
Abstract
The impact of identity-related risk factors on psychopathology was analyzed in 2,113 emerging adults (M = 22.0 years; 66% female) from France, Germany, Turkey, Greece, Peru, Pakistan, and Poland. Identity stress, coping with identity stress, maternal parenting (support, psychological control, and anxious rearing), and psychopathology (internalizing, externalizing, and total symptomatology) were assessed. After partialing out the influence of stress, coping, and perceived maternal behavior, country did no longer exert a significant effect on symptom scores. The effect for gender remained, as did an interaction between country and gender. Rather unexpected, on average, males reported higher internalizing symptomatology scores than females. Potential causes for the higher scores of males are therefore discussed. Partialing out covariates resulted in a clearer picture of country-specific and gender-dependent effects on psychopathology, which is helpful in designing interventions.
Emerging adults have an important role in the development of a nation because they will become the main workforce in the future and will lead political, economic, and social movements. Therefore, the health status of emerging adults is very important for a country in general and for countries with a large proportion of emerging adults in particular, as it is the case in many countries in the minority world (Chau & Saravia, 2016). The first onset of 20 Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), in the World Mental Health survey initiative in 21 countries revealed that maladaptive family functioning and adverse life circumstances account for 29.8% of all disorders across countries (Kessler et al., 2010). However, emerging adults are lumped together with older ages in these analyses. We therefore need more specific information about the health status of emerging adults and the factors that may influence psychological health.
In many life domains of emerging adults (such as love, work, residential independence, and identity), fluctuations and discontinuities have been documented (Shulman, Feldman, Blatt, Cohen, & Mahler, 2005; Sneed, Hamagami, McArdle, Cohen, & Chen, 2007), and the frequent changes and explorations of life directions have resulted in, for some, an increase in health problems and risk behaviors (Gralinski-Bakker et al., 2005; Skaletz & Seiffge-Krenke, 2010). Specifically, difficulties in identity formation have been established as risk factors for psychopathology in a number of studies that have investigated emerging adults in Western industrialized countries (Kroger & Marcia, 2011; Luyckx et al., 2008). Furthermore, Lemoyne and Buchanan (2011) showed that dysfunctional parenting in some Western countries adds to the difficulty in becoming independent and establishing a separate identity, which contributes to an increased symptom level of emerging adults.
Trends in empirical research about emerging adulthood revealed psychological health as an important topic (Svandson, 2016), but only 4% of studies included samples from countries other than the United States. This study, therefore, explores psychological health in emerging adults from seven countries, focusing on identity-related risk factors. Although identity challenges are universal, their impact is perhaps different across countries. Similarly, individual coping style and parenting behavior in the context of identity formation may have an impact on emerging adults’ psychopathology, and this impact may differ depending on cultural practices and values.
Psychopathology and Identity in Emerging Adulthood
Emerging adulthood is a critical juncture in the development of psychopathology (Schulenberg, Bryant, & O’Malley, 2004; Schulenberg, O’Malley, Bachman, & Johnston, 2000). Many symptoms are clearly diagnosable for the first time (such as personality disorders), and trend analyses have demonstrated that anxiety disorders and depression have become more severe (Costello, Copeland, & Angold, 2011; Gutman & Sameroff, 2004). Furthermore, concurrent with greater freedom and less control during this developmental stage, an increase in substance use and externalizing symptoms was reported (Stone, Becker, Huber, & Catalano, 2012).
In the context of our research, it is important to note that identity has been integrated as a central diagnostic criterion for several disorders in Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). Erikson (1968) has defined identity as “a sense of one’s self, resulting from the integration of past, present and future experiences” (p. 36), emphasizing that identity includes both continuity and change. Because of greater mobility, increasing freedom of choice with respect to apprenticeships, jobs, romantic partners, and ideologies, identity formation in modern Western societies is increasingly stretching beyond the adolescent ages into the period of emerging adulthood (Arnett, 2007) and is characterized by extended exploration and less commitment compared to earlier decades (Kroger, Martinussen, & Marcia, 2010).
Already in the early works of Erikson (1950), identity was inherently linked with psychopathology. Decades of research have substantiated that different aspects of identity were associated with varying aspects of psychopathology (see, for a summary, Klimstra & Denissen, 2017). Acknowledging a potentially difficult and lengthy development process, concepts such as identity conflicts and identity confusion have recently been integrated in the DSM-5 diagnostics. Identity conflicts and identity diffusion contribute to many disorders such as eating disorders, personality disorders, self-harming behavior, or depression and anxiety (Lillevoll, Kroger, & Martinussen, 2013; Schmeck, Schlüter-Müller, Foelsch, & Doering, 2013).
The study of psychopathology in emerging adults from different countries calls for standardized instruments, which assess data at the symptom level. The Young Adult Self Report (YASR; Achenbach, 1997), which was used in this study to assess the mental health status in a large cross-cultural sample, has been developed as a screening instrument for psychopathology, including a broad range of syndromes such as internalizing (e.g., anxious/ depressed) and externalizing (e.g., delinquent/aggressive) syndromes. The YASR has been widely used in many countries with good reliability (Ivanova et al., 2015). The self-ratings fit an eight-syndrome model previously derived from the self-ratings of American participants, and the broad range of syndromes has been replicated. Across countries, females obtained higher scores in symptomatology than males (Agrez, Metzke, & Steinhausen, 2011).
Rescorla et al. (2007) demonstrated enormous variations in mean level of total psychopathology but also of internalizing and externalizing symptoms in adolescents from 24 different countries. In contrast to studies on adolescents, mean levels of psychopathology in emerging adults from different countries are lacking. Instead, studies have included emerging adults in the age range of adult participants (e.g., 18–59 years; Ivanova et al., 2015), showing high diversity in symptom levels across 29 countries.
Studies on emerging adults’ psychopathology in different countries are urgently needed because societal changes may impact the psychological health of emerging adults differently across the world. Compared to earlier decades, current life conditions in most Western industrialized countries are characterized by new career options but also by greater uncertainty in career planning (Arnett, 2002; Schoon & Silbereisen, 2009). Although such societal changes may be perceived as identity challenges in the positive sense, they may impair identity formation and lead to more identity conflicts and extended exploration in the field of love and work (Bynner, 2002; Schwartz, 2012; Seiffge-Krenke & Luyckxs, 2014). Emerging adults in other parts of the world may be experiencing political unrest, facing unclear future options, or living in poverty (Larson, 2011; Tiede Call et al., 2002). They have less freedom to personally choose their future lives and explore their identity and may experience a strong gap between intended and realized identity goals.
Studies in psychopathology on emerging adults from different countries than the United States or Europe are missing (Svandson, 2016). Research two decades ago revealed stability coefficients for European emerging adults of .63 for males and .75 for females. The impact of societal changes on identity formation is highly likely and could contribute differently to levels of psychopathology in emerging adults from different countries (Schulenberg et al., 2000). Therefore, the long-term consequences of rising or changing levels of symptomatology for the individual and the society should be considered. For a substantial proportion of emerging adults who struggle with identity formation and develop psychopathological symptoms, continue with symptomatology, or show an increase in already existing psychopathology, adverse outcomes in terms of occupation, social integration, economic prospects, and future health are to be expected. For example, emerging adults who develop an internalizing disorder or show an increase in depression and anxiety during this developmental phase are at higher risk of economic hardship and dependency on parents or the welfare system (Melkevik, Nilsen, Evenson, Reneflot, & Mykletun, 2016). Untreated externalizing symptoms result in further delays in identity development (Crocetti, Klimstra, Hale, Koot, & Meeus, 2013), which reinforces higher levels of externalizing behavior in the long term.
The impact of culture on psychopathology of emerging adults in different countries is not yet clear. To date, studies on adults in several countries around the world revealed strong country-specific differences (Ivanova et al., 2015), but whether these differences also apply to the age-group of emerging adults needs to be explored. Furthermore, the extent that cultural aspects (e.g., specific values, norms, and family traditions) play a role in this process is still unclear. Of note, the concept of culture-bound syndromes was replaced by cultural concepts of distress in DSM-5, suggesting that many disorders can no longer be regarded as culturally typical Western disorders because of globalization.
Placing Identity Stress, Coping, and Parental Behavior in a Broader Cultural Context
The development of identity is one of the most important developmental processes during emerging adulthood, and the influence of a given culture as well as the active role of an individual in forming an identity is an open question (Arnett, 2002). Regarding the impact of a given culture, Oyserman, Coon, and Kemmelmeier (2002) demonstrated that the orientation toward independent or interdependent values represents a critical continuum along which a specific country is located. Most Western cultures (e.g., the United States and countries from Western Europe) show a greater orientation to individualism, characterized by the encouragement of autonomy from parents and personal choice of occupation and romantic partner (Persike & Seiffge-Krenke, 2012). Other cultures (e.g., in the Far East and in Latin American countries) value harmony and interdependence among family members and place less value on individual identity exploration in work and in love.
However, the individuals’ agency also may play a role in how identity challenges are dealt with. In general, identity development is a normative task and may not necessarily be experienced as stressful. What is perceived as stressful and how an individual cope with it is influenced by the prevailing value system for social interactions, for example, cultural aspects may have a bearing on what coping strategies emerging adults use to deal with stressors associated with the identity domain (Seiffge-Krenke & Haid, 2012). We focused in this study on perceived stressfulness in the process of identity formation, for example, on identity stressors such as a strong motivation to discover one’s needs, perceived difficulty in obtaining a desired employment, and insecurity about career choice and the family and work–life balance as potential risk factors for emerging adults’ psychopathology. We suspect that these identity stressors have increased during the last decade, as roles (e.g., job, gender, and family) are currently less clearly defined and a greater social and economic ambiguity might have resulted in the passage to adulthood becoming more unpredictable for emerging adults. Furthermore, a worldwide decrease in job security render that an individual’s coping with relevant identity stressors is not necessarily followed by success (Arnett, 2002; Bynner, 2000).
Thus, investigating the efforts that emerging adults in different countries undertake to cope with identity stressors is important. Although most young people succeed with these issues, others may have severe difficulties in making the transition to various adult roles and establishing a mature identity. Overall, coping capacities of emerging adults seem to be quite adaptive (Skaletz & Seiffge-Krenke, 2010). However, empirical evidence indicates that strong identity stressors during the transition to adulthood may overwhelm already compromised coping capacities (Schulenberg et al., 2004). Adaptive coping styles (e.g., actively tackling the issues at stake and the reflection about possible solutions) are a prerequisite for successful progress across emerging adulthood (Lam, & McBride-Chang, 2007). Coming to terms with identity-related stressors may vary, depending on life circumstances and the prevailing cultural norms. To the best of our knowledge, no study to date has controlled for identity stress and coping as risk factors for differences in psychopathology in emerging adults across countries.
Of further interest for the present study are three key aspects of parenting in the context of identity formation, which researchers have linked to negative child outcomes in Western industrialized countries. In recent years, parents have become increasingly involved in their children’s lives in many Western countries. First, the impact of parental support is unclear because research suggests that parental support is like a two-sided sword. Poor parental support has been identified as a risk factor for depressive symptoms. Several longitudinal studies found that an increase in parents’ support is associated with a decrease in depressive symptoms (Beyers & Seiffge-Krenke, 2007; Galambos, Barker, & Krahn, 2006; Fingerman, Cheng, Tighe, Birditt, & Zarit, 2012). Conversely, research has also shown that too much parental support may lead to negative outcomes for their offspring. Several studies indicate that too much parental involvement is associated with higher levels of depression and anxiety (Lemoyne & Buchanan, 2011; Schiffrin et al., 2014), with adult children reporting feeling less competent and more vulnerable to stressors (Hofer & Moore, 2010; Marano, 2008).
Second, parental psychological control (e.g., parental behaviors that are intrusive and manipulative of children’s thoughts, feelings, and behavior; Barber, 2002) appears to have a negative impact on the psychological health of the offspring. Emerging adults of parents, who are psychologically controlling, exhibit both externalizing and internalizing symptoms and are impaired in their identity development (Luyckx, Soenens, Vansteenkiste, Goossens, & Berzonsky, 2007). Third, anxious child-rearing practices should be explored. Anxious rearing or overparenting can hinder the development of coping competence and subsequently lead to increased levels of stress (Segrin, Woszidlo, Givertz, Bauer, & Taylor Murphy, 2012), which is a risk factor for the development of psychopathology. Such hovering parental behavior has been found in samples in central Europe and in North America (Kins, Beyers, & Soenens, 2013; Lemoyne & Buchanan, 2011; Padilla-Walker & Nelson, 2012).
Research is still lacking on whether certain parenting styles that have been found to represent individualistic ideals and norms in Western societies apply to parents in other countries, for example, to parents living in collectivistic cultures (Batool & Mumtaz, 2015; Georgas, Berry, van de Vijver, Kagitcibasi, & Poortinga, 2006). When analyzing emerging adults’ psychopathology across countries, the impact of different levels of support, psychological control, and anxious rearing on psychopathology needs to be controlled. We were therefore interested in studying, after controlling for these risk factors, the extent that country still affects psychopathology in emerging adults in seven countries from Western and non-Western cultures and the extent that gender plays a role.
The Present Study
The main purpose of this study was to examine the mental health of emerging adults living in different cultural contexts around the globe by controlling the influence of potential risk factors pertaining to identity issues. We addressed this research question within the context of the increasing incidence of identity aspects in disorders and the presumed great variation in identity-related risk factors in emerging adults from different parts of the world. For our study, we selected identity stressors, dysfunctional coping styles, and dysfunctional parental behaviors as factors that may impair identity development. While coping with identity-related stressors focuses on the agency perspective in this context, parental behavior focuses on the relationship aspects of identity formation. We suspect that high identity stress or a more dysfunctional coping style in coming to terms with identity-related stressors is associated with psychopathology. In addition, dysfunctional parental behavior may be considered as a risk factor and may contribute to psychopathology, but this impact may not be uniform across countries. Together, we suspect that these identity-related risk factors may contribute differently to emerging adults’ psychopathology, depending on the country.
We approach our aim by investigating emerging adults from seven countries throughout the world (e.g., France, Germany, Turkey, Greece, Peru, Pakistan, and Poland). We included two developing countries with a recent, strong growth in education and its economy (Pakistan and Peru). Both can be considered as “tight cultures,” that is, as characterized by consistent child-rearing practices and strong social and gender norms for individual exploration (Gelfand et al., 2011). In Peru, parenting seems to be characterized by warmth and permissiveness (Welti, 2002), whereas emerging adult children in Pakistan are expected to respect and submit to their parents regarding their individual strivings (Ijaz & Mahmood, 2009). In addition, we selected two countries with recent political and economic changes (Turkey and Greece), which are characterized by relatively strong parent–child bonding. Emerging adults in Greece, and to a lesser extent in Turkey, are raised in a culture that assigns great importance to family values and relations, but they are also encouraged to develop an independent self (e.g., arguments with parents are not avoided; see Georgas et al., 2006). We further included three countries from Europe (France, Germany, and Poland), where parenting practices and identity stress are more varied despite their regional vicinity. In France, the family constitutes a main value and a national issue. Family life is important for all generations and interdependence, as family values were related to life satisfaction for each generation (Sabatier & Lannegrand-Willems, 2005). Family and collectivistic orientations, but also nationalism, are stronger in Poland than in France or Germany. Nonetheless, many, especially family- and individual-level differences, seem to be systematically diminishing in Poland due to ongoing social change since 1989. In Germany, individualistic values clearly prevail with family matters being less important than individual aims and strivings with respect to identity (Seiffge-Krenke & Haid, 2012).
In our sample of countries, further differences exist with respect to religious values, job security, and gender equality. Pakistani and Turkish emerging adults are predominantly of Muslim faith, but Poland, Peru, and Greece youth are mostly Catholic. Emerging adults in Germany and France, however, show little religious bonding, whereas for Polish, Greek, and Peruvian young people, religiosity is an important value. Youth unemployment rates also differ, which are relatively low in Germany and France but quite high among emerging adults in Pakistan, Peru, and Poland (OECD, 2015). Furthermore, Pakistan and Turkey face challenging problems including terrorism, poverty, illiteracy, and corruption. Women are markedly disadvantaged in Pakistan. Nearly all family or public affairs are settled by men, and free choice in the domain of love and work is rare.
Although fathers are certainly important for emerging adults’ adaptation (Cassano, Adrian, Veits, & Zeman, 2006), we restricted our research to emerging adults’ perception of maternal parenting style. Several studies have demonstrated that the relationship with mothers remains closer when children become emerging adults, and it involves higher levels of support than relationships with fathers (Fingerman et al., 2012; Seiffge-Krenke, Overbeek, & Vermulst, 2010). Further research has shown that mothers in general were more overprotective than fathers (Fingerman, Miller, Birditt, & Zarit, 2009). We restricted our samples to sizes of about 300 per country and to the age range of 20–24 years. Hence, the emerging adults we investigated, all university students, lived in comparably modern urban environments. Nevertheless, differences might still exist in identity stress, coping, and related parenting style, which need to be statistically controlled when assessing country-specific differences in psychopathology.
Research Questions and Hypotheses
We aimed to investigate country-specific variations in psychopathology before and after controlling for identity-related risk factors. We assessed emerging adults’ psychopathology and explored differences in identity stress, coping with identity stress, and maternal parenting style as reported by emerging adults in the seven countries. Based on earlier research that showed substantial cross-country differences in stressors and coping in the relationship domain (Persike & Seiffge-Krenke, 2015) and in future-related issues (Seiffge-Krenke et al., 2012), we controlled for the impact of identity stress and coping on emerging adults’ psychopathology. We expect, based on this earlier research on adolescent samples, that the impact of identity stress on psychopathology is stronger than the impact of coping and, additionally, that these identity-related risk factors may contribute differently to emerging adults’ psychopathology, depending on the country. We further expected to find variation in emerging adults’ perception of maternal parenting behavior, measured as maternal support, psychological control, and anxious rearing, which was important to statistically control to get a clearer picture of country effects on levels of psychopathology. We expect, in accordance with earlier studies (Barber, Stolz, Olsen, & Maugham, 2005; Kins, Soenens, et al., 2013), that anxious rearing and psychological control should be associated with internalizing and externalizing psychopathology differently in all countries with a stronger impact in Western countries. Additionally, we expect that after controlling for these identity-related risk factors, a different picture about the scores in internalizing and externalizing might emerge than without controlling. Due to the lack of research in this domain, we cannot offer more specific hypotheses about country-specific variations after controlling for identity-related risk factors.
Several earlier studies pointed to strong gender differences, for example, in identity development (Cramer, 2000; Kroger et al., 2010) and in psychopathology (Agrez et al., 2011; Ivanova et al., 2015), reporting that females are more advanced in their identity development and they report higher levels of psychopathology, mostly of internalizing disorders. Studies comparing stress and coping style across countries also found strong gender differences, with females generally scoring higher in several stressors (Persike & Seiffge-Krenke, 2015; Wong & Wong, 2006), and they use negotiating and support seeking as a means of coping more often than males did (Seiffge-Krenke, 2011; Tamres, Janicki, & Helgeson, 2002).
To address the impact of stress, coping, and maternal behavior as covariates on the relationship between country, gender, and psychopathology, we conducted two blocks of analyses. First, we analyzed gender- and country-related effects on psychopathology without partialing out the covariates. We expected considerable variation in psychopathology between countries. Moreover, based on the research conducted by Ivanova et al. (2015), we expected the effects of country on psychopathology to be more pronounced than the effects of gender. The second block of analyses was conducted after partialing out identity- and parenting-related covariates at the country level to gain a more genuine picture of gender- and country-specific effects on psychopathology.
Method
Participants
Data were collected from a sample of 2,113 emerging adults from seven countries (France, Germany, Turkey, Greece, Peru, Pakistan, and Poland). Table 1 provides an overview of the sample’s demographics according to country. Mean age and age variance were reasonably well balanced among the samples (M = 22.0, SD = 2.04). The gender ratio was also well balanced for all countries except Turkey where 87% of participants were female. There were marked differences in family structure and size between countries. Most emerging adults from Turkey (91.9%), Pakistan (88.9%), and Germany (88.8%) lived in two-parent families; emerging adults from France reported the lowest rate of two-parent families (60.4%). The number of children per family varied widely across countries, with the lowest found in Germany (M = 1.10), Greece (M = 1.40), and Peru (M = 1.40) and the highest in Pakistan (M = 3.60). Romantic partner status varied between 31.4% (Pakistan) and 91.9% (Turkey). The living situation was also quite diverse. The lowest percentage of emerging adults still living with their parents was reported in Germany (4.5%), and the highest was reported in Pakistan (86.8%). Turkish participants reported the lowest rate (4.9%) of residing with their romantic partners, and the highest rate was reported in France (19.1%). Most Germans (89.1%) and few Pakistanis (11.8%) lived alone or in some form of cohabitation.
Sample Demographics According to Country.
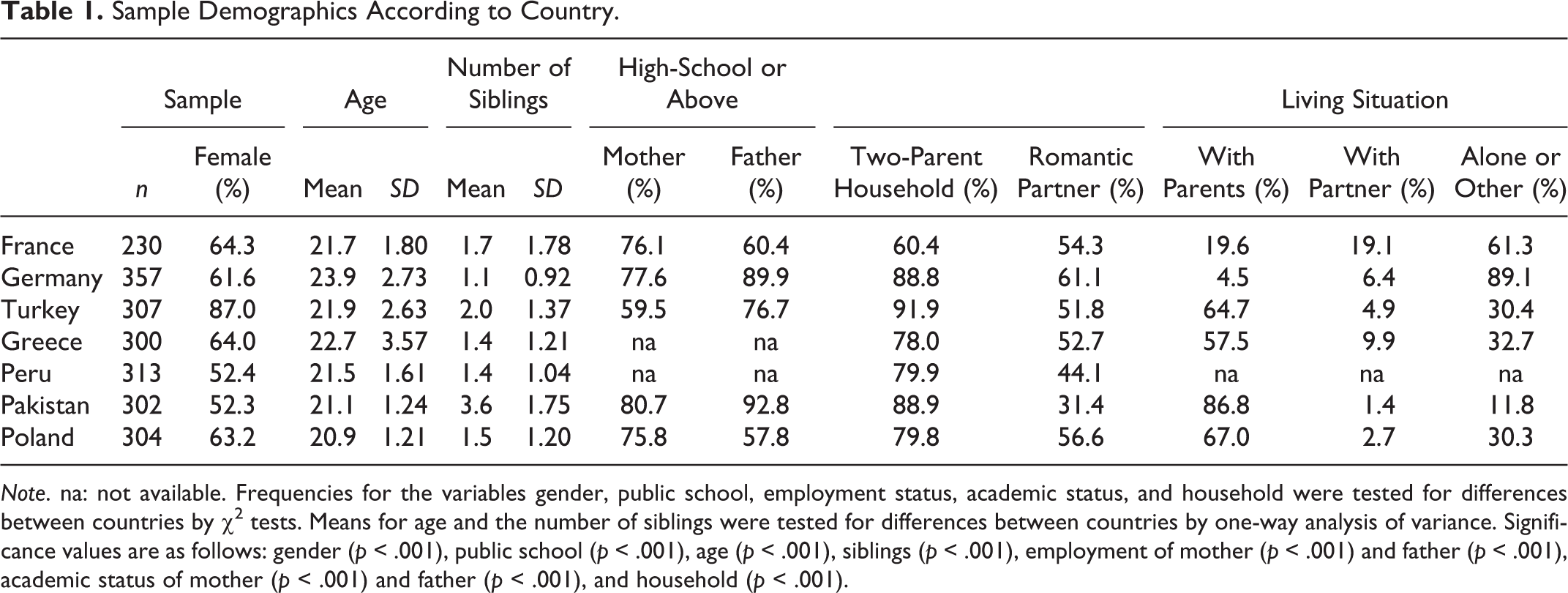
Note. na: not available. Frequencies for the variables gender, public school, employment status, academic status, and household were tested for differences between countries by χ2 tests. Means for age and the number of siblings were tested for differences between countries by one-way analysis of variance. Significance values are as follows: gender (p < .001), public school (p < .001), age (p < .001), siblings (p < .001), employment of mother (p < .001) and father (p < .001), academic status of mother (p < .001) and father (p < .001), and household (p < .001).
Instruments
Internalizing and externalizing symptom score
Psychopathology was assessed by YASR (Achenbach, 1997), a 110-item, self-report scale that measures emotional and behavioral problems, with a ternary answer format (1 = not true, 2 = somewhat or sometimes true, 3 = often or very often true). The YASR includes a broad array of syndromes of externalizing (e.g., delinquent, aggressive) and internalizing behavior (e.g., anxious/depressed, withdrawn). The YASR has been used frequently across countries with good reliability (see Agrez et al., 2011).
Identity-related stress
Emerging adults’ stress was measured with the Problem Questionnaire (PQ; Seiffge-Krenke, 1995), which assesses the perceptions of minor stressors in seven stress domains (study, job, family, peers, romantic partner, identity, and future). The instrument consists of 64 typical and salient everyday stressors that participants rate on a 5-point scale (1 = not stressful at all to 5 = highly stressful). In the present study, we used 9 items pertaining to the domain of identity-related stress (e.g., a strong motivation to discover one’s needs, perceived difficulty in obtaining desired employment, and insecurity about career choice and family and work–life balance). A sample item is, “I found it difficult to discover what profession really suits me.” The PQ has been used frequently across countries with good reliability (e.g., Seiffge-Krenke et al., 2012).
Coping with identity-related stress
Participants completed the Coping Across Situations Questionnaire (CASQ; Seiffge-Krenke, 1995), which assesses 20 coping strategies across seven problem domains on a binary scale (0 = strategy not used, 1 = used). For the present study, we selected the identity domain to complement the stress domain. Three different coping styles are assessed. The first style, termed Negotiating and Support Seeking, comprises 9 items such as “I discuss the problem with my parents” or “I try to solve the problem with the help of my friends.” The second style, termed Reflection, includes 6 items such as “I think about the problem and try to find a solution.” The third style, termed Emotional Control, is measured by 5 items such as “I try to preserve my countenance.” The CASQ has been used frequently across countries with good reliability (e.g., Persike & Seiffge-Krenke, 2015).
Perceived maternal behavior
Participants completed an instrument that comprised 17 items, assessing a variety of aspects of perceived maternal behavior, which are rated on a 5-point scale (1 = not applicable to 5 = very appropriate). Five items stemmed from the adolescent family process (AFP) measure (Vazsonyi, Hibbert & Snider, 2003) were selected assessing maternal support such as “My mother often supports me.” Six items that assess maternal psychological control were used from Barber (2002). An example item is, “My mother no longer talks to me when I disagree with her.” The final 6 items were from a measure designed by Kins, Beyers, and Soenens (2013) to measure parental overprotection, in particular anxious monitoring. An example item is, “My mother monitors each of my steps, if I want to be alone.” Reliability in the current sample amounted to α = .83 for maternal support, α = .79 for maternal psychological control, and α = .81for anxious rearing.
Procedure and Data Acquisition
Senior and junior researchers from all seven countries translated the Perceived Maternal Behavior Scale into the official language of each country and then back into English. As stated above, the PQ and the CASQ had already been translated and used in previous cross-cultural studies (Persike & Seiffge-Krenke, 2015; Seiffge-Krenke et al., 2012).
Measurement invariance (MI) analyses are available for all instruments used in the study. MI has been assessed for the stress and coping inventories in numerous studies (Persike & Seiffge-Krenke, 2012, 2015; Seiffge-Krenke et al., 2012). The YASR has been used in various countries, including MI analyses (Fonseca-Pedrero, Sierra-Baigrie, Lemos-Giráldez, Paino, & Muñiz, 2012), with satisfactory results. Likewise, the AFP has been successfully evaluated for MI (Vazsonyi et al., 2003; see also Vazsonyi et al., 2010).
In all countries, the assessments were conducted on students in university cities to limit variance caused by differences in education and urbanization. The study was approved by the ethics board in each country. Participants were recruited by several means, including flyers, placards, and leaflets in central university facilities, as well as by in-class announcements. Participants were not provided with incentives to participate. Consent forms were sent to the participants several days prior to data collection. Written consent to participate in the study was provided by 90% of the emerging adults who showed initial interest in participating. About 13% of emerging adults were absent on the day of assessment, resulting in a low overall dropout rate of about 23%. All assessments were conducted on whole seminar levels.
Plan of Data Analysis
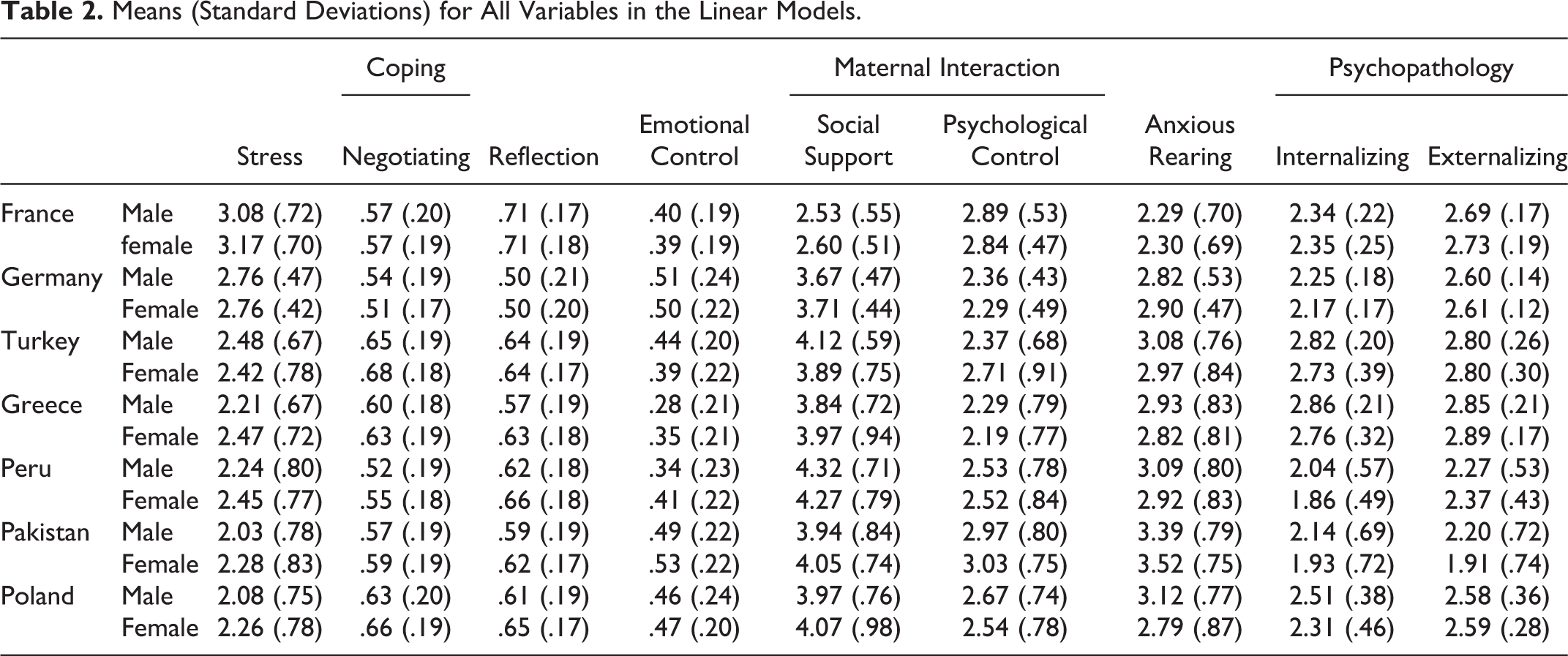
After data acquisition, scale scores for all analysis variables were computed as arithmetic means of the comprised items. Sample descriptives in Table 2 are based on these scores. Data sets with missing values for the analysis variables were excluded from further consideration, which pertained to less than 2.1% of all data sets. Multivariate outlier detection was performed individually for each country by computing the Mahalanobis distance for each data set based on a selected set of variables and by excluding data sets outside of a .999 confidence region around the country centroid based on the χ2 distribution. This led to the exclusion of an additional 0.7% of all data sets.
Means (Standard Deviations) for All Variables in the Linear Models.
Psychopathology variables were then entered as dependent variables into a multivariate analysis of variance (MANOVA), with gender and country as factors. With the same factors, the effects for single dependent variables were then tested by separate two-way analyses of variance (ANOVAs). Pairwise differences were tested with Tukey’s HSD post hoc tests. Variance explained was computed as an effect-size measure. Analyses were run on both the crude psychopathology scores and residual psychopathology scores for which the effects of stress level, coping style, and perceived maternal behavior had been partialed out.
To obtain partialed out scores, we regressed the two psychopathology variables, internalizing symptoms and externalizing symptoms, on the covariates (a) stress level, (b) coping styles (negotiating and support seeking, reflection, and emotional control), and (c) perceived maternal behavior (support, psychological control, and anxious rearing) separately for each country. These regression analyses yielded regression residuals for the two psychopathology variables for which the three covariates were partialed out. By using this procedure (see Seiffge-Krenke et al., 2018), we could analyze the effects of stress level, coping style, and maternal behavior, which were expected to be considerably different across countries (Barber, 2002; Persike & Seiffge-Krenke, 2015). Such differential influences cannot be modeled in an analysis of covariance. Hence, we decided to partial out the covariates on a per country level (see Miller, Yu, Chen, & Brody, 2015). We call the original psychopathology variables crude scores and the regression residuals partialed scores. Effects of gender and country on psychopathology were tested on both crude and partialed scores.
Results
Regression of the Psychopathology Variables on the Covariates Stress, Coping, and Maternal Behavior
Descriptive statistics for crude scores are summarized in Table 2. Correlations between the symptomatology variables and the covariates stress, coping, and maternal support are summarized in Table 3.
Correlations Between all Covariates and Dependent Variables in the Linear Models.
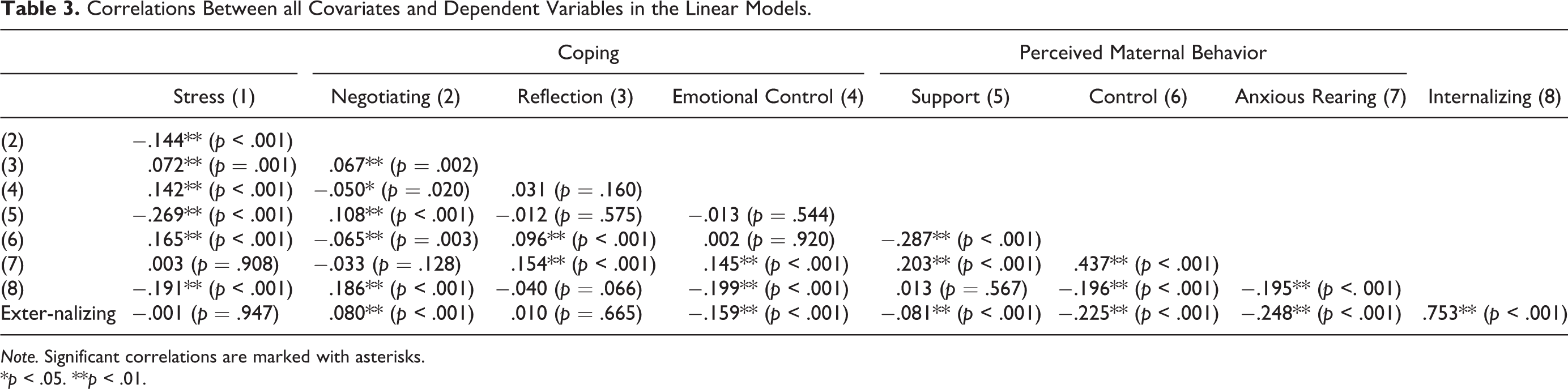
Note. Significant correlations are marked with asterisks.
*p < .05. **p < .01.
Regression analyses show that, with the exception of reflective coping (p = .115), all other continuous predictor variables were significantly related to internalizing symptoms (multivariate R = .360). Specifically, this pertains to identity-related stress (b = .14, p < .001, partial η2 = .027), maternal support (b = −.06, p = .009, partial η2 = .001), maternal psychological control (b = .12, p < .001, partial η2 = .023), anxious rearing (b = .11, p < .001, partial η2 = .021), and coping with identity-related stress by negotiating and support seeking (b = −.16, p < .001, partial η2 = .031) and emotional control (b = .14, p < .001, partial η2 = .027). Regression weights indicate that only a higher tendency to engage in negotiating and support-seeking behavior was negatively related to internalizing symptomatology. Identity-related stress, maternal psychological control, anxious rearing, and coping by emotional control were positively related with internalizing symptoms, whereas maternal support was negatively related with internalizing symptoms.
Externalizing symptoms were also predicted by maternal support (b = −.12, p < .001, partial η2 = .009), maternal psychological control (b = .19, p < .001, partial η2 = .043), anxious rearing (b = .12, p < .001, partial η2 = .031), and coping by negotiating and support seeking (b = −.09, p < .001, partial η2 = .007) and emotional control (b = .12, p < .001, partial η2 = .018). As already observed for internalizing symptoms, only a negotiating and support-seeking coping style was negatively correlated with symptomatology. Identity-related stress (p = .227) and reflective coping (p = .434) did not contribute significantly to the prediction of externalizing symptoms (multivariate R = .329).
Psychopathology Scores Before and After Partialing Out Covariates
Mean total scores and residual means for the crude and partialed psychopathology scores are summarized in Table 2 (before partialing in last three columns) and Table 4 (after partialing). The effects of country and gender on crude and partialed out psychopathology variables were first analyzed by performing MANOVA routines, with country and gender as factors.
Mean Total Scores for Psychopathology Variables and Residual Means after Controlling for the Effects of the Continuous Predictor Variables Stress, Coping, and Perceived Maternal Behavior.
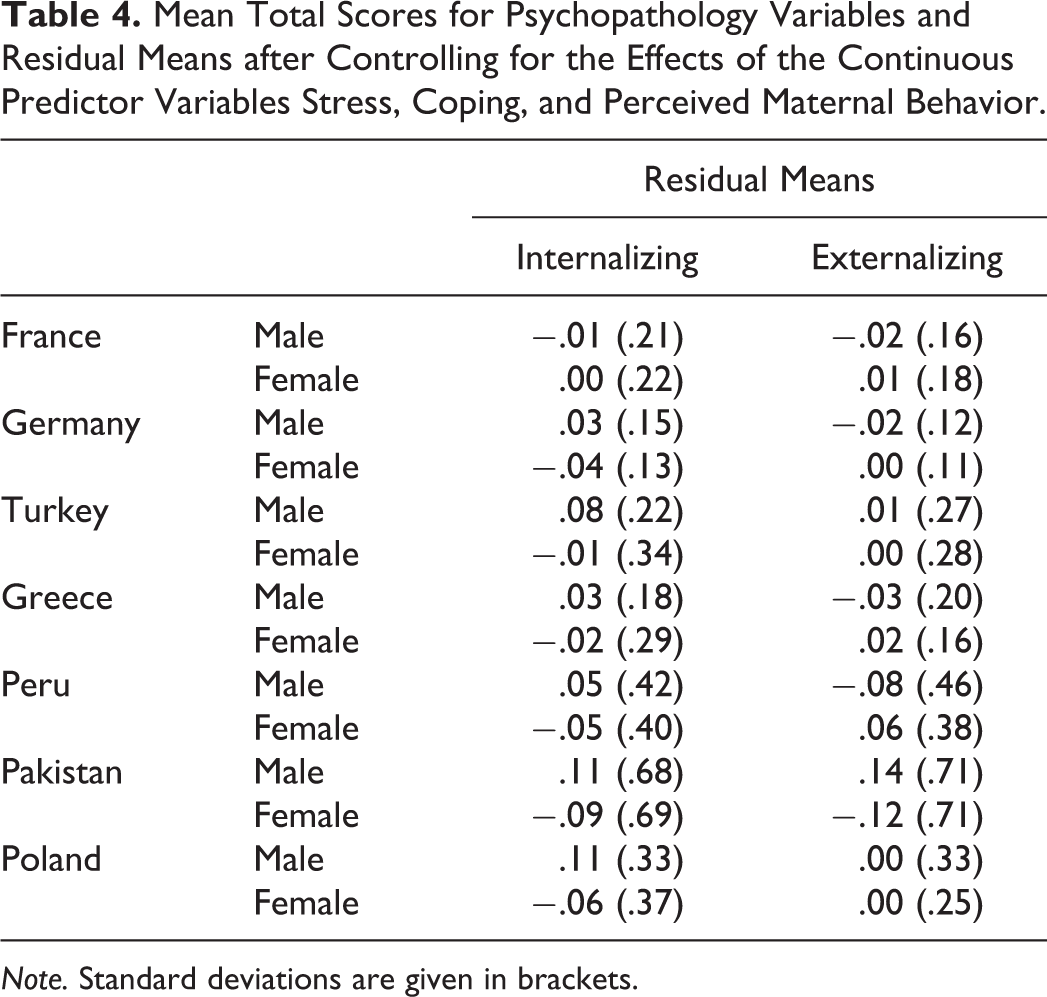
Note. Standard deviations are given in brackets.
Before partialing out psychopathology variables, we obtained highly significant effects of country (Wilks’s λ = .55, df = 12, 4050, p < .001) and gender (Wilks’s λ = .97, df = 2, 2025, p < .001) on psychopathology, and a highly significant Gender × Country interaction (Wilks’s λ = .96, df = 12, 4050, p < .001). After partialing out the psychopathology variables, we still found overall effects of gender (Wilks’s λ = .98, df = 2, 2025, p < .001) on levels of psychopathology and a highly significant Gender × Country interaction (Wilks’s λ = .96, df = 12, 4050, p < .001), but no effect was found for country. In the remainder of the Results section, effects are analyzed individually for each of the two psychopathology variables by means of ANOVA, with country and gender entered as factors.
Internalizing Symptoms
Crude scores
We observed significant effects on unpartialed internalizing symptom scores for country, F(6, 2026) = 152.0; p < .001; partial η2 = .310, and for gender, F(1, 2026) = 33.8; p < .001; partial η2 = .016. A highly significant interaction effect of Country × Gender was also found, F(6, 2026) = 2.18; p = .042; partial η2 = .006. Results are summarized in Figure 1. Self-reports of internalizing symptoms fell into three distinct groups. Scores were highest in Turkey and Greece, followed by France and Poland, and lowest in Germany, Peru, and Pakistan. This pattern of results was corroborated by significant pairwise post hoc tests between countries across the three groups (all pairwise p < .001). Overall, males reported higher levels of internalizing symptoms than females. This result, however, applied to only some countries as indicated by the significant interaction. Internalizing psychopathology reported by male and female participants was very similar in France, Germany, Turkey, and Greece (all pairwise p > .81), whereas in the remaining countries, males reported substantially higher scores (all pairwise p < .02).

Mean total scores (left) and regression residuals (right) for internalizing symptomatology according to country and gender. Error bars indicate 95% confidence intervals.
Partialed scores
After partialing out the influence of stress, coping, and perceived maternal behavior, a considerably different picture emerged. Country no longer exerted a significant effect on symptom scores (p = .936). The significant effect for gender remained, F(1, 2026) = 25.7; p < .001; partial η2 = .013, as well as a marginally significant Country × Gender interaction, F(6, 2026) = 2.32; p = .031; partial η2 = .007. As with the crude score analysis, males reported higher internalizing symptomatology scores, on average, than females. As indicated by the significant interaction, this result applied to only some of the countries. Scores were different in Peru, Pakistan, and Poland (all pairwise p < .03) but similar in France, Germany, Turkey, and Greece (all pairwise p ≥ .10).
Externalizing Symptoms
Crude scores
We found significant effects on crude externalizing symptom scores for country, F(6, 2026) = 145.0; p < .001; partial η2 = .300, but not for gender (p = .604). A significant interaction effect of Country × Gender was also found, F(6, 2026) = 7.47; p < .001; partial η2 = .022. Results are summarized in Figure 2. Scores were highest in Greece and Turkey, followed by France and Germany, and lowest in Poland, Peru, and Pakistan. This result was corroborated by significant pairwise post hoc tests between countries in the three groups (all pairwise p < .01). Externalizing symptoms were similar for male and female participants in most countries except for Pakistan where males reported substantially higher scores than females (pairwise p < .001).

Mean total scores (left) and regression residuals (right) for externalizing symptomatology according to country and gender. Error bars indicate 95% confidence intervals.
Partialed scores
Partialing out stress, coping, and perceived maternal behavior erased almost all differences between countries (p = .991) and gender (p = .808), whereas the interaction effect of Country × Gender remained significant, F(6, 2026) = 8.65; p < .001; partial η2 = .025. This result was due to the highly different symptom scores reported by Pakistani and Peruvian emerging adults. Males and females exhibited similar externalizing symptom scores in most countries (all pairwise p ≥ .99), whereas the difference remained largely unchanged in Peru (p = .040). Only in Pakistan was the gender difference significant, with males reporting much higher values than females (p < .001).
Discussion
Evidence on differences in mental health among different countries is substantial for practitioners and researchers in the context of public health care. In addition, existing cross-cultural research on emerging adults’ psychopathology has rarely considered potential risk factors that may vary depending on the country. Because of increasing identity-related disorders and because identity formation is a central developmental task, this study explored the psychological health of emerging adults living in seven countries around the globe after partialing out identity-related variables. Similarly, the effect of different maternal parenting styles, which might influence the offspring’s psychopathology, was partialed out. Controlling for parenting behavior might imply controlling for cultural influences when assuming that culture influences parental behavior. The between-country differences observed in this study after partialing out the covariates will be interpreted accordingly.
Variations in Identity-Related Risk Factors
An inspection of the descriptives showed higher variability in some variables. Of note, identity stress was perceived as quite high in emerging adults from France, Germany, Greece, and Turkey. This is in accordance with studies showing high vocational identity stress in emerging adults in France (Lannegrand-Willems, Percec, & Marchal, 2015), Germany (Seiffge-Krenke & Haid, 2012), and in many other countries suffering from recession such as Greece (United Nation International Childrenś Emegency Fund [UNICEF] Office of Research, 2014). In contrast, the coping style of emerging adults from all seven countries was quite uniformly characterized by high levels in negotiating and reflection about possible solutions, showing a good balance between the two adaptive coping styles, a finding so far reported only for German emerging adults (Haid et al., 2010). Despite different political, social, and family backgrounds as well as varying stress levels, emerging adults throughout the world use very similar strategies to cope with identity-related stressors. More divergence has been found with respect to emotional control, suggesting that culture-specific standards for an open outlet of emotions also prevail (Kagitcibasi, 2005a; Wong & Wong, 2006). Overall, coming to terms with identity-related stressors and the adaption to a “disorderly world” (Larson, 2011) is impressive in youth from all countries. This information is important to consider when designing culture-specific forms of intervention and treatment.
We also found country-specific variation in maternal parenting. In accordance with other studies, we noticed quite high levels of perceived maternal support reported by emerging adults from Peru and Turkey, for example, from countries considered to share collectivistic parenting practices (Kagitcibasi, 2005b). Remarkable are the high scores in psychological control reported by Pakistani emerging adults. These scores, which in an individualistic culture (e.g., Europe and North America) is associated with higher symptom scores (Barber, 2002; Kins, Soenens et al., 2013), seemed to not have the same negative impact in youth from other countries such as Pakistan (Ijaz, & Mahmood, 2009). Of note are the quite low scores in anxious rearing in emerging adults from France, which corresponds to earlier findings by Claes, Lacourse, Bouchard, and Perucchini (2003) who reported that French parents monitor less compared to Canadian and Italian parents. In sum, we found sufficient variation with respect to potential risk factors for emerging adults’ psychopathology in diverse countries.
When internalizing and externalizing scores were regressed on the covariates identity stress, coping with identity stress, and maternal parenting behavior on the overall sample, a clear pattern emerged. With the exception of the two adaptive coping styles, all other variables contributed significantly to symptomatology, with larger effect sizes for internalizing symptomatology. While negotiation and support seeking as a coping style served as a buffer, strong emotional control was, overall, associated with higher symptomatology.
Our findings revealed a significant impact of identity stress and certain maternal behaviors, especially psychological control and anxious rearing, on both psychopathology scores. These results suggest that, overall, the degree of dysfunctional maternal parenting was linked with psychopathology and that variations in identity stress were associated with levels of psychopathology. This pattern of results along with findings from samples in Central Europe and North America (Barber, 2002; Kins, Soenens et al., 2013; Luyckx et al., 2007) may generalize to samples from other countries.
Emerging Adults Psychopathology in Seven Countries: The Vanishing of Cultural Effects
We expected that identity challenges and the inability to cope with them, as well as maternal parenting, might differently contribute to psychopathology in youth in different countries. Of note, before controlling for these covariates, we found a clear pattern for internalizing symptomatology scores. Scores were highest in emerging adults from Turkey and Greece, followed by those from France and Poland, and were the lowest in Germany, Peru, and Pakistan. Emerging adults from Turkey and Greece are coming from two geographically close countries that, despite family and belief differences, were extremely shaken by economic and political crises, leaving an unsure future for the young generation (Welti, 2002). A reasonable assumption is that the youth from these two countries would show very high symptom levels in internalizing symptoms. Moreover, emerging adults from Europe (e.g., France and Poland), who live in relatively safe conditions despite political and economic differences, have various possibilities to explore their identity and thus exhibit medium levels in psychopathology. Emerging adults from Germany share similar life conditions than their age mates in France and Poland but seem to experience less symptoms, a finding which might be related to the comparably high security for future prospects, at least as far as employment rates are considered (Seiffge-Krenke & Haid, 2012).
The comparably low symptom levels in youth living in unsecure societal conditions, such as in Pakistan, are astounding and may have different origins. We may speculate whether a collectivistic culture with its solid ideas about the future, as well as the role individuals play in the context of the extended family, can be considered as a protective factor, buffering against adverse life conditions. Thus, the overall value orientation in a given culture may determine what is perceived as stressful, which may consequently impact the level of psychopathology. In addition, differences in illness concepts and in the openness to disclose about symptoms may play a role. For example, women in Pakistan might not report symptoms because of fearing persecution.
After partialing out the covariates, a different picture emerged. Country no longer exerted a significant effect on symptom scores. This was an interesting finding, and it parallels the recent development in the diagnostics of psychopathology. The concept of culture-bound syndromes was abandoned in DSM-5 and replaced by cultural concepts of distress. This concept describes syndromes, modes of communication for stress, or cultural explanations and attributions. Ventriglio, Ayonrinde, and Bhugra (2016) interpreted the new concept as an expression of recognizing globalized communication and a change from cultural bound to culturally influenced. Research revealed that some of the so-called culture-bound syndromes also resemble each other in different cultures. Consequently, DSM-5 lists only nine mental disorders as culturally explainable (in contrast to 25 in the DSM-IV-TR). Similarly, Pike and Dunne (2015) claimed that some disorders, such as depression and eating disorders, can no longer be regarded as typical Western disorders and argue for a negative effect of Westernization.
It needs to be stressed, however, that some clinical evidence exists for specific cultural expressions of symptoms. Studies reported a high prevalence of idiopathic somatic complaints and syndromes (ISCS) in immigrant samples (Aragona et al., 2005), for example, a high prevalence rate of 50% ISCS in young adults with migration backgrounds in Germany (Morawa et al., 2017).
Emerging Adults Psychopathology in Seven Countries: Why Are Males More Vulnerable?
Partialing out identity-related risk factors alleviated almost all differences between countries. Instead, we found substantial evidence for gender effects and for an interaction between gender and country. In three of the seven countries, males reported higher symptom levels than females. Although the higher externalizing scores of Pakistani males compared with same-aged females are consistent with previous findings, the important and new findings of this study were the higher internalizing symptom scores in males from Peru, Pakistan, and Poland. Furthermore, in France, Germany, Turkey, and Greece, gender differences vanished after partialing out identity-related risk factors. These unexpected findings stand in contrast to the cross-cultural studies of the YASR reported by Ivanova et al., (2015) in which females reported higher scores compared to males in many of the 29 investigated countries; however, the age range in that study was large (18–59 years). Another consideration is that most studies on gender effects in symptomatology were conducted several decades ago (Zahn-Waxler, 1993), reporting that females are higher in internalizing disorders such as depression and anxiety (Rescorla et al., 2007), and males are higher in externalizing disorders such as delinquency and antisocial behavior (Dishion, Andrews, & Crosby, 1995). For many years, females had much higher rates in eating disorders (9:1), and males were much more frequently diagnosed as bullies or being delinquent (Holt et al., 2015). However, recent research has reported a rise in eating disorders among males such as bulimia (Darcy & Arnow, 2017), and females have been diagnosed as exhibiting aggressive provocative behavior and binge drinking more frequently than in previous decades (Kowalski, Giumetti, Schroeder, & Lattanner, 2014). Given the lack of empirical studies, we can only presume that males and females have diverged in distinct ways from their stereotyped gender role. Clinical experience also speaks for a certain crossover effect such that males display so-called female symptoms and females adopt more and more male symptoms, suggesting that gender equality manifests itself in emerging adults’ psychopathology.
Our study shows an increasing convergence between males and females in the expressions for symptoms in several countries. The lack of gender differences in emerging adults from France, Germany, Turkey, and Greece could speak for an effect of increasing gender equality, a speculation which needs to be studied in further research. However, given the evidence of extreme sexism and misogyny in some of the countries surveyed (e.g., honor killings, high rates of domestic violence in Turkey), we should also consider the self-silencing behavior of females (Harper & Welsh, 2007), by which they choose to suppress their voice to preserve relationships and comply with norms.
In contrast to narrowing gender differences in some countries, a wider gender gap exists in others. For example, males reported higher symptomatology than females in countries such as Peru, Pakistan, and Poland. Males in these countries could currently suffer from more stress compared to earlier decades, or perhaps talking openly about distress has become more acceptable for males in these countries. Remarkable is the change toward higher symptoms reported in internalizing symptomatology. As stated above, findings from clinicians point to a crossover effect in symptomatology with males adopting more and more female symptoms. Further research is needed to clarify the potential causes for similarity between symptom levels in male and female emerging adults in some countries and the strong gender difference between males and females in other countries. Our findings could be an indication of cultural changes in gender stereotyped behaviors, especially in the reporting of symptomatology.
Future work is needed in examining why these country-specific differences exist, including its interaction with gender differences. Therefore, an important further step would include an analysis of whether specific syndromes exist in these countries (e.g., somatic complaints as part of internalizing and total symptomatology of the YASR) that assume high levels for males and thus contribute to strong gender differences as was found in these samples. In addition, future research needs to explore whether males deviate from their gender-stereotyped psychopathology by adopting more hidden female symptoms.
Potential causes also need to be clarified through research such as differences in the meaning of symptoms, differences in the level of suffering, cultural stereotypes about mental illnesses, and cultural concepts of distress, which all might contribute to the interaction between country and gender and the unexpectedly low symptoms scores of emerging adults living in dangerous environments such as Pakistan.
In short, our results show that after partialing out identity-related risk factors, culture no longer beats gender, as the study of Rescorla et al. (2007) suggests. Instead, in some countries, males suffer more than females. This unusual trend could be pertinent should it be replicated in further cross-cultural studies, also in clinical work.
Limitations and Future Directions
Despite its contributions, the study is not without limitations. First, the sample consisted of university students and therefore might not generalize to nonstudent populations. Relatively little is known about poor young adults in different countries and even less about their parents. Research has shown that parenting styles tend to vary as a function of Socioeconomic Status (SES) (see Hoff, Laursen, & Tardif, 2002, for a review). Thus, the parenting style of mothers coming from different socioeconomic backgrounds is likely to impact the mental health of their offspring differently. Second, we acknowledge that controlling for parenting behavior implicitly means controlling for specific cultural influences under the premise that culture influences parental behavior. The between-country differences observed in this study might therefore represent cultural factors that transcend parental behavior, and also coping behavior, beyond the scope of this reach. Moreover, we focused on perceived maternal behavior, but research has also shown that fathers’ parenting has an impact on psychopathology of the offspring and that fathers are important for identity development of the offspring (Cassano et al., 2006). The inclusion of fathers in the empirical investigation of child psychopathology across cultures is therefore important in future studies. Another limitation is the reliance on one resource, the emerging adult’s perspective. Perhaps an interview approach that includes other reporters may extend our findings. A notable limitation is also the cross-sectional nature of the study, which precludes testing for causal influences, the assessment of change over time, and a potential bidirectionality in influence. Thus, we were not able to detect changes in country-related or gender-specific patterns in symptomatology, which may add to the overall picture of a cultural impact on emerging adults’ psychopathology. Finally, investigating the extent that the effect of different parenting styles on symptomatology varies as a function of country is an area of research that needs more attention. With some exceptions (Barber et al., 2005; Brouwers, van Helmert, Breugelmans, & van de Vijver, 2004), most of the studies were based on North American samples with different ethnic backgrounds.
Conclusion
Overall, this study makes several unique contributions to our understanding of emerging adults’ psychopathology in different countries. Our findings highlight the importance of controlling for identity-related risk factors in psychopathology to get a clearer picture about symptom levels of emerging adults from different countries. The results of the current study clearly demonstrate a narrowing gender gap in internalizing symptomatology in emerging adults from France, Germany, Turkey, and Greece in contrast to elevated levels of psychopathology in male emerging adults from Peru, Poland, and Pakistan. They also provide an important foundation from which future work can be conducted by examining other risk factors that may affect psychopathology in young adults from different countries or by exploring background variables that may be related to emerging gender differences in some countries or the lack of gender differences in others. These findings make us more sensitive to young male patients from certain countries and may help to design country-specific approaches that consider gender differences, which are more outspoken in some cultures compared to others.
Footnotes
Acknowledgments
The authors are grateful for the Best International Research Award of SSEA, which was assigned to this study at the conference Self and Identity at Cluj-Napoca, Romania, May 2018.
Author Contributions
M. Persike contributed to analysis; drafted the manuscript. I. Seiffge-Krenke contributed to conception and design; drafted the manuscript; and critically revised the manuscript. F. Cok contributed to acquisition. K. Głogowska contributed to acquisition. V. Pavlopoulos contributed to acquisition. S. Tantaros contributed to acquisition. C. Perchec contributed to acquisition. I. Rohail contributed to acquisition. J. C. Saravia contributed to acquisition.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open Practices
Data and materials for this study have not been made publicly available. The design and analysis plans were not preregistered.