
Abstract
Significance:
Chronic wounds remain a major global health burden and often stall despite guideline-based care because of persistent inflammation, oxidative stress, impaired perfusion, and dysregulated extracellular matrix remodeling. Protein-based nutrition is best positioned as an adjunct to, rather than a substitute for, standard wound care.
Recent Advances:
Human studies, supported by mechanistic rationale, suggest that optimizing total protein intake (commonly ∼1.25 to 1.5 g/kg/day in appropriate patients) and, in selected settings, adding functional components such as arginine, glutamine, and β-hydroxy-β-methylbutyrate (HMB) may improve wound-area reduction and healing trajectories when integrated with standard care. Reported signals vary by etiology, including improved wound-area reduction and Pressure Ulcer Scale for Healing outcomes in pressure injuries, possible benefit in selected high-risk diabetic foot ulcer subgroups, and reduced venous ulcer area when supplementation is paired with consistent compression.
Critical Issues:
Evidence remains heterogeneous across wound types and study designs, with inconsistent dosing, duration, endpoints, and patient-selection criteria that limit standardized implementation. Safety and feasibility are especially important in renal risk and diabetes, where renal function and glycemic control require monitoring. Clinical evidence was interpreted with attention to study design and reporting standards, including CONSORT, STROBE, or STARD, as applicable.
Future Directions:
This review translates current evidence into a clinician-oriented framework for patient selection, prescribing, monitoring, and treatment adjustment, emphasizing initiation triggers in stalled wounds and trajectory-based reassessment every 2–4 weeks. Future work should prioritize pragmatic, well-controlled trials comparing formulations and dosing windows by wound etiology, together with biomarker-informed stratification to improve personalization, safety, and real-world uptake.
Keywords
INTRODUCTION
Scope of review and significance
Chronic wounds are a growing global health burden and often fail to progress despite guideline-based care because of persistent inflammation, oxidative stress, impaired perfusion, and dysregulated extracellular matrix (ECM) remodeling. This review frames protein-based nutrition as a co-intervention within comprehensive wound care and synthesizes mechanistic and clinical evidence to clarify its practical role across major chronic wound etiologies.
Qilong Chen, PhD

Bin Li, PhD

Translational relevance
Experimental and translational studies support the biological plausibility that protein and functional amino acids influence immune regulation, redox balance, angiogenesis, and matrix remodeling in chronic wounds. By integrating these mechanistic insights with human clinical signals, this review supports more practical and risk-informed nutritional prescribing.
Clinical relevance
Patients with chronic wounds frequently have inadequate protein intake, catabolic stress, or malnutrition risk, and clinical studies suggest that protein-based regimens may improve wound trajectory when used alongside etiology-specific standard care. This review provides a clinician-oriented framework for patient selection, prescribing, monitoring, and treatment adjustment in common comorbid settings.
Chronic wounds are commonly defined as wounds that persist for more than 12 weeks or fail to achieve a 20–40% reduction in surface area after 2–4 weeks of standard treatment,1–3 reflecting impaired progression through the canonical phases of hemostasis, inflammation, proliferation, and remodeling.4–7 These wounds affect approximately 1–2% of the global population and impose a substantial economic burden, with annual health care expenditures estimated at $28.1–96.8 billion in the United States and £8.3 billion in the United Kingdom.8,9 Despite heterogeneous etiologies, they share common pathological features, including persistent inflammation, oxidative stress, and ECM degradation.4,10–12
Protein-based nutritional interventions in chronic wound care extend beyond intact dietary protein to include specific amino acids and protein-derived metabolites with immunometabolic functions.13,14 These approaches have been investigated for their potential to support immune regulation, redox balance, angiogenesis, and ECM remodeling, particularly in patients with catabolic stress, metabolic dysfunction, and impaired nutrient utilization.4,7,15 Clinical and preclinical studies suggest that such interventions may favorably influence wound repair, although uncertainties remain regarding patient selection, composition, timing, and safety, especially in the setting of renal dysfunction, diabetes, and chronic metabolic inflammation.13,14,16–22 Accordingly, this review synthesizes current evidence and presents a pragmatic implementation framework for protein-based nutrition in chronic wound care.
EVIDENCE IDENTIFICATION AND SCOPE
This clinician-oriented narrative review prioritized human randomized trials, prospective studies, and guideline statements on protein- and amino acid–enriched supplementation in major chronic wound etiologies. Evidence was identified primarily through PubMed/MEDLINE, Embase, and Google Scholar (last updated February 2026), with additional screening of reference lists from eligible trials, prior reviews, and relevant guidelines. Mechanistic and preclinical studies were included only to support biological plausibility. As this work was not designed as a systematic review or meta-analysis, formal PRISMA reporting was not applied. Key human studies are summarized in a trial-at-a-glance table, including intervention composition, duration, endpoints, and safety signals.
HUMAN EVIDENCE SIGNAL
Human studies suggest that protein-based nutritional interventions may improve healing trajectories across major chronic wound etiologies. In pressure injuries, diabetic foot ulcers (DFU), and venous leg ulcers, clinical studies have reported improvements in wound area reduction, Pressure Ulcer Scale for Healing (PUSH) scores, prealbumin, or inflammatory markers following arginine- and antioxidant-enriched or protein-rich supplementation.15,23,24 In elderly patients with refractory pressure injuries, prolonged supplementation with β-hydroxy-β-methylbutyrate (HMB), arginine, and glutamine for ≥20 weeks shortened median healing time despite no parallel improvement in PUSH scores. 25 Overall, these studies support protein-based nutrition as a co-intervention within standard wound care, although effects vary by etiology, baseline risk, treatment duration, and endpoint selection (Fig. 1).
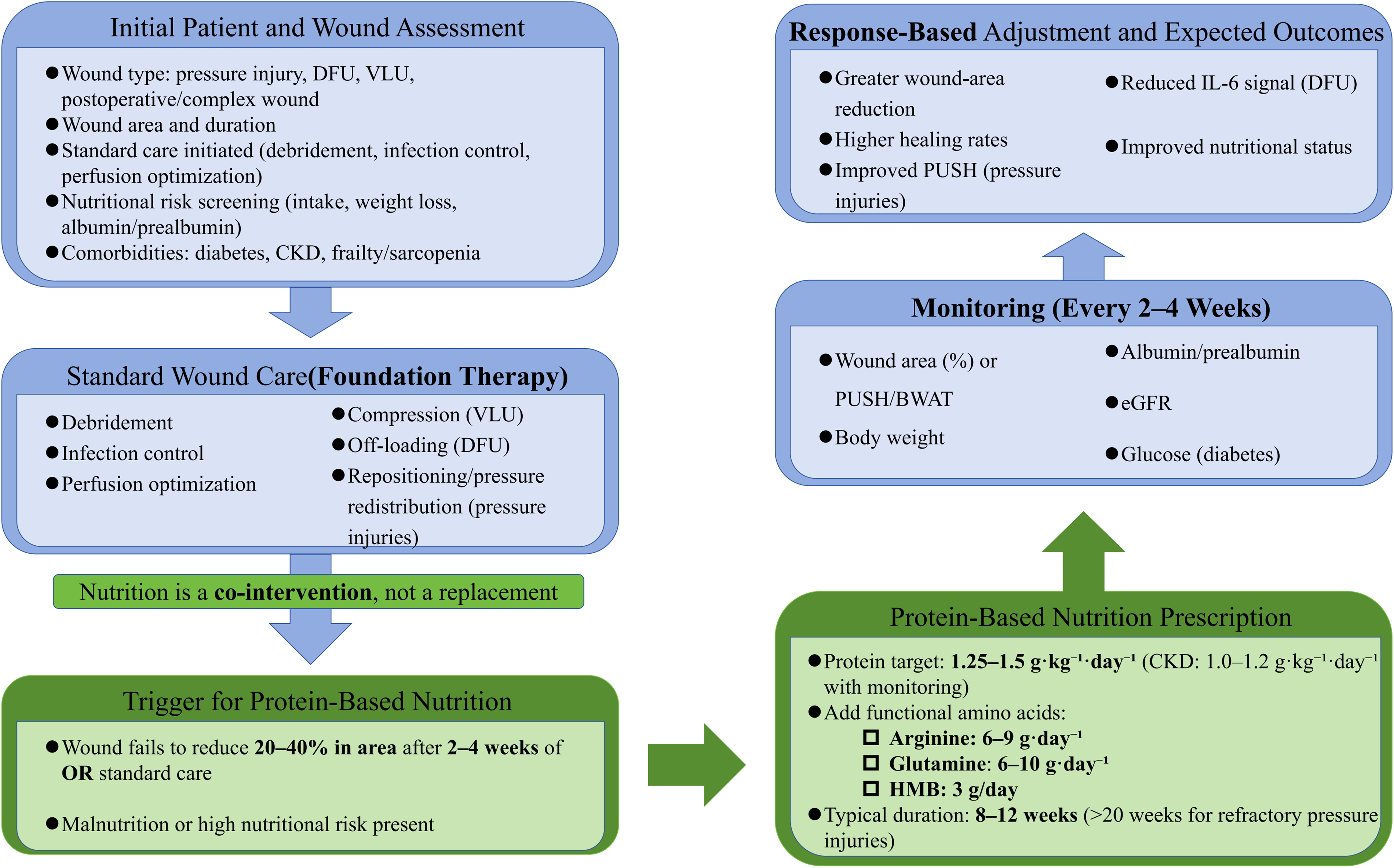
Where protein-based nutrition fits in standard wound care. Figure 1 presents a bedside workflow integrating protein-based nutrition as an adjunct within guideline-based wound care: assessment and standard modalities first, initiation triggered by stalled healing trajectory and/or malnutrition risk, followed by regimen selection and trajectory-based monitoring with safety guardrails to guide adjustment or discontinuation.
PATIENT SELECTION AND TRIAGE
Protein-based nutritional interventions should be considered as a co-intervention in patients with chronic wounds that fail to progress despite guideline-based standard care. 4 A practical trigger for initiation is failure to achieve a 20–40% reduction in wound area within 2–4 weeks, a threshold commonly used to identify wounds at risk for chronicity.4–7 Triggers and downstream steps are outlined in Figure 1. Patients with laboratory or clinical features suggestive of impaired nutritional status, including low serum albumin or prealbumin, are a priority group for nutritional assessment and intervention.13,15,24
Host-related factors further refine triage. Older adults with chronic wounds commonly require nutritional support within comprehensive wound management. 17 Patients with chronic kidney disease require dose individualization and renal monitoring because higher protein exposure may accelerate renal decline.21,22 In DFU, protein- and amino acid–enriched supplementation has been evaluated in randomized trials, and glycemic monitoring is advisable, particularly in poorly controlled diabetes.13,23
Accordingly, triage may be approached stepwise: confirm adequate implementation of standard wound care, assess wound response at 2–4 weeks, evaluate nutritional status using available clinical and laboratory markers, and select standard or modified regimens according to renal function and metabolic risk, with a defined monitoring cadence (Table 1).26–28
Eligibility and Caution Checklist for Protein-Based Nutrition in Chronic Wounds
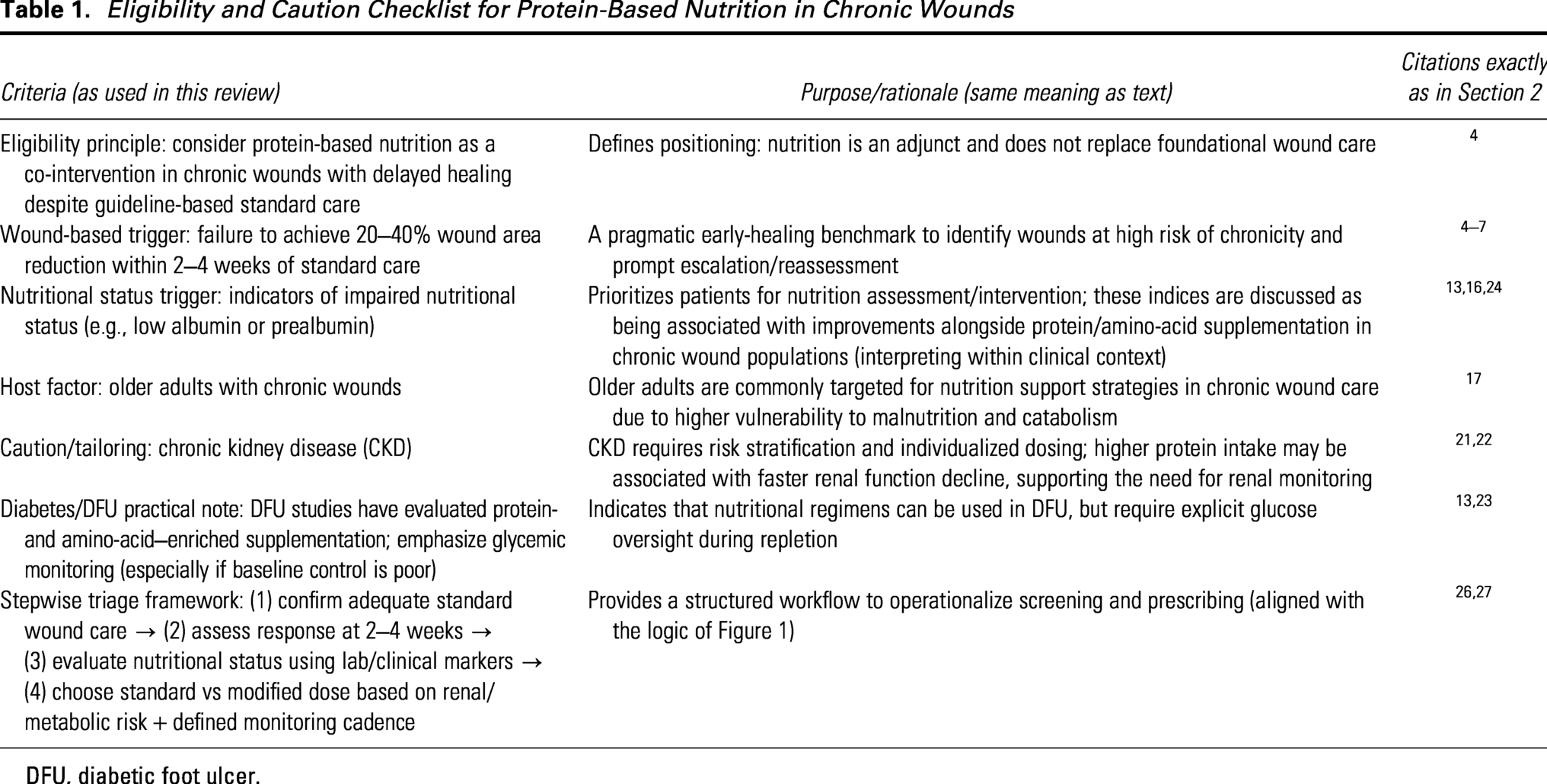
DFU, diabetic foot ulcer.
REGIMENS BY WOUND ETIOLOGY (WHAT TO PRESCRIBE)
Chronic wounds differ in metabolic demands and barriers to repair; accordingly, protein-based regimens should be tailored to wound etiology, metabolic status, renal function, and healing stage. Etiology-specific prescribing considerations are summarized below, with dosing and monitoring consolidated in Table 2 and Figure 1.
Regimens by Wound Type (Prescriber-Ready)
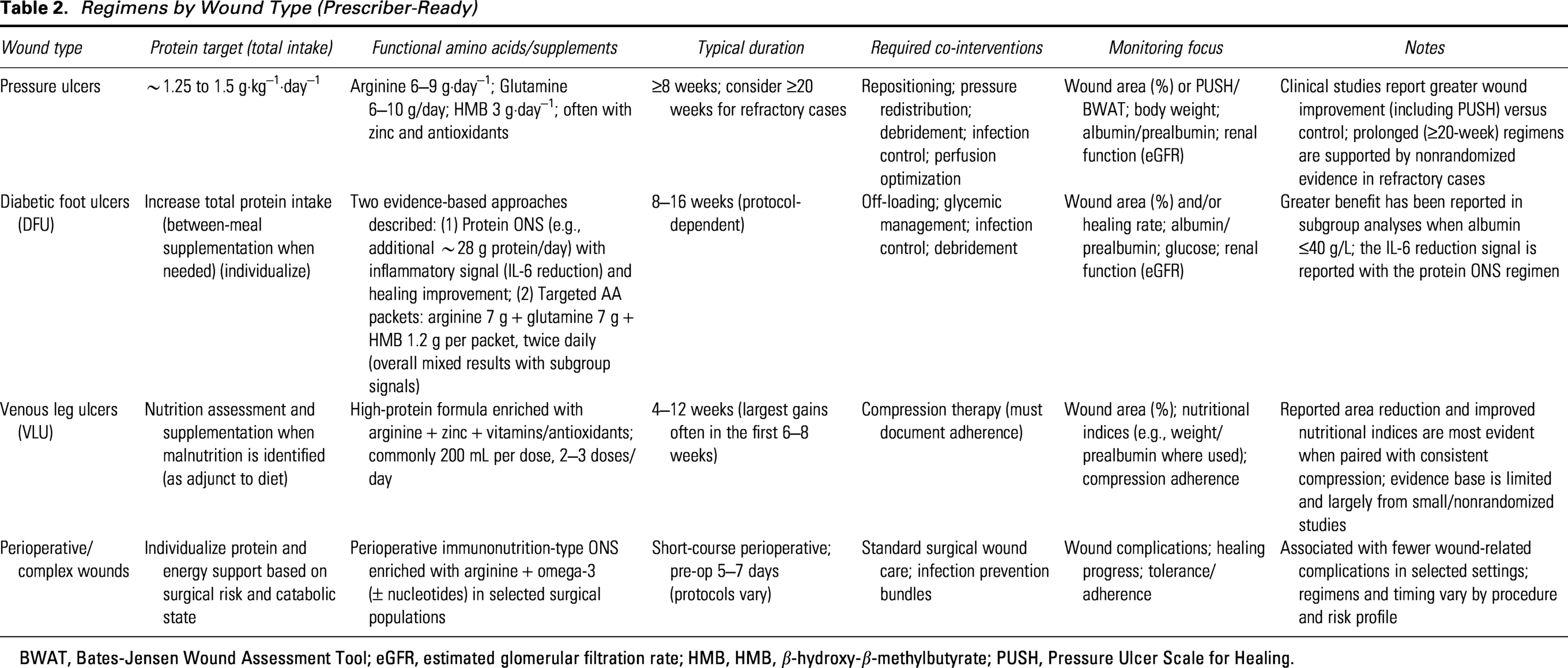
BWAT, Bates-Jensen Wound Assessment Tool; eGFR, estimated glomerular filtration rate; HMB, HMB, β-hydroxy-β-methylbutyrate; PUSH, Pressure Ulcer Scale for Healing.
Pressure ulcers
Clinical evidence supports high-protein oral nutritional formulas enriched with functional amino acids and antioxidant micronutrients as an adjunct to comprehensive pressure injury management, particularly in malnourished and older adults. 2 Guideline-based practice commonly targets approximately 1.25–1.5 g/kg/day of protein, often delivered through arginine-, zinc-, and antioxidant-enriched formulas. 22 In malnourished adults with stage II–IV pressure ulcers, a multicenter randomized, controlled, blinded trial showed that 8 weeks of an energy-dense, high-protein oral supplement (2 bottles/day; 400 mL/day providing 500 kcal and 40 g protein) enriched with arginine (≈6 g/day), zinc, and antioxidants resulted in a greater mean percentage reduction in ulcer area than an isocaloric, isonitrogenous control and a higher proportion of patients achieving ≥40% area reduction at week 8. 15 In elderly patients with refractory pressure ulcers, prolonged supplementation with HMB, arginine, and glutamine for ≥20 weeks shortened median healing time despite no parallel improvement in PUSH scores. 25 In addition, 8 weeks of arginine-, zinc-, and antioxidant-enriched high-protein nutrition was associated with reductions in wound area and tissue redox potential, supporting a possible link between local redox modulation and improved healing. 15
Diabetic foot ulcers
In DFU, randomized clinical studies suggest that higher protein intake and amino acid–enriched formulas may improve inflammatory signaling and support wound healing when used alongside optimized standard care. 1 In a 12-week randomized trial, a diabetes-specific oral supplement providing additional energy and protein reduced plasma interleukin 6 (IL-6), whereas CRP and interleukin 10 (IL-10) were unchanged. 23 In a multicenter double-blind RCT, an arginine-, glutamine-, and HMB-containing formulation did not improve overall healing rates or time to healing at 16 weeks, but post hoc analyses suggested greater benefit in predefined high-risk subgroups, including patients with albumin ≤ 40 g/L. 13 Overall, the DFU nutrition literature remains heterogeneous in both interventions and endpoints, but available evidence suggests that benefit is most likely when nutritional strategies are targeted to patients with greater nutritional or perfusion-related risk and delivered as an adjunct to optimized DFU care.13,23,29
Venous leg ulcers (VLU)
Clinical data suggest that protein-based oral nutritional supplementation enriched with arginine and antioxidants may improve healing trajectories and nutritional indices in patients with venous leg ulcers. In practice, the Society for Vascular Surgery and the American Venous Forum recommend nutritional assessment in patients with venous leg ulcers who show evidence of malnutrition, with supplementation provided when malnutrition is identified. 3 In a 4-week before–after clinical trial, a high-calorie, high-protein formula enriched with arginine, zinc, and antioxidant vitamins was associated with reduced wound area and improved PUSH scores, whereas fasting glycemia, serum albumin, and C-reactive protein (CRP) were unchanged. 24 In a 12-week prospective study combining professional wound care, specialized dressings, and an arginine-, zinc-, and vitamin-enriched oral formula, complete healing was observed in 6 of 35 patients, and median ulcer area decreased substantially; the greatest improvement in healing and prealbumin was seen during the first 6–8 weeks. 30 Evidence syntheses further suggest that nutritional status may interact with compression-based care. A systematic review including 12 studies and 631 patients found that energy- and protein-containing supplements were commonly used alongside compression modalities, with overall nutritional status associated with improved healing, although effects varied by compression type and related parameters. 31 High-quality trial evidence remains limited, however, and further randomized studies are needed to define optimal formulations and patient selection. 32
Perioperative and complex wounds
Evidence from broader clinical settings supports a role for immunonutrition-type oral supplements in perioperative and complex wound care. In perioperative surgery, short-course formulas enriched with arginine and omega-3 fatty acids, often with nucleotides, have been associated with reduced postoperative infectious morbidity. The 2025 ESPEN guideline recommends 5–7 days of preoperative immunonutrition for gastrointestinal cancer surgery, citing meta-analytic evidence for fewer infectious complications and shorter length of stay. 33 Consistently, a 2024 meta-analysis reported reductions in infectious complications and anastomotic leakage in oncology surgery, although effects on length of stay appear variable across procedures and protocols.34,35 High-protein oral nutrition support has also been associated with fewer postoperative or wound-related complications and improved recovery in selected surgical cohorts. 36 A systematic review identified 28 clinical studies of oral nutritional supplements for wound-related outcomes; formulations commonly included arginine, omega-3 fatty acids, and antioxidant micronutrients, with the most consistent signals observed for reduced complications and shorter hospitalization in surgical populations. 37 In addition, a single-blind crossover trial under acute sleep restriction showed that higher protein intake combined with multinutrient supplementation shortened skin barrier restoration time, supporting a role for targeted nutrition under physiological stress.37–39 For atypical or refractory ulcers, nutritional plans should be individualized and integrated with reassessment of vascular status, infection or bioburden control, and other systemic drivers. 40
DOSING, FORMULATIONS, AND ORDER SETS
Practical formulation selection based on clinical evidence
Across chronic wound studies, protein-based strategies have most commonly used oral nutritional supplements enriched with functional amino acids and antioxidant micronutrients rather than intact protein alone. In pressure ulcers, arginine-, zinc-, and antioxidant-enriched high-protein formulas have improved wound area reduction in randomized studies. 15 In DFU, protein-rich and amino acid–enriched formulations containing arginine, glutamine, and HMB have shown signals for inflammatory biomarker modulation and possible benefit in selected high-risk subgroups.13,23,29 In venous leg ulcers, arginine- and micronutrient-enriched high-protein supplements given alongside compression-based care have been associated with reduced wound area and improved wound scores. 24 In perioperative and complex wound settings, immunonutrition formulas enriched with arginine and omega-3 fatty acids, often with nucleotides, have guideline-supported employ in oncology surgery.33–35
Duration of supplementation in clinical studies
Supplementation duration varies by wound etiology and clinical context. In venous leg ulcers, studies have commonly evaluated approximately 4 weeks of supplementation. 24 In DFU, randomized trials have generally evaluated supplementation over 12–16 weeks, including 12-week protocols and 16-week double-blind supplementation studies.13,23 In refractory pressure ulcer cohorts, prolonged supplementation for ≥20 weeks with HMB-, arginine-, and glutamine-containing regimens has been associated with shorter time to healing. 25 These observations suggest that duration should be individualized according to wound chronicity, response trajectory, and tolerability.
Amino acid components used in clinical formulations
Clinical studies have most commonly evaluated arginine-enriched formulations, with selected protocols also incorporating glutamine and HMB (Fig. 2). Arginine–glutamine–HMB combinations have been tested most directly in DFU and slow-healing or refractory wound cohorts, with heterogeneous overall results but signals of benefit in selected subgroups and longer-duration regimens.13,25 In pressure ulcers, arginine-centered immunonutrition formulas enriched with antioxidant micronutrients have demonstrated improved wound area reduction in randomized trials. 15
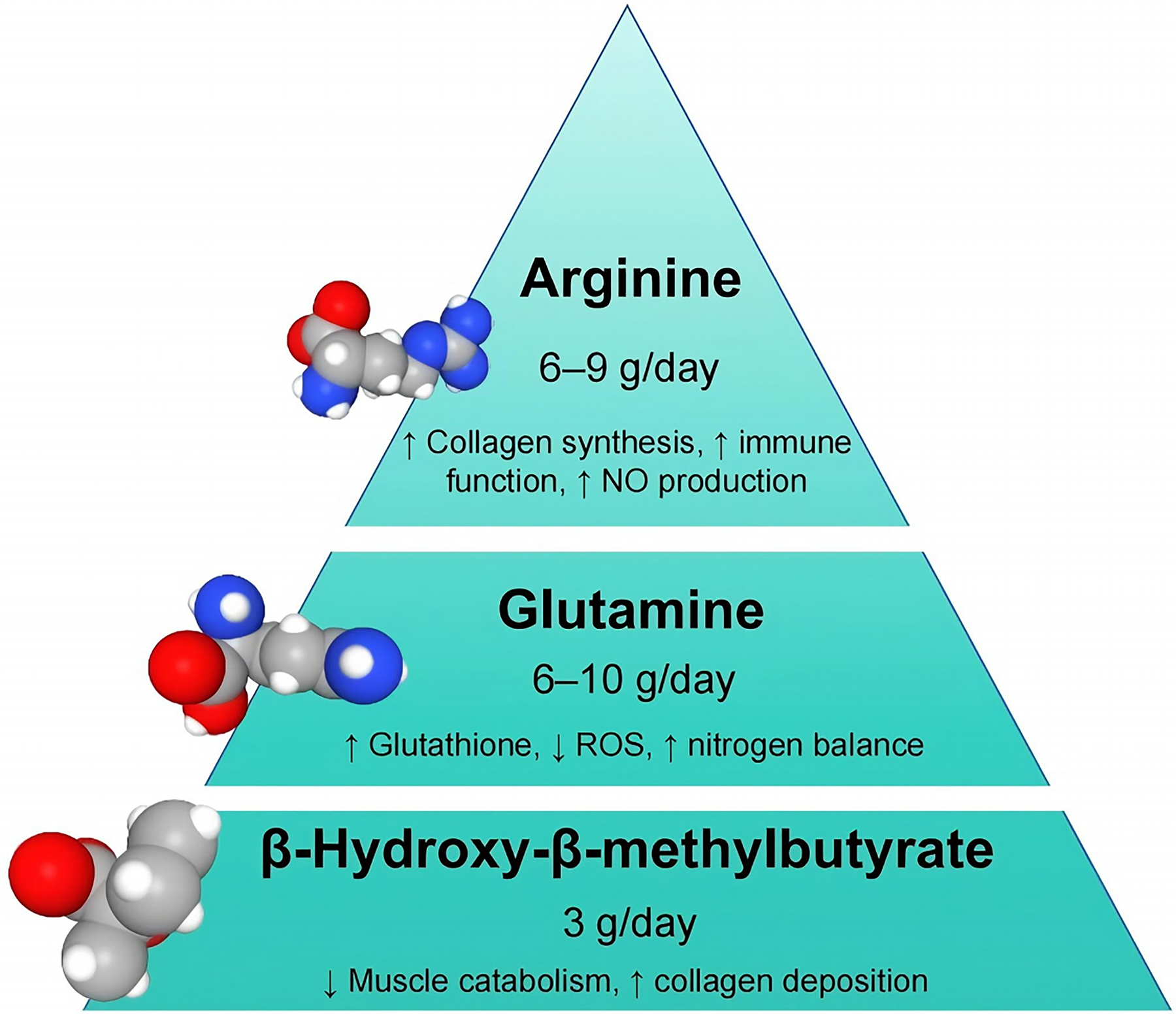
Targeted amino-acid supplementation: core components and rationale. This figure summarizes commonly used targeted components in protein-based nutrition for chronic wounds, highlighting arginine, glutamine, and HMB as recurrent ingredients in studied formulas. Mechanistic support links arginine to nitric oxide–related perfusion and collagen synthesis, glutamine to glutathione/redox homeostasis and nitrogen economy, and HMB to anti-catabolic support.
MONITORING, SAFETY, AND STOPPING RULES
Monitoring and safety are central to implementing protein-based nutrition as an adjunct in chronic wound management. Across clinical studies, response has most often been assessed using wound area change, PUSH scores, healing endpoints, and selected nutritional or inflammatory indices.13,15,23–25,29 Because comorbidities and metabolic risk vary substantially, supplementation should be individualized and reassessed at predefined intervals, particularly in patients with diabetes, advanced age, or renal dysfunction. Practical monitoring items, safety guardrails, and scenario-based adjustments are summarized in Table 3.
Safety and Scenario-Based Adjustments for Protein-Based Nutrition in Chronic Wound Care
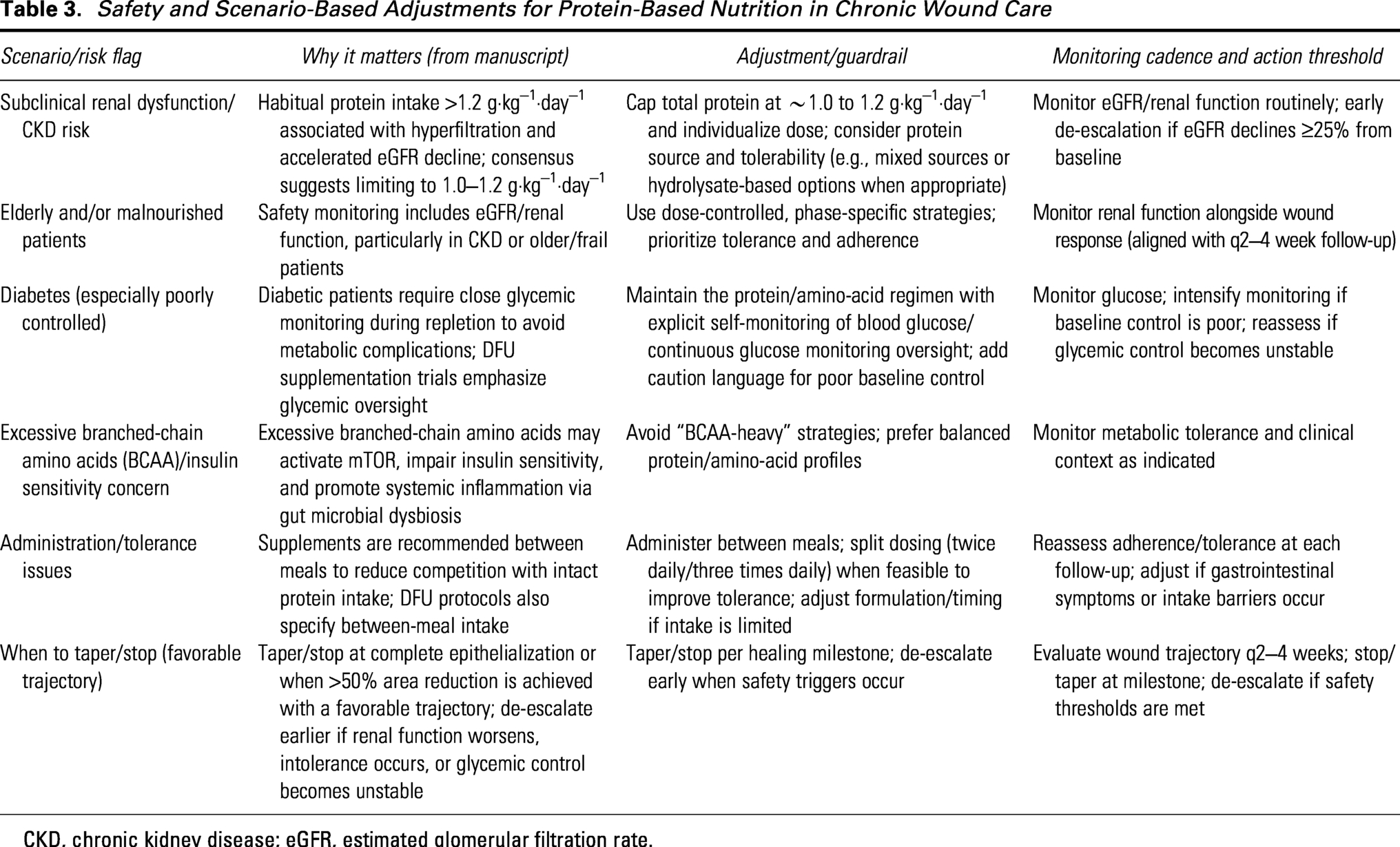
CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate.
What to monitor and when (pragmatic cadence)
A practical reassessment cadence is every 2–4 weeks, aligned to routine wound clinic follow-up. At each visit, clinicians should document:
Wound response: wound area change by standardized measurement/planimetry and/or PUSH/Bates-Jensen Wound Assessment Tool, with trajectory used to guide continuation versus escalation of standard care. Nutrition status: body weight or body mass index (BMI) trend, intake, and adherence; albumin or prealbumin may be followed as supportive indices but should be interpreted in clinical context. Key co-interventions: adherence to compression (VLU), off-loading (DFU), pressure redistribution/repositioning (pressure injuries), and indicated debridement or infection control. Safety parameters: estimated glomerular filtration rate (eGFR)/renal function, glycemic control in diabetes, and tolerance, including gastrointestinal symptoms.
Safety guardrails (renal risk, diabetes, and metabolic context)
Renal impairment. Higher habitual protein intake above approximately 1.2 g/kg/day has been associated with hyperfiltration and faster eGFR decline in individuals with subclinical renal dysfunction. 21 In patients with kidney risk, expert guidance supports dose individualization, consideration of approximately 1.0–1.2 g/kg/day, and routine renal monitoring. 22
Diabetes and metabolic inflammation. During nutritional repletion, patients with diabetes require close glycemic monitoring to reduce metabolic destabilization. 41 Excess branched-chain amino acid exposure may also promote mTOR activation, impair insulin sensitivity, and contribute to systemic inflammation.20,42 Dose and phase specificity. Preclinical data suggest that prolonged high-protein feeding may delay wound closure and induce organ hypertrophy despite preserved body weight, supporting phase-specific and dose-controlled strategies rather than indiscriminate escalation. 43
Tolerance and implementation (start-low/go-slow)
Gastrointestinal tolerance is a practical barrier, particularly with energy-dense or immunonutrition-type formulations. Meta-analytic evidence in oncology surgery suggests that immunonutrition is unlikely to increase nutrition-related adverse events overall, although guidelines note that immediate advancement to goal enteral feeding may be associated with more intolerance than gradual advancement.33,34 A start-low/go-slow approach with symptom-triggered adjustment may therefore improve adherence and reduce interruptions.
Putting it into practice (individualization)
To maximize benefit and minimize harm, regimens should be aligned with renal function, glycemic status, and overall nutritional reserve (Table 3). In kidney dysfunction, protein intake should generally remain individualized and paired with routine eGFR monitoring, whereas metabolically stable but malnourished patients may benefit from short-term support within guideline-based protein targets. Mixed protein strategies and hydrolyzed formulations may improve tolerability and bioavailability, although stronger comparative evidence is still needed.
Box 1. Stopping and taper rules (pragmatic)
Stop targeted supplementation at complete epithelialization/closure.
Consider tapering once a favorable healing trajectory is established, such as >50% wound-area reduction with continued improvement at the next reassessment (typically within 2–4 weeks).
De-escalate or stop early if eGFR declines ≥25% from baseline, intolerable gastrointestinal adverse effects occur, or glycemic control becomes unstable despite monitoring and adjustment.
Maintain standard wound care throughout, including wound-type–specific measures such as compression (VLU) and off-loading (DFU) as indicated.
IMPLEMENTATION IN CLINICAL PATHWAYS
Protein-based nutrition should be implemented as an adjunct within comprehensive wound care, alongside wound-type–specific standard measures such as compression for venous leg ulcers, off-loading for DFU, and pressure redistribution for pressure injuries.1,3,44 A pragmatic workflow includes nursing screening for trigger criteria and malnutrition risk, dietitian assessment of protein needs, and clinician prescription of etiology-aligned supplementation with renal and glycemic safeguards, followed by reassessment every 2–4 weeks using standardized wound metrics and adherence to key co-interventions.15,24
Implementation may be supported by structured EHR documentation of wound response, nutrition status, and safety monitoring, including renal function, glycemic control, and tolerance/adherence.15,23,24 Consistent documentation of these fields, together with key co-interventions such as compression or off-loading adherence, supports reproducible reassessment across care settings.1,3 Patient education should reinforce daily protein goals, supplement administration, adherence to co-interventions, red-flag symptoms, and follow-up plans, with practical supports such as smaller-volume or energy-dense formulations, integration into daily routines, and simple intake tracking.3,13,22–24,39,45–49
MECHANISTIC SUPPORT AND THERAPEUTIC IMPLICATIONS
Inflammation and immune regulation
Persistent inflammation in chronic wounds reflects failed immune resolution rather than an amplified acute response. Prolonged infiltration of M1-polarized macrophages and neutrophils, sustained elevation of pro-inflammatory cytokines such as tumor necrosis factor–α (TNF-α), IL-6, and interleukin 1 beta (IL-1β), and excessive formation of neutrophil extracellular traps establish a self-perpetuating inflammatory microenvironment that impairs transition to tissue repair.4,50 Excess reactive oxygen species (ROS), generated through mitochondrial dysfunction and nicotinamide adenine dinucleotide phosphate (NADPH) oxidase activation, further amplify inflammatory signaling through NF-κB, p38 mitogen-activated protein kinase (MAPK), and the NOD-like receptor family pyrin domain–containing 3 (NLRP3) inflammasome, while increased matrix metalloproteinase-2 and 9 activity relative to tissue inhibitor of metalloproteinases-1 reinforces a proteolytic, nonhealing state.7,11,12
Impaired coordination between innate and adaptive immune responses further contributes to chronic wound pathology. Regulatory T cells facilitate inflammatory resolution through IL-10 and support fibroblast and keratinocyte function, whereas cutaneous γδ T cell subsets promote epidermal repair and regulate macrophage activation.51–53 In metabolically compromised wounds, particularly diabetic wounds, these regulatory circuits are disrupted, leading to persistent M1-like macrophage activation, increased TNF-α, IL-1β, matrix metalloproteinase 9, and STAT1 signaling, and delayed tissue repair. 54 Consistent with this framework, immunonutrients have been proposed to facilitate inflammatory resolution through coordinated effects on immune cell polarization, cytokine balance, and redox homeostasis. 55
Protein intake in animal models with chronic wound healing
Animal models provide mechanistic insight into how protein-based interventions influence inflammatory resolution and wound repair. In a rat model of ischemic full-thickness wounds, oral supplementation with
Potential molecular mechanisms of protein and immune regulation
Amino acids function not only as metabolic substrates but also as regulators of immune responses and tissue repair. Supplementation with Arg and Gln has been associated with improved wound healing, partly through enhanced nitric oxide (NO) bioavailability, support of collagen synthesis and wound contraction, and reductions in systemic inflammatory markers such as CRP, IL-6, and TNF-α. 14 At the cellular level, Gln supports endothelial cell proliferation by serving as an anaplerotic carbon source for the tricarboxylic acid cycle (TCA cycle); glutamine deprivation or glutaminase-1 inhibition disrupts this pathway, whereas α-ketoglutarate supplementation can restore mitochondrial metabolism and cell growth. 59 By contrast, EC migration appears less dependent on glutamine and relies more heavily on glycolysis, indicating distinct metabolic requirements for proliferation and motility. 59 In parallel, glutaminase-1–dependent Gln metabolism supports EC survival through cyclin A and heme oxygenase-1 regulation, while endothelial nitric oxide synthase (eNOS)–derived NO contributes to angiogenic signaling through a complementary pathway. 60 Protein-derived biomaterials may directly modulate immune responses within the wound microenvironment; leucine-derived pseudo-protein biomaterials accelerated wound closure in vitro and shifted macrophage cytokine profiles toward a reparative phenotype. 61 Together, these findings support a coordinated role for protein-based interventions in immune regulation, endothelial metabolism, and tissue repair (Fig. 3).
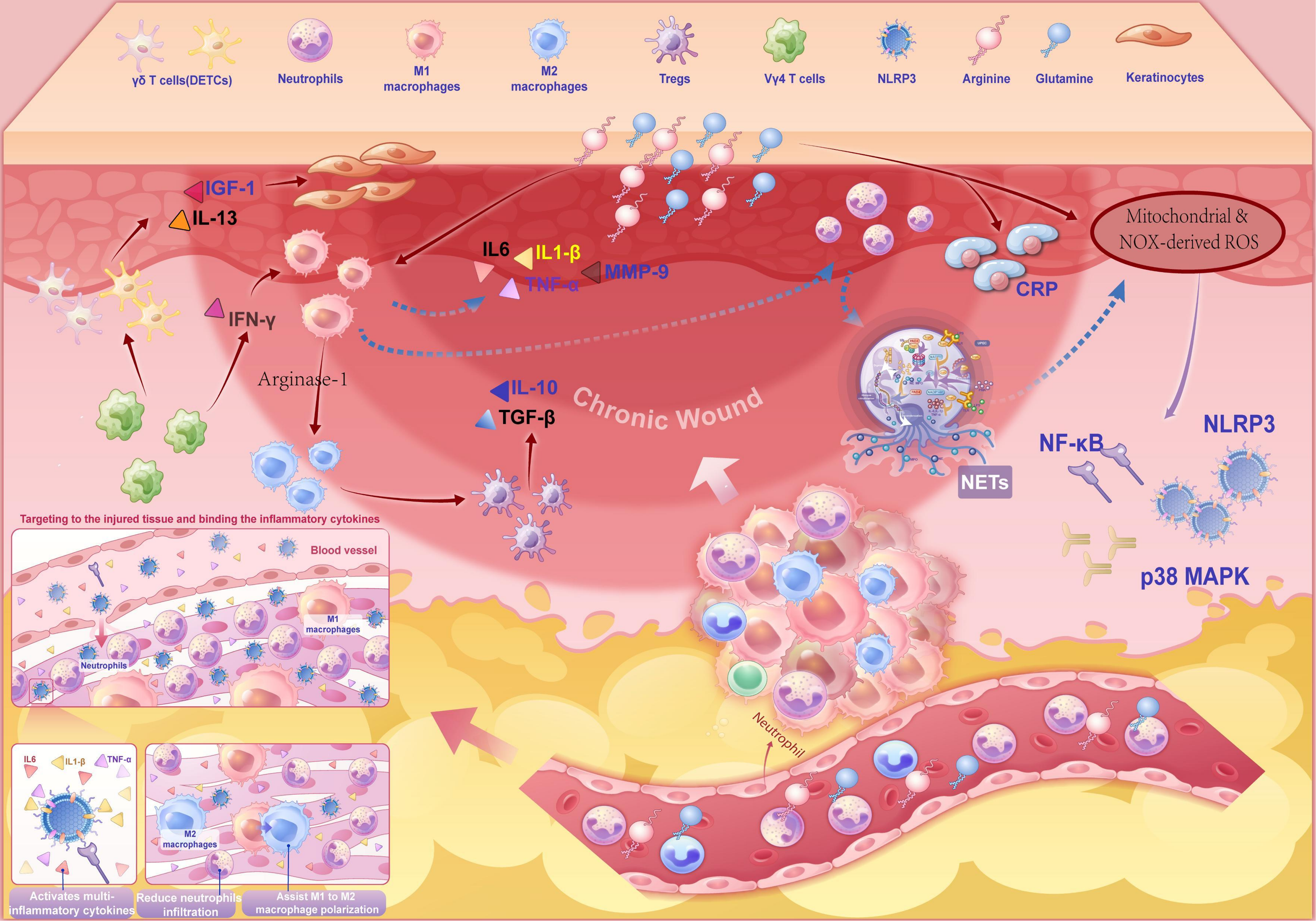
Modulation of inflammatory components by protein-based interventions in chronic wounds. Neutrophils, macrophages (M1 and M2), regulatory T cells (Tregs), and γδ T cells participate in the inflammatory microenvironment of chronic wounds. Abbreviations: γδ T cells, gamma delta T cells; DETCs, dendritic epidermal T cells; Tregs, regulatory T cells; Vγ4 T cells, V gamma 4 T cells; IGF-1, insulin-like growth factor 1; IL-13, interleukin 13; IFN-γ, interferon gamma; IL-6, interleukin 6; IL-1β, interleukin 1 beta; TNF-α, tumor necrosis factor alpha; IL-10, interleukin 10; TGF-β, transforming growth factor beta; MMP-9, matrix metalloproteinase 9; CRP, C-reactive protein; NETs, neutrophil extracellular traps; ROS, reactive oxygen species; NOX, nicotinamide adenine dinucleotide phosphate oxidase; NF-κB, nuclear factor kappa B; NLRP3, NOD-like receptor family pyrin domain–containing 3; p38 MAPK, p38 mitogen-activated protein kinase.
Oxidative stress and redox balance
Redox imbalance is a central feature of chronic wound persistence. Excess ROS damage cellular components and sustain inflammation by promoting M1 macrophage polarization and increasing TNF-α, IL-1β, and IL-6. NADPH oxidase activity and mitochondrial dysfunction further amplify ROS and activate NF-κB, p38 MAPK, and NLRP3 pathways, reinforcing an oxidative-inflammatory cycle.12,62 Single-cell transcriptomic studies also show reduced expression of antioxidant defense genes in keratinocytes, fibroblasts, and macrophages in chronic wounds, underscoring redox dysregulation as a therapeutic target. 4 Evidence beyond wound-specific cohorts further supports a role for amino acid supplementation in restoring redox homeostasis: in elderly individuals with impaired glutathione synthesis, 14 days of cysteine and glycine supplementation nearly doubled erythrocyte glutathione and reduced plasma F2-isoprostanes, while a meta-analysis of 17 randomized trials found that cysteine-rich whey protein reduced malondialdehyde (MDA) and CRP and improved the glutathione (reduced form)/glutathione disulfide (oxidized form) ratio.63,64
Enhancement of mitochondrial and antioxidant capacity in vivo
Animal studies indicate that targeted protein and amino acid supplementation can improve mitochondrial function and antioxidant defenses in chronic wound models. In inducible nitric oxide synthase (iNOS) knockout mice, oral
Cell-autonomous mechanisms revealed by in vitro studies
Physiological ROS participate in normal repair, but excessive or sustained ROS disrupt redox-sensitive signaling and contribute to chronic wound stalling.16,68,69 In macrophages, persistent ROS promotes a proinflammatory phenotype linked to mitochondrial dysfunction, reinforcing an oxidative-inflammatory loop.
16
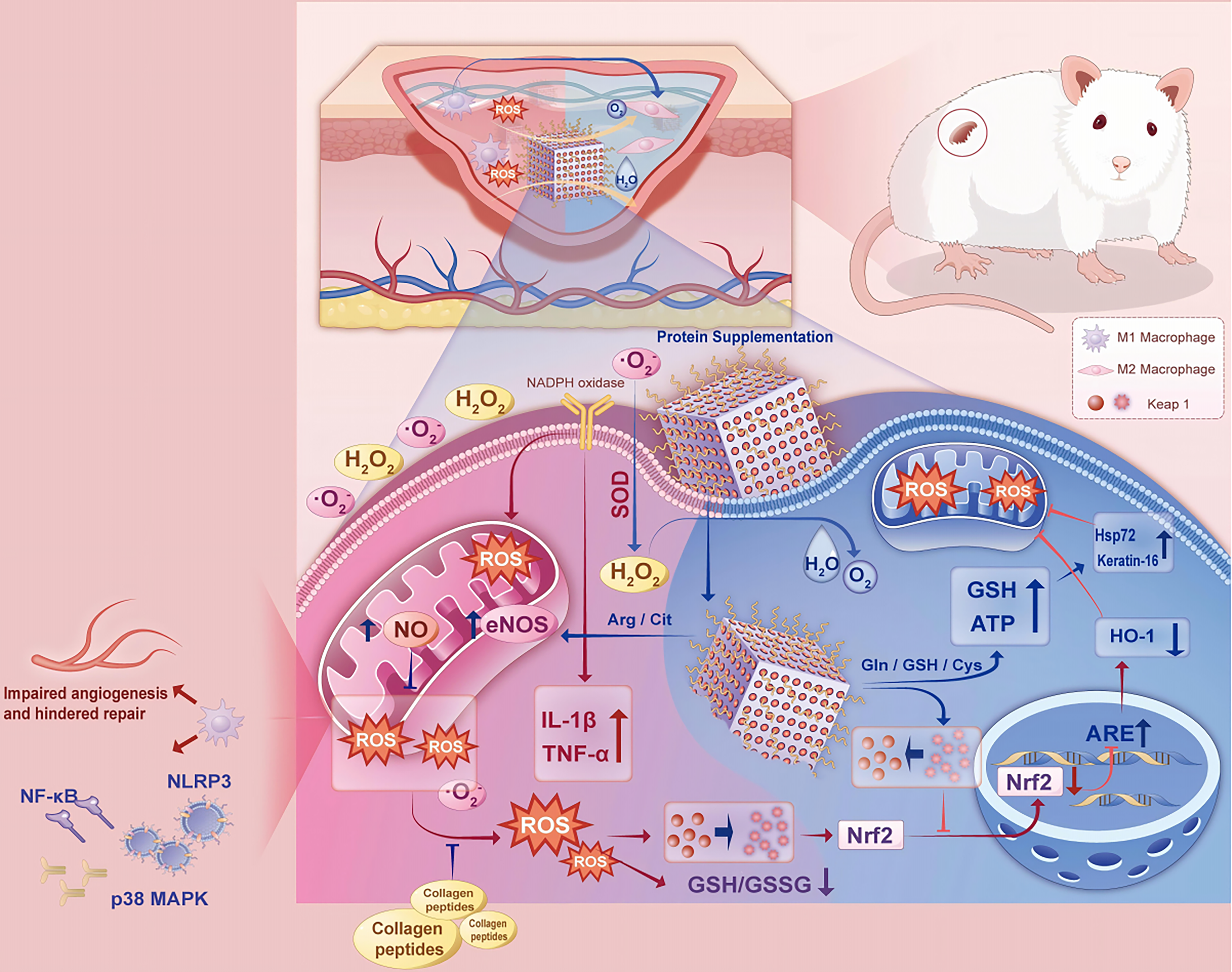
Protein-based interventions targeting oxidative stress–associated cellular responses in chronic wounds. Arg, arginine; Cit, citrulline; Gln, glutamine; Cys, cysteine; GSH, glutathione (reduced form); GSSG, glutathione disulfide (oxidized form); ROS, reactive oxygen species; NO, nitric oxide; eNOS, endothelial nitric oxide synthase; NADPH oxidase, nicotinamide adenine dinucleotide phosphate oxidase; SOD, superoxide dismutase; H2O2, hydrogen peroxide; O2−, superoxide anion; IL-1β, interleukin 1 beta; TNF-α, tumor necrosis factor alpha; NF-κB, nuclear factor kappa B; NLRP3, NOD-like receptor family pyrin domain–containing 3; p38 MAPK, p38 mitogen-activated protein kinase; Nrf2, nuclear factor erythroid 2–related factor 2; ARE, antioxidant response element; HO-1, heme oxygenase 1; Hsp72, heat shock protein 72; ATP, adenosine triphosphate.
Angiogenesis and perfusion
Chronic wounds exhibit impaired angiogenesis because ischemia, hypoxia, and inflammation disrupt endothelial function, reduce perfusion, and delay granulation tissue formation. Adequate protein intake may help restore angiogenesis through metabolic support and pro-angiogenic signaling.
Protein-induced neovascularization in chronic wound animal models
Preclinical models provide mechanistic evidence that systemic protein supplementation and bioactive peptide–based strategies can enhance angiogenic responses during wound repair. In a full-thickness excisional wound model in male Sprague–Dawley rats, oral supplementation with a whey protein–oligopeptide formulation increased vascular endothelial growth factor (Vegf), fibroblast growth factor-2 (Fgf-2), and insulin-like growth factor-1 (Igf-1) expression at wound margins, together with higher capillary density, reduced neutrophil infiltration, and greater early collagen deposition. 19 In male C57BL/6J mice, topical Igf-1 inhibited Ras–PI3K–IKK–NF-κB signaling and increased CD31+ microvessel density, consistent with concurrent suppression of inflammation and enhancement of microvascular regeneration. 70
In a frostbite mouse model, intravenous trans-activator of transcription–cold-inducible RNA-binding protein peptide suppressed Tnf-α, Il-6, and MD2 expression; increased CD31+ vessel density and Ki67+ cell proliferation; and accelerated wound closure and epidermal regeneration. 71 In diabetic wound models, a nanozyme-based arginine delivery system promoted localized NO production and improved revascularization in ischemic tissue, whereas reduced endothelial glutaminase-1 (GLS1) expression in diabetic skin was linked to impaired angiogenesis and was partially restored by glutathione-related metabolites.72,73
Potential molecular mechanisms of protein and angiogenesis
In vitro and ex vivo studies provide mechanistic insight into how protein-rich matrices and amino acid–dependent metabolism regulate endothelial angiogenic behavior. In a bone–endothelial coculture system using primary osteoblasts and human endothelial outgrowth cells, platelet-rich fibrin (PRF) increased VEGF expression and promoted formation of lumen-containing microvessel-like structures. 74 Endothelial dependence on glutamine metabolism is supported by studies showing that glutaminase-1 (GLS1) knockdown in human endothelial cells causes G0/G1 arrest, impaired migration, increased intracellular ROS, and reduced HO-1 and VEGF expression. 60 GLS1-driven glutamine catabolism supplies α-ketoglutarate to the TCA cycle, supporting mitochondrial adenosine triphosphate production for endothelial proliferation; by contrast, glutamine repletion rescues proliferation more effectively than migration or vascular morphogenesis, indicating distinct metabolic requirements for endothelial growth and angiogenic remodeling (Fig. 5). 59
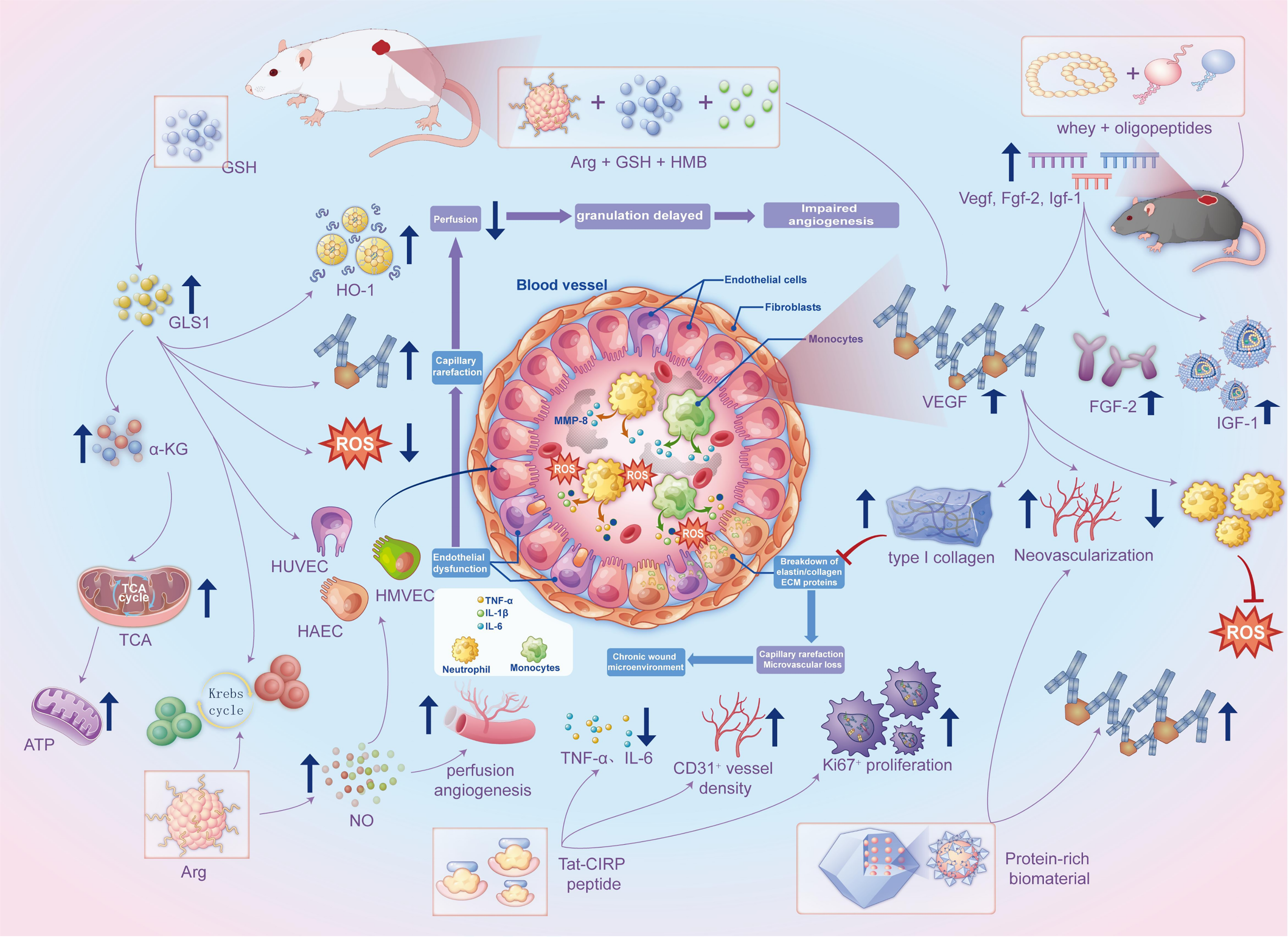
Modulation of angiogenesis and perfusion by protein-based interventions in chronic wounds. Arg, arginine; GSH, glutathione (reduced form); HMB, β-hydroxy-β-methylbutyrate; α-KG, alpha-ketoglutarate; GLS1, glutaminase 1; TCA cycle, tricarboxylic acid cycle; ATP, adenosine triphosphate; NO, nitric oxide; ROS, reactive oxygen species; HO-1, heme oxygenase 1; VEGF, vascular endothelial growth factor; FGF-2, fibroblast growth factor 2; IGF-1, insulin-like growth factor 1; MMP-8, matrix metalloproteinase 8; TNF-α, tumor necrosis factor alpha; IL-1β, interleukin 1 beta; IL-6, interleukin 6; CD31, cluster of differentiation 31; Ki67, marker of proliferation Ki-67; HUVECs, human umbilical vein endothelial cells; HMVECs, human microvascular endothelial cells; HAECs, human aortic endothelial cells; Tat-CIRP, trans-activator of transcription–cold-inducible RNA-binding protein peptide; ECM, extracellular matrix.
ECM remodeling
Defective ECM remodeling is a major barrier to chronic wound healing. Persistent inflammation and proteolysis accelerate collagen degradation, while fibroblast senescence and dysfunction reduce type I and III collagen synthesis, producing a disorganized, mechanically weak matrix with reduced tensile strength and impaired contraction.7,50
ECM remodeling in animal models with chronic wound healing
Preclinical studies indicate that targeted protein and peptide supplementation can improve ECM remodeling in chronic wounds. In male Sprague–Dawley rats with full-thickness dorsal wounds, oral whey–oligopeptide supplementation promoted earlier transition into the remodeling phase, with increased VEGF, IGF-1, and FGF-2 expression and improved collagen bundle organization.14,19 In female Sprague–Dawley rats with cesarean incision wounds, marine-derived collagen peptides increased tensile strength, hydroxyproline content, CD34, and connective tissue growth factor expression, consistent with enhanced collagen–smooth muscle matrix reconstruction. 75 In streptozotocin-induced diabetic C57BL/6 mice, tilapia collagen peptides shortened the latency phase and increased IGF-1, FGF-2, VEGF, and TGF-β1 levels, supporting granulation and matrix repair. 76 In a murine full-thickness excisional wound model, oral egg-white peptides achieved 90% wound closure, and transcriptomic/proteomic analyses identified PI3K–Akt as a central pathway associated with proliferation and matrix deposition. 77 Nutritional geometry analyses in severe thermal injury further suggested that macronutrient timing influences repair, with prolonged high-protein feeding potentially delaying healing. 43
Potential molecular mechanisms of protein and ECM remodeling
Matrix-derived peptides and amino acids can directly stimulate fibroblast activity and ECM synthesis. In primary human dermal fibroblasts, human collagen α-2(I) fragments enhanced fibroblast migration and increased type I collagen and elastin production.
78
Similarly, collagen α-1(I)-derived peptides upregulated the COL1A1–COL3A1–ELN gene cluster and increased soluble collagen secretion.
79
Proline supplementation in human skin fibroblasts under glutathione-deprived conditions increased COL1A1 and HIF-1α expression, prolidase activity, p-Akt signaling, and collagen biosynthesis, effects attenuated by glutathione repletion.
80
In human dermal fibroblasts,
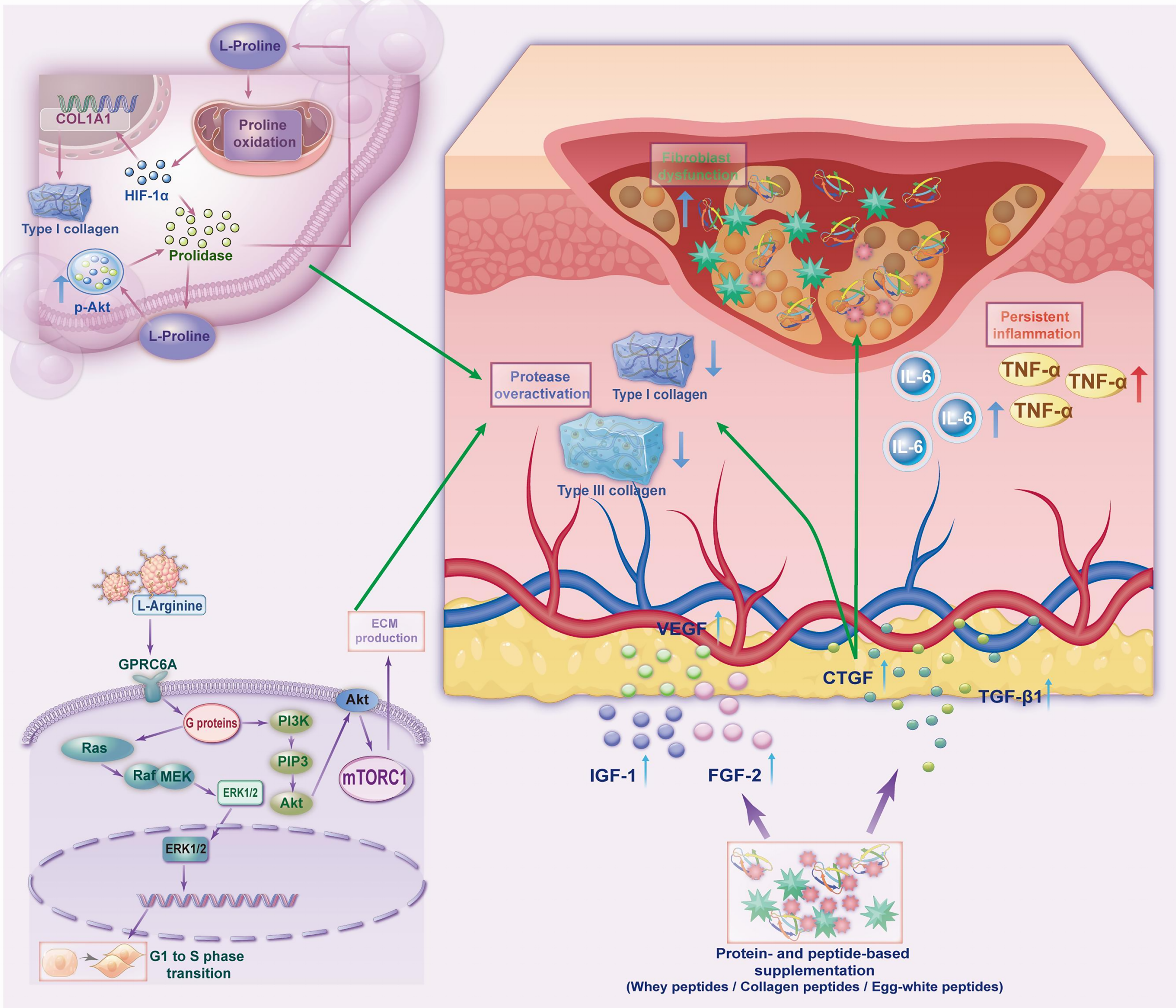
Protein-based nutritional modulation of extracellular matrix remodeling in chronic wounds.
Protein source selection and emerging formulations
Protein source influences amino acid profile, bioavailability, and immunometabolic effects. Animal-derived proteins provide complete amino acid compositions and are rapidly absorbed, supporting collagen synthesis and tissue repair; experimental studies suggest benefits for collagen deposition, inflammation control, and glycemic regulation.67,76,77 Plant proteins may offer complementary antioxidant and anti-inflammatory effects, as illustrated by soy protein–based scaffolds that accelerate reepithelialization and reduce local inflammation.56,83 Hybrid, hydrolyzed, and nanocarrier-based formulations may further improve bioavailability and wound-related efficacy, although stronger human evidence is still needed.
SUMMARY
Targeted protein-based nutritional interventions represent a promising adjunct in chronic wound care by addressing persistent inflammation, redox imbalance, impaired angiogenesis, and defective ECM remodeling. Beyond serving as structural substrates, proteins and functional amino acids may act as immunometabolic regulators that influence the wound microenvironment and reparative trajectory. Current mechanistic and clinical evidence supports a more individualized approach in which protein composition, dose, and timing are aligned with wound etiology and metabolic context. Future studies should refine biomarker-guided stratification and clarify safety, durability of response, and long-term healing outcomes.
TAKE-HOME MESSAGES: PROTEIN-BASED NUTRITION IN CHRONIC WOUND CARE
Why this matters
Chronic wounds often stall because persistent inflammation, oxidative stress, impaired perfusion, and ECM dysregulation disrupt progression to proliferation and remodeling. Protein-based nutrition should be viewed as an adjunct to, not a substitute for, etiology-specific standard wound care.
Who benefits
Consider protein-based nutrition in chronic wounds that fail to achieve 20–40% area reduction after 2–4 weeks of guideline-based care. Patients with malnutrition risk, reduced intake, frailty, sarcopenia, or high inflammatory burden may be more likely to benefit.
What to prescribe
Total protein intake is commonly targeted at approximately 1.25–1.5 g/kg/day, with lower individualized targets in chronic kidney disease. In selected patients, formulations enriched with arginine, glutamine, and/or HMB may be considered. Protein-based regimens should always be paired with core standard-of-care measures.
What to monitor
Reassess every 2–4 weeks using wound trajectory, nutritional status, and treatment tolerance. Monitoring should include wound area change or validated wound scores, body weight/BMI trends, relevant laboratory markers interpreted in clinical context, renal function, glycemic status in diabetes, and adherence.
What outcomes to expect
Clinical studies suggest that, when added to standard wound care, protein-based regimens may improve wound-area reduction and healing trajectory, although results vary by wound etiology, baseline risk, and study endpoints. Signals of benefit have been reported in pressure injuries, DFU, and venous leg ulcers, particularly when patient selection and adherence to co-interventions are appropriate.
When to taper or stop
Tapering or discontinuation may be considered after wound closure or when a sustained favorable healing trajectory has been achieved. Early de-escalation and reassessment are warranted if renal function worsens, tolerance is poor, or glycemic control becomes unstable despite adjustment.
AUTHORS’ CONTRIBUTIONS
Zilong Tan and Yi Ru: wrote the original article and collated the literature. Caiyun Zhang and Xinxin Wu: carried out the literature screening and data extraction and assisted with drafting the article. Qingkai Liu: contributed to article revision and coordination. Qilong Chen and Bin Li: supervised the work, critically reviewed the article, and approved the final version. All authors have reviewed and approved the final version of the article and agree to be accountable for all aspects of the work.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This work was financially supported by the Natural Science Foundation of Shanghai Science and Technology Commission [grant number: 23ZR1456000] and the Hospital-level Fund of Shanghai Skin Disease Hospital [grant number: 2022KYQD02].
AUTHOR DISCLOSURE AND GHOSTWRITING
No competing financial interests exist. The content of this article was expressly written by the author(s) listed. No ghostwriters were used to write this article.