
Abstract
Collagen, the most abundant structural protein in the human body, plays a vital role in wound healing, tissue repair, and skin integrity. Collagen-based products—ranging from wound dressings, skin substitutes, dental and orthopedic scaffolds, to topical cosmetics and oral supplements—have proliferated rapidly across healthcare and consumer markets. Medical applications leverage collagen’s biocompatibility, biodegradability, and scaffold-forming properties to manage chronic wounds, burns, and bone defects, while emerging technologies such as recombinant collagen and phage-integrated dressings target future innovations. Topical collagen improves skin hydration but is unlikely to replace endogenous collagen; injectable fillers offer temporary cosmetic enhancement with some potential risks. Oral collagen supplements, although marketed for skin, joint, and hair health, primarily serve as incomplete proteins and require cautious interpretation, as rigorous clinical evidence supporting transformative outcomes remains limited. Specific formulations such as undenatured type II collagen show promise for inflammatory joint conditions by promoting immune tolerance. In wound care, collagen-based scaffolds enhance healing by supporting fibroblast proliferation, reducing inflammation, and modulating moisture balance, while novel crosslinked matrices and living skin equivalents push regenerative medicine boundaries. Not all collagen-based products are the same. As the global collagen market surges toward $18.7 billion by 2030, users must distinguish between marketing claims and evidence-based benefits of specific preparations. Proper product selection should be guided by clinical context, molecular source (animal, marine, recombinant), and intended use with awareness of underlying scientific evidence critical to therapeutic success. Continued innovation, rigorous validation, mechanism of action studies and rigorous clinical testing are essential to fully realize collagen’s therapeutic potential across medicine and wellness.
Keywords
Chandan K. Sen
SCOPE AND SIGNIFICANCE
This article provides an overview of collagen-based products spanning wound care, skin health, regenerative medicine, orthopedics, dentistry, and consumer wellness. It critically examines collagen’s biomaterial properties—biocompatibility, biodegradability, and scaffold-forming capacity—that underpin its widespread applications. Common collagen-based products are systematically categorized based on scientific levels of evidence, offering users an evidence-based framework to navigate a rapidly expanding market. The work highlights emerging innovations such as recombinant collagen, 3D-printed skin grafts, and phage-integrated dressings, while cautioning against unsupported marketing claims. This work is not intended to be a systematic review. This is specifically a critical review (note peer-review process in Acknowledgments). While briefly noting key milestones in product development, the focus remains on technological trends, biomolecular sources, and functional advances. Projected to drive a $18.7 billion global market by 2030, collagen’s future hinges on rigorous validation, innovation, and responsible translation. 1 Serving health care providers, researchers, manufacturers, and informed consumers alike, this article delivers a critical, science-grounded roadmap to understanding collagen’s evolving impact across medical, cosmetic, and biotechnology sectors.
TRANSLATIONAL RELEVANCE
Collagen, the dominant structural protein in the human body (25–30% of total body protein), has been incorporated into a multitude of medical devices designed for wound healing, tissue regeneration, and skin care. Collagen can easily be isolated from animal, plant and marine sources, as well as be produced in a laboratory synthetically or as recombinant protein (Fig. 1). The abundant accessibility and ease of use in clinical applications has led to a global market of patient-accessible products that promote positive healing outcomes compared with more traditional approaches.
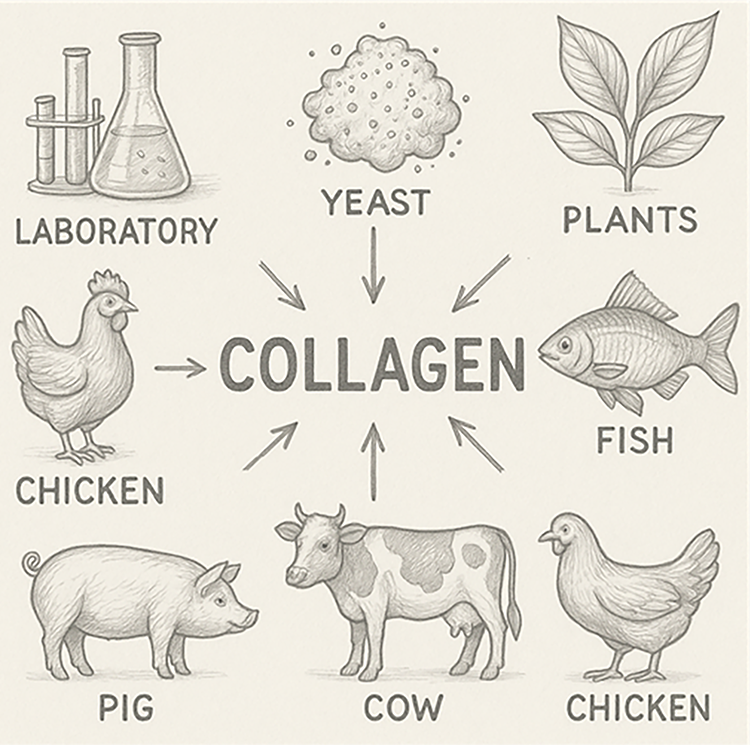
Collagen sources. Collagen is a protein abundantly available from a variety of sources. Collagen can easily be isolated from animal, plant, and marine sources. Collagens can also be produced in a laboratory synthetically or as yeast/fermentation-derived recombinant protein.
CLINICAL RELEVANCE
This article delivers critical insights for health care providers utilizing collagen-based products in clinical and wellness practice. It sketches the biological roles of collagen in wound healing, skin regeneration, orthopedic repair, and dental reconstruction, emphasizing how product-specific properties—such as molecular structure, source, crosslinking, and bioactivity—affect clinical outcomes. By categorizing commonly used collagen products according to levels of scientific evidence, the work offers an essential guide for evidence-based product selection. It highlights the importance of matching the product’s mechanism of action—such as scaffold support, moisture balance, matrix metalloproteinase inhibition, or antimicrobial enhancement—to the patient’s wound type and healing phase. Furthermore, it addresses emerging challenges such as biofilm resistance, impaired vascularization, and chronic wound recurrence, suggesting collagen innovations that may overcome these barriers. Health care providers are encouraged to critically evaluate marketing claims, understand product-specific risks, and prioritize products validated by rigorous clinical trials to optimize patient outcomes.
WOUND HEALING AND CARE
Collagen is the most abundant protein in the human body (25–30% total protein). There are at least 28 types of collagens of which over 90% of the collagen in humans is type I & III. Collagen-based products have proven beneficial, with utility spanning a range of products from medical devices to cosmetic and food applications. In 1981, Collagen Corporation (later Integra LifeSciences), launched CollaDerm, one of the first commercial collagen wound dressings with pre-marketing approval. In 1985, Johnson & Johnson introduced Instat, a collagen sponge indicated for hemostasis. 2 In 1996, Integra LifeSciences introduced Integra Dermal Regeneration Template (collagen-GAG matrix for burns and complex wounds). 3 In 1997 Smith & Nephew released Biostep (collagen-alginate dressing for moist wound healing). In 2000, SouthWest Technologies launched ColActive bovine collagen wound dressing. In 1998 and 2002, Johnson & Johnson received FDA approval for Fibracol (collagen-alginate wound dressing) and Promogran (collagen-oxidized regenerated cellulose matrix for chronic wounds), respectively (originally developed by J&J, now manufactured and sold by Solventum). 4 These products represent several historical examples showing progressive developments in collagen-based product development. An increasing demand for these products is showing economic impact at the U.S. and global scales. In 2024 U.S. collagen market reached $2.5 billion USD (Global $9.9 billion) and, with compound annual growth rate (CAGR) of 12.9%, is estimated to reach $4.94 billion USD by 2030 (Global CAGR 11.3%, $18.7 billion). 1 Collagen dressings and scaffolds are currently used to manage chronic wounds such as diabetic ulcers, venous stasis ulcers, and pressure ulcers. Useful collagen-based products seem to support wound care by providing a scaffold or matrix for new tissue growth, reducing inflammation, and helping maintain a moist wound environment. This work evaluates the state of scientific evidence on the most common collagen-based products in the market.
Wound care
Wound healing can be defined by four chronological, overlapping phases that include hemostasis, inflammation, proliferation and maturation.5,6 The hemostasis phase of wound healing consists of platelet hemostatic plug formation and fibrin crosslinking that creates a clot to prevent bleeding. 7 This response is immediate and can last hours depending on wound size and depth. Once the wound opening has been plugged, initial inflammatory response activates and recruits immune cells, such as neutrophils and macrophages, that in turn, recruit fibroblasts, epithelial and endothelial cells from surrounding tissues through proinflammatory cytokine release. 8 This initial inflammatory response occurs within hours and may last for days while infection surveillance and removal of bacteria and necrotic tissue is performed. Breached skin barriers allow for the introduction of microorganisms that can begin colonizing the wound surface, without impeding wound healing. However, if bacteria reach critical colonization, wound healing is hindered without triggering acute inflammation. A wound is considered infected when colony counts reach 100,000 organisms per gram of tissue per milliliter of fluid. 9 Compared with acute wounds, chronic wounds that have been infected are often complicated by a chronic inflammatory response that can disrupt subsequent stages of wound healing and result in impaired wound closure. 10 Overlapping with the resolution of the initial inflammatory phase, the proliferation phase expands and drives the activities of recruited fibroblasts, epithelial and endothelial cells, lasting on a scale of days to weeks. 5 Fragments from degraded collagen promote infiltrating fibroblast proliferation, deposition of collagen and extracellular matrix (ECM) components during granulation tissue formation. Fibroblast-like cells, originating from wound-macrophages, populate the granulation tissue. 11 Immune cells also contribute through the release of growth factors that promote keratinocyte re-epithelialization and endothelial cell angiogenesis programs. 12 The maturation phase of wound healing regulates ECM remodeling, which occurs during new ECM synthesis where fibroblasts, endothelial and epithelial cells release matrix metalloproteases (MMPs) that balance this process with degradation activity. 13 This balance ultimately defines the barrier functionality and tensile strength of healed skin, which due to differences in glycosylation and organization, can only reach up to 80% of original tissue maximum. 14 Hypertrophic and keloid scars form as this balance shifts toward excessive ECM formation and fibrosis, which continues to undergo remodeling for months or years after wound closure. During the process of wound healing and ECM remodeling, relative abundance of collagen I and collagen III change to support different biological processes. In early wound healing, collagen III is more prevalent to support the inflammatory and proliferative phases. Collagen I, however, becomes more prevalent than collagen III as the wound progresses through ECM remodeling in the late stages of wound healing. 15
Collagen synthesis is a tightly regulated biochemical process that begins with transcription of pro-α1 and pro-α2 chains and translation to pre-pro-polypeptide chains. 16 These chains undergo N-terminal cleavage, lysine and proline hydroxylation, and glycosylation post-translational modifications in the rough endoplasmic reticulum, necessary for the assembly of the procollagen triple helix structure. 17 Processing continues in the Golgi apparatus where procollagen is packaged into vesicles before secretion into extracellular space. Collagen peptidases then cleave the ends of procollagen to produce tropocollagen. 18 Lysyl oxidase facilitates subsequent tropocollagen molecule cross-linking to form collagen fibrils. 19 Molecular oxygen incorporation into nascent collagen is a critical step for collagen escape to extracellular space and proper maturation that provides tensile strength. 20 In ascorbate insufficient conditions (e.g., scurvy) collagen molecules do not undergo post-translational hydroxylation by prolyl hydroxylase and lysyl hydroxylase and fail to mature, resulting in weakened vessel formation during angiogenesis and impaired wound healing.20,21
Wound care is often complicated by factors associated with disease states and comorbidities. For example, diabetes is associated with peripheral arterial disease (PAD), a peripheral vascular disease, that is present in 7–12 million individuals in the United States with a prevalence disproportionately affecting black American patients. 22 PAD can result in ischemic peripheral tissues that experience tissue loss, ulcers, and gangrene. 20 Venous insufficiency, another peripheral limb ulcer-inducing condition, is a result of inflammatory-induced changes in venous walls and valves that cause retrograde blood flow. Interrupted blood flow in capillaries from hypervolemia or hypertension in veins can cause peripheral edema, deoxygenated venous blood pooling under the skin, venous ischemia and venous hypoxia. Subsequent skin damage in these areas can result in venous leg ulcers (VLUs). 23 These hypoxic conditions are detrimental to wound healing. Hypoxia in wounds can be mild-modest to near-anoxic depending on factors restricting O2 supply and lead to chronic non-healing or stalled wounds.24,25 Chronic wounds in the United States continue to be a significant health care burden, affecting upwards of 10.5 million Medicare beneficiaries, and are a major contributing factor to lower extremity amputations.26,27 Lower extremity amputation mortality rates at 1- and 10-year follow-ups reached staggering rates of 33.7% and 80%, respectively. 28
Acute moderate hypoxia, but not severe hypoxia, in wound beds stimulate healing through pro-angiogenic hypoxia inducible factor-1 and vascular endothelial growth factor (VEGF) signaling. 20 Severe near-anoxic hypoxia, however, leads to stalled wound healing by downregulating cell signaling and angiogenesis, inhibiting aerobic glycolysis that is required to meet the energy demands of a healing wound as well as by inhibiting collagen synthesis.20,29,30 Oxygen supply is required for stages of collagen deposition, polymerization, and maturation that are necessary structural components for new capillary tube formation during angiogenesis.31,32 With poor collagen deposition, weak tensile strength, and immature vessel formation, stalled wound healing exposes the wound bed to greater risk of infection and subsequent complications. Collagen-based dressings can be utilized to improve healing outcomes in ischemic wounds. In recent porcine ischemic full-thickness excisional wound studies, application of a modified collagen gel (MCG) induced monocyte chemoattractant protein-1-1 and VEGF expression, resulting in more endothelial cell infiltration and vascularization during healing. 33 Specifically, the MCG increased the initial transitory inflammation response, proliferative phase, angiogenesis and tissue maturation during remodeling, which showed improvement in three of the four phases of wound healing (inflammation, proliferation, maturation). 34 Mechanistically, a MCG dressing improved anti-inflammatory signaling through interleukin (IL)-10 production via the cytokine regulating miR-21-c-Jun N-terminal kinase pathway, increased the ratio of anti-inflammatory/pro-inflammatory macrophage polarization, and promoted angiogenesis through VEGF expression. 35 The microRNA miR-200 family has been implicated in hypoxia and ischemic tissue damage. 36 In an in vivo diabetic wound healing animal model, topical tissue nanotransfection of anti-miR-200b oligonucleotide promoted therapeutic tissue vascularization with significantly increased collagen deposition at the ischemic wound site. 37
Microbes infecting an open wound have the potential to develop a planktonic (free-living) infection, or they may form a polymicrobial aggregate known as biofilm. 38 Biofilm aggregates are able to adapt to their environment, as well as evade host immune cells and antimicrobials due to a protective extracellular polymeric layer. 39 Treatment of infected wounds is typically a combination of standard of care debridement and topical antimicrobials (such as hypochlorous acid) used in conjunction with systemic antimicrobial therapy. However, the resistant/evasive nature of biofilms coupled with an inability to easily visualize them results in high rates of biofilm recidivism. Biofilm infection not only contributes to open wound chronicity but also undermines the structural integrity of collagen as wound closure occurs. S. aureus biofilm infection, for example, represses miR-143, resulting in an upregulation of collagenolytic matrix metalloproteinase-2 and subsequent degradation of collagen type I as the wound heals. This results in a wound that achieves visual closure; however, the compromised tensile integrity of the newly formed skin means that the wound is likely to recur, seemingly spontaneously over time. 40 The transepidermal water loss study performed by the NIDDK Diabetic Foot Consortium shows that wounds that close without re-establishing barrier function are likely to recur.41,42 With 78.2% of chronic wounds showing signs of biofilm infection, identifying or synthesizing wound dressings that not only promote wound healing, but also eradicate biofilms, is a high priority in wound care. The use of biomaterials, including collagen-based dressings and scaffolds, has been beneficial in treating chronic wounds due to their biocompatibility and biodegradability, as well as properties that promote fibroblast infiltration and proliferation. 43 Stabilized pericardial collagen matrix, a cross-linked stabilized acellular equine pericardium-derived collagen matrix dressing, has been mechanistically shown to recruit macrophages to wounds and upregulate antimicrobial peptide human keratinocyte β-defensin (HDB-1) during wound healing, as well as calgranulin S100A9. HDB-1 protects the wound from microbial growth by directly disrupting bacterial membranes while S100A9 suppresses bacterial and fungal growth and recruits phagocytic immune cells to the site of injury. 44
Collagen-based dressings
Collagen serves as the principal structural ECM protein in the skin, tendon, and bone. 45 The most common collagen types (I–V) are differentially expressed within various tissues throughout the body: collagen I primarily in skin, tendon, bone, muscle, heart, lungs, and vessels; collagen II in cartilage; collagen III in vessels uterus and bowel; collagen IV in basement membranes; and collagen V in hair and nails.15,46 Because of its biocompatibility, biodegradability, and low immunogenicity, collagen has been used as a biomaterial for a wide range of applications. Collagen has been incorporated into products used for wound dressings, dental surgery, orthopedics, tissue engineering, pharmaceutical therapeutics, as well as food and cosmetic products (Fig. 2). 47 Traditional dressings composed of inert materials, such as cotton gauze, provide a passive protective barrier to prevent environmental debris and contamination from entering a wound. These dressings provide a layer of protection to promote healing and minimize risk of infection; however, they also have poor absorptive properties and moisture regulation that can cause wounds to dry out or dressings to adhere to wound and result in the need for frequent dressing changes. 48 Alternatively, semi-permeable wound dressings can adhere tightly to wounds to confine wound exudates and maintain a moist and oxygenated wound healing environment.48,49 While semi-permeable polyurethane-based dressings permit oxygen, carbon dioxide, and water vapor to pass through, they do not have moisture absorption or MMP neutralizing properties, thus limiting their most effective application to acute wounds and pressure ulcer prevention. 50 Managing wound exudates, moisture control, MMP neutralizing activity, biocompatibility, low immunogenicity, biodegradability, and antimicrobial activity are desirable properties in wound dressings that have prompted advances in dressing innovation and the development of collagen, alginate, elastin, hyaluronic acid (HA), and chitosan-based bioactive dressings, as well as living skin equivalents.51–56 Bioactive dressings are often combined with synthetic, chemical, or metallic antimicrobial agents to prevent wound infection during the healing process, which can be essential in the treatment of chronic slow-healing wounds. 57 Collagen-based bioactive wound care products have been developed for a multitude of applications and come in a variety of forms including dressings, sponges, gels, cross-linked hydrogels, powders, acellular scaffolds, and skin-like substitutes.
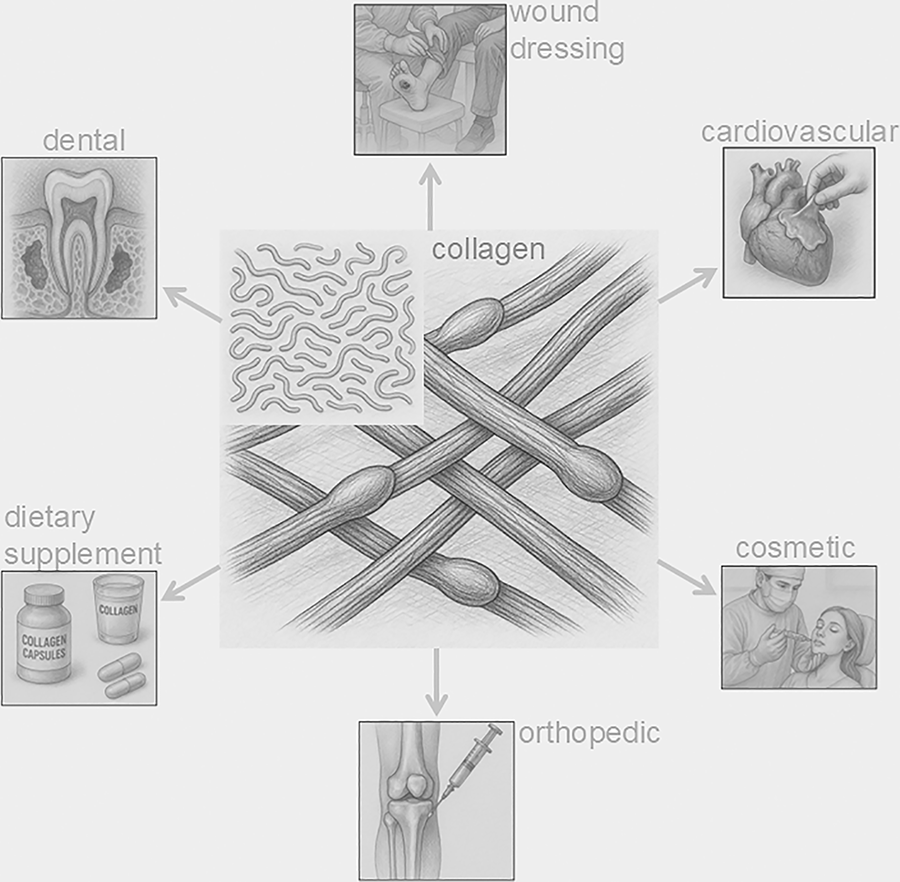
Collagen devices. Collagen, both native and hydrolyzed (image inset), has been used in a multitude of clinical products and devices. These products have shown positive outcomes in patients with regard to wound healing, cardiovascular regeneration, orthopedic repair, dental plugs and regeneration, dietary supplementation, and cosmetic implant and augmentations.
Collagen, as the primary structural protein in extracellular matrices, serves as a base material for wound dressings that are biocompatible, low antigenic, nontoxic, and biodegradable. 58 Collagen can be sourced from animals, plants or produced as recombinant protein, with porcine collagen being most similar to human collagen. Other animals commonly sourced include bovine, equine, ovine, rodent, poultry, and various marine animals.59–62 Air-drying or freeze-drying collagen can produce collagen film dressings that easily adhere to wounds and can promote keratinocyte proliferation and epidermal remodeling. 63 These films can be combined with growth factors, drugs, or nanoparticles for the slow-release treatment of wounds. However, collagen films are restricted for use on smaller wounds as excessive exudate and leakage can lead to pathogenic infiltration and infection. 64 Freeze-drying is also used to make collagen sponges that are porous scaffold materials, which retain mechanical strength, plasticity, and absorptive properties. 65 Collagen sponge properties are arguably more suitable for chronic wounds, dental applications, ulcers, and full-layer burn wounds with high levels of exudate as they are highly absorptive without adhering to wound beds. Native fibrous collagen matrix membranes have been utilized as guided bone regeneration dressings because of claimed better mechanical and osteoinductive properties than collagen sponges. 66 Collagen membranes combined with growth factors can promote an osteogenic environment that promotes horizontal bone augmentation and regeneration. 67 With similar activity, collagen plugs have been developed to guide bone regeneration following tooth extractions. Placed in the extraction socket, collagen plugs stabilize blood clots and support an osteogenic environment that can be further promoted with the addition of autologous bone chips. 66
Crosslinked collagen hydrogels may provide a transparent semi-permeable scaffold with high moisture content to possibly promote wound healing and necrotic tissue autolysis debridement.68–70 Nonadherence to the wound prevents tissue agitation and damage when the dressing is replaced. Additional crosslinking with HA and chitosan can improve the hydrogel water retention and bacterial barrier function, while also promoting cell migration, proliferation, and adhesion. 71 Collagen hydrogels, like other collagen dressings, can be combined with antibacterial peptides or growth factors to prevent bacterial growth and promote angiogenesis, granulation tissue formation, and tissue regeneration.72–74
Granulated or powdered hydrolyzed collagen, unlike hydrogels, tends to have minimal crosslinking and can vary in particle size based on methods of preparation (Fig. 3). 75 Collagen powders can be packed into ulcers, second-degree burns and wounds where they absorb exudate, control minor bleeding, and form a gel-like barrier that protects a moist wound environment. 5 Collagen powders, similar to hydrogels, can be used as drug delivery systems that are activated upon contact with the wound where high surface area ratio lends rapid delivery for treatments. 76
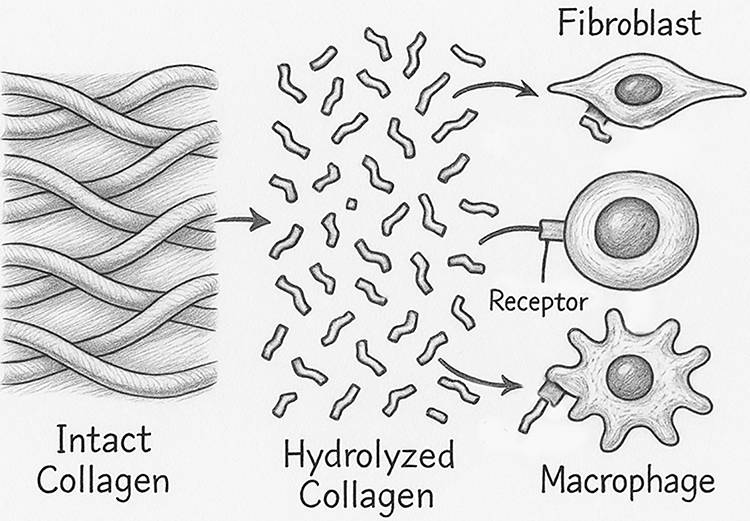
Intact versus hydrolyzed collagen. Intact collagen contains substantial crosslinking necessary for the structural support network it forms in the extracellular matrix. Hydrolyzed collagen peptides (often in granulated or powder products) tend to have minimal crosslinking and can vary in size based on methods of preparation. Receptors on fibroblasts and macrophages can bind hydrolyzed or degraded collagen peptides, which signal for proliferation, infiltration, and immune responses necessary in the wound healing process.
In addition to collagen being used as a bioactive dressing, acellular collagen scaffolds and living skin equivalents are also being utilized as effective skin graft substitutes. Decellularized fish skin, for example, is structurally similar to mammalian skin and exhibits high biocompatibility, porosity, absorptive capacity, biodegradability, and low immunogenicity. 77 Decellularized marine collagen appears to offer a notable advantage over mammalian-derived collagens by exhibiting a reduced risk of disease transmission when used as a graft in human patients.78–81 Decellularized collagen grafts from marine or mammalian sources have a structural advantage in the treatment of full thickness wounds and soft tissue augmentation with positive outcomes in thousands of clinical cases dating back to the mid-1990s. 82 Living skin equivalents are being designed to treat similar severe wounds through tissue engineering. Using a collagen gel, sponge, scaffold, or hydrogel as a common starting material, living skin equivalents are seeded with autologous (patient-derived) or allogenic (neonatal or newborn foreskin-derived) fibroblasts and keratinocytes to create a biocompatible dermal graft equivalent. 56 These living skin equivalents are applicable to deep wounds where collagen sponges and membranes are insufficient, including diabetic ulcers, venous ulcers, full-thickness burns, and other skin replacement procedures. Decellularized collagen scaffolds are also being used in the development of biological medical devices for hernia and heart valve repair.83–88
The collagen-based wound care market is evolving rapidly, with several innovative products in the pipeline leveraging advanced biomaterials, bioengineering, and antimicrobial technologies. Rigorous clinical studies are required as new products advance to the market. CollPlant (Israel) is developing rhCollagen (recombinant human collagen) from tobacco plants, expected to enter advanced wound care applications (e.g., 3D-printed skin grafts). 89 Potential benefits include lower immunogenicity, scalable production, and no animal-derived risks. Yeast/fermentation-derived collagen are under development for the wound care market. Companies such as Geltor (United States) 90 and Jellatech (Denmark) 91 are working on biosynthetic collagen for medical use, including wound dressings. Phage-integrated collagen comprises bacteriophage-infused dressings designed to target pathogens such as MRSA and Pseudomonas. These dressings are currently in clinical trials by Nextbiotics & Adaptive Phage Therapeutics. In addition, companies such as Pandorum Technologies (India) 92 are developing 3D-printed collagen-based corneas, while Poietis (France) 93 is testing 3D-printed collagen-based living skin for the treatment of burns and chronic ulcers. Drug-eluting collagen dressings are in the pipeline. Platelet-derived growth factor/VEGF-loaded collagen (similar to Regranex but cheaper) are in development by Helix Biomedix.
REGENERATIVE MEDICINE
Regenerative medicine 94 is a rapidly developing field in health care. This evolving field of study harnesses cells, scaffolds, gene delivery, or their combination to heal damaged or diseased tissue back to their native functional state. 95 Since the first U.S. FDA approved skin substitute came to market in 1997, tissue engineers have developed multiple approaches to treat a variety of wounds, from mild and severe burns to abrasions and lacerations. While mild wounds may heal in days, severe wounds or wounds with complications from underlying disease or infection require the assistance of a scaffold structure capable of maintaining a moist wound environment, as well as modulating the phases of healing to bring complete closure. Collagen has come to the forefront of many approaches because of its biocompatibility, bioactivity, and low antigenicity. 58 Often used as a wound dressing, collagen-based products come in sheets, powders, and hydrogels, among others (Tables 1–6).
Level of evidence 1
Collagen-based products levels of evidence. Level 1 ≥ 3 RCT; Level 2 = 1 well-designed RCT/multi-site study; Level 3 = clinical studies—observational/mechanism of action (MoA); Level 4 = historical cohort (retrospective) or case-control studies (retrospective with control group); Level 5 = other clinical studies (case series or studies as reference treatment, human ex vivo MoA); Level 6a = large animal with MoA; Level 6b = large animal observational; Level 7a = small animal with MoA; Level 7b = small animal observational and in vitro. FDA status: □ - cleared; ■ - approved.
Level of evidence 2
Collagen-based products levels of evidence. Level 2 = 1 well-designed RCT/multi-site study; Level 3 = clinical studies—observational/mechanism of action (MoA); Level 4 = historical cohort (retrospective) or case-control studies (retrospective with control group); Level 5 = other clinical studies (case series or studies as reference treatment, human ex vivo MoA); Level 6a = large animal with MoA; Level 6b = large animal observational; Level 7a = small animal with MoA; Level 7b = small animal observational and in vitro. FDA status: □ - cleared; ■ - approved.
Level of evidence 3
Collagen-based products levels of evidence. Level 3 = clinical studies—observational/mechanism of action (MoA); Level 4 = historical cohort (retrospective) or case-control studies (retrospective with control group); Level 5 = other clinical studies (case series or studies as reference treatment, human ex vivo MoA); Level 6a = large animal with MoA; Level 6b = large animal observational; Level 7a = small animal with MoA; Level 7b = small animal observational and in vitro. FDA status: □ - cleared; ■ - approved.
Level of evidence 4
Collagen-based products levels of evidence. Level 4 = historical cohort (retrospective) or case-control studies (retrospective with control group); Level 5 = other clinical studies (case series or studies as reference treatment, human ex vivo MoA); Level 6a = large animal with MoA; Level 6b = large animal observational; Level 7a = small animal with MoA; Level 7b = small animal observational and in vitro. FDA status: □ - cleared; ■ - approved.
Level of evidence 5

Collagen-based products levels of evidence. Level 5 = other clinical studies (case series or studies as reference treatment, human ex vivo MoA); Level 6a = large animal with MoA; Level 6b = large animal observational; Level 7a = small animal with MoA; Level 7b = small animal observational and in vitro. FDA status: □ - cleared; ■ - approved.
Level of evidence 7
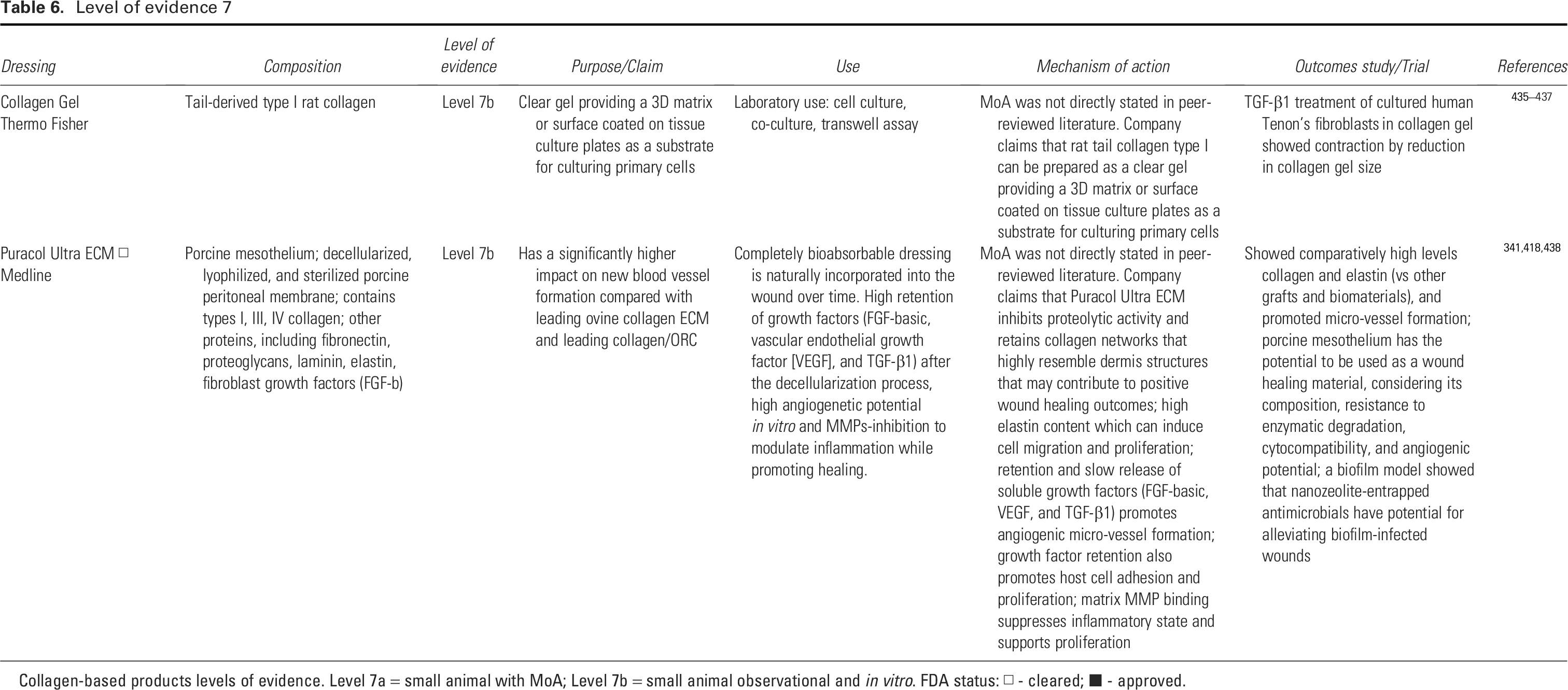
Collagen-based products levels of evidence. Level 7a = small animal with MoA; Level 7b = small animal observational and in vitro. FDA status: □ - cleared; ■ - approved.
Skin substitutes
Natural wound healing re-establishes a barrier between vulnerable inner tissues and an environment full of harmful substances and pathogens. Skin is the body’s first line of defense against environmental factors. Disrupting this barrier through wounds or disease exposes the body to risk of infection, which is exacerbated in individuals with compromising medical conditions such as diabetes and obesity. 439 The ability to restore damaged skin with surgical intervention dates back 2,600 years ago. The “father of plastic surgery,” Sushruta, was an innovative surgeon in Kashi, India in the year 600 BCE. 440 He was renowned for reconstructive surgeries, such as utilizing cheek flaps for nose reconstruction, as well as developing a code of medical ethics. Grafting techniques progressed steadily in the 19th and 20th centuries, leading to a profound breakthrough in 1981 when John Burke and colleagues developed an artificial skin substitute with a top layer of silicone polymer and bottom layer of crosslinked collagen and glycosaminoglycans (GAGs). 441 This provided the foundation for tissue engineering techniques that led to modern collagen-based products designed for biocompatibility, while establishing a structural framework to promote more efficient tissue growth, reduce inflammatory response, maintain a moist environment, and inhibit microbial infection.
The first U.S. FDA approved skin substitutes were TransCyte (Advanced Tissue Science, La Jolla, CA) and Dermagraft (developed by Advanced Tissue Sciences, now marketed by Organogenesis Inc., Canton, MA). These products consisted of a polymer mesh scaffold on which human fibroblasts were cultured which secreted collagen, along with other ECM proteins, growth factors, and cytokines, to support skin wound healing. In the case of TransCyte, the scaffold includes a silicone membrane and the tissue was frozen to kill the cells and allow storage. 442 Dermagraft was cryopreserved and the cells retained some viability. 95 As dressings, they are indicated for partial thickness burns, surgical wounds, and diabetic foot ulcers without tendon, muscle, or bone exposure, providing improved patient wound healing outcomes compared with standard of care.272,442 More recent dressings have drifted away from the necessity of culturing live human fibroblasts, rather, developing dressings comprised of collagen has increased the shelf-life, long-term stability, and shortened preparation time prior to use, while still promoting wound healing outcomes. Combining modern collagen-based biomaterials with growth factors is an approach being used to support tissue regeneration in chronic wounds. For example, VEGF fused with a collagen-binding domain has been incorporated into a collagen-based biomaterial to essentially create a slow-release drug delivery system that promotes angiogenesis and revascularization of chronic diabetic wounds. 443 Similar methods have been developed for collagen-B-cell leukemia/lymphoma 2-adipose-derived stem cell scaffolds, 444 collagen-copper/cobalt bioactive microfibrous glass mats, 445 and collagen matrix hydrogel delivery of basic fibroblast growth factor (bFGF). 446 Puracol Ultra ECM has also been used to deliver FGF to promote regenerative wound healing in a small animal aortic ring assay. 447
Cardiovascular collagen
Defects in collagen from mutations in the collagen type I/III genes can be responsible for cardiovascular diseases and abnormalities such as aortic dilation, aortic aneurysms, arterial dissection, and rupture. 448 While defects in collagen can result in cardiovascular abnormalities, tissue engineered collagen products can be used to treat them in vivo. The most common surgical treatments for atherosclerosis, for example, still include vascular bypass and replacement. Patents with atherosclerosis, however, often have poor vein and artery health, making them poor candidates for autograft harvesting. Collagen-based vascular grafts have become alternative materials for transplantation when combined with other natural (fibrin, elastin) or synthetic (polyurethane, polydioxanone, polycaprolactone) materials, which can bolster collagen’s mechanical properties without diminishing the beneficial biocompatibility, cell adhesion, biodegradability, hydrophilicity, and weak immunogenicity properties of collagen. 449 Dacron vascular grafts, for example, when coated with collagen have long-term secondary corrected 8-year patency rates >90%. 450 Collagen engineered vascular products can also be utilized as drug delivery systems with VEGF and bFGF, promoting post-transplant endothelialization while limiting thrombosis and intimal hyperplasia. 451 In the case of bFGF delivery, heparinized collagen-coated vascular grafts (with embedded heparin) resulted in long term patency by mimicking the mechanism of heparin sulfate present in native ECM of endothelial cells that binds and stabilizes bFGF, releasing it upon vascular wall damage, resulting in localized bFGF release and proliferation of endothelial cells. 451 Antibiotics and antimicrobial peptides have also been incorporated into collagen-based vascular grafts to prevent perioperative infection. 452 Collagen-based hydrogels have also been used as an injectable therapeutic to prevent myocardial infarction by providing ventricular wall thickness and mechanical support without hindering myocardial contraction. Studies have shown, however, that there is a therapeutic window post-myocardial infarction when this treatment is most beneficial because of pathophysiological stages of necrosis, inflammation, proliferation, and maturation.453,454 These collagen hydrogels have also been used as delivery systems for therapeutic drugs and stem cells to treat cardiovascular disease. 449 Akin to hydrogels, collagen-based patch scaffolds have been developed to serve as epicardial dressings for reconstruction of large cardiovascular defects. These dressings can be loaded with conductive material, bioactive drugs, stem cells, and exosomes to facilitate the reconstruction and regeneration of large cardiac and vascular defects. 449
SKIN HEALTH
Skin collagen synthesis
Skin, the body’s largest organ, structurally serves as a protective barrier against environmental stressors and damage. The importance of maintaining skin health throughout one’s lifetime has become a more widely accepted practice as awareness has spread of skin cancer as being the most diagnosed cancer in the world that is also preventable. 455 Evidence for age-related weakened barrier functions has also supported the need for healthy skin practices. 456 Photoaging, caused by prolonged exposure to extrinsic ultraviolet (UV) radiation, has not only been identified as one of the main risk factors for melanoma, but also has a profoundly detrimental effect on ECM deposition in the dermis. 457 Photoaging causes fragmentation and degradation of collagen, the main structural component of ECM.458,459 Disruptions in collagen synthesis have been correlated with a spectrum of diseases that have been traced back to over 1,000 mutations in patients. 460 Heritable genetic disorders have been identified that cause disrupted collagen fibril formation in skin biopsies. 461 Ehlers-Danlos Syndrome, for example, is one such disorder mostly attributed to mutations in COL5A1 and COL5A2 genes, and in rare cases COL3A1. Resulting haploinsufficiency of type V collagen can manifest symptoms in varying degrees of severity from mild to fatal, including skin hyperextensibility, joint hypermobility, tissue fragility, delayed wound healing and atrophic scarring, and vascular ruptures.462–467
Skin collagen is primarily derived from triple helix procollagen produced by fibroblasts. 15 Collagen turnover occurs at different rates in different tissues, with a half-life of skin collagen (insoluble) of approximately 15 years, whereas cartilage collagen half-life can reach 117 years. 468 Endogenous synthesis of skin collagen studies in 1964 revealed glycine as the most abundant amino acid making up its triple helical structure.469,470 Further study has shown that collagen’s amino acid composition is roughly 1/3 glycine, 0.7/3 proline (+hydroxyproline), and 1.3/3 other amino acids, and that limiting glycine and proline limits maximal collagen synthesis, 471 with proline biosynthesis as a rate limiting factor. 472 Glycine, proline, and hydroxyproline have now made their way into global markets in the form of hydrolyzed collagen peptides present in wound dressings, as well as skin care and food products.
Topical collagen applications
Topically applied collagen products are becoming more popular in skin care markets. However, topical applications of intact collagen capable of replacing endogenous collagen within the skin is a common misconception. Native collagen that has been topically applied has poor permeability and cannot penetrate the skin barrier. 473 When hydrolyzed, even collagen peptides larger than six to seven amino acids cannot be efficiently absorbed (Fig. 3). 474 One of the most common used topical collagen products is hydrolyzed collagen tripeptide (CTP) sequence Gly-X-Y (often Gly-prolyl-hydroxyproline [Pro-Hyp]). It is an abundantly available biological material that has low allogeneic properties, making it a desirable component for topical and oral collagen-based products. 475 The application of CTP has been considered to contribute to smoothing of facial wrinkles and improving skin elasticity; however, these observations are also coupled with increased moisture content. Collagen is hygroscopic (attracts water), so when applied topically, it forms a moisturizing film that plumps the skin, reducing fine lines temporarily. It may also temporarily strengthen the skin barrier, preventing moisture loss (e.g., in dry or aged skin). High-molecular-weight collagen (in creams/sheets) may sit on the skin’s surface, creating an optical smoothing effect—similar to silicone scar sheets. 476 Some hydrolyzed collagen peptides (small fragments) can arguably signal fibroblasts (skin cells) to boost collagen and elastin synthesis (via transforming growth factor-β [TGF-β] and other growth factors). 476 Some collagen products may have antioxidant properties that neutralize free radicals (reducing UV-induced damage). 474 Most of these plausible mechanisms require rigorous testing in appropriately designed clinical trials. The hype for such cosmetic and aesthetic products in the market seems to be frequently generated by aggressive marketing strategies not supported by rigorous science. Appropriate consumer caution and due diligence are thus warranted.
Collagen-based fillers
Collagen injections have been a trend in cosmetic research to fill facial voids, enhance volume and remove wrinkles. Conceptually, collagen injections in the mid-to-deep layers of the skin act as support structures that remove wrinkles and skin folds. Products claim that injected collagen is absorbed within a month of injection and replaced by native de novo synthesized collagen by 3 months postinjection.477,478 Rigorous clinical studies are necessary to support these claims. Recent retrospective analysis of clinical data for facial wrinkles treated with collagen type III injections showed significant improvement in experimental subjects compared to control subjects at 30 days postinjection. 479 Ninety days postinjection, however, there was no significant difference between the groups, suggesting that the collagen filler was broken down and resorbed rather than replaced. 479 Individuals considering use of collagen dermal fillers should also be cautioned that mild to severe complication risks have been associated with their use, including discoloration, necrosis, infection, vision loss, granuloma formation, foreign body reaction, and biofilm formation.480,481 Because of potential adverse events, including autoimmune response, which required sensitivity reaction testing, several collagen fillers (including Zyderm, Zyplast, Cosmoderm, Cosmoplast) have been discontinued.399,400 Noncollagen dermal fillers have also been developed as potentially safer or longer lasting alternatives. Injectable poly-L-lactic acid (PLLA), HA, calcium hydroxyapatite (CaHA), polymethyl methacrylate (PMMA), polyalkylimide, and silicone implants have been used to varying degrees of success.263,482 Challenges and complications vary depending on biodegradable (PLLA, HA, CaHA) and nonbiodegradable (PMMA, polyalkylimide, silicone) properties. 483 Because of the short-term effects of collagen fillers that are typically depleted 3–4 months postinjection, HA has become a more commonly used alternative which can last 12–24 months. 484 Collagen and HA dermal fillers currently have in vivo mechanisms of action that are not fully understood, as well as short and long-term complication risks that should be discussed with physicians before injection procedures. Additional rigorous scientific studies are required.
ORTHOPEDICS AND DENTAL APPLICATIONS
Tendon repair
Collagen-based scaffolds and matrices are used in bone grafts, cartilage repair, and tendon or ligament reconstruction (Fig. 2). They serve as a scaffold that promotes the regeneration of bone and soft tissues in joint repairs and spinal surgeries. Sports injuries, for example, are often associated with bone and tendon injury as a result of overuse or trauma. Tendons are connective tissues with a multitude of organized collagen fiber bundles. 485 Tendon injuries are painful and typically slow to heal, even when treated with nonsurgical drug, stem cell, or physical therapies. 486 bFGF can aid in accelerated tendon healing by promoting neovascularization during the pro-inflammatory phase, while also stimulating fibroblast production of type III/I collagens during the cell proliferation phase of healing. Overuse of bFGF can overstimulate these processes however, leading to fibrotic scar formation and potential tendon adhesions. 487 A common musculoskeletal disability that occurs in approximately 8% of adults is rotator cuff damage, resulting from acute tear injuries or age-related degeneration. 488 The use of acellular scaffolding, such as GraftJacket, retains intact collagen ECM and blood vessel channels with low immunogenicity.296,297 These acellular dermal matrices show promising results in repairing large rotator cuff tears in patients, with little to no adverse events. 297 Another application of collagen-based products to support orthopedic regeneration comes from the use of dehydrated human placental allograft amnion-chorion membrane material (NuShield) that retains collagens, ECM proteins, growth factors, elastin, glycoproteins, and proteoglycans. 305 When applied to tendon, spinal or nerve damage, placental allografts release growth factors and cytokines to promote fibroblast and keratinocyte migration and proliferation, while paracrine signaling subsequently regulates localized inflammatory responses. 305 This dehydrated placental allograft material has shown promising results as regenerative treatments for tendons, nerves, spinal adhesions, and fibrosis, as well as treatment for chronic wounds.489,490
Bone grafting
Bone repair is a major challenge in the musculoskeletal regenerative therapy field. Common bone defects are the result of osteoporosis weakening of bones, traumatic fractures and breaks, osteomyelitis, periodontitis, congenital defects, and hereditary diseases. 491 Mutations in the COL1A1 and COL1A2 genes can result in multiple subtypes of osteogenesis imperfecta or “brittle bone disease.” 467 The lack of suitable donors for bone grafting is compounded by the risk of immune rejection, while autologous bone grafting is limited by the patient’s own available donor material, which also carries the risk of causing irreversible damage when harvested. The application of collagen-based biomaterials provides a matrix for cell infiltration and proliferation that, when combined with porous material and factors such as connective tissue growth factor (CTGF) or bone morphogenic proteins (BMP), establish an osteogenic microenvironment that promotes osteoblast deposition of bone matrix.492,493 Recent clinical trials have shown that the use of calcium phosphate cement is useful in reducing fractures and pain while improving functional outcomes. 494 However, limited osteoinductivity and resulting tensile strength make it an undesirable void filler for larger defects. 494 Biomaterials have been making significant progress as alternative bone void filler options that contain collagen to promote bone healing processes. A combination of calcium phosphate, dibasic (DICAL), and purified type 1 bovine collagen (CopiOs) has been used as an osteoconductive sponge scaffold to promote regeneration of bone voids (Table 3). The DICAL-collagen product, when coated with BMP, has shown success in filling post-harvest iliac crest donor sites in spinal fusion surgery and in promoting bone growth in large tibial defects in animal models by creating a microenvironment that supports osteogenesis. 346 This approach is designed to mitigate donor site risk complications of morbidity (9.4 − 49%) and chronic pain at iliac crest autograft harvest sites.495–499 Combining collagen-based biomaterial (Healos) with bone marrow aspirate (BMA), that has undergone selective cell retention of mesenchymal stem cells (MSCs), has produced a substitute for autologous iliac crest bone grafts in lumbar spinal fusion procedures. 382 Strips of this biomaterial loaded with MSCs and CTGF have been implanted in posterolateral fusion procedures in 21 patients, 100% of which achieved successful solid bilateral fusions. 382 For the treatment of long bone fractures, porous beads comprised of hydroxyapatite, tricalcium phosphate ceramic, and fibrillar type 1 bovine collagen (CollaGraft) have been developed to create a biodegradable osteoconductive scaffold. 253 When preloaded with BMA, this biodegradable scaffold has been used successfully to promote bone repair in patients with long bone fractures.253,254 This combination has also shown promise as an autologous bone graft substitute in large animal models. 255 The use of collagen-based biomaterials for treatment of bone damage has proven to be beneficial in repairing small bony voids and long bone fractures, as well as providing scaffold and osteogenic support for bone fusion procedures (Tables 1–6). These same principles have been used to promote wound healing and bone regeneration in oral and maxillofacial surgeries.
Dental applications
Collagen membranes and graft materials are used in oral surgery, particularly for periodontal regeneration and guided bone regeneration (Fig. 2). Periodontal disease, or gum disease, commonly refers to inflammatory disorders ranging from mild reversible gingivitis to the more severe irreversible periodontitis gum infection that causes loss of connective tissue and bone support, often leading to tooth loss. 500 Beyond causes such as plaque buildup, periodontal disease has been defined as a systemic disease associated with a host of other morbidities. 501 Severe periodontitis reached a prevalence of 23.6% in dentate adults in 2020, which is striking when considering that periodontitis is the medical basis for roughly 25–38% of tooth extractions. 502 To promote better healing and recovery following dental surgery procedures, researchers have been developing collagen-based materials that promote clotting, tissue regeneration, and bone preservation. The use of bioabsorbable collagen membranes in periodontal regeneration procedures also prevents the need for membrane removal surgery while also limiting the risks of bacterial colonization. 503
An absorbable porous collagen sponge material (CollaCote) is beneficial as a collagen-based product that can be packed into a root canal space following debridement, along with a barrier of mineral trioxide aggregates (Table 2). This collagen matrix is fully absorbed in 10–12 days and promotes obturation, or closure, of the canal space through host cell migration and osteoinductivity into homogeneously spaced micropores.246,247 After tooth extraction, applying a biodegradable collagen plug (CollaPlug) before socket suturing has been shown to reduce postoperative bleeding and pain. The plug acts as a hemostatic material by absorbing fluids, enhancing clot formation, and accelerating granulation tissue development. 341 The same collagen plug has demonstrated, with the addition of platelet rich fibrin, that it contributes to alveolar ridge preservation in extraction sockets, preserving bone width for up to 4 months. 342 Animal studies have shown that fibrillar collagen (CollaTape) promotes early phases of bone healing through osteoblast surface fibronectin-mediated adhesion and collagen-driven angiogenesis. 248 This effect was limited by the degradation of collagen dressing within 5 weeks of application. Longer-term ridge preservation could be achieved by adding synthetic bone particles to the extraction socket prior to closing the wound with collagen dressing.
Other collagen products used in oral surgery are applied to cover socket void fillers as a membranous sheet. For example, a non-crosslinked bilayer collagen membrane osteophilic matrix (Bio-Gide) has a film layer designed to prevent soft tissue invasion into the socket, thus promoting alveolar ridge preservation and bone regeneration.133,504 A comparable product with a sugar crosslinked collagen membrane (Ossix Plus) prevented host cell infiltration 409 (Tables 1, 5). The noncrosslinked structure of collagen membranes (Bio-Gide) promoted angiogenesis and vascularization in the wound; whereas crosslinked collagen membranes (Ossix Plus) were not permissive for angiogenesis, yet still allowed nutrient permeation. 410 Filling extraction sockets with deproteinized bovine bone mineral and 10% porcine type 1 collagen (Bio-Oss) prior to sealing with extraction sockets with noncrosslinked bilayer collagen membrane (Bio-Gide) significantly improved bone height and width preservation for 6 months postextraction. 133 The use of collagen products singly, or in combination, can preserve alveolar bone which otherwise would undergo the healing-induced remodeling and volumetric loss of socket contour post-tooth extraction. 133 Thus, use of these collagen products may preserve alveolar ridge necessary for subsequent dental implants without the need for additional bone grafting.
COLLAGEN AS DIETARY SUPPLEMENT
The greatest proportion of collagen products currently resides with the food industry, reaching just over 55% of the total U.S. collagen market in 2024, followed by medical products. The food industry use of collagen shows up in a variety of forms from the casings around sausages, to thickening agents such as gelatin that are used to increase viscosity or as a way of regulating flavor release.505,506 Collagen is also used in the food preservation industry to prevent water loss from meat during freezing/thawing and even shows up in ice cream products to prevent ice crystal formation. With such a large portion of the multi-billion-dollar collagen market being dedicated to the food industry, an important question comes to the forefront: Is collagen beneficial to eat?
Collagen supplements are showing up in food and beverage products across the globe, with claims of a variety of health benefits (Fig. 2). Predominantly found in connective tissues such as skin, cartilage, and bone, cartilage is recognized as source of fiber and protein. Protein Digestibility-Corrected Amino Acid Score evaluation following World Health Organization guidelines marks collagen as an incomplete protein source because of lack of tryptophan. Even so, peptides can substitute up to 36% of the daily protein requirements in the Western diet. 507 This means that, while collagen cannot be used as a complete protein substitute, it may be a safe dietary supplement when used up to approximately one-third of a mixed protein diet.
One of the common health benefits advertised for ingested collagen products is healthier, more elastic skin with reduced wrinkle lines. It is unclear, however, what direct mechanisms of action may be responsible for these proclaimed benefits. There have been studies that make correlations between ingesting collagen bioactive dipeptides (Pro-Hyp and Hyp-Gly) or tripeptides (Gly-X-Y) and increased skin water content.508–511 There is also evidence that oral ingestion of collagen peptides increases natural moisturizing factors in the stratum corneum including urea, lactic acid, filaggrin-derived amino acids, pyrrolidone carboxylic acid, and urocanic acid.512,513 However, these observations did not show that ingestion of bioactive collagen peptides have an effect on collagen production, or retention of native collagen, within the skin.
Randomized controlled trials (RCTs) have shown that the ingestion of collagen hydrolysates and hydrolyzed collage-based supplements have a beneficial effect on wound healing for patients with burn wounds or pressure ulcers, respectively.514,515 More recently, collagen peptides administered in combination with omega-3 fatty acids have been suggested as oral supplements with the potential to improve inflammatory responses and dysbiosis in burn patients. An RCT was performed on burn patients to determine if ingested collagen peptides were beneficial to regulate gut microbiome colonization, acting as a preventative treatment for dysbiosis. Patients did not, however, have any significant changes in Lactobacillus, Enterobacteriaceae, or F. prausnitzii concentrations between treatment groups. 447 The mechanism for how ingested collagen is utilized for therapeutic benefit in wound healing or skin elasticity has not yet been defined, yet there are still strong correlative findings in experimental trials.475,514–516 Rigorous scientific studies are needed. It is unlikely that ingested collagen is incorporated directly, for example, into the dermis to supplant and replace regions of damaged or degrading collagen. It seems much more likely that once ingested, collagen is digested down to amino acids and short peptides that can circulate and be utilized by regenerative processes as base material for de novo collagen synthesis.
Oral collagen consumption has also been investigated for benefits independent of skin elasticity and wound healing. Ingestion of undenatured type II collagen can result in an oral immune tolerance response that can serve as a therapeutic treatment for autoimmune inflammatory disease, such as rheumatoid arthritis. 517 Oral immune tolerance can occur through multiple mechanisms, which begin with microfold epithelial cells (in Peyer’s patches of the gut-associated lymphoid tissue) transporting ingested antigens across the mucosal barrier.518,519 Antigen presenting cells in the Peyer’s patches associate with T cells, which in turn circulate to mesenteric lymph nodes and, subsequently, to the peripheral immune system. 520 T cells activated by type II collagen enter the blood stream and secrete anti-inflammatory cytokines TGF-β, IL-4, and IL-10 when in contact with articular cartilage. 518 This mechanism may result in a bystander effect that inhibits T helper (Th)1 response in arthritic lesions. Rigorous RCTs are required. Oral collagen has also shown potential benefits in cartilage degenerative conditions such as osteoarthritis. In a canine model of osteoarthritis, ingestion of undenatured type II collagen markedly reduced arthritic pain through a mechanism of action independent from glucosamine hydrochloride and chondroitin sulfate. 521 In a clinical trial, osteoarthritis patients receiving undenatured type II collagen oral doses over a 12-week period exhibited significant improvement in knee flexibility and mobility as well as reduced knee and back pain. 522 This same principle has held true in clinical studies with healthy individuals that have activity-related joint discomfort. Treatment with undenatured type II collagen oral supplements resulted in improved knee joint range of motion flexibility and extensibility. 523
Oral consumption of enzymatically decomposed collagen peptides and tripeptides have also been correlated with improvement in hair condition (Fig. 3). In ex vivo human culture and in vivo animal models, oral collagen peptides activated the tissue homeostasis regulating canonical Wingless-related integration site (Wnt) (Wnt/glycogen synthase kinase-3β/β-catenin) signaling pathways and stimulated growth factor (insulin-like growth factor binding protein-6, PDGF-AB, placental growth factor, VEGF, keratin27, Gprc5d, Ki67) expression.524,525 This mechanism was associated with proliferation of human dermal papilla and outer root sheath cells, as well as human hair follicle elongation and increased hair growth. While this mechanism has not been shown in patients, it does provide insight into collagen peptide signaling mechanisms and the broader range of impacts oral collagen supplements may have in the body. These findings are promising but not definitive. Rigorous clinical studies are required.
TAKE HOME MESSAGES
Wound Healing and Collagen-Based Products
Collagen is the dominant structural protein (25–30% of total body protein), with types I and III being most abundant in skin (80–85% and 8–11%, respectively).
549
Mechanisms of Action Historical Milestones:
1981: First commercial collagen dressing (CollaDerm, Integra LifeSciences). 1985: Instat (collagen sponge for hemostasis, J&J). 1996: Integra dermal regeneration template (DRT) (collagen-GAG template for burns). 2000: ColActive (bovine collagen dressing by SouthWest Technologies). 2002: Promogran (collagen-cellulose matrix for chronic wounds, J&J, now Solventum). Mechanisms of Action
Provides scaffold for tissue growth, reduces inflammation, maintains moist wound environment. Regulates mechanisms associated with diabetic ulcers, venous stasis ulcers, and pressure ulcers.
Collagen-Based Dressings and Innovations
Types of Collagen Dressings:
Films (adherent, for small wounds) Sponges (absorbent, for high-exudate wounds) Hydrogels (moisture-retentive, nonadherent) Powders (for exudate absorption) Acellular scaffolds (e.g., fish skin grafts—low immunogenicity). Emerging Technologies
3D-printed collagen skin (Pandorum Tech). Recombinant human collagen (CollPlant’s plant-based rhCollagen). Phage-integrated dressings (target MRSA/Pseudomonas).
Regenerative Medicine and Skin Substitutes
Skin Substitutes:
Dermagraft (living fibroblast scaffold) and Integra DRT (collagen-GAG matrix) improve healing in burns/diabetic ulcers. Growth factor–collagen combos (e.g., VEGF + collagen) enhance angiogenesis. Cardiovascular:
Collagen-coated vascular grafts (e.g., Dacron) show >90% patency at 8 years Injectable collagen hydrogels support post-heart attack repair.
Topical and Injectable Collagen
⚠ Topical Collagen Does NOT Replace Skin Collagen
Large molecules cannot penetrate skin but may:
Hydrate (temporarily plumps skin) Signal fibroblasts (via peptides like Gly-Pro-Hyp). Provide antioxidant protection Injectable fillers
Short-term effects (absorbed in 1–3 months) Risks: Granulomas, necrosis, biofilm formation Alternatives: Hyaluronic acid (lasts 12–24 months)
Orthopedics and Dental Applications
Tendon/Bone Repair
Acellular collagen scaffolds (e.g., GraftJacket) aid rotator cuff healing Collagen + BMP promotes bone growth in spinal fusion/tibial defects Dental Uses
CollaPlug: Reduces postextraction bleeding/pain Collagen membranes (e.g., Bio-Gide) preserve alveolar bone for implants.
Collagen as a Food Supplement
Limited Protein Value
Incomplete protein (lacks tryptophan); max 36% of daily protein intake Claimed Benefits: skin hydration (via peptides like Pro-Hyp), but no proven collagen synthesis Joint health: Undenatured Type II collagen may reduce arthritis pain (oral tolerance mechanism).
Marketing Hype: Many claims lack rigorous clinical evidence.
Future Directions
Pipeline Innovations
Biosynthetic collagen (yeast/fermentation-derived) Drug-eluting dressings (e.g., VEGF/PDGF-loaded collagen) Artificial intelligence-monitored collagen scaffolds (Integra LifeSciences).
When considering oral undenatured type II collagen supplements for personal therapeutic use, it is worth noting that not all products are created equal. Physiochemical and analytical characteristics can differ between products, with appreciable differences in color, coarseness, molecular size, and proportion of undenatured collagen to hydrolyzed collagen peptides per dose. 526 These differences can be attributed to the mechanical processes and milling approaches used by the manufacturer. 527 The difference in undenatured collagen per dose could have direct effects on pharmacological therapeutic benefit. Collagen as an oral supplement or therapeutic is not harmful and has several potential health-related benefits for malnutrition and inflammatory joints. However, specific uses for oral collagen supplements can often be overshadowed or sensationalized by media and advertising that boast outcomes that are not supported by rigorous science. 528
FUTURE PERSPECTIVES
By 2030, collagen will no longer be seen as just a cosmetic ingredient—it will be a cornerstone of regenerative medicine and personalized health care. The transformation is already underway.
Wound Healing: From Passive Dressings to Bioactive Therapies: Companies are pioneering the next generation of wound care with collagen-infused calcium alginate dressings that not only protect wounds but actively accelerate healing.529,530 These dressings maintain a moist environment, reduce scarring, and are increasingly used outside hospital settings—empowering patients to manage recovery at home. Products enriched in specific hydrolysis of collagen will serve wound dressing functions with outcomes far superior to anything we know of today. Hydrolyzed collagen hydrogels, nanofibers, and sponges will promote angiogenesis, reduce inflammation, and stimulate tissue regeneration.529,531 These materials are being tailored for chronic wounds, burns, and surgical recovery, with smart dressings on the horizon that can release drugs or signal infection in real time.532,533
Skincare: From Anti-Aging to Skin Regeneration: In the consumer space, collagen is evolving from a buzzword to a bioactive ingredient with clinically validated benefits. Topical formulations are being enhanced with collagen peptides, encapsulated delivery systems, and synergistic compounds like HA and vitamin C to improve skin elasticity, hydration, and repair.474,534–536 The next frontier is personalized collagen skincare, where products are tailored to an individual’s skin microbiome, genetic profile, and environmental exposures.537,538 Artificial intelligence-driven diagnostics and 3D skin printing may soon allow consumers to “print” collagen patches at home for targeted treatment.539–541
Healthcare and Regenerative Medicine: Beyond skin, collagen is being integrated into tissue scaffolds, injectable fillers, and implant coatings to support healing in joints, bones, and internal organs.121,382,542–544 Innovations in recombinant collagen production and production of hydrolyzed collagen active principles—using yeast, bacteria, or even plants—are making it safer, more sustainable, and customizable for medical use.545–547 In the near future, collagen-based biosensors may monitor healing progress or detect early signs of infection.532,548 Combined with wearable tech, this could revolutionize postoperative care and chronic disease management.
Sustainability and Ethical Sourcing: As demand grows, the industry is shifting toward non-animal sources of collagen, including marine collagen and lab-grown alternatives.61,77,545,546 These options reduce the risk of disease transmission, align with ethical consumer values, and open doors for vegan-certified products.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors thank the 13 peer reviewers for their critical comments that were helpful in improving this work. Relevant work in C.K.S. laboratory is supported by grants awarded to C.K.S. as PI by the U.S. Department of Defense [Grants MTEC/2019-447, MTEC/2021-425]; the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) [Grants DK119099, DK125835, DK128845, DK135447, DK143282, DK141513]; and the Biotech 2023-2024 PACommonwealth BT McGowan Grant.
AUTHOR DISCLOSURE AND GHOSTWRITING
Chandan K Sen serves as a paid consultant for Sanara MedTech Inc as well as for SouthWest Technologies.