
Abstract
Objective:
To evaluate the clinical efficacy of negative pressure wound therapy (NPWT) combined with topical oxygen therapy (TOT) for chronic refractory wounds (CRWs), addressing potential hypoxia limitation of NPWT through oxygen supplementation, thereby offering an innovative therapeutic approach for CRWs.
Approach:
The study was performed according to the 2015 Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols statement. A comprehensive search was conducted in PubMed, Cochrane, Embase, Web of Science, CNKI, VIP, and Wanfang databases for randomized controlled trials (RCTs) on the treatment of CRWs with NPWT combined with TOT (inception to October 2024). Studies were screened based on predefined criteria, and data were extracted and assessed using RevMan 5.4. Meta-analysis, sensitivity analysis, and publication bias assessment were performed using Stata 15.0.
Results:
Eleven RCTs (844 patients) were included. Compared with NPWT, the combination therapy was associated with the following outcomes: increased healing rate (risk ratio [RR] = 1.51, 95% confidence interval [CI]: 1.36–1.69, I2 = 18.1%), reduced time from debridement to skin grafting (mean difference [MD] = −2.82 days, 95% CI: −3.15 to −2.50, I2 = 4%), shortened healing time (MD = −9.09 days, 95% CI: −11.98 to −6.20, I2 = 91.2%), enhanced granulation coverage (MD = 7.56%, 95% CI: 6.09–9.03, I2 = 0.0%), and decreased bacterial positivity (RR = 0.27, 95% CI: 0.18–0.41, I2 = 0.0%).
Innovation:
This study provides evidence-based medical research supporting NPWT plus TOT as a synergistic strategy for CRWs.
Conclusion:
Combined therapy may offer benefits over NPWT alone in CRW treatment, suggesting a promising approach to improve healing outcomes.
Keywords
Haowei Zhou

Jing Li

INTRODUCTION
Chronic refractory wounds (CRWs) refer to wounds that fail to heal after more than 4 weeks of systematic treatment. With changes in social structure and lifestyle, the incidence of CRWs has been increasing year by year. Various pathological factors, such as arteriovenous insufficiency, diabetes, and continuous skin compression, contribute to the development of CRWs, keeping them in the inflammatory phase for a long time. This leads to a dull or even nonresponsive skin reaction to healing stimuli, making wound healing difficult.1,2 Patients with CRWs often require long-term hospitalization, regular dressing changes, and multiple debridement surgeries. However, the treatment effect is often poor, and the wounds persist, which can ultimately lead to limb deformity or even amputation. 3 This not only severely damages the physical and mental health of patients but also consumes a large amount of medical resources. Therefore, improving the healing rate of CRWs has become a hot and difficult topic in current medical research. The treatment of CRWs involves wound debridement, regular wound dressing, skin grafting, or flap surgery. In recent years, with the rapid development of tissue regeneration science, significant progress has been made in wound care products and treatment methods. Among them, negative pressure wound therapy (NPWT) has become one of the important methods for treating CRWs. 4
NPWT refers to connecting a drainage tube linked to a dedicated vacuum suction pump to a polyurethane sponge or polyvinyl alcohol dressing on the wound surface. Then, a transparent film is used to seal the wound, and the pump creates a negative pressure environment for wound treatment. The mechanisms by which NPWT promotes wound healing include promoting wound contraction, inducing micro-deformation of the wound surface, draining wound exudate, and maintaining a stable wound environment. Under the combined influence of these mechanisms, NPWT can affect cell proliferation, 5 reduce bacterial load in the wound, 6 promote granulation tissue growth, and shorten healing time. 7 The application of NPWT can reduce the need for frequent dressing changes in clinical practice, alleviating patient discomfort and economic burden. However, researchers have also identified certain limitations of NPWT, as it tends to reduce the oxygen levels in the wound.8–11 During tissue recovery, the imbalance between the limited oxygen environment and high oxygen demand can delay wound repair. Therefore, combining oxygen therapy with NPWT can directly compensate for this oxygen-related shortcoming.
It is well known that oxygen is crucial for wound healing, as it involves many biological processes such as cell proliferation, 12 angiogenesis, 13 and protein synthesis, 14 which are essential for restoring tissue function and integrity. Appropriate oxygenation in wound tissue can initiate the healing response and synergize with other treatment methods for better effects. Clinically, oxygen-promoting wound healing methods mainly include hyperbaric oxygen therapy (HBOT) and topical oxygen therapy (TOT). HBOT requires patients to inhale 100% pure oxygen in a pressurized chamber to achieve supersaturated oxygen levels in the blood and tissues. However, this method requires specialized equipment, limiting its clinical application. 15 TOT is a therapeutic modality that involves the local application of oxygen to injured tissues via a continuous diffusion or pressurized system. Its advantages lie in its independence from the microcirculation of the wound, relatively lower cost, and its simplicity and portability in application. Researchers have found that TOT can continuously increase tissue oxygen levels in CRWs and promote neovascularization by inducing vascular endothelial growth factor (VEGF) production. 16 To address the challenge of insufficient oxygen supply caused by NPWT, some researchers have attempted to combine NPWT with TOT and found that this combined therapy is more effective than NPWT alone.17,18 However, the number of clinical studies on such combined therapy is currently limited, and there is no consensus on the treatment effect. Therefore, this study retrieved and analyzed published clinical studies on the combination of NPWT and TOT for the treatment of CRWs. The aim is to explore the effectiveness of the adjunctive treatment modality for CRWs, provide a reference for clinical treatment, and guide future research and practice.
INNOVATION
The use of NPWT alone has shown benefits in wound healing, but its efficacy can be limited by local hypoxia. The integration of TOT addresses the limitation by enhancing oxygen supply. This meta-analysis demonstrates that combining NPWT with TOT may enhance the wound healing rate. The findings indicate that the combined therapy could be a potentially effective approach for managing CRWs and improving patient outcomes, although further research is needed to fully establish its clinical utility.
Clinical problem addressed
CRWs are often trapped in the inflammatory phase of wound healing, failing to progress to the proliferative phase. This stagnation necessitates adjunctive treatments to facilitate the transition to the next stage of healing. CRWs not only severely impact patients’ quality of life but also impose a significant economic burden on patients, families, and health care systems. This study represents a substantial advancement in the field, highlighting the clinical significance of optimizing wound healing environments through synergistic therapies.
MATERIALS AND METHODS
Our research investigates the differences between NPWT combined with TOT and NPWT alone in terms of wound healing rate, time from debridement to skin grafting, granulation tissue coverage rate, healing time, and positive bacterial culture rate among patients with CRWs. The study was performed according to the 2015 Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols statement 19 and was registered at PROSPERO (CRD42024618561). Electronic laboratory notebook was not used in this study.
Inclusion criteria
(1) Participants: patients with CRWs (including diabetic foot ulcers [DFUs], pressure ulcers, varicose ulcers, and other types of CRWs); (2) Intervention: the control group was treated with NPWT, while the experimental group received NPWT combined with TOT; (3) Primary outcome variable: wound healing rate; (4) Secondary outcome variables: time from debridement to skin grafting, granulation tissue coverage rate, wound healing time, and bacterial culture positivity rate; (5) Study design: randomized controlled trials (RCTs).
Exclusion criteria
Repeatedly published articles, literature lacking complete original data or full text, reviews, case reports, systematic reviews, conference papers, and animal studies were excluded.
Information sources and literature search strategy
RCTs on the use of NPWT combined with TOT for the treatment of CRWs were searched in PubMed, Cochrane, Embase, Web of Science, CNKI (China National Knowledge Infrastructure), VIP, and Wanfang databases from inception to October 2024. The search was conducted using a combination of subject headings and free-text terms, including “negative pressure wound therapy,” “topical negative pressure therapy,” “vacuum-assisted closure,” “negative pressure dressing,” “vacuum-assisted closure therapy,” “vacuum-assisted wound closure,” “vacuum therapy,” “topical oxygen therapy,” “local oxygen therapy,” “continuous diffusion of oxygen,” “chronic refractory wounds,” “diabetic foot,” “diabetic foot ulcer,” “pressure ulcer,” “bedsore,” “pressure injury,” “leg ulcer,” “stasis ulcer,” “ischemic ulcer,” “varicose ulcer,” “venous stasis ulcer,” and “venous ulcer.” We also read the relevant articles and used the reference lists to gain further studies.
Study selection, data extraction, and data items
The retrieved literature was imported into EndNote X9, and duplicate entries were deleted. Two researchers independently reviewed the titles, abstracts, and full texts for screening based on inclusion and exclusion criteria. Data extraction was performed using Excel software by two researchers, focusing on key information such as the first author, publication year, sample size, gender, age, and outcome measures. Any discrepancies were resolved through discussion or consultation with a third researcher.
Outcome variables
Primary outcome variable
The primary outcome variable was the wound healing rate, defined as the proportion of patients achieving 100% epithelialization at the end of the study, expressed as a percentage (%).
Secondary outcome variables
The secondary outcome variables were time from wound debridement to skin grafting, coverage rate of the granulation tissue, wound healing time, and the positive bacterial culture rate. Specifically, the debridement-to-grafting interval referred to the time period from the initiation of debridement to the performance of skin grafting, measured in days. The granulation tissue coverage rate was determined by photographing the wound at treatment completion and measuring the granulation tissue area relative to the total wound area using ImageJ software, with results expressed as a percentage (%). Wound healing time was measured in days and referred to the period from the start of treatment to complete wound healing (100% epithelialization) in patients who achieved full epithelialization. Lastly, the wound bacterial culture positivity rate denoted the proportion of patients with positive bacterial cultures at treatment completion, expressed as a percentage (%).
Quality evaluation
The Cochrane Collaboration’s tool for assessing risk of bias in Review Manager 5.4 was used to evaluate the quality of the included studies. This tool covers seven domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attribution bias), selective reporting (reporting bias), and other biases. Grading of evidence was assessed using GRADEpro. Both assessments were completed independently by both reviewer authors. Any disagreement was resolved by discussion or, if necessary, by a third party.
Summary measures, synthesis of results, and statistical methods
Stata 15.0 software was used for data analysis. Dichotomous variables were expressed as risk ratios (RRs) with 95% confidence intervals (CIs), while continuous variables were expressed as mean differences (MDs) with 95% CIs; p < 0.05 corresponded to the combined effect size, which indicated that there was a significant difference between the experimental group and the control group. The Cochrane Q test and I2 test were used to assess heterogeneity among studies. 20 A fixed-effects model was adopted to synthesize each outcome, while a random-effects model was used in cases where statistically significant heterogeneity was observed among studies. An I2 value exceeding 50% was considered evidence of significant heterogeneity. Subgroup analyses and sensitivity analyses were also conducted. Sensitivity analysis was performed using Stata 15.0. In this analysis, each individual study or specific category of studies was sequentially excluded to compare the newly combined effect size with the original one. The primary goal was to determine whether the exclusion of any particular study or category would significantly alter the results. If no substantial changes were observed, the stability of the findings was thereby confirmed. Funnel plots and the Egger’s test were used to evaluate publication bias.
RESULTS
Literature screening
A total of 362 relevant records were retrieved through searching, and 223 studies were retained after removing duplicates. Following an initial review of titles and abstracts, 150 articles were excluded. After reading the full texts, 11 studies were finally included for analysis (Fig. 1).
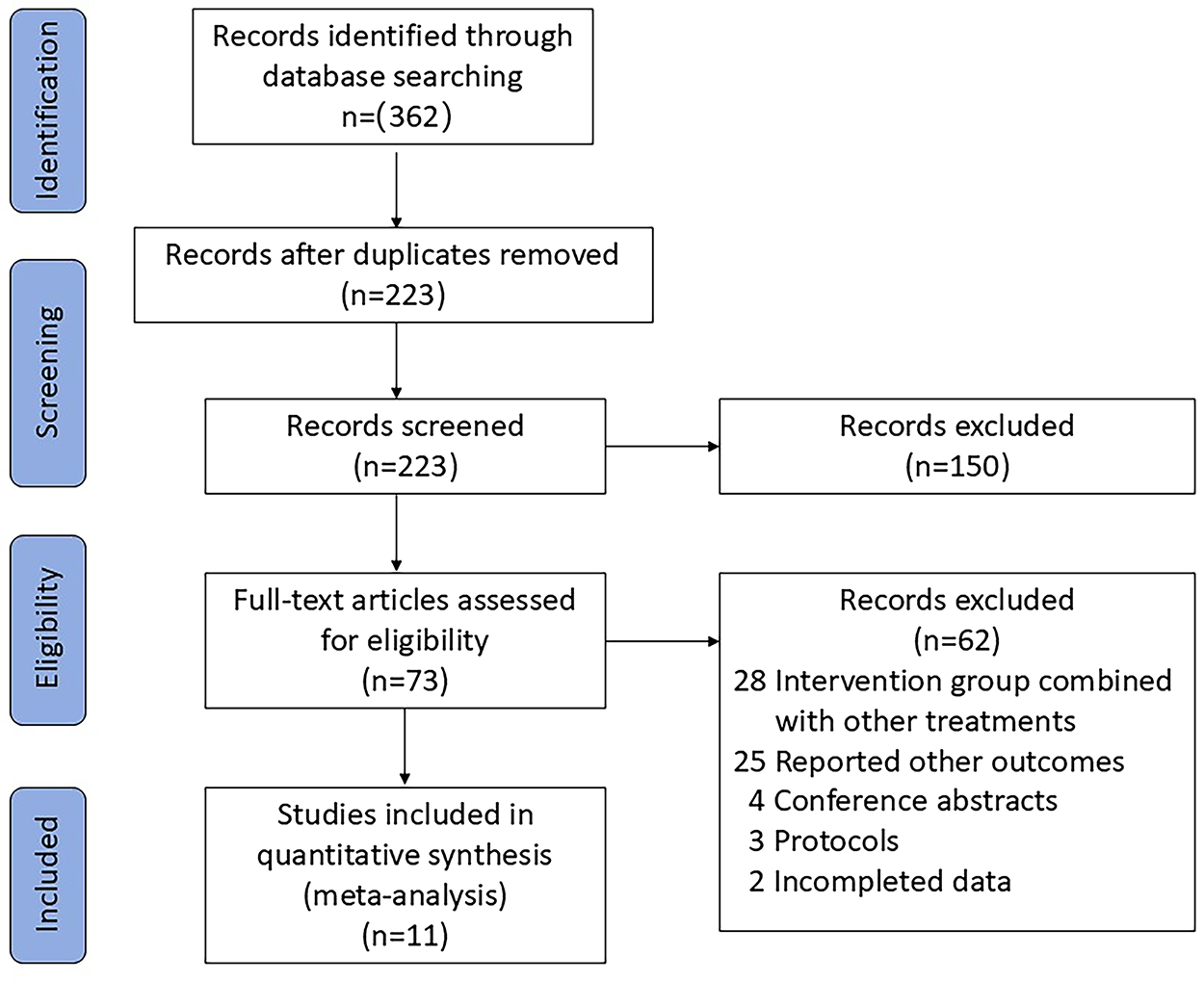
The flow diagram of the literature search process.
Basic characteristics of the studies
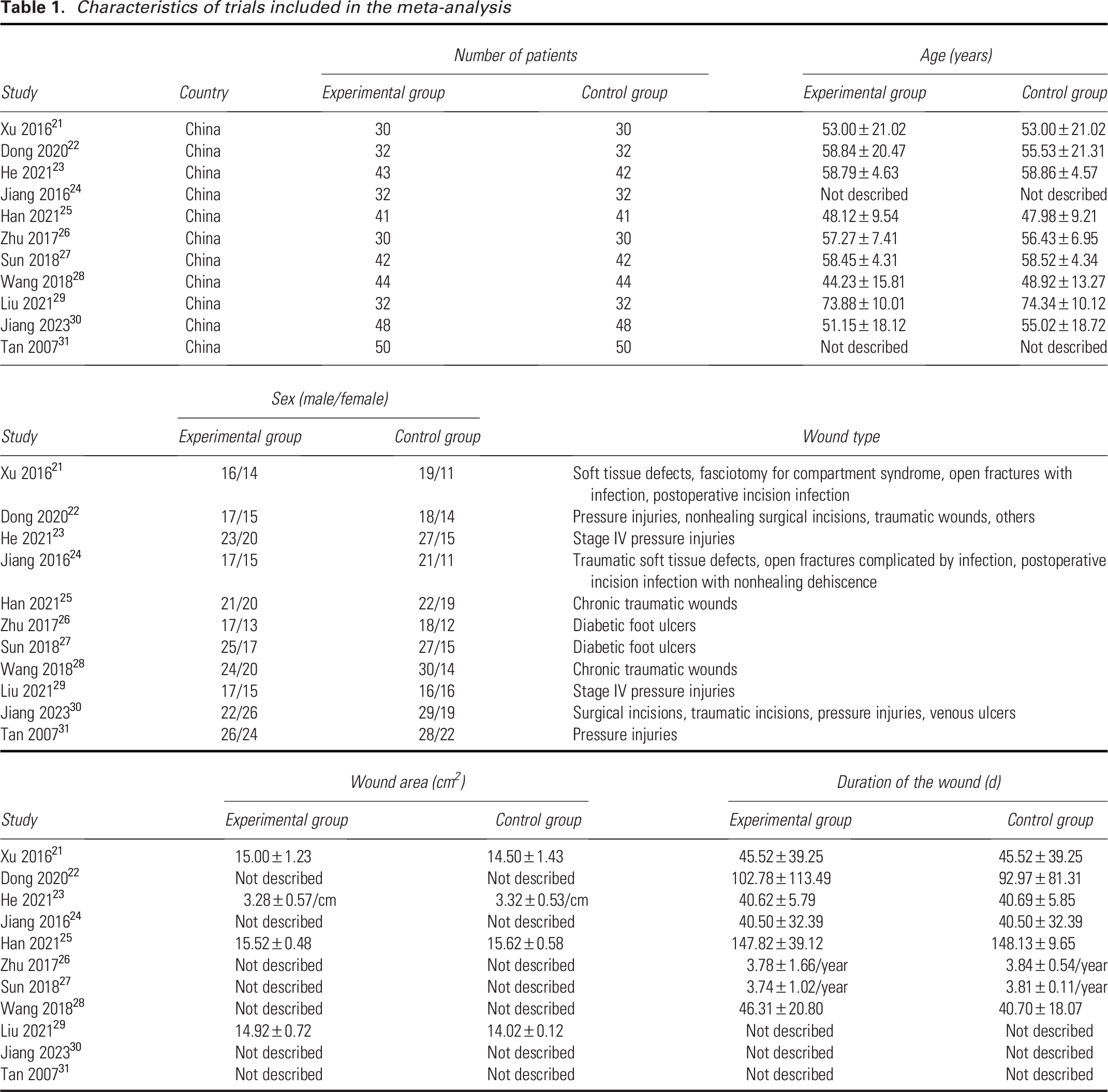
In this study, 11 RCTs involving 844 patients were included. Among them, six trials enrolled patients with CRWs due to various etiologies, three trials specifically focused on pressure ulcers, and two trials concentrated on diabetic ulcers. The basic characteristics of the included literature are shown in Table 1. The data used for analysis have been uploaded to the Figshare platform.
Characteristics of trials included in the meta-analysis
Quality evaluation
Literature quality assessment is shown in Fig. 2. The bias risk assessment of the included studies indicated the following: in terms of allocation concealment, eight studies were rated as moderate risk. Regarding the blinding of participants and researchers, all 11 studies exhibited a moderate bias risk. For blinding of outcome assessment, 10 studies showed a moderate bias risk. However, all studies achieved a low bias risk in random sequence generation, data integrity, and selective reporting. It is worth noting that none of these studies were rated as high bias risk.
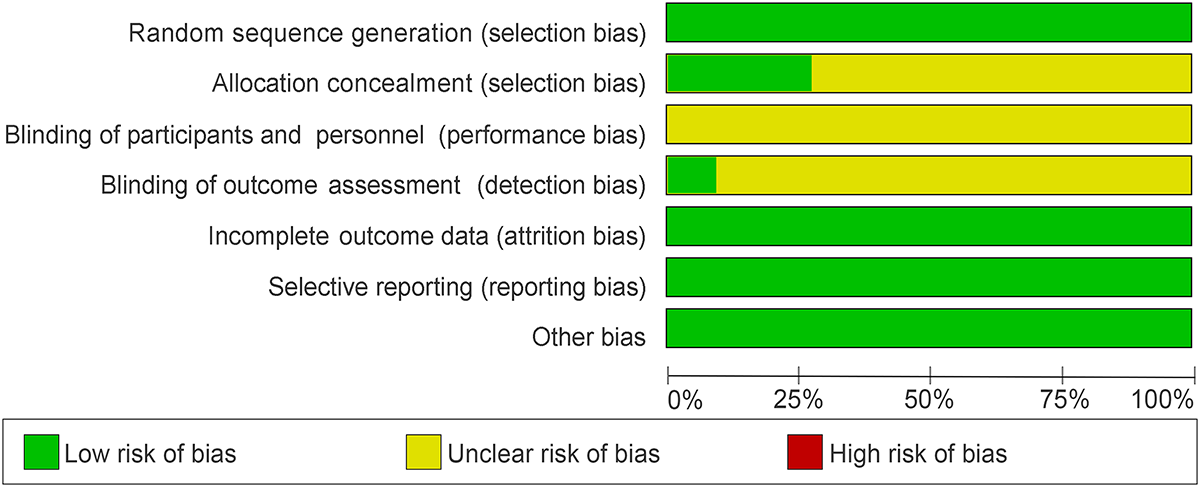
Risk of bias graph.
The GRADE evidence levels for all outcome measures are as follows: wound healing rate and bacterial culture positivity rate were graded moderate, wound healing time very low, and all remaining outcomes low. These evidence profiles are detailed in the Supplementary Data.
Primary outcome
Wound healing rate
Eleven studies21–31 reported the outcome variable of wound healing rate, including 844 patients divided into the NPWT combined with TOT group (n = 423) and the NPWT group (n = 421). Upon analysis, low heterogeneity was found among the studies (I2 = 18.1%, p > 0.1), so a fixed-effects model was used for analysis. The meta-analysis result showed that the wound healing rate was higher in the NPWT combined with TOT group than in the NPWT group (RR = 1.51, 95% CI: 1.36–1.69, p < 0.05) (Fig. 3). This suggests that the cure rate in the combined treatment group was 1.51 times higher than that in the NPWT group. Furthermore, we conducted subgroup analyses based on different etiologies, and the results are presented in the Supplementary Data (Supplementary Fig. S1). Within the subgroup analyses, the findings for pressure injuries (PIs; RR = 1.89, 95% CI: 1.44–2.48, I2 = 2.4%) and various types of CRWs (RR = 1.38, 95% CI: 1.23–1.54, I2 = 0.0%) remained statistically significant. However, the results for the DFUs (RR = 1.75, 95% CI: 0.96–3.20, I2 = 0.0%) did not reach statistical significance, possibly due to the limited number of studies and cases included in this subgroup.
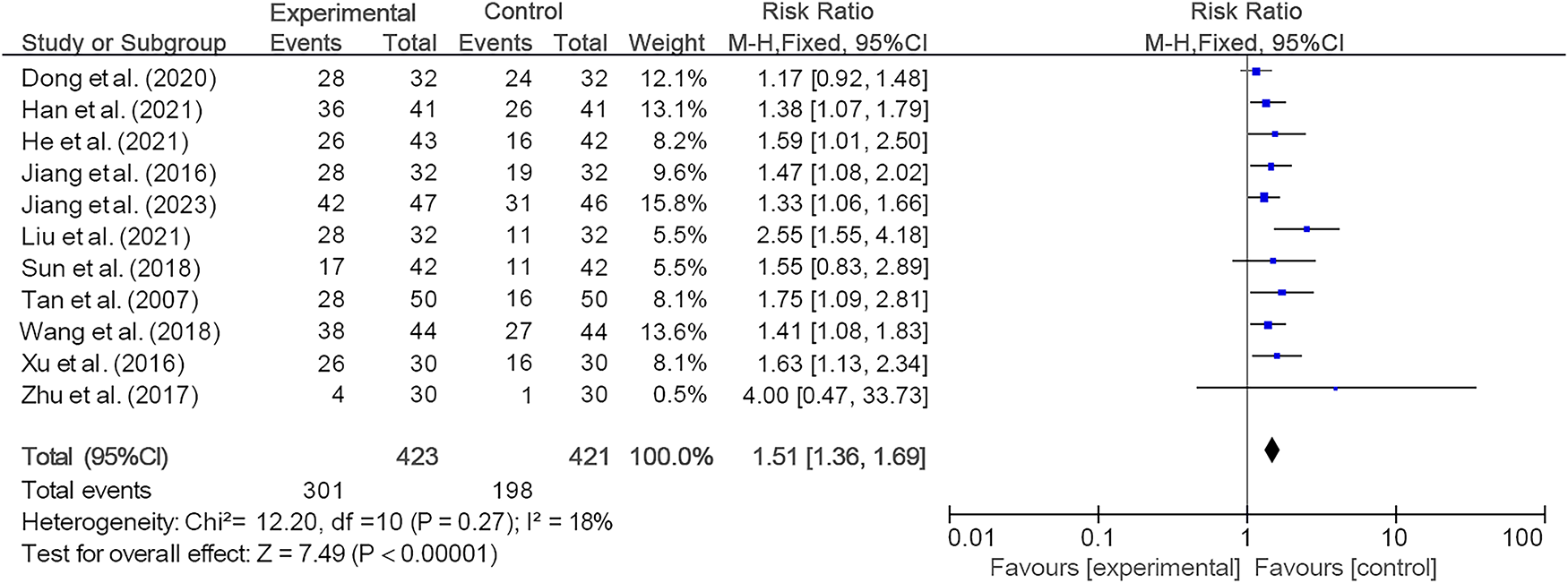
Forest plot of the meta-analysis of wound healing rate. CI, confidence interval.
Publication bias
A funnel plot and Egger’s test were used to detect publication bias (Fig. 4). Egger’s test detected publication bias in the currently included trials (p = 0.010). However, after performing Egger’s test among different subgroups, no significant publication bias was found in the other two groups (p = 0.162 and p = 0.062), except for the diabetic ulcer group, which could not be tested due to having only two studies.
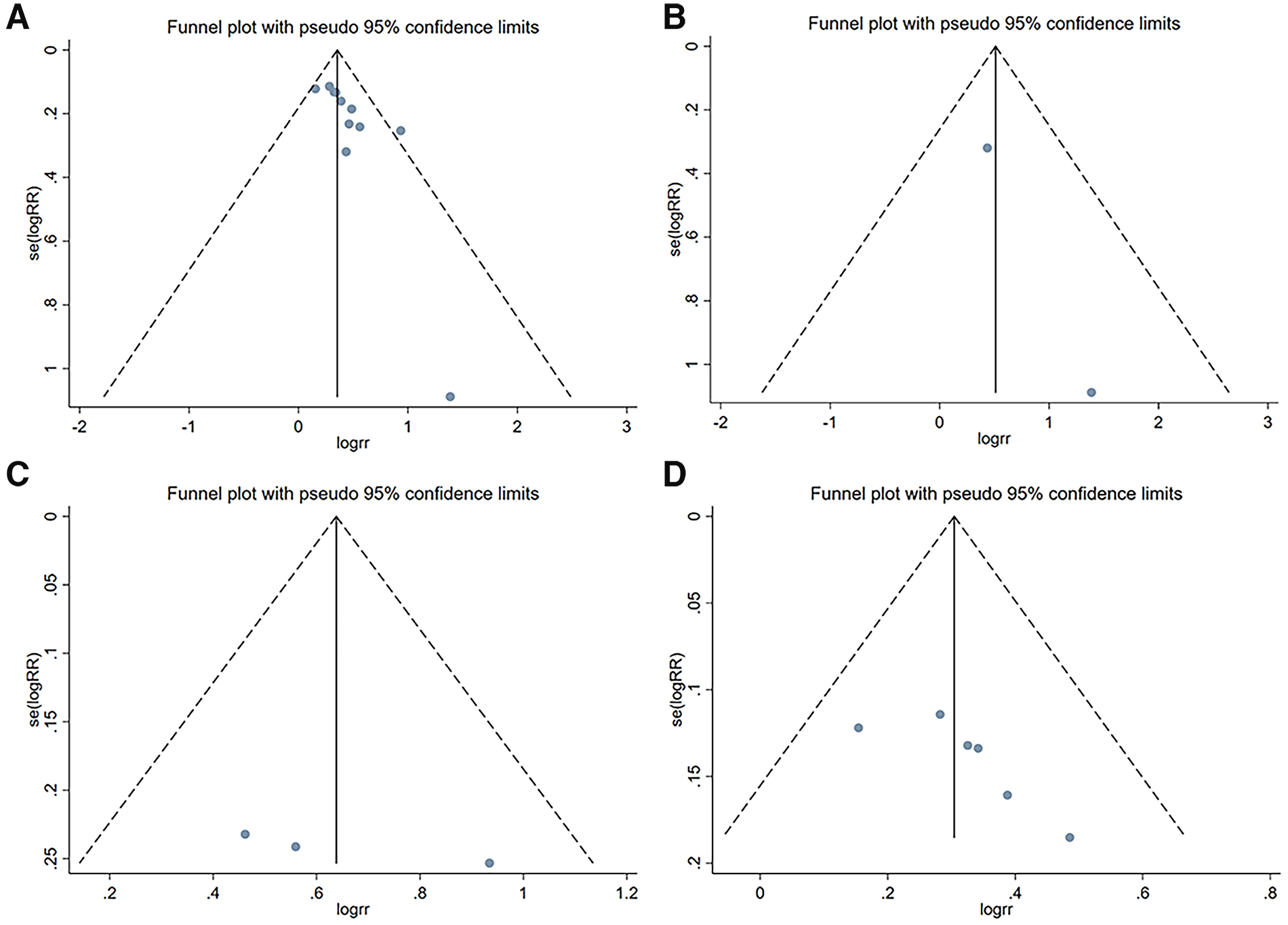
Funnel plots of the publication bias of the pooled included trials
Sensitivity analysis
We conducted a sensitivity analysis on the wound healing rate to evaluate the robustness of our findings. Initially, we recalculated the overall pooled effect size after excluding each study individually (Fig. 5). The results indicated that the overall effect size remained statistically significant, suggesting that individual studies had minimal influence on the pooled effect size and verifying the reliability of our findings. Subsequently, we excluded wound data from different etiologies sequentially and recalculated the pooled effect size (Supplementary Figs. S2–S4). The results are as follows: After excluding studies related to DFUs, RR = 1.50, 95% CI: 1.34–1.67, I2 = 26.9%; upon excluding studies related to PIs, RR = 1.41, 95% CI: 1.26–1.58, I2 = 0.0%; and when excluding studies related to various types of CRWs, RR = 1.86, 95% CI: 1.45–2.39, I2 = 0.0%. These findings consistently demonstrate that even after excluding wound data from different etiologies, our study conclusions remain statistically significant, further corroborating the robustness of our results.
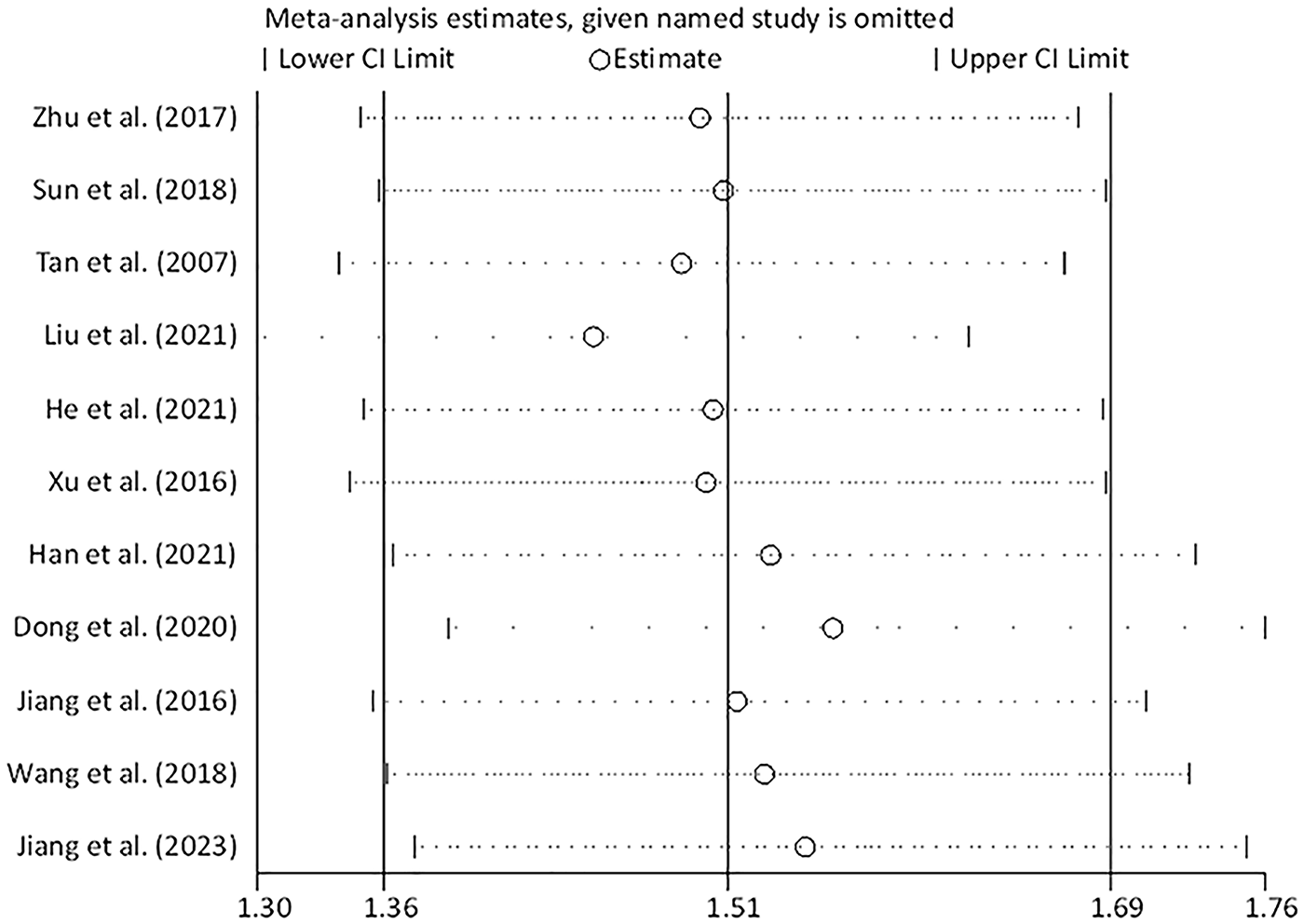
Sensitivity analysis of the wound healing rate in patients allocated to the experimental group and the control group.
Secondary outcomes
Time from debridement to skin grafting
After strict inclusion and exclusion criteria, three studies21,26,27 reported the time from wound debridement to skin grafting, with 204 patients allocated to either the NPWT in conjunction with TOT group (n = 102) or the NPWT group (n = 102). After heterogeneity analysis, minimal heterogeneity was found among the studies (I2 = 4%, p > 0.1), so a fixed-effects model was used for analysis. The result showed that compared with the NPWT group, the time from debridement to skin grafting was significantly shortened in the NPWT combined with TOT group (MD = −2.82 days, 95% CI: −3.15 to −2.50, p < 0.05) (Fig. 6A). Specifically, the combined treatment group achieved skin grafting 2.82 days earlier than the NPWT group.
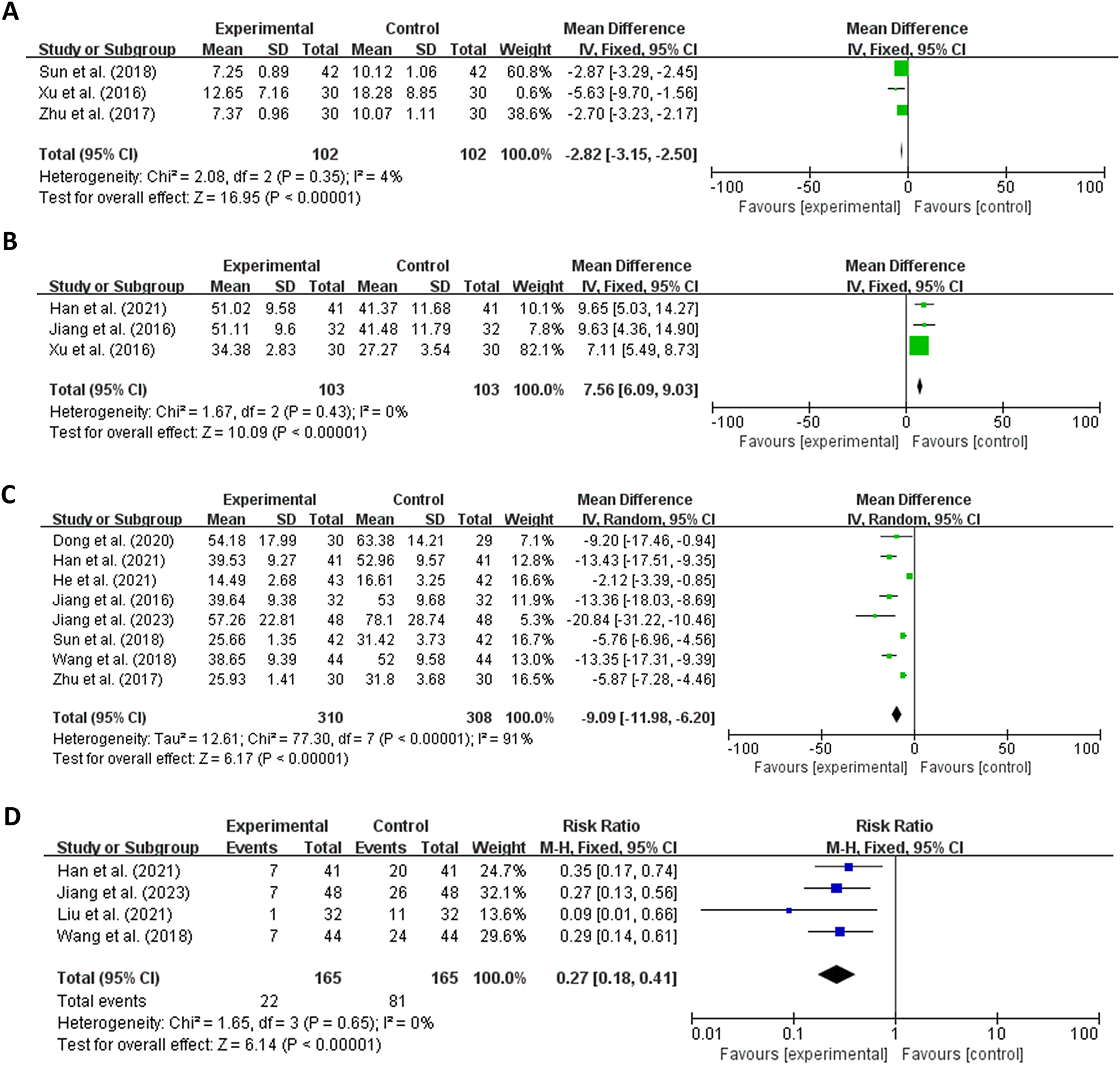
Forest plot of each secondary outcome variable (
Granulation tissue coverage rate
In the analysis of granulation tissue coverage rate, three studies21,24,25 were included, encompassing 206 patients segregated into the NPWT combined with TOT group (n = 103) and the NPWT group (n = 103). In the aftermath of heterogeneity scrutiny, no significant heterogeneity was detected among the studies (I2 = 0.0%, p > 0.1), leading to the adoption of a fixed-effects model for analytical purposes. The meta-analysis revealed that the granulation tissue coverage rate was significantly higher in the NPWT and TOT amalgamated group when juxtaposed with the NPWT group, with a MD of 7.56 percentage points (MD = 7.56%, 95% CI: 6.09–9.03, p < 0.05) (Fig. 6B).
Wound healing time
After article screening, eight studies22–28,30 reported wound healing time, involving 618 patients divided into the NPWT concomitant with TOT group (n = 310) and the NPWT group (n = 308). Heterogeneity was found among the studies after analysis (I2 > 50%, p < 0.1), so a random-effects model was used for analysis. The meta-analysis result demonstrated a reduction in wound healing time for the NPWT combined with TOT group compared with the NPWT group, with an effect size of 9.09 days (MD = −9.09 days, 95% CI: −11.98 to −6.20, p < 0.05) (Fig. 6C).
Positive bacterial culture rate
In the assessment of positive bacterial culture rate, a total of four studies25,28–30 comprising 330 patients were incorporated. These patients were divided into the NPWT combined with TOT group (n = 165) and the NPWT group (n = 165). After heterogeneity analysis, no significant heterogeneity was discerned among the studies (I2 = 0.0%, p = 0.649), so a fixed-effects model was used for analysis. The meta-analysis finding revealed that the positive rate of bacterial culture was lower in the NPWT combined with TOT group than in the NPWT group, with a RR of 0.27 (95% CI: 0.18–0.41, p < 0.05) (Fig. 6D), indicating that the rate was only 0.27 times that of the NPWT-alone group.
DISCUSSION
Numerous meta-analyses have independently evaluated the efficacy of NPWT and TOT in wound treatment, concluding that both therapies demonstrate definite therapeutic effects.32–35 However, no meta-analysis has systematically summarized the effectiveness of combining NPWT and TOT in treating CRWs. This study aims to fill this gap. Our meta-analysis results indicate that, compared with NPWT alone, the combination of NPWT and TOT enhances wound granulation tissue coverage, reduces bacterial culture positivity rates, and effectively shortens both the time from debridement to skin grafting and overall wound healing duration, ultimately improving the final healing rate.
This study possesses certain strengths. First, during the literature search phase, two researchers were assigned to conduct the search, ensuring comprehensiveness and accuracy. In addition, we not only carefully read relevant articles but also expanded the search scope by reviewing reference lists, striving to collect all pertinent literature as comprehensively as possible and minimizing the likelihood of missing any. Second, in terms of outcome measures, we utilized wound healing rate as the primary endpoint, while considering granulation tissue coverage, bacterial culture positivity, time from debridement to skin grafting, and overall wound healing duration as secondary endpoints. This comprehensive and detailed evaluation of treatment effects aimed to reflect the effectiveness of the therapeutic regimen from multiple perspectives. Third, during sensitivity analysis, we not only excluded single studies to observe their impact on the overall results but also recalculated the pooled effect size after excluding each category of related studies based on different wound etiologies. The final results remained statistically significant even after these rigorous sensitivity analysis steps, indicating the robustness and reliability of our findings.
However, several inherent limitations existed in our study. First, despite our best efforts to be comprehensive during the search process, the existence of gray literature may have resulted in the exclusion of some unpublished studies. Second, some studies demonstrated moderate bias in terms of allocation concealment and blinding implementation. This reminds us that when applying the conclusions to clinical practice, we should make comprehensive judgments in combination with the individual circumstances of patients and more high-quality primary research evidence. Additionally, all included studies were published in Chinese, potentially introducing language bias. While Singh et al. 18 documented 100% healing in stage IV PIs with NPWT plus TOT compared with 86.7% with NPWT alone, this study had a nonrandomized design and lacked statistical comparisons. These constraints prevent it from fully counteracting the language bias or confirming the cross-regional applicability of our findings. Combined with the relatively small sample size, these factors limit the generalizability of our results. Therefore, the findings of this study can only provide researchers with a reference regarding relevant treatment options from Chinese researchers, rather than fully reflecting the international research landscape. Finally, the standardization of NPWT and TOT usage can be challenging. Parameter selection often relies heavily on clinicians’ experience, resulting in discrepancies across studies and contributing to the clinical heterogeneity observed in this research.
The therapeutic advantages of combination therapy over the use of NPWT alone primarily stem from the integrated application of TOT alongside NPWT. This combined approach significantly ameliorates the local hypoxic state that may arise from NPWT, optimizing the microenvironment for wound healing and thereby accelerating the healing process. Oxygen plays a pivotal role in wound healing, and while local hypoxia can trigger hypoxia-inducible factor-1α to promote angiogenesis, sustained angiogenesis and normal tissue function require adequate oxygen levels.36,37 The level of oxygen not only influences the rate of new blood vessel growth but also impacts its quality. VEGF, a primary stimulant of angiogenesis in wounds, can be induced by oxygen in endothelial cells and macrophages, promoting blood vessel formation. 38 Furthermore, the continuous presence of oxygen fosters the proliferation of endothelial cells and fibroblasts, influencing collagen synthesis and deposition, thereby facilitating granulation tissue growth. In addition, TOT restores mitochondrial oxidative phosphorylation, activates the respiratory burst of neutrophils, and enhances their bactericidal effect, providing a cleaner and healthier environment for wound healing. 39
These findings offer valuable insights for clinical applications and suggest the potential of combination therapy in treating CRWs. However, future research necessitates additional experiments to uncover the underlying mechanisms and requires data from broader populations and larger sample sizes to further validate the conclusions.
CONCLUSION
The results of this meta-analysis suggest that the combined therapy may be correlated with a shortened time from debridement to skin grafting, increased granulation tissue coverage, and reduced positive bacterial culture rates. All of these factors contribute to shortened wound healing time and improved healing rates. However, the generalizability of these conclusions still requires further validation in a broader population.
Footnotes
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare that there are no conflicts of interest. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
AUTHORS’ CONTRIBUTIONS
J.S. and D.Z. collected all data and analyzed data. J.D., R.X., and Z.L. contributed to data verification and statistical analysis. J.S. contributed to article writing. H.Z. and Y.L. revised the article. J.L. contributed to design of this study. All listed authors checked and agreed to the final article.
ABOUT THE AUTHORS
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.