
Abstract
Objective:
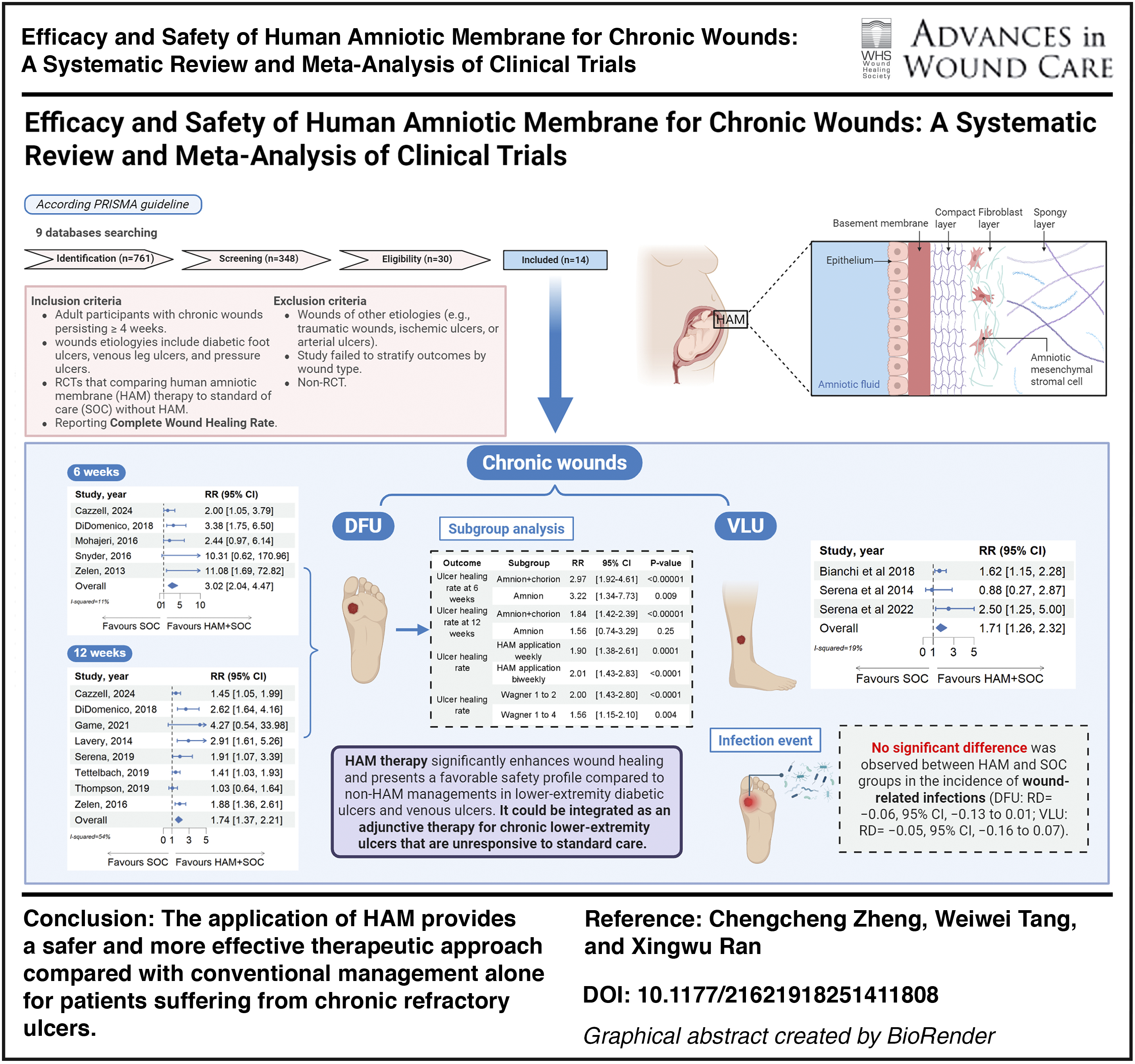
The meta-analysis was performed to evaluate the efficacy and safety associated with the application of human amniotic membrane (HAM) in individuals with chronic nonhealing wounds.
Approach:
The research conducted a comprehensive search of nine electronic databases from their inception to August 1, 2024, aiming to identify randomized controlled trials (RCTs) that evaluated the efficacy of HAM compared with conventional management alone in individuals suffering from chronic wounds. The risk of bias of included studies and the certainty of the evidence in the meta-analysis were evaluated by two investigators and confirmed by a third. The meta-analysis was performed using RevMan 5.4 software.
Results:
We identified 14 RCTs encompassing a total of 1,056 participants. The potential risk of bias was determined to be moderate. HAM therapy demonstrated significantly greater efficacy than conventional treatment alone in achieving complete wound healing among patients with chronic ulcers (relative risk [RR] = 1.82; 95% confidence interval [CI]: 1.48–2.24; moderate-quality evidence). In patients with diabetic foot ulcers, HAM reduced the mean time to complete healing by 22 days compared with standard care alone (mean difference = −22.09 days; 95% CI: −39.13 to −5.05; low-quality evidence) and increased the rate of complete healing at 6 weeks (RR = 3.02; 95% CI: 2.04–4.47; moderate-quality evidence) and at 12 weeks (RR = 1.74; 95% CI: 1.37–2.21; low-quality evidence). Similarly, in patients with venous leg ulcers, HAM was associated with more than twice the likelihood of complete healing (RR = 2.03; 95% CI: 1.45–2.86; moderate-quality evidence). No statistically significant differences were noted in the incidence of adverse events among patients with chronic ulcers (moderate-quality evidence).
Innovation:
Our study suggests that HAM represents a promising and viable therapeutic strategy for the management of chronic wounds, including lower-extremity diabetic ulcers and venous ulcers.
Conclusion:
The application of HAM provides a safer and more effective therapeutic approach compared with conventional management alone for patients suffering from chronic refractory ulcers.
Keywords
CLINICAL RELEVANCE
Chronic wounds, including DFUs and VLUs, represent a significant health care burden due to prolonged healing times and high recurrence rates. This study highlights that HAM therapy, as an adjunct to standard care, promotes faster and more reliable healing with a safety profile comparable to conventional treatments.
Xingwu Ran, MD, PhD

RECOMMENDATIONS FOR PRACTICE
Clinicians should consider incorporating HAM into treatment regimens for patients with chronic DFUs and VLUs, particularly when conventional treatments have failed or healing is delayed. The use of HAM, regardless of application frequency (weekly or biweekly), offers consistent therapeutic benefits and can be integrated into existing wound care protocols. Given the moderate- to low-quality evidence, future studies should focus on further validating the optimal application frequency of HAM and exploring long-term clinical outcomes, including recurrence and cost-effectiveness, to provide better evidence for clinical application and health care policy.
INTRODUCTION
Chronic wounds impose a considerable burden on the health care system due to their escalating prevalence and associated economic costs. These wounds affect approximately 15% of Medicare beneficiaries, with annual health care expenditures estimated to range between $28 and $96 billion. 1 Patients suffering from chronic wounds often experience a significant decline in quality of life, comparable to that observed in individuals with chronic renal and cardiovascular diseases. 2 The most common types of chronic wounds include diabetic foot ulcers (DFUs), venous leg ulcers (VLUs), and pressure injuries. Conventional treatment approaches for nonhealing wounds, regardless of their underlying etiology, typically focus on addressing comorbid disorders while emphasizing evidence-based wound care practices aimed at facilitating the formation of healthy granulation tissue.3,4 More advanced therapeutic approaches aim to enhance the microenvironment for wound healing beyond the standard of care (SOC) through the application of various bioactive agents and cellular therapies, such as platelet-rich plasma, extracellular matrix components, and stem cell therapy. 5 Human amniotic membrane (HAM), recognized as a more promising allograft for wound healing, has been extensively utilized across various clinical fields, including ophthalmology, chronic wounds management, burn treatment, plastic reconstruction surgery, and periodontal therapy for over a century.6,7 Although multiple observational studies have reported notable efficacy of HAM in treating chronic wounds, such as VLUs,8–10 DFUs,11–19 and pressure ulcers, 20 its broader clinical application remains limited due to insufficient high-quality evidence. Although a limited number of randomized controlled trials (RCTs) have demonstrated HAM is superior to conventional management in promoting healing of chronic ulcers, these studies were generally small in scale and lacked sufficient statistical power to confirm clinically relevant outcomes. Therefore, this systematic review was conducted to comprehensively evaluate the efficacy and safety of HAM specifically in the treatment of lower-extremity diabetic ulcers, lower-extremity venous ulcers, and chronic pressure ulcers.
INNOVATION
Current approaches to the management of chronic wounds continue to face challenges in achieving timely and effective healing, despite the application of advanced therapeutic modalities. Although HAM has emerged as a promising adjunctive treatment, its broader clinical adoption has been limited by a lack of high-quality evidence. This is the first meta-analysis to comprehensively include all recent RCTs evaluating HAM for the treatment of VLUs and DFUs. We demonstrate that HAM significantly enhances complete healing rates and reduces healing time comparing with the conventional treatment, without any associated increase in the risk of infection. These findings provide robust evidence supporting the integration of HAM into standard wound care protocols, offering a clinically effective strategy to improve outcomes for patients suffering from refractory diabetic and venous ulcers.
CLINICAL PROBLEM ADDRESSED
Chronic wounds, particularly lower-extremity diabetic and venous ulcers, impose a substantial burden on health care systems due to their high prevalence, prolonged healing duration, and frequent recurrence. Conventional therapeutic approaches often fail to achieve complete wound closure, leading to impaired quality of life and escalating medical costs. While various treatment modalities have demonstrated efficacy, many are associated with high costs or limited accessibility for certain patient populations. HAM, as a well-established biological scaffold, has been widely utilized for decades in the management of wound healing. Accumulating evidence from well-conducted studies underscores its potential to accelerate the healing process in chronic wounds. This study employed a systematic review and meta-analysis of RCTs to evaluate the efficacy and safety of HAM in treating chronic wounds, addressing critical gaps in the existing evidence and providing actionable insights for its clinical practice.
MATERIALS AND METHODS
Search strategy
The meta-analysis was conducted in accordance with the 2009 guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analyses, 21 and the detailed process is illustrated in Figure 1. A comprehensive literature search was carried out across multiple electronic databases, including Ovid Medline, Embase, PubMed, Web of Science, and the Cochrane Central Register of Controlled Trials, China National Knowledge Infrastructure, China Biology Medicine, Wan Fang database, and VIP database, covering all publications from the inception of each database up to August 1, 2024, without any language restrictions. In addition, a comprehensive search was carried out on the clinicaltrials.gov database to identify any relevant ongoing or unpublished clinical trials. Our retrieval strategy combined Medical Subject Headings with relevant free-text terms. A detailed description of the search strategy is provided in Supplementary Table S1. Furthermore, reference lists of original studies, systematic reviews, and meta-analyses deemed relevant were screened to identify additional eligible literature. The systematic review and meta-analysis were prospectively registered in International Prospective Register of Systematic Reviews (CRD42024586718).

Flow diagram of the study selection for the systematic review and meta-analysis.
Eligibility criteria and exclusion criteria
Eligible RCTs enrolled adult participants with chronic wounds that persisted for a minimum of 4 weeks, including lower-extremity diabetic ulcers, lower-extremity venous ulcers, pressure ulcers, or a combination of these etiologies. The selected RCTs compared HAM management with any form of conventional wound care that did not involve HAM and reported outcomes in terms of complete wound healing. There were no restrictions regarding publication language. Trials were excluded if they included wounds of other etiologies (e.g., traumatic wounds and those associated with peripheral arterial disease); failed to stratify outcomes by wound type; repeated publication of literature; employed a crossover design; and lacked original data such as narrative reviews, editorials, or secondary analyses of previously published trials.
Inclusion criteria
RCTs enrolling adult participants with chronic wounds (including DFUs, VLUs, and pressure ulcers) lasting for a minimum of 4 weeks. A comparison between HAM therapy (in any preparation or form) and standard wound care that does not involve the use of HAM. Reporting of the complete wound healing rate. No restriction on the publication language.
Exclusion criteria
Studies that encompass wounds of other etiologies, such as traumatic wounds, ischemic ulcers, or arterial ulcers. Studies that failed to stratify the outcomes based on the wound type. Repeated publication of academic literature. Crossover designs, narrative reviews, editorials, or secondary analyses of previously published data.
The titles and abstracts retrieved from the database search were preliminarily screened by two independent reviewers (C.Z. and W.T.). Studies deemed eligible by either reviewer were selected for full-text assessment. Subsequently, a comprehensive evaluation of the full-text articles was conducted. Any discrepancies between the two reviewers were resolved through consultation with a third, senior investigator (X.R.).
Primary and secondary outcomes
The primary outcome assessed in this review was the proportion of complete wound healing. Secondary outcomes included the average time required to achieve complete healing, the percentage of patients achieving a ≥50% reduction in ulcer area, and any adverse events reported during the study period. Complete healing was defined as the complete reepithelialization of ulcers, with no signs of drainage or need for dressing. 22
Data extraction
The paired reviewer (C.Z. and W.T.) independently extracted the following data: (1) publication details, including authors, study title, year of publication, study design, intervention setting, Universal Trial Number (UTN), and enrollment period; (2) patient characteristics, such as age, gender, body mass index, and mean glycated hemoglobin levels; (3) baseline ulcer characteristics, including ulcer location, position, size, and grade of ulcers; (4) details of the intervention groups, including the brand and manufacturer of amnion used, as well as the frequency of application; (5) details of the control groups; and finally, (6) outcome assessments, including the proportion of ulcers achieving complete healing, mean time to complete healing, the proportion of patients with a ≥50% reduction in ulcer area, and any adverse events reported. Any discrepancies were resolved by discussion with a third author (X.R.).
Assessment of risk of bias
The Cochrane Collaboration’s Risk of Bias 2 (RoB 2) tool was independently applied by two independent reviewers (C.Z. and W.T.) to evaluate potential biases in the included studies systematically. Any discrepancies between the reviewers were resolved through a third author (X.R.).
Assessment of the certainty of evidence
The certainty of the evidence was evaluated by two reviewers (C.Z. and W.T.) in accordance with the Grading of Recommendations Assessment, Development and Evaluation Approach (GRADE) system. The GRADE system divides the certainty of evidence into four levels: high, moderate, low, and very low. These levels are based on five factors: risk of bias, inconsistency, indirectness, imprecision, and publication bias. 23 Any discrepancies between the reviewers were resolved through a third author (X.R.).
Statistical analyses
The clinical and methodological heterogeneities across the included studies were systematically evaluated based on their study characteristics. In cases where substantial homogeneity was observed among these characteristics, a quantitative data synthesis was conducted using Review Manager software (Version 5.4, The Cochrane Collaboration, 2020). Statistical heterogeneity was evaluated utilizing both the Cochran Q test and the I2 statistic. An I2 value <50% was considered to indicate acceptable heterogeneity, in which scenario a fixed-effects model was employed. Otherwise, if the I2 statistic exceeded this threshold, suggesting significant heterogeneity, a random-effects model with Mantel–Haenszel weighting was utilized. All analyses were conducted in accordance with the intent-to-treat principle. For binary outcomes, relative risks (RRs) and risk differences (RDs) were calculated and reported. With respect to continuous variables, mean differences (MDs) along with their corresponding 95% confidence intervals (CIs) were presented as measures of effect size. All statistical tests were conducted using two-sided tests at a significance level of 0.05. To evaluate the robustness of the findings, sensitivity analyses were performed through leave-one-out meta-analyses in Stata version 18.0. 24 Funnel plots and Egger’s regression test were utilized to evaluate potential publication bias for the key outcome. 25
RESULTS
The initial search across nine databases identified a total of 761 articles. Ultimately, after applying screening criteria and assessing eligibility, 14 studies involving 1,056 patients were included in the final meta-analysis (Fig. 1). Among these, 11 studies investigated patients with lower-extremity diabetic ulcers,26–36 whereas 3 studies focused on lower-extremity venous ulcers.37–39 Unfortunately, no eligible RCTs were identified for inclusion in the analysis of chronic pressure ulcers. Most studies were conducted in the United States,26,28–33,35–39 with one study 27 conducted in the United Kingdom and another 34 conducted in Iran.
In the meta-analysis of chronic ulcers, the initial wound size exhibited considerable variation across trials, with average sizes ranging from 0.62 cm2 to 9.48 cm2. Most ulcers involved the dermis, subcutaneous tissue, or tendon; only two studies26,34 reported cases where ulcers extended to the bone. With regard to the types of amniotic membrane utilized, seven studies employed dehydrated human amnion and chorion membrane, four studies used dehydrated human amnion membrane, one study utilized acellular HAM, one applied cryopreserved amnion and chorion membrane, and one implemented hypothermically stored human amnion membrane. In the majority of studies, a screening or run-in period lasting 1–2 weeks was conducted prior to randomization to ensure the eligibility of participants. This intervention was done only when ulcers persisted for more than 4 weeks and exhibited no response to standard wound care protocols. The potential risk of bias, assessed using the RoB 2 tool, was determined to be moderate (Fig. 2). A funnel plot depicting the rate of complete wound closure displayed visual asymmetry, indicating the possibility of publication bias (see Supplementary Fig. S1). To further evaluate the robustness of our findings, a sensitivity analysis was performed using a leave-one-out analysis. However, no significant difference in the overall results was observed (see Supplementary Fig. S2). HAM therapy demonstrated a statistically significant advantage compared with conventional management without HAM (RR = 1.82; 95% CI: 1.48–2.24; I2 = 48%; 14 RCTs, 1,056 patients; moderate-quality evidence; Fig. 3). In addition, no statistically significant difference was found between the two groups regarding wound-related infection rates (RD = −0.05; 95% CI: −0.11 to 0.01; I2 = 0%; 6 RCTs, 552 patients; moderate-quality evidence; Fig. 4). The details of GRADE scoring are reported in Supplementary Table S2.
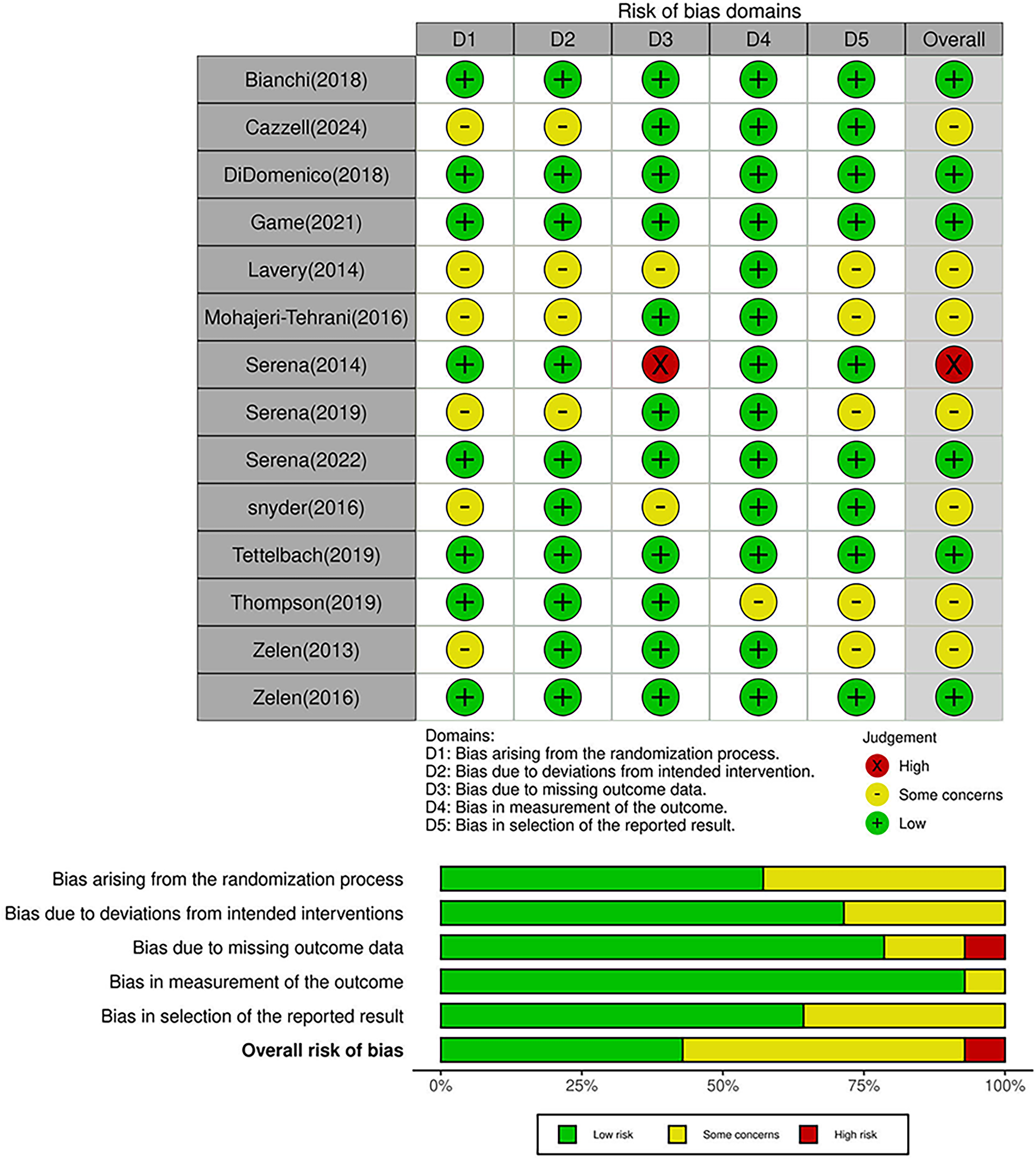
Risk of bias assessment across included studies in chronic ulcers by using Cochrane Collaboration’s Risk of Bias 2.
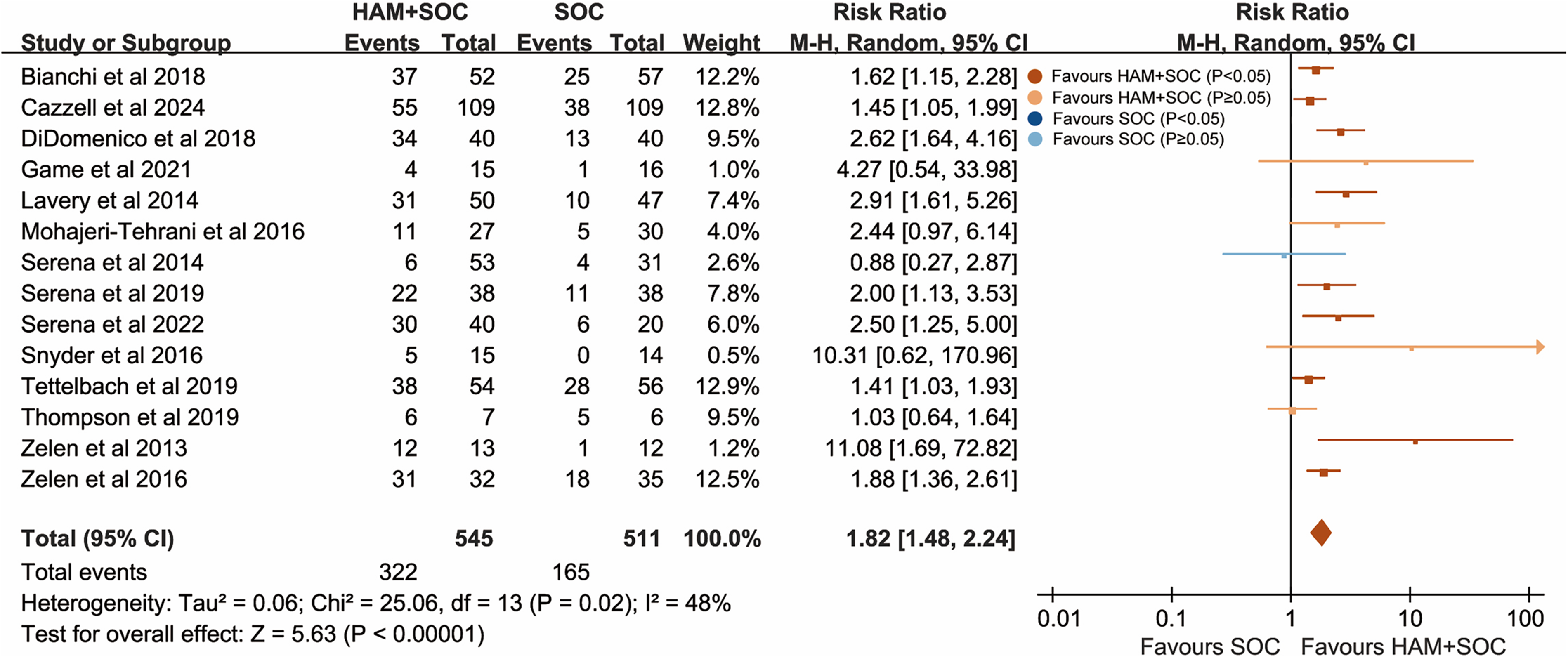
Forest plot of comparisons of ulcer healing rate for combined HAM + SOC treatment versus SOC alone in patients with chronic ulcers. CI, confidence interval; HAM, human amniotic membrane; SOC, standard of care.

Forest plot of comparisons of the number of patients with wound-related infection for combined HAM + SOC treatment versus SOC alone in patients with chronic ulcers.
DFU outcomes
In the evaluation of HAM for the treatment of lower-extremity diabetic ulcers, a total of 803 patients from 11 RCTs were analyzed. The detailed characteristics of each included trial are presented in Table 1. All wounds included in these studies were managed according to the SOC, which consisted of meticulous surgical debridement, moist wound healing techniques, and off-loading strategies. Most of the studies employed dehydrated human amnion and chorion membrane or human amnion membrane only, one study utilized acellular HAM, one applied cryopreserved amnion and chorion membrane, and one hypothermically stored human amnion membrane. Two studies28,29 incorporated total contact cast (TCC) treatment in both intervention and control arms. The majority of studies had a follow-up period of 12 weeks; however, three studies33,34,36 followed patients for 6 weeks, whereas one study 28 extended the follow-up duration to 16 weeks. Most studies employed HAM on a weekly basis, except for two studies27,36 that utilized biweekly applications. Overall, the methodological quality of the included RCTs was moderate, with some risk of bias identified (refer to Supplementary Fig. S3). Nevertheless, the funnel plot exhibited visual asymmetry, and the p values from Egger’s regression test were < 0.05 (p = 0.031), indicating the possibility of publication bias (refer to Supplementary Fig. S4). A sensitivity analysis was conducted by sequentially excluding one study at a time; however, no significant difference was observed in the pooled estimates (refer to Supplementary Fig. S5). The addition of HAM to SOC significantly increased the proportion of complete wound healing at both 6 weeks (RR = 3.02; 95% CI: 2.04–4.47; I2 = 11%; 5 RCTs, 409 patients; moderate-quality evidence; Fig. 5A) and 12 weeks (RR = 1.74; 95% CI: 1.37–2.21; I2 = 54%; 8 RCTs, 692 patients; low-quality evidence; Fig. 5B) compared with SOC alone. Furthermore, the intervention group demonstrated a significantly shorter time required for achieving complete wound closure (MD = −22.09 days; 95% CI: −39.13 to −5.05; I2 = 82%; 4 RCTs, 166 patients; low-quality evidence; refer to Supplementary Fig. S6). One study 29 included TCC treatment in both the HAM group and the SOC group, and an outlier in the HAM group with the longest healing time had multiple comorbidities. After excluding this study, a sensitivity analysis showed the HAM group achieved 31 days faster wound healing compared with conventional treatment, with a significant reduction in heterogeneity (MD = −30.90 days; 95% CI: −39.25 to −22.55; I2 = 0%; 3 RCTs, 155 patients; moderate-quality evidence; refer to Supplementary Fig. S7). Besides, the interventional group had higher rate of achieving more than a 50% reduction in wound area compared with the control group (RR = 2.26; 95% CI: 1.05–4.86; I2 = 71%; 3 RCTs, 158 patients; very low-quality evidence). In the subgroup analyses of lower-extremity diabetic ulcers (Table 2), the ulcer healing rates in the HAM treatment groups were consistently higher than those in the control group, regardless of whether the HAM products were applied on a weekly (low-quality evidence) or biweekly (low-quality evidence) schedule. Similarly, irrespective of whether the HAM products contained both amnion and chorion (moderate-quality evidence) or only amnion (low-quality evidence), the complete healing rates at 6 weeks were significantly higher in the HAM group compared with the SOC group alone. However, no statistically significant difference was observed in the ulcer healing rates at 12 weeks between the HAM group using products composed solely of amnion and the control group (very low-quality evidence). In addition, despite the treatment of more complex and severe ulcers, the HAM group demonstrated a greater proportion of wound healing compared with the control group (moderate-quality evidence).

Forest plot of comparisons of ulcer healing rate for combined HAM + SOC treatment versus SOC alone in patients with lower-extremity diabetic ulcers:
General characteristics of included studies for diabetic foot ulcers
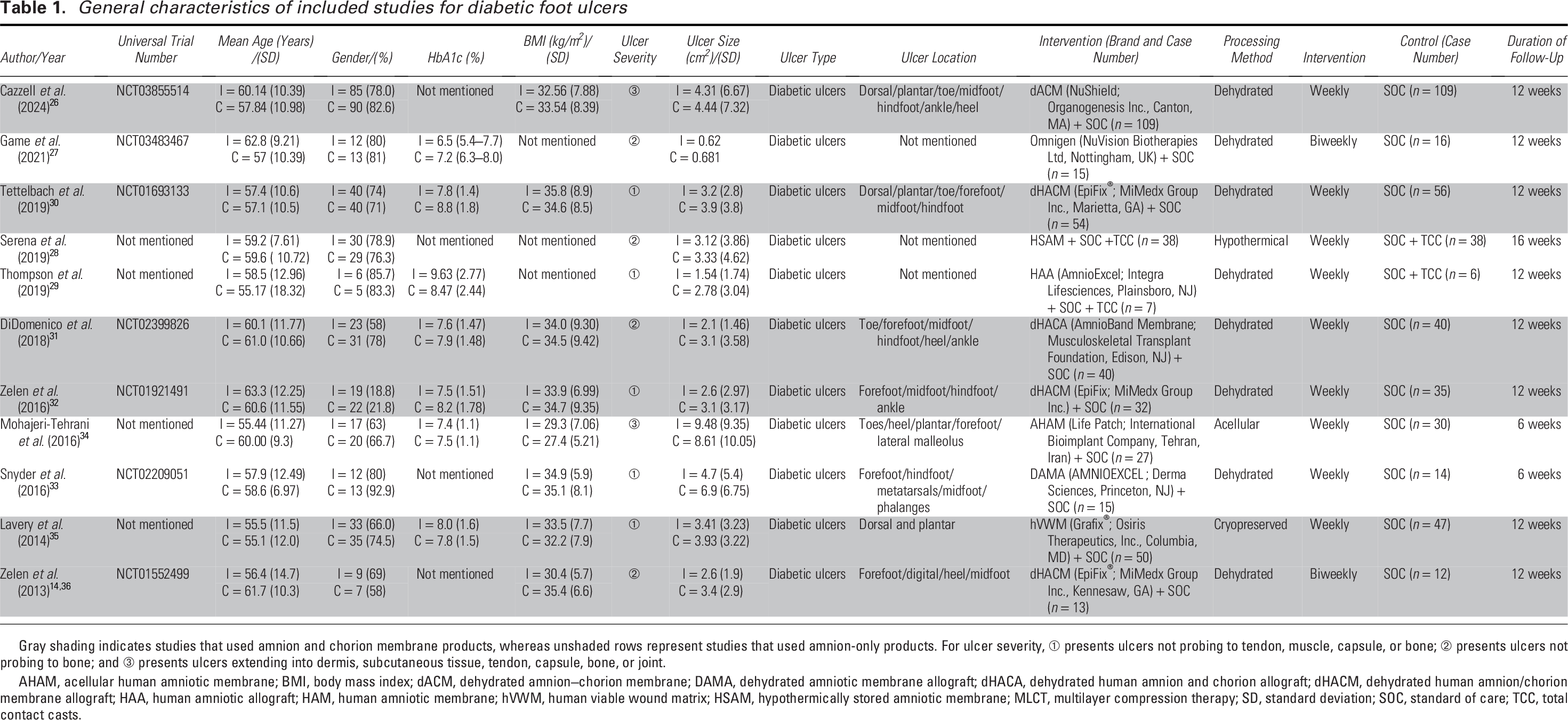
Gray shading indicates studies that used amnion and chorion membrane products, whereas unshaded rows represent studies that used amnion-only products. For ulcer severity, ① presents ulcers not probing to tendon, muscle, capsule, or bone; ② presents ulcers not probing to bone; and ③ presents ulcers extending into dermis, subcutaneous tissue, tendon, capsule, bone, or joint.
AHAM, acellular human amniotic membrane; BMI, body mass index; dACM, dehydrated amnion–chorion membrane; DAMA, dehydrated amniotic membrane allograft; dHACA, dehydrated human amnion and chorion allograft; dHACM, dehydrated human amnion/chorion membrane allograft; HAA, human amniotic allograft; HAM, human amniotic membrane; hVWM, human viable wound matrix; HSAM, hypothermically stored amniotic membrane; MLCT, multilayer compression therapy; SD, standard deviation; SOC, standard of care; TCC, total contact casts.
The final pooled results of subgroup analysis in patients with diabetic foot ulcers
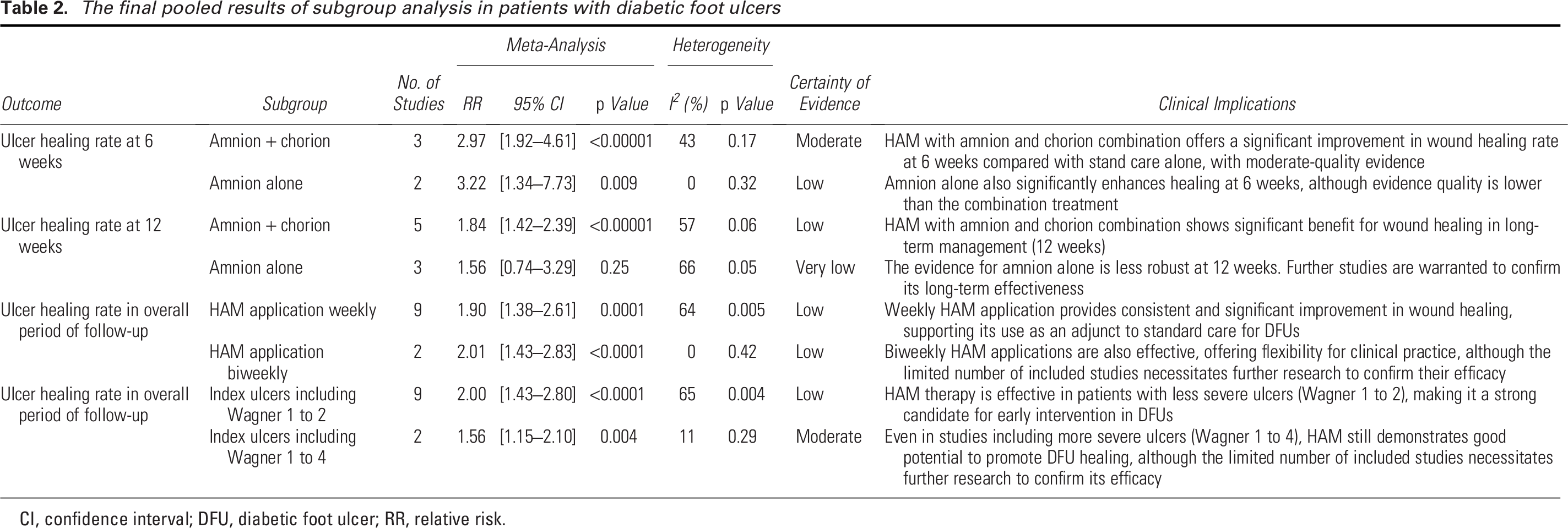
CI, confidence interval; DFU, diabetic foot ulcer; RR, relative risk.
VLU outcomes
In the management of lower-extremity venous ulcers, three RCTs involving a total of 253 patients compared the use of HAM with SOC without HAM. The detailed characteristics of the included trial are presented in Table 3. All included trials received SOC and applied multilayer compression bandages in both treatment arms. In each of the three studies, the HAM group received dehydrated human amnion and chorion membrane. The follow-up durations varied across studies: one study 38 lasted 16 weeks, another 37 for 12 weeks, and a third 39 for 4 weeks. With regard to the assessment of bias risk (see Supplementary Fig. S8), one trial was identified to have a high risk of bias due to missing outcome data. However, sensitivity analyses, which involved excluding one study at a time, did not reveal any significant influence on the overall findings (see Supplementary Fig. S9). Compared with management without HAM, HAM therapy demonstrated a statistically significant improvement in achieving complete wound closure (RR = 1.71; 95% CI: 1.26–2.32; I2 = 19%; 3 RCTs, 253 patients; moderate-quality evidence; Fig. 6).
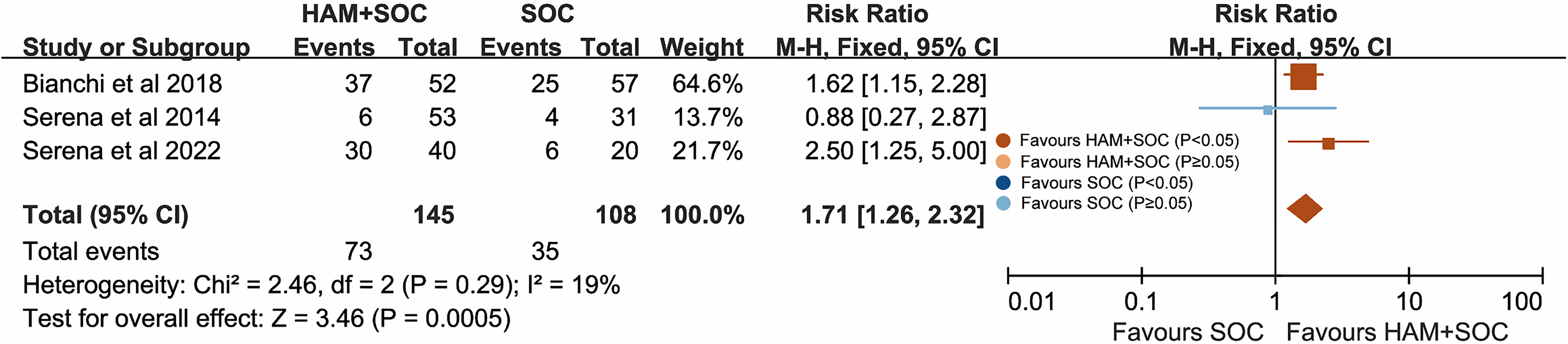
Forest plot of comparisons of ulcer healing rate for combined HAM + SOC treatment versus SOC alone in patients with lower-extremity venous ulcers.
General characteristics of included studies for venous leg ulcers
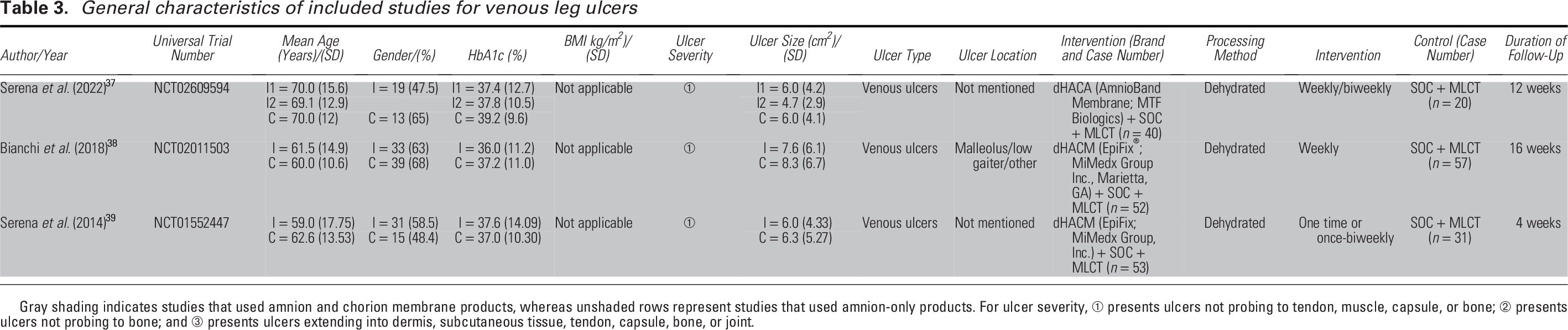
Gray shading indicates studies that used amnion and chorion membrane products, whereas unshaded rows represent studies that used amnion-only products. For ulcer severity, ① presents ulcers not probing to tendon, muscle, capsule, or bone; ② presents ulcers not probing to bone; and ③ presents ulcers extending into dermis, subcutaneous tissue, tendon, capsule, bone, or joint.
Safety profile
No statistically significant difference was observed between the HAM and SOC groups in terms of the incidence of wound-related infections, including cellulitis and osteomyelitis, for both DFUs (RD = −0.06; 95% CI: −0.13 to 0.01; I2 = 0%; 6 RCTs, 408 patients; moderate-quality evidence; Fig. 7) and VLUs (RD = −0.05; 95% CI: −0.16 to 0.07; I2 = 0%; 2 RCTs, 144 patients; low-quality evidence; Fig. 8).

Forest plot of comparisons of the number of patients with wound-related infection for combined HAM + SOC treatment versus SOC alone in patients with lower-extremity diabetic ulcers.

Forest plot of comparisons of the number of patients with wound-related infection for combined HAM + SOC treatment versus SOC alone in patients with lower-extremity venous ulcers.
DISCUSSION
This systematic review evaluated the efficacy and safety of HAM therapy in the treatment of chronic wounds. Our analysis, which encompassed 14 RCTs, demonstrated that HAM therapy was more effective than non-HAM management in promoting complete wound healing (moderate-quality evidence), with no significant differences in the rates of wound-related infections (moderate-quality evidence).
These findings are consistent with those of previous meta-analyses.40–48 However, seven of those meta-analyses specifically focused on patients with DFUs,40–42,44,45,47,48 and six42,44–48 included only relatively early publications. Four40,41,46,48 published meta-analyses incorporated duplicated RCTs,49,50 which may have compromised the validity of their results. One recent meta-analysis failed to include all relevant RCTs. 43 Moreover, one trial incorporated in that analysis compared different administration frequencies of HAM rather than comparing HAM with SOC; nevertheless, it was still included in the pooled analysis. 51 Another recent meta-analysis 41 included two RCTs involving amniotic powder 52 and amniotic gel, 53 respectively, which may potentially increase statistical heterogeneity and limit interpretability and clinical utility. In contrast, we meticulously reviewed the detailed information of all included studies to ensure the exclusion of any duplicate publications. In addition, we incorporated three recent studies26,27,37 involving a total of 309 participants into our analysis, which may enhance statistical power and mitigate the risk of publication bias. Furthermore, we employed the GRADE approach to assess the overall strength of evidence, which had not been considered in prior meta-analyses. A detailed comparison of the current meta-analysis with previous literature is presented in Table, Supplementary Table S3. Chroniculcers hinder the timely and orderly process of tissue repair due to disturbance in the local microenvironment caused by chronic inflammation, cellular senescence, an adverse cytokine milieu, and bacterial colonization. 54 HAM exhibits multifaceted regenerative properties, including the promotion of neovascularization and epithelization, anti-inflammatory and antimicrobial effects, antifibrotic effect, mechanical protection, and low immunogenicity.55–58 The human amnion contains a diverse range of growth factors, such as epidermal growth factor, basal fibroblast growth factor, platelet-derived growth factor, transforming growth factors, nerve growth factor, keratinocyte growth factor, and placental growth factor. 59 These bioactive components play crucial roles in various physiological processes associated with wound healing and tissue regeneration. In addition, human amnion-derived cells, such as human amniotic epithelial cells and human amniotic mesenchymal stem cells, exhibit anti-inflammatory and immunomodulatory properties, which can effectively reduce the levels of proinflammatory cytokines and proteases, thereby alleviating tissue damage. 60 Moreover, the basement membrane and extracellular matrix structures serve as an optimal scaffold, facilitating cell adhesion, proliferation, and differentiation.58,61
For lower-extremity diabetic ulcers, the combination of HAM with SOC demonstrated a significantly higher rate of complete wound closure at 6 weeks (moderate-quality evidence) and 12 weeks (low-quality evidence), and a reduced time (low-quality evidence) to complete healing compared with SOC alone. In subgroup analyses of DFUs, no statistically significant difference was observed in the proportion of complete healing between the once-weekly and biweekly groups, which is consistent with findings from previous RCTs.51,62 For instance, Lavery et al. found no difference in the incidence of healing and time to healing between weekly and biweekly applications of HAM in patients with DFUs. Furthermore, Zelen et al. reported no significant differences in the total number of HMA applications and overall healing rate between the two treatment regimens; however, once-weekly HAM applications resulted in a significantly faster time to healing compared with biweekly application (2.4 weeks vs. 4.1 weeks, p = 0.039). Overall, both weekly and biweekly HAM application regimens for DFUs treatment demonstrated low-quality evidence regarding complete wound healing, whereas the optimal application frequency remains debated. Therefore, further large-scaled and well-powered studies are warranted. The meta-analysis included various commercially available HAM products, which differed in composition and processing methods. These differences may represent key factors influencing the efficacy of HAM products in promoting ulcer healing. 63 Our study indicated that both types of HAM products, despite compositional differences, demonstrated improvements in ulcer healing rates, except for HAM composed solely of amnion, which exhibited no statistically significant difference in healing proportion at 12 weeks compared with the control group. However, among the three studies27–29 exclusively using amnion-based HAM products, two28,29 applied TCCs in both treatment and control arms, whereas the third had a limited sample size; consequently, its finding was assessed as very low-quality evidence. Therefore, no definitive conclusion can be drawn regarding the comparative effectiveness of different HAM products. Although adverse events such as osteomyelitis and cellulitis were reported in some studies, no statistically significant differences were observed between the intervention and control groups (moderate-quality evidence). Impaired diabetic wound healing is primarily attributed to underlying pathophysiological factors, including neuropathy, vascular disease, chronic inflammation, and increased susceptibility to infection. In addition to its antibacterial, anti-inflammatory, and angiogenic properties, HAM has been demonstrated to have the ability to facilitate the proliferation, migration, expression, and secretion of cytokines in diabetic adipose-derived stem cells, thereby promoting diabetic wound healing. 64
VLUs are the most prevalent cause of lower-extremity ulceration and are typically characterized by prolonged healing periods and a high recurrence rate. 65 In our meta-analysis, which encompassed three RCTs on VLUs, HAM therapy exhibited significant efficacy in achieving complete wound closure compared with management approaches without HAM (moderate-quality evidence). Furthermore, no statistically significant difference was observed between the two groups in terms of the incidence of wound-related infections (low-quality evidence). VLUs are associated with elevated levels of proinflammatory cytokines, such as interleukin (IL)-1α, IL-1β, tissue necrosis factor, and increased protease activity, including matrix metalloproteases (MMPs) and serine proteases. HAM plays a role in modulating the balance between tissue degradation/regeneration homeostasis by upregulating potent inhibitors of MMPs, such as tissue inhibitor of metalloproteinases-1, type-1 plasminogen activator inhibitor, and thrombospondin-1. This mechanism contributes to the mitigation of inflammatory responses and the improvement of the microenvironmental conditions that are crucial for the healing of chronic venous ulcers.65,66
To the best of our knowledge, this meta-analysis represents a comprehensive and systematic update that incorporates all currently available studies on the most prevalent types of chronic ulcers. In comparison to other studies focusing on specific etiologies of chronic wounds, our study provides a more systematic and comparable understanding of the effects of amniotic membrane across various types of chronic wounds. Furthermore, we meticulously verified the UTN and other relevant details in each included article to ensure the exclusion of duplicate publications and to minimize potential biases associated with multiple publications. The risk of bias of included studies and the certainty of evidence for all outcomes in the meta-analyses were fully assessed. The overall quality of the included RCTs was assessed as moderate, indicating a reasonable strength of evidence. In addition, sensitivity analyses were performed to evaluate the robustness and stability of the pooled results.
Our findings, which demonstrate enhanced healing rates (RR = 3.02 at 6 weeks for DFUs; RR = 2.03 for VLUs) and a safety profile, provide moderate-quality evidence indicating that HAM can be integrated as an adjunctive therapy for chronic lower-extremity ulcers unresponsive to standard care. Incorporating HAM into evidence-based wound management guidelines may contribute to standardizing its clinical application and optimizing patient selection. From a reimbursement standpoint, these results support the consideration of HAM for conditional or value-based coverage, as its utilization may reduce long-term costs by shortening the healing period and decreasing complication rates. However, further large-scale and cost-effectiveness studies are warranted prior to widespread policy implementation.
Some limitations of this meta-analysis should also be acknowledged. First, although all available studies were included, the total sample sizes remained relatively small, thereby limiting certain analyses such as evaluating the impact of product processing on ulcer healing. In addition, the assessment of the cost-effectiveness of HAM for chronic wounds is limited by insufficient data and substantial heterogeneity across studies. Nevertheless, several studies on cost-effectiveness have indicated that the adjunctive use of HAM with SOC results in lower costs and improved quality-adjusted life years (QALYs). For example, Carter et al. 67 reported that the incremental cost-effectiveness ratio for dehydrated human amniotic chorion allograft (dHACA) compared with SOC in the treatment of Wagner 1 DFUs was −$4,373, suggesting that dHACA is highly cost-effective. Similarly, Guest et al. 68 proposed that if the cost of dHACA were ≤£3,250 per ulcer, treating nonhealing DFUs with adjunctive dHACA, rather than SOC, would break even and have a 0.95 probability of being cost-effective at the £20,000 per QALY threshold. Second, the majority of participants were recruited from the United States and exhibited milder ulcer severity, which may restrict the generalizability of our findings to more diverse populations. In addition, variations in HAM product types and application frequencies across studies might have influenced the observed outcomes. However, consistent subgroup analyses showed higher wound healing rates in the HAM group compared with the control group, regardless of differences in application frequency and baseline ulcer severity. In addition, no studies focusing on pressure ulcers met the inclusion criteria, suggesting that the current findings may not be generalizable to this specific type of wound. Finally, the maximum follow-up duration across the included studies was 16 weeks, which may be inadequate for evaluating the long-term clinical efficacy or recurrence rates associated with HAM therapy.
CONCLUSIONS
The present meta-analysis of RCTs demonstrates that HAM therapy significantly enhances wound healing and presents a favorable safety profile compared with non-HAM managements in patients with chronic lower-extremity diabetic ulcers and venous ulcers. Nevertheless, the current evidence is constrained by the limited number of adequately powered RCTs and variability in study designs. Further high-quality RCTs employing rigorous methodologies with minimized bias are warranted to assess the relative efficacy of HAM products, determine optimal application frequencies, and evaluate long-term outcomes through extended follow-up periods.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The present study was financially supported by the Health Commission of Sichuan Province (Grant No. 23LCYJ042), the Science and Technology Bureau of Sichuan Province (Grant No. 2024YFFK0290), the 1.3.5 Project of Center for High Altitude Medicine, West China Hospital, Sichuan University (Grant No. GYYX24002), and the 1.3.5 Project for Disciplines of Excellence, West China Hospital, Sichuan University (Grant No. ZYGD24005).
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare no competing financial interests to disclose. The content of this article was independently developed and authored by the listed individuals, without any form of ghostwriting or external editorial assistance.
ABOUT THE AUTHORS
DATA AVAILABILITY
The authors confirm that data are available upon reasonable request.
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.