children was 11.27 ± 1.98 years, the mean age at diagnosis was 4.33 ± 2.17 years, and 60.5% were male. The majority of the mothers and fathers in all groups had a high school or higher education level. Most parents did not have consanguineous marriages or anyone with FMF in their families. There was no significant difference between the groups in terms of the time of the last attack, the number of attacks in the last year, and the duration and degree of attacks (P > 0.05). All children and their parents were similar in terms of descriptive and disease-related characteristics (P > 0.05; Table 1).
Descriptive and Disease-Related Characteristics of the Children (n = 43)
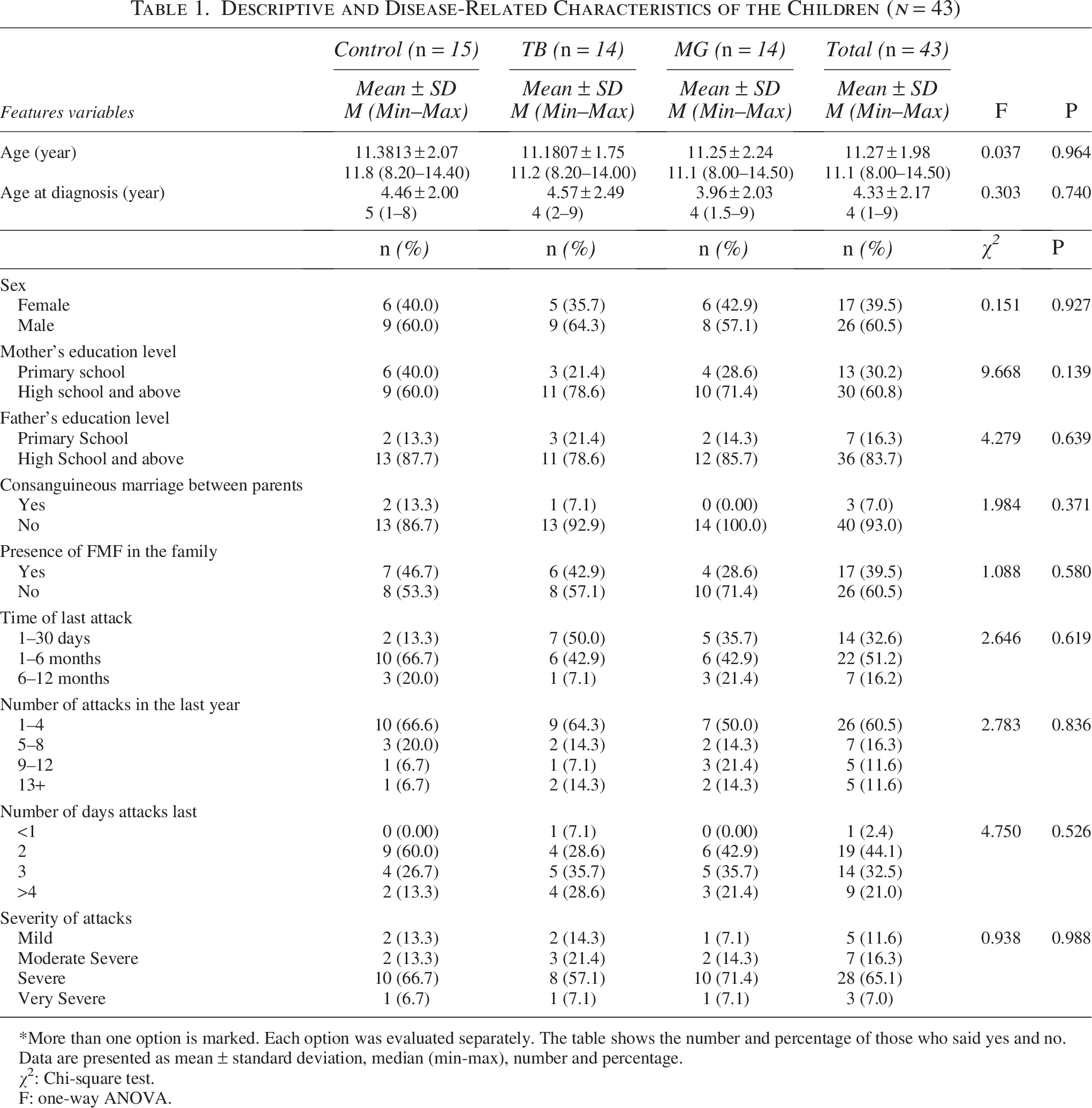
*More than one option is marked. Each option was evaluated separately. The table shows the number and percentage of those who said yes and no.
Data are presented as mean ± standard deviation, median (min-max), number and percentage.
χ2: Chi-square test.
F: one-way ANOVA.
The rate of those who applied the information they learned in the MG group (71.4%) was higher than in the TB group (21.5%), and the difference was statistically significant (P = 0.023). The rate of those who would continue to apply what they learned later was higher in the MG group (78.6%) than in the TB group (50.0%), but the difference was not statistically significant (P > 0.05).
Self-efficacy
When the children’s current attack status was examined (while data were collected), it was determined that most children in all groups were not in attacks, and the groups were similar at all three measurement times (P > 0.05). When the current disease status (while data were collected) was examined at all three measurement times, the majority of children in all groups stated that they had no symptoms, and a significant difference was found between the groups at post-test 1 (P = 0.006). The number of children with no symptoms was significantly higher in the MG group than in the TB and control groups (P < 0.001). When the disease status was examined after the last examination at all three measurement times, the majority of children in all groups stated that they had significantly improved, and a significant difference was found between the groups at post-test 2 (P = 0.008). The number of those with significant improvements after the last examination was significantly higher in the MG group than in the TB and control groups (P < 0.001). Table 2 shows the distribution of children’s disease-related characteristics according to the time of measurement.
Distribution of Children’s Disease-Related Characteristics According to the Time of Measurement (n = 43)
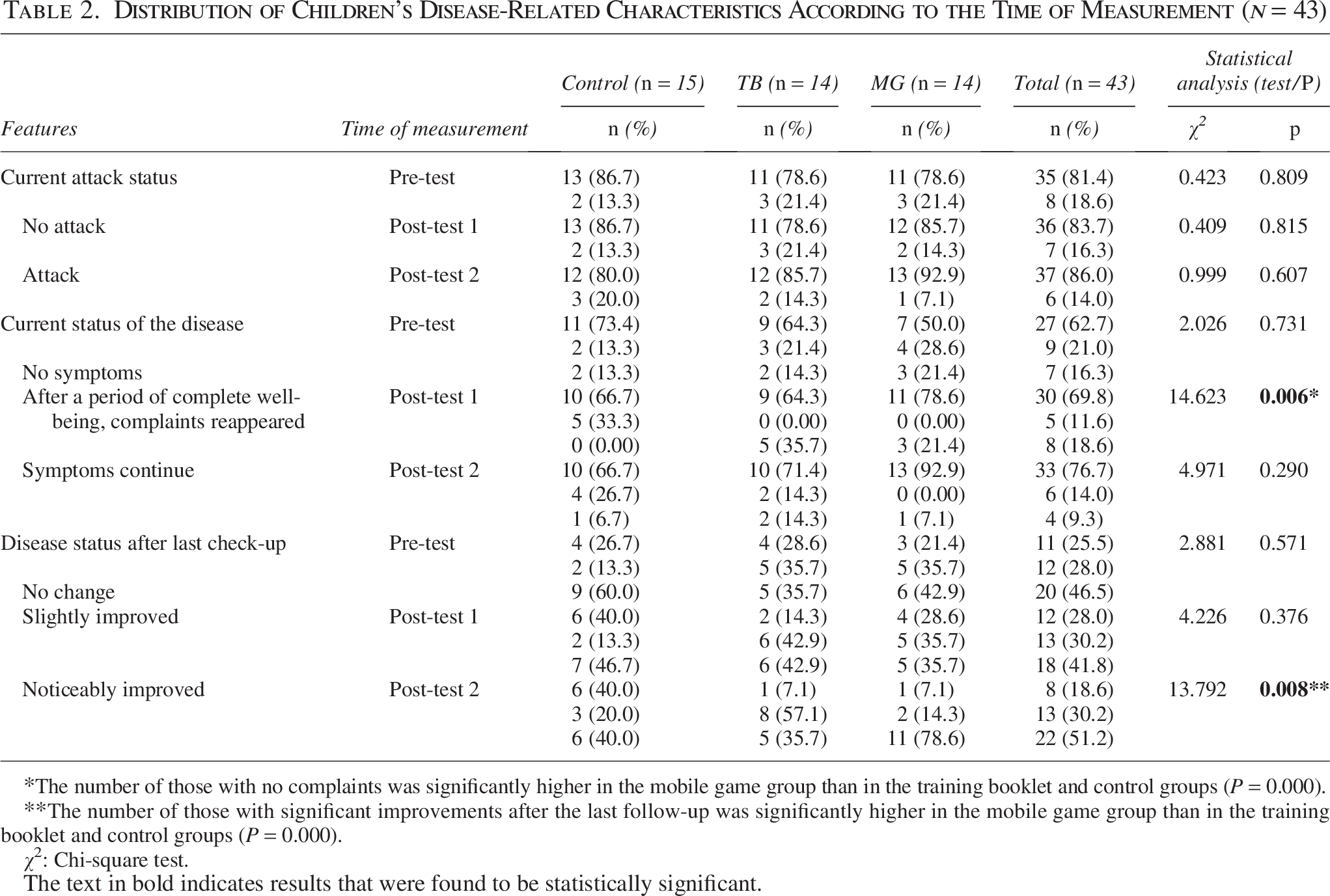
The number of those with no complaints was significantly higher in the mobile game group than in the training booklet and control groups (P = 0.000).
The number of those with significant improvements after the last follow-up was significantly higher in the mobile game group than in the training booklet and control groups (P = 0.000).
χ2: Chi-square test.
The text in bold indicates results that were found to be statistically significant.
Symptom management, HRQoL
In the MG group, the mean PRCISE score increased in post-test 1 and post-test 2 (P < 0.001; P = 0.001), and the mean HRQoL total score decreased (P = 0.001; P = 0.001). The mean PRCISE score of the TB group increased only in post-test 1 (P = 0.008), and the mean HRQoL total score did not change significantly in either post-test measurement (P > 0.05). In terms of symptom management, the mean medication adherence scores of the MG group increased in post-test 1 and post-test 2 (P = 0.002; P = 0.004), and the mean pain scores decreased (P = 0.044; P = 0.010). The number of symptoms decreased in the MG group in post-test 1 and post-test 2 (P < 0.001; P < 0.001) and continued to decrease over time (P < 0.001). The TB group’s symptom management indicators were similar at all measurements (P > 0.05). The control group’s PRCISE and HRQoL scores and symptom management indicators were similar at the three measurement times (P > 0.05). Table 3 shows the distribution of mean PRCISE scores, Table 4 shows the distribution in terms of symptom management, and Table 5 shows the distribution of mean total and sub-dimension scores for HRQoL.
Distribution of PRECISE Scores by Groups and Time (n = 43)
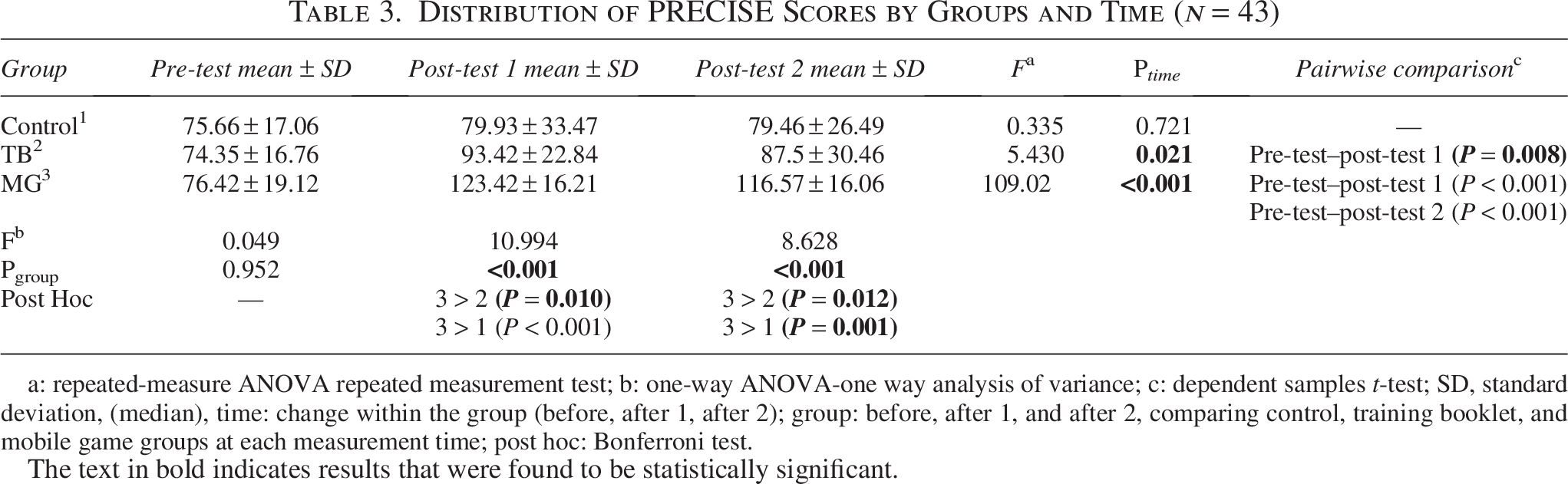
a: repeated-measure ANOVA repeated measurement test; b: one-way ANOVA-one way analysis of variance; c: dependent samples t-test; SD, standard deviation, (median), time: change within the group (before, after 1, after 2); group: before, after 1, and after 2, comparing control, training booklet, and mobile game groups at each measurement time; post hoc: Bonferroni test.
The text in bold indicates results that were found to be statistically significant.
Distribution of Groups in Terms of Symptom Management (n = 43)
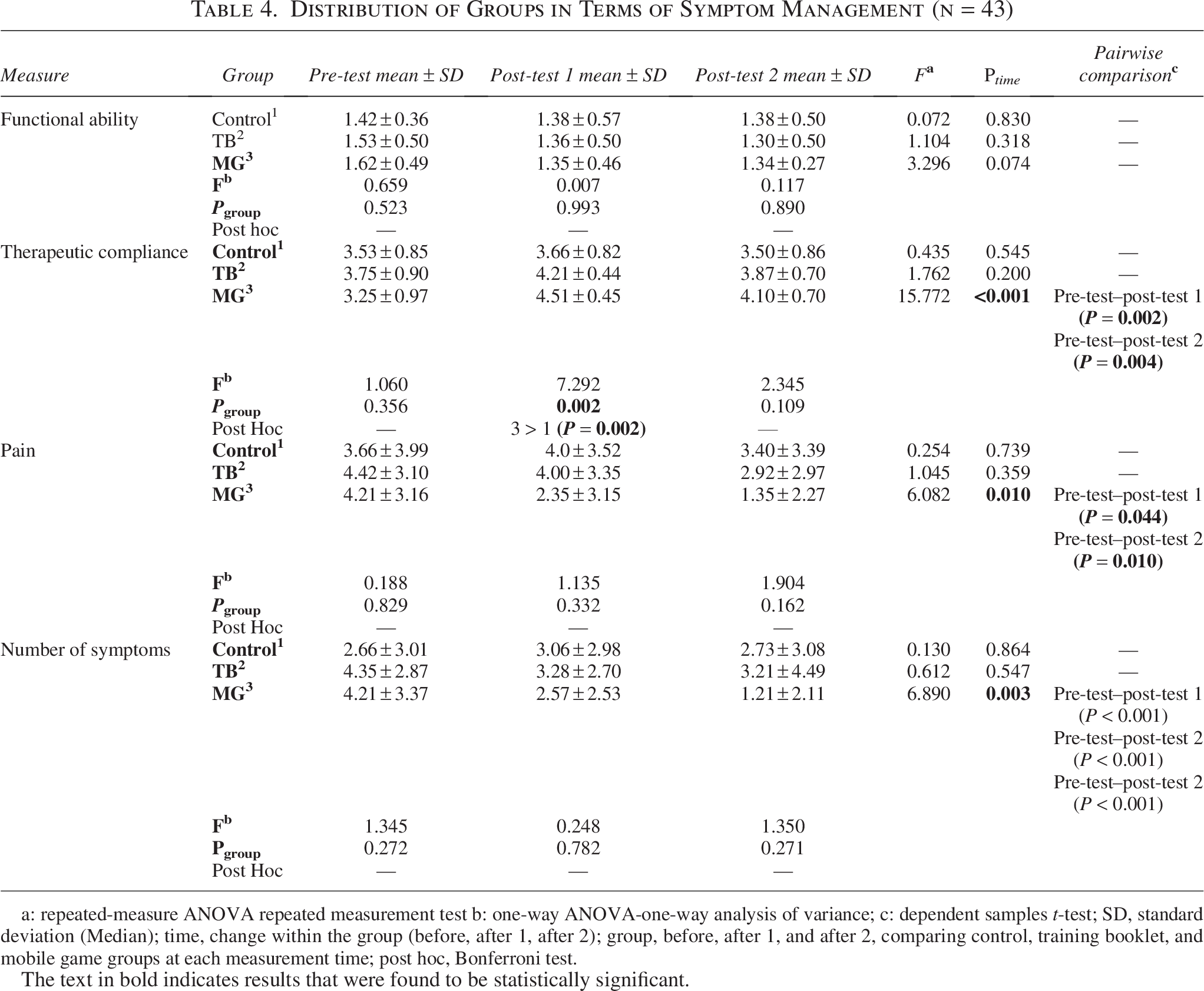
a: repeated-measure ANOVA repeated measurement test b: one-way ANOVA-one-way analysis of variance; c: dependent samples t-test; SD, standard deviation (Median); time, change within the group (before, after 1, after 2); group, before, after 1, and after 2, comparing control, training booklet, and mobile game groups at each measurement time; post hoc, Bonferroni test.
The text in bold indicates results that were found to be statistically significant.
Distribution of the Groups’ Total and Sub-Dimension Quality of Life Score Averages (n = 43)
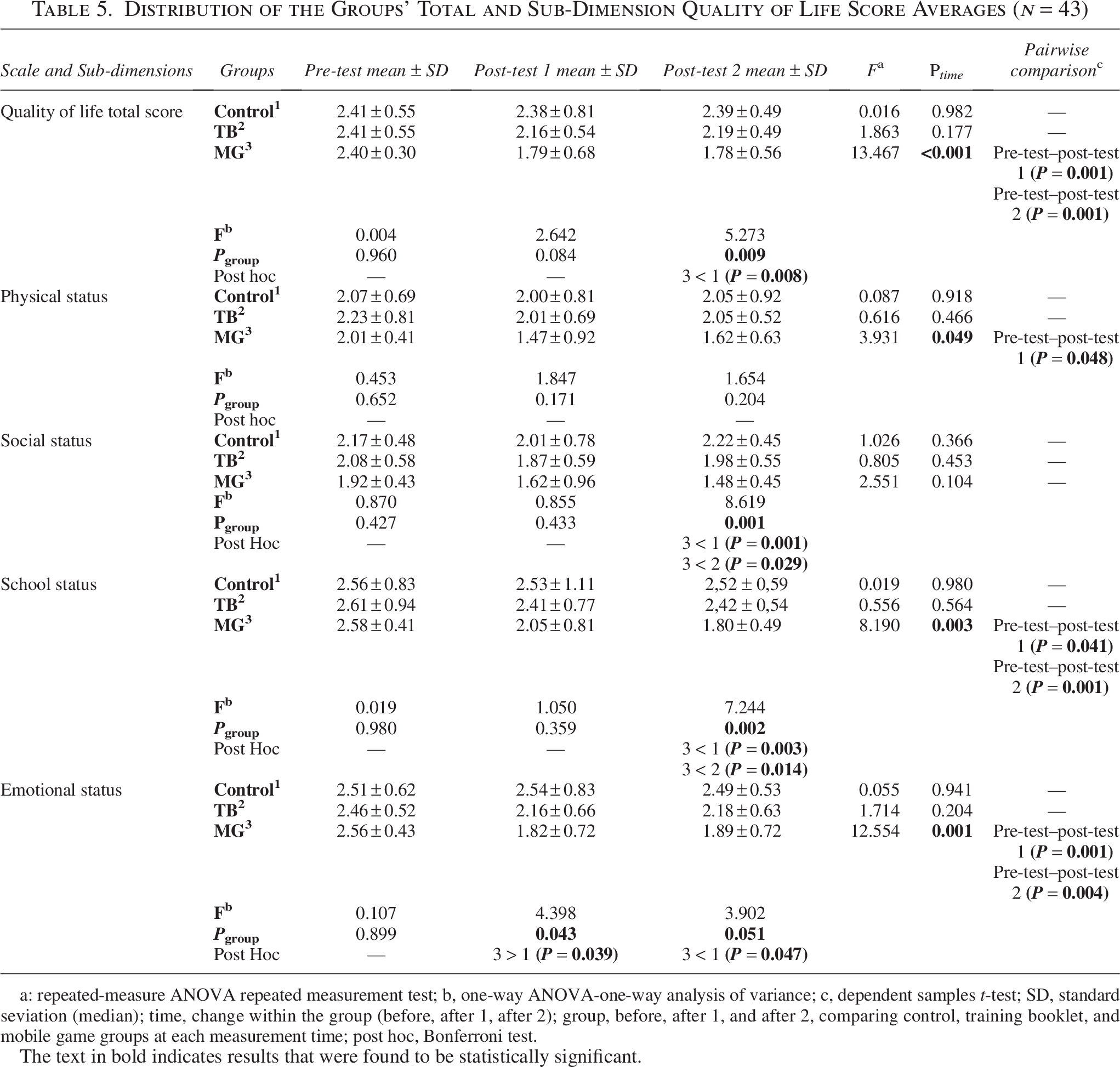
a: repeated-measure ANOVA repeated measurement test; b, one-way ANOVA-one-way analysis of variance; c, dependent samples t-test; SD, standard seviation (median); time, change within the group (before, after 1, after 2); group, before, after 1, and after 2, comparing control, training booklet, and mobile game groups at each measurement time; post hoc, Bonferroni test.
The text in bold indicates results that were found to be statistically significant.
Discussion
This study examined the effects of education using MG or TB on self-efficacy, symptom management, and HRQoL in children with FMF. The findings indicated that MG had positive effects on self-efficacy, symptom management, and HRQoL, whereas TB increased self-efficacy only at post-test 1, with no changes across all measures in the control group. These results provide important information regarding the use of technology-based educational interventions such as MG in improving disease management and quality of life in children with FMF.
Self-efficacy
Solving problems related to chronic disease requires high self-efficacy. 24 In the study, it was determined that MG and TB increased self-efficacy, and because the effect of MG continued over time, it could be said that it was a more effective method than TB. MG may have increased the coping power of children by helping them understand the symptoms better, and thus children may have been less affected by the distress caused by the symptoms and their self-efficacy may have increased. Education or behavioral methods increase the self-efficacy of children with chronic diseases.33,34 When studies conducted on children with chronic diseases were examined, it was seen that motivational interviewing, which is a good method for providing behavioral change, increased self-efficacy, 35 education booklets increased the HRQoL and disease self-efficacy in asthma, 34 an asthma management education program increased asthma management, self-efficacy, and disease control, 36 and an interactive education method increased disease knowledge, self-efficacy, and HRQoL in epilepsy. 37 Studies in the literature have shown that self-efficacy is closely related to disease adaptation, disease management, and HRQoL.33,34 Teaching strategies aimed at promoting self-efficacy may also promote self-management because self-management and self-efficacy are significantly related. 11 In this case, we can say that the MG group’s disease self-management also increased more.
Symptom management
Ensuring compliance with medical treatment and regular medication use, increasing the ability to cope with stress, and increasing supportive practices during attacks are important in providing symptom management.6,10,38,39 The functional ability measure is related to the physical difficulty that occurs during attack periods and because the children’s attack states were similar in all measurements, MG and TB may not have affected the functional ability score. In addition, functional ability is a concept that is affected and can change in the long term, and we think that the period in which we collected data may have been insufficient for this change. In our study, it was determined that only the pain score and symptom count of the MG group decreased over time and the therapeutic compliance scores increased. The number of children in the MG group who had no symptoms increased in post-test-1 and the number of children who stated that they had improved significantly since the last follow-up in post-test-2. The education given for 1 month with MG for disease control may have prevented the children from making the mistakes they had previously made in their daily lives and thus prevented their symptoms from recurring. Regular medication use and compliance with treatment provide symptom management by keeping attacks under control. 39 The fact that the medication compliance increased among children in the MG group and improved significantly after the last follow-up in our study also supports this result.
It is thought that as children practice disease education, they will be more successful in symptom control and will be able to cope more easily with the low HRQoL caused by symptoms. 9 In the study, most of the children in the MG group, compared with those in the TB group, stated that they applied the information they learned from the education method and wanted to continue applying it. Considering that the number of symptoms in the MG group decreased significantly in post-test-2, it was understood that the children continued to apply what they learned from the game. This situation shows that MG provides permanent learning by increasing the interest and motivation in the subject and is effective in symptom management. 18 Similar to our study, Karakul et al. 18 determined that mobile games increased the skills of inhaler use and reduced symptoms and treatment requirements of children with asthma. Unlike our results, in the study of Yıldız et al., 12 no difference was found between the groups in terms of symptom managements in children with cancer aged 10–16 years who were trained with an education booklet and a video game. Because age is an important factor depending on the education method, this difference may be due to the ages of the children in the sample group. Traditional education focuses on knowing rather than doing, whereas digital games allow players to learn by doing and help them develop real-world skills with transferable knowledge. 18 Thus, it supports positive behavioral change by improving the individual’s understanding of the disease and treatment.14,40 MG increased the knowledge level of children with FMF and provided positive behavioral changes that were reflected in their daily lives; medication compliance increased, and the number of pain and symptoms decreased. These results show that MG offers a more effective and motivating approach to symptom management than traditional education.
HRQoL
It is known that chronic diseases with attacks such as FMF negatively affect areas such as school, social life, and psychological status, reducing HRQoL.3,4,8,10,25 In the study, MG continued its effect over time by decreasing the mean total score of HRQoL immediately after the application. In two different studies, similar to our study, the HRQoL of children with cancer 12 and asthma 18 in the MG group was found to be higher than in the control groups. Kaçan et al. 10 determined that the HRQoL of adolescents with FMF who were informed about disease management using an education booklet increased. The reason why the HRQoL of the TB group did not change in our study may be that our sample was younger than in study by Kaçan et al. 10 Adolescents may be willing to read printed materials, but interactive methods such as games are more attractive for younger children. 13 High self-efficacy in chronic disease is a factor that increases therapeutic compliance and HRQoL. 41 In our study, the therapeutic compliance and HRQoL of the MG group, whose self-efficacy increased more, were better and the disease status improved significantly after the last follow-up.
In our study, it was found that the physical condition sub-dimension score of the MG group decreased immediately after the application. In a study, the physical status of children who had fewer attacks per year was found to be better than those who had more attacks. 6 Although the follow-up period of our study was too short to follow the number of attacks, the decrease in the pain levels and symptom counts of the children in the MG group showed that MG positively affected their physical well-being. In addition, the fact that the number of children who had no symptoms after the application decreased in the MG group was an important finding showing that their physical status was better. As in the study of Yıldırım et al., 6 the most affected area in our study was the school status sub-dimension. MG decreased the school status and emotional status sub-dimension scores immediately after the application and continued its effect over time. Missing school due to routine hospital visits and unplanned emergency room visits due to attacks are the most important factors that negatively affect children’s school status. 6 In this direction, the fact that children with increased compliance with medication and decreased pain and symptom numbers had fewer school problems supports the consistency of our findings.
In FMF, good education and compliance with medication have been shown as a factor that reduces anxiety levels. 42 In our study, the fact that the emotional status of the children in the MG group, whose compliance with medication increased, was also good was consistent with the literature. Similar to the TB group, Kaçan et al. 10 also determined that education given to adolescents with FMF with an education booklet did not change their anxiety scores. The authors attributed this situation to the decrease in the effect of the education over time because no reinforcement education was given during the 2-month follow-up period. However, in our study, despite regular training, the emotional state did not change in the TB group. This finding is important because it shows that TB is not as permanent as MG even with regular education. The area least affected in our study was the social status sub-dimension, and there was no change in all group. We think that the follow-up period may have been insufficient to create a large difference in the social area, which was already good at the beginning.
Strengths and limitations
The strengths of the study were that it was a randomized controlled study, that it was the first known study to use MG in children with FMF, and that repeated follow-ups were performed. The limitations of the study were that the study data were collected in a single center, that children were not able to choose their educational method because they were randomly assigned to groups, and that the game could only be played on Android devices. Also, masking could not be performed because the interventions were applied under the supervision of the researcher. The researchers monitored the number of times the children in the MG group entered the game via email, but this was not possible for the TB group. The TB group may have read the booklet more or less than requested and may have reported to the researchers that they had read the required amount. The fact that the researchers were unable to control for this is another significant limitation.
Conclusion and recommendations
Disease information provided through an MG increased the therapeutic compliance of children with FMF and supported the reduction of the number of symptoms and pain during attack periods. MG facilitated children’s learning as an entertaining and informative method and increased the retention of information. The study shows that playing an educational MG for FMF positively affects disease self-efficacy and HRQoL up to 8 weeks after the intervention and thus may be an effective tool for disease self-management. It is clear that TB, which is one of the traditional education methods, is not interesting for children and is unsuccessful due to lifestyle changes. Methods such as MG, which have no time or place limitations in disease education and allow access for children whenever they want, need to be made widespread. However, although the study highlights the positive aspects of MG use, age can be considered a significant limitation in interpreting these findings. Especially in younger age groups, the duration of exposure to MGs and the type of content can lead to developmental differences. Therefore, recommendations regarding mobile phone and MG use should be considered within age-appropriate limits and recommended under parental supervision.
In this respect, MGs can be considered as effective and sustainable digital tools in supporting children’s disease self-management. The use of MGs as educational materials in clinical practices can provide effective guidance for both children and their families in outpatient clinic interviews, hospital education, and home care processes. Nurses can increase the active participation of children in the management of chronic diseases by presenting such tools with a child-friendly approach. However, studies with longer follow-up periods are important to evaluate the permanence of these findings.
Clinical Trial Registration
Clinical trial registration for this study was completed on 08.08.2023. Clinical Trials ID: NCT05980780.
Authors’ Contributions
G.K.A. and B.M.: Contributed to the conception and design of the study. G.K.A.: Performed literature screening, drafted the article. G.K.A.: Collected and assembled data. G.K.A. and B.M.: Performed the analysis. G.K.A. and B.M.: Wrote the main article text. All authors reviewed the article. All authors contributed to article revision and read and approved the submitted version.
Footnotes
Acknowledgments
The authors would like to thank all the children who participated in the study, as well as Associate Professor Selçuk Sevgen and Onur Saltan for their support in the development of the mobile game.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research and/or authorship of this article.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.