
Abstract
Introduction:
Hospitalized patients and their caregivers experience anxiety and fear, which are associated with medical noncompliance and delayed medical care. While virtual reality (VR) is a safe and effective therapeutic adjunct in reducing distress and increasing cooperation, design aspects that contribute to software effectiveness remain limited. This prospective, observational study evaluated VR elements that increased awe, a psychological state correlated with improved behavior, satisfaction, and anxiolysis.
Methods:
Fifty-five patients (ages 6–25 years) and 65 parental caregivers (ages ≥18 years) at a quaternary care academic pediatric hospital interacted with a custom-developed VR program comparing design elements: sound (audible compared to mute), involvement (active compared to passive), and perspective (first person compared to third person) for 15 seconds each. Within-subject outcomes investigated included self-reported awe, perceived vastness, perceived need for accommodation, and engagement. Data were analyzed using repeated-measure analysis of variance tests.
Results:
Audible sound increased perceived awe and need for accommodation in adults, while the third-person perspective improved the need for accommodation in patients and adults. Active or passive involvement did not affect perceived awe nor aspects of awe. All measures of awe were positively correlated with game engagement.
Discussion:
When software designers and clinicians are designing and selecting VR applications for patients and their caregivers, third-person perspectives may be considered for all audiences, while audible sound settings are optimal for adult audiences.
Introduction
Anxiety and fear are common among hospitalized patients and caregivers, leading to withdrawal, lack of cooperation, and aggression.1–3 These responses delay medical care and detract from the patient experience. 4 Traditional anxiolytics include pharmacotherapy, education about upcoming procedures, child-centered therapy by certified child life specialists (CCLS), and parent-present inductions of anesthesia.5–10
Virtual reality (VR) is a safe, effective, and practical adjunct to reduce anxiety in patients and caregivers.11–16 Given the side effects of pharmacological agents and the limited availability of CCLS, VR has emerged as a low risk, affordable alternative that increases patients’ sense of agency and promotes compliance.9,11,17,18 VR has been increasingly implemented worldwide across inpatient and outpatient settings, including applications in venous access, dental procedures, and burn care.11–16 However, many VR applications are developed by commercial entities without rigorous clinical validation, resulting in heterogeneity in efficacy outcomes and a lack of standardized protocols (e.g., variability in hardware configurations, scenario fidelity, and interaction mechanisms) across studies. 19 In addition, usability challenges and variable user engagement have been reported and may limit effectiveness or increase attrition in certain populations. 20 Collectively, these limitations suggest that anxiety reduction alone may not fully capture the therapeutic mechanisms of VR, underscoring the need to examine additional affective and cognitive outcomes that may contribute to its clinical benefit.
One such outcome is awe, a multifaceted emotion encompassing reverential respect intertwined with wonder. 21 Interest in awe has grown across the humanities, social sciences, and psychology, where it is defined by two key components: perceived vastness (PV) and need for accommodation.22,23 As outlined in Piaget’s theory of cognitive development, PV refers not only to physical scale but also to conceptual or experiential magnitude that exceeds an individual’s current frame of reference, while the need for accommodation describes the cognitive process by which existing mental schemas are modified to integrate novel or complex information.21–23 Within clinical contexts, these components are particularly relevant, as experiences that elicit vastness and require accommodation may shift attentional focus away from immediate stressors, disrupt maladaptive cognitive patterns, and foster meaning-making, thereby contributing to reductions in anxiety and depressive symptoms and increases in positive affect and well-being.24–26 It alleviates daily stress, stimulates curiosity, and promotes deeper engagement, which all contribute to cognitive and emotional enhancement.27,28 The potential for awe to be evoked by VR applications is particularly promising. VR’s immersive qualities heighten feelings of awe and activate the autonomic nervous system, promoting its therapeutic potential as an anxiolytic in medical settings.21,29
Prior studies demonstrate that VR environments can reliably induce awe by presenting expansive, novel, or aesthetically rich stimuli that are difficult to access in real-world clinical settings.21,29 Specific VR design elements may differentially contribute to awe by modulating PV and the need for accommodation. For example, audio enhancement has been shown to enhance immersion and emotional intensity, thereby potentially amplifying perceptual vastness; perspective (e.g., first-person vs. third-person viewpoints) can influence self-relevance and embodiment, which may affect cognitive accommodation; and the degree of user involvement or interactivity may deepen engagement and facilitate schema updating by actively integrating the user into the virtual environment.30–32 Despite theoretical relevance, these design features have not been systematically evaluated in clinical populations, and their contributions to awe and related mechanisms remain poorly understood.
Accordingly, this study was guided by the following research questions: (1) Which VR design elements—specifically audio, perspective, and level of involvement—are most effective in eliciting awe in hospitalized patients and adult caregivers? (2) How do these design elements influence the core components of awe, namely, PV and perceived need for accommodation (PNA)? and (3) To what extent are these design elements associated with user engagement? Addressing these questions may inform evidence-based design principles for VR interventions aimed at optimizing affective and anxiolytic outcomes in clinical settings.
Methods
Design
This was a prospective, observational clinical trial (NCT05743062, 6/29/2023) approved by Stanford University Internal Review Board (IRB-69170) that adhered to STrengthening the Reporting of OBservational studies in Epidemiology cohort study guidelines. 33
Setting
This study was conducted at Lucile Packard Children’s Hospital Stanford (LPCHS), an academic, quaternary care children’s hospital in Northern California containing 365 beds, 16 operating rooms, and 10 preoperative bays. Patients have access to CCLS, anxiolytic medications, and technology-based adjuncts such as tablets and VR. Participant recruitment and data collection were conducted from February 27, 2024, to August 19, 2024.
Participants
Patients aged 6–25 years in preoperative and inpatient acute care areas of LPCHS, and their adult caregivers ≥18 years were eligible. Exclusion criteria included nausea at time of recruitment, history of severe motion sickness, history of seizures, history of facial abnormalities or injuries prohibiting comfortable headset use, vision impairment, hearing impairment, and significant developmental delay. Trained research assistants (RAs) and study investigators recruited participants through in-person solicitation. Eligible patients and their caregivers were sequentially approached for participation as they were admitted to the hospital or preoperatively. There were no financial payments for participation.
Intervention
Participants were seated and equipped with a Quest 2 (Meta, Inc., Menlo Park, CA) displaying Wonder Reef (Stanford Chariot Program, Stanford, CA). 34 While experiencing the Wonder Reef application, participants were immersed in an underwater world. They used virtual magical wands to direct fish to their reef. 34 The benefit of an underwater setting was that it did not have a horizon line, important for shifting orientations in the hospital setting and to reduce the risk of nausea. Variations of the program displayed three VR elements in series, including audio (underwater instrumental music vs. muted), involvement (actively controlling virtual wands to usher fish to their reef vs. passively observing fish swim to their reef), and perspective (first-person perspective with wands directly in front of participants vs. third-person perspective displaying a diver holding the wands) (Table 1). Participants interacted with each of the elements for approximately 15 seconds, balancing the need for immersion with brevity to reduce fatigue and increase practicality in this hospital setting. The software included a random number generator to display the test condition sequences within each element in random order.
Experimental Variables in the Virtual Reality Application

After being fitted with the VR headset, RAs oriented participants to the program. Participants interacted with the element series in a randomized order while seated. After each of the conditions, participants completed three questionnaires: Global Perceived Awe (GPA) survey (Appendix 1), PV survey (Appendix 2), and PNA survey (Appendix 3).29,35 At the end of all conditions, participants completed the Game Engagement Questionnaire (GEQ) (Appendix 4). 36
Variables
The primary outcome examined self-reported awe within each category: audio, involvement, and perspective. Group differences between patients and adult caregivers were also compared. Secondary outcomes compared the three categories and patient and caregiver results in terms of vastness, accommodation, and engagement, which are related to the feeling of awe.22,23 Engagement was also correlated with self-reported awe, vastness, and accommodation to determine whether GPA, PV, and PNA surveys were reliable measures of engagement.
Measurements
The primary outcome was measured through the GPA survey, a Likert scale measuring eight emotions (awe, anger, disgust, fear, pride, sadness, amusement, joy) on a 7-point scale ranging from 1 = Strongly disagree to 7 = Strongly agree (Appendix 1). 29 Each participant experienced three sets of two contrasting conditions. For example, for the set that measured audio, each participant experienced an underwater instrumental audio and a muted version of the VR application in random order. Assuming a small effect size (η2 = 0.025), 40 adult caregivers and 40 patients were needed to achieve a power of 80% with a type I error rate (ɑ) of 0.05. 34
Secondary outcomes were measured through the PV survey, PNA survey, and GEQ.35,36 The PV survey measured four aspects of vastness (What I watched provided me with a deep sense of vastness; I felt small in front of what I watched; I felt meaningless in front of what I saw; I felt my sense of self diminish in front of what I saw) on a 7-point Likert scale. 35 Similarly, the PNA survey measured three aspects of accommodation (It was hard to grasp what was going on; I felt confused and bewildered in front of what I saw; I was struck by the VR) on a 7-point Likert scale. 35 The GEQ posed 19 questions investigating immersion, presence, flow, psychological absorption, and dissociation on a 7-point Likert scale. 36 The GPA, PV, and PNA surveys were selected for this study because of its use in seminal work and its high internal consistency for the latter two (Cronbach’s α = 0.77 and 0.81, respectively). 29 The GEQ was chosen because this scale has shown high internal consistency, too (Cronbach’s α = 0.85). 36
Bias
To reduce bias, participants were blinded to the categories of VR elements that were tested during the trial, and the order within categories was randomised. Data were analyzed by a statistician blinded to the study outcomes.
Statistical methods
Continuous demographic data were reported as means ± standard deviation, and categorical variables were reported as percentages. For primary and secondary outcomes, the interaction effects were analyzed using repeated-measure analysis of variance tests because each participant completed two conditions per category. Corrected P value via the Sidak method accounted for multiple comparisons, ensuring a lower chance of falsely rejecting the null hypothesis when conducting multiple tests. 37 P values <0.05 were considered significant.
Engagement data were analyzed through correlation analyses to obtain Pearson’s correlation coefficient. Pearson’s correlation coefficient, ranging from −1 to +1, was considered weakly correlated at an absolute value of 0.10–0.39, moderately correlated at 0.40–0.69, and strongly correlated at 0.70–0.89. 38 All statistics were conducted through R software v4.4.2 (R Core Team, 2025). 39
Results
Participants
A total of 138 participants were recruited, of whom 120 participants completed data collection (Table 1). Fifty-five were patients, and 65 were adult caregivers. Patients were 13.1 ± 3.8 years, while caregivers were 36.3 ± 9.6 years. Within the patient group, 53% were male, 47% were female; within the caregiver group, 46% were male, 52% were female, and 2% chose not to disclose. Among patients, 42% had zero previous encounters with VR; among caregivers, 40% had zero previous encounters (Table 1). Eighteen participants were not included in the final analysis due to incomplete surveys (N = 15) or inadequate time to complete the intervention (N = 3) (Fig. 1).

VR, virtual reality.
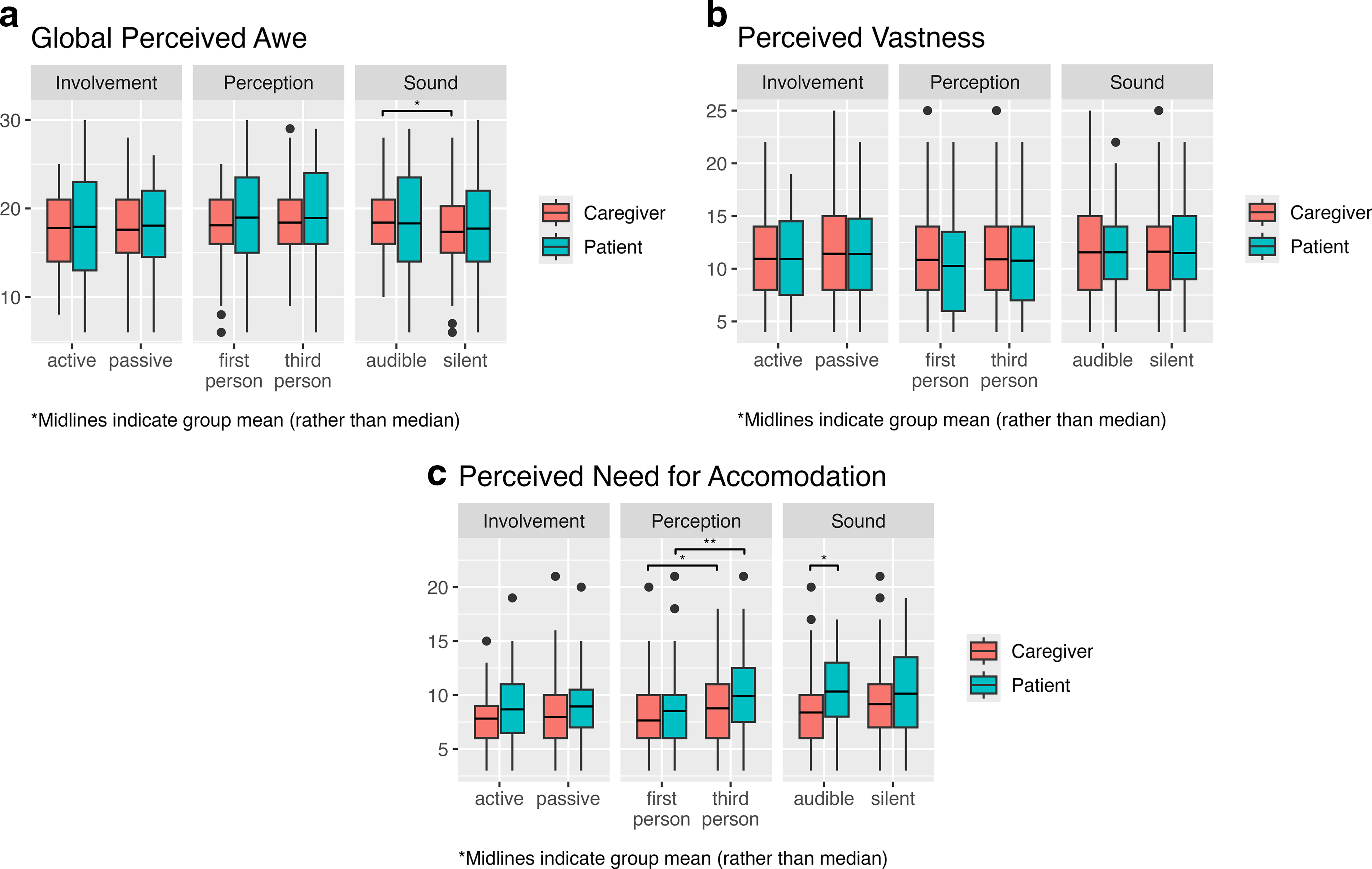
Primary outcome: GPA
The presence of sound did not impact GPA with patients (
Participant Demographics
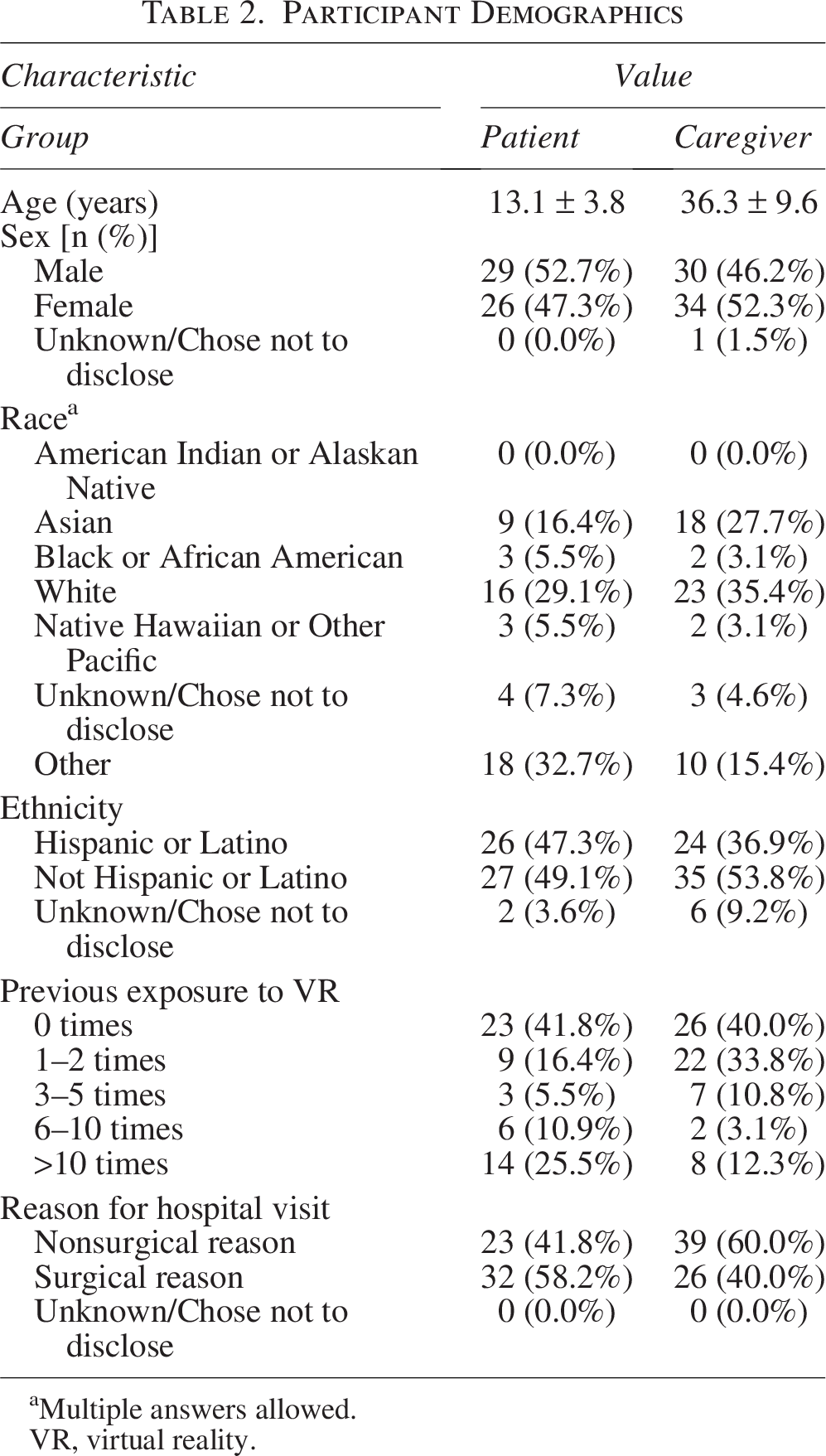
aMultiple answers allowed.
VR, virtual reality.
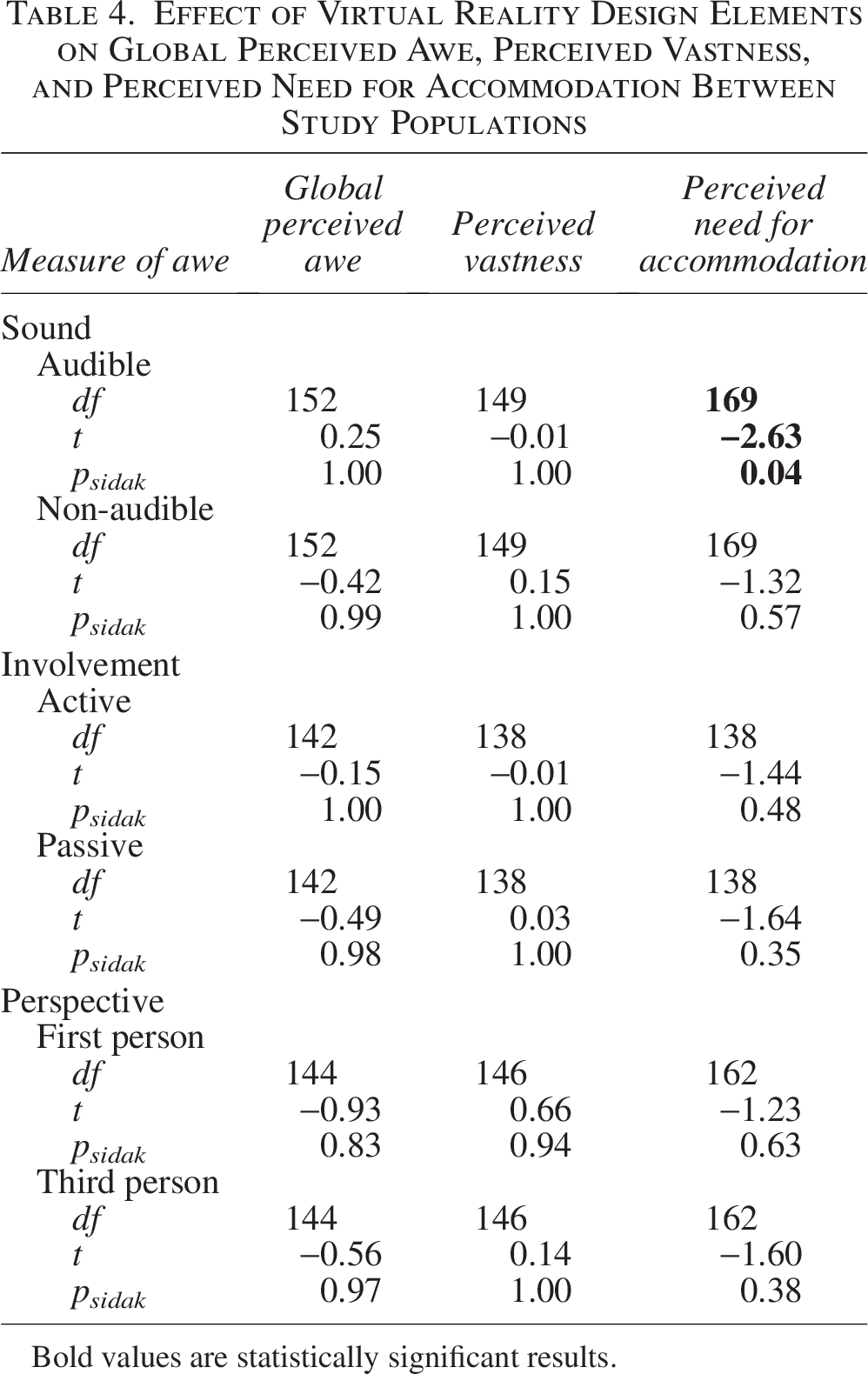
Effect of Virtual Reality Design Elements on Global Perceived Awe, Perceived Vastness, and Perceived Need for Accommodation

Bold values are statistically significant results.
Secondary outcomes: PV, need for accommodation, and engagement
Sound, involvement, and perspective did not affect PV in patients (
The presence of sound and the difference of involvement did not impact PNA for patients (
Between patients and caregivers, there were no differences in engagement with the VR application (
Effect of Virtual Reality Design Elements on Global Perceived Awe, Perceived Vastness, and Perceived Need for Accommodation Between Study Populations
Bold values are statistically significant results.
Correlation Between Global Perceived Awe, Perceived Vastness, and Perceived Need for Accommodation with Engagement

***P ≤ 0.0001.
Discussion
Audible sound increased awe and the need for accommodation in adult caregivers. Third-person perspective increased the need for accommodation in patients and caregivers. There were no changes in PV among VR elements for patients or caregivers. Regarding engagement, all measures of awe were positively correlated with increased engagement, indicating that GPA, PV, and PNA surveys were reliable measures for engagement, most significantly with PNA in patients and PV in adult caregivers.
Adult caregivers demonstrated a greater propensity to experience awe in response to audible sound, potentially due to the role of auditory stimuli in enhancing emotional engagement and promoting relaxation within immersive environments.40–42 Auditory combined with visual inputs increase relaxation response with reduced heart rate, respiration rate, and blood pressure, with improved neural communication on electroencephalogram.40,41 Sound increases the sense of presence and elicits strong emotional responses in VR, contributing to both psychological and physiological benefits.40–42 When designing VR applications for individuals aged 18 years and older—especially in health care settings—the incorporation of carefully selected audio features may improve therapeutic efficacy and emotional engagement. In contrast, muted applications did not affect awe in patients in the pediatric hospital setting, suggesting that auditory components may be nonessential for engagement among pediatric patients. This may reflect a preference among children to hear their environment—such as parental voices—over application audio. Given the common use of VR to promote pediatric compliance, these findings support the use of muted applications that preserve the child’s ability to hear procedural instructions. 43 Communication is central in the design of VR applications for pediatric procedures, and those that do not interfere with parental and clinician interaction are ideal for optimal compliance. 43
Both patients and adult caregivers reported greater feelings of awe when using VR presented from a third-person perspective. This perspective may offer cognitive and perceptual advantages by providing broader spatial context and reducing sensory conflict.44,45 Third-person VR experiences are also associated with a lower risk of simulator-induced nausea, a common barrier to VR adoption in clinical populations.45,46 The enhanced stability and detachment afforded by this viewpoint may facilitate more reflective and immersive engagement with VR content. These findings provide insights for software developers seeking to develop therapeutic adjuncts, as the development of VR applications is resource-intensive and time-consuming.47,48 Certain VR features that do not support optimal outcomes may not justify substantial investment.
For example, user involvement did not have an impact on awe in either patients or caregivers, suggesting that this element may be deprioritized in future application development. This finding contrasts with other studies where active VR engagement more effectively reduced fear or anxiety than passive engagement in pediatric patients during procedures like phlebotomy and peripheral intravenous catheter placement.49,50 The variation in findings may be attributed to differences in procedural context and setting. Passive engagement, characterized by minimal or no controller interaction, may be particularly effective for procedures requiring limited patient movement to ensure procedural success.
Increased awe during therapeutics improves engagement in medical care and the patient experience.24–26 Awe is associated with increased well-being, reduced stress, and a decrease in somatic symptoms such as pain and sleep disturbances.24,25 The mechanisms through which awe promotes mental and physical health include an enhanced sense of meaning, greater social network integration, heightened prosocial behaviors, and decreased sympathetic arousal. 26 These pathways contribute to reduced anxiety and depression while simultaneously enhancing emotional and psychological well-being. 26 This is particularly relevant given the rising prevalence of anxiety and depression, underscoring the urgent need for effective treatments. 51 VR is a proven, effective therapeutic adjunct for anxiolysis.11–15 When selecting VR software for therapeutic purposes, it is critical to carefully consider content that optimally induces awe. This investigation’s findings, taken together with previously studied elements, indicate that the most optimal VR software has high graphic fidelity, fictional settings, audible sound, and a third-person perspective. 34
This study had several limitations. First, the age range was large, which may have obscured differential findings between age groups. However, subgroup age analyses would not have been appropriately powered to draw meaningful conclusions. Second, the study excluded patients under 6 years due to the VR headset’s fit and weight, which limits generalizability to younger children. Third, the VR application was underwater-themed which may have appealed to some participants more than others, potentially biasing the results in an unpredictable direction. Fourth, the study was conducted at a single site, which may restrict the applicability of the findings to populations different from the demographic and cultural characteristics of the LPCHS patient population. Fifth, while the surveys were previously validated, they may not fully capture the nuanced aspects of engagement and awe. To reduce survey fatigue, the number of measures was limited, which means that there may be additional measures that may have identified other differences. Last, the intervention duration for each individual condition was around 15 seconds, which reflects the lower bound of anticipated clinical use (e.g., during brief procedures such as vaccine administration) and was intentionally chosen to capture a minimal yet measurable awe response. However, this assumes that longer exposures would further enhance immersion and awe.
Conclusion
This study demonstrated that the third-person perspective is more effective at increasing awe factors in both patients and adult caregivers, while the presence of sound is more effective in increasing awe factors in caregivers. Involvement did not seem to influence awe in either patients or caregivers. Future investigations will explore differently themed applications and populations beyond Northern California.
Authors’ Contributions
E.M.H.: Conceptualization, methodology, software, investigation, data curation, writing—original draft, writing—review and editing, visualization, project administration, and funding acquisition. A.M.Y.S.: Investigation, review, editing, and project administration. P.L., M.Z.-H., R.F., and K.G.: Investigation, review, and editing. C.J.: Formal analysis, data curation, visualization, review, and editing. S.T.R. and E.W.: Software, resources, supervision, funding acquisition, review, and editing. T.J.C.: Conceptualization, methodology, software, resources, writing—review and editing, supervision, project administration, and funding acquisition.
Footnotes
Author Disclosure Statement
S.T.R., E.W., and T.J.C. are on the board of a nonprofit (Invincikids, Inc.) that seeks to distribute immersive technology to hospitalized children at no cost. They receive no compensation for their roles at Invincikids, Inc. The Stanford Chariot Program has received philanthropic donations from Meta, Inc. and Magic Leap, Inc. S.T.R. has received consultation fees from Apple, Inc. All other authors declare no competing interests or conflicts of interest.
Funding Information
This research was supported by an internal grant from the Medical Scholars Research Program at Stanford University School of Medicine and the Stanford Chariot Program.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.