
Abstract
Pediatric cancer caregivers are typically present at their child’s frequent, invasive treatments, and such treatments elicit substantial distress. Yet variability exists in how even the most anxious caregivers cope. Here we examined one potential source of this variability: caregivers’ tendencies to self-distance when reflecting on their feelings surrounding their child’s treatments. We measured caregivers’ self-distancing and trait anxiety at baseline, anticipatory anxiety during their child’s treatment procedures, and psychological distress and avoidance 3 months later. Self-distancing buffered high (but not low) trait anxious caregivers against short- and long-term distress without promoting avoidance. These findings held when controlling for other buffers, highlighting the unique benefits of self-distancing. These results identify a coping process that buffers vulnerable caregivers against a chronic life stressor while also demonstrating the ecological validity of laboratory research on self-distancing. Future research is needed to explicate causality and the cognitive and physiological processes that mediate these results.
Keywords
Pediatric cancer is the leading cause of disease-related deaths for children and adolescents in the United States (American Cancer Society, 2014). Although the threat of losing a child to cancer and the multiple psychosocial challenges faced by caregivers clearly contribute to their distress, the difficult, invasive, treatment-related procedures that their child undergoes play a major role in predicting caregivers’ distress (Best, Streisand, Catania, & Kazak, 2001; Kazak et al., 1995; Norberg & Boman, 2008, 2013; Phipps, Dunavant, Lensing, & Rai, 2005). Caregivers are almost invariably present during these procedures, which they often describe as worse than the disease itself (Hedström, Haglund, Skolin, & Von Essen, 2003; Ljungman et al., 1996).
To date, most research on pediatric cancer caregivers has focused on answering questions about the level of the modal caregiver’s long-term stress reactions (e.g., Dunn et al., 2012; Phipps et al., 2015; Stuber, Christakis, Houskamp, & Kazak, 1996) and identifying the social and environmental resources that generally endanger or protect caregivers from the psychosocial difficulties associated with their situation (e.g., Greening & Stoppelbein, 2007; Pai & Kazak, 2006; Rosenberg et al., 2014). Although this research generally ignores individual differences among caregivers, other research on pediatric cancer caregivers suggests that individual differences in personal dispositions play an important role in determining which caregivers are most likely to experience high levels of distress. Specifically, this research suggests that high levels of trait anxiety put caregivers at risk for both heightened anxiety at the time of treatments and longer-term symptoms of psychological distress (e.g., Dunn et al., 2012; Harper et al., 2013; Harper et al., 2015; Harper, Peterson, et al., 2014; Peterson et al., 2014; Sloper, 2000). Indeed, in an earlier study of pediatric cancer caregivers, Hoekstra-Weebers, Jaspers, Kamps, and Klip (1999) concluded that “trait anxiety was the strongest predictor of [caregivers’] future distress” (p. 1526).
Yet even highly anxious caregivers vary substantially in their immediate and long-term reactions to their child’s treatments, but beyond some prior work, by the first author and his colleagues (Harper et al., 2013; Harper et al., 2015; Peterson et al., 2014), little is known about the sources of such variability. In the present study we aimed to fill this knowledge gap by turning to basic psychological theory and research on self-distancing. Specifically, we examined whether a caregiver’s tendency to spontaneously self-distance when reflecting on their feelings surrounding their child’s painful cancer treatments plays a role in explaining this variability, as the body of work on emotion regulation suggests it should.
When people encounter stressful events they often try to make sense of their feelings (Wilson & Gilbert, 2008) by visualizing them in their imagination (Kross & Ayduk, 2011). Prior research performed with unselected, subclinical, and clinical samples indicates that people who adopt a self-distanced or “fly on the wall” visual perspective (versus a self-immersed, first-person visual perspective) are buffered against many of the harmful consequences associated with analyzing negative experiences (e.g., rumination, exaggerated emotional and physiological reactivity; e.g., Kross, Ayduk, & Mischel, 2005; Kross & Ayduk, 2008; Kross, Gard, Deldin, Clifton, & Ayduk, 2012; Wisco et al., 2015; Wisco & Nolen-Hoeksema, 2011). This has been found in studies where participants self-distanced in the context of experimental manipulations and studies where participants engaged in this process spontaneously (e.g., Ayduk & Kross, 2010; Grossmann & Kross, 2010; Kross et al., 2005; Verduyn, Van Mechelen, Kross, Chezzi, & Van Bever, 2012). Moreover, many of these studies find that self-distancing is particularly helpful for buffering vulnerable individuals against exaggerated distress (Bruehlman-Seneca, Orvell, Kross, & Ayduk, 2015; Kross & Ayduk, 2009; Kross et al., 2012).
Collectively, these findings suggest that self-distancing may serve as a buffer against stress among high trait anxious pediatric cancer caregivers. However, all of this self-distancing work with vulnerable groups has been performed in the laboratory. No research of which we are aware has examined whether these findings would be observed in vulnerable individuals as they grapple with ongoing stressors in their daily lives. The primary goal of this work was to address this issue. In so doing, we aimed to simultaneously address two basic science questions: (a) Does research on self-distancing generalize to the real world? and (b) Does self-distancing buffer high vulnerable pediatric cancer caregivers against short- and longer-term distress?
Guided by the self-distancing research described earlier, we predicted that high trait anxious caregivers who spontaneously self-distanced as they reflected on their child’s painful treatments would be buffered against both heightened anticipatory anxiety just prior to their child’s treatments and against longer-term distress associated with these anxiety reactions. Because prior research has generated conflicting findings on the benefits of self-distancing for people not identified as psychologically vulnerable, with some work indicating that self-distancing is useful for such individuals (Wisco & Nolen-Hoeksema, 2011) and other work indicating an absence of any effects (e.g., Kross & Ayduk, 2009; Kross et al., 2012), we were agnostic about whether these beneficial effects would be present but much weaker in low trait anxious caregivers or simply not present at all.
We also aimed to address two important secondary questions. First, does self-distancing have significant buffering effects even when “pitted” against other variables that buffer caregiver distress? Prior research has identified two significant buffers of caregiver distress: the size of the caregivers’ social support network (Harper et al., 2015) and the caregivers’ perceived self-efficacy for caregiving tasks at the time of treatments (Harper et al., 2013; Peterson et al., 2014). Therefore, an important test of whether self-distancing serves as a protective factor for high anxious groups is whether it moderates the effects of trait anxiety on short- and long-term distress while controlling for these other protective factors. We expected that it would.
Second, prior research has yielded conflicting findings regarding the relationship between spontaneous self-distancing and avoidance. Studies examining people’s tendency to adopt a self-distanced perspective as they analyze their feelings has consistently failed to reveal significant relationships between self-distancing and avoidance (e.g., Ayduk & Kross, 2009, 2010; Kross et al., 2012). However, some other studies examining people’s tendency to adopt a self-distanced perspective when they simply recall negative experiences has found positive links between self-distancing and avoidance (e.g., Kenny et al., 2009; Williams & Moulds, 2007; cf. McIsaac & Eich, 2004). In the current study, caregivers provided data on their levels of avoidance at the 3-month follow-up. This provided a naturalistic opportunity to study how self-distancing and avoidance are related. Guided by prior research indicating that self-distancing does not promote avoidance when people adopt this perspective to analyze their feelings—that is, the process we measured in the current study—we did not expect self-distancing to promote avoidance.
Method
Overview
This study was part of a larger, longitudinal study of families of children in active treatment for cancer. It was conducted at two major children’s hospitals; one was in the Midwest and the other in the south-central part of the United States. All families were initially contacted by medical staff to take part in the study. Research assistants obtained consent from eligible families, 87% of whom agreed to participate. Families were eligible if (a) the child was between 3 and 12 years old, (b) the parent and child were able to speak and the parent could read English, and (c) the child had been diagnosed with cancer within the past 18 months and was receiving cancer treatment-related procedures regularly. Data were collected at study entry, immediately before and after up to three subsequent treatment procedures, and at follow-ups 3 and 9 months after the last treatment procedure at which data were collected. Although the larger study concerns both primary caregivers and their children, in this study we focus only on the primary caregivers who provided data at more than one treatment. Furthermore, because prior research has not yet documented a direct relationship between anticipatory anxiety before treatments and psychological distress measured at nine months (and we expected self-distancing to primarily affect anticipatory anxiety), we examined only data from the 3-month follow. Primary caregivers received $15 gift cards for initial assessments and $20 gift cards for each subsequent assessment; their children received $10 gift cards for the same assessments. The Institutional Review Boards at both hospitals approved the study.
Participants
Participants were 99 primary caregivers from the larger sample who had answered two questions about self-distancing questions and provided data for at least two of their children’s treatment procedures. Some of these participants or their children participated in other cross-sectional or longitudinal studies on coping with pediatric cancer (Harper et al., 2013; Harper et al., 2015; Harper, Goodlett, et al., 2014; Harper, Peterson, et al., 2015; Peterson et al., 2014). 1 Their mean age was 33.98 (SD = 6.96; children age M = 6.59, SD = 3.11). Caregivers were either parents (97%) or grandparents (3%). Of caregivers, 82% were the mothers of the child in treatment and 73% self-identified as White, 20% as Black/African American, 4% as Hispanic/Latino, and 3% as other racial/ethnic identities. A majority (60%) of the children were male; 79% were diagnosed with acute lymphocytic leukemia, the most frequent pediatric cancer in the United States. Children’s ethnicities reflected those of their caregivers.
Procedure
Upon entry into the study, caregivers completed an interview and several questionnaires about themselves and their children. In the months that followed, we assessed how anxious caregivers felt just prior to cancer-related treatments. Data were collected for up to three cancer-related treatments. These treatment procedures involved port starts (insertion of a needle into a port implanted in the child’s chest), lumbar punctures, or bone marrow aspirations. Three months after the last procedure at which data were collected, caregivers were mailed questionnaires that asked questions relevant to their current psychosocial status.
Independent variables
Trait anxiety
Caregivers’ trait anxiety was assessed at study entry with the 20-item Trait Anxiety subscale of the State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983). The Trait Anxiety subscale is intended to measure the predisposition to experience chronically high levels of anxiety. A representative item is “I feel nervous and restless” (item M = 2.33, SD = 0.63, α = .91.). Caregivers used a 5-point Likert-type scale (not at all like me to exactly like me). The Trait Anxiety subscale of the STAI is a widely used measure of anxiety as a personality attribute; an extensive literature supports both the reliability and construct validity of this measure (Spielberger, 1989; Spielberger & Reheiser, 2004).
Spontaneous self-distancing
Caregivers’ tendency to spontaneously self-distance while reflecting on their feelings surrounding their child’s painful cancer treatments was also assessed at study entry as part of an interview. Prior research has assessed this tendency by asking participants to first recall and then try to make sense of a recent painful past experience. Subsequently, participants are asked to answer two questions that assess their tendency to spontaneously adopt a self-distanced or “fly on the wall” visual perspective as they try to make sense on their feelings (e.g., Kross et al., 2014; Mischkowski, Kross, & Bushman, 2012; Park et al., 2014). The self-distancing questions that accompany these instructions have been used in multiple studies and have been demonstrated to be construct valid (e.g., Ayduk & Kross, 2010; Kross et al., 2012; Kross et al., 2014; Mischkowski et al., 2012; Park et al., 2014).
The current study employed a version of this protocol and two questions that were tailored to target caregivers’ experiences thinking about their child’s stressful cancer procedures. Specifically, a research assistant instructed each caregiver to
think back to your child’s most recent hospital visit, and your experience while he or she received treatment or a diagnostic procedure related to their illness. Please go back to the time and place of the experience and see the scene in your imagination. Take a few moments to recall this event. Once you have it in mind, let me know.
The assistant waited for the caregivers to indicate that they recalled the event. The research assistant then instructed the caregivers “to spend about a minute thinking about the causes and reasons underlying the thoughts and feelings you experienced during that experience. Try to understand the emotions you experienced during the event.”
Caregivers were given up to 60 seconds to complete this imagery task. Next, we used two items to assess spontaneous self-distancing. First, participants rated the extent to which they adopted the perspective of an immersed participant (i.e., “saw the event replay through my own eyes, as if I were right there”) versus a distanced observer (i.e., “watched the event unfold from the perspective of an observer, in which I could see myself from afar”) as they pondered their deepest thoughts and feelings during the task. Caregivers used a scale from 1 (predominantly immersed participant) to 7 (predominantly distanced observer). Next, we had participants rate how far they were from the scene in their mind’s eye during the task; responses were made on a scale from 1 (very close, saw it through my own eyes) to 7 (very far, saw it as if an observer). Responses to the two questions were averaged to create a single self-distancing index (M = 2.55, SD = 1.66). 2
Although responses to the two questions were significantly related (α = .75), preliminary analyses revealed that several participants gave quite different responses to them. Given that the two questions are intended to assess the same construct (i.e., self-distancing), we performed a residual analysis to identify outliers with regard to consistency in response to the two questions—that is, we plotted the standardized residuals for the two self-distancing items on a boxplot, used the 1.5 interquartile range away from the 25th and 75th percentiles as cutoffs, and identified eight participants who were outliers (i.e., the size of their residuals exceeded these parameters); they were removed from the primary analyses. When these eight cases were removed, the mean, standard deviation, and coefficient alpha for the remaining primary caregivers were M = 2.45, SD = 1.69, α = .89. The results of analyses with and without the eight outliers were virtually identical. However, because the self-distancing scores of the latter group were more reliable, we report the findings of analyses that exclude the outliers.
Covariates
Social support network size
Size of the caregivers’ social support network was assessed with I. G. Sarason, Levine, Basham, and Sarason’s (1983) brief measure of social support. Specifically the size of the network was operationally defined as the average of caregivers’ report of the number of people who would provide support across the six different areas of need (e.g., providing dependable help; M = 4.23, SD = 2.46; α across six areas = .95). A large research literature supports the reliability and validity of this assessment of perceived size of one’s social support network (Prodicano & Smith, 2013; B. R. Sarason, Sarason, Hacker, & Basham, 1985; I. G. Sarason & Sarason, 1985).
Caregiver self-efficacy
The procedures for assessing caregiver treatment self-efficacy are described in detail in Harper et al. (2013). Prior to each treatment, caregivers were presented with six caregiving tasks specific to their child’s treatment procedure that day (e.g., keeping the child calm before the procedures began; gaining needed information from medical staff). For each task, caregivers rated its importance and their confidence in performing the task effectively. Self-efficacy was operationalized as the product of these scales. Peterson et al.’s (2014) findings indicate that this measure is construct valid. These scores were averaged across treatment sessions (all αs across treatment sessions >.76) and then standardized with a z-score transformation. Research using this measure of self-efficacy (Harper et al., 2013; Peterson et al., 2014) finds that self-efficacy about keeping the child calm before the procedure predicts caregivers’ state anxiety prior to cancer-related procedures, self-rated distress during the actual procedures, mood following the procedures, and symptoms of posttraumatic stress at the 3-month follow-up. As would be expected, all of these relationships are negative; that is, the greater the self-efficacy, the less psychological distress. 3
Dependent variables
Anticipatory anxiety prior to treatment procedures
Caregivers’ anticipatory anxiety just prior to their child’s treatment procedures was assessed with the 20-item State Anxiety subscale of Spielberger’s STAI (Spielberger et al., 1983). This subscale is intended to measure anxiety in response to a specific stimulus or situation; this kind of anxiety is considered transitory (Hedberg, 1972). A representative item is “I am worried.” Caregivers used a 5-point response scale (not at all to exactly) to indicate their level of state anxiety. A large research literature supports the reliability and construct validity of this subscale of the STAI (Spielberger, 1989; Spielberger & Reheiser, 2004).
All caregivers provided state anxiety scores for at least two treatments and 85 of them (87%) provided state anxiety scores for all three treatments. State anxiety scores were reliable across treatment procedures (α = .87). Thus, they were averaged across treatments to form a single state anxiety index (item response M = 2.50, SD = 0.42). 4
Psychological distress at 3-month follow-up
Three months after the last treatment procedure (months since baseline assessment: M = 6.83, SD = 2.62, range = 3.65–13.17) 5 caregivers received a mailed questionnaire that contained two scales that assessed symptoms of psychological, distress—the 18-item Brief Symptom Inventory (BSI-18; Derogatis, 2001) and the 22-item Impact of Events Scale (IES-R; Horowitz, Wilner, & Alvarez, 1979; Weiss & Marmar, 1997). Both measures had a 0 (never) to 4 (very often) response scale, which caregivers used to describe how frequently they were currently experiencing the symptoms presented in each measure. The BSI-18 asked caregivers about psychiatric symptoms of anxiety (6 items, M = 0.82, SD = 0.71, α = .84), depression (6 items, M = 0.76, SD = 0.66, α = .84), and somatization (6 items, M = 0.53, SD = 0.69, α = .88 ). A large literature supports the reliability and construct validity of BSI-18 as a screening for symptoms of psychiatric distress (Boothroyd, 2003; Maruish, 2004; Zabora et al., 2001).
The IES-R asked participants about symptoms associated with posttraumatic stress: hyperarousal (6 items M = 0.98, SD = 0.76, α = .73), intrusion (8 items, M = 1.38, SD = 0.87, α = .90), and avoidance (8 items M = 1.03, SD = 0.74, α = .82) in relation to their child’s previous treatments over the past several months. The IES-R has been shown to correlate well with independent assessments of posttraumatic stress disorder using criteria from the Diagnostic and Statistical Manual of Mental Disorders. Research on the IES-R indicates it is a reliable and construct valid measure of symptoms of posttraumatic distress (Creamer, Bell, & Failla, 2003; Weiss, 2004).
The subscales were all significantly intercorrelated within each measure and across the two measures. We combined all of these BSI and IES subscales (except Avoidance) to create a reliable single composite measure of psychological distress at the 3-month follow-up. To do this we z-score-transformed the Anxiety, Depression, Somatization, Hyperarousal, and Intrusion subscales and then averaged them to create a single composite index of global psychological distress. The measure was internally consistent, α = .85. We did not include Avoidance in this composite measure because, as noted earlier, we wanted to examine the relationship between self-distancing and avoidance independently of the other psychological distress measures.
Results
Overview of analyses
First, zero-order correlations were computed to determine if trait anxiety and spontaneous self-distancing measured at study entry correlated with caregivers’ anticipatory (i.e., state) anxiety during treatments, their symptoms of psychological distress (i.e., total score on the composite measure), and avoidance at the 3-month follow-up or any of the covariates.
Next, Model 1 of Hayes’s (2013) regression utility for SPSS (Process) was used to determine whether trait anxiety and self-distancing interacted to affect either anticipatory anxiety (short term outcome), or the composite measure of psychological distress, and avoidance (longer-term outcomes). In these analyses all predictor variables were centered.
Prior studies with pediatric cancer caregivers (e.g., Harper et al., 2013; Harper, Peterson, et al., 2014) have shown that anticipatory anxiety mediates the relationship between trait anxiety and the measures of longer-term psychological distress used in the present study (specifically, the BSI-18 and the IES-R [including Avoidance] measured separately). To determine whether self-distancing moderates this relationship, we used Model 8 of Hayes’s (2013) regression utility for SPSS (Process), which tests for moderated mediation. Again this was done with and without the covariates.
Because all variables in the regression equations had been converted to z-scores, the correlation coefficients presented in Table 1 and the regression coefficients reported in the text or Table 2 represent standardized estimates of effect size. Specifically, the standardized regression coefficients (β) are the amount of change in the dependent variable for each change of one standard deviation in the variable of interest, while holding all other predictor variables in the equation constant. All estimates of regression effect sizes (i.e., standardized regression weights) in the equations are accompanied by 95% confidence intervals. Each regression coefficient was tested for significance using a t test with the alpha level set at .05.
Zero-Order Correlations Among Primary Variables
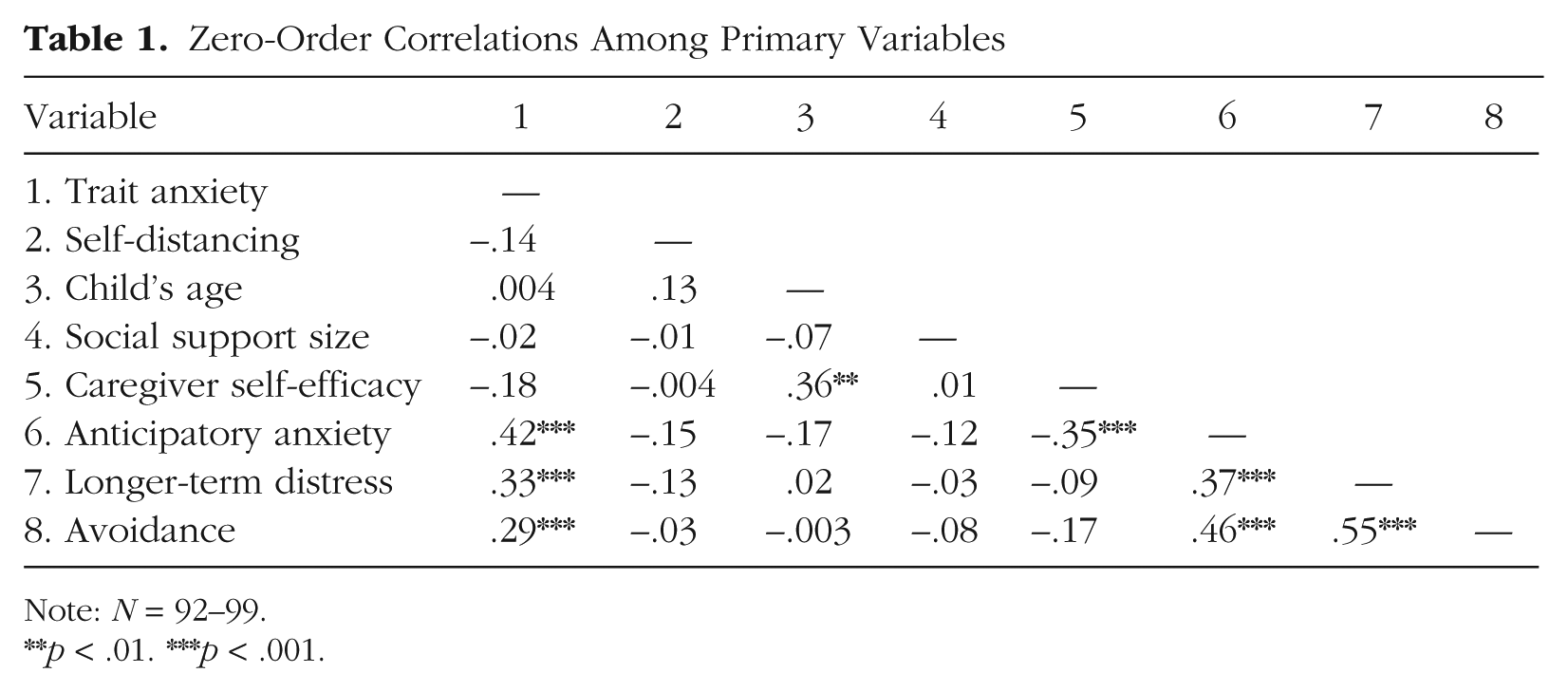
Note: N = 92–99.
p < .01. ***p < .001.
Summary of Regression Analyses for Anticipatory Anxiety, 3-Month Longer-Term Distress, and 3-Month Avoidance
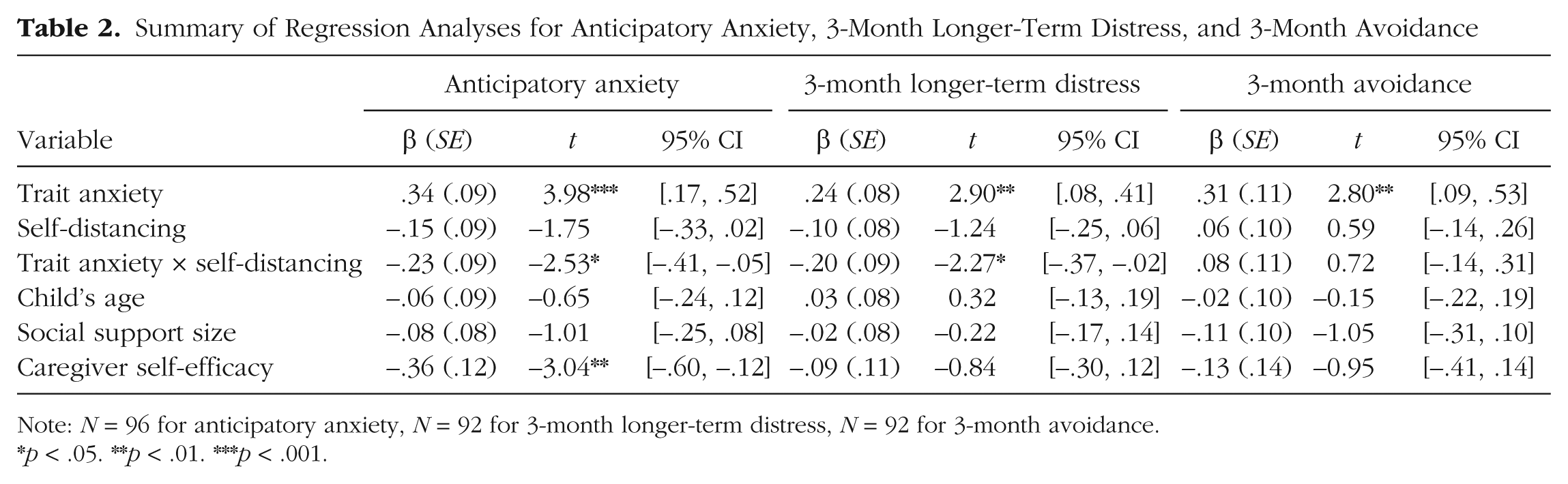
Note: N = 96 for anticipatory anxiety, N = 92 for 3-month longer-term distress, N = 92 for 3-month avoidance.
p < .05. **p < .01. ***p < .001.
Correlates of caregivers’ trait anxiety and self-distancing
Prior research with different samples from the larger study (e.g., Harper et al., 2013; Harper et al., 2015; Harper, Peterson, et al., 2014) has shown that trait anxiety significantly affects anticipatory (i.e., state) anxiety at treatment procedures and psychological distress during the follow-up. As Table 1 shows, this was also the case with this particular sample for both anticipatory anxiety and the composite measure of psychological distress assessed 3 months after the last treatment. Table 1 also shows that spontaneous self-distancing was not significantly correlated with trait anxiety, any of the covariates, state anxiety, or the composite measure of longer-term psychological distress. It was also uncorrelated with avoidance.
Moderation of caregivers’ anticipatory anxiety before treatment procedures
We predicted that spontaneous self-distancing would have a buffering effect on high trait anxious caregivers. That is, we expected high self-distancing would minimize the impact of trait anxiety on their anticipatory anxiety. This prediction was confirmed; we found a significant interaction between trait anxiety and spontaneous self-distancing, β = −.23, 95% CI [–.41, –.05], t(89) = 2.53, p = .01. The full regression equation is presented in Table 2. Figure 1a presents the regression slopes for low and high trait anxious caregivers. Among caregivers who were low in trait anxiety (i.e., 1 standard deviation below the sample trait anxiety mean), their tendency to spontaneously self-distance had no implications for how much anticipatory anxiety they experienced before their child’s treatments. However, among high trait anxious caregivers (i.e., 1 standard deviation above the sample trait anxiety mean), self-distancing served a protective function. That is, among high anxious caregivers trait anxiety significantly affected anticipatory anxiety only for caregivers who were low in self-distancing, β = −.37, 95% CI [–.65, –.10], t(89) = −2.67, p = .01. Among the high self-distancing caregivers, this relationship was not significant, β = .07, 95% CI [–.14, .28], t(90) = 0.67, p = .50.
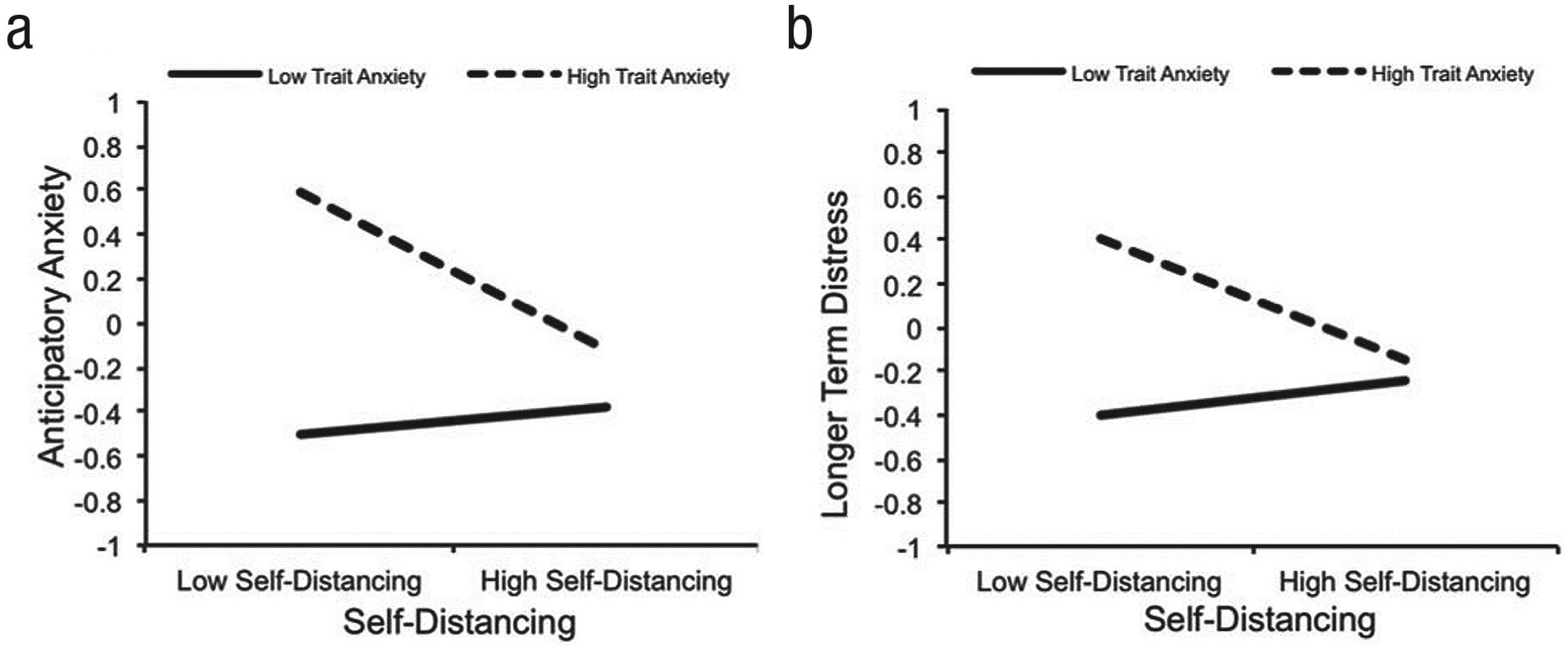
The effect of self-distancing and trait anxiety on anticipatory anxiety (a) and longer-term distress (b). The scores on the y-axis represent z-scores.
Moderation of caregivers’ longer-term symptoms of psychological distress
As expected, we observed a significant trait anxiety by spontaneous self-distancing interaction, β = −.20, 95% CI [–.37, –.02], t(85) = 2.27, p = .03. As Figure 1b demonstrates, the nature of this interaction was similar to the interaction reported for anticipatory anxiety. Specifically, if a caregiver scored low on trait anxiety, their tendency to spontaneously self-distance had no implications for their longer-term psychological distress. However, if a caregiver scored high on trait anxiety, spontaneous self-distancing served a protective function. That is, among high anxious caregivers trait anxiety significantly affected longer-term psychological distress only among caregivers who were low in self-distancing, β = −.28, 95% CI [–.53, –.03], t(85) = 2.19, p = .03. Among the high self-distancing caregivers, this relationship was not significant, β = .08, 95% CI [–.11, .27], t(85) = −.87, p = .39. 6
Moderation of caregivers’ avoidance
Self-distancing did not interact with trait anxiety to predict avoidance at the 3-month follow-up, β = .08, 95% CI [–.14, .31], t(85) = 0.72, p = .47.
Moderation of relation between caregiver anticipatory anxiety and longer-term psychological distress
Our final set of analyses aimed to enhance our understanding of how self-distancing buffers high trait anxious caregivers against long-term distress. Toward this end, we first examined whether participants’ anticipatory anxiety mediated the relationship between trait anxiety and longer-term psychological distress—as noted earlier, this meditational pathway has been documented in prior research with another subset of the caregivers in the larger study (e.g., Harper, Peterson, et al., 2014). There was also significant mediation in the present subsample with the composite measure of psychological distress at the 3-month follow-up as the outcome, indirect effects, β = .10, 95% CI [.03, .19] (Hayes, 2013, Model 4, simple mediation).
Next, we examined whether self-distancing affects this pathway. That is, we conducted an analysis of moderated mediation (Hayes, 2013, Model 8 for SPSS) of the indirect path from trait anxiety to longer-term psychological distress. We expected that the indirect path with state anxiety as the mediator would only be significant among the low self-distancing caregivers.
The overall moderated mediation model was significant, β = −.04, 95% CI [–.13, –.001]. Inspection of the indirect effects of state anxiety on psychological distress among caregivers low and high in self-distancing indicated that whereas there was a significant indirect effect among low self-distancing caregivers, β = .10, 95% CI [.01, .25]; there was no significant indirect effect among high self-distancing caregivers, β = .02, 95% CI [–.03, .11]. This analysis indicates that higher levels of self-distancing may serve a buffering function by disrupting the relationship between caregivers’ state anxiety in response to the treatments and their psychological distress 3 months following their child’s final cancer treatment.
Discussion
These findings demonstrate that among high trait anxious pediatric cancer caregivers, high levels of spontaneous self-distancing served to virtually eliminate the impact of trait anxiety on (a) anticipatory anxiety during the time of children’s painful cancer treatments and (b) longer term psychological distress. These effects were found when controlling for other established buffers of caregiver trait anxiety, highlighting the specificity and robustness of the effects of self-distancing. Finally, consistent with prior work (e.g., Ayduk & Kross, 2009, 2010; Kross et al., 2012), self-distancing did not promote avoidance.
These findings have three important basic science implications. First, they add to our understanding of the well-documented individual differences in how pediatric cancer caregivers cope with the psychosocial effects of their child’s cancer. As the literature review presented in the introduction indicates, there is widespread agreement on the important role trait anxiety plays in the way in which pediatric cancer caregivers react to the treatments their children receive and other aspects of the disease (e.g., Hoekstra-Weebers et al., 1999; Link & Fortier, 2015). Yet there is relatively little research on the cognitive processes that mitigate the impact of trait anxiety on these caregivers. The present research begins to fill this knowledge gap by identifying spontaneous self-distancing as a moderator that buffers high trait anxious caregivers against short- and longer-term distress related to coping with their child’s painful cancer treatments.
These findings also have important implications for theory and research on self-distancing. First, and perhaps most important, they show that laboratory research on self-distancing is ecologically valid (Shadish, Cook, & Campbell, 2002) and can be conceptually replicated in the real world. Second, they provide additional evidence suggesting that self-distancing is specifically useful for helping “high-risk,” highly vulnerable individuals cope with ongoing emotional threats. Indeed, the data represented in Figures 1a and 1b indicate that on both measures of distress the high trait anxious/high self-distancing caregivers were almost indistinguishable from the low trait anxious caregivers. In this vein it is noteworthy that we did not observe any comparable beneficial effects of self-distancing for people who scored low on trait anxiety. This finding is consistent with a number of recent laboratory studies on self-distancing that have likewise found that emotional vulnerability factors moderate the benefits of this process in the same direction observed here (Kross & Ayduk, 2009; Kross et al., 2012). More broadly, they suggest that a certain level of emotional distress may be needed for self-distancing to exert its beneficial effects; if not enough distress is experienced, there may be little room for self-distancing to operate.
Finally, the fact that self-distancing led to reductions in long-term distress without increasing avoidance conceptually replicates prior work (Ayduk & Kross, 2010; Kross & Ayduk, 2009; Kross et al., 2012) and argues against the idea that self-distancing is a de facto form of avoidance. This is not to say that we expect self-distancing to invariably be beneficial. Instead, whether this process is adaptive or not likely depends critically on the context in which people engage in this process. That is, are people self-distancing to approach or avoid their feelings? In this vein, it is important to emphasize that all participants were specifically asked to confront their emotions in this study—that is, “think about the causes and reasons underlying the thoughts and feelings [you] experienced during [your] child’s last cancer treatment experience.” We then asked participants to report on the degree to which they self-distanced as they engaged in this meaning-making process.
A number of caveats are in order before we turn to suggestions for future research. First, the real-world context in which this study was conducted—caregivers coping with the cancer-related treatment procedures their children receive—provided a unique opportunity to expand our understanding of how spontaneous self-distancing operates outside the laboratory, as vulnerable individuals grapple with intense emotional experiences. Although there are clear advantages associated with this approach, there are also disadvantages. For example, as is the case in any naturalistic study of psychological processes, our ability to include the kinds of control conditions and experimental manipulations that would permit strong inferences about causality was limited in this study. Thus, although the results regarding the links between self-distancing and our outcomes are consistent with our a priori hypotheses and a large body of prior research, in the absence of random assignment to experimental conditions we are unable to state it was spontaneous self-distancing, independent of any unmeasured other variables, that was responsible for the buffering effects among the high trait anxious caregivers.
In a similar vein, a caveat is in order when considering the mediation analyses we reported, which suggested that the interaction between trait anxiety and spontaneous self-distancing predicted longer-term distress because of their impact on caregivers’ anticipatory anxiety at the time of the children’s treatments. Although this meditational analysis was theory-predicted and utilized temporally distinct longitudinal data points to test the predicted pathway of interest—both assets for drawing inferences about likely causal sequences from nonexperimental data—we were not able to manipulate either of the major predictor variables (trait anxiety and spontaneous self-distancing) or the mediating variable (anticipatory anxiety). Thus, causality cannot be determined with the present data.
Finally, it is important to acknowledge that we did not include multiple types of measures of our constructs of interest. Thus, although the self-report tools we used to assess our core independent and dependent variables have all been validated and used extensively in the past, future research should consider measuring these constructs with other types of measures, such as physiological (Ebner-Priemer & Kubiak, 2007) and linguistic measures (Dirkse, Hadjistavropoulos, Hesser, & Barak, 2015) of anxiety, neural measures of self-distancing (Park et al., 2014), or informant measures of a person’s distress or psychosocial adjustment (e.g., McDade-Montez, Watson, O’Hara, & Denburg, 2008).
Although these finding raise multiple questions for future research, three stand out to us as most pressing. First, future research is needed to test the causal relationships that are suggested, but cannot be tested or proven with the present data. Although trait anxiety cannot be meaningfully manipulated among pediatric cancer caregivers (or other vulnerable groups) for ethical reasons, it would be possible to conduct small randomized field experiments that enhance caregivers’ propensity to self-distance and compare their responses to an untreated comparison group. Such experiments are justifiable on the basis of the present findings and would speak directly to the causal impact of self-distancing on caregivers’ short and longer-term distress.
Second, what are the pathways through which self-distancing buffers high anxious pediatric cancer caregivers or other vulnerable individuals? It is possible that self-distancing leads to adaptive shifts in the way caregivers mentally present their child’s cancer treatments. For example, rather than focusing on the concrete, aversive features of these events (i.e., the invasive nature of the procedures, the child’s displays of distress—crying, for example), self-distancing might lead caregivers to focus more broadly on the potential good that may come from the treatment (i.e., they will help my child live). It is also possible, however, that self-distancing instigates physiological changes that work to combat their anxiety. For example, prior research indicates that self-distancing buffers individuals against the autonomic consequences of ruminating over negative experiences (i.e., chronically elevated cardiovascular reactivity and shortened cardiovascular recovery; e.g., Ayduk & Kross, 2008; Brosschot, Gerin, & Thayer, 2006; Wisco et al., 2015). Thus, it is possible that there is simply less aversive physiological reactivity among high self-distancing, high trait anxious caregivers. Future research is needed to examine the role that these different pathways play in either independently or jointly accounting for the current results.
A third important question is whether there is a “tipping point” that captures when self-distancing ceases to be useful and becomes harmful. The current study was motivated by research suggesting that encouraging people to “take a step back” in the heat of the moment can be useful for allowing them to confront and approach negative experiences constructively, in ways that facilitating adaptive coping and self-reflection. However, the distribution of responses to the self-distancing questions in the current study indicates that even caregivers classified as high self-distancing (i.e., those who scored 1 SD above the group mean) engaged in only moderate levels of distancing (just above the midpoint on the 7-point scale of tendency to self-distance). It is possible that caregivers could distance themselves too much from their child’s treatment experience, which could diminish their care and concern for the child. The absence of such feelings make treatments much more difficult for children (see Cline et al., 2006). Future research is needed to address this question and is important for refining our understanding of self-distancing and the factors that promote effective pediatric cancer caregiving.
Footnotes
Authors’ Note
Portions of this research were presented in a poster at the 12th annual meeting of the International Psycho-Oncology Society, Brisbane, Australia.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This work is part of a larger investigation of caregivers’ influence on child coping with cancer treatment and was supported by the National Cancer Institute at the National Institutes of Health (NCI#1R01CA138981; principal investigator: Louis A. Penner) and the Herrick Foundation (principal investigator: Louis A. Penner).