
Abstract
Objective:
Frozen shoulder is a common condition causing shoulder pain and stiffness, with conventional therapies often hindered by low adherence due to their repetitive and painful nature. This randomized clinical trial aimed to evaluate the clinical effectiveness of immersive virtual reality (VR) exergaming in frozen shoulder rehabilitation.
Materials and Methods:
Fifty-four patients with primary frozen shoulder were randomly assigned to a VR therapy (VRT) group or a conventional therapy (CT) group. Both groups underwent 18 sessions over 6 weeks, consisting of 20 minutes of continuous passive motion exercises followed by 20 minutes of either VR exergaming or conventional functional exercises. We chose Beat Saber for the VR intervention, a rhythm game in which players slice blocks in sync with music. Its “level editor” allowed us to customize block patterns to simulate therapeutic shoulder movements.
Results:
Primary outcomes included passive range of motion (PROM) in external rotation, abduction, and flexion. Secondary outcomes assessed shoulder function (Disabilities of the Arm, Shoulder and Hand [DASH] questionnaire) and resting pain (visual analog scale [VAS]). Assessments were conducted at baseline, postintervention, and 12 weeks after the trial. Both groups showed significant improvements in PROM, DASH, and VAS scores compared with baseline (P < 0.001). Between-group analysis revealed no significant differences in DASH (P = 0.483) or VAS (P = 0.220). However, the VRT group achieved superior abduction (P = 0.015) and flexion (P = 0.031), with no significant difference in external rotation (P = 0.637).
Conclusion:
These findings suggest VR exergaming is a promising adjunct to CT for frozen shoulder. Further studies are needed to investigate the influence of VR game design on rehabilitation outcomes.
Introduction
Frozen shoulder, also known as adhesive capsulitis, manifests as a disabling condition marked by pain and stiffness within the glenohumeral joint. With an incidence ranging from 2% to 5% across the general population, frozen shoulder predominantly afflicts individuals between the ages of 40 and 60, emerging as the primary cause of shoulder pain among middle-aged and elderly populations.1–4
The primary objective in managing frozen shoulder is mitigating pain while enhancing shoulder functionality. However, there is no consensus on a definitive treatment strategy. Therefore, a combination of treatment modalities is typically employed, which most commonly includes physical therapy as the primary treatment option.1,3–7
Nevertheless, the problem with conventional physical therapy is that it necessitates prolonged and frequent visits to rehabilitation clinics, involving repetitive, often painful movements, which can significantly demotivate patients, preventing them from fully engaging in the required movements. Furthermore, given the slow rate of recovery, consistent encouragement throughout the rehabilitation process becomes imperative for patients. To overcome these challenges, recent research highlights the potential of integrating virtual reality (VR) into physical therapy as a promising solution.4,8–11
VR is a computer-generated simulation of a three-dimensional environment with which users can interact, creating an immersive experience. VR technology has matured and become more accessible over the past decade, leading to extensive research on its rehabilitative benefits. The term “virtual reality” encompasses a spectrum of technologies, from nonimmersive systems like the Microsoft Kinect to immersive systems using head-mounted displays. These different settings provide varying levels of immersion, which impacts the user’s sense of “presence” within the virtual environment. The presence refers to the degree to which the brain perceives the virtual world as real, creating a state of “simulated embodiment” that is associated with the clinical outcomes of VR therapy.12,13 Immersive VR can reduce procedural pain and kinesiophobia and increase motivation and exercise time, thereby potentially increasing the quality of physical therapy.11,14–17
In line with these benefits, VR therapy has been studied in conditions such as fibromyalgia, low back pain, and postoperative rehabilitation of surgeries such as anterior cruciate ligament reconstruction, total hip replacement surgery, and total knee replacement surgery.18–23 The literature on upper-limb rehabilitation has been expanding, with a few recent studies targeting frozen shoulder. However, they have not led to a clinically relevant and replicable rehabilitation approach due to methodological limits.11,24–26
For instance, Lee et al. demonstrated improved outcomes using nonimmersive VR for frozen shoulder but did not include a control group. Therefore, it is unclear whether the improvements were due to the VR element or the physical exercises themselves. 25 Wankhade et al. reported superior outcomes for immersive VR with a control group but provided insufficient methodological details on the VR exercises, hindering reproducibility and clinical application. 26 Ota et al. conducted a randomized clinical trial that included a gamified immersive VR rehabilitation protocol for frozen shoulder but did not measure clinically relevant metrics, as the participants were healthy individuals. Thus, while they demonstrated that immersive VR gaming increases willingness to engage in frozen shoulder therapy, they could not establish its clinical relevance for actual patients. 11 Demir et al. addressed this issue by conducting a clinical trial on actual frozen shoulder patients, testing a gamified VR rehabilitation. However, like the study of Wankhade et al., they provided little information regarding the specific shoulder movements required in the VR content and whether those movements were justifiable therapeutic shoulder exercises without the VR immersion. 24 Furthermore, none of the studies mentioned above included a follow-up clinical assessment, which is a notable limitation in chronic musculoskeletal conditions. 27 Frozen shoulder can persist for 2–3 years, and without planned follow-up, it remains unknown whether the benefits of a short course VR interventions are sustained over time. 2
To address these gaps, the primary objective of this randomized clinical trial is to evaluate whether a gamified immersive VR therapy produces greater improvements in passive range of motion (PROM) for patients with primary frozen shoulder compared with conventional physical therapy. Secondary objectives are to compare changes in patient-reported shoulder function (Disabilities of the Arm, Shoulder and Hand—[DASH]) and resting pain (visual analog scale [VAS]) and to assess the feasibility of a clinic-ready VR exergaming protocol. In addition, this trial incorporates a planned follow-up assessment to determine whether any observed initial benefits are maintained.
For the VR intervention we selected Beat Saber, a commercially available rhythm game that was not originally designed for rehabilitation. Beat Saber requires players to slice flying blocks of objects in specific directions synchronized to music and provides multimodal feedback. 28 The original game levels are unsuitable for therapeutic purposes. However, the game provides a “level editor” feature, which we utilized to customize block patterns, tempo, and direction, in order to create movement patterns that replicate therapeutic shoulder movements (abduction, flexion, and rotation), as detailed in the Materials and Methods section.
We hypothesize that the gamified VR therapy will yield a significantly larger increase in PROM, greater improvements in shoulder function (measured by DASH), and greater pain reduction (measured by VAS) compared with conventional physical therapy.
Materials and Methods
Ethics and design
This study utilized a randomized clinical trial with parallel-group design to assess the effectiveness of gamified VR therapy among individuals diagnosed with frozen shoulder. The study is part of a dissertation conducted at the Shahid Beheshti Medical University and received approval from the National Committee for Ethics in Biomedical Research in May 2023 (approval ID: IR.SBMU.MSP.REC.1402.010), in addition to being approved by the Iranian Registry of Clinical Trials (trial registration number: IRCT20230522058251N1). Verbal and written informed consent were obtained from all of the participants using a protocol approved by the university’s ethics committee. This study adheres to the guidelines outlined in the Consolidated Standards of Reporting Trials and complies with the Declaration of Helsinki. 29
Recruitment and randomization
The study was conducted between July 2023 and June 2024 at Akhtar Orthopedic Hospital on patients diagnosed with idiopathic (primary) frozen shoulder and referred to the designated rehabilitation clinic.
Inclusion/exclusion criteria
Patients presenting with shoulder pain and stiffness at the clinic underwent a thorough initial assessment. Following a comprehensive history and physical examination, individuals diagnosed with idiopathic (primary) frozen shoulder were enrolled, adhering to the criteria outlined in Zuckerman and Rokito’s study to differentiate idiopathic (primary) from secondary frozen shoulder. 30 The inclusion and exclusion criteria are detailed in Table 1. Shoulder X-rays were ordered for all patients, unless previously conducted postonset of the symptoms. Patients were excluded if X-rays revealed calcification, arthrosis, fracture, or dislocation.
Inclusion and Exclusion Criteria

PROM, passive range of motion.
Randomization/blinding
Eligible patients were instructed to select a sealed envelope from a preprepared pool, each marked on the inside with either a “1” or “2” label on a 1:1 ratio. The label “1” corresponded to the VR therapy (VRT) group, while “2” denoted the conventional therapy (CT) group. Due to the use of VR hardware, blinding of participants and clinicians was not feasible. To minimize bias, the following procedures were implemented: The clinician who supervised and delivered the exercise sessions was not the person who performed outcome measurements; a trained assessor, blinded to group allocation, conducted all PROM, DASH, and VAS measurements at baseline, week-6, and week-12. The data analyst remained blinded to group assignment until completion of the primary analysis.
Sample size calculation
The determination of sample size was based on passive shoulder abduction, which was our primary outcome measure established prior to the trial initiation. In a previous study involving 60 frozen shoulder patients, a baseline of 69° with a standard deviation of 11° was reported. 31 Assuming a similar effect size (9° difference between groups), a power of 80%, and a type I error of 0.05, the required sample size was initially calculated to be 24 patients per group. Factoring in an anticipated dropout rate of 15%, the final required sample size increased to 27 patients per group.
VR setup
We utilized the HTC Vive Pro2 headset, two base stations for tracking head movements, and two controllers. To prioritize patient safety, we designated a 2 × 2-m platform within the clinic, enclosed by ropes on all sides. The platform was equipped with soft rubber padding to reduce the risk of injury in the event of a fall. The VR content was presented on a desktop monitor, allowing the research team and family members to observe users’ immersive experience.
Game design
We integrated gaming into the repetitive nature of rehabilitation while aligning in-game movements closely with therapeutic shoulder exercises. We selected Beat Saber as the gaming platform because it (1) allows precise placement of targets (blocks) via an in-game level editor, (2) provides immediate multimodal feedback (visual, audio, and haptic), and (3) is intuitive and engaging for patients.
Basic mechanics and therapeutic mapping
In Beat Saber, colored blocks approach the player in time with the music; each block has an arrow indicating the required slicing direction. Participants hold a controller in each hand, which is seen as a lightsaber in the game, and must perform a deliberate slicing motion through the block in the indicated direction to register a successful hit. For therapeutic use we slowed the tempo, reduced block density, and customized block placement so that block position (height and lateral offset), number of simultaneous blocks, and distance from the center map to specific shoulder movements and ranges of motion (e.g., abduction, flexion, and internal/external rotation) were optimized. For example, three simultaneous blocks placed at higher screen coordinates require greater abduction ROM than two or a single block positioned closer to the center. Left-hand and right-hand mirrored versions of each level were created. Customized block patterns and their correlation to rehabilitation movements are illustrated in Figure 1.

Examples of customized block patterns and their corresponding shoulder movement.
Feedback mechanisms and performance measures
The game provides immediate visual feedback (hit/miss indicators, score popups, and combo counters), audio feedback (music and hit sounds), and controller haptics (vibration on successful hits). The in-game score and accuracy were used as objective adjuncts to monitor performance and engagement but were not used as the sole criterion for clinical decisions.
Progression criteria
Three complementary criteria guided advancement from easy to medium to hard and were recorded in the session log. Progression required explicit approval by the treating physiotherapist and was based on (1) patient-reported pain/discomfort, (2) therapist assessment of movement quality (adequate movement control and absence of clinically important compensatory patterns observed during the session), and (3) consistent in-game performance (improved accuracy/score across two consecutive sessions). The customized rehabilitation-specific Beat Saber levels used in this study are available to researchers upon request.
Intervention
All participants completed an 18-session program spanning 6 weeks. Each group received 40 minutes of physical therapy per session. The regimen comprised 20 minutes of continuous passive motion exercises followed by 20 minutes of functional exercises involving active flexion, abduction, and internal/external rotation. While the CT group performed standard active exercises, the VR therapy (VRT) group engaged in active exercises through the proposed VR exergaming module. Additionally, all patients were instructed to perform pendulum exercises at home three times daily, for 5 minutes each session. Patients were reminded of home exercises at the end of each in-clinic session; however, due to staffing constraints and participant load, no routine objective adherence monitoring (daily diary or phone check-ins) was implemented.
Outcome measures
Our primary outcome measure was PROM in abduction, flexion, and external rotation of the affected shoulder. These measurements were conducted using a clinical goniometer while patients were in a supine position. PROM was selected as the primary outcome because it is an objective, directly measured biomechanical outcome that closely reflects the movement capacity targeted by the intervention. Shoulder function (DASH questionnaire) and pain (VAS at rest) were prespecified as secondary outcomes to capture patient-reported disability and symptom change.
The technique for assessing PROM adheres to the clinical guidelines outlined by the orthopedic section of the American Physical Therapy Association, 32 as summarized in Table 2, which details the location of the axis, the stationary arm, and the movable arm of the goniometer in each measurement.
Description of the Placement of Goniometer Arms and Axis for Passive Range of Motion Measurements

Secondary outcome measures included shoulder function and pain at rest. To assess shoulder function, we employed the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire, consisting of a 30-item scale. The DASH questionnaire has demonstrated validity and reliability across various upper limb disorders. A change of 10.2 points in the DASH score is considered clinically significant. 33 Pain experienced at rest was assessed using a VAS ranging from 0 to 10 cm, where 0 denotes “no pain” and 10 indicates the “worst pain imaginable.” The VAS has exhibited validity and reliability in assessing chronic pain. 34 While the minimal clinically important difference (MCID) for VAS generally varies between 1.0 and 2.0 cm in the literature,31,34 we adopted the threshold of 1.4 cm established by Tashjian et al. for rotator cuff diseases, to strictly evaluate clinical significance in the context of the current study. 35 The PROM, DASH score, and VAS for each patient were collected at the baseline, at the end of the 18th session (sixth week), and on a follow-up examination session at the end of the 12th week.
Adverse events monitoring
Anticipated adverse events were defined based on the VR and exergaming literature and included nausea, dizziness/vertigo, headache, general discomfort, and an increased risk of falling down. 36 Safety measures included therapist supervision during all VR sessions and a padded, enclosed 2 × 2-m gaming platform. All adverse events were documented on each patient’s registration form under “Additional notes” with the event type, date, session number, any immediate action taken (e.g., session termination, observation, or referral), and subsequent outcome.
Statistical analysis
The normality of the data was validated using the Kolmogorov–Smirnov test, along with a visual examination of histograms and Q–Q plots. Categorical variables are shown as counts, while continuous variables are described using means and standard deviations (SD). Baseline characteristics were compared using the independent t-test for normally distributed continuous variables and the Mann–Whitney U test for nonnormally distributed continuous variables. Categorical variables were compared using the Chi-square test or Fisher’s exact test, as appropriate. Confidence intervals (CI) were calculated at the 95% level, and statistical significance was defined as P < 0.05. A two-way repeated measures analysis of variance (ANOVA) was utilized to assess the outcome measures, with “time” as the within-group factor and “study group” as the between-group factor. Box’s test was used to evaluate the equality of variances, and Mauchley’s test was employed to assess the sphericity assumption. The Greenhouse–Geiser correction was applied when the sphericity assumption was violated. Partial eta-squared was calculated to estimate the effect size. All statistical analyses were performed using SPSS 26.0 for Windows (IBM Corp., Somers, NY, USA).
Results
Between July 2023 and June 2024, a total of 82 patients were initially assessed for eligibility. Among them, 54 patients fulfilled the criteria and were enrolled in the study. Random assignment allocated 27 patients to each group, moving through the trial as illustrated in Figure 2.
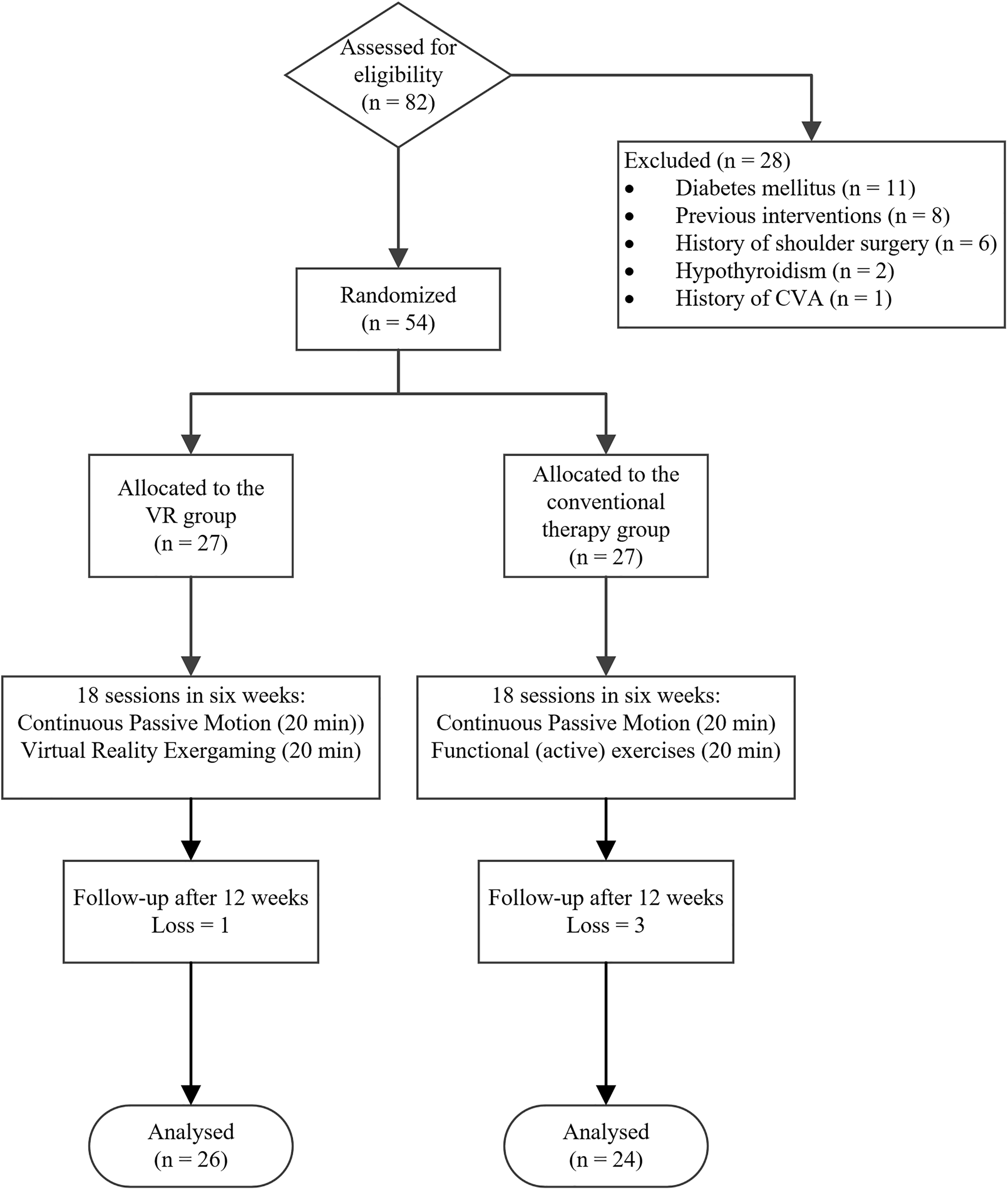
Flowchart of the randomized clinical trial.
We conducted a per-protocol analysis including only participants who completed the full 18 sessions and attended the follow-up. Participants with incomplete intervention or missing follow-up were excluded from the primary analysis, and no last observation carried forward or other single-value imputation was applied. This approach was chosen because the trial was designed as an explanatory/efficacy study to estimate the intervention effect under full adherence. Moreover, since the missing data were minimal (4/54, 7.4%) and predominately in the control arm, any conservative intention-to-treat imputation would, if anything, be expected to increase the observed advantage of VRT.
One patient in the CT group did not complete the 18 session and was therefore eliminated from the study. Furthermore, two patients from the same group did not show up for the follow-up assessment visit; they were also omitted from the trial. In the VRT group, all patients completed the 18-session trial. However, one was lost in the follow-up. No instances of cybersickness or any other adverse events throughout the study were observed.
Table 3 presents the demographic characteristics of the participants, detailing age, biological sex, affected shoulder dominance, symptom duration (weeks postonset), and baseline measurements for all of the outcome measures. No statistically significant differences were found in demographic characteristics or baseline measures between the two groups.
Demographic Data and Baseline Measurements
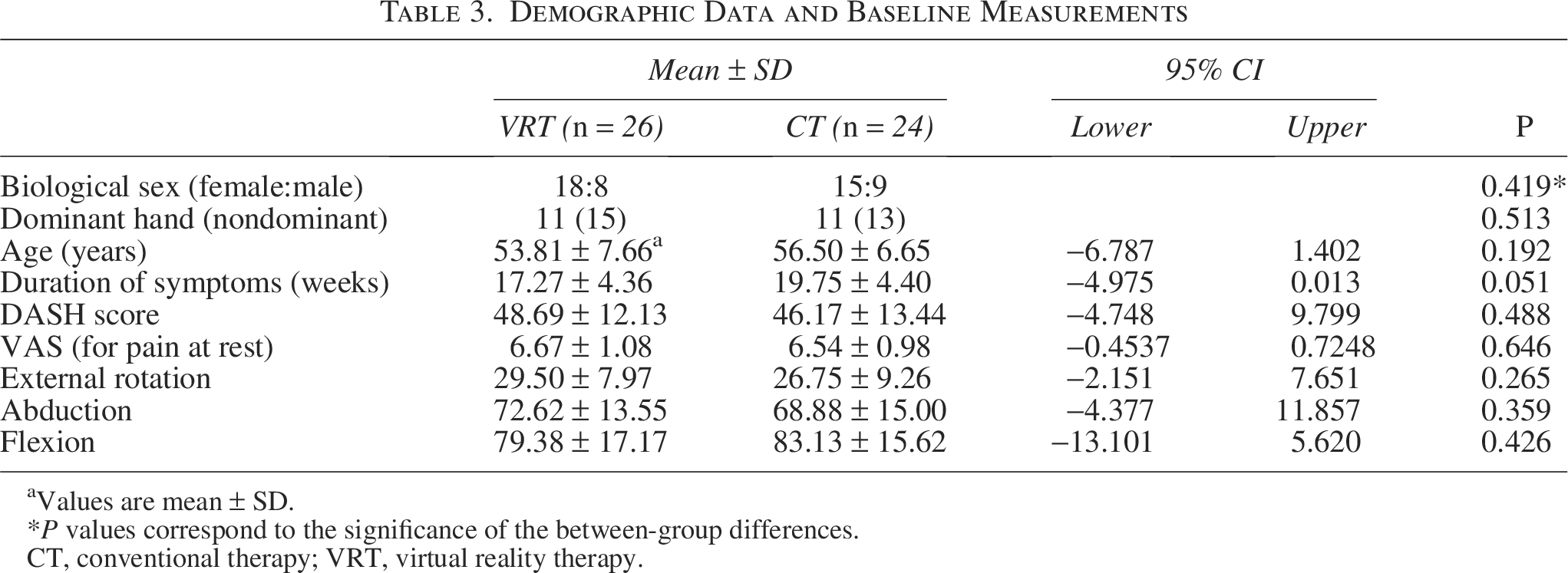
Values are mean ± SD.
P values correspond to the significance of the between-group differences.
CT, conventional therapy; VRT, virtual reality therapy.
Table 4 presents the baseline, posttrial, and follow-up measurements for all dependent variables, and Figure 3 illustrates the observed changes. A two-way repeated measures ANOVA for the main effect of time revealed that both groups demonstrated significant improvements in PROM as measured in external rotation (F(2,96) = 467, P < 0.001, η2 = 0.907), abduction (F(2,96) = 1689, P < 0.001, η2 = 0.972), and flexion (F(2,96) = 2350, P < 0.001, η2 = 0.980). As for the secondary outcome measures, both groups demonstrated significant improvements in the DASH score (F(2,96) = 391.7, P < 0.001, η2 = 0.891) and the pain at rest as measured by VAS (F(2, 96) = 1446.8, P < 0.001, η2 = 0.968). Using the specific MCID threshold of 1.4 cm for shoulder pain,
35
both groups demonstrated clinically significant improvements from baseline to 6 weeks. In the subsequent period from 6 weeks to the 12-week follow-up, the reduction in VAS scores in the CT group (
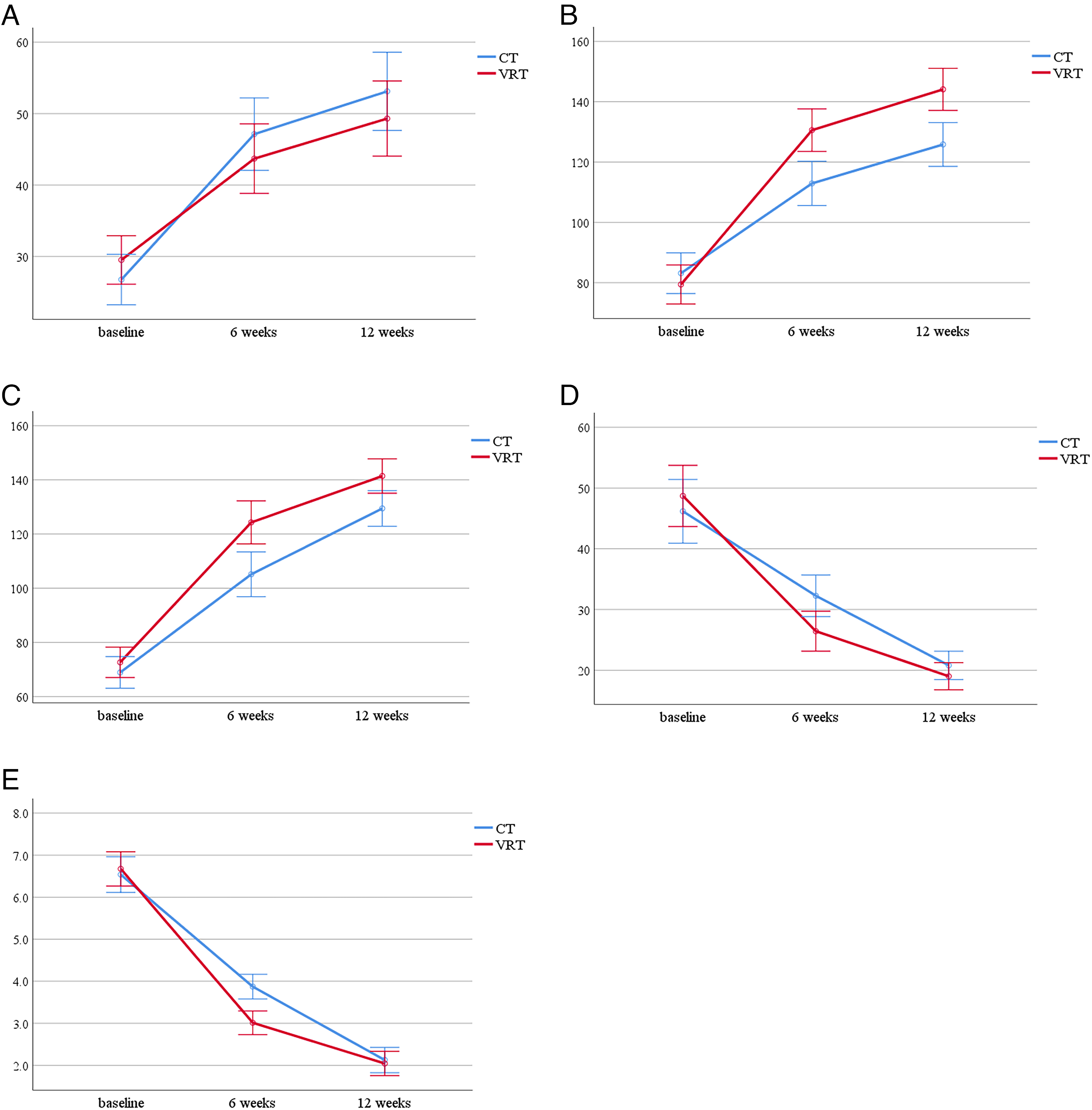
Changes in independent variables from baseline to posttrial (6 weeks) and follow-up (12 weeks). The subplots represent the variations in
The Measurements at Baseline, After 6 Weeks, and After 12 Weeks for All Outcome Measures
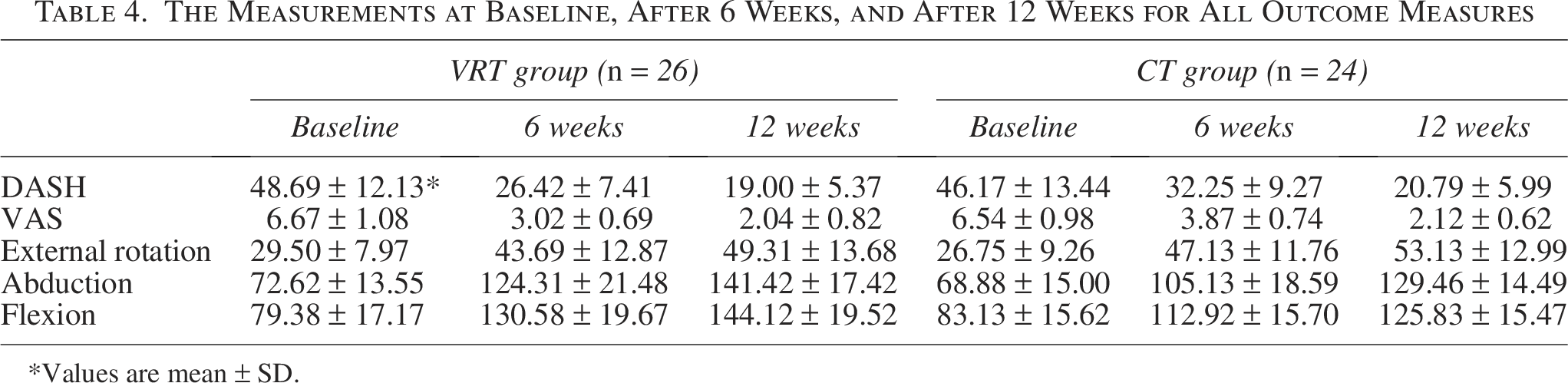
Values are mean ± SD.
The MCID for the DASH score was 10.2 points, 33 which was exceeded in both groups at both time points, from baseline to 6 weeks and from 6 weeks to follow-up.
Two-way repeated measures ANOVA for between-group analysis revealed no significant difference in the DASH score (F(1,48) = 0.501, P = 0.483, η2 = 0.010), or in the VAS (F(1,48) = 1.543, P = 0.220, η2 = 0.031). For passive range of motion, no significant difference was found between groups in external rotation (F(1,48) = 0.225, P = 0.637, η2 = 0.005); however, significant differences were observed in abduction (F(1,48) = 6.302, P = 0.015, η2 = 0.116) and flexion (F(1,48) = 4.957, P = 0.031, η2 = 0.094), with the VRT group demonstrating superior results. It can also be noted that the within-subject effect sizes for PROM, DASH, and VAS were extremely large (partial η2 range of 0.89–0.98), indicating substantial pre-to-post and follow-up improvements across both groups. Between-group effects for abduction (η2 = 0.116) and flexion (η2 = 0.094) corresponded to medium-to-large effects favoring the VRT group, while between-group effects for external rotation, DASH, and VAS were small or negligible.
Discussion
The primary aim of this randomized clinical trial was to evaluate the efficacy of immersive VR exergaming in rehabilitating patients with frozen shoulder. Additionally, we proposed a user-friendly gaming interface for integration into the rehabilitation process. Our results demonstrated statistically significant improvements in PROM, DASH score, and pain at rest (VAS) for both groups from baseline to the 12-week follow-up. Regarding clinical significance, the total change scores for both DASH (MCID = 10.2 points) and VAS (MCID = 1.4 cm) exceeded established thresholds, confirming that the overall intervention was clinically meaningful for all patients. However, a phase-specific analysis reveals distinct trajectories. While both groups met clinical thresholds during the active intervention (0–6 weeks), only the control group exceeded the VAS MCID during the maintenance period (6–12 weeks). The VRT group’s smaller change during this second phase (
While no significant differences were observed between groups in VAS, DASH score, and external rotation, the VRT group exhibited statistically significant superior outcomes in shoulder flexion and abduction.
One possible explanation for the better outcomes in abduction and flexion, but not in external rotation, could be the movements required in the VR exergaming module, which primarily mimicked abduction and flexion. This was due to the fact that imitating external rotation in Beat Saber was not as straightforward as imitating abduction and flexion. The Beat Saber module we used required frequent straight and diagonal slicing trajectories that, as implemented, produced combined flexion/abduction movements rather than isolated external rotation. Although orienting the arm between each two consecutive slices demanded internal/external rotation, isolated shoulder rotations were not practiced as a primary, repeated movement. Thus, the observed gains might be attributable to the frequency of practiced movements, rather than the total time spent in VR.
An exact quantitative analysis of the overlap between in-game actions and therapeutic shoulder movements would require instrumented motion capture using wearable inertial measurement units (IMUs), capturing three degrees of freedom for glenohumeral joint rotation and three for wrist position relative to the thoracic midline. Without such data, our mapping remains inferential, based on observed slicing patterns and biomechanics. Future studies could use IMUs to objectively map in-game actions to flexion/extension, abduction/adduction, and internal/external rotation, allowing designers to quantify the therapeutic dose delivered by specific VR content. An iterative process of custom level design and outcome analysis could further optimize VR exergaming modules for rehabilitation.
The content-dependence of VR therapy can also be inferred from the literature. In other words, while evidence suggests that an immersive VR experience by itself holds rehabilitative potential,13,37 maximizing the efficacy of VR technology necessitates careful consideration of the VR content. For instance, Hoffman et al. introduced “SnowWorld,” a game designed to immerse burn patients in an Antarctic-like setting where they interact with ice and snowballs. Their study demonstrated the effectiveness of SnowWorld in reducing procedural pain during wound care for burn patients. 15 However, when the same game was used in another study by Igna et al. on low back pain patients, results revealed no significant difference between the VR group playing SnowWorld and the control group. 36
This insufficient consideration of the VR content can also be found in the previous studies related to frozen shoulder rehabilitation. While they successfully demonstrated the feasibility of integrating the technology of VR in frozen shoulder rehabilitation, they paid less attention to the content actually being delivered in the virtual environment. In other words, they failed to raise and answer the question of whether the VR content incorporates sufficient therapeutic movements (flexion, abduction, internal/external rotation) to be acknowledged as a justifiable physical therapy for frozen shoulder. For instance, Wankhade et al. mentioned using “Hand Physics Lab” in the Oculus Quest 2 platform without any further explanation on the design of the shoulder movements required in their study. As another example, Demir et al. chose the game ‘The Climb,’ also on Oculus Quest 2, and justified their choice based on the enjoyable environment of the game and the fact that patients were required to reach out and stretch their arms to climb virtual rocks. While it is true that the game involves shoulder movements, it is questionable whether those movements are in compliance with established protocols for the treatment of frozen shoulder. This prompts a critical question to be answered: If the VR immersion was removed, would the underlying shoulder movements performed by patients still constitute a viable, evidence-based physical therapy for frozen shoulder?
In this regard, we advocate considering VR as a platform for gamification of the treatment, as opposed to considering VR as the standalone treatment. A reasonable strategy, therefore, is to design VR gameplay to imitate established rehabilitative movements while leveraging the immersive experience to overcome kinesiophobia, provide VR analgesia, and enhance patient motivation.10,14,15,38 Accordingly, we selected Beat Saber as it includes a “level editor” tool, enabling us to create custom levels with slicing patterns that closely replicate therapeutic movements for frozen shoulder. Inherently, the game demands focused attention and precise hand–eye coordination—qualities that, despite not being designed originally for rehabilitation, have proven transferable to clinical settings. 28 For instance, it has enhanced hand–eye coordination in stroke rehabilitation; improved sustained attention, processing speed, and working memory in traumatic brain injury patients; and boosted coordination and reaction time in students.28,39,40
The results of the current study align with previous research. Lee et al. devised seven tasks simulating frozen shoulder rehabilitation movements within a nonimmersive VR setting. Although their study lacked a control non-VR group, their results demonstrated enhanced Constant–Murley scores and shoulder PROM. 25 Wankhade et al. and Demir et al. conducted randomized controlled trials comparing the effectiveness of VR rehabilitation with conventional approaches for frozen shoulder. The trials indicated that the VR group exhibited superior outcomes in all metrics, including pain, shoulder function, and ROM compared with the conventional group. However, none of the studies mentioned above included a follow-up assessment to determine whether the superior results for the VR group were maintained. 26
In the absence of a follow-up assessment, an independent t-test conducted after 6 weeks of the current study would have indicated a statistically significant difference between the two groups, with the VRT group demonstrating superior results in the DASH score (P = 0.017), VAS (P < 0.001), flexion (P = 0.001), and abduction (P = 0.002). However, upon considering the follow-up assessment, a two-way repeated measures ANOVA revealed that the differences in the DASH score and VAS between the two groups were not sustained after 12 weeks. This finding suggests that VR rehabilitation may initially accelerate therapeutic outcomes. However, confirming this hypothesis requires further clinical trials.
Regarding the nonsignificant between-group differences in DASH and VAS scores—despite significant within-group improvements over time—one plausible explanation involves central sensitization, which can sustain pain amplification and functional deficits in frozen shoulder even as ROM enhances. As Balasch-Bernat et al. demonstrated, greater spatial extent of pain in these patients correlates with elevated pain intensity, catastrophizing, and central sensitization indicators (e.g., altered pressure pain thresholds and temporal summation), implying that our VR intervention may not have sufficiently targeted central nervous system mechanisms beyond CT. 41 Moreover, although the immersive VR experience likely mitigated pain during exercise performance through distraction mechanisms, 15 it did not alter resting pain as measured by VAS, significantly different compared with the CT group. Furthermore, by emphasizing therapeutic movements for ROM gains rather than integrating activities of daily living (ADL), the gameplay might have limited broader functional carryover to ADL-dependent metrics like DASH. Future studies could augment VR with ADL-simulated tasks or central sensitization-focused elements, such as graded exposure or multimodal pain education, to potentially yield superior between-group outcomes.
Due to the use of VR hardware in this study, it was not feasible to blind the patients or the clinician. Therefore, the potential for bias in patient responses and clinician assessments cannot be entirely ruled out. Another limitation of the current study is that we did not perform staging of the frozen shoulder patients. Exact staging typically requires shoulder arthrography and histopathologic findings, which were not conducted in our study due to budget constraints. However, we attempted to exclude stage-one frozen shoulder patients by not including individuals who experienced exacerbating shoulder pain in the past 2 weeks prior to recruitment. Another limitation is that although we instructed all patients to perform pendulum exercises at home three times a day for 5 minutes each time, we could not monitor adherence to this instruction. Variations in adherence could potentially affect the results of the clinical trial. Furthermore, the use of a VR controller by patients in the VR group, weighing approximately 200 grams and exerting a dynamic torque on the shoulder during active exercises. The impact of this additional loading on the rehabilitation process was not evaluated in our study. Additionally, the follow-up period in our study was limited to 6 weeks, whereas frozen shoulder recovery typically extends over a much longer course; therefore, long-term effects could not be assessed. Finally, as this was a single-center study with a relatively small sample size, the generalizability of our findings is limited.
Conclusion
This study assessed the effectiveness of immersive VR gaming in the rehabilitation of patients with frozen shoulder. Our findings indicated significant improvements in PROM, shoulder functionality, and pain in both the VR and control groups, with the VR group achieving better results in shoulder flexion and abduction. These results suggest that immersive VR exergaming may be a useful adjunct to conventional physical therapy for frozen-shoulder patients; however, given our limited sample size and evaluation of a single VR module, larger and more diverse trials are needed to confirm effectiveness and generalizability. An effective approach would involve designing VR gameplay that mimics established rehabilitative exercises, using the immersive nature of VR to boost patient participation. This study presents a novel and practical VR exergaming module suitable for clinical use. However, further research is necessary to determine the impact of various game designs on therapeutic outcomes.
Authors’ Contributions
A.B.: Conceptualization (equal) and writing—review and editing (equal). M.H.M.: Conceptualization (equal), writing—original draft (lead), formal analysis (lead), software (equal), and writing—review and editing (equal). M.H.: Conceptualization (equal), resources (equal), and software (equal). B.M.: Methodology (lead) and writing—review and editing (equal). R.M.: Resources (equal) and writing—review and editing (equal). S.M.: Conceptualization (equal) and supervision (lead).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.