
Abstract
Objective:
Burn injuries affect over 11 million people annually, and methicillin-resistant Staphylococcus aureus (MRSA) infection significantly delays healing by sustaining inflammation and promoting scarring. This study evaluated N-benzyl benzenamine 4k—a novel dual-action compound with antibacterial and anti-inflammatory properties—in a murine model of MRSA-infected burn wounds.
Approach:
Skin safety of 4k was assessed through acute toxicity, sensitization, and irritation tests in BALB/c mice. A full-thickness burn model infected with MRSA2858 (1 × 108 CFU/mL) was treated topically with 4k, vancomycin (VAN), or vaseline. Outcomes included wound closure, bacterial load, histology, collagen organization, macrophage polarization markers (CD86/inducible nitric oxide synthase [iNOS] for M1; CD206/vascular endothelial growth factor [VEGF] for M2), cytokine levels, and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway proteins.
Results:
4k demonstrated excellent dermal tolerability with no toxicity or irritation. Topical 4k reduced MRSA colonization and accelerated wound closure (residual wound area at day 15: 4k = 8.4 ± 2.2%, VAN = 17.8 ± 3.5%). Histology revealed organized collagen deposition and minimal scarring in the 4k group (scar score: 2.33 ± 0.58 vs. 13.33 ± 0.58 for vaseline). Mechanistically, 4k suppressed NF-κB activation, downregulated M1 markers (CD86, iNOS, tumor necrosis factor-alpha, and interleukin [IL]-6), and upregulated M2 markers (CD206, VEGF, transforming growth factor-beta 1, and IL-10), promoting a prohealing immune environment.
Innovation:
This study introduces a dual-action topical therapy that combines potent antibacterial activity with immunomodulation, offering a promising strategy to overcome antibiotic resistance and improve burn wound outcomes.
Conclusions:
N-benzyl benzenamine 4k effectively eradicates MRSA, accelerates wound healing, and minimizes scarring through NF-κB inhibition and macrophage polarization, supporting its potential as a next-generation burn care agent.
INTRODUCTION
Annually, burn injuries affect approximately 11 million people worldwide, representing a significant global health burden. 1 The clinical management of these wounds becomes profoundly more challenging when complicated by methicillin-resistant Staphylococcus aureus (MRSA) infection. Antibiotic resistance and persistent inflammation in such cases severely hinder recovery,2,3 and patients with MRSA-infected burns are at a high risk of developing hypertrophic scars, which impose long-term physical and socioeconomic burdens. 4
Wenjian Tang, PhD

Dandan Liu, MSc

Jing Zhang, MSc

A pivotal driver of this pathological progression is dysregulated immune response, particularly an imbalance in macrophage polarization. Macrophages, as critical regulators of wound healing, can differentiate into a proinflammatory (M1) phenotype or an anti-inflammatory (M2) phenotype. 5 In MRSA-infected burns, the persistent infection sustains M1 activation via the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway, leading to excessive release of cytokines such as interleukin (IL)-6 and tumor necrosis factor-alpha (TNF-α) that cause tissue damage and delay healing.6–8 Conversely, although M2 macrophages typically promote repair and angiogenesis, their dysregulation in this context results in aberrant vascular endothelial growth factor (VEGF) accumulation and fibrotic remodeling, culminating in scar formation. 9 This creates a critical knowledge gap: while targeting NF-κB to rebalance macrophage polarization is a promising strategy, current therapeutic options fail to simultaneously eradicate the MRSA infection and correct the underlying immune dysregulation.10,11
To bridge this gap, this study turns its focus to FabI, a key enzyme in the bacterial FAS-II pathway that is essential for MRSA membrane integrity and is an attractive target for selective antibacterial action. 12 In recent work, N-benzyl benzenamine 4k was identified as a novel inhibitor that competitively binds the NADH site, disrupting fatty acid synthesis and demonstrating potent anti-MRSA and anti-biofilm activity (Minimum inhibitory concentration [MIC] = 1.25 mg/L; Minimum biofilm eradication concentration [MBEC] = 1.5 mg/L against MRSA). 13 Notably, 4k also exhibited significant anti-inflammatory properties (IC50 = 5.86 μM for nitric oxide [NO] inhibition). 14 Therefore, 4k would be used to validate its dual-action therapeutic potential and investigate its capacity to serve as a targeted therapy that concurrently addresses the unmet clinical need by eliminating MRSA infection and modulating the dysregulated macrophage response to improve healing outcomes in burn wounds.
INNOVATION
The dual-action topical agent 4k introduces an innovative strategy for treating MRSA-infected burn wounds by simultaneously targeting the pathogen and reprogramming the wound immune microenvironment (Fig. 1). 4k not only exerted direct antibacterial effects through specific FabI inhibition, effectively eradicating MRSA and its biofilms, but also reprogrammed the dysregulated immune microenvironment by shifting macrophage polarization from the proinflammatory M1 state toward the prohealing M2 phenotype. This approach moves beyond conventional antibiotic paradigms by concurrently disrupting bacterial fatty acid synthesis and inflammatory pathways, offering a promising, well-tolerated topical candidate for next-generation burn care.
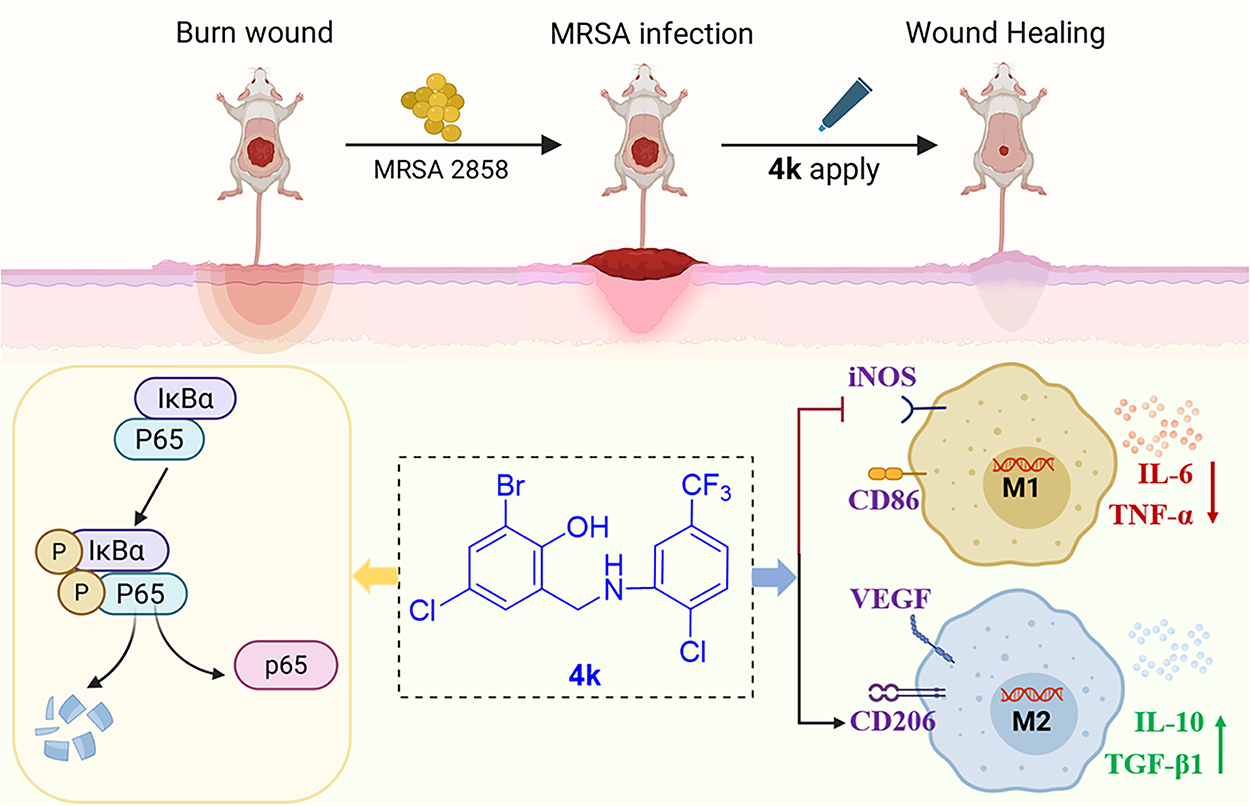
Innovation figure summary graphic. Schematic diagram elucidates the mechanism of 4k accelerated the healing of MRSA-infected burned wounds by inhibiting macrophage polarization and NF-κB pathway. MRSA, methicillin-resistant Staphylococcus aureus; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells.
CLINICAL PROBLEM ADDRESSED
Burn care faces a dual challenge: MRSA infection and dysregulated inflammation.15–17 Existing antimicrobials often fail to address both, leading to persistent tissue damage and scarring. 18 This creates an urgent need for safe, topical therapies that can simultaneously eradicate pathogens and promote a prohealing immune response in the compromised wound bed. The dual-action topical agent 4k addresses this by simultaneously clearing pathogens and reprogramming local immunity. Its localized action and favorable safety profile make it a promising candidate to accelerate healing and reduce scarring without systemic toxicity.
MATERIALS AND METHODS
Electronic laboratory notebook was not used.
Bacterial strains
The compound 4k was found to be a potent antibacterial agent against MRSA and high purity (Supplementary Fig. S3). The MRSA2858 strain used in this study was isolated from a patient blood at Anhui No.2 Provincial People’s Hospital and showed multiresistant to methicillin, oxacillin, clindamycin, erythromycin, gentamicin, and levofloxacin.14,19 To prepare bacterial suspension, MRSA was cultured in Mueller–Hinton broth (MHB) at 37°C, consistent with the standardized medium used in the cited studies supporting 4k’s antibacterial activity against MRSA.
Cell culture and treatment
Mouse monocyte–macrophage leukemia cells (RAW264.7 cells, Taxus chinensis Biology #STCC20020P) were cultured in DMEM medium (Servicebio #G4525) supplemented with 10% fetal bovine serum (Servicebio #G8003) and 1% penicillin/streptomycin (Servicebio #G4016) at 37°C in a 5% CO2 incubator.
The RAW264.7 cells were seeded into 24-well plates at a density of 2 × 104 cells per well and incubated in the cell culture incubator for 24 h. After this period, the original medium was aspirated, and fresh DMEM medium (containing 10% serum) supplemented with MRSA suspension (at multiplicities of infection [MOIs] of 10, 20, 40, 80, and 100) and various concentrations of 4k was added to each well. The cells were then incubated for another 12 h.
Cell activity assay
RAW264.7 cells were seeded in 96-well plates at a density of 1 × 104 cells per well. Following 24 h of culture, the cells were treated with 1 μM dexamethasone (MCE #HY-14648) and 4k at various concentrations (5, 10, 20, 30, and 40 μM). After 24 h of treatment, CCK-8 reagent (Servicebio #G4103) was added to each well of the 96-well plate, and the plate was incubated at 37°C for 1 h. The absorbance at 450 nm was measured using a microplate reader. Based on these results, 4k concentrations of 5 and 10 μM were selected for subsequent experiments.
Evaluation of anti-inflammatory activity
NO production from activated RAW264.7 cells was determined by measuring the amount of nitrite, a relatively stable oxidation product of NO. RAW 264.7 cells were cultured in 48-well plates at a density of 7 × 104 cells/mL overnight. After adding different concentrations of 4k (1, 2.5, 5, 20, 50, 75, and 100 μM) for 1 h, lipopolysaccharide (Servicebio #GC205009) was prepared by dissolving in sterile PBS, followed by 10 min of sonication (40 kHz, 300 W) at room temperature to ensure uniform dispersion. Cells were stimulated with LPS (10 ng/mL) for 24 h. The determination of the nitrite concentration is based on the Griess reaction by colorimetry (Griess reagent, Beyotime, China). Briefly, the Griess reagents Ι and II were added to 50 μL supernatant of the cultured media, and the solutions were mixed and determined at 540 nm in an automated microplate reader.
Experimental animals
This study followed the ARRIVE 2.0. A total of 118 BALB/c mice (6–8 weeks old, 18–20 g, half male and half female) were used across all experiments. These mice were supplied by Jiangsu Huachuang Xinnuo Pharmaceutical Technology Co., Ltd. (Nanjing, China), with the animal license number SCXK [Su] 2024-0004. The experimental unit for all in vivo experiments was the single animal. All mice included (free of preexisting skin lesions or systemic infections) were provided free access to a commercial solid diet and water under specific pathogen-free controlled conditions (25 ± 2°C, 12 h light/dark cycle, 55 ± 5% humidity) for at least 1 week prior to the start of the experiment. No animals were excluded during the experiment. Mice were randomly allocated to experimental groups by a dedicated researcher (Researcher A) using a computer-generated random number table (via GraphPad Prism 9.0 software), with sex stratified to ensure equal distribution of males and females across groups. Researcher A, who held the allocation code and prepared treatments, had no role in outcome assessment. All subsequent procedures (CFU counts, wound measurements, histological/scar scoring, enzyme-linked immunosorbent assay [ELISA], WB, and quantitative polymerase chain reaction [qPCR] analyses) were performed by independent researchers (B and C) who were blinded to group assignments. The code was broken only after all data collection and preliminary statistical analysis were complete. All samples were labeled with anonymous codes during processing, and the allocation code was only unmasked to both researchers after all data were collected and preliminary statistical analysis was finalized, eliminating observer bias for every key endpoint. All animal procedures were performed in accordance with the National Institutes of Health (NIH) Guide for the Care and Use of Laboratory Animals (8th edition, 2011), available at: https://www.ncbi.nlm.nih.gov/books/NBK54050/. The protocol was approved by the Institutional Animal Care and Use Committee of Anhui Medical University (Approval No. K2021016).
Acute skin toxicity test
Mice were randomly divided into two groups: control group (treated with an equal volume of water, n = 10) and 4k treatment group (an equal volume of 2% 4k solution, n = 10). Before the experiment, the dorsal fur of the mice (Veet #Wt001) was removed using a depilatory agent, exposing an area of approximately 20 cm2. The assigned solutions were applied evenly to the depilated area. After 24 h, the treatments were washed off with warm water. Local skin reactions and systemic toxicity were assessed daily over a 14-day period. Dorsal skin reactions were evaluated using the Draize irritation scale. Systemic toxicity was monitored by recording abnormal clinical signs—including lethargy, hypoactivity, abnormal grooming, diarrhea, and piloerection—as well as by measuring body weight (before treatment, on day 7, and on day 14) and quantifying daily food and water intake. A body weight loss exceeding 10% or a sustained reduction (≥3 days) in consumption was considered indicative of systemic toxicity. 20 In case of mortality during the experiment, autopsies were conducted immediately, and histopathological examinations were performed. On day 14, skin samples from the treatment area and kidney samples collected systemically were harvested from each group. These samples were stained with hematoxylin–eosin (H&E) and examined for histopathological changes. 21 All researchers involved in histological assessment remained unaware of treatment allocation during both data collection and evaluation.
Skin sensitization test
Mice were randomly divided into three groups (n = 6). Group I served as the normal untreated control and received vaseline (Sigma-Aldrich #16415). Group II was marked as positive control and was treated with an aqueous solution of formalin (0.8% v/v), and group III was treated with the 2% 4k local treatment. The 4k was each mixed with white vaseline to create 2% ointments. Before the experiment, the backs of the mice were depilated. Subsequently, treatments were applied on the back of mice after 24 h. Sensitization was conducted again on the 7th and 14th days using the same procedure. On the 14th day, the skin allergic reaction was observed immediately after drug removal (0, 24, and 72 h) for erythema and edema scores. Erythema and edema were scored separately using a standardized scale: erythema: 0 = none, 1 = mild, 2 = moderate, 3 = severe, and 4 = erythema with edema; edema: 0 = none, 1 = mild, 2 = moderate, and 3 = severe. Average sensitization score was calculated as: (total erythema scores + total edema scores)/number of animals. Sensitization rate was defined as: (number of animals with a score ≥1)/total animal × 100%. The cumulative score of each group was reported as mean ± standard deviation (SD). 22
Skin irritation test
Mice were randomly assigned to four groups (n = 6). Before the experiment, the backs of the mice were depilated. A “#”-shaped incision was made, penetrating the epidermis and superficial dermis, causing mild bleeding while avoiding deeper tissue damage. Intact skin: Only hair removal was performed, without any scratching or incisions. Group I was the intact skin control group, Group II was the damaged skin control group, Group III was the intact skin + 4k group, and Group IV was the damaged skin + 4k group. Each group of depilated areas was evenly coated with 0.2 mL of the corresponding medication or vaseline, covered with sterile gauze, and secured with nonirritating rubber adhesive to maintain semiocclusive contact. Coverings were removed after 4 h per Organization for Economic Co-operation and Development [OECD] Test Guideline 404, and residual treatment was gently cleansed with warm water. This experiment lasted for 7 days, with treatments applied twice daily. Skin irritation at the application site was observed 1 h after each treatment, before reapplication, and 1, 24, 48, and 72 h after the drug was removed from the last treatment, and the corresponding scores were recorded. The cumulative scoring report for each group was the average ± SD. In multiple skin irritation experiments, the average score per animal per day was calculated as (total score for erythema formation + total score for edema formation) / (number of animals × 6). Based on this, the average score value was used to rate the intensity of irritation.
MRSA-infected skin burn model
Immediately prior to burn induction, mice were anesthetized with 2,3% isoflurane (in oxygen) via inhalation, and the dorsal skin was disinfected with 70% ethanol. Anesthesia depth was monitored by assessing paw withdrawal reflex and respiratory rate throughout the procedure to ensure animal welfare and stable anesthesia. Buprenorphine (0.1 mg/kg, SC) was given 30 min preburn, then every 12 h for 3 days, tapered to once daily on days 4–5. Monitoring of anesthesia depth and adherence to predefined humane endpoints (e.g., >20% weight loss and severe lethargy) are now explicitly described, ensuring full compliance with Animal Research: Reporting of In Vivo Experiments [ARRIVE] guidelines (Supplementary Table S6). The area had been prepared 24 h earlier by shaving with electric clippers, followed by application of depilatory cream to remove all hair. A copper rod (10 mm in diameter) was preheated in boiling water for 10 min and applied to the dorsal skin of each mouse for 10 s, without applying pressure. The burn wound exhibited a white, wrinkled appearance, and significant edema was observed within 3 h, confirming the successful creation of a full-thickness burn model.
After injury (within 10 min), a small gauze was placed over the wound, and the area was inoculated with 50 μL of MRSA suspension (1 × 108 CFU/mL), prepared by diluting logarithmic-phase cultures in sterile MHB. Infection is defined as the presence of high concentrations (>105 organisms/g of tissue) of bacteria in the burn wound and scab. 23 4k and vancomycin (VAN) was prepared using white petrolatum to ensure consistent formulation and fair efficacy comparison, with the same topical application protocol (25 mg per application [0.1 mL/cm2] on 1.5 cm2 of area, twice daily for 15 days).14,24 To evaluate the efficacy of 4k treatment, mice were randomly assigned to four groups (n = 14 per group): control group (neither burns nor any topical application), vaseline group (burned but treated only with vaseline), 2% 4k ointment (burned and treated with 2% 4k ointment), and 2% VAN ointment (burned and treated with 2% VAN ointment). Beyond local infection control, perioperative nutrition substantially influences wound outcomes and recovery trajectories; contemporary Enhanced Recovery After Surgery [ERAS]-based evidence supports minimizing prolonged fasting and optimizing nutritional support to reduce complications and length of stay.25,26
Macroscopic analysis of burn wound
The burn wound images were collected and recorded on days 1, 4, 7, 10, and 15 (n = 4). Wound area (percentage of residual wound area to initial wound area) was assessed using ImageJ software (NIH, USA), and wound healing rates were quantified using GraphPad Prism software.
Quantitation of bacterial wound infection and histopathological examination
Mice were anesthetized by intraperitoneal injection of 10% (w/v) chloral hydrate (350 mg/kg; Shanghai Yuanye Bio-Technology #R21477). After sample collection, euthanasia was performed via cervical dislocation in accordance with the American Veterinary Medical Association Guidelines (2020 Edition). Wound surface (5 mm around the wound edge) was disinfected with 75% ethanol to eliminate surface contaminants (e.g., environmental bacteria) without affecting the underlying burn wound tissue. Next, using sterile surgical scissors and forceps excised the entire wound tissue along with a 2-mm wide margin of surrounding intact skin to ensure inclusion of the full wound healing zone, including the wound bed, granulation tissue, and adjacent normal skin. A 1 cm2 skin sample from the wound margin was homogenized via physical homogenization: it was added to 1 mL of sterile 0.9% NaCl and processed with a tissue grinder (TissueLyser II, Qiagen) at 30 Hz for 2 min to preserve bacterial viability. Followed by 10-fold serial dilutions to achieve a final dilution of 10−6, 100 μL of each dilution was taken at 10−4, 10−5, and 10−6 and was performed on blood agar plates (Luria-Bertani). Culture plates were incubated for 24 h at 37°C and CFUs counted.
H&E staining and Masson staining
Tissues were fixed in 4% paraformaldehyde (Beijing Solarbio) at 37°C for 48 h, embedded in paraffin, and sectioned at 5 μm. Sections were dewaxed and rehydrated using standard protocols. H&E staining was performed using hematoxylin (3–5 min) and eosin (15 s), followed by dehydration and clearing. Masson’s trichrome staining was carried out using a commercial kit (Servicebio #G1006) with appropriate differentiation and blue staining steps.
All sections were imaged under a Nikon Eclipse E100 microscope. Ten consecutive serial sections (consecutive 5 μm sections) were obtained per tissue block. From each section, six nonoverlapping fields of view were systematically sampled: one in the wound center, two in the wound edges, two in peri-wound normal skin, and one in areas showing pathological features. Collagen content was quantified as the percentage of the dermal area positively stained blue in Masson’s trichrome sections. A specific color threshold was applied to isolate the blue-stained collagen areas, and the ratio of this collagen-positive area to the total dermal area was calculated for each field. The average value from 10 randomly selected fields per sample was used for statistical analysis.
Sample processing and cytokine analysis by ELISA
Skin tissues were homogenized in ice-cold lysis buffer (PBS with protease inhibitor [Servicebio #G2006] and 0.1% Triton X-100) and centrifuged (12,000g, 20 min, 4°C). Supernatants were collected and analyzed using commercial ELISA kits (Elabscience) for IL-6 (#E-EL-M0044), IL-10 (#E-EL-M0046), TNF-α (#E-EL-M3063), and transforming growth factor-beta 1 (TGF-β1; #E-EL-0162). Acid activation (1N HCl, 10 min) and neutralization were performed for TGF-β1. All samples and standards were run in duplicate. Plates were incubated under optimized conditions: IL-6 and TNF-α at 4°C overnight and IL-10 and TGF-β1 at 37°C for 2 h. After washing, biotinylated detection antibodies (1: 100) were applied, followed by HRP-streptavidin (1: 100, Elabscience #E-EL-M002) and TMB substrate. Absorbance was measured at 450 nm with a 630 nm reference. All investigators performing ELISA were blinded to treatment groups to minimize assessment bias.
Immunohistochemistry
Deparaffinized sections underwent antigen retrieval (CD86/CD206: EDTA buffer, pH 8.0, 95°C, 25 min; inducible nitric oxide synthase [iNOS]/VEGF: citrate buffer, pH 6.0, 95°C, 20 min), peroxidase blocking (3% H2O2, 10 min), and incubation with primary antibodies at 4°C overnight: anti-CD86 (Servicebio #GB115630, 1: 200), anti-CD206 (#GB113497, 1: 400), anti-iNOS (Abcam #ab15323, 1: 200), and anti-VEGF (Servicebio #GB15165, 1: 200). After washing with PBS, they were incubated with the secondary antibody (#GB23303, 1:200), stained with DAB solution (#G1212), and observed at a magnification of × 100. All histological assessments were performed by researchers blinded to treatment groups.
Western blotting
Burn wound tissue samples were collected, washed with PBS, and cut into small fragments. The fragments were homogenized in RIPA lysis buffer (Servicebio #G2002) containing protease (Servicebio #G2006) and phosphatase inhibitors (Servicebio #G2007), followed by incubation on ice for 1 h. The homogenate was then centrifuged at 12,000g for 15 min at 4°C to collect the supernatant.
Protein concentration was determined using a bicinchoninic acid assay kit (Servicebio #G2026). Proteins were separated by sodium dodecyl sulfate-polyacrylamide gel electrophoresis and transferred to 0.45 μm PVDF membranes via wet transfer. Prior to transfer, the membranes were activated in methanol and equilibrated in transfer buffer containing 20% methanol. Transfer was carried out at 100 V for 90 min under cold conditions (4°C). Membranes were blocked with 5% skim (TBST buffer solution (Servicebio #G2150) + 0.1% Tween-20 (Servicebiot #GC204002) milk in TBST for 1 h at 37°C and then incubated overnight at 4°C with the following primary antibodies: anti-P65 (Servicebio #GB11997, 1: 1000), anti-p-P65 (Cat #GB113882, 1: 1000), anti-IκBα (#GB111509, 1: 1000), anti-p-IκBα (#GB15212, 1: 1000), anti-iNOS (#GB115703, 1: 1000), anti-CD86 (#GB115630, 1: 1000), anti-GAPDH (#GB15004, 1: 2000), and anti-β-actin (#GB1500, 1: 2000). After washing, membranes were incubated with HRP-conjugated secondary antibodies (antirabbit proteintech #SA00001-2, 1: 3000; antimouse, #SA00001-1, 1: 3000) at room temperature for 1 h.
Protein bands were quantified using ImageJ software. Images were converted to 8-bit grayscale, and a consistent threshold was applied to exclude background. The integrated density of each target band and corresponding β-actin reference band was measured, and relative expression was calculated as the ratio of target to reference density (n = 3).
Analysis of mRNA expression by qPCR
The mRNA expression levels (n = 3) were determined using quantitative real-time polymerase chain reaction (qRT-PCR). Total RNA was extracted from skin tissue biopsies using TRIzol reagent, followed by reverse transcription into cDNA with SuperScript™ III First-Strand Synthesis SuperMix for qRT-PCR (Invitrogen, USA). Quantitative analysis was performed using a Light Cycler 96 instrument (Roche, Switzerland). The qPCR reactions were carried out in a final volume of 20 μL under the following cycling conditions: initial denaturation at 95°C for 3 min, followed by 40 cycles of denaturation at 95°C for 10 s, annealing at 60°C for 10 s, and extension at 72°C for 15 s. All samples were analyzed in triplicate. The primer sequences are listed in Supplementary Table S5. GAPDH was used as the internal control, and data were analyzed using the 2-ΔΔCt method.
Statistical analysis
Data normality was assessed via the Shapiro–Wilk test (SPSS 27.0) and visual validation with Q–Q plots to verify statistical assumptions. For normally distributed data, results are presented as mean ± SD: Longitudinal data were analyzed using mixed-effects models, and cross-sectional data via one-way analysis of variance (ANOVA) with Tukey’s post hoc test or independent samples t-tests as appropriate (GraphPad Prism 9.0). Bonferroni correction was applied to pairwise comparisons in mixed-effects and one-way ANOVA analyses to control family-wise error, whereas False Discovery Rate [FDR] correction was reserved for potential high-dimensional data analyses (not required here due to no such datasets). No violations of normality assumptions were observed in our dataset, so no corrective transformations or robust methods were needed. A two-tailed p < 0.05 was considered statistically significant.
RESULTS
Acute dermal toxicity test
Throughout the trial period, the growth of mice in all groups remained normal. No abnormal secretions were observed in the mouth, ears, nose, or eyes, and no signs of abnormalities in skin, fur, respiration, drinking, eating, or excretion were noted. In addition, no neurological symptoms such as convulsions, spasms, or ataxia were observed. No adverse skin reactions occurred, and no mortality occurred. Body weights were recorded and compared between the control group and the 2% 4k treatment group. No statistical differences were observed between the two groups either before treatment (95% confidence interval [CI]: 0.86 to 0.56, p = 0.55), on day 7 post-treatment (95% CI: 0.83 to 0.61, p = 0.75), or on day 14 post-treatment: (95% CI: 0.95 to 0.49, p = 0.51) (Supplementary Table S1).
Histopathological studies were conducted to confirm any changes in tissue morphology of kidneys and skin (Fig. 2A). Microscopic evaluation of the tissues from the kidneys of control and 4k groups showed normal histology (95% CI: 1.57 to 1.02, p = 0.65). The cortex had multiple normal glomeruli with normal capillary loops, no extra mesangial cells, and normal mesangial matrix deposition. The medulla, interstitial, and proximal convoluted tubules were all normal, and no area of ischemia or necrosis was seen.
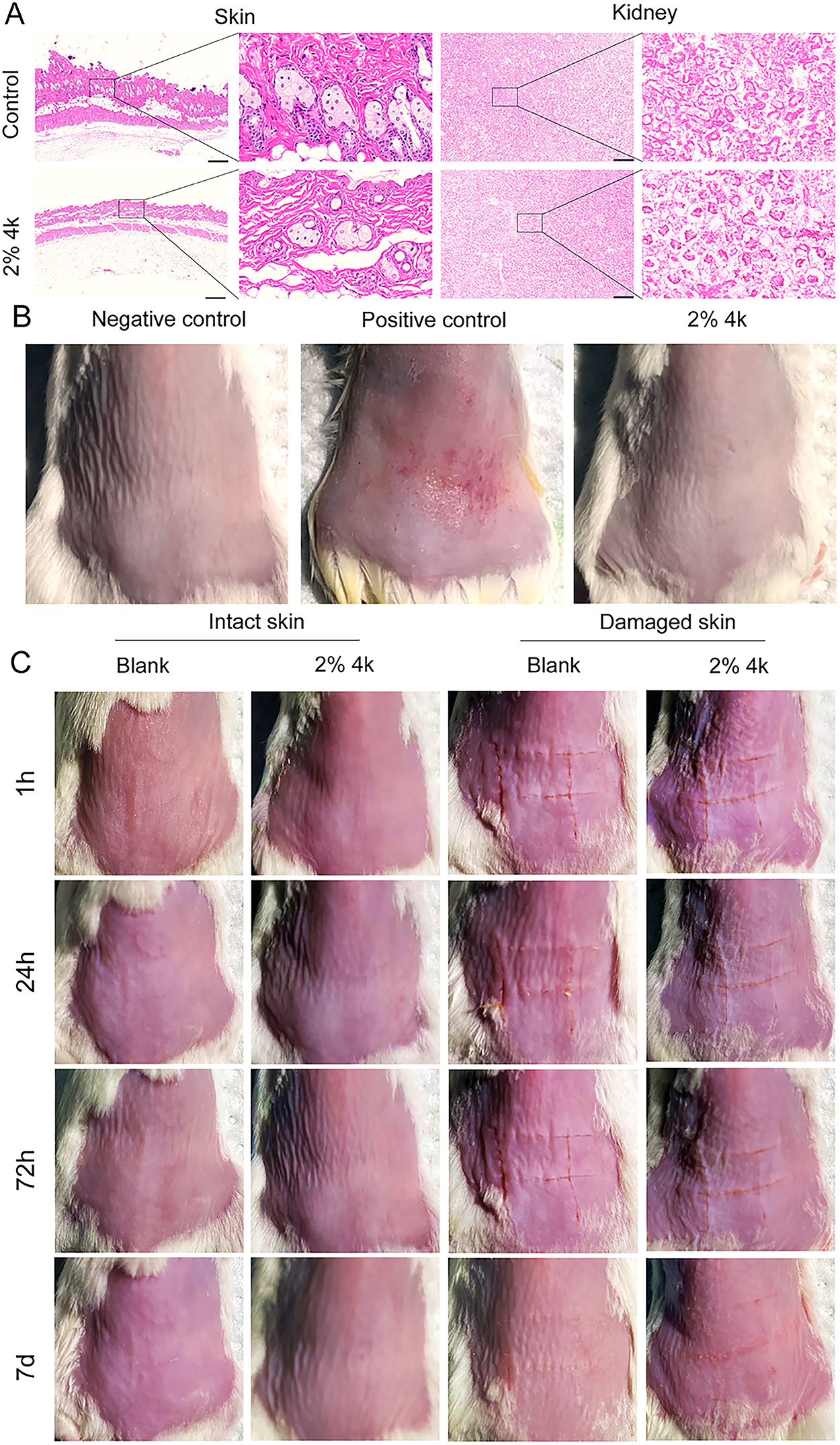
4k demonstrates good skin safety.
The skin structure was organized into three distinct layers, from outermost to innermost: the epidermis, dermis, and subcutaneous tissue. In addition, the skin contained accessory structures, including hair follicles, sweat glands, sebaceous glands, as well as abundant nerves, blood vessels, lymphatic vessels, and muscle tissue. Microscopic examination of the 4k group skin tissue revealed no histological differences compared with the control group (95% CI: 0.99 to 1.62, p = 0.65; Fig. 2A). This study confirmed that compound 4k is safe with no acute toxicity.
Skin allergy test
The mice in allergic allergy test were treated with a 2% 4k solution. 21 In the formalin (0.8% v/v) group, a severe sensitization response was observed just 5 min after the final sensitization on 14 days. The animals displayed clear signs of restlessness, including frequent licking and biting of the skin where the solution had been applied, along with moderate local erythema. These behaviors indicated a strong allergic reaction. In contrast, mice treated with vaseline or 2% 4k solution remained calm and exhibited no such behaviors, suggesting that they either did not experience an allergic response or showed minimal sensitivity to the treatment (Fig. 2B). On day 14, the sensitization mice of formalin group were 100% (0 h), 80% (24 h), 20% (48 h), and 0% (72 h), and the average scores of allergic reaction were 2.0 (0 h), 1.0 (24 h), 0.2 (48 h), and 0 (72 h) (Supplementary Table S2), respectively. No erythema or edema was observed in the vaseline and 2% 4k groups at each time point, with sensitization mice and average scores of allergic reactions both being 0. Therefore, the allergic test on the skin of the mice showed no allergic reaction to 2% 4k.
Skin irritation test
At 1 h, 24 h, 72 h, and 7 days postadministration, no erythema, eschar, or edema was observed in either the intact or damaged skin of mice in the blank and 2% 4k groups. The skin appearance was comparable to that of the blank group (Fig. 2C). Skin irritation scores for all four groups were 0, indicating the absence of any skin irritation response.
Wound healing
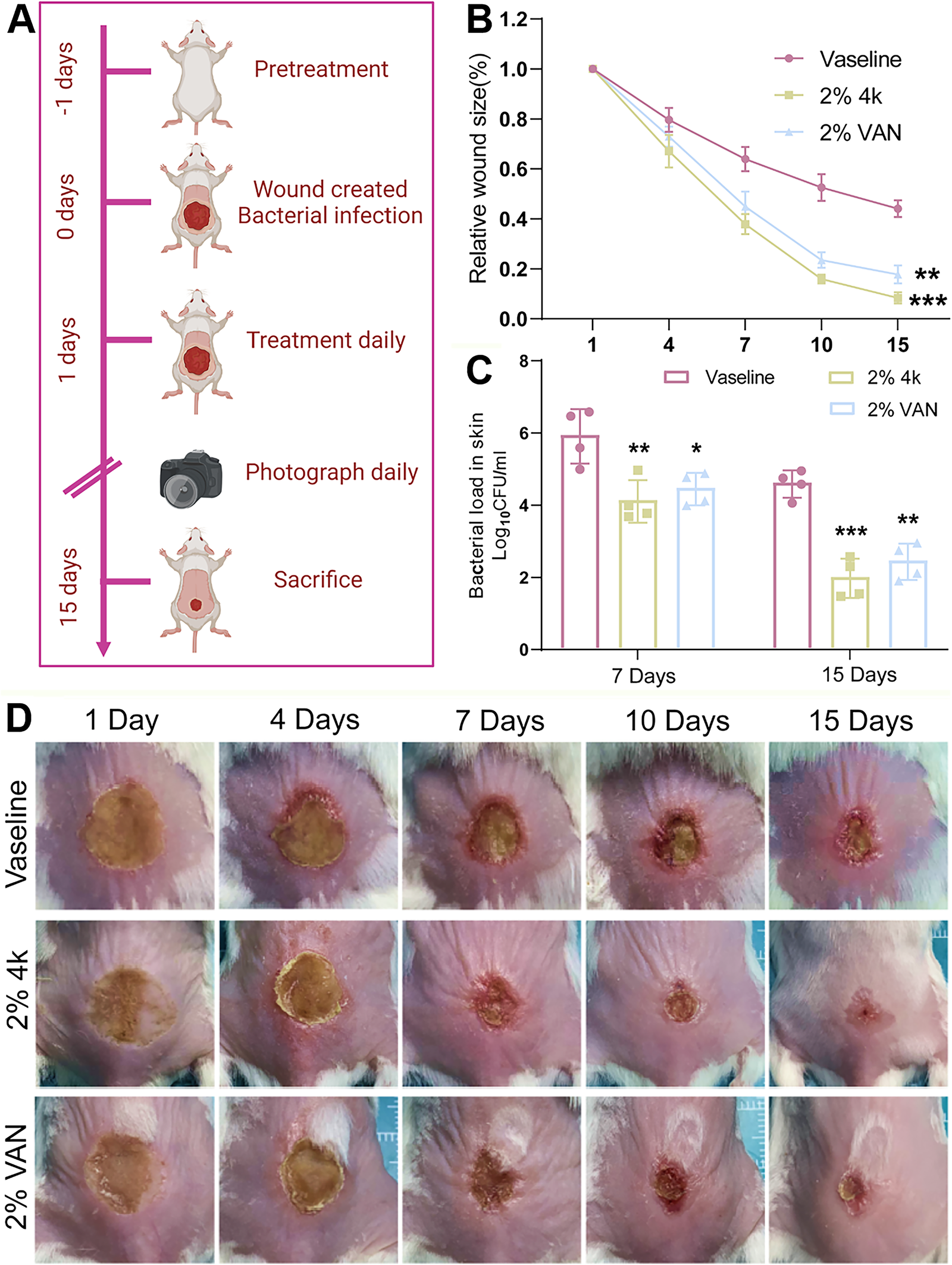
To investigate the potential healing ability of 4k on burn wounds, a mouse model was established, and the timeline for model preparation, treatment, and evaluation in vivo is shown in Figure 3A. During the entire experimental procedure, no mice died from anesthesia, infection, or other complications. The control group exhibited the lowest healing effect accompanied by blisters, redness, and swelling. It indicated that the burn model had been successfully established, which is a reliable method to evaluate the antibacterial and anti-inflammatory activity of 4k. 27
Healing effects of 4k on burns in mice with MRSA2858.
As shown in Figure 3B and D, the healing effect of each group increased significantly after 7 days. In contrast to the vaseline group, with continuous treatment of each administration group with drugs, the wounds began shrink over time.
Notably, nearly complete wound healing was observed in the 2% 4k treatment group by day 15, with no significant scar formation detected. Compared with the vaseline group, treatment with 4k significantly shortened wound healing time (8.4 ± 2.2% vs. 44.1 ± 3.3% for vaseline, p = 0.0005; 17.8 ± 3.5% for 2%VAN), demonstrating a clear advantage in promoting burn wound closure.
MRSA colonization is closely related to skin infection, so inhibiting the bacterial burden slows down the symptoms of skin burns in mice. On 7 days and 15 days after MRSA infection, colonies were counted at the wound site. As illustrated in Figure 3C, on day 15, 2% VAN group showed a significant difference compared with the control group (p = 0.00158). Treatment with 4k led to a significant reduction in CFU counts in a dose-dependent manner (2.0 ± 0.5 vs. 4.6 ± 0.4 for vaseline, p = 0.000029). 4k significantly reduced bacterial load by >90%. These findings indicated that 4k not only decreased MRSA colonization but also promoted wound healing and reduced burn scar formation, indicating excellent burn healing ability.
Histology
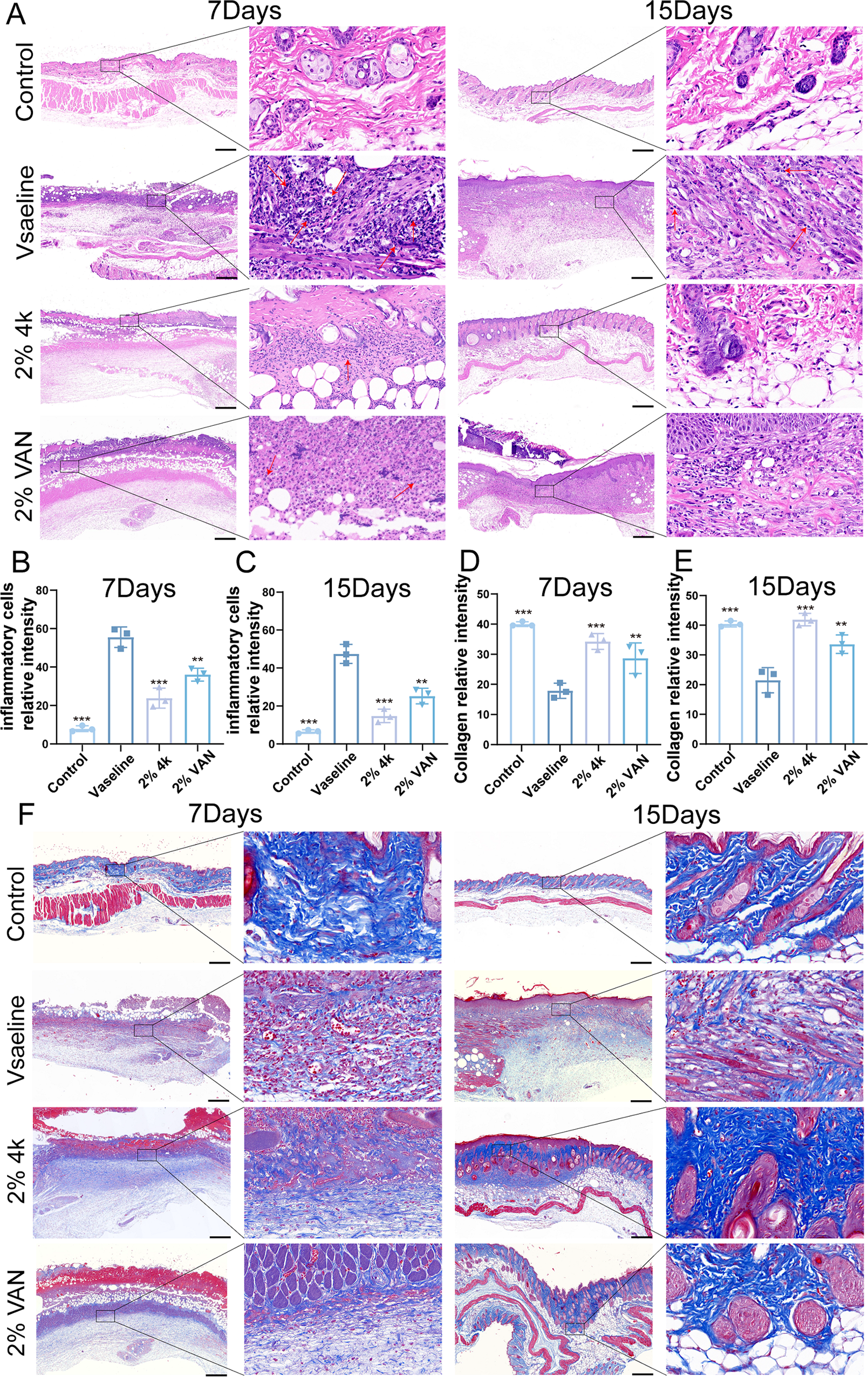
The effect of 4k on the histopathological changes and collagen deposition was determined by H&E staining and Masson staining, respectively. At the end of 7 days and 15 days, the animals were sacrificed, and skin samples were taken for histological examination. The result is shown in Figure 4A. The skin of the normal untreated group had a complete cuticle, hair follicle and accessory structure, clear prickle cell layer, and horizontal stripes in the deep leather muscle. In the burn model group, there was severe injury, including the damaged structure of the skin, necrotic cells, severe subcutaneous edema, and inflammatory cells in burn wound tissues on 7 days. On 15 days, re-epithelization of the wound was still incomplete. In the 2% 4k group, fewer inflammatory cells were observed under the microscope, and more granulation tissue grew on 7 days. The wound was covered with epithelium, and many fibroblast cells could be seen under the microscope on 15 days. There was full-thickness re-epithelization, in which the epidermis was thin and well organized: control group versus vaseline group (p = 0.000209); 2% 4k group versus vaseline group (p = 0.000827); and 2% VAN group versus vaseline group (p = 0.00244).
4k attenuates inflammation and accelerates burn wound closure.
Moreover, the epidermis and dermis were similar to healthy skin, the hair follicle structure was well formed, and most of the area was covered with hair. Compared with the 2% 4k group, there was still much necrotic tissue in the VAN group on 7 days, and little hair follicle structure existed on 15 days (Fig. 4A, B, C). In summary, 4k exerts anti-inflammatory effects, with efficacy profiles overlapping those of VAN.
Collagen deposition and remodeling are essential processes in deep burn wound repair. To evaluate these processes, Masson’s trichrome staining was performed on wound tissues collected on days 7 and 15 postburn. As shown in Figure 4F, on day 7, wounds in the vaseline group exhibited severe structural disruption, including necrotic cells, marked subcutaneous edema, and inflammatory infiltration. By day 15, these wounds were covered by thin granulation tissue with minimal hair follicle regeneration, indicating impaired healing.
In contrast, wounds treated with 2% 4k showed improved architectural restoration as early as day 7, characterized by more densely packed and parallelly aligned collagen fibers—features associated with reduced scarring (Fig. 4B; p = 0.00089). By day 15, these wounds displayed robust collagen deposition, along with the presence of newly formed hair follicles and sebaceous glands, suggesting not only structural but also functional recovery of the skin (Fig. 4C).
Quantitative analysis (Fig. 4D, E, Supplementary Table S3) confirms that the control group showed no scar formation (mean score = 0.00 ± 0.00), whereas the vaseline group exhibited severe scarring (mean = 13.33 ± 0.58, p < 0.001 vs. control). The 2% 4k group achieved significantly milder scarring (mean = 2.33 ± 0.58, p < 0.001 vs. vaseline) with improved collagen organization (95% CI: –21.43 to –25.18, p = 0.00073) and no significant difference from the control group (p = 0.086). Moreover, the 2% 4k group outperformed the 2% VAN group (mean = 6.33 ± 3.06, p = 0.005 vs. 2% 4k), which showed less organized collagen consistent with early scar formation. These findings highlight 2% 4k’s superior antiscarring efficacy in MRSA-infected burn mice. In line with our collagen findings, specialized nutrition—notably combinations of arginine, glutamine, and β-hydroxy-β-methylbutyrate—has been associated with increased collagen synthesis and improved wound repair, underscoring the systemic milieu as a codeterminant of healing. 28
These findings demonstrate that 2% 4k not only accelerates wound closure but also promotes a collagen architecture histologically associated with regenerative healing rather than fibrotic scarring.
NF-κB signaling pathway
Previous studies have shown that the NF-κB pathway plays a crucial role in skin fibrosis and macrophage proinflammatory responses. To further verify the 4k in inhibiting inflammation of MRSA-infected skin burn model, western blot detection of the NF-κB signaling pathway was performed (Fig. 5A), in which burn can upregulate profibrotic and proinflammatory cytokines through activation of NF-κB. Therefore, the effects of 4k on NF-κB pathway were further investigated the expression of NF-κB signaling pathway-related proteins with P65 and IκBα.
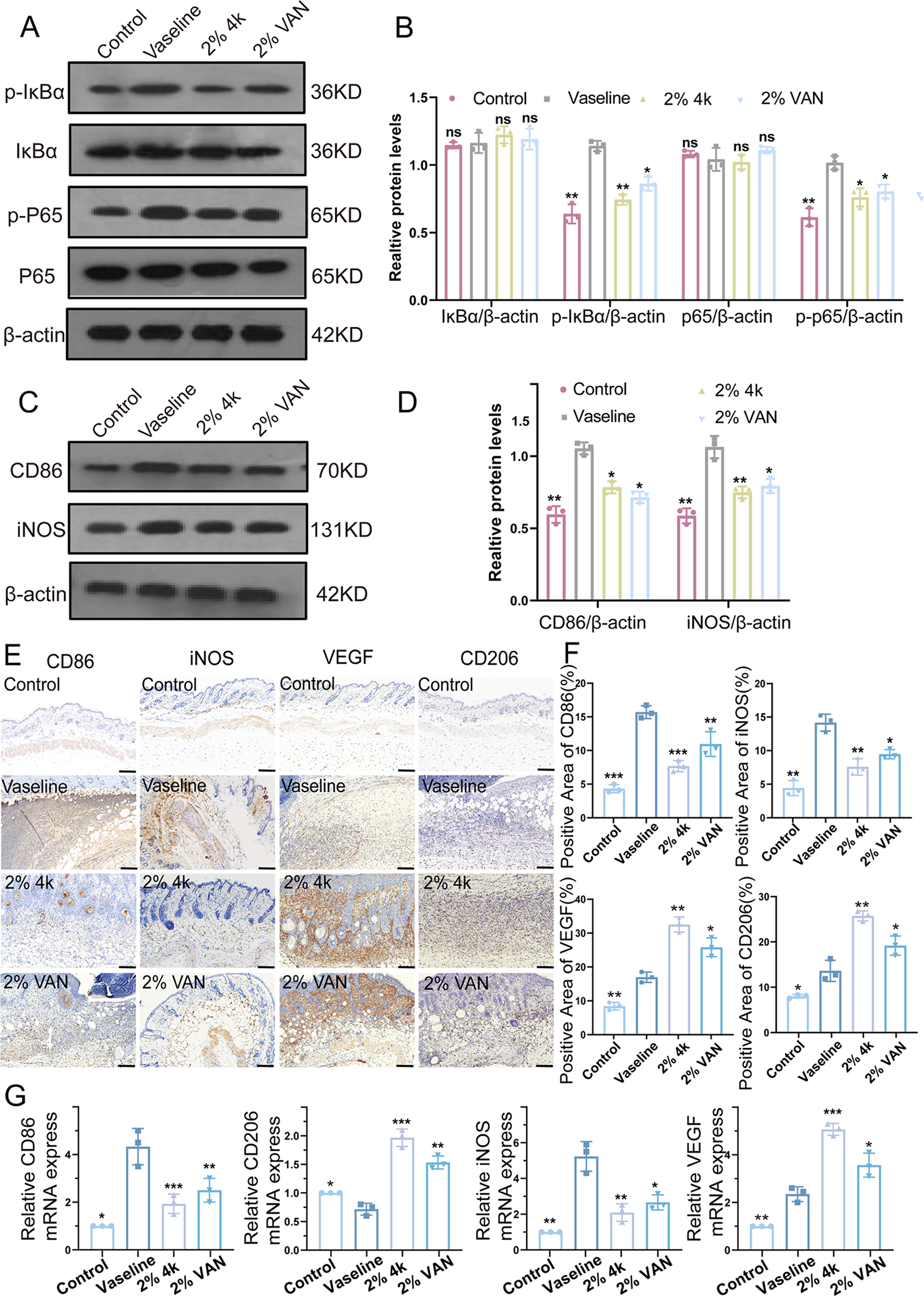
Analyses of IκBα/P65 phosphorylation, CD86/iNOS/CD206/VEGF expression, and mRNA levels in MRSA-infected mouse skin tissues
In the vaseline group, the protein expression of p-P65 and p-IκBα in the skin of mice was significantly increased, whereas all these proteins were significantly suppressed after 4k and VAN treatment (Fig. 5A, B, Supplementary Fig. S4, Supplementary Table S4; p < 0.05). This indicated that 4k may exert antibacterial and anti-inflammatory effects by attenuating the NF-κB pathway. 29
Macrophage polarization
4k was found to promote wound healing in MRSA-infected burn wounds, although its underlying mechanism remained unclear. Given the critical role of inflammation in recruiting immune cells such as macrophages and its close association with disease progression, we focused on the inflammatory cytokines regulated by NF-κB, including IL-6, IL-10, TNF-α, and TGF-β1. Previous studies have indicated that attenuation of the NF-κB pathway can shift macrophage polarization from the proinflammatory M1 phenotype to the prohealing M2 phenotype, thereby attenuating disease progression.
Given the importance of macrophage polarization in wound repair, we evaluated the protein expression of M1 markers (CD86 and iNOS) and M2 markers (CD206 and VEGF) on day 15 postinfection to investigate their correlation with skin fibrosis in MRSA-infected burn wounds. Western blot analyses (Fig. 5C, D, Supplementary Table S4, Supplementary Fig. S4; p < 0.05), IHC (Fig. 5E, F, Supplementary Table S4; p < 0.05), and qRT-PCR (Fig. 5G, Supplementary Table S4; p < 0.05) revealed significantly elevated expression of CD86 and iNOS, along with slightly increased levels of CD206 and VEGF, in the vaseline group compared with the control group.
Notably, in the infected wounds, treatment with 2% 4k downregulated CD86 and iNOS expression and markedly upregulated VEGF and CD206 expression relative to the vaseline group; this directional change was identical to that observed in the 2% VAN group, whereas the response magnitude varied between the two treatments. These results suggest that 4k inhibits M1-skewed polarization and promotes M2 macrophage activation in MRSA-infected burn wounds.30,31
Cytokine analysis in mice skin tissues
The cytokines associated with macrophage polarization were further measured by ELISA in mice skin tissues. It was observed that TNF-α and IL-6 levels were significantly elevated in the vaseline group. In contrast, treatment with 4k inhibited the promotion of M1 macrophage polarization induced by burns (Fig. 6A, B, Supplementary Table S4; p < 0.05). Moreover, the levels of inflammation-suppressing cytokines associated with M2 macrophages (IL-10 and TGF-β1) showed distinct patterns, with IL-10 and TGF-β1 levels significantly elevated in the 2% 4k and 2% VAN groups (Fig. 6C, D, Supplementary Table S4; p < 0.05). These data confirmed that 4k effectively inhibited proinflammatory cytokines (TNF-α and IL-6) and M1 macrophage polarization in the skin burn model of MRSA infection, while increasing anti-inflammatory cytokines (IL-10 and TGF-β1) and M2 macrophage polarization.
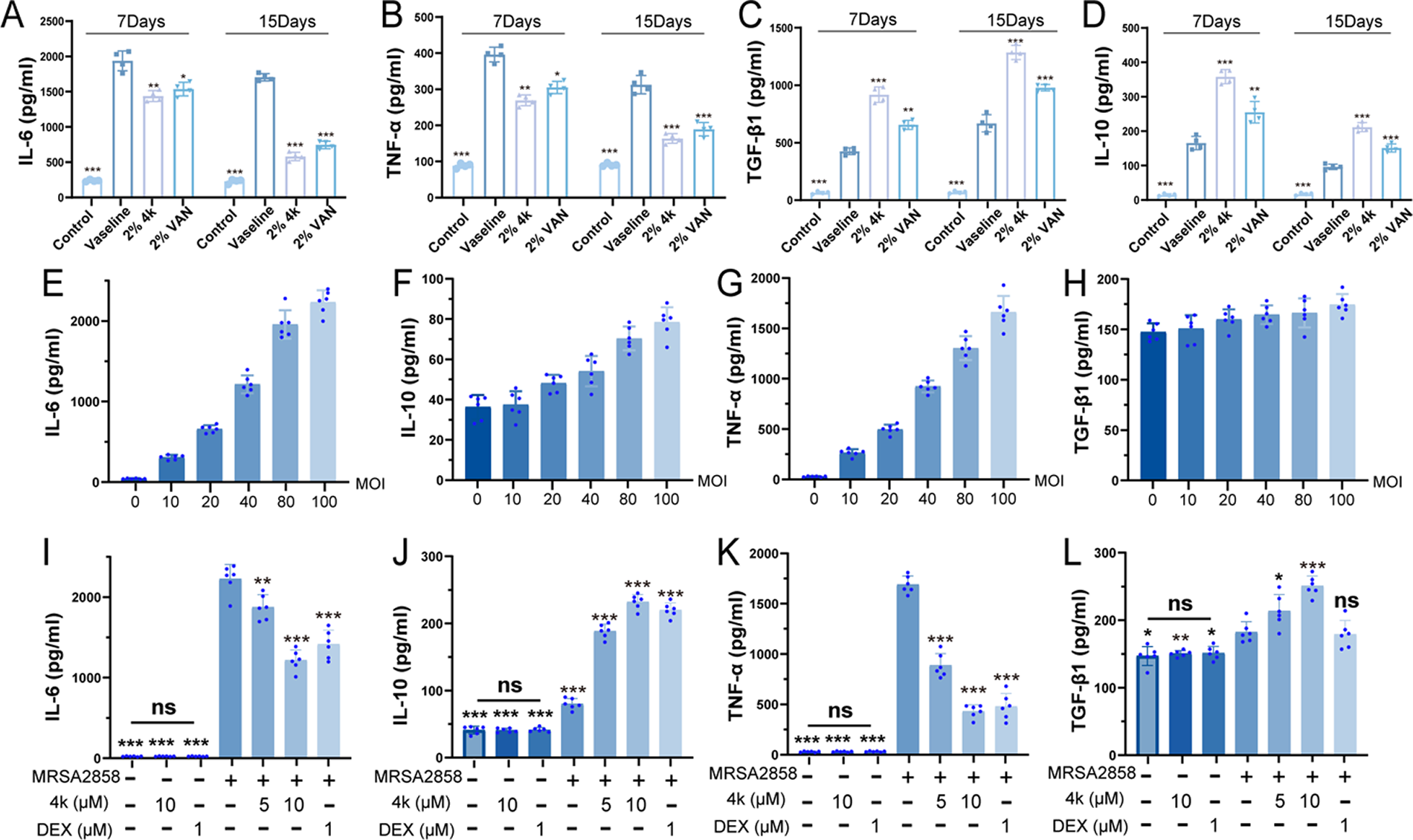
ELISA detection of IL-6, IL-10, TGF-β1, and TNF-α in scalded mouse skin tissue and RAW264.7 cell supernatants. (
Anti-inflammatory activity of 4k
Griess reagent was used to evaluate the anti-inflammatory effect of 4k by detecting the level of the LPS-induced NO release in the RAW264.7 cells. LPS treatment caused significant increase of NO release compared with blank; after pretreatment with 4k at concentration gradients of 1100 μM, the production of LPS-induced NO could be gradually reduced in the supernatant. The result indicated that 4k possessed anti-inflammatory activity (IC50 = 5.86 μM) in Supplementary Figure S2A. The inhibitory effect of 4k on LPS-induced inflammation provided a basis for studying its anti-inflammatory mechanism; however, its anti-inflammatory effect in MRSA infection needs to be analyzed in combination with MRSA-specific inflammatory pathways.
MRSA-infected model of RAW264.7 cells
The CCK-8 kit was used to evaluate the effect of 4k on the viability of RAW264.7 cells. Specifically, RAW264.7 cells were seeded in 96-well plates and treated with 4k at concentrations of 5, 10, 20, 30, and 40 μM. As shown in Supplementary Table S2B, after 24 h of exposure, 4k did not significantly reduce the viability of RAW264.7 cells even at the concentration of 20 μM. Based on these results, 5 and 10 μM of 4k were selected for subsequent experiments.
MRSA-infected inflammation in RAW264.7 cells
To confirm the role of 4k in anti-MRSA infection, we first examined the levels of IL-6, IL-10, TNF-α, and TGF-β1 in RAW264.7 cells infected with MRSA at various MOIs (Fig. 6E, F, G, H). At 12 h postinfection, MRSA significantly increased IL-6 and TNF-α levels but had no significant effect on IL-10 and TGF-β1 levels. In addition, IL-6 and TNF-α levels rose dose-dependently when stimulated with MOIs of 10 to 100. We chose an MOI of 100 as optimal for RAW264.7 cells, as this MOI triggered the highest release of IL-6 and TNF-α, and a higher IL-10 release compared with lower MOIs.
Next, we evaluated the effect of 4k on inflammatory factors in MRSA-infected cells. 4k alone had no impact on cellular inflammatory factor levels. Both 5 and 10 μM 4k effectively suppressed the release of IL-6 and TNF-α while promoting the expression of IL-10 and TGF-β1 (Fig. 6I, J, K, L, Supplementary Table S4; p < 0.05). These results indicate that 4k is safe and effectively inhibits MRSA-infected inflammation.
DISCUSSION
Burn injuries represent a significant global health burden, with approximately 11 million new cases annually worldwide. 32 The clinical challenge is particularly acute in MRSA-infected burns, where conventional topical antimicrobials are partially effective but often produce complications including organ toxicity, delayed healing, and scarring. 33 The persistent morbidity associated with MRSA underscores the urgent need for novel antibiotics that combine antibacterial efficacy with favorable safety profiles.
Our findings established that the dual-action topical 4k effectively addressed this need by simultaneously eradicating MRSA and reprogramming the wound immune microenvironment. This represented a paradigm shift from conventional antibiotics such as VAN, which solely targeted bacterial elimination. While VAN demonstrated bactericidal activity, it lacked direct immunomodulatory capacity. In contrast, 4k not only exerted potent FabI-mediated antibacterial effects but also directly attenuated NF-κB signaling—a key driver of pathological inflammation. 13
The most significant evidence of 4k’s immunomodulatory action was its ability to reprogram macrophage polarization from a proinflammatory M1 to a prohealing M2 phenotype. 34 This transition was functionally consequential: we observed coordinated downregulation of TNF-α and IL-6 alongside elevated TGF-β1 and IL-10, enhanced collagen deposition, and accelerated re-epithelialization. Mechanistically, 4k suppressed IκBα and p65 phosphorylation,35,36 thereby disrupting the signaling cascade that perpetuates M1 dominance and tissue damage.37,38
The clinical implications are substantial. For burn patients with compromised skin barriers, the favorable safety profile and localized action of topical 4k were particularly advantageous. Its ability to concurrently clear infection and resolve inflammation positioned it as a promising candidate to reduce healing time, minimize scarring, and potentially diminish reliance on traditional antibiotics. Future studies will focus on further elucidating the precise crosstalk between bacterial clearance and immune reprogramming, paving the way for its clinical translation.
This study had two primary limitations. First, the similar anti-inflammatory effects observed with 4k and VAN suggested that NF-κB attenuation may partially result from effective bacterial clearance. Future studies employing sterile inflammation models and specific MRSA component challenges will help dissect 4k’s direct immunomodulatory properties. Second, techniques such as p65 nuclear translocation assays, Electrophoretic Mobility Shift Assay [EMSA], and flow cytometry will provide more direct validation of NF-κB regulation and macrophage polarization.
CONCLUSION
The novel N-benzyl benzenamine 4k demonstrated exceptional dual efficacy in a murine model of MRSA-infected burn wounds, combining potent FabI-mediated antibacterial activity with direct immunomodulation through NF-κB pathway attenuation. This dual mechanism drove a critical transition in macrophage polarization from pro-inflammatory M1 to prohealing M2, resulting in accelerated wound closure, improved collagen architecture, and a balanced cytokine milieu. Together with 4k’s excellent topical tolerability, these findings underscore the translational potential of 4k as a promising therapeutic candidate. Future work will focus on formulation optimization and validation in more complex wound models to advance 4k toward clinical application.
KEY FINDINGS
AUTHORS’ CONTRIBUTIONS
M.X.: Writing—original draft, software, methodology, investigation, formal analysis, data curation, and conceptualization. Z.Y. and W.S.: Software, investigation, and data curation. W.S.: Software, methodology, data curation, and conceptualization. M.C.: Software, methodology, and investigation. D.L.: Supervision and investigation. W.T. and D.L.: Software, resources, data curation, and conceptualization. J.Z.: Writing—review and editing, validation, project administration, funding acquisition, conceptualization, data curation, methodology, and supervision.
Footnotes
FUNDING INFORMATION
Financial support was provided by Scientific Research Project of Education Department of Anhui Province (2022AH052333), Anhui Provincial Natural Science Foundation (2408085MH190), Open Project of Anhui Province Key Laboratory of Occupational Health (2024ZYJKA002), and Research Funds of Joint Research Center for Occupational Medicine and Health of IHM (OMH-2024-043).
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
DATA AVAILABILITY
The data that have been used are confidential. The authors confirm that the data supporting the findings of this study are available within the article as its supplementary materials.