
Abstract
Introduction:
Falls severely affect older adults and are emerging as a global health and financial burden for public health care systems. Multiple studies have validated the use of virtual reality (VR) to prevent falls and reduce the risk of falls among older adults with cognitive deficits. Therefore, we evaluated the effectiveness of VR-based cable car simulation (CCS) using a Nintendo Wii Balance Board (WBB) to assess balance and profile individuals based on fall risk and age, and validated using the Biodex Balance System. Center of pressure (COP) displacement and mean velocity (MV) metrics obtained from the WBB were used for balance assessment.
Methods:
A total of 23 young participants (10 females; M = 29.9, SD = 5.0) were recruited from the Agência Regional para o Desenvolvimento da Investigação, Tecnologia e Inovação, and 25 older participants (19 females; M = 71.2, SD = 7.8) were recruited from a local senior gymnasium in Funchal, Portugal. All participants took part in a repeated-measures study design. Results indicated that young adults exhibited greater COP displacement than older adults in the anterior–posterior (AP) direction.
Results:
Significant differences were found in COP displacement between the groups, confirming age-related variations in balance performance. However, no significant differences were observed in MV. Discriminant analysis models were employed using COP displacement and MV to classify participants by age and fall risk. The best classification performance was achieved for the CCS at 77%, with average turns at 80%, average speeds at 86%, and 83% for the combined features using stepwise regression.
Discussion:
The selected features included the COP displacement for speeds and turning angles in both AP and medial–lateral (M-L) directions, as well as the mean values of speeds and turns for both AP and M-L. The system can accurately differentiate balance patterns across age groups and risk categories, indicating a reliable and ecologically valid assessment method.
Keywords
Introduction
Falls severely affect older adults and are becoming a global health and financial burden for public health care institutions. 1 The prevention of falls is a significant health challenge. Fall-related injuries and their associated costs are higher in older adults than in younger adults.2,3 International experts from multiple disciplines and stakeholders proposed a new global strategy for guidelines on preventing and managing falls. 4 About 30% of older adults aged 65 and above fall once a year. In comparison, 60%–80% of those with mild cognitive impairment and dementia fall every year. 5
The leading causes of morbidity and mortality among older adults are the prevalence of chronic diseases and external factors such as falls and accidents, which create a significant impact on older adults’ health. 6 Additionally, frequent incidents of falls can have a profound effect on the quality of life of older adults, resulting in long-term hospitalization, institutionalization, disability, impaired balance and postural control, social isolation, anxiety, and depression. 7
The literature highlights four major factors that contribute to the incidence of falls: biological (e.g., age and disease), behavioral (e.g., sedentary lifestyle), socioeconomic (e.g., lack of awareness), and environmental (e.g., hazards or uneven surfaces). 8 Therefore, it is necessary to identify the potential risk factors and take preventive measures to avoid incidents of falls.
Several methods have been introduced to assess the risk of falls, including physical tests, perturbation-based evaluations, and surveys. They have advantages and limitations. For example, surveys can be helpful when assessing the external risk factors for incidents of falls; however, they must be used in conjunction with physical measurements to evaluate intrinsic risk factors. Physical fitness procedures, such as the timed “up and go,” gait speed, Short Physical Performance Battery, and the Tinetti Balance and Gait-Evaluation Scale, require less administration but lack ecological validity and cannot identify specific sensory impairments.9,10
Ecological validity refers to the degree to which results from assessments conducted in controlled or laboratory settings can be generalized to real-world conditions. Literature reviews and studies indicate that gait and sensor data collected in ecologically valid environments are more effective in predicting fall risk than traditional clinical laboratory tests. However, these findings show considerable variation, highlighting the need for greater standardization.11,12
The one-legged balance test can be used to collect information, but it needs standardization for diagnosis. 13 The perturbation-based tests can assess specific sensory components, but they require expensive laboratory setups and have issues with portability. 14
Balance is defined as maintaining the posture in an upright standing position for the maximum time with minimal body sway or the ability to keep the body’s center of gravity within the base of support. 15 Maintaining balance is a complex mechanism that involves processing information from the visual, somatosensory, and vestibular systems. Ruhe et al. reported in their review that the traditional center of pressure (COP) metric serves as a reliable tool for evaluating postural stability and balance under specific study conditions. Analyzing COP displacement has been employed as an index of postural stability in the upright stance. 16 The significant change in COP displacement indicates instability or reduced postural control, which is associated with a high risk of falls.16,17
Mean velocity (MV) represents the average speed of COP displacement over time and reflects the frequency of balance adjustments. Frequent balance adjustments result in a high MV, reflecting poor postural stability as individuals strive to maintain an upright standing position. 18 Some studies suggest MV as a highly reliable metric for postural control.19,20 In static posturography (SP), the displacement of the COP is measured on the two-dimensional platform. It has been widely known in research on human posture for several years. The traditional static platforms only work with static balance, and a different approach is required to assess dynamic balance. 21
The COP has been used to analyze motor strategies to prevent falls,22,23 classify pathologies, 24 and assess fall risk in combination with other posturographic metrics. 25 Studies have reported significant differences in several sway parameters between fallers and nonfallers during upright standing, particularly in the mediolateral direction, indicating their potential as strong predictors of high fall risk. 26 Moreover, balance and sway have been considered as reliable measures for predicting fall risk in healthy older adults.27,28
The modified Clinical Test of Sensory Integration (mCTSIB), a time-based balance assessment, has been used to evaluate static balance by varying postural challenges. It has been used to assess the impact of visual, vestibular, and somatosensory inputs on an individual’s static balance. 29 The mCTSIB comprises four tests: eyes open on a flat surface, eyes closed on a flat surface, eyes open on a surface with foam, and eyes closed on a surface with foam. Balance control requires coordination from the sensory, neurological, and musculoskeletal systems. 30 The commercial force platforms can assess the risk of falls by measuring the individual’s COP (with or without balance impairment). 31 These platforms allow for rapid collection of various balance metrics, including COP displacement, stabilogram bandwidth, MV, oscillation area, and total displacement. COP values can be measured along with the anterior–posterior (AP) direction and medial–lateral (M-L) direction. 32
Virtual reality (VR)-based training in health care applications has recently gained more attention and progressed rapidly in the area of healthy aging.33,34 The literature validated the use of VR in fall prevention and reduction studies in older adult populations with cognitive deficits.35,36 VR can play an essential role in enhancing older adults’ motivation for their physical rehabilitation and can be a valuable tool in promoting active aging objectives. 37 It is well known that older adults are generally less motivated to engage in traditional physical exercise programs 38 ; a combination of immersive VR and traditional physical exercise may serve as a feasible training program tailored to individual physical conditions and needs. 39 Further research is needed on VR-based simulations to predict fall risk. However, most studies have employed VR-based exergames in conjunction with training programs to reduce fall risk.
Related Work
The Balance Rehabilitation Unit (BRU™; Medicaa, Montevideo, Uruguay) implemented SP by combining VR technology and a video game for balance assessment and rehabilitation. It provides real-time feedback during the interventions, such as displacement of the COP and sway velocity. 40 Profiling for the risk of falls is a complex process, but posturography methods are promising for evaluating the risk of falls among individuals due to impaired postural control. However, more strategies to prevent fall incidents are needed, 41 as the systems for assessing balance are costly, have longer execution times, and require trained health care professionals and laboratory setups. 42 Therefore, home-based assessments and interventions would be more feasible. 43
Over the past few years, the Wii Balance Board (WBB) has gained widespread recognition among researchers and health care professionals for its effectiveness in functional assessment and physical rehabilitation due to its accessibility, affordability, portability, and reduced evaluation time. 44 The WBB (Nintendo, Tokyo, Japan) is a low-cost, portable platform validated as an alternative to traditional force platforms. The WBB was introduced in 2007 as a game controller for the Nintendo Wii exergames and used in clinical rehabilitation setups globally. 45 The WBB comprises four strain gauge-based load sensors, which collect COP excursions and use Bluetooth technology to transmit data wirelessly to the computer. It has been used for several applications, including balance assessment, 46 neurorehabilitation, 47 balance training, and balance and fall risk assessment.47–49 Clark et al. 50 validated the WBB and suggested a reliable platform compared to the conventional force platforms.
Gonzalez et al. implemented a serial chain method in a COP computing system to estimate the center of mass using Kinect and WBB. The authors reported that the statically equivalent serial chain (SESC) method can be applied outside the laboratory environment using a Kinect. 51 Another study developed a platform to assess fall risk factors using Microsoft Kinect technology to track full-body movements and collect relevant metrics for the Gait Speed test. 52 In the Gait Speed test, 53 the participants are instructed to walk up to 10 meters. Spatiotemporal metrics such as step length, foot swing velocity, highest and mean gait speed, and the percentage difference between the highest and mean gait speed are measured and assessed. Results indicated that the Kinect-derived variables were found to be highly reliable, but some of them were redundant. The Kinect model presented 15% more variance than the traditional method, suggesting the addition of the Kinect systematic error to the test.
Lubetzky et al. simulated a virtual park scene using Oculus Rift, providing a highly immersive experience to assess dynamic balance and head movements. 54 Significant between-group differences were observed in the head path (patients exhibited more significant lateral head movements), head acceleration (controls showed higher acceleration, particularly during translational movements), and peak frequency (controls peaked near the ball’s frequency, while patients presented more variability). 54 One study created a stepping exercise simulation tool to assess the fall risk in older adults using an HTC (vive.com) VR head-mounted display (HMD). The VR-based tool implemented the Choice-Step Reaction Time (CSRT) test and collected the stepping performance metrics to process them for the fall risk assessment. The VR tool offers high immersion and provides a cost-effective and reliable solution for assessing fall risk, potentially enhancing the ecological validity of the CSRT test. 55
Machine learning (ML) and deep learning algorithms have demonstrated high efficiency in analyzing and solving complex patterns, high-dimensional data, and outperforming traditional statistics methods. 56 These machine learning techniques can detect nonlinear relationships and learn from data, making them suitable and adaptable for various populations and conditions. 57 Researchers have recognized mathematical modeling and artificial intelligence as powerful tools for investigating impairment in postural control.56,58,59 One study employed machine learning techniques, including support vector machines (SVM), to automatically differentiate between young and older adults’ gait patterns using a PEAK-2D motion analysis system. The SVM achieved an accuracy rate of 83.3%. 60 Another study developed a novel machine learning-based tool utilizing a force platform and anomaly detection to assess balance across all age groups. The artificial neural network was trained on 19 socioanthropometric and postural features, achieving an exceptional classification accuracy of 99.9% for different balance profiles. 61
A recent study introduced transient visual perturbations in immersive VR to modify electrocortical activity, which may improve balance performance. The results indicated that VR training with perturbations increased balance performance more than without perturbations. 62 Gonçalves et al. investigated the feasibility of VR-based bus ride simulation for balance assessment. Results showed significant differences in the maximum displacement of the COP along with the M-L axis during changes in the bus’s trajectory and speed conditions. 63 A comparison was conducted between the VR HMD and force platforms to assess fall risks. The participants exhibited greater postural movements in the AP direction than the control group. They reported minimal VR simulation sickness and heightened visual perturbation compared to traditional platforms for evaluating balance’s multisensory aspects. The VR HMD presents a portable and cost-effective alternative, offering reduced simulation sickness and visual disturbance relative to conventional force platforms. 10
A study used VR with the combination of low-cost balance platforms for the balance assessment and showed promising results compared with the EquiTest assessment. 64 Another study showed that VR headsets do not impact individuals’ risk of falling during the intervention, similar to the eyes-closed condition. 65 Although several studies have used the latest VR HMDs for balance assessments,64–66 the usability and validity of VR applications for older adults are scarce in the literature. The VR-based application without the participant’s body may cause a low sense of spatial presence. 67 Therefore, augmented reality (AR) can offer a higher sense of presence and embodiment than VR and provide comparable benefits for limb recovery function.68,69 AR provides the interaction of virtual objects with real-world environments in real time, which is more suitable and feasible for older adults. 70
Therefore, we evaluated the effectiveness of the VR-based cable car simulation (CCS), which was previously designed and developed in our research lab, using the WBB to assess fall risk in both young and older adults. We hypothesized that CCS assessment may identify individuals’ fall risk and age differences through COP displacement and MV. We compared the findings of our study
71
with results from a prior study
72
that employed the gold-standard Biodex Balance System (BBS) (biodexrehab.com) as a reference to address the following research questions: Which is more relevant in identifying fall risks: COP displacement or MV? Can the CCS classify users based on risk and age?
The ML techniques, such as discriminative analysis models and an SVM, were applied to classify fall risk in young and older adults. The following section outlines the methods (hardware and software) and presents the results of our study.
Methods
Participants
For the first study, 71 a convenience sample of 23 participants (10 females, ages: M = 29.9 SD = 5.0) was recruited from the Agência Regional para o Desenvolvimento da Investigação, Tecnologia e Inovação. The participants were healthy young adults, including undergraduate and graduate students, as well as research assistants, all of whom were proficient in English and without physical disabilities. Written informed consent was obtained from all participants, who received no compensation for their involvement. Two participants were excluded due to errors in the projector’s display settings.
For the second study, 72 employing a repeated measures design, 25 participants (19 females, ages: M = 71.2, SD = 7.8) were recruited from a local senior gymnasium in Funchal, Portugal, through invitations extended by the sports science professionals working there. The participants were healthy, Portuguese older adults with no physical injuries, balance impairments, or prior history of falls, who provided written informed consent, were informed of the study protocol, including procedures and safety measures, and received no compensation. Five participants were excluded due to loss of heart rate data caused by connectivity issues with the chest band sensors. One participant was also removed due to a knee injury. Balance assessments were conducted at the University of Madeira’s Laboratory of Pedagogy and Optimization of Sports Performance. All procedures complied with the Declaration of Helsinki and were approved by the Faculty of Human Kinetics Ethics Committee (CEIFMH No. 3/2023). This sampling method introduces selection bias because individuals who regularly attend the gym are typically more active, mobile, and health conscious than the average older adult. As a result, the study sample is limited to healthier and fitter older adults and may not accurately represent community-dwelling older adults who are less active, frailer, or living with mobility limitations or chronic health conditions. Moreover, certain populations were excluded for safety considerations and to reduce confounding variables, including medication use and fall history, that might compromise the study’s internal validity. Young, healthy adults were included for comparison with older adults to evaluate the system’s sensitivity and fall risk assessment in the context of active aging. Future research should include more diverse samples to determine whether similar outcomes occur in less active or medically vulnerable populations.
Apparatus
The KAVE (Kinect-Cave Automatic Virtual Environment) was developed and implemented at our NeuroRehabLab to provide an immersive virtual environment for our application. 73 The KAVE comprises three walls with a width and height of 2.2 and 2.8 m, respectively. The other hardware components include four HD projectors, external speakers, and a personal computer processing system. The Kinect v2 sensor was installed at the front wall of the KAVE for full body tracking to interact with the virtual environment, creating a parallax effect, Figure 1a.
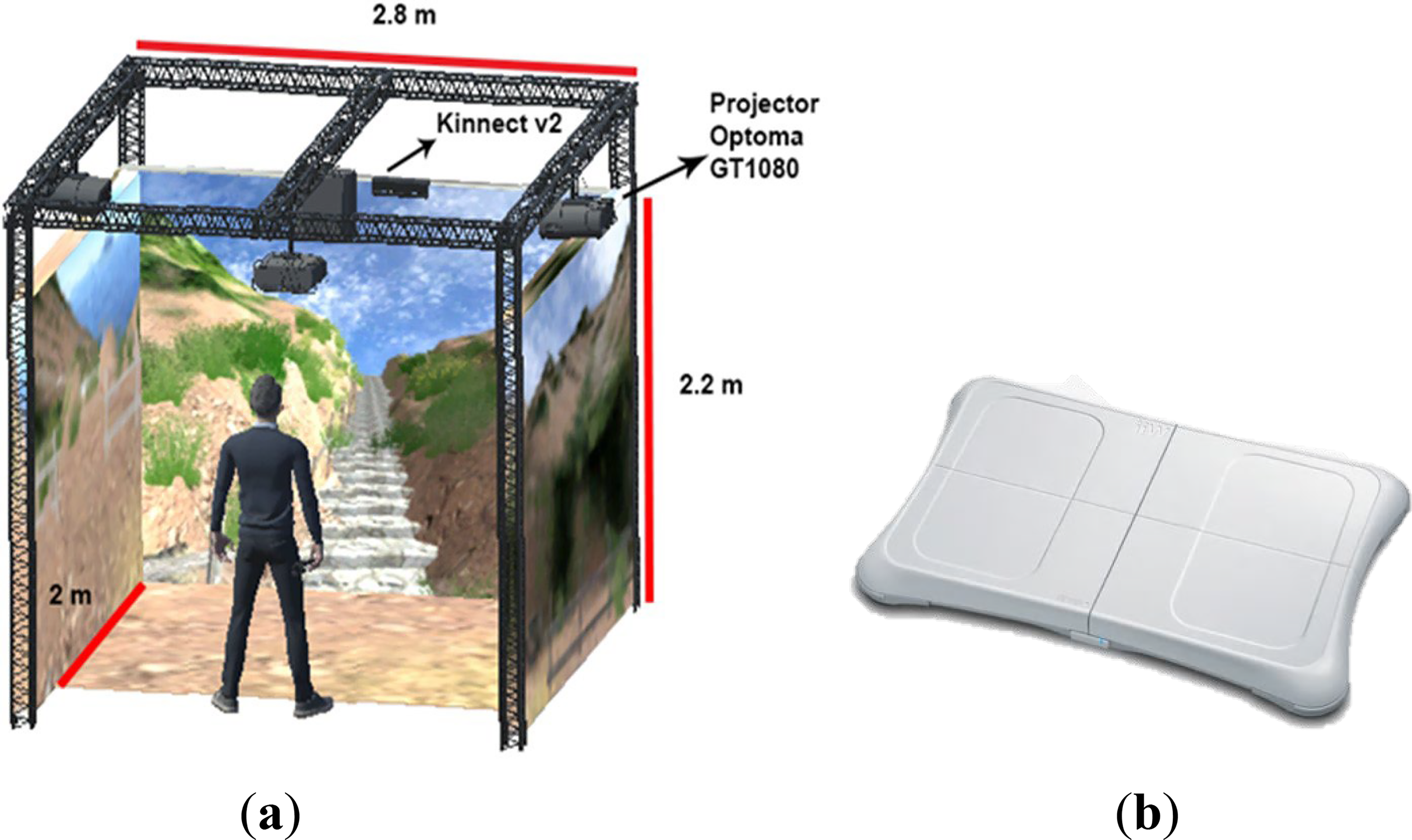
Hardware setup.
The KAVE application was developed with a Unity 3D Plugin comprising scripts, prefabs, objects, and the Microsoft Kinect libraries (https://assetstore.unity.com/packages/tools/camera/kave-113090). Unity 3D is a cross-platform game engine offering advanced features such as sophisticated animations, particle systems, high-definition audio, and comprehensive tools for developing 2D and 3D games.
The Nintendo WBB was used to evaluate participants’ balance by measuring their COP (Figure 1b). Manufactured in Japan by Nintendo Co. Ltd. (Kyoto), the WBB has been widely used by neurotologists and neurologists 50 for balance assessment. The WBB has been used in commercial gaming consoles such as the Wii and Wii U. It features four pressure sensors to track COP displacement and connects to a user’s personal computer via Bluetooth. The board is available in two variants with maximum weight limits of 136 and 156 kg, while its structure can withstand forces up to 300 kg. 74
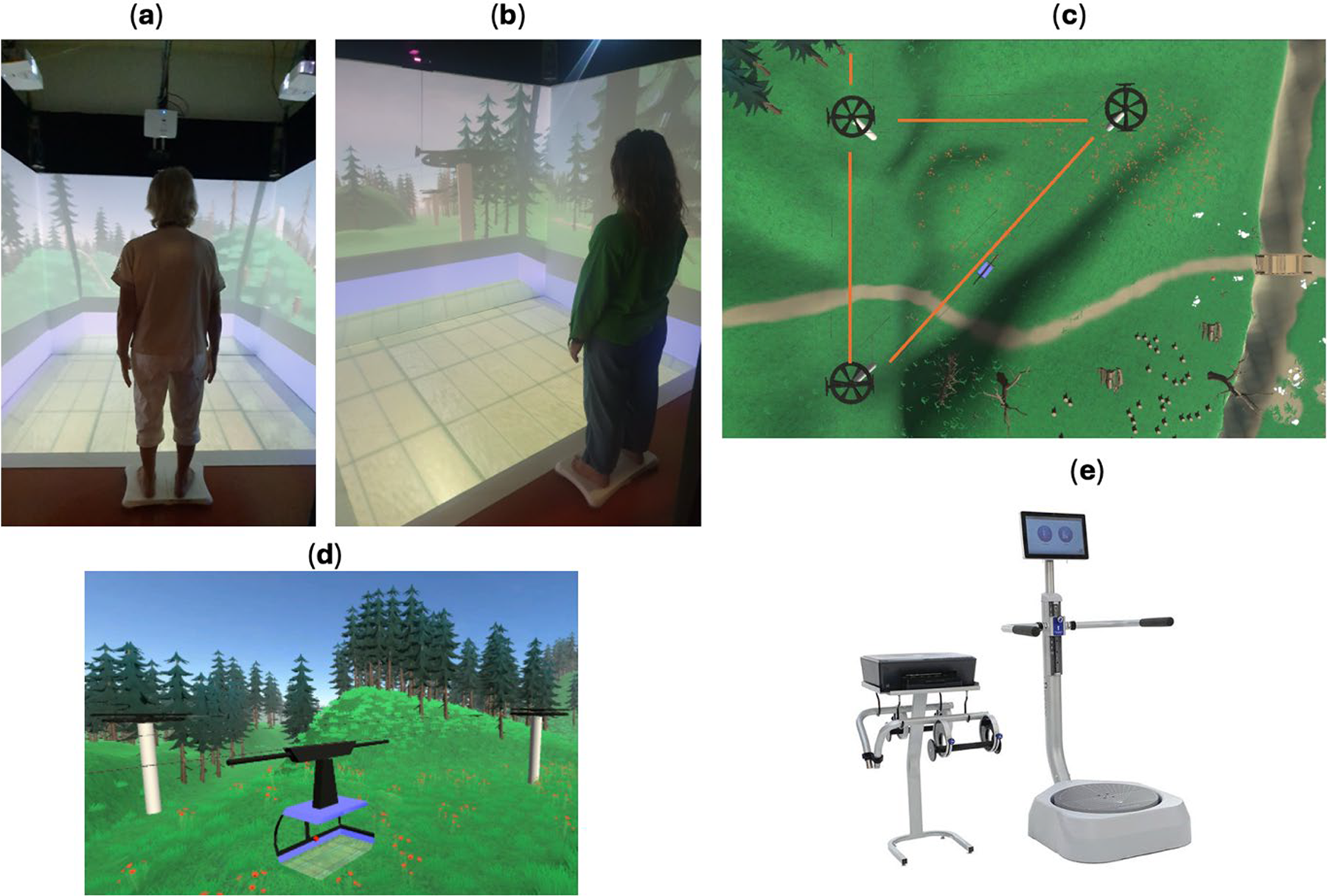
The VR-based CCS was designed and developed in Unity 3D (unity3d.com) to ensure high immersion and an ecologically valid environment for assessing static balance in young and older adults. The virtual environment featured 3D objects such as mountains, trees, grass, cable car poles, wires, and stations. These objects were created using the open-source software Blender (Blender Foundation, Amsterdam, Netherlands). The CCS application connects to the WBB via Bluetooth and measures COP at a frequency of 30 Hz. Its trajectory includes turns at angles of 0°, 45°, 90°, −45°, and −90°, with speed variations of 3, 5, 7, and 9 m/s (Fig. 2c and d). The cable car restarts automatically after the initial round, and the CCS records COP displacements for each speed and turning angle combination.
Experiment setup.
The BBS SD (biodexrehab.com) assesses static and dynamic balance and fall risk. We used the BBS as a reference to validate and compare our system (Fig. 2e). 72 The benefits of BBS include the development of muscle tone, balance, and agility; improvement; and treatment for various pathologies. The user interface is highly friendly and features a touchscreen display and a manual with step-by-step instructions for running static and dynamic balance tests and training. The BBS is fast and effective for assessing fall risk and has been validated significantly in older adults. 75
Procedure
Informed consent and the study protocol were provided before the experiment began. A 2-minute demonstration session was conducted to familiarize young, healthy participants with the application and objectives. Participants were instructed to stand upright on the WBB for 5 minutes without performing any voluntary body movements, except for natural head movements to explore their surroundings. No physical supports were provided; however, a lab assistant remained positioned immediately behind each participant throughout the experiment to ensure safety and prevent falls if necessary. The same procedure was repeated for the older participants, as shown in Figure 2a and b. 72
Older adult participants were instructed to perform balance tests on the BBS platform as a reference for validating the CCS results. Each participant required approximately 15–20 minutes to complete the test. All results were recorded and stored on a personal computer.
Statistical analysis
The independent variables included five trajectory angles and the four cable car speed limits. The trajectory angles had five levels, while the speed limits had four. The dependent variables were the maximum displacement of the COP along with AP and M-L directions. The metrics from BBS include EOMeanScore; ECMeanScore; Composite Mean Score; Stability Overall; Stability AP; M-L; Percentage of Time in Zone A, B, and C; Percentage of Time in Quadrant 1, 2, 3, and 4; Stability Index Front–Back and Left–Right. The Composite Mean score was used to classify participants as high-risk or low-risk falls. Participants were classified into high- and low-risk groups based on their Composite Mean BBS scores. Individuals scoring 11 points or higher (upper 50th percentile) were categorized as high fall risk, while those scoring below 11 points were categorized as low fall risk. This threshold was derived from the BBS fall-risk reports for the studied population, which indicate that scores in this range are associated with increased fall risk in similar cohorts. The linear discriminant analysis (DA) and the LeaveOneOut cross-validation method in MATLAB R2023 b (Mathworks Inc., Natick, MA, USA) were used to estimate the classifiers’ accuracy, precision, and recall. The statistical analysis was conducted using IBM SPSS Statistics, version 26 (IBM, New York, NY, USA).
Results
The WBB was used to measure the COP displacement CCS. The three parameters from the mCTSIB were recorded: the maximum displacement of COP in M-L, AP, and mean speed. The angle and cable car speed were the factors from the CCS with five and four levels, respectively. The normality tests (e.g., Shapiro–Wilk, Kolmogorov–Smirnov) reported significant differences (P < 0.05), indicating a non-normal distribution (P < 0.05); thus, we performed a Kruskal–Wallis test for metrics, including COP displacement along with the M-L and AP directions, and MV. Figures 3 and 4 present box plots illustrating the differences in COP displacement along with the AP and M-L directions. Examining the results, the older adults responded with a higher displacement of COP along with the M-L direction for nearly all of the angles (0, 45, 90, −45, −90) and speeds (3, 5, 7, 9 m/s) than the young adults. For example, the older adults with low risk responded with higher COP displacement along with M-L direction (M = 2.89, SD = 1.37) for the speed limit of 3 m/s at a 0° angle than the young adults (M = 2.24, SD = 1.26). Likewise, the young adults responded with higher COP displacement along with AP (M = 1.0, SD = 1.13) for the speed limit of 3 m/s at a 0° angle than the older adults with low risk (M = 1.9, SD = 3.5).

Box plot indicating the variation of maximum displacement of COP (cm) along with AP direction among young, older adults with no risk, and older adults with risks. The asterisks and circles are the far-out and far outliers, respectively. AP, anterior–posterior; COP, center of pressure.
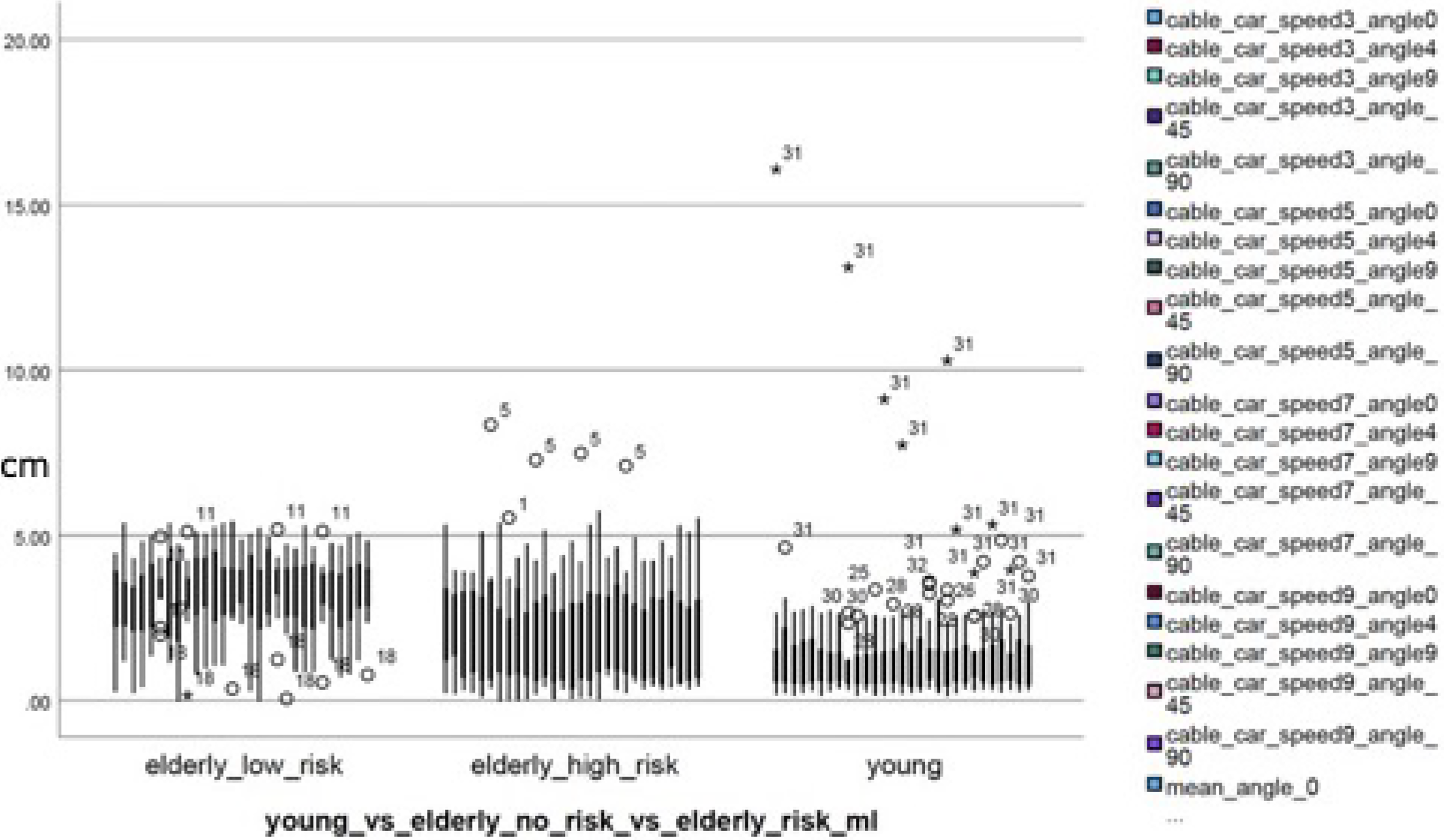
Box plot indicating the variation of maximum displacement of COP (cm) along with M-L direction among young, older adults with no risk, and older adults with risks. The asterisks and circles are the far-out and far outliers, respectively.
Figures 3 and 4 illustrate the box plots for the discrimination accuracies among young versus older adults-with-no-risk versus older adults-at-risk for the maximum displacement of COP in the AP and M-L directions, respectively. The results show that young adults had a higher displacement of COP along with the AP direction than older adults. However, the older adults-high-risk group (participants with predicted Composite Mean scores in the upper 50th percentile [11 points]) had a slightly higher COP displacement than the older adults-low-risk group. The young adults’ responses were significantly higher than those of the older adults in CCS, indicating the simulation’s high impact on their somatosensory and vestibular systems. Likewise, the older adults responded more to COP displacement along with the M-L direction than the young adults.
The COP displacement for nearly all angles (0, 45, 90, −45, −90) and speeds (3, 5, 7, 9 m/s) along with M-L direction was significantly different across young versus older adults, with no risk versus older adults at risk, H(3) = 7.95, P = 0.019 (Fig. 5). After performing an independent Kruskal–Wallis test, pairwise comparisons were conducted, and we report both uncorrected P-values and Bonferroni-adjusted P-values for clarity. While the corrected values account for multiple comparisons, the uncorrected values are also provided because this analysis was exploratory and involved a small number of planned comparisons. Strict corrections such as Bonferroni can substantially increase Type II error in small samples, potentially masking meaningful trends. Therefore, presenting both values allows readers to interpret the results with full transparency. Likewise, for the AP direction, COP displacement was significant across young versus older adults, with no risk versus older adults at risk, H(2) = 15.1, P < 0.001. The results along with the AP direction were like those observed in the M-L direction during pairwise comparisons. Table 1 presents the effect sizes for COP displacement along with the AP and M-L axes at a speed limit of 3 m/s and a 0° angle. The effect sizes were observed to be higher for the AP direction than for the M-L. However, no significant differences were observed for the MV metric.
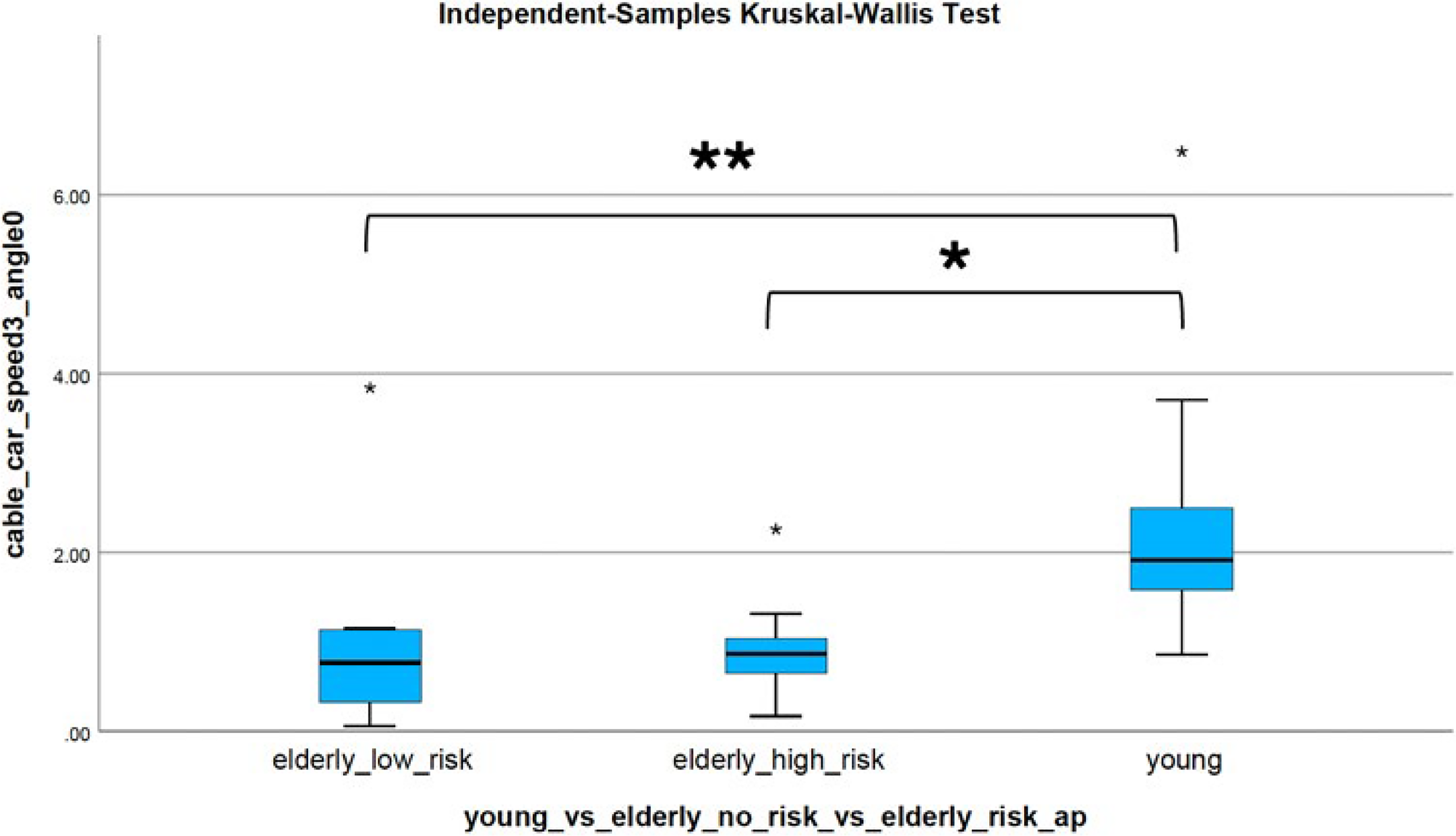
Boxplot of COP displacement for angle 0° and speed 3 m/s along with the AP direction across three groups: older adults with no fall risk, older adults at risk, and young adults. Independent-samples Kruskal–Wallis test indicated overall group differences. Pairwise comparisons showed significant differences between young adults and older adults with no risk (P < 0.05) and between young adults and older adults at risk (P < 0.01), while no significant difference was found between the two older adult subgroups (P > 0.05). P-values were not adjusted for multiple comparisons.
Effect Sizes for the Cable Car Speed Limit 3 m/s and Angle 0°

AP, anterior–posterior; M-L, medial–lateral.
Statistical power was low across nearly all cable car turning and speed conditions. Table 2 shows the observed power for some cable car turns and speed conditions.
Observed Power for the Center of Pressure Distance in the Anterior–Posterior Axis for Cable Car Speed and Trajectory Angles Among Young, Older Adults with No Risk, and Older Adults with Risks

The maximum displacement of COP in the AP and M-L directions for all combinations of angles (0, 45, 90, −45, −90) and speeds (3, 5, 7, 9 m/s) was recorded during the experiment. DA was conducted to evaluate the effectiveness of Kave-based CCS in classifying all participants (both young and older adults) as high-risk falls or low-risk falls based on the tests performed by the BBS. The participants who were classified in the higher 50th percentile predicted Composite Mean score (11 points) were referred to as high-risk falls, and those below were in low-risk falls. However, healthy young adults were at low risk for falls. Multiple DA models, including linear, pseudolinear, diaglinear, pseudoquadratic, diagquadratic, and SVM, were developed along with the leave-one-out cross-validation (LOOCV) method to evaluate the performance of the models (accuracy, recall, precision, and F-score). To estimate generalization performance and reduce overfitting, we initially considered LOOCV, but due to its computational cost and limited efficiency, we adopted a k-fold cross-validation (KFCV) approach. This method partitions the dataset into k folds, trains the model on k–1 folds, and validates on the remaining fold, iterating through all folds. This provides a more robust estimate of model performance and mitigates overfitting compared to LOOCV. 76 Feature selection was performed using a stepwise linear regression model (SLRM), which iteratively added or removed predictors based on statistical significance. Parameters were organized into four sets: cable car raw (COP distance in AP and M-L axes for all angles and speeds), turns (COP distance in M-L and AP axes averaged across speeds), speeds (COP distance in M-L and AP axes averaged across angles), and all (combining all parameters). The same procedure was applied to the COP MV. The highest-performing model for each group was identified using KFCV and SLRM (see Tables 3 and 4). For DA, models were trained assuming a linear decision boundary and equal covariance matrices across classes. For SVM, models were trained using a linear kernel, a regularization parameter C = 1 C = 1 C = 1, and automatic feature scaling.
Discrimination Accuracies Among Young Versus Older Adults for the Maximum Displacement of Center of Pressure

LOO, leave-one-out.
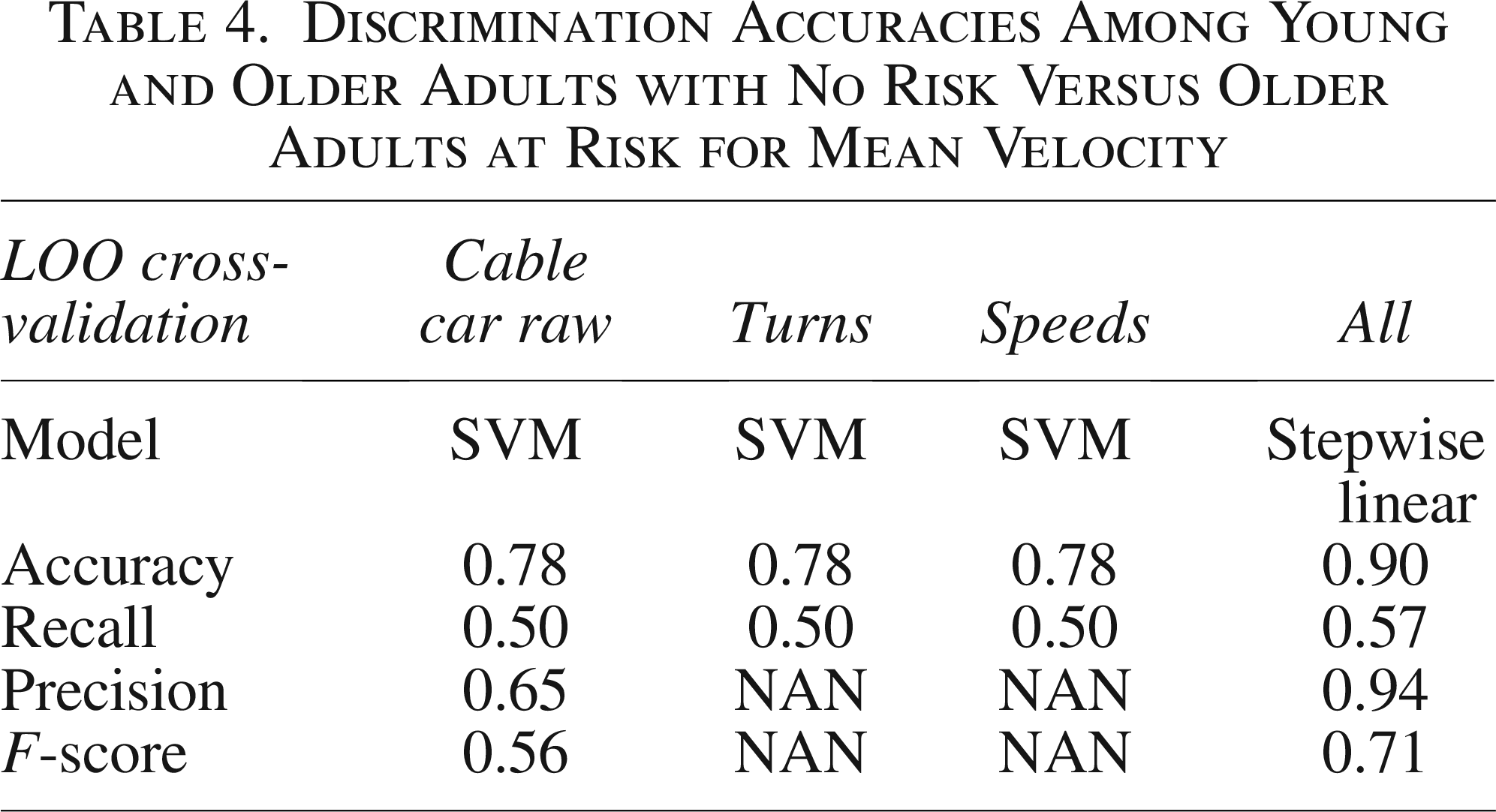
Discrimination Accuracies Among Young and Older Adults with No Risk Versus Older Adults at Risk for Mean Velocity
Before running the DA, the participants were classified into three groups: young and older adults with no risk versus older adults at risk; young versus older adults; and young versus older adults with no risk versus older adults at risk for the maximum displacement of COP, MV, and combining COP and MV. The selected input features for the classifier included CCS speeds and turning angles, as well as the mean of the angles and CCS speed limits. The DA for each feature was performed to estimate the prediction power of each feature modality. Moreover, a posterior stepwise regression method was employed to select the features. Table 3 shows that discrimination accuracy varies significantly between young and older adults for the maximum displacement of COP. The best classification was for the CCS at 77%, average turns at 80%, average speeds at 86%, and 83% for the combined features through a stepwise regression. The selected features were the maximum displacement of the COP for speeds and turning angles for both AP and M-L, and the mean of the speeds and turns for both AP and M-L.
Likewise, Table 4 shows that discrimination accuracies significantly differed between young and older adults for the MV. The best classification was achieved for the CCS, average turns, and average speeds, with accuracies of 78% and 90% for the combined features using a stepwise regression. The selected features were the MV for speeds and turning angles for both AP and M-L, and the mean of the speeds and turns for both AP and M-L. However, pseudoquadratic classifier was among the lowest classification accuracies (Table 5).
Misclassification Rates Among Young and Older Adults with No Risk Versus Older Adults at Risk for Mean Velocity
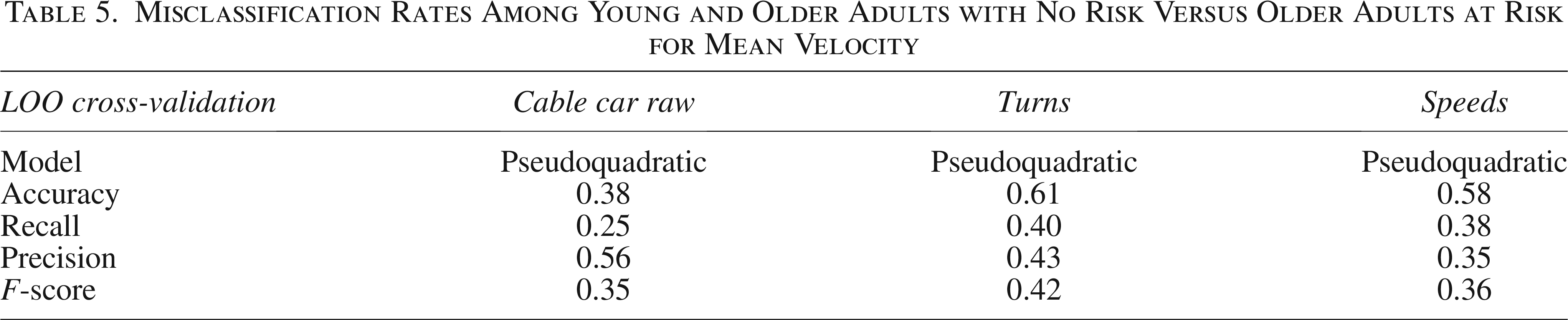
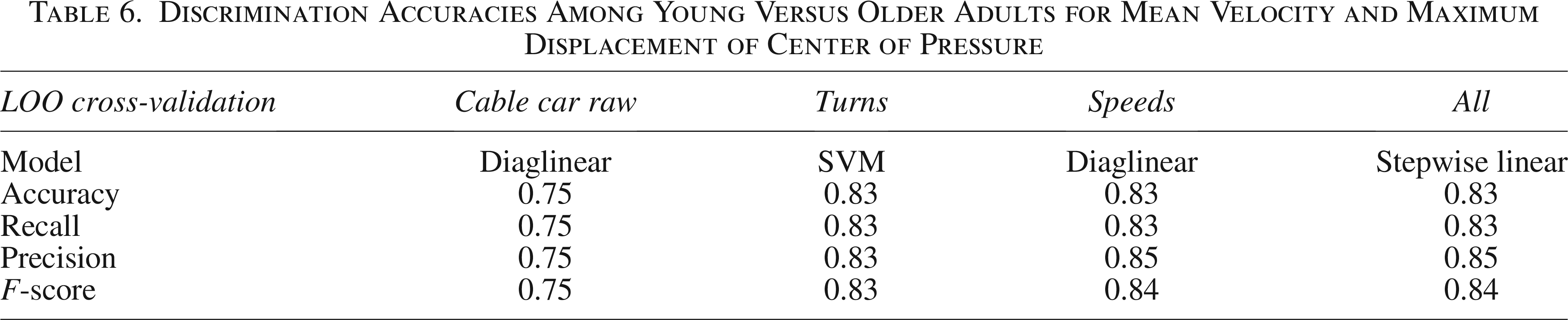
Table 6 shows that discrimination accuracies vary significantly between young and older adults for the MV and COP. The best classification was for the CCS at 75%, average turns and average speeds at 83%, and 83% for the combined features through a stepwise regression.
Discrimination Accuracies Among Young Versus Older Adults for Mean Velocity and Maximum Displacement of Center of Pressure
Discussion
In this study, we assessed the effectiveness of the CCS in evaluating static balance and fall risk among young and older adults. The gold-standard BBS was used as a reference to validate the feasibility and sensitivity of the CCS for fall risk classification and balance assessment. The traditional balance assessments are task specific and may not be feasible according to postural requirements and thus require more ecologically valid assessments. The CCS does not fully provide the simulation aspects of a real cable car, such as vibrations, environmental factors, and movements. However, we added variations of cable car speeds and trajectories to create an impact on the participants. The CCS was designed with four distinct speed limits and five manouvring angles to generate optical flow along with both M-L and AP directions. Static balance was evaluated by measuring the maximum displacement of COP and MV. The results indicate that the CCS greatly impacted young adults’ postural control due to their significant COP displacement along with the AP direction, suggesting a greater optical flow effect for young adults. However, older adults had higher COP displacement than young adults along with the M-L direction.
The efficiency of the DA was assessed by profiling participants as young and older adults with no risk versus older adults at risk, and young versus older adults with no risk versus older adults. Excellent classification results were achieved using stepwise feature selection. The linear DA performed on the selected features achieved classification accuracies of 90% and 83%, indicating that CCS can differentiate populations based on age and fall risk, which supports our first research question. However, pairwise comparisons showed no statistically significant differences between older adults with and without fall risk. This outcome is likely influenced by the limited sample size and the relatively healthy status of participants, which reduces variability and statistical power. The consistently low statistical power across nearly all cable car turning and speed conditions indicates a high probability of a type II error (false negative) and could be addressed by increasing the sample size. While this does not necessarily indicate a lack of sensitivity of CCS, it highlights the need for studies with larger and more diverse samples to confirm its clinical relevance. MV achieved 90% accuracy following DA, indicating greater effectiveness in profiling fall risk than COP displacement, which answers our second research question. Instead, we relied on classification performance and supporting evidence from the literature. MV reflects the rate of neuromuscular corrective actions during quiet standing, whereas COP amplitude primarily captures sway magnitude. Prior studies have shown that MV is more sensitive to subtle postural control deficits because it represents the frequency and intensity of corrective torques rather than overall displacement. 77 This physiological basis, combined with the higher classification accuracy observed in our analysis, supports the claim that MV is more effective for distinguishing fall-risk profiles.
The findings suggest that VR-based simulations can be alternatives to traditional balance and fitness assessments, offering custom environments with high ecological validity, portability, and cost-effective platforms. VR-based simulations could potentially be implemented outside specialized laboratory settings because they rely on commercially available hardware and do not require advanced equipment. However, their use in home-based environments would depend on factors such as usability, accessibility, and adherence among older adults, which were not evaluated in this study. Therefore, we present this as a future research direction rather than a current recommendation. Romeo et al. developed a vision-based system using three low-cost cameras to assess balance and fall risk in older adults. Image processing techniques were used to obtain dynamic user skeletons and extract relevant features. A decision tree classifier was trained to predict fall risk, achieving a prediction accuracy of 79.1%. 78 Another study developed an automatic motion data analytics framework using signal data collected from an inertial sensor for balance activity analysis in community-dwelling older adults. 79 The Tinetti Performance-Oriented Mobility Assessment-Balance was used as a standard to profile abnormal sit-to-stand, 360° turning, and stand-to-sit motions using one-class SVM and k-nearest neighbors, achieving accuracies of 90%, 92%, and 86%, respectively.
A recent study developed a stability index estimation algorithm using COP metrics for older adults and validated it against the stability index from the BBS (SD). 80 Using a linear regression model, the system confirmed R-values ranging from 0.943 to 0.983. The system, incorporating a custom capacitive and resistive sensing force mat, is suitable for home-based setups. To validate the similarity between the WBB and the flexible force mat, each COP feature was applied to the developed regression model, confirming a strong correlation with an R-value of 0.96.
KAVE-based VR setups have limitations, including space constraints and challenges with portability. Therefore, a mobile-based VR environment could be a more acceptable and widely adopted alternative to the KAVE system. The CCS could be improved by increasing environmental depth, incorporating trajectory turning angles, and adjusting the cable car's linear and rotational speeds to enhance the impact on the user’s somatosensory and vestibular systems. The WBB also has limitations, such as consistent hardware design and signal loss. Additionally, Nintendo has discontinued production of the WBB, and no longer offers support. Given its limited reliability and quality, it cannot be considered a viable alternative to clinical platforms. 46 This reduces the chances of securing identical units for future studies, which in turn undermines standardization. The WBB has been used as a de facto standardized low-cost platform; its large availability once made it easy to execute multisite protocols and compare results across cohorts for meta-analyses.81,82
Several low-cost technologies may serve as alternatives to WBB for future research. Recent advances in sensor technology have led to the development of low-cost force mats and plates that match or surpass the WBB’s accuracy, while integrating seamlessly with open-source software. 83 Likewise, smartphone-integrated inertial measurement units (IMUs) provide an economical option for assessing balance capabilities. Multiple studies have demonstrated that pelvic- or trunk-mounted IMUs can closely approximate sway metrics with high temporal resolution and suitable reliability for clinical or field evaluations. 84 Furthermore, markerless motion-capture technologies, including RGB-D cameras and monocular pose-estimation algorithms,85,86 have shown growing potential for evaluating balance.
We performed this study on a limited sample size of healthy young and older adults. The older adults were physically active and members of a gym. However, further studies should include a larger sample of older adults with balance impairments, a history of falls, and medication to analyze postural performance and determine classification accuracy, as well as to compare results with gold-standard clinical assessments.
Conclusion
To conclude, we evaluated the effectiveness of the VR-based CCS in assessing balance and fall risk in both young and older adults. Machine learning techniques—including DA models and SVMs—were applied using COP displacement and MV to classify participants by age and fall risk. The system accurately distinguished balance patterns across age groups and risk levels through machine learning techniques, suggesting an ecologically valid assessment tool. Additionally, longitudinal studies are needed to validate the predictive accuracy of CCS over time and assess its ability to monitor changes in fall risk. Finally, comparisons against the gold-standard clinical trial to establish the clinical relevance and practical applicability of CCS. The Nintendo WBB may be a cost-effective alternative tool for assessing balance and fall risk across all age groups.
Authors’ Contributions
M.A.A.: Conceptualization, methodology, software, validation, formal analysis, investigation, writing—original draft preparation, writing—review and editing, and visualization. É.R.G.: Conceptualization, validation, resources, writing—review and editing, supervision, and project administration. S.B.i.B.: Conceptualization, validation, formal analysis, resources, writing—review and editing, visualization, supervision, project administration, and funding acquisition. All authors have read and agreed to the published version of the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work is supported by NOVA LINCS (UID/04516/2025) with the financial support of FCT.IP (https://doi.org/10.54499/UID/04516/2025).