
Abstract
The disclosure of absences from professional sporting activities to the media is a routine and generally unproblematic part of a sporting career. However, when the reason for the absence relates to mental health concerns, players can encounter difficulties in trying to define, describe and conceptualise their own issues while attempting to maintain privacy as they undergo assessment and treatment. Drawing on ethnomethodology and conversation analysis principles and methods, this paper explores first/initial public mental health disclosure narratives produced by players and sporting organizations across several professional sports via media interviews, press statements, and social media posts. The analysis focuses on (in)voluntary accounts produced by teams or players themselves during their careers and examines the different communication strategies they employ to categorise and explain their predicament. The analysis reveals how some players provide partial or proxy public disclosure announcements (due to a desire to mask issues or delayed help-seeking and assessment), whereas others prefer fuller disclosure of the problems experienced, including diagnoses and on-going treatment and therapy regimes. The paper outlines the consequences of these disclosure strategies and considers the implications they can have for a player’s wellbeing in these stressful circumstances.
The disclosure of mental health issues by professional sports players and organizations have been previously explored, and reveal how such absences are ordinarily communicated to fans via various media channels (e.g. press statements, media interviews, team websites, social media posts) (Elsey, 2019; Lavelle, 2020; Parrott et al., 2019). These studies show several barriers to disclosure that adversely impact help-seeking. For example, timely help-seeking for mental health issues by sports players can be impacted by the fear of revealing symptoms to other people, the negative perception of counselling as being for “weak” people, the continued use of the dominant “no pain, no gain” injury maxim, and the lack of healthy coping mechanisms in response to failures (Curry, 1993; Gulliver et al., 2012; Putukian, 2016). In short, the stigma of mental health in sport retains a strong influence, especially when it comes to disclosure in male-dominated environments (Messner, 1992; Young et al., 1994).
In terms of mental health disclosure in the general population, previous research highlights a range of factors that can encourage or inhibit these conversations. The process captured in the literature outlines the possibility of “selective,” partial or gradually evolving disclosures in which an individual can devise a plan based on their own disclosure preferences which sets out “what can and should be disclosed and to whom, and of what and when it is advisable to conceal” (Bril-Barniv et al., 2017, p. 9; Pahwa et al., 2017). These decisions to disclose (as well as involuntary or “forced exposures”) apply to encounters with family members, friends, and within workplaces and healthcare settings (Bril-Barniv et al., 2017; Pahwa et al., 2017).
In the media-oriented context of professional sport another layer of disclosure recipients is added: the public as an “over-hearing audience,” via journalists (Heritage & Clayman, 2010). The reporting of a player’s health status is a structured and organised feature of sports “media strategies” from press conference announcements to teams' publicly available “injury reports” (Armstrong et al., 2016; Smith & Keeven, 2019). In terms of welfare issues, for players and teams, the difficulty stems from managing these competing interests.
The disclosure of mental health issues within professional sport has received a noticeable increase in media coverage. In part, this trend has been interpreted by players and the media as an eroding of the stigma associated with mental health issues within sporting circles (Elsey, 2019; Lavelle, 2020; Parrott et al., 2019), as well as reflecting wider societal trends towards promoting the “parity of esteem” between physical and mental health (The King’s Fund, 2017).
The process of diagnosis and treatment of any injury revolves around the medical and sports science staff employed by clubs and associations. Common and typical physical injuries can be diagnosed and treated, with clear and relatively unambiguous details released to the public via the media (e.g. nature/cause of injury, treatment details, approximate timeframe for return) (Sanderson et al., 2016). However, in comparison, the diagnosis of mental health conditions can be complicated and protracted. As a result, differential or provisional diagnoses can be put in place and be subject to change with further assessment and information. This points to delayed diagnosis, from the initial onset of symptoms to the commencement of appropriate treatment and management of the presenting issues (Wang et al., 2005). This extended process can include delays in help-seeking (Souter et al., 2018), problems accessing services (Royal College of Psychiatrists, 2018) and misdiagnosis (Wang et al., 2005).
The focus of this paper is to examine a player’s absence in relation to mental health disclosure: how does their disclosure become a matter of public/media interest? And how are diagnoses attributed as the “official” reason for a specific public disclosure? In this study, we present an original contribution to research on professional sport and communication which showcases how players (whether personally or via their sporting agent, club or association) provide the first or initial public disclosure of mental health issues to account for their absence from competition in the form of “coming out” announcements (Corrigan & Matthews, 2003; Lavelle, 2020; Parrott et al., 2019). One critical aspect of these disclosure narratives is their social and interactional organisation e.g. Who is told what, when and how? (Sacks, 1995).
A recurrent feature of these first announcements is the issue of the timing of the public disclosure. These can be accelerated (compared to non-sporting contexts) and delivered at the time of the absence or withheld until retirement (Elsey, 2019; Lavelle, 2020; Parrott et al., 2019). This, in part, relates to whether the player/team were aware of the (eventual) mental health diagnosis at the time of the various communications (e.g. routine press conferences with injury updates). The timing aspect also relates to the degree of openness or transparency that a sportsperson feels comfortable with when dealing with the media (Reng, 2011). One potential issue in the professional sporting context is that accurate mental health diagnosis and competitive schedules are not necessarily aligned in that a “reason” for an absence is always pursued by the media and the public. This can result in partial, delayed, and gradual public disclosure, and can ultimately lead to complications and unwanted knock-on effects (e.g. invasive fan and media interest). Another background factor that may impact a player’s willingness to speak openly relates to how information about their mental health could negatively affect future employability i.e. will teams be less likely to give them a contract (Bauman, 2016; Merz et al., 2020).
While there is a growing body of sociological literature on the wider debates and consequences of disclosure, little is known about players’ disclosure practices across the diverse range of (sports) media texts. This article aims to address this gap by exploring the actual statements of disclosure by professional sports people and organisational representatives (e.g. coaches, teams, law enforcement) allowing for a more fine grained analysis of the evolving processes of announcing disclosures.
Methods
This research employs the principles and methods of ethnomethodology and conversation analysis (CA) in order to examine official public statements produced by players, players’ agents and their clubs or organizations (Garfinkel, 1967; Lynch, 2007; Sacks, 1995). These modes of analysis focus on the accounting practices used in these contexts that provide a public and “inferentially-rich” official reason for absence on the record (Sacks, 1995).
As part of our analysis, seven case studies of professional sports players were selected from prominent sporting figures (Denison, 1996). These include British football/soccer (Lenny Pidgeley), American Football (Brandon Brooks; Brandon Marshall; Everson Griffen), cricket (Marcus Trescothick; Sarah Taylor), and Basketball (Imani Boyette). Cases reflected different diagnoses (i.e. stress, depression, anxiety and borderline personality disorder). In this study, mental health was defined as any common psychological or psychiatric conditions which received formal diagnoses (e.g. anxiety, stress, depression, bi-polar disorder, schizophrenia, borderline personality disorder, etc). We selected these cases on the basis of whether the mental health issues had an impact on the player’s on-going career and were disclosed during their career, thereby excluding cases disclosed post-retirement (Schwenk et al., 2007). Comparison was made between team-led disclosure (where a team employee speaks on behalf of a player) and player-led disclosure (where a player voluntarily discloses in their own words) to explore the variety of media disclosure practices and the implications of the strategies.
We then constructed a retrospective “mental injury” timeline for each case.
1
The timelines capture the prospective-retrospective nature of the accounts as provisional, changeable, and evolving (Elsey, 2019; Lavelle, 2020; Stokoe & Attenborough, 2015). The timelines utilise official or authorised public announcements about a player’s mental health using a range of public-facing media sources (e.g. media interviews, press statements and conferences, social media, (auto)biographies, sports media websites). Analysis then retrospectively/prospectively tracks when and how mental health is referred to in relation to player’s participation in competitive fixtures (i.e. past, present and future appearances). In particular, this study focuses on the first known disclosure of a player’s mental health situation which occurred during their career. For audio-visual sources, transcripts were produced using the CA transcription conventions to represent the interactional features of the original recordings (Jefferson, 2004). In doing so, we analyse and compare the following features of the “mental injury” timelines and ask the following questions: What was the context of the first known disclosure? Why was the disclosure made now? Who performs the disclosure? What platform was used to release the information and what form did the disclosure take? (e.g. personal/team social media posts, press statement, press conference, media interviews etc) What was the impact and consequences of the disclosure for the player?
We encourage readers to view available videos alongside the analysis.
Results
Team-Led Disclosures
Analysis begins with two contrasting cases in which the sporting organisation or team discloses a player’s mental health issues to the media on behalf of the player with or without their permission.
“Outed” by the team
The first case is based on Farnborough Football Club’s (FC) statement regarding Lenny Pidgeley (Case 1 in the supplementary timelines). Pidgeley was a goalkeeper who started his career in 2002 with Chelsea FC in the English Premier League before finishing his career in the semi-professional leagues with Farnborough FC. Pidgeley retired in September 2018 due to ongoing difficulties related to depression. Pidgeley had suffered from bouts of depression throughout his career (notably while at Millwall between 2006 and 2009, Newport County 2012–2015 and Margate FC in 2017) but he felt it was a “private matter” and therefore he “was never, ever going to speak in public about it” (Pearlman, 2018). Here we present how the player’s disclosure preferences (i.e. to withhold his medical history from fans) are framed using public/private or front-stage/back-stage distinctions, and as revealed involuntarily against his wishes (Goffman, 1990a, 1990b).
On 12 September 2018 Farnborough FC, via their official team website, announced Pidgeley’s retirement from football with immediate effect due to, what they defined as, a “significant long term personal medical condition” in the lead up to an FA Cup match against Lewes. Pidgeley reacted angrily to this disclosure on Twitter: I’ve never talked about my depression in the last 10 years…but after that club statement [the issue] seems to be out the bag. With no goalkeeper available that night we owed the fans an explanation [why midfielder CJ Fearn played as goalkeeper] before kick-off…[The] Club fully backs the support and care required in dealing with all mental health issues and meant no harm to Lenny and sincerely apologise for any hurt. Pidgeley said he is upset he did not get to decide if he went public with his illness, even revealing that close family members, including his own mother, were unaware of his plans to retire. “When the statement came out, it put me in a dark place. The way the club have conducted themselves is not right…They mentioned my illness, which I have never been comfortable talking about. For 10 years I’ve tried to keep it undercover…I have never wanted this to come out, never ever.” (Pearlman, 2018)
The second team-led disclosure case reveals a very different set of circumstances in which mental health issues are made public by sporting organizations where the team is responding to specific events or incidents.
Law enforcement: Police enforced psychiatric/psychological evaluation
The disclosure of mental health difficulties can also relate to circumstances in which players are detained by law enforcement officers. Under police protection, players (like any citizen) may be admitted for psychiatric evaluation due to safety concerns for the individual and/or the public. In contrast with Pidgeley’s case (private/backstage issues), the visible/public manifestation of a player’s problems forces their organization to make press statements (with the agreement of a player and/or player’s family) in order to respond to the unfolding situation. These very public help-seeking behaviors can point to a currently undiagnosed and untreated psychological issue.
The mental injury timeline of American Footballer Everson Griffen (Case 2) began with unusual and “erratic” behavior around 16 September 2018 according to his wife. On 20 September 2018 the Minnesota Viking’s reportedly sent Griffen a letter stating that he would not be welcome at training until he underwent a mental health evaluation following recent verbal outbursts at training. Two days later Griffen was detained by the local Minnetrista Police Department (in Minnesota) under a “health and welfare hold” and escorted to a mental health facility for evaluation. The Department’s incident report documented Griffen’s behavior during his detention as not “acting normal,” “sleep deprived,” “delusional,” “paranoia,” “rapid speech,” “irrational,” “rambling” and “repeating himself” (Graff, 2018).
On the day of his detainment (22 September 2018) Griffen was sent away from training, before causing a “disturbance” at the hotel where he was temporarily staying. Griffen then allegedly broke into the house of a teammate and accosted a man at a petrol station (who drove him home). Neighbours contacted the police after observing Griffen outside his house yelling (“777” and how “God made me do it”). One officer reported that Griffen had mentioned being afraid of people trying to kill him. While Griffen eventually agreed to attend hospital, the officer in charge still produced a “hold form” and paramedics were called. On route to hospital Griffen escaped from the ambulance and more police officers were called to assist. Eventually persuaded to return to the ambulance, the vehicle was followed by a police officer (with Griffen’s permission) to make sure Griffen arrived at his destination. The police dashboard camera which recorded this event was leaked to the media a few weeks later (TMZ, 2018). The official outcome of the situation was that “no criminal charges [were] forthcoming.”
Two days later the team would issue a statement on behalf of the player (technically the first official disclosure). This announcement represented a “forced exposure” given the recent very public and visible conduct of the player and was announced as part of the team’s weekly injury report (Bril-Barniv et al., 2017). In this case it is the timing of the announcement that is involuntary in nature. The Viking’s General Manager Rick Spielman stated that: We are aware of the situation involving Everson Griffen and certainly concerned by what we have heard. We are currently focused on Everson’s well-being and providing the appropriate support for him and his family. (Graff, 2018) After five weeks of work and evaluation [in September 2018], the doctors concluded Everson’s erratic behavior resulted from significant unresolved emotional distress, emotional incongruence and a lack of healthy coping skills (Pelissero, 2020).
Player-Led Disclosures
Compared with team-led announcements, player-led mental health disclosure narratives are informed by a different set of considerations. While disclosure preferences and match schedules remain relevant, a major factor impacting what is revealed at a specific moment in time is diagnostic certainty.
Mental health issues pre-dating sporting career
The first player-led case represents a unique context in which a player’s own volition results in a public disclosure. Imani Boyette, nee McGee-Stafford, was the latest of a long line of successful female basketball players in her family (Case 3). Boyette joined the Texas Longhorns (University of Texas) on a college scholarship in November 2011 where she enjoyed four successful seasons between 2012 and 2016 (Berkman, 2016). During this time Boyette was reported to have had only one significant time away from basketball to recover from ankle surgery (Texas Longhorns Online, 2014).
On 27 February 2015 the team announced that Boyette would be appearing on an ESPN show in a feature entitled “Her Voice” (Broadcast 1 March 2015). The 7-minute video features both snippets of Slam Poetry read by Boyette and interviews with Boyette and her father Kevin Stafford about her career trajectory, suicide attempts, molestation (“I’m a suicide survivor, I’m a molestation survivor”), and how she was able to manage these traumatic experiences through Slam Poetry (“found solace in words”). Below is an excerpt from the video which represents the first time Boyette’s history of suicide attempts and molestation was disclosed to the public via the words of its narrator, including her own account of the third suicide attempt before University: Imani was a ten-year-old struggling with her parents’ divorce when she first attempted suicide. In high school she would try twice more. Her third attempt came upon the realisation that as a child she had been molested by a family member—“I started having really bad nightmares and just remembering things that I had probably repressed or had not really been aware of […] I lashed out, I was like a walking cry for help. I got suspended from high school—there was a lot happening at that time. I overdosed and went to the Hospital and I was committed for [Pause] about, almost two weeks? And that was a lot—I basically took a really long look at myself because I had everything at high school it was really easy to me and I almost threw it all away.” In terms of just mental illness and depression, you don’t think there’s an end (to the suffering). To be here now and see the other side and remember what it felt like when I was in it, I just want to grab people and say, “Please just hold on!” (Thompson, 2016)
Delayed help-seeking and diagnosis
A frequently reported problem associated with professional sport and mental health is significant and consequential delays in seeking medical help, which can impact the clarity and certainty of information made public (Gulliver et al., 2012; Sacks, 1995; Souter et al., 2018). The contrasting experiences of NFL players Brandon Brooks and Brandon Marshall illustrate some of the important factors involved.
For Brandon Brooks (Case 4), ritualistic pre-game routines had been misinterpreted and misdiagnosed throughout his college and professional career, whereby his sickness was seen as a purely physical problem (and treated as such), rather than it being understood to be symptomatic of his anxiety. Prior to his public disclosure (via a locker room interview following training) in the 2016 season Offensive Guard Brooks had missed two out of three Philadelphia Eagles games (against the Green Bay Packers and the Washington Redskins) because of his anxiety and four NFL games across his career (including 2 years at the Houston Texans). At the time the official reasons provided to the media for these missed games was that he had suffered from “stomach ulcers” or “pains,” uncontrollable vomiting and severe dehydration, which had led to him being hospitalised (Kapadia, 2017). This unusual and recurrent behavior (throwing up right before his games to “feel better”) eventually drew the attention of the Eagles’ doctors who sought to identify the cause of the problem.
After missing the game against the Washington Redskins in December 2016, Brooks opened up about his battle with anxiety in a short interview (transcript in Table 1):
Brandon Brooks “Anxiety” Disclosure Interview (14 December 2016).

Video source:
Speaker:
BB = Brandon Brooks (Philadelphia Eagles player)
Brooks’ candid interview outlines when the diagnosis was made (“recently”—line 1), as well as the nature of his “anxiety condition.” His description of his issues reveals how this type of “unhealthy obsession” goes beyond the expected level of pre-game “nervousness or fear” and therefore required medical support (lines 2–8). This key message is then reiterated (lines 8–10), before Brooks thanks his team, organization, and coaches for their support. Furthermore, he states that this type of issue is “nothin’ I’m ashamed of…I own it” (lines 15-17). Brooks would repeat this message to educate, tackle and support other people in future interviews (Erby, 2019). This desire to speak out comes from a “dark place” (recall Pidgeley’s language about the impact of his “outing” on his health) in which Brooks admitted that the anxiety made him miserable to the extent that he considered retirement (Friedman, 2018).
In contrast, NFL wide-receiver Brandon Marshall’s (Case 5) delayed mental health diagnosis of Borderline Personality Disorder (BPD) was dramatically different as his behavior directly impacted others and crossed criminal boundaries. Clearly Marshall’s case shares some similarities with the domestic violence case of Ray Rice (Smith & Keeven, 2019) who also had a history of misdemeanours throughout his football career. However, Marshall would later attribute these actions to his BPD. Marshall’s chaotic off-field life included (alleged) theft, damage to property, being drunk and disorderly, assaulting police officers, resisting arrest, and domestic violence (Jones & Klis, 2011). Marshall’s problems came to a head in 2011 when he was reportedly stabbed by his fiancée in self-defence. Around this time teammate Ricky Williams recommended that Marshall seek professional help at the Mclean Psychiatric Hospital (Jaslow, 2011).
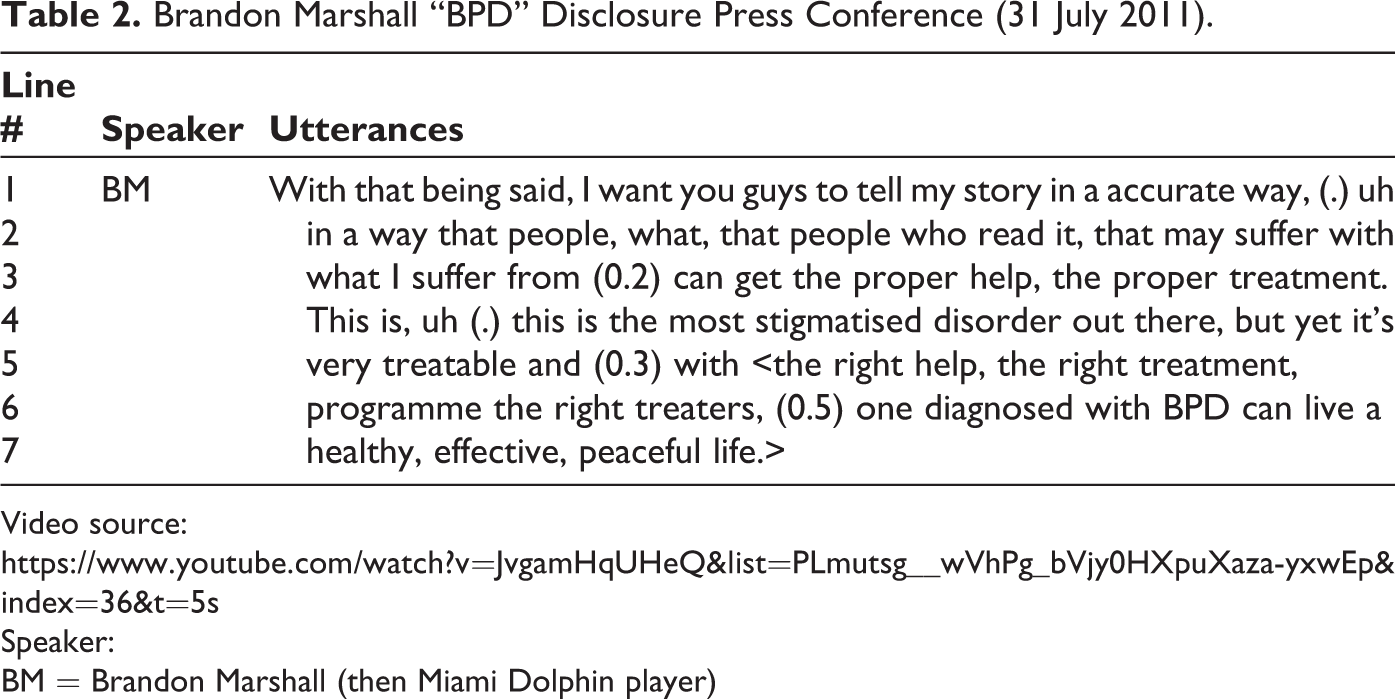
At a press conference on 31 July 2011 Marshall announced that he had been diagnosed with BPD and was undergoing treatment (transcript excerpt in Table 2). Marshall revealed his entire professional career and adult life had been marred with symptoms that left him unhappy, despite his (successful) life. He also pleaded with the media to “tell my story in an accurate way” (line 1). During his treatment Marshall reported that he had learned to deal with the consequences of his actions that were influenced by his BPD. Before his diagnosis he was known as “The Beast” and seen as a deviant, but the diagnosis of BPD offered an alternative explanation for his behavior and altered the perception of his past actions. This chimes with Smith’s (1978) analysis of how single instances of potentially mentally disordered actions are perceived as being connected, and therefore each new instance interpreted as indicative of an underlying problem. Marshall spoke out about his diagnosis in the hope that it would end the stigma attached to the condition, to raise awareness and understanding, and to encourage others in a similar situation to seek the appropriate support (lines 2–3).
Brandon Marshall “BPD” Disclosure Press Conference (31 July 2011).
Video source:
Speaker:
BM = Brandon Marshall (then Miami Dolphin player)
“Cover-up”—proxy/surrogate terms
The next case looks at England international cricketer Marcus Trescothick (Case 6). Unlike the cases of Brooks and Marshall, where alternative explanations (e.g. physical sickness or deviant behavior) were originally employed as their mental health diagnoses had yet to be determined, Trescothick’s diagnosis had already been established. However, in Trescothick’s case he was reluctant to disclose details of his mental health to the media and the public. When he did eventually disclose, Trescothick opted to employ a surrogate term (“virus”) in place of a mental health diagnosis.
At the time his mental health issues were deteriorating, Trescothick was vice-captain of England and an experienced opening batsman. However, Trescothick’s international career was prematurely ended by depression and anxiety (undiagnosed at the time) that took hold during England’s tour of India in February 2006. During the tour, the England and Wales Cricket Board (ECB) provided various reasons to account for his absence from tour games (“migraine”) and his early return to the UK for “family, personal reasons” on 25 February 2006. The unintended consequences of using surrogate terms to gloss Trescothick’s situation produced rumours in the UK media (e.g. his wife’s post-natal depression, extra-marital affairs) and caused a great deal of distress for him and his family.
Around 6 weeks after his return to the UK (and subsequent medical consultations) Trescothick decided that he needed to set the record straight about his exit from the tour. The ECB and his agent arranged a choreographed interview with Sky Sports journalist (and friend) Ian Ward. All questions were pre-screened and Trescothick’s answers rehearsed. In his autobiography, Trescothick reveals that, when he was prompted to account for his departure by the journalist, he had agreed to state that he left the tour as a result of having picked up a virus and also had some personal issues to resolve because of which he then “decided to return home…” (Trescothick, 2008, p. 227). This was meant to be the first step in his evolving disclosure that was in line with his on-going therapy and treatment for depression (Lavelle, 2020). An excerpt from the interview transcript is shown in Table 3.
Sky Sports News “Tresco Interview” (10 April 2006).

Video from Sky Sports News interview with Ian Ward (archive footage)
Broadcast: 10 April 2006, 5 pm
Adaptation of ESPN transcript:
Speakers:
JT = Sky Sports Journalist Ian Ward
MT = Marcus Trescothick (then England Cricketer)
Trescothick’s (2008) autobiography revealed how the pressure of discussing his “personal” situation in public (let alone disclosing the under-lying psychological issues that he was addressing in private) led to him panicking and retreating to offering a purely physical explanation for his return (“I picked up a bug”) (lines 2–3). This answer would further deepen the media suspicion with former cricketers critical of the baffling logic behind the ECB’s reluctant non-disclosure of a “virus.” It would not be until September 2006 that the ECB would release a statement drafted by Trescothick (2008, pp. 299–300) and his psychologist stating that: In addition to the deleterious effects of the acquired gastrointestinal infection on his health, it later became evident that he was also suffering from an underlying stress-related illness. Sarah is taking a break from cricket at the moment having decided to take some personal time away from the game. We will support her, keep in touch and talk with her prior to selection for the Pakistan series and the start of the Kia Super League. (BBC, 2016)
Discussion
This paper captures seven mental health disclosure discourses drawn from different professional sport contexts. The public nature of this workplace means that the disclosure of players’ mental health issues takes place in the public eye and any personal concealment preferences cannot always be factored into the decision-making process (Bril-Barniv et al., 2017; Pahwa et al., 2017). The mental injury timelines that we analyse show how these preferences vary quite profoundly. Therefore, it is important to recognise the circumstances in which the disclosure occurs as this informs the reasoning and language used in any announcement. Cumulatively the cases display how these barriers to help-seeking and delays in diagnosis are not perfectly suited to 24/7 worldwide media coverage that increasingly dominates professional sport and makes players’ careers and health visible and publicly accountable (Boyle, 2006; Steen, 2015).
One common factor across all the cases is the need to account for any absence from competition, which can accelerate the process of disclosure of mental health issues and force players and organizations to make public statements in line with routine media appearances scheduled during the playing season. For players and team staff the content, timing and platform of any statement or announcement requires close consideration and agreement as part of a reflexive “media strategy” (Armstrong et al., 2016; Smith & Keeven, 2019). This analysis raises questions about best practice in this context. While there is no single model of best practice that can be employed under all circumstances, based on the case studies presented here it is possible to outline some recommended disclosure practices.
In terms of the “timing” of any announcement, a player’s personal preferences cannot always be respected. For example, Imani Boyette was not known to be under any external pressure to reveal her depression and was able to decide when and how to disclose. In contrast, for Lenny Pidgeley (whose personal preference to conceal his depression was complied with by all his football clubs), his mental health issues were inadvertently and involuntarily revealed by his final club without his permission. These matters are critically important as they can “impact outcomes in the context of mental illness” and Pidgeley’s case should therefore serve as a stark lesson for sporting organizations (Pahwa et al., 2017, p. 583). However, sometimes players and teams cannot manage the timing of an announcement, particularly where law enforcement is involved. The very visible and public conduct of Everson Griffin in which he was considered a threat to himself and others was caught on video camera and therefore accelerated the team’s disclosure announcements.
Another major consideration is the “content” of the disclosure. The cases of Sarah Taylor and Imani Boyette suggests that (when possible) players should speak plainly and frankly in these circumstances. To minimise unwanted scrutiny and speculation from the media and fans, players and/or teams should seek to provide factual and accurate explanations for absences due to mental health, including, where appropriate, symptoms, diagnoses, and treatment. In part, this speaks to players’ responsibility as public role models who educate, advocate and promote mental health literacy and awareness (Corrigan & Matthews, 2003; Pahwa et al., 2017; Parrott et al., 2019). The goal is for culture change in sport and wider society, so that talking openly and honestly about mental health is “normalized” (Charlesworth & Young, 2006; Curry, 1993; Young et al., 1994).
However, this study also reveals that barriers to the normalisation of mental health disclosure remain. For example, the complexity of accomplishing a mental health diagnosis and its diagnostic uncertainty can make it difficult for players to feel able to speak coherently and knowingly of their situation. The case of Marcus Trescothick (2008) provides a cautionary example of how ambiguous language, such as surrogate terms like “personal/family issues,” to refer to mental health matters can be misleading for the media and public and result in further unwanted scrutiny that has negative psychological effects. This study also raises vital questions about patient confidentiality and media ethics. Marrying the needs and welfare concerns of players and the “public interest” is not always satisfactorily achieved when the competing interests of coaches, team-mates, team medical staff, media and fans can place pressure on players to “hide” their mental health issues and play through them (Charlesworth & Young, 2006; Greenslade, 2019; Reardon et al., 2019).
Players and teams should consider where to draw lines or mark boundaries between public and private matters in which players' rights under disability legalisation might be systemically undermined. One consideration linked to this is that due to the persistence of stigma, mental health issues can (hypothetically) impact a player's chances of being offered a contract and realizing the monetary value of these agreements (Merz et al., 2020). This speaks to a critical question of how organizations speak and act on behalf of players in the digital age (Armstrong et al., 2016).
Limitations
By almost exclusively relying on publicly available data, this study is limited to the inferences that can be drawn from such announcements. It is therefore critical that the views of players, coaches, media workers and the like are sought in order to assess their personal motivations, intentions and rationale for these key decisions. Furthermore, the case study approach which was adopted in this study has relied upon a small number of examples to illustrate key features of disclosure narratives. More comparative work along these lines is needed, as is a close examination of the gendering of disclosures.
Footnotes
Acknowledgments
The paper is indebted to Derek Edwards who helped identify some of the media sources for the cases and discussed some of the ideas contained in the final paper. The contributions of Leanne Billington and Cait Mansfield to the project also require appreciation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Small internal grant paid for additional data collection and analysis by the research assistants. De Montfort University (DMU) Frontrunner internship scheme funded contributions of James Southwood and Susan Jayne Litchfield.