
Abstract
Schizophrenia, bipolar disorder, and major depression share several clinical and etiological factors. Coping is a critical mediator of the relationship between stress and psychopathology and a point of clinical intervention for all three disorders; however, little is known about their degree of overlap in coping style or the influence of unique or shared genetic diathesis. In this study, we examined five factors of coping within and across disorder proband and co-twin groups, modeled heritability, and tested for endophenotypic pattern in a sample of twin pairs recruited from the Swedish Twin Registry (N = 420). Although there was substantial phenotypic overlap across disorders, including low levels of productive problem-focused coping and high levels of disengagement, each disorder was associated with a unique profile across other dimensions of coping. We also found evidence of heritability for three of five factors, yet we found little evidence of genotypic overlap among disorders contributing to similar strategy use.
Although initially conceptualized as entirely distinct syndromes, schizophrenia, bipolar disorder, and major depression are multidetermined phenomena that share certain clinical features as well as risk factors. At the same time, the cardinal symptoms of these disorders are different, and it is generally assumed that some of the causal contributors will not be overlapping. In situations in which there are common risk factors and mechanisms, common treatment approaches would be indicated, and in situations in which there are disparate risk factors and mechanisms, different treatment approaches would likely be appropriate. A key question thus concerns discerning whether a particular risk factor or mechanism operates similarly or differently across these illness contexts.
Stressful life events play a particularly strong role in depression (Kendler, Karkowski, & Prescott, 1999), but these factors are also elevated in patients with bipolar disorder (Hlastala et al., 2000) and schizophrenia (Norman & Malla, 1993). Regardless of disorder, coping with stress would need to be considered as a critical bottleneck process in evaluations of how stress may contribute to psychopathology—a routing of all environmental stressors through a narrow array of available strategies that in some cases are inadequate to meet the demand. Coping may be defined as the process of responding to and potentially regulating stress, and it is a multidimensional and multidetermined set of constructs. It is fundamental to our understanding of psychopathology, given that it represents the interaction of stress and diathesis (Kendler, Kessler, Heath, Neale, & Eaves, 1991) and partially mediates the relationship between stress and psychopathology (e.g., McLaughlin & Hatzenbuehler, 2009; Meng, Tao, Wan, Yan, & Wang, 2011). Coping with stress and with symptoms is also a critical point of intervention in psychotherapy and predicts symptom severity within these disorders (e.g., Meyer, 2001; Van Rheenen, Murray, & Rossell, 2015).
Kendler et al. (1991) suggested that in some disorders, coping may be an endophenotype that marks one avenue of genetic influence on the etiology of psychopathology in interaction with exposure to stress. Endophenotypes are “risk traits” that lie on the pathways between the genetic and syndromal elements of various forms of psychopathology (Gottesman & Gould, 2003). Some coping styles, as assessed using various measures, have in fact been shown to be moderately heritable in the general population (see Table S1 in the Supplemental Material available online; e.g., Busjahn, Faulhaber, Freier, & Luft, 1999; Kendler et al., 1991; Kozak, Strelau, & Miles, 2005) and, thus, could be considered as candidate endophenotypes for psychiatric disorders. Alternatively, proclivity to a particular coping style may be an epiphenomenon of a disorder itself—whether by way of symptoms, medication, or another factor.
Although criteria for endophenotype status initially included specificity to one disorder (Tsuang, Faraone, & Lyons, 1993), this criterion does not hold up against more recent discoveries about shared genetics among disorders. It stands to reason that the higher the degree of genetic overlap, the more likely it is that the disorders share endophenotypes. Schizophrenia and bipolar disorder share a very high level of genetic overlap—on the order of 50% to 65% (Craddock, O’Donovan, & Owen, 2006; Lichtenstein et al., 2009; Purcell et al., 2009)—and bipolar disorder shares approximately 25% of its genetic factors with major depression (McGuffin et al., 2003). If any coping style is an endophenotype for one disorder, it may thus also be an endophenotype for the other disorders with which it overlaps genetically.
Using a diverse set of coping measures, researchers in separate studies have compared coping styles of patients with schizophrenia, bipolar disorder, and major depressive disorder with healthy volunteers (e.g., Lam & Wong, 2005; Van den Bosch, Van Asma, Rombouts, & Louwerens, 1992). In general, these studies have shown that patients with each of these disorders show lower levels of active, productive coping than do healthy volunteers. There are also findings suggestive of potentially diverse coping mechanisms across these disorders, in that patients with schizophrenia tend to use distancing, avoiding, and disengaging coping styles (e.g., Tait, Birchwood, & Trower, 2004); patients with depression tend to use ruminative styles (Nolen-Hoeksema, 2000) and escapism (Rohde, Lewinsohn, Tilson, & Seeley, 1990); and patients with bipolar disorder may also make greater use of avoidance (Goossens, Knoppert-van der Klein, & van Achterberg, 2008). In addition, stimulation avoidance and modifying excessive behavior during prodrome reduces the probability of manic episodes (Lam, Wong, & Sham, 2001). Bipolar disorder has also been associated with emotion-regulation abnormalities that predict aspects of symptomatology (Van Rheenen et al., 2015) and are linked with reduced frontal-amygdala connectivity (Kanske, Schönfelder, Forneck, & Wessa, 2015). However, no prior study has directly compared these three groups of patients with each other on the same measures of coping, which makes it difficult to discern whether these patterns are truly disorder specific. Furthermore, in no prior study have researchers used a genetically informative design to examine whether coping styles represent endophenotypes of these three disorders.
It thus remains unclear whether any coping style is shared phenotypically across schizophrenia, bipolar disorder, and depression; whether any aspect of coping reflects an underlying genetic diathesis for any of these disorders; and whether any such coping-related endophenotype is shared with one or both of the other disorders as a result of their genetic overlap.
To address these questions, we evaluated coping styles in samples of twins concordant and discordant for schizophrenia, bipolar disorder, and major depression, along with healthy comparison twin pairs. This approach permits tests of not only whether a coping style is shared phenotypically across disorders but also whether it is shared by non–clinically affected co-twins of probands with the three diagnoses. The non–clinically affected co-twins are at increased genetic risk for the disorder shown by their affected co-twin, but because they do not have the disorder overtly, these participants represent a form of control for phenotypic expression of illness, exposure to treatments, and other secondary factors. In other words, the nonaffected co-twins provide the basis for evaluation of whether a particular coping style is likely to be associated with a genetic diathesis to each illness and whether any aspect of coping helps to define that part of the genetic diatheses that overlap across these three disorders. Given the limited scope of the prior literature on these issues, as summarized earlier, there is little basis for specifying a model that predicts discrete areas of overlap and nonoverlap in terms of coping styles across disorders or across nonaffected co-twins. Rather, we used the logic of the discordant twin-pair design to parse the various possible patterns empirically, with an appropriate control for multiple testing, thereby hoping to provide a set of observations useful for subsequent model building.
Method
Participants
Participants were identified through the Swedish Twin Registry, which is managed by the Karolinska Institutet. Full recruitment procedures have been described by Lichtenstein et al. (2006). Twin pairs were eligible for inclusion if they were the same sex, between the ages of 25 and 65, and born in Sweden between 1940 and 1985 (inclusive). The age range was intended to exclude individuals who were young enough that they had not yet developed an emerging disorder or old enough that they had already developed signs of dementia. Other exclusion criteria were presence of a neurological disorder, history of significant head injury with loss of consciousness, mental retardation, history of substance dependence within 6 months of the screening interview, inability to read or comprehend spoken and written Swedish, or pregnancy/lactation at the time of evaluation.
This population of twins was screened by using hospital admission and discharge diagnosis information from the Swedish National Patient Registry to ascertain twin pairs with psychopathology. Screening for pairs comprising at least one twin with a diagnosis of schizophrenia or bipolar disorder yielded 562 potential probands: 257 male and 305 female. Monozygotic (MZ) and dizygotic (DZ) pairs were recruited randomly from this population. Zygosity was determined for twin pairs by using either DNA testing or a well-validated screening measure administered to parents and twins (Lichtenstein et al., 2006), which yielded 177 complete twin pairs with impulsivity data and of whom 77 were MZ, 97 were DZ, and 3 had undetermined zygosity. Healthy control twin pairs were recruited to match proband pairs on age, sex, and zygosity. Healthy control participants were excluded if they had a family history of schizophrenia or bipolar disorder.
Diagnostic interviewing was used in conjunction with hospital records to determine diagnosis for each individual, and twin pairs were then classified as controls or as concordant or discordant for schizophrenia or bipolar disorder, regardless of the initial recruitment classification. Individuals with schizoaffective disorder were included in the schizophrenia group. Discordant co-twins of probands were also included regardless of a history of nonpsychotic psychopathology, such as depression. Individuals recruited as control participants were also included regardless of history of depression, thereby creating for our purposes another diagnostic group of participants with major depressive disorder without a twin affected by schizophrenia or bipolar disorder. Individuals diagnosed with a different psychotic disorder were excluded from analyses that compared diagnostic groups.
Tests of sample representativeness
We tested whether the studied probands were comparable with the remainder of the recruited twin proband population in terms of sex, age, age at first hospitalization, and number of hospitalizations. For sex, we used a chi-square test of independence and phi (ϕ) as an estimator of effect size. For other variables, we used Cohen’s d. Cohen (1992) suggested that values below 0.2 may be considered small effect sizes, 0.5 is a medium effect size, and 0.8 is a large effect size.
Procedure
All measures were approved by the Regional Ethics Review Board, Stockholm, Sweden.
Clinical evaluation
Final diagnostic status was determined by consensus using both clinical interviews and register data, which included hospital records and lifetime history of hospital admissions from 1973 until the time of evaluation. A clinical psychiatrist interviewed each participant by using the Structured Clinical Interview for DSM–IV Axis I Disorders (SCID; First, Spitzer, Gibbon, & Williams, 1997) and the Structured Clinical Interview for DSM–IV Axis II Personality Disorders (SCID-II; First, Gibbon, Spitzer, Williams, & Benjamin, 1997). The SCID has demonstrated superior validity over standard clinical intake interviews (First, Spitzer, et al., 1997). Current symptoms were also rated by using the Hamilton Depression Rating Scale (Hamilton, 1960), Young Mania Rating Scale (Young, Biggs, Ziegler, & Meyer, 1978), Scale for Assessment of Negative Symptoms (Andreasen, 1983), and Scale for Assessment of Positive Symptoms (Andreasen, 1984). Acceptable validity and reliability have been demonstrated for each of these measures (Peralta, Cuesta, & De Leon, 1995; Williams, 2001; Young et al., 1978). Consensus diagnosis was determined by the clinical evaluation team at the Karolinska Institutet, which comprised two psychiatrists and one clinical psychologist (Dr. Hultman). All participants were clinically stable at the time of evaluation. No changes to medication regimen were made in relation to participation in the study.
Zygosity
Zygosity was initially determined using a self-report measure that includes physical similarity ratings and family conclusions about “identical” or “fraternal” status. This measure has demonstrated good validity (Reed et al., 2005). For participants with available DNA information, DNA zygosity tests were then conducted to determine percent of allele sharing between twins. This procedure modeled Hannelius et al. (2007) and used a highly multiplexed 47 single nucleotide polymorphism panel, including a sex-specific marker. Likelihood of zygosity for each pair was calculated assuming a 1% genotyping error rate (false positives).
Brief COPE scale
The Brief COPE scale (Carver, 1997) is an abbreviated coping measure that assesses 14 distinct types of coping. Carver (1997) found that the measure had adequate validity and reliability, and Meyer (2001) found evidence of concurrent and predictive validity in a psychiatric sample. A subset of 18 items was administered and scored on a 4-point scale from 0 to 3, and possible total scores ranged from 0 to 54. The scale directed participants to indicate their typical coping behaviors, not their responses to an individual stressor and not during a particular time frame. Thirty-five participants missed items. These participants were excluded from analyses of the derived factors for which they missed items.
Statistical analyses
Prior studies have used a wide variety of measures of coping, including factor scores derived from other samples as well as their own samples. Researchers in several studies have derived higher-order structures of the longer version of the COPE scale by using factor analysis, and there is substantial variability among reported results (Hasking & Oei, 2002). Three-factor (e.g., Lyne & Roger, 2000) and four-factor (Carver, Scheier, & Weintraub, 1989) solutions have been found, with inconsistencies in which items load on which factors. Very few factor analyses of the Brief COPE have been reported (Hasking, Lyvers, & Carlopio, 2011), but some support has been found for a three-factor structure containing problem-focused coping, emotion-focused coping, and either dysfunctional coping (Cooper, Katona, & Livingston, 2008) or avoidant coping (Hasking et al., 2011). Factor structure may vary as a function of sampling and, in particular, the relative numbers of individuals with different forms of psychopathology. Given this, and as suggested by the author of the Brief COPE (Carver, 2007), we undertook an analysis of its factor structure in the sample under study.
Our analysis used principal axis factoring with varimax rotation. Fit of the factor model was evaluated using the Tucker-Lewis index (TLI) and the root-mean-square error of approximation (RMSEA). The TLI, or nonnormed fit index, is an incremental fit index that penalizes for complexity. Hu and Bentler (1999) suggested using at or above .95 as a cutoff value for the TLI to indicate good model fit. The RMSEA is an absolute measure of fit, and it also penalizes complexity. Lower values on the RMSEA indicate better fit, and MacCallum, Browne, and Sugawara (1996) have used .01, .05, and .08 as indicators of excellent, good, and mediocre fit, respectively. Factor scores were derived and carried forward into subsequent analyses. To facilitate interpretation of factor content, we examined the highest loadings on each factor. In our interpretation, loadings less than .3 were excluded, and in the case of double loadings, items were assigned to the factor on which their loading was strongest. For an item to be included in a factor, its loading on that factor was required to be at least .05 higher than its loading on any other factor. Factor scores based on simple addition of these items were also derived and tested to ensure robustness of results, but factor scores were chosen because of small differences in loadings on multiple factors (less than .1 difference) for two items.
Group-level differences were analyzed using linear mixed modeling, given that this method allows for correlations, unequal variances, or both between within-group error terms. To control for the correlations between co-twins, we entered twin-pair number as a random variable in all analyses. Age and gender were entered as covariates. To examine levels of each phenotype across disorders and co-twins, we tested a model including all groups for each coping factor. Given that we tested the overall main effects of five factors of coping, Bonferroni correction for multiple testing was used to set a p-value threshold of .01. If the effect of group was significant, we examined pairwise comparisons. Eta squared (η2) was used as an estimator of effect size for the overall effect and for the effect of significant continuous predictors. 1 Cohen’s d was used for pairwise comparisons.
Heritability
Individual variation in coping may arise as a product of genetic differences, differences in environment, or a combination of both. Comparison of MZ twins, who share 100% of their genetic code, with DZ twins, who on average share 50% as would any two siblings, makes it possible to partition variance of a trait into components attributed to genetics and environment (Plomin, DeFries, Knopik, & Neiderhiser, 2013).
Structural equation modeling techniques use covariance matrices from twin pairs as well as these expected ratios of correlations to determine the relative effects of additive genetics (A), dominant genetics (D), common environment (C), and unique environment (E). Given that they make different predictions about the similarity of DZ twins relative to MZ twins, it is not possible to model both C and D effects simultaneously by using only data from twins reared together. A model incorporating A, C, D, and E terms would result in an underidentified model, in which the number of free parameters exceeds the statistics it predicts (Neale & Maes, 2004), unless the data could account for an additional parameter. Instead, ACE and ADE models can be tested separately. It is also not possible to model both dominant and epistatic effects simultaneously, and this use of the term dominant subsumes both dominant and epistatic genetic effects. Tests of ACE, ADE, AE, DE, and E models allows for comparison so that the best-fitting model may be selected. To test these models, we used the matrix algebra program Mx (Neale, Boker, Xie, & Maes, 2003), which uses maximum likelihood estimation to fit models to covariance matrices.
We used the chi-square statistic, the RMSEA, and the Akaike information criterion (AIC) to test model fit. The AIC is a relative measure of fit (Akaike, 1987). Lower values indicate a better fit, and the score penalizes additional parameters and, therefore, favors parsimonious models (Kline, 2011). Standardized maximum likelihood estimates were squared to yield proportion of phenotypic variance accounted for by each term.
Results
Diagnostic information and demographic characteristics are listed in Table 1. All participants were Caucasian. Diagnostic groups did not differ significantly in age or sex. The studied probands were comparable with the remainder of the twin proband population in terms of sex, χ2(1, N = 771) = 0.10, p = .92, ϕ = 0.01, age at first hospital admission, t(211) = 0.38, p = .70, d = 0.05, and number of hospital admissions, t(216) = 0.31, p = .75, d = 0.04. However, we detected age effects in our sample. Studied probands were younger than the remainder of the twin proband population, t(241) = 3.33, p = .001, d = 0.43, by a mean difference of 4 years—proband participants: M = 49.24, SD = 10.44; proband nonparticipants: M = 53.65, SD = 10.22.
Demographic Information
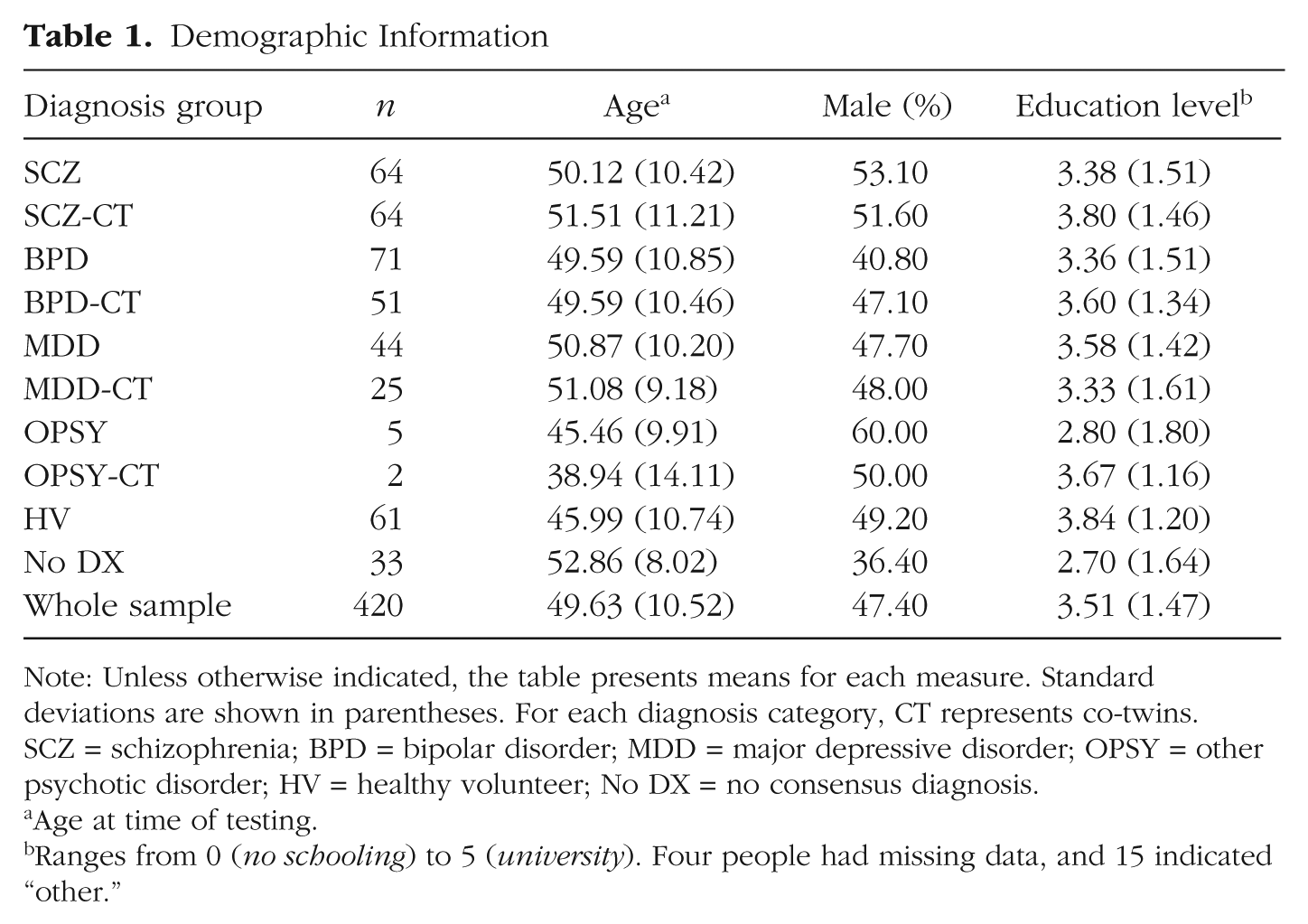
Note: Unless otherwise indicated, the table presents means for each measure. Standard deviations are shown in parentheses. For each diagnosis category, CT represents co-twins. SCZ = schizophrenia; BPD = bipolar disorder; MDD = major depressive disorder; OPSY = other psychotic disorder; HV = healthy volunteer; No DX = no consensus diagnosis.
Age at time of testing.
Ranges from 0 (no schooling) to 5 (university). Four people had missing data, and 15 indicated “other.”
Factor structure
Exploratory factor analysis yielded five factors with eigenvalues higher than 1. The results of an orthogonal rotation of the solution are shown in Table S2 in the Supplemental Material. The model showed good fit, TLI = .97, RMSEA = .03, 90% confidence interval = [0, 0.05]. For the purpose of interpreting the factors, we examined factor loadings at or above .3 onto each factor.
Four items loaded above .3 onto Factor 1: self-blame (.66), venting (.47), substance use (.34), and humor (.31). All four items are coping behaviors that involve the recognition of a problem but the failure to engage in productive, active responses. This factor was labeled nonproductive problem focused. Three items loaded onto Factor 2: active coping (.70), positive reframing (.55), and planning (.47). These three coping behaviors represent both recognition of a problem and active, productive responses to the problem. These behaviors are those most likely to effect a change in the stressful situation. This factor was labeled productive problem focused.
The two items that loaded onto Factor 3 were use of emotional support (.65) and use of instrumental support (.40). This factor was labeled support seeking. A fourth factor contained behavioral disengagement (.47), acceptance (.46), and self-distraction (.41). These three coping behaviors have in common a lack of recognition of a problem. In this context, we believe that acceptance items were rated in such a way to reflect passive, avoidant behaviors rather than active acceptance—a skill central to various psychotherapies. This factor was therefore labeled disengagement.
The two remaining items, denial and religion, loaded onto a fifth factor (.51 and .31, respectively). The relationship between these two coping styles is more complex but may represent cognitive, belief-based mechanisms of downregulating negative affect. They also may represent use of spiritual or mystical thinking, given that the denial item used is “I say to myself ‘this isn’t real.’” For this reason, the factor was labeled belief based.
Although we did not have sufficient power to use only the healthy subsection of the sample to derive the final model, performing the analysis in this subsample yielded a similar factor pattern. The primary difference observed was that items in productive problem-focused and support-seeking coping factors grouped together onto one factor, thereby leaving disengagement more differentiated into single-subscale factors.
Group differences
Linear mixed modeling yielded significant overall effects of group on four of the five factors (all but support-seeking coping). Pairwise comparisons yielded somewhat different patterns for each factor of coping style, as described later and illustrated in Table 2. For purposes of display, standardized means of regression-based scores are used to display group differences in Figure 1.
Profiles of Coping by Disorder
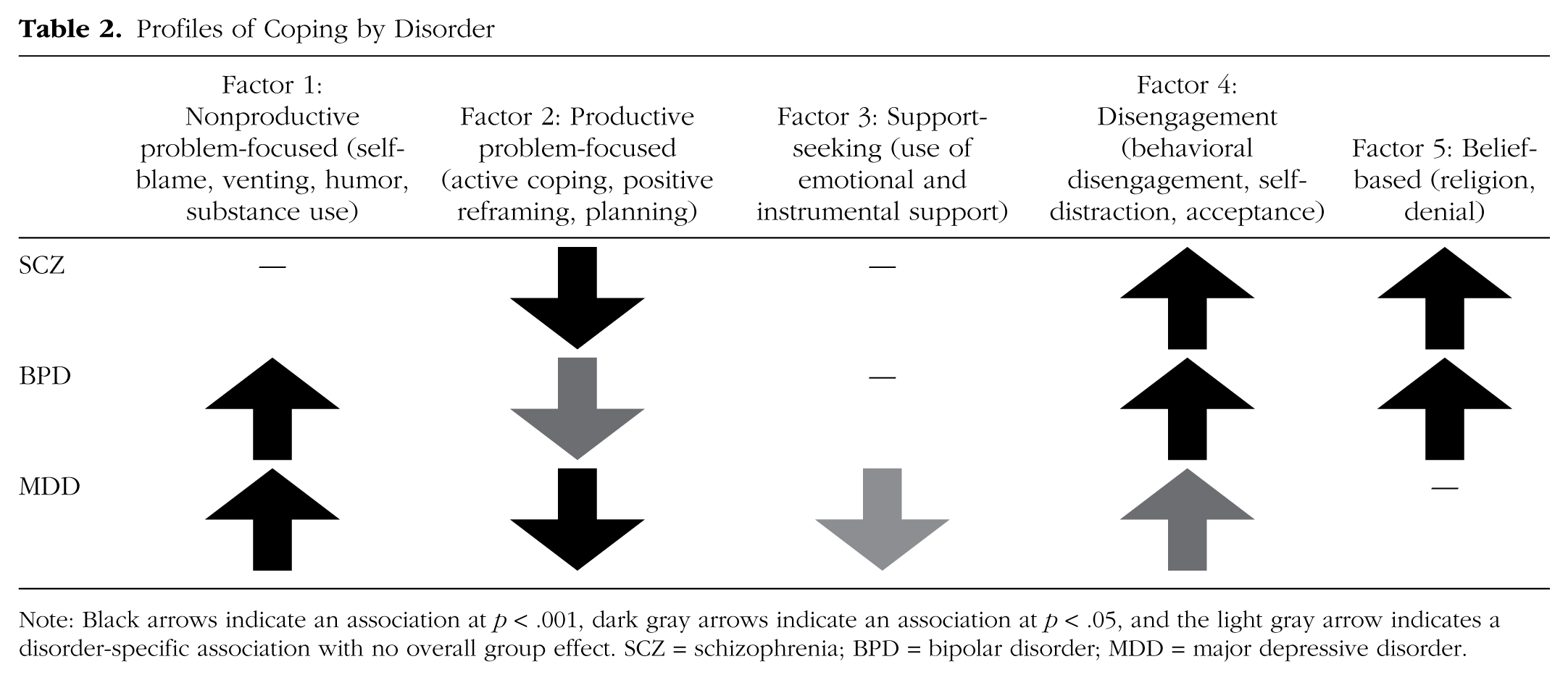
Note: Black arrows indicate an association at p < .001, dark gray arrows indicate an association at p < .05, and the light gray arrow indicates a disorder-specific association with no overall group effect. SCZ = schizophrenia; BPD = bipolar disorder; MDD = major depressive disorder.
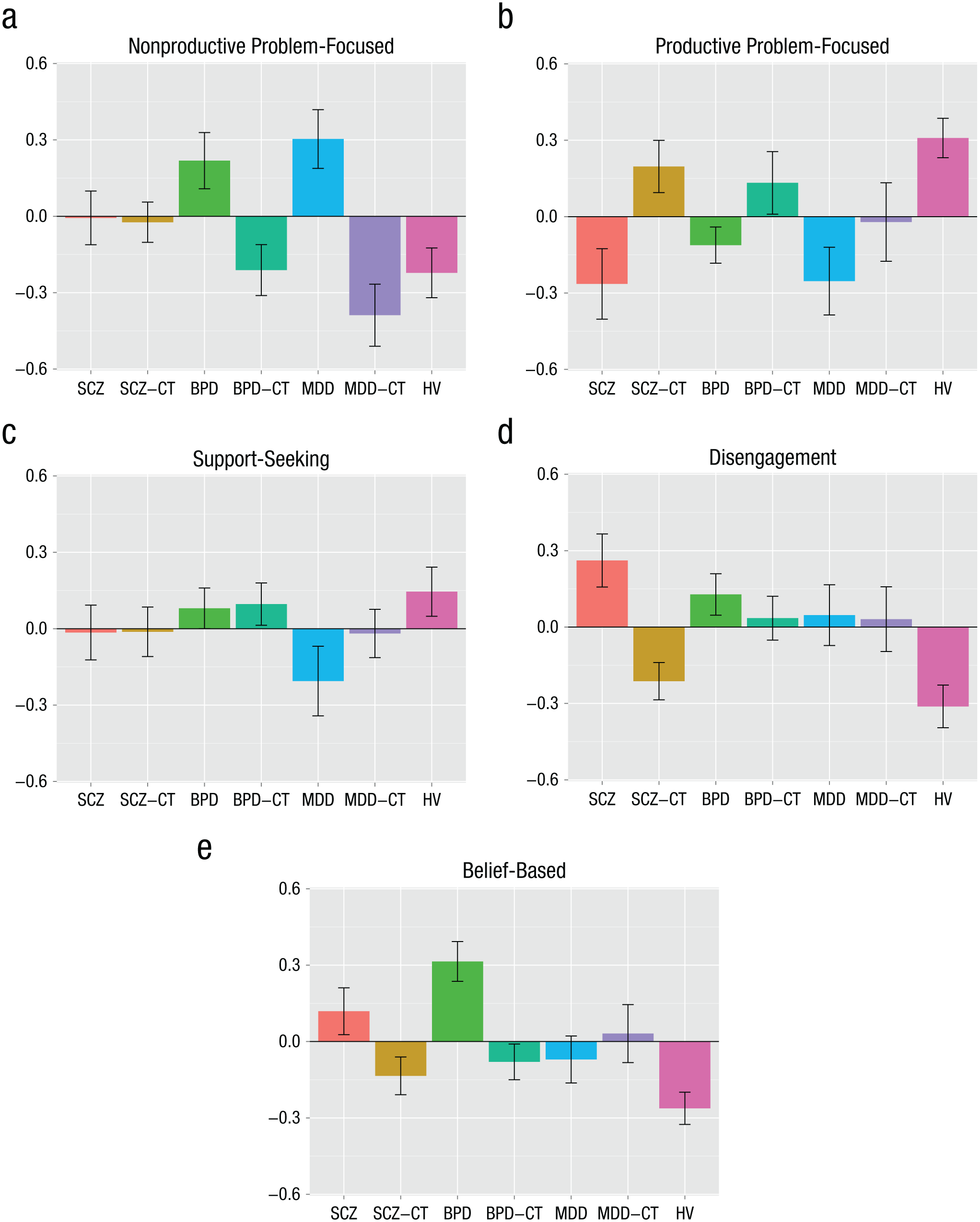
Results: group differences by coping factor. The graphs show standardized means for each measure. Error bars represent standard errors. For each diagnosis category, CT represents co-twins. SCZ = schizophrenia; BPD = bipolar disorder; MDD = major depressive disorder; HV = healthy volunteer.
Factor 1: Nonproductive problem-focused coping
There was a significant overall main effect of group on nonproductive problem-focused coping, F(6, 276.25) = 5.15, p < .001, η2 = .08. There was also a significant main effect of age, F(1, 214.06) = 10.85, p = .001, η2 = .03, such that younger individuals were more likely to engage in this form of coping, and no significant effect of sex. Individuals with major depression reported significantly higher levels of nonproductive problem-focused coping (M = 0.3, SD = 0.74) compared with healthy control participants (M = −0.22, SD = 0.75), p < .001, d = 0.77. Although individuals with major depression showed the highest levels of nonproductive problem-focused coping, individuals with bipolar disorder (M = 0.22, SD = 0.89) also scored significantly higher than did healthy control participants (p = .001, d = 0.58). Proband groups did not differ significantly from each other. Individuals with schizophrenia were intermediate (M = −0.01, SD = 0.80). Their scores were higher than those of healthy volunteers (p = .05, d = 0.35), lower than those of individuals with depression (p = .06, d = 0.24), and lower than those of individuals with bipolar disorder (p = .14, d = 0.38), but these differences were not statistically significant. Nonproductive problem-focused coping did not show familial association in any included disorder. Individuals with major depression scored significantly higher than their co-twins did (M = −0.39, SD = 0.61), p < .001, d = 0.94, as did individuals with bipolar disorder compared with their co-twins (M = −0.21, SD = 0.69), p = .002, d = 0.52.
Factor 2: Productive problem-focused coping
There was a significant overall main effect of group on productive problem-focused coping, F(6, 253.96) = 3.49, p = .002, η2 = .06, and no significant effect of age or sex. Healthy control participants (M = 0.31, SD = 0.59) were significantly higher on this active coping style than were individuals with schizophrenia (M = −0.26, SD = 1.05), p = .002, d = 0.60, major depression (M = −0.25, SD = 0.85), p = .001, d = 0.79, and bipolar disorder (M = −0.11, SD = 0.57), p = .01, d = 0.72. All co-twin groups showed values intermediate between probands and control participants, but these relationships are not significant. Schizophrenia was associated with the lowest scores on this factor.
Factor 3: Support-seeking coping
There was no significant overall main effect of group on support-seeking coping, F(6, 274.21) = 0.75, p = .61, η2 = .01, so we did not test pairwise comparisons. Major depression was associated with the lowest scores on this factor. There was a significant effect of age, such that younger individuals were more likely to engage in this form of coping, F(1, 189.58) = 27.95, p < .001, η2 = .07, and of sex, such that females (M = 0.18, SD = 0.69) engage in this form of coping more than males do (M = −0.20, SD = 0.72), F(6, 274.21) = 0.75, p = .61, d = 0.54.
Factor 4: Disengagement coping
There was a significant overall main effect of group on disengagement coping, F(6, 284.86) = 5.02, p < .001, η2 = .08, and no significant effect of age or sex. Individuals with schizophrenia were associated with the highest scores on this factor (M = 0.26, SD = 0.79)—significantly higher than control participants (M = 0.31, SD = 0.59), p < .001, d = 0.82. Control participants also scored lower than did individuals with bipolar disorder (M = 0.13, SD = 0.66), p < .001, d = 0.68, and individuals with major depression (M = 0.05, SD = 0.76), p = .01, d = 0.55. Individuals with schizophrenia scored significantly higher compared with their co-twins (M = −0.21, SD = 0.57), p < .001, d = 0.68, who did not differ from control participants. However, control participants scored significantly lower than did co-twins of individuals with bipolar disorder (M = 0.03, SD = 0.60), p = .01, d =0.57, and co-twins of individuals with major depression (M = 0.03, SD = 0.64), p = .03, d = 0.55, thereby indicating familial segregation.
Factor 5: Belief-based coping
There was a significant overall main effect of group on the factor comprising religion and denial as coping strategies, F(6, 282.00) = 5.67, p < .001, η2 = .09, and no significant effect of age or sex. Pairwise comparisons revealed that individuals with bipolar disorder (M = 0.31, SD = 0.63) were associated with the highest scores on this factor—significantly higher than co-twins of individuals with bipolar disorder (M = −0.08, SD = 0.49), p = .001, d = 0.65, healthy control participants (M = −0.26, SD = 0.48), p < .001, d = 1.00, individuals with major depression (M = 0.07, SD = 0.59), p = .003, d = 0.58, co-twins of individuals with major depression (M = 0.03, SD = 0.57), p = .05, d = 0.45, and co-twins of individuals with schizophrenia (M = −0.13, SD = 0.57), p < .001, d = 0.69. There was no significant difference between individuals with bipolar disorder and individuals with schizophrenia (M = 0.12, SD = 0.70), which was associated with scores significantly higher than those of their co-twins (p = .02, d = 0.37) and healthy control participants (p = .001, d = 0.64). Healthy control participants scored the lowest on this factor. Although individuals with major depression did not differ from healthy control participants on this factor (p = .100, d = 0.39), their co-twins had significantly higher scores than did healthy control participants (p = .04, d = 0.57).
Heritability
Estimates of proportion of variance accounted for by additive and nonadditive genetic and common and unique environmental effects are presented in Table 3 for all models tested, along with goodness-of-fit statistics for each model. The best-fitting models indicate heritability for Factors 1 (nonproductive problem-focused), 4 (disengagement), and 5 (belief-based) but not for Factors 2 (productive problem-focused) or 3 (support-seeking).
Heritability Models
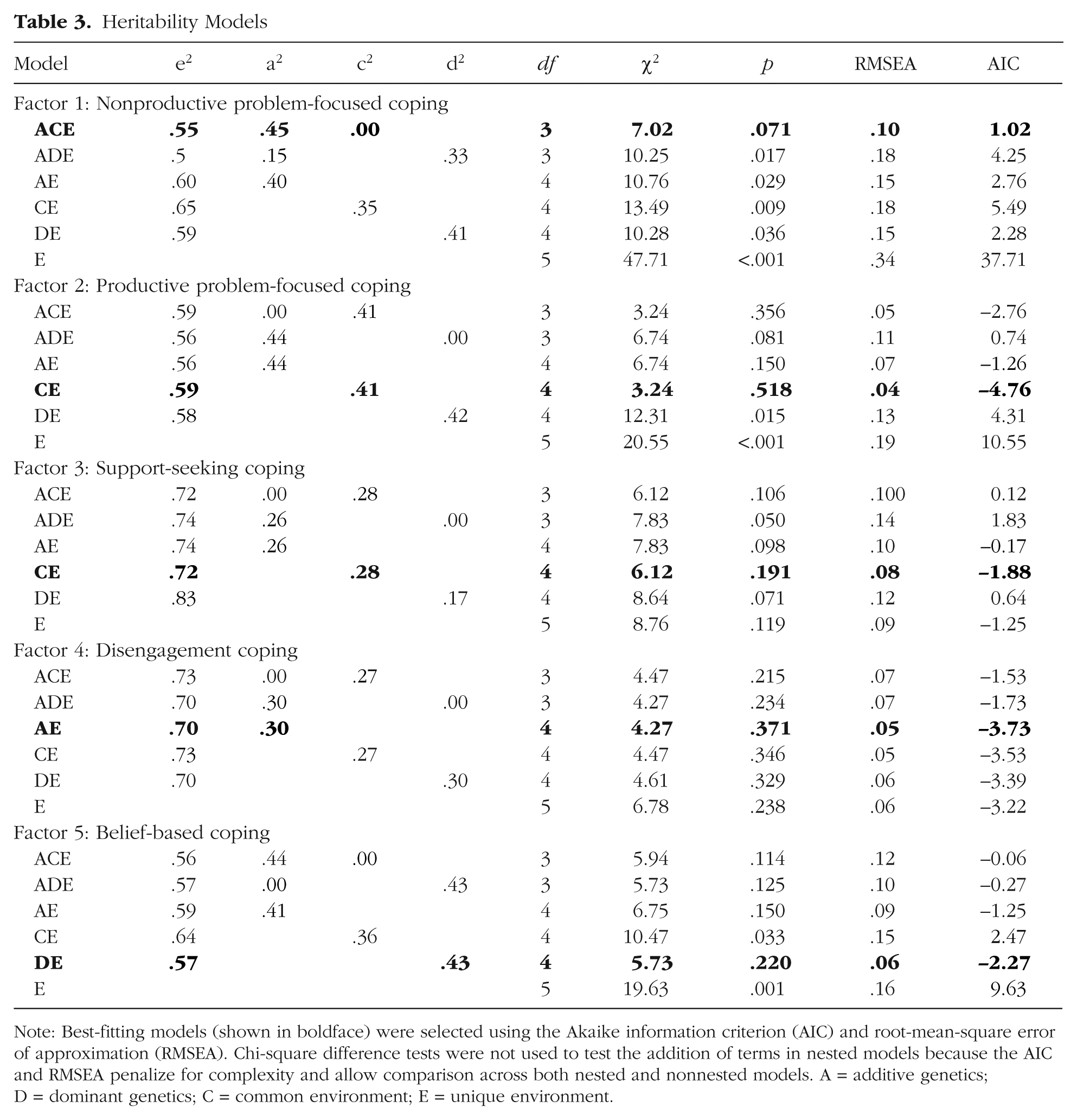
Note: Best-fitting models (shown in boldface) were selected using the Akaike information criterion (AIC) and root-mean-square error of approximation (RMSEA). Chi-square difference tests were not used to test the addition of terms in nested models because the AIC and RMSEA penalize for complexity and allow comparison across both nested and non-nested models. A = additive genetics; D = dominant genetics; C = common environment; E = unique environment.
For Factors 1 (nonproductive problem-focused) and 4 (disengagement), the best-fitting models (i.e., with the lowest AIC) included additive genetic effects (39.5% and 30.3% heritable, respectively). For Factor 4, the remainder was attributable to unique environmental effects. For Factor 1, the best-fitting model also included a term for common environmental effects, although the variance component was negligible. For Factor 5 (belief-based), the best-fitting model according to the AIC included dominant genetic effects accounting for 42.8% of the variance, thereby reflecting that the observed correlations between MZ twins was more than twice that of DZ twins. Chi-square difference tests indicated that DE provided satisfactory fit without addition of an A term.
For Factors 2 (productive problem-focused) and 3 (support-seeking), best-fitting models did not include a genetic component. They did include common environment, which accounted for 41.5% and 28.2% of the variance, respectively. The largest proportion of variance accounted for in all coping factors was unique environment.
Discussion
Coping styles show considerably more phenotypic than genetic overlap across schizophrenia, bipolar disorder, and depression. Patients from all three diagnostic groups showed lower than normal levels of productive problem-focused coping and higher than normal levels of disengagement coping. Furthermore, patients with depression and bipolar disorder were similar (but distinct from patients with schizophrenia) in showing higher than normal levels of nonproductive problem-focused coping (e.g., self-blame, venting), whereas patients with schizophrenia and bipolar disorder were similar (but distinct from patients with depression) in showing higher than normal levels of belief-based coping (e.g., religion). Nevertheless, although nonproductive problem-focused, disengagement, and belief-based coping all showed evidence of heritability, only disengagement coping patterned as an endophenotype and only for depression and bipolar disorder. Thus, other than for disengagement coping, there is little evidence that coping styles as measured in this study represent endophenotypic traits for these disorders or that genetic factors are responsible for the similarities in coping styles across them.
The five-factor structure derived included nonproductive problem-focused coping, productive problem-focused coping, support-seeking coping, disengagement coping, and belief-based coping. Both nonproductive and productive problem-focused coping styles involve the recognition that there is a problem, and the key division between them is the use of productive efforts toward mitigating the situation versus the use of nonproductive behaviors found in Factor 1—behaviors that indicate a focus on the problem but no attempt to fix it. The major distinction between both of these factors and disengagement coping is the recognition of a problem; disengagement behaviors all involve a lack of acknowledgment, which also leads to a lack of problem-solving behaviors. Support-seeking coping comprises both emotional and instrumental support seeking, but it does not include venting, which may be considered less productive. Belief-based coping, although it comprises religion, may not be captured by religiosity per se but rather by an ability to depersonalize and to have a sense of unreality and transience of the outside world.
We also found differential profiling of etiological inputs across the coping factors. Three of the five factors had significant genetic involvement and others did not; two showed an effect of common environment and others did not. In particular, the best-fitting models for productive problem-focused coping and support-seeking coping were CE models, which suggests no role in our sample for a genetic contribution but a substantial role for the common environment. This indicates that twin pairs were correlated, but there was not a stronger correlation for MZ twins than for DZ twins, thereby suggesting an influence of home environment, parenting, or other shared experience in promoting these coping styles. Although this sample did not show evidence of heritability, it is not possible to conclude that these coping styles truly are not heritable in the general population. These data do support, however, a greater role for common environment in promoting these more active coping styles than in encouraging more avoidant or escapist styles.
Substantial additive genetic influence was identified for productive problem-focused coping and for disengagement coping with no evidence of common environmental influence. Belief-based coping showed dominant genetic effects, which suggests that although three of the factors are heritable, this may result from different kinds of genetic input. It is also possible that the low correlation between DZ twins was spurious, in which case the effects may not genuinely be dominant in nature. Overall, these findings suggest that avoidant and escapist coping are substantially heritable but that common environment can contribute to more active coping styles, which may have a buffering effect against psychopathology.
Consistent with prior findings in which a diverse array of coping measures were used, results indicated that all groups showed lower than normal levels of productive problem-focused coping. The schizophrenia group showed substantial elevations on the disengagement factor and the belief-based factor, as well as the lowest score on the productive problem-focused factor. In previous studies, researchers have also linked schizophrenia with avoidant and distancing coping (Jansen et al., 1998; Tait et al., 2004). Lower threshold for disengagement may be present in schizophrenia as a result of reduced cognitive capacity, working memory, and problem-solving abilities. It is possible that stressors are more readily perceived as overwhelming and impossible to surmount, thereby causing individuals to “give up” and disengage from the situation entirely. Lysaker, Bryson, Marks, Greig, and Bell (2004) found that among individuals with schizophrenia, neurocognitive impairment predicted greater reliance on passive, avoidant coping strategies and reduced use of active, productive strategies.
Individuals with bipolar disorder were elevated on nonproductive problem-focused, disengagement, and belief-based coping styles. Although we were not able to assess this in the current study, it is possible that use of disengagement strategies is beneficial in the context of mania, whereas it is potentially maladaptive in the context of schizophrenia. Use of these strategies in bipolar disorder may represent active efforts to downregulate mania.
Individuals with depression showed higher levels of nonproductive problem-focused coping, which comprised self-blame and substance abuse. They also showed elevation on disengagement coping but lower levels than were observed in individuals with schizophrenia. Again, disengagement may occasionally be an adaptive process in the context of depression, given that the tendency of depressed individuals is to overengage with stressors. In fact, rumination, a core coping and emotion-regulation process associated with depression (Nolen-Hoeksema, 2000), reflects a difficulty disengaging. Alternatively, disengagement may be associated specifically with anhedonic symptoms. Depression was also associated with the lowest scores on the support-seeking factor, although this factor did not show significant differences in an overall analysis including all diagnostic and twin groups. This is consistent with the notion that social support buffers against depression and that depressed individuals may isolate themselves further.
Within disorders, most coping factors do not appear to be endophenotypes. However, disengagement coping showed familial segregation in bipolar disorder and major depressive disorder. This suggests that disengagement coping styles are genetically related to both disorders and may in fact be influenced by a section of the 25% of genetic inputs shared between the disorders. Although disengagement coping was highest in individuals with schizophrenia, it did not appear to be an endophenotype of this disorder, which suggests it is secondary to symptomatic status. This also indicates that although disengagement coping is elevated in all three disorders, the mechanisms underlying this elevation differ across disorders.
It could be questioned whether the patterns of group differences observed in this study would be altered with a different (more or less granular) representation of coping dimensions, such as a simpler two-factor solution with adaptive and maladaptive components. In secondary analyses, we derived a two-factor model, and, indeed, all psychiatric groups were significantly higher on the factor that would be considered maladaptive, whereas the healthy volunteers were higher on a factor comprising more typically adaptive strategies. We ultimately selected a five-factor model for both empirical and theoretical reasons. Empirically, the two-factor model had substantially poorer fit. The five-factor model had superior fit to one-, two-, three-, and four-factor models. When two factors were imposed, two coping subscales did not load at above .3 onto a factor. The five-factor model had simple structure, and every subscale loaded at above .3 onto a factor. Theoretically, although the two-factor model supports the elevation of maladaptive coping broadly in psychopathology, it obfuscates the underlying relationships between coping behaviors and disorders that aggregate to appear as comparable total sums. In the context of psychopathology, there is apparent merit to considering more differentiated models.
Given that this analysis is cross-sectional, no conclusions can be drawn about whether observed associations between psychopathology and coping style suggest that poor coping predisposed to vulnerability for the disorder or that the illness reduced coping efficacy. Longitudinal studies of coping could allow researchers to tease apart these two possibilities, both of which may contribute to observed differences in patient and healthy populations. It is also important to consider that this factor structure was derived in the context of psychopathology, which naturally leads to factors that reflect group differences in psychopathology. A very similar factor structure was produced by performing the analysis with the affected individuals excluded, but the sample size left us underpowered to use this model in our final analyses. In addition, heritability modeling was performed in the entire sample as a result of sample size; thus, heritability may be underestimated if individuals with psychopathology show larger differences from co-twins generally.
Given that the version of the Brief COPE used was further abbreviated, results may not generalize to the structure of the complete scale. We also relied entirely on self-report, and memory fallibility as well as biased reporting may influence validity of the data. In addition, only three diagnostic groups were included; thus, we cannot infer information about coping style across more disorders, despite its association with many. Our major depressive disorder group was also created post hoc and was not specifically recruited. Finally, our sample size was relatively small, and a larger sample would potentially yield more accurate estimates of heritability and group means, as well as the comparison of MZ and DZ twins within diagnostic group. A larger sample would also allow heritability calculation in healthy control participants and diagnostic groups separately, which could illustrate whether the effect of psychopathology masks predispositions for coping style.
Despite these limitations, the observed pattern of findings represents a step toward uncovering the relationship between coping with stress and development of psychopathology. This set of analyses helps to uncover differential relationships of coping style across disorder by offering suggestions as to the plausible causal mechanisms involved in the etiology and maintenance of different symptom clusters in the face of stress, but much more is still obscured. For example, longitudinal work can help to tease apart the cases in which coping style created vulnerability and risk for psychopathology from those in which it emerged as a clinical phenotype in the context of the illness. Experience sampling methodology may illuminate what coping styles predict increases or decreases in symptoms during the course of a day or a week, thereby providing clues about the role of coping in maintenance of psychopathology.
In addition, here we are still wedded to diagnostic categories as indicators of symptom clusters, but use of symptom-level data may tease apart what symptom or symptoms are specifically related to these coping factors. For example, schizophrenia comprises multiple factors of symptomatology that can be present to varying degrees across individuals (e.g., Wallwork, Fortgang, Hashimoto, Weinberger, & Dickinson, 2012), and there may be coping styles that uniquely associate with symptom clusters. Moreover, a focus on context may be particularly important in understanding the process of coping and regulating emotions in psychopathology (Aldao, 2013), given that flexibility in coping style is associated with lower levels of psychopathology (e.g., Bonanno, Papa, Lalande, Westphal, & Coifman, 2004). The field of coping research is rich, complex, and longstanding. As it extends into the future, there is more to be done to uncover how the structure of coping can be understood in the context of varying environments and clusters of psychiatric symptoms.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This work was supported by National Institutes of Health Grant ROIMH052857, the Swedish Research Council, and Stockholm County Council.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.