
Abstract
The transition to high school coincides with an increase in the prevalence of depressive symptoms. Could this be due in part to increasing beliefs about the fixedness of personal traits at a time of frequent social setbacks? And could teaching adolescents that people can change help prevent the increase in depressive symptoms? A longitudinal intervention experiment involved three independent samples of students entering high school (N = 599). A brief self-administered reading and writing activity taught an incremental theory of personality—the belief that people’s socially relevant characteristics have the potential to change. The intervention reduced the incidence of clinically significant levels of self-reported depressive symptoms 9 months postintervention by nearly 40% among adolescents assigned to the intervention condition, compared with control participants. Analyses of symptom clusters, measures of self-esteem, and measures of natural language use explored the outcomes that did and did not show treatment effects. Moderation analyses confirmed theoretical expectations. Among adolescents assigned to the control condition, those who endorsed more of an entity theory of personality—believing people cannot change—showed greater increases in depressive symptoms during the year. The effect of this risk factor was eliminated by the intervention.
Keywords
Major depressive disorder (MDD) is a serious public-health and human-capital problem (Kessler, Chiu, Demler, & Walters, 2005; Mathers, Fat, & Boerma, 2008). Many lifelong cases have their origins in midadolescence, when the prevalence of depression rises substantially (Merikangas et al., 2010). Indeed, adolescence is a developmental period characterized by school transitions filled with social adversity (Barber & Olsen, 2004; Benner, 2011; Newman, Newman, Griffen, O’Connor, & Spas, 2007) as well as by pubertal and cognitive changes (Avenevoli & Steinberg, 2002). These factors may contribute to the onset of depressive symptoms as well as eventual diagnoses of MDD (Newman et al., 2007).
Many programs have attempted to prevent increases in the prevalence of MDD and other internalizing symptoms during adolescence (Muñoz, Cuijpers, Smit, Barrera, & Leykin, 2010; Stice, Shaw, Bohon, Marti, & Rohde, 2009). Selective and indicated preventative interventions lasting many weeks and requiring intensive training have had small to medium effect sizes on average (Garber et al., 2009; Gillham, Hamilton, Freres, Patton, & Gallop, 2006; Horowitz & Garber, 2006). Yet universal preventative interventions—those delivered to large groups of adolescents regardless of level of risk—have so far yielded a disappointing meta-analytic average (d = 0.02; Stice et al., 2009). For example, Spence, Sheffield, and Donovan (2003) delivered a universal preventative intervention lasting eight classroom sessions to more than 1,000 high school students. The intervention unfortunately increased the incidence of clinically significant levels of depressive symptoms a year later by 2 percentage points (also see Sheffield et al., 2006; Wong et al., 2012). This type of result raises the possibility that there are underlying causes of adolescence-onset depression that are not fully understood or successfully targeted by existing universal prevention approaches (see McLaughlin, 2011). A crucial scientific and public-health objective is to close this gap in knowledge (see Muñoz et al., 2010).
To do this, we build on cognitive theories of depression (Beck, 1976, 2008; Disner, Beevers, Haigh, & Beck, 2011; Gotlib & Joormann, 2010; Lakdawalla, Hankin, & Mermelstein, 2007). These theories emphasize that the hopelessness and despair that feed into depression can result in part from the belief that one’s social adversities are likely to be a fixed, stable part of one’s future (Abramson, Seligman, & Teasdale, 1978; Janoff-Bulman, 1979; also see Graham & Juvonen, 1998; Tangney, Stuewig, & Mashek, 2007). We propose that if despair has its basis in a worldview that negative events cannot change, then perhaps teaching adolescents about the potential for change could provide a foundation for hope. This might prevent adolescents from developing symptoms of depression during times of social adversity, such as the 1st year of high school (see Benner, 2011; Crosnoe, 2011).
Indeed, a large amount of past research has focused on implicit theories of personality, which are people’s underlying assumptions about the malleability of personal characteristics (Chiu, Hong, & Dweck, 1997; Dweck, 1999; Erdley, Loomis, Cain, & Dumas-Hines, 1997; Yeager, Trzesniewski, Tirri, Nokelainen, & Dweck, 2011). Past research has consistently shown that if adolescents or adults hold a theory that people’s traits are fixed and unchangeable—called an entity theory of personality—then they are more likely to show helpless responses to peer victimization or exclusion (saying, for instance, “Maybe I’m just not a likable person”; Erdley et al., 1997; Yeager al., 2011; also see Rudolph, 2010; Yeager, Miu, Powers, & Dweck, 2013). However, if adolescents are taught a theory that people’s traits have the potential to change and be developed—called an incremental theory of personality—then helplessness is less likely to follow (Yeager et al., 2011; Yeager, Trzesniewski, & Dweck, 2013). It stands to reason then that an intervention that teaches an incremental theory of personality—by providing teens with a belief system that facilitates their ability to see negative social events as changeable—might prevent or slow the onset of symptoms of depression.
Implicit Theories Are Meaning Systems That Shape Responses to Adversity
Research on implicit theories grows out of a long line of experiments reaching back to early research on learned helplessness in humans (Diener & Dweck, 1978; Dweck, 1975; Dweck & Leggett, 1988). Implicit theories have been applied to understanding helpless responses to social situations (Beer, 2002; Chiu et al., 1997; Yeager et al., 2011) as well as to academic situations (e.g., Dweck & Leggett, 1988). Looking broadly across these findings, implicit theories are known to operate as schemas for understanding the world, acting as a “lens” for focusing attention on fixed versus changeable causes of events (Chiu et al., 1997; Dweck & Leggett, 1988; Molden, Plaks, & Dweck, 2006). Following an adverse event, this focus can lead to a corresponding set of helpless versus resilient causal attributions, emotions, and behaviors (e.g., Dweck, 1999; Molden & Dweck, 2006; Yeager & Dweck, 2012; for a meta-analysis of effects on motivation and behavior, see Burnette, O’Boyle, Vanepps, Pollack, & Finkel, 2013).
Although the current research looks directly at the impact of implicit theories of personality on symptoms of depression during the transition to high school and does not explore the psychological processes that might contribute to this effect, here we present a background on proximal social-cognitive consequences of implicit theories. Research on implicit theories of intelligence provides a helpful analogy (see, e.g., Dweck & Elliott-Moskwa, 2010). Specifically, an entity theory of intelligence—the belief that “smartness” is a fixed trait that you either have or do not have—has been associated with maladaptive explanations for failures in school (Ahmavaara & Houston, 2007; Blackwell, Trzesniewski, & Dweck, 2007; Hong, Chiu, Dweck, Lin, & Wan, 1999; Robins & Pals, 2002). This includes self-talk, such as “I’m failing because I’m stupid” (Robins & Pals, 2002) or “I guess I’m not very smart” (Dweck & Leggett, 1988; see Dweck, 1999). Individuals with more of an entity theory, compared with those with less, also show more helpless patterns of behavior, such as avoiding challenges, hiding deficiencies, or just giving up (Blackwell et al., 2007). Moreover, interventions that teach students an incremental, malleable theory of intelligence allow students to show greater resilience when making a difficult school transition. In one study, students who participated in an incremental theory workshop in school showed a clear rebound in their declining academic achievement roughly 3 months posttreatment, which signified greater resilience (Blackwell et al., 2007; see Yeager & Dweck, 2012).
Implicit Theories of Personality
Analogously, a number of past investigations have suggested that it may be possible for an implicit theory of personality to increase risk for depression. First, implicit theories measured on a questionnaire reliably predict adverse responses to a social conflict. Yeager et al. (2011, Study 1) measured an entity theory of personality and asked adolescents to write about a time during which they felt left out or excluded by an acquaintance. Individuals with more of an entity theory were significantly more likely to say that they “felt bad about” themselves. Similarly, Yeager et al. (2014) found that an entity theory of personality predicted greater negative emotionality (negative self-feelings, stress, and anxiety) after an experience of peer exclusion—that is, ostracism by peers during the Web-based game Cyberball (Williams & Jarvis, 2006).
Short-term experimental studies have confirmed a causal role for implicit theories of personality. Yeager et al. (2011, Study 3) showed that a brief “teen self-help” article that had an incremental theory of personality embedded within it could alter adolescent participants’ implicit theories and reduce helpless responses to a bullying scenario, including fewer reports of shame. Yeager, Miu, et al. (2013, Study 2) used a slightly more elaborate manipulation. Teens read a scientific article that conveyed the possibility of personality change, which was followed by quotes from older students who endorsed the same message. Participants then wrote a brief essay reiterating the incremental theory. This changed implicit theories of personality and attributions in response to a hypothetical peer conflict. Furthermore, Yeager et al. (2014) showed that this incremental theory intervention could reduce negative affect (negative self-feelings, stress, and anxiety) after an experience of peer exclusion.
Finally, incremental theory interventions have induced changes in responses to social difficulties up to 1 month later. Yeager, Trzesniewski, and Dweck (2013) implemented a face-to-face school-based incremental theory workshop that lasted six classroom sessions during a 3-week period. As expected, at a 2-week follow-up, the incremental theory group changed their implicit theories, whereas the control group did not. One month later, adolescents completed a seemingly unrelated activity in which they were excluded by a peer (again, via Cyberball). Compared with control participants, incremental theory participants reacted less negatively and more prosocially. Furthermore, the six-session classroom intervention reduced depressive symptoms among victimized adolescents at a 2-week follow-up (Yeager, Trzesniewski, & Dweck, 2013).
In sum, individual differences in an entity theory of personality consistently predict negative affect and helpless behavior during social adversities. Furthermore, teaching its opposite—an incremental theory of personality—can improve short-term reactions to a peer conflict, including behavioral and self-reports of depressive symptoms. The present research builds on this and focuses on whether the single-session intervention used in our earlier study (Yeager, Miu, et al., 2013) could alter levels of depressive symptoms many months later across the socially difficult transition to high school.
Implicit Theories During the Transition to High School
Implicit theories may be particularly important during a sensitive developmental period, such as high school transition. Adolescents entering high school think more about peer relationships (e.g., Richards, Crowe, Larson, & Swarr, 1998) and are more likely to face uncertainty in peer relationships, given that 50% of casual friendships change during each month of freshmen year of high school (Chan & Poulin, 2007). Without a stable social network in a new environment, freshmen are more likely to feel anxious about the possibility of being socially excluded, which threatens their social status (Juvonen & Graham, 2014). In response to potential social conflicts, high school students, compared with younger children, are more likely to interpret social attributes as fixed and unchangeable (e.g., Killen, Kelly, Richardson, & Jampol, 2010), which means that they are more likely to believe social adversities or setbacks to be stable. Given the increase of uncertainty in peer relationships and the belief in fixed attributes, implicit theories can be especially relevant in interpreting social uncertainties during high school transition. Building on this idea, we propose that one helpful strategy for preventing the onset of depressive symptoms might be to teach an incremental theory of personality.
Brief Psychological Interventions
Somewhat in contrast to the nonsignificant effects of comprehensive and time-intensive universal preventative interventions for adolescents (Stice et al., 2009), the literature has produced many examples of brief but theoretically precise psychological interventions that have affected mental and physical health or academic achievement over time (for reviews, see Cohen & Sherman, 2014; Walton, 2014; Yeager & Walton, 2011). For instance, research by Pennebaker (1997) and Petrie, Booth, and Pennebaker (1998) has shown that expressive writing exercises that last just a few minutes can affect reports of stress and health weeks or months later and improve immune functioning. Walton and Cohen (2011) found that a 1-hr attributional retraining intervention conducted in the 1st year of college could improve minority students’ health, happiness, and grade point averages 3.5 years later at the end of senior year (for many other examples, see Wilson, Damiani, & Shelton, 2002). Even though the mediating mechanisms for these psychological interventions are not fully understood, they have an important status in clinical and social psychological theory (Pennebaker, 2004; Walton, 2014).
Informed by these past studies, the present research is the first to test the effect of a brief implicit-theories-of-personality intervention on longer-term depressive symptoms. This is critical to test because it is a scientific priority to identify scalable, brief, and low-cost preventative interventions for depression (Muñoz et al., 2010). Even modest preventative effects, occurring during a critical developmental juncture, can have important psychological and policy implications. Such effects can slow or stop depression from gaining momentum, thus preventing long-term losses in wages or human-capital development (e.g., Frieden, 2010; Glasgow, Lichtenstein, & Marcus, 2003; also see Abelson, 1985; Cohen, Garcia, Purdie-Vaughns, Apfel, & Brzustoski, 2009). In many cases, this possibility justifies the economic cost of even time- and labor-intensive preventative interventions. However, the marginal cost of teaching an incremental theory to an adolescent over the Internet approaches zero. This means that if the present brief intervention produced even modest treatment effects, it would have important implications for public health and human capital.
Overview of Present Research
The present research used a longitudinal, randomized intervention experiment to test the causal effect of an incremental theory of personality on levels of depressive symptoms. Because the incidence of adolescent depression approximately doubles during the high school transition (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003; Lewinsohn, Rohde, & Seeley, 1998; Merikangas et al., 2010), we recruited ninth graders at the beginning of the school year, before increases in depressive symptoms were likely to occur. We hypothesized that adolescents who did not receive the treatment would show the typical increase in depressive symptoms but that those who learned, in the 1st few weeks of the school year, that people can change, might be protected.
The present research involves nearly identical experiments carried out in three independent samples totaling roughly 600 adolescents. The first experiment was small, involving just 77 adolescents. The second, a replication, was larger, involving 143 students. Both of these were conducted to test other research hypotheses. However, both included measures of depressive symptoms that have not been reported elsewhere. Wishing to confirm these results, we conducted another experiment, this time involving more students (n = 379). We aggregated the data from these three studies in what was, in effect, a raw-data meta-analysis of original experiments. Thus, more reliable effect size estimates were possible (for descriptions of raw-data meta-analysis, see Cooper & Patall, 2009; Schimmack, 2012).
These studies used a strict, active-placebo control group. In past research, we have compared an incremental theory group with a group receiving no message or with a group receiving a more conventional treatment, such as a coping-skills treatment (Yeager et al., 2011; Yeager, Trzesniewski, & Dweck, 2013). Thus, in those past studies, it was not possible to rule out the alternative hypothesis that observed differences between the treatment and control groups were due to the possible benefits of receiving any optimistic message about growth and improvement from senior and junior students. To overcome this limitation, in some research, we have used control conditions that taught an optimistic message about change but not specifically about traits relevant to peer exclusion or victimization (e.g., study skills or athletic ability; Yeager et al., 2014; Yeager, Miu, et al., 2013). In the present study, we did this as well.
Method
Participants
Participants came from three schools in Northern California (N = 599; 48% female, 52% male). Two schools (providing Samples 1 and 3) were in upper-middle-class neighborhoods and were generally high performing. Students were predominately White (43%) or Asian American (46%). Only 6% of these students were eligible for free or reduced-price lunch, an indicator of low socioeconomic status. A third school (providing Sample 2) was one of the lowest-income and poorest-performing schools in the San Francisco Bay Area. Of these students, 80% were Hispanic/Latino, and 73% were eligible for free or reduced-price lunch. 1
Despite these differences in the samples, social adversities were common across samples; on a survey we conducted in the 3rd week of the school year, many students (75%) reported being the victim of at least some physical, verbal, or social aggression, and this was not significantly different across schools. Even those students who did not experience victimization might be aware of the possibility that they could be “next.” Indeed, of the minority of students reporting no victimization at baseline, nearly half reported at least some victimization at the 9-month follow-up. Thus, there were ample opportunities for all students to experience—or at least worry about experiencing—social adversity involving peers (also see Crosnoe, 2011), which could contribute to depression in the absence of our intervention (Newman et al., 2007).
Sample 1 was the first study we conducted. We recruited all of the students in Algebra 1 in the school, which is a lower-performing math class. All provided consent: 82 students provided baseline data, and 77 provided follow-up depressive-symptoms data and constituted the analytic sample. Sample 2 was a replication and involved all of the students in Algebra 1 at a different, lower-performing school; 95% provided consent. Of the 161 students who completed the baseline survey, 143 also provided depressive-symptoms data in May. In Study 3, students entering ninth grade—regardless of math placement—were recruited, and 96% provided consent; 427 provided baseline data and of these, 379 provided longitudinal data. Nearly all of the students who did not provide longitudinal data were either chronically truant or had dropped out of high school or moved. Across studies, 66 students did not complete both the baseline and the follow-up studies; these students were excluded from analyses, but the statistical significance of the results was no different when we imputed values and included them. A chart that details all data included or excluded from analysis is presented in Figure S1 in the Supplemental Material available online.
Procedure
In the 1st week of the school year, in September, parental consent was obtained for all students. In the 3rd week, students assented and completed an initial survey that measured baseline characteristics (e.g., demographics and levels of depressive symptoms). One week later, students were randomly assigned to the intervention. In May, at the end of the school year, roughly 9 months later, students were again surveyed to assess depressive symptoms (see Fig. 1 for a flowchart of experimental procedures). Some of the students in Sample 2 had poor English skills, so we provided them the option of reading the intervention in Spanish (which had been translated by native Spanish speakers); 7% of Sample 2 participants chose to read the intervention in Spanish, and this did not differ by condition and did not have an effect on experimental outcomes.
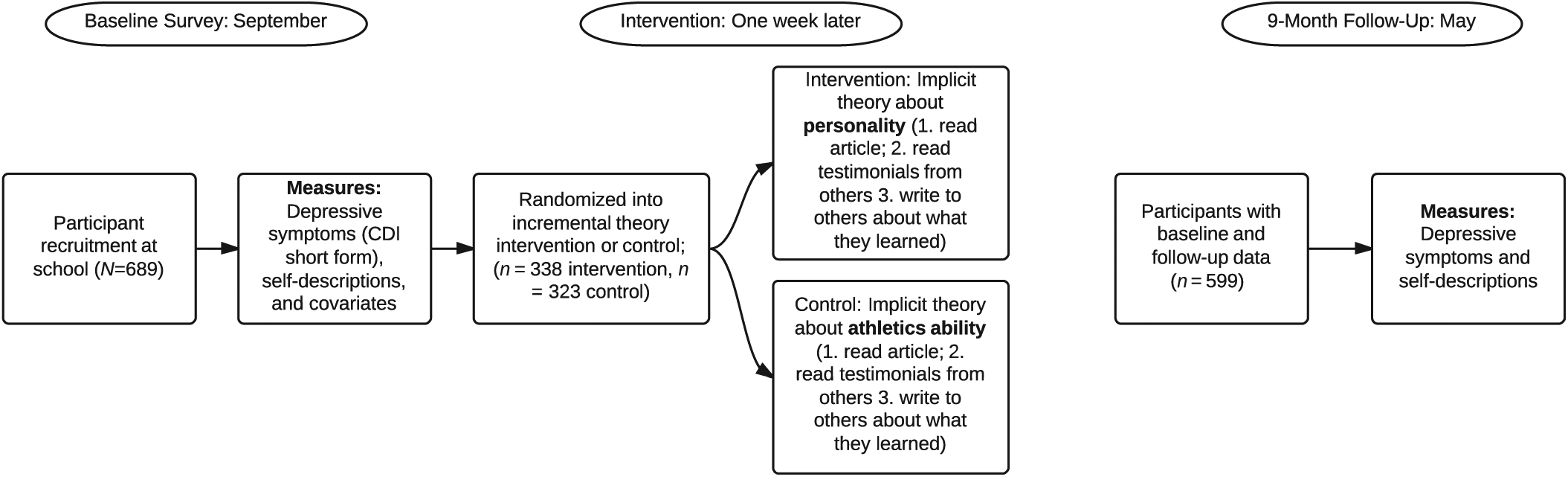
Flowchart of experimental procedures. CDI = Children’s Depression Inventory.
In the current, early stage investigation of the incremental theory intervention, the primary outcome was self-reported symptoms of depression—consistent with many universal prevention evaluations (Stice et al., 2009). Advantages of this approach involve the reduced possibility of sample attrition due to burdens of study participation and the resulting increase in statistical power. Disadvantages, of course, involve the need to rely on only one measure—for example, meeting a clinical threshold on a self-reported measure—to assess the presence of problematic levels of depressive symptoms, as well as an inability to assess impact within clinically diagnosed subgroups.
The intervention procedure is described in greater detail in our previous studies (e.g., Yeager, Trzesniewski, & Dweck, 2013) and in the Detail on the Experimental Intervention section in the Supplemental Material. A brief overview follows.
In the 3rd week of the school year, using a true random-number generator (www.Random.org), researchers randomly assigned participants within classrooms—that is, at the individual level—into intervention or control groups. During normal class time, participants in each group completed either an experimental intervention or a control activity on paper (Sample 1) or computer (Samples 2 and 3) quietly for one class period. The average completion time for the intervention was approximately 25 min. Research assistants who administered the interventions were different from those who administered the surveys, and all members of the research team were blind to participants’ assigned condition throughout the study. Teachers were blind to study hypotheses and students’ assigned experimental conditions. 2 All that was required of the teachers or research assistants was to keep the class working quietly. No staff person who interacted with students (research assistants, teachers) was briefed on any of the content of the intervention.
The treatment intervention taught an incremental theory of personality by presenting evidence that individuals have the potential to change. It conveyed that (a) if you are excluded or victimized, it is not due to a fixed, personal deficiency on your part; and (b) people who exclude or victimize you are not fixed, bad people but, instead, have complicated motivations that are subject to change. Participants were then asked to read a brief article on actual neuroscience studies that showed that behaviors are controlled by “thoughts and feelings in their brains” and that such pathways in the brain can be changed. This was done to provide adolescents with a scientific basis for believing in the potential for change (rather than telling adolescents the platitude that “people can change”). Afterward, participants read two quotes purportedly written by senior and junior students who had previously read the same article and endorsed its conclusions. As with the scientific summaries, the testimonials were designed to bring credibility to the incremental theory via admired role models (i.e., seniors and juniors in one’s high school).
Finally, participants were asked to write their own version of such a narrative to share with future ninth graders by drawing on the examples they had just read from the seniors and juniors or on their own experiences in high school or middle school. This “saying-is-believing” activity has been shown to facilitate the internalization of the intervention message (see Aronson, 1999; Walton & Cohen, 2011) and has been implemented before (e.g., Yeager, Trzesniewski & Dweck, 2013). After this one-time activity, the intervention was not mentioned again to students by researchers or teachers.
The control condition was designed to be exactly parallel to the experimental condition, except that the control condition focused on malleability of athletic ability, a nonpersonality domain that was never linked directly to responses to exclusion or victimization, as the treatment was. Nevertheless, athletic ability was also thought to be important to adolescents, thus eliminating the possibility that simple optimism about the potential for growth in any important domain might account for our results. And, of course, an entity-theory-of-personality control group would have been unethical and, furthermore, would not have allowed us to separate the negative effects of learning an entity theory from the positive effects of learning an incremental theory.
Measures
Depressive symptoms
To measure depressive symptoms, we administered the 10-item short form of the Children’s Depression Inventory (CDI:S; Kovacs, 1992) on the September and May surveys. 3 Each CDI:S item asked participants which of three levels of a symptom described them best (e.g., 2 = I feel like crying every day, 1 = I feel like crying many days, 0 = I feel like crying once in a while). The 10 items were summed and showed adequate internal consistency (preintervention α = .82, postintervention α = .87). CDI:S scores were first analyzed dichotomously; participants were categorized into clinically significant and nonsignificant symptom levels. We selected a cut point of 6 out of 20 points, which corresponds to the 81st to 87th percentile of depressive symptoms (for boys and girls, respectively; Kovacs, 1992), 4 because it best approximates the cut point identified by past research as striking the optimal balance between false positives and false negatives (Timbremont, Braet, & Dreessen, 2004). Dichotomization of continuous measures can sometimes result in misleading conclusions if the results are not robust to different cut points and if they do not replicate across multiple independent samples (MacCallum, Zhang, Preacher, & Rucker, 2002). Therefore, sensitivity analyses were conducted with a cut point of 7 out of 20 points, and we present results for all three replication samples in Table 1.
Participants Who Met the Threshold for Clinically Significant Levels of Depressive Symptoms at Baseline and 9 Months Postintervention by Condition and Sample

Note: The table presents raw data. To designate status as meeting clinically significant levels of depressive symptoms, we used a cut point of 6 out of 20 points on the short form of the Children’s Depression Inventory; this corresponds to the 81st to 87th percentile for boys and girls, respectively (Kovacs, 1992).
To supplement this primary analysis, we conducted continuous depressive-symptom analyses on each of the subscales of the CDI:S. These subscales were based on factor analyses of the full CDI scale reported in the literature (e.g., Helsel & Matson, 1984; Kovacs, 1992; Saylor, Finch, Spirito, & Bennett, 1984; Weiss & Weisz, 1988; Weiss et al., 1991). Kovacs (1992) reported five factors, including negative mood (e.g., I am sad all the time), ineffectiveness (e.g., I do everything wrong), anhedonia (e.g., I feel alone all the time), and negative self-esteem (e.g., I hate myself). The fifth factor (Kovacs, 1992), interpersonal problems, had no items on the CDI:S. We aggregated the relevant items corresponding to the four factors following standard procedures, thereby producing four separate subscales, each of which ranged from 0 to 2. Exact items for each of the four subscales are presented in the Depressive Symptoms section in the Supplemental Material.
Self-esteem
Supplementing the CDI:S items, two self-esteem items were administered on the September and May surveys: “I feel that I am a person of worth, at least on an equal basis with others” and “I feel that I have a number of good qualities”; responses were made using a scale from 1 (strongly disagree) to 7 (strongly agree). Items were averaged and, as expected, were negatively correlated with the negative self-esteem CDI:S subscale (September: r = −.47, p < .001). In Sample 1, self-esteem was assessed in May only. Sample 1 data could not be used in the analyses of change scores but were used in analyses of year-end levels.
Textual analysis of self-descriptions
In Samples 2 and 3 only, the first question on the September and May surveys was “In general, what do people in your grade at school think about you? Type as many or as few words that people in general might think about you in the box below.” Responses to this question were first spell-checked to correct common errors and increase match rates for the Linguistic Inquiry and Word Count software (LIWC; Pennebaker, Booth, & Francis, 2007). Next, the default LIWC dictionaries were applied to each response. At each time point, we averaged three categories to create an index of linguistic styles that signal maladaptive self-views: negative emotion or trait words (hurt, ugly, nasty), past tense (went, ran, had), and discrepant thinking (should, would, could). It was predicted that thinking of the self in terms of negative emotions or traits, dwelling on the past, and engaging in counterfactual thinking about what one should or could be would signal maladaptive self-views (and the latter category, discrepant thinking, has been correlated with poorer mental and physical health in much past research; Higgins, Vookles, & Tykocinski, 1992; Pennebaker & King, 1999). Supporting this theory, in the present research, the composite negative self-views index from the September preintervention survey was significantly correlated with preintervention levels of depressive symptoms, r = .16, p < .001, and self-esteem, r = −.17, p < .001.
Covariates and moderators
On the September preintervention survey, participants reported sex, race/ethnicity, entity theories of personality (Yeager et al., 2011), and self-reported frequency of bullying (for details on the two measures, see the Implicit Theories of Personality and Peer Victimization sections in the Supplemental Material). From school records, we obtained test scores earned the prior year, in eighth grade.
Results
Analytic plan
All analyses were intent to treat and did not drop participants who wrote brief or incomplete summaries of the intervention materials. Thus, the results are conservative. Our primary interest was in a person-centered analysis of whether the intervention prevented clinically significant levels of depressive symptoms. Treatment effects on the incidence of serious depressive symptoms are one policy-relevant analysis (Muñoz et al., 2010) because real-world diagnosis and treatment of MDD involves individuals, not variables (Farrington & Loeber, 2000; Rutter, 2003). Obtaining effect sizes that are relevant to the real-world use of a measure is one of the rare cases when dichotomization of continuous variables is appropriate (DeCoster, Iselin, & Gallucci, 2009). 5 Treatment effects on incidence rates are also essential for estimating the cost-effectiveness of an intervention.
Our secondary interest was in developing theory about the generality or specificity of effects of implicit theories on different groupings of depressive symptoms. Thus, we conducted variable-centered analyses of which symptom subgroups were most affected by the incremental theory intervention. We extended these analyses by conducting analyses of explicit and implicit measures of individuals’ construals of themselves: explicit self-esteem and linguistic categories that signal implicit negative self-views.
Third, we carried out moderation analyses to understand the predicted mechanisms for the results. We examined whether, as expected, the incremental theory of personality intervention had its effects by preventing those individuals with more of an entity theory at baseline from developing higher levels of depressive symptoms during the year. Results for all outcomes are presented in Table 2, which presents the raw means and proportions as well as statistical tests from models with a number of covariates (see Tables S2 through S5 for full regression models with and without covariates, see the Supplemental Material).
Effects of a Brief Implicit-Theories-of-Personality Intervention on Depressive Symptoms and Self-Views at 9-Month Follow-Up
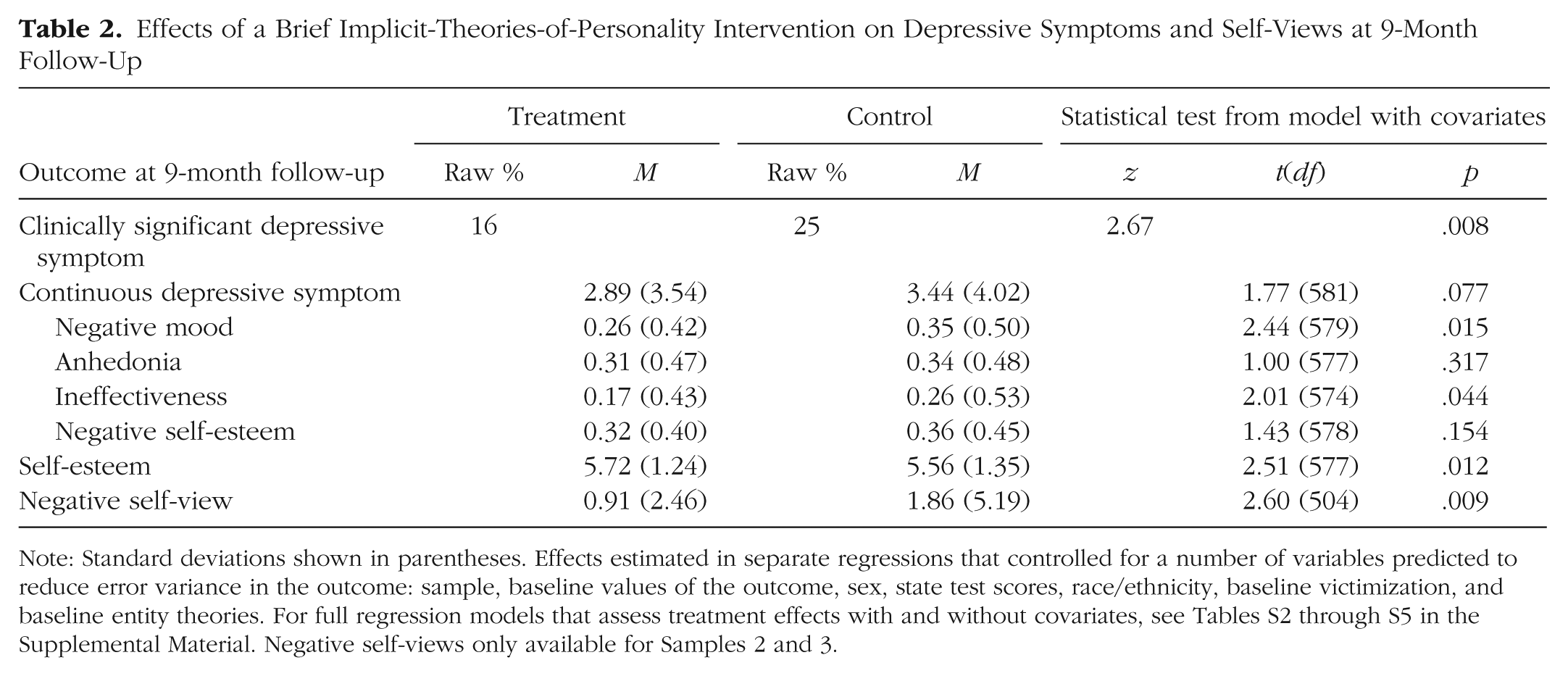
Note: Standard deviations shown in parentheses. Effects estimated in separate regressions that controlled for a number of variables predicted to reduce error variance in the outcome: sample, baseline values of the outcome, sex, state test scores, race/ethnicity, baseline victimization, and baseline entity theories. For full regression models that assess treatment effects with and without covariates, see Tables S2 through S5 in the Supplemental Material. Negative self-views only available for Samples 2 and 3.
Preliminary analyses
Randomization was effective. There were no significant main effects of condition on covariates measured at baseline, including sex, race/ethnicity, academic test scores, depressive symptoms (coded continuously), implicit theories, or bullying (see Table S1 in the Supplemental Material). However, an examination of the incidence of clinically significant depressive symptoms yielded a significant baseline difference in Sample 1 but not Samples 2 and 3 (see Table 1). Therefore, we also carried out supplemental analyses that excluded Sample 1 (see the Supplementary Analyses section in the Supplemental Material).
Next, students did in fact appear to learn the incremental theory. Two coders, who were blind to experimental hypotheses and to participant identities and characteristics, independently and reliably judged whether participants’ responses appeared to answer the writing prompts in the intervention materials sufficiently. The interrater reliability was adequate (Krippendorff’s α = .85), and inconsistencies were resolved by consensus. More than 94% of responses were judged to have sufficiently answered the prompt and referred to a belief in the potential for change.
Sample responses in the treatment condition include
People can change and be a better person then [sic] before and I think those people just try to do that because they used to get picked on in school. They all have a different personality and it could change as they go on in school. For example, a bully that is always picking on kids can be doing that because he’s having trouble with his grades, but if he gets help and gets better grades he can realize what he’s done and change the way he is. I knew that they would one day change but I didn’t know when. I always thought . . . maybe they were going through a hard time. People could change over time. Maybe they had a bad day or something.
Seeing that individuals wrote about the incremental theory as expected, we proceeded to test our primary hypotheses concerning long-term depressive symptoms (for other sample excerpts, see the Additional Unedited Written Samples From Treated Students section in the Supplemental Material).
Preventing the incidence rates of clinically significant depressive symptoms
In the control group, the incidence of clinically significant levels of depressive symptoms rose from September to May by roughly 39% (September raw data: 18% above the clinically significant cut point of 6; May: 25%), a significant increase (test of equality of proportions: z = 2.07, p = .038). This is similar to the proportional increase typically seen for adolescents across the transition to high school (Merikangas et al., 2010). However, among students assigned to the incremental theory intervention condition—who learned at the beginning of the year that people’s socially relevant characteristics are not fixed but have the potential for change—there was no significant increase during the year in the prevalence of clinical levels of depressive symptoms (September: 14%; May: 16%; z = 0.54, p = .592). As a result, at the May follow-up, participants assigned to the incremental theory condition were roughly 40% less likely to report clinical levels of depressive symptoms than were participants assigned to the control condition (16% vs. 25%), χ2(1, N = 599) = 7.90, p = .005, odds ratio = 0.55 (see Table 1). Logistic regressions that controlled for baseline depressive symptoms and a number of additional covariates supported this significant effect, z = 2.67, p = .008, odds ratio = 0.50 (see Table 2). The treatment effect remained even after we excluded from analysis those participants who met clinical levels of depressive symptoms at baseline (see Table S8 in the Supplemental Material). Treatment effects were significant (at p < .05) when we analyzed a cut point of 7 out of 20 points as opposed to 6 out of 20 or when we limited analyses to Samples 2 and 3 only (see Table S7 in the Supplemental Material). It is interesting that the treatment effect was not significantly moderated by sample, level of victimization, sex, or race (all interaction effect ps > .10; exact tests are reported in Table S6 in the Supplemental Material).
Note that the incremental theory intervention did not reduce depressive symptoms so much as it statistically halted age-related increases in depressive symptoms. This is consistent with existing theory that brief psychological interventions affect long-term outcomes by slowing negative, self-reinforcing processes before they gain momentum (e.g., Cohen et al., 2009; Walton, 2014; Yeager & Walton, 2011).
Effects on specific symptom clusters
To provide a more theoretically precise understanding of these overall treatment effects, we next tested for treatment effects on subscales assessing symptom groups, with each analyzed as continuous variables. There was a marginally significant omnibus effect of the incremental theory intervention on the full, continuous CDI:S, b = −0.44, t(581) = 1.77, p = .077, d = −0.15 (see Table 2 and Fig. S2 in the Supplemental Material). However, this marginal effect masked important heterogeneity across symptom clusters.
In separate linear regression analyses predicting continuous subscales, there was a significant treatment effect on May values of negative mood (I am sad all the time; I feel like crying everyday; Things bother me all the time), b = −0.08, t(579) = 2.44, p = .015, d = −0.20, and ineffectiveness (I do everything wrong), b = −0.08, t(574) = 2.01, p = .044, d = −0.17 (see Table 2). The treatment effect on May values of anhedonia (I feel alone all the time; I do not have any friends) was not close to significant, b = −0.04, t(577) = 1.00, p = .317, d = −0.08. The nonsignificant treatment effect on anhedonia is perhaps unsurprising because anhedonia has a genetic and temperamental component (Hasler, Drevets, Manji, & Charney, 2004; Loas, 1996). Finally, the effect on negative self-esteem (Nothing will ever work out for me; I hate myself; I look ugly; Nobody really loves me) approached but did not reach significance, b = −0.04, t(578) = 1.43, p = .154, d = −0.12 (see Table 2 and Fig. S3 in the Supplemental Material).
The nonsignificant finding regarding negative self-esteem was surprising. Fortunately, however, it was possible to use an additional measure of September and May self-esteem to directly test the notion that negative self-esteem was unaffected by the intervention (recall that self-esteem was assessed at both waves only in Samples 2 and 3). Participants assigned to the control condition reported significantly lower self-esteem in May as compared with September (September: M = 6.11, SD = 1.02; May: M = 5.66, SD = 1.35), t(253) = 4.89, p < .001, d = −0.61. This signals a strong loss of self-esteem during the year. But for participants assigned to the treatment condition, the decrease in self-esteem during the year was present but did not reach significance at a .05 level (September: M = 6.00, SD = 1.13; May: M = 5.83, SD = 1.24), t(262) = −1.78, p = .08, d = −0.22 (see Fig. S4 in the Supplemental Material). A comparison of change scores (May values minus September values) showed that the incremental theory intervention was in fact more effective at warding off a decline in self-esteem during the year, b = 0.26, t(514) = 2.44, p = .015, d = 0.22. Confirming this, using data from all three samples and imputing baseline values for Sample 1, we found a significant main effect of the intervention on higher self-esteem in May, b = 0.24, t(577) = 2.51, p = .012, d = 0.21 (see Table 2). Thus, the nonsignificant finding for negative self-esteem in the CDI:S subscale did not capture an effect that became more apparent using this supplemental measure.
Linguistic indicators of maladaptive self-views
Analyses of more indirect negative self-views assessed through subtle features of language mirrored the self-reported self-esteem results. Prior to the intervention, in September, there were no differences between participants assigned to the treatment and control conditions on the linguistic indicators of maladaptive self-views (i.e., negative emotion words, talking in the past tense, and talking in terms of what “could” or “should” have been; raw data, incremental theory condition: M = 1.10, SD = 3.00; raw data, control condition: M = 1.35, SD = 3.50), t(505) = 0.89, p = .374, d = 0.08 (recall that self-views were assessed in Samples 2 and 3 only). However, in May, at the end of the year, treated students described themselves in significantly less maladaptive ways (raw data, incremental theory condition: M = 0.91, SD = 2.46; raw data, control condition: M = 1.86, SD = 5.19), t(520) = 2.60, p = .009, d = 0.23. In an ordinary least squares regression predicting May self-views and controlling for September self-views and a number of additional covariates (i.e., those reported in Table S2 and Fig. S5 in the Supplemental Material), the condition effect remained significant, b = −0.90, t(504) = 2.60, p = .009, d = 0.23. Thus, the finding that the intervention prevented a worsening of negative self-views was confirmed by using this more indirect assessment: nonconscious use of linguistic categories that signal negative self-construals.
Moderation by baseline implicit theories?
Our theory leads to the expectation that the incremental theory intervention should have its effect chiefly by preventing an entity theory from undermining resilience and fueling depressive symptoms. Therefore, individuals with more of an entity theory at baseline should benefit most (Yeager et al., 2014, Study 3; also see Blackwell et al., 2007). Moderation analyses tested this possibility using the full, continuous measure of depressive symptoms to increase statistical precision.
Within the control group, an entity theory in September was correlated with significantly more depressive symptoms at the May follow-up, b = 0.60, t(292) = 2.67, p = .008, β = 0.14. This relation was eliminated in the treatment group, b = 0.12, t(301) = 0.68, p = .500, β = 0.04, and the difference in correlations was significant, evidenced by a significant Incremental Intervention × Baseline Entity Theory interaction, b = −0.51, t(590) = 2.14, p = .033, β = −0.10, in a model controlling for September levels of depressive symptoms and with fixed effects for sample.
Figure 2 illustrates this interaction using values estimated at 1 SD above and below the mean in terms of baseline theories, adjusting for sample fixed effects. It shows that in September, before the intervention, treatment and control participants did not differ in terms of their depressive symptoms. Furthermore, Figure 2 shows that baseline implicit theories were a strong predictor of baseline depressive symptoms (i.e., symptoms differed as a function of theories in September). Next, among individuals with more of an entity theory at baseline who participated in the control activity, there were also marked increases in levels of depressive symptoms during the year. Yet among adolescents with an entity theory at baseline who were assigned to the incremental theory intervention condition, levels were flat over time; the intervention statistically halted the normative increase in depressive symptoms during the freshman year (see Fig. 2). Thus, by May, there was a treatment effect on the continuous measure of depressive symptoms among students who began the year with more of an entity theory (+1 SD), simple effect b = −0.93, t(590) = 2.58, p = .010, d = 0.21. Those students who began the year with an incremental theory did not differ as a function of whether they were assigned to the treatment or control condition (see Fig. 2).
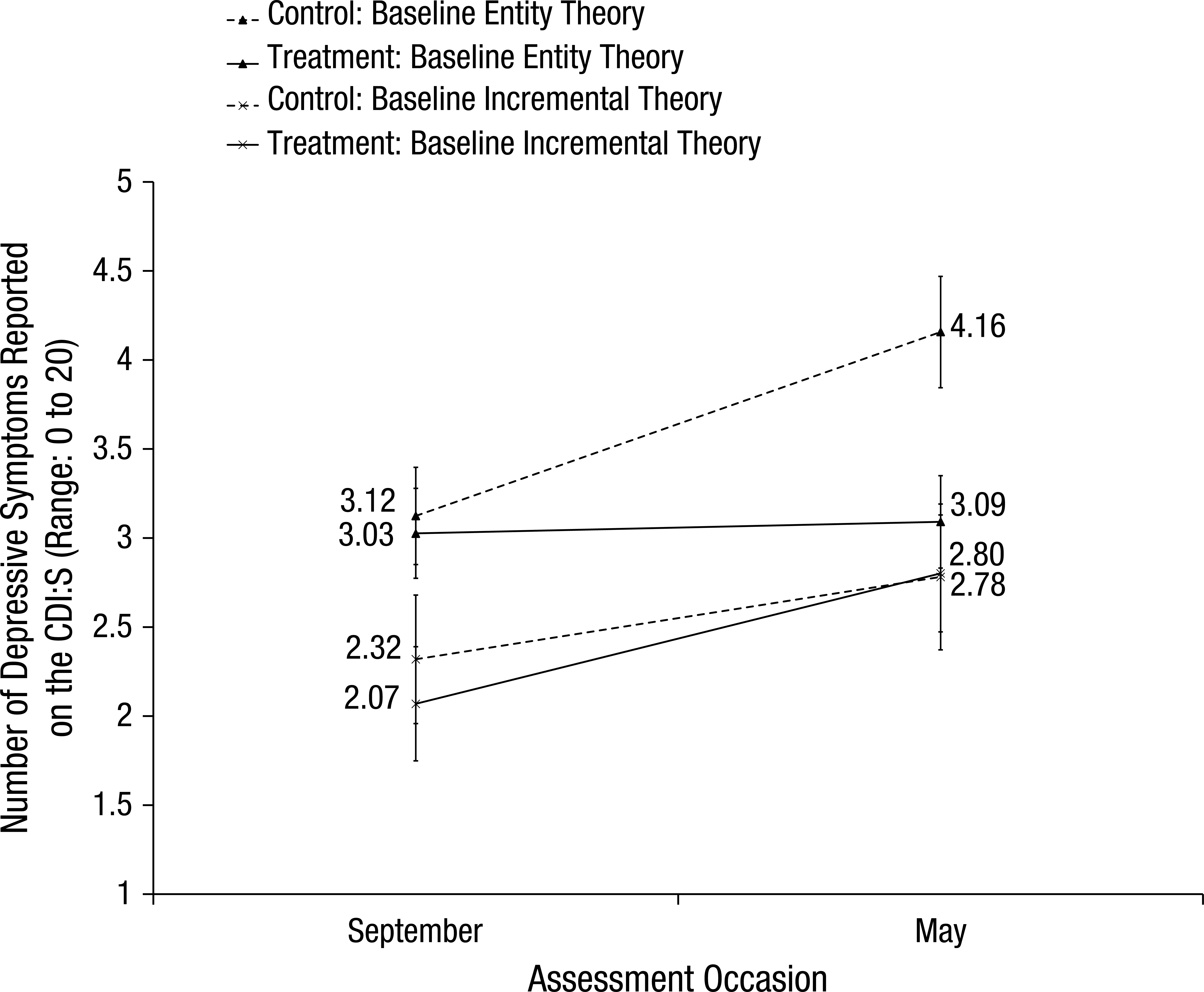
Changes in depressive symptoms from September to May of ninth grade, by baseline implicit theories and experimental condition. Baseline implicit theories correspond to estimated values at 1 SD above or below the mean for that scale, from models removing fixed effects for sample. Error bars represent standard errors. CDI:S = short form of Children’s Depression Inventory.
Note that the intervention did not seem to treat depression—that is, depressive symptoms did not appear to decrease in any group of students over time. Instead, the incremental theory intervention seems to have had its effects by neutralizing a risk factor’s effects, thereby preventing an entity theory from increasing risk for depression over time.
Discussion
If the seed of depression is the belief that negative events cannot improve, then one way to prevent depressive symptoms from growing might be to teach the idea that people can change. This might prevent depression from taking root in a way that, absent timely intervention, can be difficult to reverse during the ensuing decades of life. To investigate this possibility, we used a double-blind, active-placebo-controlled, individual-level, universal, preventative experimental design. Across three replications that included nearly 600 adolescents, a one-time intervention teaching an incremental theory of personality in September of participants’ ninth-grade year appeared to reduce the prevalence of clinical levels of depressive symptoms in May of that school year by approximately 40%. This finding was robust to a number of sensitivity analyses (see Tables S2 through S8 in the Supplemental Material). Analyses of self-esteem mirrored these findings. Finer-grained examinations of CDI:S symptom subscales showed significant treatment effects on negative mood and ineffectiveness but not on anhedonia.
Textual analyses (Pennebaker et al., 2007) further explored the psychological impact of the intervention on adolescents’ self-views. Assessing subtle linguistic clues in response to an open-ended writing prompt, we found that treated teens were less likely to use negative emotion and trait words, to talk about the past, and to talk about discrepancies (linguistic indicators of maladaptive counterfactual thinking) in their self-descriptions during the May follow-up. This index was also correlated with depressive symptoms at baseline and at follow-up. This means that the intervention may have influenced individuals’ self-schemata, perhaps even changing their unconscious perceptions about themselves during times of difficulty. This finding opens up new avenues for research on the effects of implicit theories as well as on mechanisms that sustain treatment effects on depressive symptoms.
Furthermore, moderation analyses supported our theoretical account for these effects. Adolescents with more of an entity theory of personality at baseline showed marked increases in depressive symptoms during the year if they were assigned to the control group. However, those individuals who were assigned to the incremental theory of personality intervention showed no such increase, which suggests that the intervention was particularly effective for people with an entity belief. Conversely, the current study did not find a significant sex moderation of the treatment effect on depressive symptoms or depression subscales, even though past research has shown that females develop adolescent depression at a higher rate than do males, possibly as a result of greater peer stressors and stress reactivity among females (Cyranowski, Frank, Young, & Shear, 2000; Hankin et al., 1998; Hankin, Mermelstein, & Roesch, 2007). Nevertheless, regardless of sex, the intervention precisely targeted one contributor to the onset of depressive symptoms during the transition to high school—an entity theory of personality—and reduced its impact on depressive symptoms.
Limitations
There are clear limitations to this research. First, these studies did not show that teaching adolescents that people can change treats depression. We found no evidence that levels of depressive symptoms decreased for any group of students. Instead, the intervention seemed to slow the normative increase in depressive symptoms, especially among students with an entity theory at baseline.
Next, the current research does not speak to the issue of whether an incremental theory intervention would be helpful in therapy. Our intervention was, very intentionally, quite “stealthy” (Yeager & Walton, 2011). That is, we did not directly tell students that it is in their best interest to believe people can change or that it would help them be less stressed or depressed. Instead, the intervention asked students to author the intervention content by writing notes to future students, avoiding the implication that they were getting treatment for depression. This saying-is-believing tactic can be helpful for promoting deeper processing of the material and avoiding stigma (Aronson, 1999; Walton, 2014; Yeager & Walton, 2011).
Moreover, it is unknown whether individuals who are currently depressed or who are at high risk for depression—for example, individuals who have a mother with a history of MDD (Goodman & Gotlib, 1999)—will benefit from an incremental theory intervention. Furthermore, we have not documented whether pubertal timing can interact with the treatment effects on depressive symptoms.
Relatedly, it is crucial to emphasize the context dependency and developmental dependency of the present intervention strategy. We do not expect that an incremental theory of personality would prevent risk for depression in all contexts or during all developmental periods. Our study was built on a precise theory of the role of social-cognitive interpretations of social adversity in spurring recursive thoughts that increase the risk for depression during high school. We predicted that if social difficulties, such as peer exclusion, rumormongering, and other forms of social aggression, are nearly ubiquitous—as in the transition to high school (Barber & Olsen, 2004; Crosnoe, 2011)—then there will be a greater tendency for many teens to engage in thoughts that could increase vulnerability to depression. During those times, students may be more likely to develop depression unless they are given a framework for understanding social events that prevents them from engaging in those thoughts. An implication of this account is that, potentially, the present intervention might have little or no effect on depression if the timing were different, perhaps even if it were delivered just a few weeks later in the first semester of high school when negative thinking may have already taken root (see Cook, Purdie-Vaughns, Garcia, & Cohen, 2012).
As with other brief psychological interventions that are a part of the canon of strategies available to clinical psychologists (see Pennebaker, 2004), the mechanisms that produced a sustained effect of this brief intervention are not fully understood. For instance, did teens clearly remember the specific content of the incremental theory message during the year, or did they forget it but only after it affected their self-schemata and began to provide a new lens for interpreting social adversity? Or did the intervention have the short-term effect of causing teens to make more friends, thereby buffering them from depressive symptoms and maladaptive self-schemas in the long run? The intervention may also have been effective as a result of biological mechanisms, such as stress reactivity, a predictor of higher rates of depression (e.g., Gotlib, Joormann, Minor, & Hallmayer, 2008). Indeed, Yeager et al. (2014) found that ninth graders who received an incremental theory intervention reported less stress in response to peer ostracism. These possibilities and others warrant further investigation (see Walton, 2014; Yeager & Walton, 2011).
Another limitation is our use of only a brief self-report measure of depressive symptoms. This is, of course, common in large-scale, light-touch studies like the present research, in part because the CDI has shown convergent validity with a clinical diagnostic interview despite its convenience and efficiency (Timbremont et al., 2004). Yet it is possible that adolescents may not have full insight into their depressive symptoms. Future research would greatly benefit from additional measures, such as a clinical diagnostic interview or a parent report of depressive symptoms, which would reduce false positive and false negative rates. Although we found treatment effects 8 months later, it is always possible that the intervention requires a booster session for even longer-term effects. Administering booster sessions and engaging in a longer-term follow-up may be informative about treatment effects on depressive diagnoses over time.
A final set of limitations is analytic rather than theoretical. First, the smallest of our three samples (Sample 1), which represented 13% of our data, happened to show significant baseline condition differences, by chance, but only for the dichotomized measure of depressive symptoms and not for the continuous measure of depressive symptoms. We did not exclude that sample entirely from the present report because systematically omitting data on the basis of the findings can lead to publication bias. Instead, we used a number of analytic methods to show that our conclusions did not depend on that baseline difference. Next, the treatment effect on continuous depressive symptoms in the full sample was marginally significant (p = .07), whereas there were significant effects (at p < .05) on the dichotomized clinically significant symptoms variable, two of the four symptom clusters, and the continuous depressive symptoms among students with an entity theory at baseline. Of course, a CDI:S measure would produce greater measurement error than would the full long-form CDI; thus, some inconsistency across analyses should be expected as a result of random variability alone. However, this result highlights the more general need to replicate the present study’s results and to more fully understand their boundary conditions before it would be responsible to apply them broadly in clinical or educational settings.
Implications
Although we acknowledge the limitations of this research, it is important to emphasize a number of potential implications of this study for mental-health policy. First, the intervention appears to have been effective at reducing the overall percentage of students with significant levels of depressive symptoms. Although it may be more effective to have a targeted treatment for students with an entity theory, researchers may have difficulty in categorizing students into entity theorists reliably, given that our study measured implicit theory on a continuous scale. Moreover, students with an entity theory may feel stigmatized if they are pulled from class to receive the intervention. Instead, our past studies have shown that the intervention helps reduce aggression, stress, and health for students regardless of baseline theories (Yeager et al., 2014; Yeager, Trzesniewski, & Dweck, 2013). Thus, the intervention appears to be best used as a “universal prevention” for all students—something that has been very difficult to accomplish in past studies (Stice et al., 2009). In fact, Stice et al. (2009) stated, “It may be prudent to . . . discontinue evaluation of universal prevention programs” (p. 499). The potential suggested by the present early stage research will hopefully breathe new life into universal prevention efforts.
Second, the present intervention was cost-effective and highly scalable. In the two larger samples—Samples 2 and 3—the intervention was delivered via the Internet in the school computer lab with no specialized training of school staff. It involved only one class period (although some students also received a background session about the brain that, as noted, did not seem to enhance treatment effects). This does not mean that the intervention had zero cost. In fact, a great deal of work was done in the piloting phase to customize the intervention for the given populations—for instance, changing the normative quotes from peers to match local colloquialisms and programming the intervention to seem like a normal survey that students would complete in the course of everyday schooling (see Yeager & Walton, 2011). Effort also went into designing procedures that fit within the fabric of the school day so that the experimental session could be carried out with high treatment fidelity. Nevertheless, the intervention had near-zero marginal cost. That is, after initial customization, there was little or no additional cost of giving the intervention to more students within the school. Given the relatively small investment of time and effort, and the possibility of saving many tens of thousands of dollars in lost productivity over a lifetime for a person who is prevented from depression in adolescence, the present intervention (or an improved version of it) may, after replication and extension, eventually prove to be a cost-effective option for educators and policymakers.
The present research also has a number of theoretical implications. First, this research reinforces social-cognitive theories of development (Olson & Dweck, 2008). Historical data have suggested that dramatic increases in depression during the transition to high school are inevitable (e.g., the control group in the present study; see Benner et al., 2011; Merikangas et al., 2010; Newman et al., 2007). Yet the present research confirms the classic notion that adversities in life do not have a direct effect on poor mental health but, instead, are filtered through a person’s social-cognitive style (Beck, 1976). This provides an important opportunity for intervention. It suggests that it can be possible to weaken the effect of an environmental risk on mental health by precisely targeting relevant social-cognitive factors before negative, self-reinforcing patterns of thinking have an opportunity to gain momentum (Cohen & Sherman, 2014). In the present research, we attempted to alter an implicit theory that, in much past research, has been shown to give rise to negative responses to social adversity, and we did it at a time known to be laden with difficulties, such as exclusion and victimization. 6 We showed that when this was done, the typical increases in depressive symptoms during freshman year were slowed substantially.
Second, this research adds to a growing number of experimental studies that have shown that, when attempts are made to address important social problems that have a psychological component, sometimes “less is more.” For example, in some cases, 2 to 5 min of expressive writing exercises can be more effective than extensive counseling sessions for individuals coping with trauma (Pennebaker, 2004), and a 7-min writing exercise can halt the year-over-year decrease in marital satisfaction (Finkel, Slotter, Luchies, Walton, & Gross, 2013; for many more examples, see Walton, 2014, or Wilson, 2011). It is interesting that the Stice et al. (2009) meta-analysis of depression prevention programs showed that briefer programs were more effective than longer programs at preventing depression and that programs that involved homework—requiring individuals to write at home—were more effective than those that did not. Coincidentally, the present implicit-theories intervention involved expressive writing and was brief. Viewed from that perspective, the present findings are quite consistent with existing best practices.
Conclusion
It is important to replicate and extend these findings to deepen our understanding of the moderating and mediating mechanisms of the specific symptom clusters that are affected. Doing so is the most responsible next step before broader application. Nonetheless, it is encouraging that the present theoretically informed strategy of intervening to teach an incremental theory of personality appears to have made some headway on a seemingly intractable issue—universal prevention for depressive symptoms during adolescence.
Footnotes
Acknowledgements
We are grateful to the students and teachers involved in this research for their cooperation. We also thank Cary Catching, April House, Ahmad Saleh, Kerry Morrissey, Shannon Morrissey, Joseph Powers, Brian Spitzer, Rebecca Johnson, April Scott, and Hector Villalpando for their help with data collection and entry. We are also grateful to Chris Beevers, David Sherman, James Pennebaker, Kali Trzesniewski, Carol Dweck, and Patricia Brennan for their feedback or suggestions. All remaining errors are the authors’.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This work received funding from the Thrive Foundation for Youth, the Spencer Foundation, and the Raikes Foundation.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.