
Abstract
Immersive virtual reality (VR) has emerged as a promising application for neurological conditions in hospital care. This study explores the experiences of patients with neuromuscular diseases using a virtual supermarket to entertain patients in a real-life task. Twelve patients from the NeuroMuscular Omnicentre in Milan were interviewed to evaluate their impressions after interacting in a fully immersive virtual environment. Questions were related to first impressions, positive and negative aspects, willingness to use the application again, suggestions for improvement of the game, and general reflections; a thematic analysis of the replies’ content was performed. The main topics identified were engagement, technological features, sensory experience, usefulness, improvement, and recommendation. The results indicate that the VR experience was generally well received, with participants describing it as enjoyable, immersive, and relaxing. Some expressed curiosity about this new technology, while others appreciated the feeling of immersion and distraction from their condition. However, minor annoyances were reported, such as the headset’s weight and the need for an enhanced interaction. Suggestions included improving interaction, fine-tuning visual and auditory elements, and optimizing comfort. Overall, the study highlights the potential of immersive VR as a valuable tool in hospital care to provide enjoyable moments for neuromuscular patients. Further studies could expand the sample size and explore how different sociodemographic variables impact user experience. Longitudinal studies might also assess the sustained effects of VR interventions on patients’ well-being, mood, and overall quality of life during extended hospital stays.
Introduction
Neuromuscular diseases (NMDs) affect the peripheral nervous system and muscles, leading to significant impairment in voluntary movement and, in severe cases, complete paralysis. 1 NMDs include amyotrophic lateral sclerosis (ALS), congenital muscular dystrophies and myopathies, and spinal muscular atrophy. These patients face significant challenges not only on a physical level but also from psychological and social perspectives.2,3 The chronic and progressive nature of these conditions often necessitates frequent hospitalizations, continuous medical monitoring, and rehabilitation.4,5 These repeated and extended hospital stays can contribute to feelings of isolation and anxiety, worsening mental health and overall well-being. Furthermore, the progressive loss of mobility and independence associated with these disorders can affect social interactions and reduce participation in daily activities, leading to a substantial decline in quality of life (QoL).6,7 In this context, providing access to entertaining and engaging activities becomes essential to alleviate mental and emotional strain.8–10 Entertainment during hospitalization is a crucial factor for the psychological well-being of different types of patients,11,12 contributing to stress reduction and enhancing treatment adherence. Moreover, a relaxed atmosphere helps patients feel more at ease, reducing anxiety and stress. 13
In this context, integrating digital applications for patient entertainment and support presents an innovative opportunity to enhance the chronic patient experience.14,15 Research indicates that digital solutions are increasingly being incorporated into health care settings, demonstrating positive effects on both physical recovery and psychological well-being.16,17 Virtual reality (VR) offers patients an engaging escape from the monotony of hospital stays, helping to relieve stress and anxiety, and improve mood through interactive and immersive experiences.18–20 Research indicates that VR-based interventions effectively reduce perceived pain and enhance emotional well-being. 21
For its immersive and interactive nature, VR can be especially beneficial for patients facing the physical and psychological challenges of NMDs. Therapies that require repetitive and demanding exercises are often discouraging and boring,22,23 while VR has demonstrated the potential to improve patient engagement, delay functional decline, and improve the QoL of individuals with NMD.24–28 In our study, we aimed to take this a step further by introducing a tool that engages these patients in a real-life task, such as grocery shopping.
Building on previous work 29 assessing acceptability, flow, cybersickness, and anxiety in NMD patients through standardized questionnaires, this study expands the investigation by incorporating in-depth qualitative interviews. The aim is to investigate the entire subjective experience and explore how technical design choices can be improved to accommodate the needs of hospitalized NMD patients and make their interaction with the virtual contents as efficient as possible.
Materials and Methods
Setting and participants
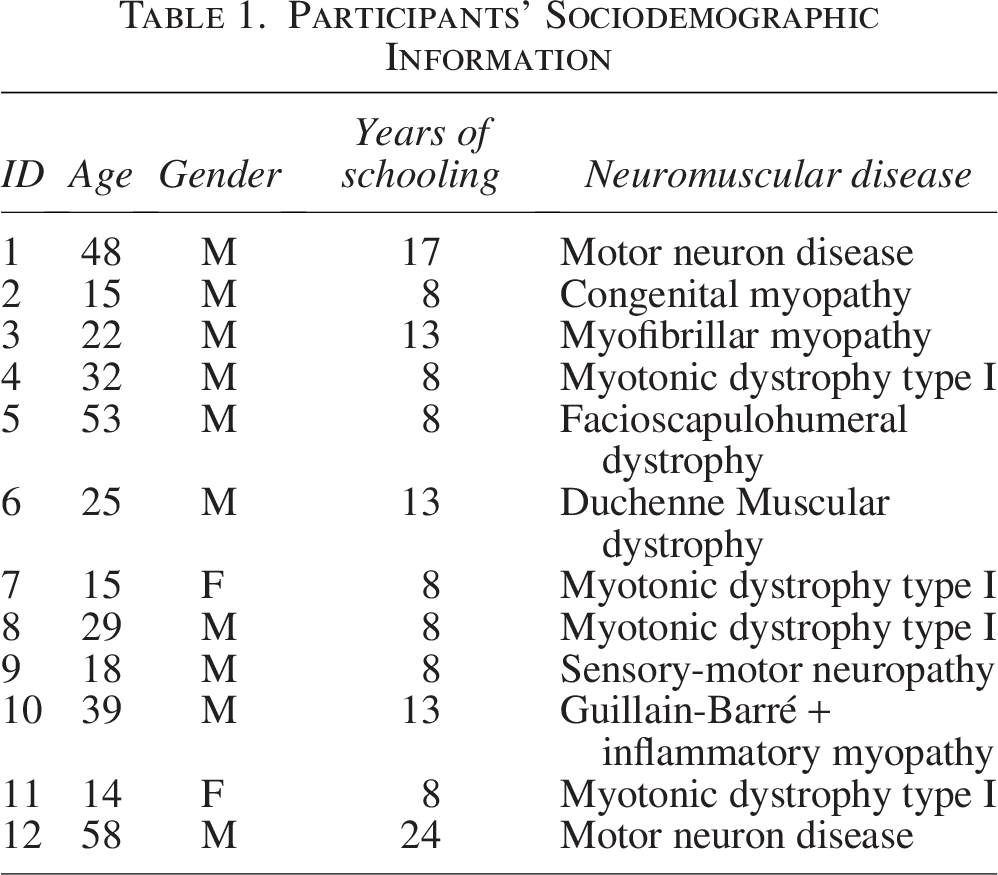
In clinical practice, patients admitted to the NeuroMuscular Omnicentre (NeMO) in Milan can utilize the VR experience for recreational purposes during hospitalization. Among these patients, 12 individuals were enrolled in the study. Inclusion criteria required a confirmed clinical and/or genetic diagnosis of a neuromuscular disorder and an age of at least 12 years. Patients with severe cognitive impairment (intelligence quotient ≤85 or equivalent score), epilepsy, severe vision problems, or an internal defibrillator were excluded. Clinical staff informed eligible patients of the possibility of participation and provided an explanation of the study. No eligible patients refused to participate or to be interviewed after completing the VR experience. The mean age of the sample was 31.17 years (standard deviation = 16.4, range = 14–59 years; 10 males, 2 females). Other collected participants’ characteristics were the number of years of schooling and the specific neuromuscular disorder (Table 1).
Participants’ Sociodemographic Information
VR sessions and interviews took place at NLAB in Milan. The study was conducted in accordance with the Declaration of Helsinki and the ICH E6 Guideline for Good Clinical Practice. Ethical approval was granted by the Niguarda Hospital Ethics Committee (No. 353-05062023). All participants received comprehensive verbal and written information about the study. Informed consent was obtained from their legal guardians.
The VR application
The application, depicting a virtual supermarket (VS), was developed with Unity and deployed for Meta Quest 2, a stand-alone VR system. The application was proposed to entertain neuromuscular patients during their stay at the hospital, and it was the result of several adaptations proposed for different types of end users.30–32 This application featured two main scenarios: a supermarket aisle and a cash register scene (see Figs. 1 and 2). Both scenarios contained realistic items, though sometimes simplified to accommodate the difficulty. Supermarket background noises were played throughout the entire session (i.e., cash register sounds, people talking, etc.). Positive or negative auditory feedback was provided when picking an item, indicating the correctness of the choice.

Scene from the virtual supermarket during shopping. The user navigates through the aisles and selects items from the shopping list using a laser pointer and trigger button, with the chosen products automatically placed in the basket. This task mainly involves visuospatial functions.

Scene from the virtual supermarket during payment. The user completes the purchase at the virtual checkout by selecting the correct amount and choosing between the available banknotes and coins. The activity is designed to stimulate the executive function of planning and mathematical calculation.
To enhance accessibility, we implemented a laser-ray interaction system requiring minimal wrist and finger movements, eliminating the need to elevate the arm. Unlike hand-tracking systems, which demand sustained arm support against gravity, the controller can rest on the patient’s thigh or wheelchair armrest, reducing physical strain while maintaining accurate tracking. The choice of a stand-alone head-mounted display (HMD; i.e., Meta Quest 2) was made to further enhance accessibility, allowing patients to engage in the VS experience from their wheelchair or bed without additional setup constraints.
The shopping task, structured into nine adaptive difficulty levels, accommodated different cognitive abilities and mental requests. This allowed patients to participate in playing without exacerbating their cognitive workload or inducing anxiety. The possibility of choosing an appropriate level of difficulty, along with the immersive nature of VR, enhanced the accessibility of the experience while providing an adequate level of challenge. A full description of the VS, including its development and usability evaluations, was provided in a previous study. 29
Procedure
Patients at the NeMO clinical center could undergo VR experiences offered during hospitalization for recreational purposes. Patients were assisted in wearing the HMD properly; furthermore, the psychologist set the initial difficulty of the experience. During the experience, the progression (or regression) through levels was handled automatically depending on the committed errors. The session duration was not fixed and depended on patient preference, consistent with the recreational nature of the activity. In our previous work, 29 technical details regarding the level structure and average usage times are reported.
Following the VR session, participants were administered a semi-structured interview. Interviews were conducted face-to-face immediately after the VR session by the same psychologist who assisted participants during the task.
Interview
A semi-structured interview was explicitly designed to explore patients’ subjective experiences of interaction in the VS. To minimize potential bias, the interviewer refrained from providing evaluative feedback during the session and emphasized that responses would not impact clinical care or access to future patients’ recreational activities. Participants were encouraged to freely express both positive and negative impressions. Responses were transcribed verbatim during the interview.
The questions were related to:
Immediate impressions after the VR experience: aiming to capture spontaneous emotional and cognitive reactions. Emotion: insights into what participants enjoyed most, least, and any difficulties. Intention to use: exploring willingness and motivations to repeat the VR experience, and how often. Recommendations: whether participants would recommend the VR experience and why. Suggestions for improvement. Overall reflection: a response summarizing the participant’s experience, possibly with examples.
Analysis
Data were analyzed using the Framework Method as described by Ritchie and Spencer. 33 Coding followed a predominantly inductive approach. Two psychologists trained in qualitative methods independently coded all transcripts. Discrepancies were resolved through discussion until consensus was reached. An audit trail documenting coding decisions and theme development was maintained. Furthermore, the concept of pattern saturation was employed; all identified themes were reported by multiple participants, indicating that the main patterns were stabilized within the dataset.
Results
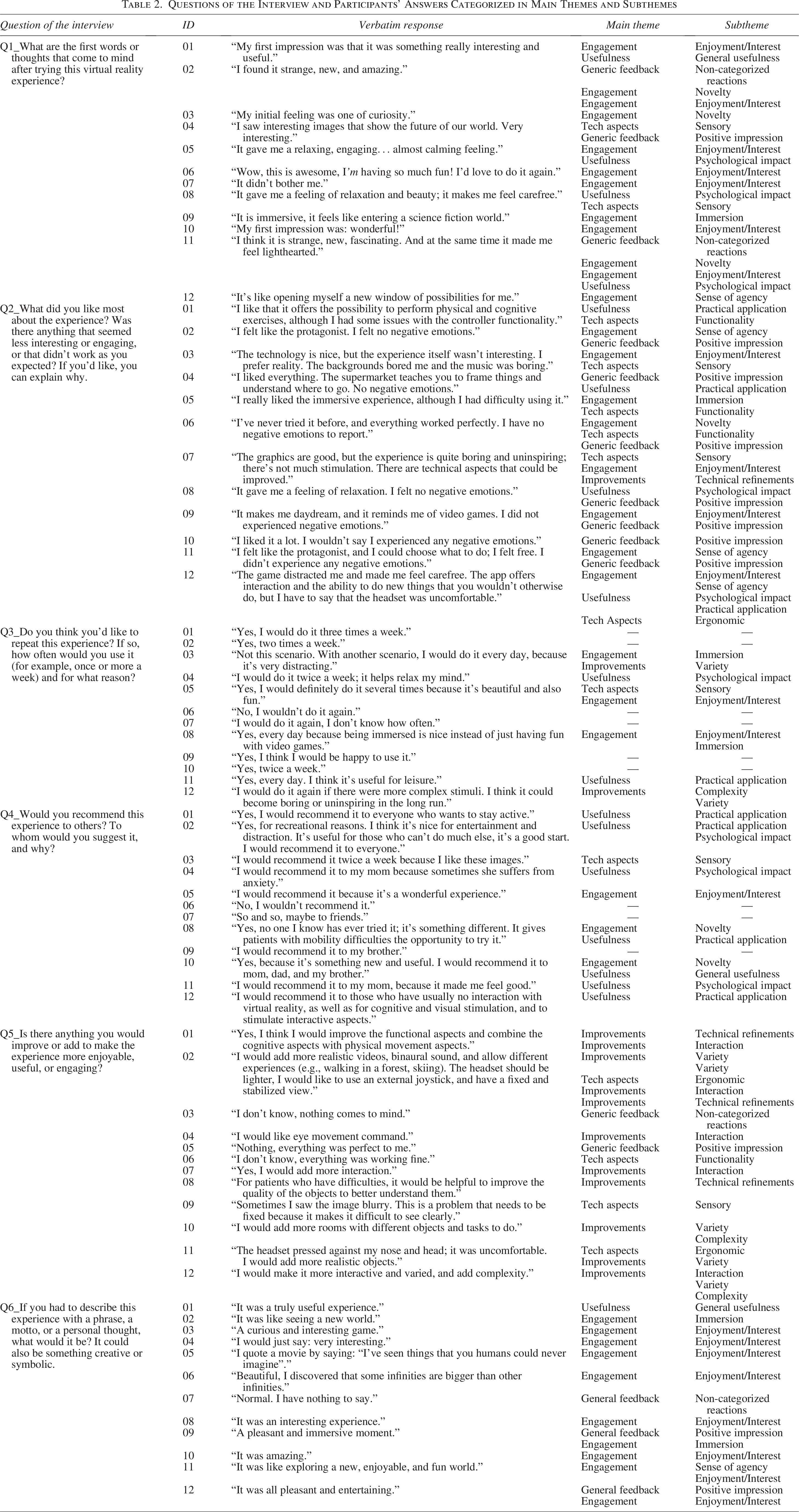
The analysis of the interviews revealed five themes describing how hospitalized patients with NMDs experienced the immersive VS: engagement, technological aspects, usefulness, improvements, and general feedback. An overview, including all verbatim excerpts, is presented in Table 2, categorized by themes and subthemes. Supplementary Tables S3–S7 provide detailed frequency summaries for each subtheme, including corresponding participant IDs and the questions from which each phrase emerged.
Questions of the Interview and Participants’ Answers Categorized in Main Themes and Subthemes
Engagement was discussed by all participants, and four subthemes emerged. “Engagement” captures how much the experience engages patients, how much it intrigues them, how much they feel like protagonists, and how much they feel “inside” the scene. Enjoyment/interest was the most frequently mentioned category, noted by all participants, although with mixed valence: while most described the experience as pleasant or interesting, a few comments expressed neutral or negative reactions (3/22). Novelty was mentioned by six participants who described the experience as innovative and different from the usual. Sense of agency was reported by 3 out of 12 participants, who appreciated feeling like a protagonist or freedom. Immersion was mentioned by 5 out of 12 participants, who described a feeling of daydreaming.
Within technological aspects, three subthemes emerged related to the technical and physical quality of the experience. Functionality was explicitly mentioned by three participants: despite being unfamiliar with VR, most participants did not encounter any issues during their interaction with the system. However, two people reported experiencing difficulties using it and interacting with the controller. The sensory aspect combines visual and auditory features of experience. Visual aspects were mentioned by eight participants, who generally found the images interesting or visually appealing. However, three reported difficulties, including one who was unable to clearly recognize objects or had blurred vision. Only one participant reported feedback on the auditory aspect. Additionally, ergonomic issues were reported by 3 out of 12 participants, mainly describing the helmet as uncomfortable, pressing on their nose and head.
The perceived usefulness of the VR experience varied among participants, with responses falling into three main subcategories. General usefulness was mentioned by two participants, who considered the experience to be broadly useful. Two subthemes are more focused: the topic “practical applications” (N = 6) collects the sentences related to specific practical applications, particularly in the health care field. One response, in particular, highlights VR’s potential for enhancing accessibility and inclusion for individuals who have limited opportunities to engage in real-world experiences. Seven participants referred to a psychological impact, mainly describing the experience as relaxing. Most of them (N = 6) reported their own emotional response; but some (N = 3) considered relaxation as a key benefit that would make the experience valuable for other patients.
Participants also offered several suggestions to enhance the VR experience, which clustered in the main category “Improvements” around four main areas: interaction, complexity, variety, and technical refinements. Interaction was a recurrent theme, with five participants expressing the desire to interact with the environment in different ways. Three individuals suggested introducing more complexity, noting that the current scenario might become monotonous. Five participants proposed expanding the number of available environments, adding new rooms, objects, or tasks. These comments reflected a desire for greater variety. Finally, four participants mentioned technical refinements: these included general comments about technical aspects, as well as more specific suggestions such as improving the quality and recognizability of objects to support users with greater difficulties. Some of these suggestions implicitly pointed to a desire for greater personalization, such as having access to different environments or alternative modes of interaction that could better match individual preferences or abilities.
Finally, some comments were highly generic and did not clearly align with the thematic structure. For transparency, we grouped them under the macro-category “Generic Feedback,” distinguishing between positive impressions (e.g., “I liked it”), which emerged from 9 out of 12 participants, and non-categorized reactions (e.g., “strange”or “nothing comes to mind”) noted by 4 out of 12 participants.
In addition to the qualitative themes, the results, which include the frequency of use and recommendations, help to outline the general perception of the experience. Regarding the intended frequency of use, 9 out of 12 participants indicated they would use the system regularly, although with varying intensities (N.1 three times per week, N.3 twice per week, N.2 daily, N.3 no specific frequency). Three participants stated they would not use the current version: one reported no interest, while two clarified they would consider frequent use only if the environment were modified.
Furthermore, 10 participants stated they would recommend the experience to others. One participant reported s/he would not recommend it, and one expressed uncertainty.
Discussion
This qualitative study enables us to gain a deeper understanding of how individuals with neuromuscular disorders experience VR. Overall, the findings suggest that VR offers a novel, engaging, and potentially useful experience for patients with NMDs, although some areas, particularly comfort, interactivity, and content diversity, could be improved to enhance both enjoyment and practical application. Previously, only quantitative data were considered, and no differences in the quality of the participants’ experience were found. 29 In this work, by incorporating participants’ responses, we obtained a deeper and broader overview of the subjective experience.
Three elements emerged as most strongly shaping engagement: absence of discomfort, agency, and personalization. These factors influenced enjoyment, immersion, and willingness to repeat the experience, offering clear priorities for future refinement.
Comfort emerged as a key determinant of acceptability. Participants who perceived less pressure from the headset or had no visual difficulties tended to describe the experience as more pleasant and were more inclined to use it again. Conversely, discomfort reduced immersion even when the content was appreciated. Although the VR design minimized cybersickness (the VR experience did not include any form of artificial locomotion, and participants remained static within the environment), hardware still shaped the experience. Comfort can be improved through individual adjustments, such as adjustable and supportive straps and additional padding. Research indicates that lighter, better-balanced devices reduce pressure loading and discomfort. 34 The Meta Quest 2 concentrates its weight on the front of the headset, which may increase pressure on the forehead and nose, potentially exacerbating neck fatigue, especially in patients with muscular weakness. However, it remains one of the lightest stand-alone options available.
Sense of agency also played a central role. Those who reported feeling free and proactive also reported greater engagement. Even minimal opportunities to act or make choices increased stimulation and pleasure, consistent with flow theory 35 and the motivational value of perceived control. 36 This is especially true in patients with disabilities, who can experience limitations in their autonomy in daily life and in their choice-making capability. 37 This suggests that significant engagement is possible even with limited motor skills.
Personalization also emerged as a key factor for sustaining engagement across diverse needs and profiles. Participants differed in their reactions to sensory elements; for example, background noise was not always appreciated, highlighting the importance of allowing users to adjust or disable auditory settings. Some participants also expressed a need for variety in the environment, suggesting that being able to choose their preferred scenario or task would help tailor the experience to individual preferences. Although impressions were generally positive, satisfaction varied considerably, likely reflecting individual factors such as familiarity with technology, personal preferences, and subjective expectations; these factors were not investigated in-depth, but they may have influenced responses and could help explain interindividual variability beyond diagnostic labels.
Willingness to repeat the experience was high, but some participants anticipated that prolonged use might lead to boredom or fatigue, highlighting the importance of evaluating long-term engagement and potential habituation effects. Although the study was not designed to examine associations between participant characteristics and perceptions, a descriptive inspection of the data suggested a weak, but not definitive, trend whereby individuals with higher education levels tended to express more favorable impressions. As expected, those willing to repeat the experience were also more likely to recommend it, indicating coherent patterns of positive involvement. Importantly, it remains difficult to attribute specific response patterns to diagnostic categories alone, as subjective impressions are shaped not only by medical conditions but also by prior technological experience and individual personality traits. Certain disease-specific trends emerged. Individuals with NMD, especially those with ALS, often expressed enthusiasm and a sense of novelty. However, they reported problems with the controllers and the headset weight, likely reflecting disease-specific physical impairments. Participants with myotonic dystrophy type 1, instead, particularly appreciated the carefreeness element that the VR environment offered, suggesting that VR may provide these individuals a brief reprieve and counteract apathy and reduced initiative. 38 Although exploratory, these patterns underscore the importance of tailoring VR design to diverse neuromuscular profiles.
The qualitative findings are consistent with our previous quantitative study, 29 which showed stable anxiety, high levels of flow, good acceptability, and low levels of cybersickness. The interviews confirm and expand on these findings, highlighting enjoyment, a sense of agency, perceived usefulness, and comments regarding overall comfort, along with concrete suggestions for improving interactivity and variety.
The study has limitations, including recruitment from a single specialized center and an unbalanced gender distribution. Moreover, the sample includes only individuals who were able to complete both the VR session and the interview, potentially excluding patients with more severe impairments. Session length varied, although the interview questions were designed to capture perceptions independent of performance. Familiarity with technology and personality traits were not assessed and may have influenced responses.
Overall, the results suggest clear design implications: improving ergonomics, offering customizable sensory and interaction settings, and expanding content variety. Future studies should examine longitudinal use to understand how engagement, comfort, and perceived usefulness evolve over time, and whether adaptive task complexity can sustain motivation across repeated sessions.
Conclusions and Future Work
This research enabled us to explore the subjective experiences of patients with NMD in depth when interacting with VR, highlighting the potential of this technology for both entertainment and clinical purposes. By integrating qualitative feedback, we identified key elements that shape engagement—comfort, agency, and personalization—and highlighted the importance of ergonomic optimization, accessible interaction modes, and adjustable sensory settings to accommodate diverse needs.
Future research should test improved or alternative scenarios with a larger and more heterogeneous population of NMD patients, enabling a clearer assessment of accessibility across different motor and cognitive profiles. A codesign approach would help tailor VR experiences to individual skill levels and perceived challenges, supporting flow and enhancing engagement across diverse neuromuscular profiles. A larger sample would also contribute to assessing whether subjective impressions align with clinical characteristics or physiological indicators of involvement. Finally, longitudinal studies are needed to examine short- and long-term use, including repeatability, evolving comfort, and the durability of perceived benefits over time, combining both standardized questionnaires and interviews.
Authors’ Contributions
M.M.: Conceptualization (equal), formal analysis (equal), methodology (equal), writing—original draft (lead), visualization (lead), and resources (equal). L.G.: Investigation (lead), data curation (lead), conceptualization (equal), methodology (equal), writing—review and editing (equal), and resources (equal). S.B.: Formal analysis (equal) and writing—review and editing (equal). V.C.: Writing—review and editing (supporting). R.P.: Supervision (supporting). M.S.: Supervision (supporting). S.R.: Supervision (supporting). V.A.S.: Supervision (supporting). S.A.: Conceptualization (equal), methodology (equal), software (lead), resources (equal), and writing—review and editing (lead). E.C.: Project administration (lead), supervision (lead), and writing—review and editing (equal).
Footnotes
Acknowledgment
The authors would like to express their gratitude to all the patients who participated and provided their data to the study.
Author Disclosure Statement
V.A.S. participates in Advisory Boards or Teaching activities for Biogen, Roche, AveXis, PTC, Santhera, Sarepta, and Dyne. E.C. received compensation for occasional scientific and educational activities for Biogen, Roche, Novartis, and Sanofi Genzyme. Other authors declared no disclosures.
Funding Information
This study did not receive any funding.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.