
Abstract
Objective:
This study aimed to evaluate the effects of a gamified virtual reality (VR) rehabilitation program, using immersive VR combined with conventional conventional physical therapy (CPT), on pain, functional mobility, disability, and balance in individuals with knee osteoarthritis (OA).
Methods:
A randomized controlled trial was conducted on 90 volunteered participants diagnosed with knee OA, equally divided into VR and control groups. VR group received VR + CPT, while the control group received only CPT. Outcome measures included Visual Analog Scale (VAS) for pain, 6-minute walk test (6MWT) for function, Western Ontario and McMaster Universities Arthritis Index (WOMAC) for disability, and the Berg Balance Scale (BBS) for balance. Participants underwent three sessions per week for 6 weeks. Assessments were performed at baseline, after 3 weeks, and after 7 weeks (postintervention). The level of significance was set at P ≤ 0.05.
Results:
The VR group demonstrated greater improvements than the control group, including a 38.6% reduction in pain compared with 26.3% in the control group, and a 39.9% increase in 6MWT distance compared with 19.4% in the control group. WOMAC improved substantially in the VR group (57.9%) compared with the control group (25%). Pain reduction became significantly greater in the VR group in the third week. Significant between-group differences at postintervention (P < 0.001) were observed for VAS, 6MWT, and WOMAC. Both groups demonstrated significant within-group improvements in balance; however, no significant between-group difference was found for BBS (P = 0.090).
Conclusion:
Integrating a gamified VR rehabilitation program alongside CPT significantly reduces pain and improves mobility and knee function in individuals with knee OA. The findings support using VR as an effective adjunct to traditional physiotherapy, improving engagement and clinical outcomes.
Keywords
Introduction
Knee osteoarthritis (OA) is a degenerative joint disease characterized by the progressive deterioration of articular cartilage, leading to pain, stiffness, and functional limitations. 1 It is a significant cause of disability, particularly in older adults, affecting their quality of life and physical activity levels.2,3 Traditional rehabilitation methods often involve physical therapy, focusing on pain relief, improving mobility, and enhancing strength.4,5 However, despite their efficacy, these conventional approaches often face long-term adherence and patient engagement challenges.
Individuals with knee OA commonly report significant pain and disability, leading to decreased physical function and increased reliance on healthcare services.6–8 Standard therapeutic interventions include pharmacological and physical therapy involving exercise, manual therapy, and educational programs to improve patient understanding and promote self-management.5,9 Although these strategies can be effective, they often lack engaging elements that foster sustained patient motivation and adherence to exercise regimens. Evidence suggests that adherence to prescribed exercises is a key predictor of rehabilitation success, highlighting the need for more interactive and enjoyable rehabilitation methods.10–12 Moreover, traditional exercise therapies often require patients to attend in-person sessions at healthcare facilities, demanding considerable time, motivation, and financial resources. 13 Conversely, while more cost-effective, home-based exercise programs frequently suffer low adherence due to limited supervision and access to appropriate resources. 14 These limitations highlight the need for innovative solutions that balance engagement, accessibility, and efficacy.
To address these challenges, virtual reality (VR) technology has emerged as a promising approach to rehabilitation. VR offers a novel approach to rehabilitation by immersing patients in interactive environments that can enhance motivation and engagement. 15 By simulating real-life scenarios that require movement and balance, VR-based rehabilitation programs provide a more dynamic and appealing experience than traditional approaches. Research has shown that VR interventions can significantly improve pain management, physical function, and overall patient satisfaction across various populations, including individuals with neurological and musculoskeletal conditions.15–17 Incorporating game-like elements into rehabilitation exercises has been associated with enhanced motivation and improved adherence to exercise programs. The engaging nature of games encourages users to participate in the exercise, providing an opportunity for consistent practice and improvement.
Several studies have explored the application of VR in knee OA rehabilitation, reporting positive outcomes in pain reduction, functional improvement, and enhanced quality of life.17–19 A randomized controlled trial (RCT) found that participants who engaged in a VR-based rehabilitation program demonstrated significant reductions in pain scores and improved functional mobility compared with a control group receiving standard physiotherapy. 20 Furthermore, studies maintained that VR interventions led to higher patient satisfaction rates than traditional rehabilitation methods, suggesting that incorporating technology into therapy could bridge the gap between treatment recommendations and patient compliance.21,22 On the other hand, some researchers failed to find any superior effect of VR training on pain, disability, and knee range of motion or balance as compared with traditional exercise as a control treatment.21,23–26
The Meta Quest-3 headset was chosen due to its advanced graphics, motion tracking, and real-time feedback, enabling personalized rehabilitation experiences tailored to individual needs. 27 Its stand-alone design eliminates the need for external sensors, making it more practical for clinical and home use than alternatives like the HTC Vive. While its features enhance engagement and confidence during rehabilitation, potential barriers such as cost, technological literacy, and platform access must be considered, especially for older adults and resource-limited settings. 27
Despite the growing evidence supporting VR-based rehabilitation, current research is limited by small sample sizes, short intervention periods, and a lack of long-term adherence data. In addition, previous studies have not consistently examined gamified VR’s impact on balance and functional mobility in knee OA populations. This study aimed to address these gaps by investigating whether a 6-week gamified VR rehabilitation program enhances pain reduction, functional capacity, balance, and joint mobility. The primary hypothesis was that integrating gamified VR with a conventional physical therapy (CPT) program would lead to superior outcomes compared with CPT alone.
Methodology
Study design
This study utilized an RCT design to investigate the effects of a Meta Quest 3-based gamified VR rehabilitation program, combined with CPT, on pain, function, disability, and balance in individuals with knee OA. Ethical approval was obtained from Umm Al-Qura University Biomedical Research Ethics Committee (HAPO-02-K-012-2024-12-2379). The clinical trial was officially registered with ClinicalTrials.gov under the unique identifier (NCT06735963).
Power analysis
A power analysis was conducted by G*power software for Windows to determine the required sample size. Based on a significance level (α error probability) of 0.05, a power (1 − β error probability) of 0.9, using t-test to measure the difference between two independent means (two groups) and an expected moderate effect size (Cohen’s d = 0.7). The estimated effect size was based on two studies on VR in knee OA17,19 and one on chronic OA. 27 An estimated sample size was 88 in two groups. The number of participants in each group was increased for possible dropouts between participants. A sample size of 45 participants per group was deemed sufficient to detect significant between-group differences.
Participants
A total of 150 participants were assessed for eligibility criteria. Based on the American College of Rheumatology criteria, the inclusion criteria were (1) adult participants with age range from 40 to 64 years diagnosed with knee OA (Kellgren and Lawrence grade II or III), 4 (2) patients had knee pain on most days in the last 3–6 months, (3) pain severity above a minimum threshold on a Visual Analog Scale (VAS ≥ 30 mm/100 mm), (4) patients reported some difficulty in daily activities (e.g., walking, climbing stairs). (5) The ability to read and understand Arabic, (6) willingness to participate in the physiotherapy intervention and follow the study protocol. (7) Participants agreed not to take any medication like analgesic during the study period. Exclusion criteria encompassed (1) recent lower extremity surgery or fractures, (2) history of meniscus or ligament tears and other rheumatologic diseases, (3) cardiovascular conditions limiting exercise, balance impairments (e.g., vestibular issues), and visual or auditory impairments, (4) patients who received intra-articular injections (e.g., corticosteroids or hyaluronic acid) in the last 3 months, (5) any concurrent participation in other knee-related rehabilitation programs, and (6) any condition that altered the potential relevance to VR and exercise interventions such as epilepsy and pregnancy (Fig. 1).
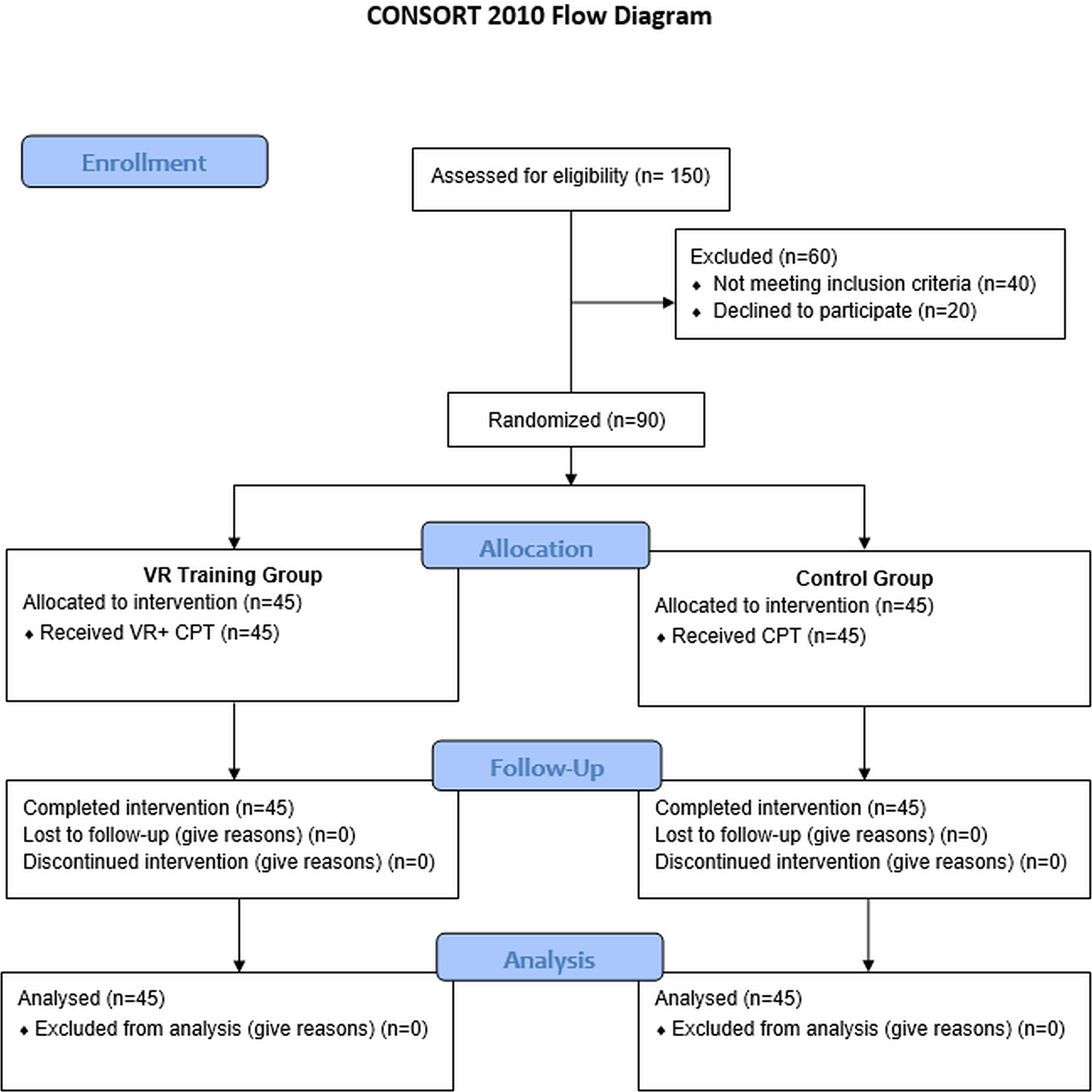
CONSORT flowchart illustrating the participant flow.
Randomization procedures
A total of 90 participants enrolled in the study were randomly assigned using computer-generated block randomization with a 1:1 allocation ratio to ensure balanced group sizes. Allocation concealment was maintained using sealed, opaque envelopes. Allocation concealment was performed by an independent person not involved in the study. Participants were randomly assigned to two groups. Group 1 (VR groups) received a VR rehabilitation program and CPT, and group 2 (control group) received CPT alone and served as a control group. A single-blind study, with assessors blinded to group assignment and patients’ enrolment. Patients signed an informed consent, including their approval of study participation and results publication.
Conventional Physical Therapy Program
Participants in both groups received CPT, which included ultrasound (Combi 400, Gymna unify, continuous 1 MHz, 0.8 W/cm2, 5 minutes), transcutaneous electrical nerve stimulation (TENS) (two electrodes, bilateral symmetrical waveform, 100 Hz, 125 µs, 15 minutes), and exercise therapy. Exercise therapy included unweight-bearing active knee range of motion exercises for 5 minutes and was considered warming up. Stretching of the hamstrings, quadriceps, and calf muscles was performed three repetitions in 10 minutes. Strengthening exercises included isometric quadriceps sets, straight leg raises, short arc quadriceps, and seated knee extensions (with variable weights according to patients’ tolerance). Strengthening was performed 10 repetitions three times in 20–25 minutes. Balance and proprioception training was performed by single-leg stance (3 repetitions), mini squats (10 repetitions) with reach, and heel-to-toe walking along a straight line (2–3 passes). Balance was performed in approximately 5–10 minutes. Patients in both groups were instructed to perform the same CPT program at home. An exercise booklet was given to every patient, including a description, frequency, and repetitions. Exercise compliance was maintained by adherence to checklists. CPT program was performed and supervised by the same therapist for both groups. CPT was performed for 6 weeks, with 18 sessions conducted three sessions per week. Exercise prescription and supervision were performed by the same therapist (M.S.A.).
VR rehabilitation program
In addition to CPT, participants in the VR group received a VR rehabilitation program for a 15-minute each session. The time was recommended in previous studies. Patients in the VR group received the VR-based gamified exercise with the Meta Quest-3 headset.
Two gamified exercise modules were performed: Fruit Ninja and Power Beats VR Games. The Fruit Ninja and Power Beats VR games incorporate engaging, gamified movements, promoting balance, proprioception, and knee stability.
In the Fruit Ninja game, participants interacted in a virtual environment where various fruits were launched into the air, and they had to “slice” using hand and arm movements. As they reach to slice fruits at different angles, participants engaged in core stabilization, weight shifting, and lateral movements. In the Power Beats VR game, participants performed a series of lunges, squats, and punches, requiring simultaneous lower body coordination. As participants punched objects in various directions, they engaged in lateral and rotational knee and hip movements. Sessions were conducted under the supervision of a trained therapist to ensure proper form and safety. VR prescription and supervision were performed by the same therapist (F.M.A.).
Outcome measures
All outcome measures were recorded at baseline, after 3 weeks, and postintervention after 7 weeks. Outcome assessors were blinded to the group allocation to minimize bias during data collection. The same assessor performed each type of assessment.
Pain evaluation
The primary outcome measures were pain measured by the VAS, where 0 represents no pain and 10 describes the highest pain level imaginable. Its validity and reliability have been well-established, particularly in conditions like knee OA.28–30 VAS evaluation was performed by A.F.
Functional mobility evaluation
Functional mobility was measured by the distance walked in 6 minutes (6MWT). The 6MWT is a widely used functional test to assess submaximal aerobic capacity and physical endurance. In patients with knee OA, it is also a practical measure of functional mobility and overall physical performance. The 6-MWT is a highly reliable and valid measure of functional capacity in patients with knee OA.31,32 Functional mobility evaluation was performed by M.S.A.
Functional disability evaluation
Functional disability was evaluated using the Western Ontario and McMaster Universities Arthritis Index (WOMAC). WOMAC is one of the most widely used, validated, and reliable patient-reported outcome measures for evaluating pain, stiffness, and physical function in individuals with knee OA.33,34 It has 5 items for pain, 2 for stiffness, and 17 for measuring physical function. In the current study, the authors used an Arabic version of WOMAC, which is considered a reliable tool for evaluating knee symptoms/function. 35 Functional disability evaluation was performed by M.S.A.
Balance evaluation
Balance was assessed using the Berg Balance Scale (BBS). BBS is a clinical test to assess static and dynamic balance abilities in older adults and individuals with knee OA. 36 It has a 14-item scale that assesses balance through various functional tasks. The lower the score, the greater the risk of fall with high intra- and inter-rater reliability. 37 Balance evaluation was performed by A.F.
Statistical analysis
All data were analyzed using the Statistical Package for the Social Sciences (SPSS, version 25.0 for Windows). Data normality was examined with the Shapiro–Wilk test, and homogeneity of variances was evaluated using Levene’s test. Descriptive statistics were presented as mean ± standard deviation (SD) for continuous data and as frequencies (percentages) for categorical data.
At baseline, independent samples t-tests were used for normally distributed continuous variables, while Mann–Whitney U tests were used for non-normally distributed variables. Chi-square (χ2) tests were applied for categorical variables such as gender.
To assess within-group changes over time (baseline, week 3, and postintervention week 7):
For normally distributed data (6MWT, WOMAC, and BBS), a repeated measures analysis of variance (ANOVA) was used, followed by Bonferroni-adjusted post hoc tests. For non-normally distributed data (VAS), the Friedman test was applied, followed by Wilcoxon signed-rank post hoc tests with Bonferroni correction.
To examine between-group differences (VR vs. control) at each time point, independent samples t-tests were used for normally distributed data and Mann–Whitney U tests for non-normally distributed data. Effect sizes (Cohen’s d) were calculated for between-group differences and interpreted as small (0.2), medium (0.5), or large (0.8). The level of statistical significance was set at P ≤ 0.05 for all analyses.
Results
A total of 90 participants completed the study, 45 in the VR group and 45 in the control group. There were no significant differences in baseline characteristics, including age, gender distribution, or body mass index, indicating successful randomization (Table 1).
Participants Demographic Data
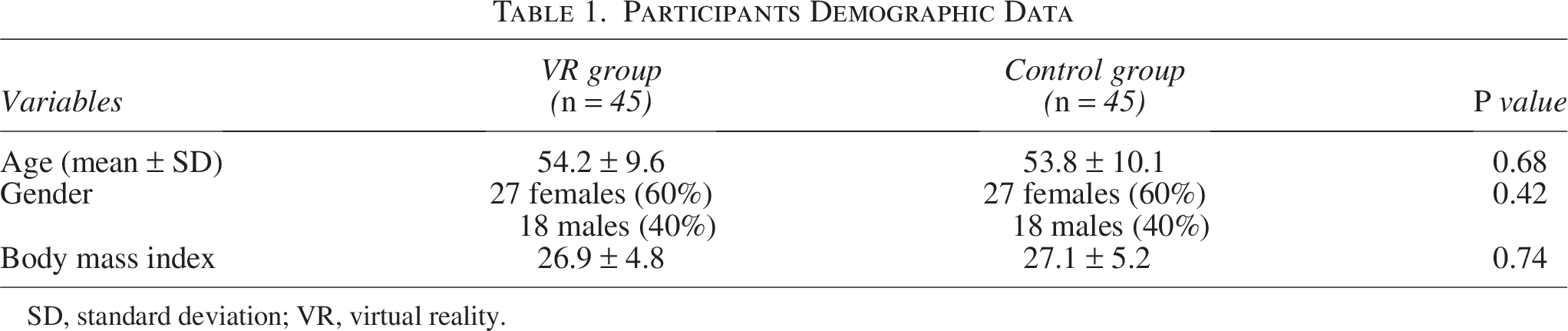
SD, standard deviation; VR, virtual reality.
The Shapiro–Wilk test indicated that the VAS data were non-normally distributed, while 6MWT, WOMAC, and BBS met normality assumptions. Accordingly, VAS was analyzed using the Friedman test and Wilcoxon signed-rank post hoc tests, while 6MWT, WOMAC, and BBS were analyzed using repeated measures ANOVA with Bonferroni post hoc comparisons.
Between-group differences at each time point were assessed using independent samples t-tests or Mann–Whitney U tests, as appropriate.
Both groups showed significant within-group improvements across all outcome measures. The VR group demonstrated a greater reduction in pain (VAS) and significant improvement in 6MWT and WOMAC scores compared with the control group, particularly at postintervention (week 7). Between-group comparisons revealed significant differences in VAS, 6MWT, and WOMAC scores at week 7, favoring the VR group (P < 0.001).
Although BBS scores improved significantly within both groups over time (P < 0.001), the between-group difference was not statistically significant at any time point, suggesting that both interventions effectively enhanced balance. The corresponding effect sizes indicated a large effect for pain reduction (Cohen’s d = 0.80), moderate effects for function and disability (Cohen’s d = 0.60–0.85), and a small-to-moderate effect for balance (Cohen’s d = 0.40).
The results of the comparative analyses between the VR and control groups across all outcome measures are summarized in Table 2.
Comparison Between the VR and Control Groups on Pain, Function, Disability, and Balance Among Treatment Groups
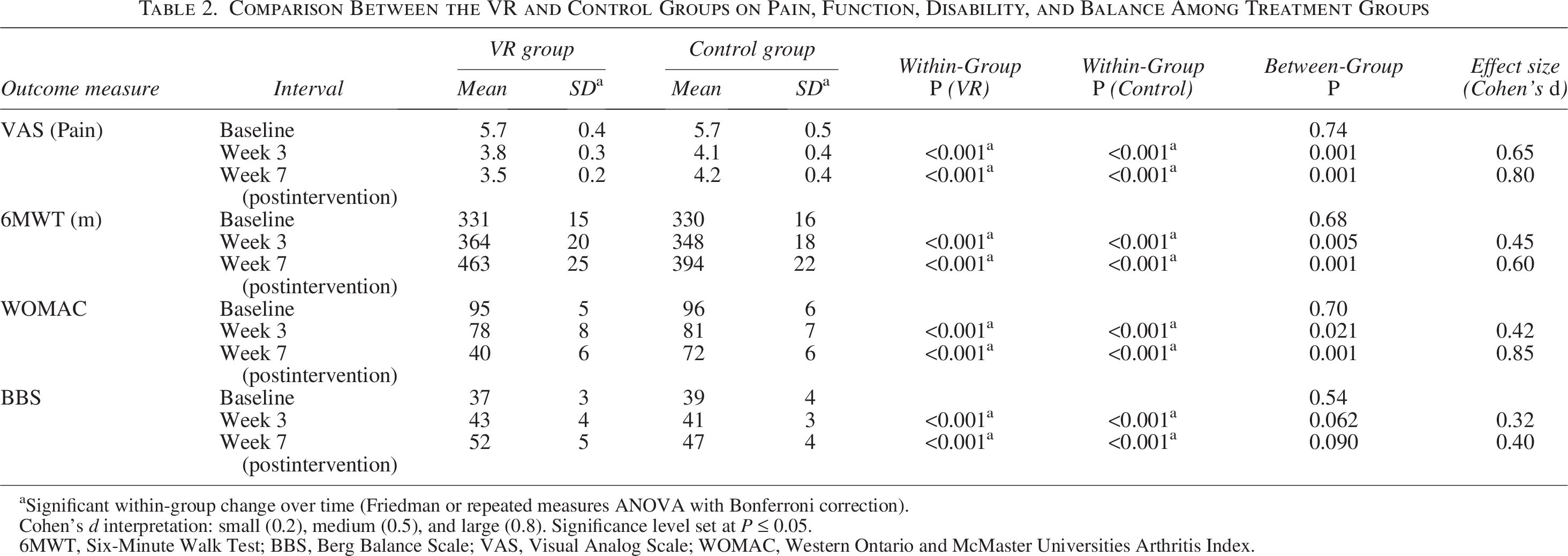
Significant within-group change over time (Friedman or repeated measures ANOVA with Bonferroni correction).
Cohen’s d interpretation: small (0.2), medium (0.5), and large (0.8). Significance level set at P ≤ 0.05.
6MWT, Six-Minute Walk Test; BBS, Berg Balance Scale; VAS, Visual Analog Scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Discussion
This study evaluated the effects of a gamified VR rehabilitation program using the Meta Quest 3 on pain, functional capacity, disability, and balance in individuals with knee OA. The VR group showed greater pain reduction with a greater improvement in walking capacity and joint function than the control group. Significant between-group differences were observed for VAS, 6MWT, and WOMAC scores in the 7th week. Both groups showed significant within-group improvements in balance, but no between-group differences were observed. The findings indicate that integrating VR-based exercises with CPT significantly improved clinical outcomes, particularly for pain reduction, functional performance, and joint mobility. These results align with prior research, highlighting the efficacy of VR interventions in musculoskeletal rehabilitation.17,19
The significant decrease in VAS scores in the VR group compared with the control group highlights the effectiveness of immersive VR in managing pain. Previous studies suggest that VR can reduce pain perception by providing an engaging distraction that modulates pain pathways through neuroplastic changes. 17 This supports the hypothesis that interactive VR environments can complement traditional pain management techniques by improving adherence and engagement.16,38 The result of the current study supports the previous finding that VR training significantly reduced pain intensity in patients with chronic knee OA, compared with the sensory-motor and conventional training. 27 Moreover, VR showed greater pain relief than standard exercise post-total knee arthroplasty. 39 The extended pain relief effect at postintervention was concurrent with another study, which showed that VR intervention provided longer lasting analgesia after total knee arthroplasty than control interventions. 40 The reduction of pain may be attributed to the distracting attention of VR, which modulates sensory input. Similar to mirror therapy, this may influence the neuroplasticity and pain perception pathways,41,42 previously demonstrated in conditions like phantom limb pain and neuropathic pain. 19
The improvements observed in the 6MWT in the 7th week indicate that the VR-based program contributed to enhanced endurance and mobility. Although no significant differences were detected in the third week, the results at the 7th week suggest that prolonged exposure to gamified VR exercises improves walking capacity over time. This is consistent with studies reporting increased endurance following VR interventions incorporating dynamic and repetitive lower-limb movements.16,19,20 As reported in literature, the increased endurance needs time to develop significant changes postexercise.19,20
WOMAC scores in the VR group demonstrated significant improvement, indicating improved knee mobility and reduced disability and joint stiffness. The engaging nature of the VR exercises likely contributed to better adherence, leading to superior functional outcomes. The integration of rhythm-based tasks and proprioceptive feedback in the VR program aligns with recommendations that rehabilitation programs targeting knee OA should include controlled movement patterns to enhance joint stabilization and proprioception.20,43
The current result was in line with the result of another study that reported that VR training significantly improved knee function, joint proprioception, and quality of life in patients with chronic knee OA compared with conventional and sensory-motor training. 27 Lin et al. found that VR training improved physical functional performance more than standard therapeutic exercises in patients with knee OA. 24 This improvement may be due to pain reduction, which facilitates movement or engagement and motivation, promoting visual and auditory feedback and increasing patient motivation, adherence, and active participation during rehabilitation exercises.19,24
While both groups demonstrated significant within-group improvements in BBS scores, no significant between-group differences were found; this may be attributed to the control group receiving standard balance-focused exercises as part of the CPT program. In addition, the relatively short intervention period may not have been sufficient to detect substantial between-group differences in BBS scores. Nonetheless, the experimental group’s performance highlights the potential benefits of interactive VR for improving dynamic balance. Previous research emphasizes that VR programs incorporating lateral and rotational movements can enhance neuromuscular coordination, which is critical for maintaining postural stability.15,16,38,44
The Fruit Ninja and Power Beats VR games incorporate engaging, gamified movements promoting balance, proprioception, and knee stability. These interactive exercises help patients overcome the repetitive nature of CPT by providing an immersive experience that motivates regular participation and adherence. Both games offer a variety of movement patterns that target core stability, weight shifting, and functional coordination, which are essential for knee OA management.
Across both groups, participants were expected to complete 18 sessions over the 6-week intervention period (total expected sessions = 1620). Adherence to the intervention was high in both groups. In the VR group, seven participants missed between two and four sessions, corresponding to an estimated attendance rate of approximately 97%–98%. In the control group, three participants missed between two and four sessions each, resulting in an estimated attendance rate of 98.5%–99.3%. No participants discontinued the intervention, and all completed the postintervention assessment.
The results highlight the potential for gamified VR programs to improve adherence and clinical outcomes in knee OA rehabilitation. The significant improvements in pain and functional mobility suggest that VR’s immersive and interactive nature may enhance patient engagement, leading to more meaningful rehabilitation gains. This intervention may be particularly valuable in outpatient and home-based settings where adherence to conventional exercise programs is a common challenge. However, unlike prior studies that primarily focused on pain outcomes, this study demonstrates significant improvements across multiple domains, including disability and endurance. These findings suggest that combining rhythmic, gamified movements with a CPT program may provide synergistic benefits. However, cost and technological literacy remain barriers to implementing VR rehabilitation widely. Addressing these barriers through low-cost hardware options and patient training modules could enhance adoption in community clinics.
Conclusion
This study demonstrates that a VR-based gamified rehabilitation program, combined with a CPT program, significantly reduces pain and disability and improves functional performance in individuals with knee OA. The findings highlight the potential of immersive VR technology to enhance adherence, engagement, and clinical outcomes in rehabilitation. Including gamification fosters motivation and encourages consistent participation, making it a valuable adjunct to traditional therapy.
These results support the feasibility and efficacy of integrating gamified VR into clinical practice for managing knee OA. Future research should explore the long-term effects of VR-based rehabilitation, assess its cost-effectiveness, and investigate its applicability in diverse populations, particularly older adults. Expanding VR to home-based rehabilitation programs could improve accessibility and patient outcomes, paving the way for innovative, patient-centered care solutions.
Limitations and future research
Participants reported mild dizziness in three cases during the first two sessions, which resolved and completed the sessions without further incidents. No serious adverse events were recorded, and all participants completed the program without requiring modifications to the VR protocol. Despite its promising results, this study has limitations. The 6-week intervention period may not reflect the long-term sustainability of the observed improvements. The lack of a long-term follow-up was considered a limiting factor. In addition, the sample was limited to participants aged 40–64, which may limit generalizability to older populations. The time for VR gaming in VR group was not compensated for the CPT group by placing additional exercises that allow the participants to practice at the same time as in VR group. Although the previous literature did not apply this compensation, unequal time for exercise practicing may be considered as a limiting factor. Future research should explore more extended intervention periods, more extensive multicenter trials, and the cost-effectiveness of implementing VR-based rehabilitation in clinical practice.
Ethical Approval
Ethical approval was obtained from the Local Committee for Biological and Medical Ethics at Umm Al-Qura University (NJDD0110253). The clinical trial was officially registered with ClinicalTrials.gov under the unique identifier (NCT06735963).
Footnotes
Author Disclosure Statement
The authors declare no competing interests. All authors confirm that no financial or personal relationships could have influenced the work reported in this article.
Funding Information
The authors declare that no funding was received for this research.