
Abstract
Although menstrual cycle-related changes in psychological and physical symptoms have been the focus of study for decades, important gaps remain in our understanding of these changes. In the present study we test for individual differences and covariations in cyclical changes across diverse symptom domains, including physical symptoms, affective disturbances, and attributional style. Using prospective daily reports across two full menstrual cycles from n = 163 young adult women (M = 19.54 years), the present study applies a combination of within-person analyses (cosine function regressions) and structural equation modeling to examine individual differences, factor structure, and symptom-specific associations. Results suggest that (a) individual differences in cyclical change are consistently significant and relatively more important than average levels of change, (b) cyclical change across diverse symptom types are best modeled as separate but correlated factors, and (c) future research should also consider attributional style, along with cyclical changes in affective and physical symptoms.
Decades of research have examined the prevalence, diversity, and correlates of menstrual-cycle-related symptoms (McCance, Luff, & Widdowson, 1937; Moos, 1968), consistently showing that menstrual cycle changes in physical, psychological, and vegetative symptoms are common (Halbreich, Borenstein, Pearlstein, & Kahn, 2003; Logue & Moos, 2005; Takeda, Tasaka, Sakata, & Murata, 2006), robustly correlated with each other (Kiesner, 2009; Kiesner & Pastore, 2010), and clinically significant in up to 13% to 19% of women (Halbreich et al., 2003). The personal and societal burden of these symptoms is high, with 4.5 million disability adjusted life years lost per year in the United States (Halbreich et al., 2003). Moreover, women who experience severe levels of these symptoms are more likely to also experience other mood disorders, including postpartum depression (Bloch, Rotenberg, Koren, & Klein, 2005; Buttner et al., 2013), perimenopausal depression (Freeman, Sammel, Rinaudo, & Sheng, 2004), and major depressive disorder (Graze, Nee, & Endicott, 1990; Halbreich & Endicott, 1985; Hartlage, Arduino, & Gehlert, 2001).
Although decades of research have examined menstrual-cycle-related changes, we still lack a clear understanding of individual differences in within-person symptom change. This is because past research on menstrual cycle symptoms has typically focused on characterizing the average or typical experience of women (Laessle, Tuschl, Schweiger, & Pirke, 1990; Ramcharan, Love, Fick, & Goldfien, 1992), comparing clinically diagnosed and symptom-free controls (Schmidt, Nieman, Danaceau, Adams, & Rubinow, 1998; Soares, Cohen, Otto, & Harlow, 2001), or establishing epidemiological estimates of symptoms or disorders (Halbreich et al., 2003; Takeda et al., 2006). Thus, we lack insights regarding heterogeneity across women in the direction, magnitude, and symptom specificity of menstrual cycle symptoms.
This knowledge gap is important because failing to model within-person effects will likely result in underestimated effect sizes and wrongfully accepting a false null hypothesis. For example, studies testing for average effects across women often find no evidence for cyclical changes in affective and behavioral symptoms associated with the menstrual cycle (e.g., Laessle et al., 1990; Ramcharan et al., 1992), a result that could be an artifact of grouping all women together to characterize the average woman’s experience. Similarly, research comparing premenstrual syndrome or premenstrual dysphoric disorder (PMDD) diagnoses and controls fails to consider the heterogeneity of individual and symptom-specific response to the menstrual cycle.
Recent research highlights the benefits of examining individual differences in within-person menstrual cycle change. For example, although premenstrual mood deterioration is sometimes assumed to be typical (see Romans, Clarkson, Einstein, Petrovic, & Stewart, 2012), research has shown that a substantial minority of women experience affective symptoms midcycle or show no premenstrual change (Kiesner, 2011; Kiesner & Martin, 2013) and that significant individual differences are present in the association between daily hormonal changes and borderline personality symptoms (Eisenlohr-Moul, DeWall, Girdler, & Segerstrom, 2015). These findings are consistent with past research demonstrating individual differences in response to pharmacological manipulations of reproductive steroids (Schmidt et al., 1998).
A second gap in our understanding of menstrual-cycle-related symptoms regards the covariation of cyclical change across diverse symptoms. At a basic level, we are lacking both an adequate description of which symptoms covary across the menstrual cycle and insight as to whether these associations are important for understanding individual pathology or well-being. For example, although physical symptoms of the menstrual cycle are common (Arora, Seth, & Dayal, 2010; Bernstein et al., 2014; Martin & Lipton, 2008) and correlated with psychological fluctuations (Kiesner, 2009; Kiesner & Pastore, 2010), the specificity and relevance of physical symptoms for psychological adjustment are not well understood.
It previously has been argued that examining the associations among the heterogeneous and tissue-specific symptoms of the menstrual cycle (e.g., skin, gastrointestinal [GI], central nervous system [CNS]) may provide a better understanding of the causes and consequences of those symptoms (Kiesner, 2009). This issue is related to understanding the tissue-specific mechanisms (steroid regulated changes in protein expression) and possibly overlapping pathways to symptom expression (e.g., inflammatory processes common to multiple symptoms). For example, there are multiple pathways that could potentially link physical and psychological symptoms, including social embarrassment for acne (Stoll et al., 2001), molecular signaling of cytokines associated with changes in inflammation (Dantzer, O’Connor, Freund, Johnson, & Kelley, 2008; Puder et al., 2006; Wander, Brindle, & O’Connor, 2008), and acute distress caused by physical pain (Kiesner, 2009), to name a few.
Although some studies have examined factor structures of premenstrual symptoms (e.g., Freeman, DeRubeis, & Rickels, 1996; Mira et al., 1995), these studies have not specifically modeled within-person change across time. Moreover, the few studies that have examined within-person covariations (across time) among various symptoms associated with the menstrual cycle (Eisenlohr-Moul et al., 2015; Kiesner & Pastore, 2010) have not specifically modeled the covariation of cyclical change in symptoms. Thus, two symptoms could have covaried across time even though neither was synchronized with the menstrual cycle. Finally, although Kiesner and Martin (2013) demonstrated a significant association between cyclical change in headaches and cyclical change in affective symptoms, their analytic approach was based on a categorization into trajectory groups, a method that becomes unmanageable when considering more than two variables.
A third limitation of past research on menstrual-cycle-related symptoms is the lack of attention to mechanistic psychological variables such as attributional style. Although research has clearly demonstrated that affective, physical, and vegetative changes are commonly associated with the menstrual cycle (Freeman, 2003; Woods, Most, & Dery, 1982), the literature is primarily descriptive and fails to incorporate the underlying processes that may explain these symptoms. Of particular interest is the large body of psychological research that roots affective difficulties within cognitive interpretations of situational events. We have minimal understanding of whether and how attributional style is associated with the menstrual cycle, despite strong awareness of the link among attributional style and various affective (Cole et al., 2008), physical health (Grewen, Girdler, West, Bragdon, Costello, & Light, 2000; Hemenover & Dienstbier, 1998), and behavioral (Rowe, Maughan, & Eley, 2006) symptoms. The only extant study on this topic suggested that women with PMDD show premenstrual increases in self-focused attention (Craner, Sigmon, & Young, 2016), supporting potential cyclical variations in attributional style.
A link between menstrual-cycle-related affective symptoms and attributional style could be hypothesized for at least three reasons. First, menstrual cycle fluctuations in steroids may result in CNS changes that directly affect both affective symptoms and attributional style. Second, one symptom may be directly influenced by steroid changes (e.g., neurosteroid regulation of GABAA receptor complex; Brot, Akwa, Purdy, Koob, & Britton, 1997; Freeman, Frye, Rickels, Martin, & Smith, 2002), which may then result in changes in the other. Third, cyclical changes in other menstrual cycle symptoms, such as feelings of loss of control (Freeman et al., 1996; Steiner et al., 2011), emotional and impulsive eating (Klump et al., 2014; Racine et al., 2013), and changes in school or work performance (Borenstein, Chiou, Dean, Wong, & Wade, 2005; Borenstein, Dean, Leifke, Korner, & Yonkers, 2007), may be interpreted by the individual as stable personal attributes, thus shifting the individual’s attributional style.
The present study responds to these core gaps in research in three ways. First, to develop our understanding of within-person change, we focus specifically on modeling individual differences in within-person cyclical change across multiple menstrual cycles and across multiple symptoms. This approach provides tests of whether significant individual differences exist in cyclical change of menstrual-cycle-related symptoms and whether diverse symptoms show similar levels of individual variation. Second, modeling within-person cyclical change across multiple symptoms allows analyses to test for covariation in cyclical change across symptoms. Doing so eliminates ambiguity in whether symptom covariation is specific to the menstrual cycle or is part of a more general covariation independent of the menstrual cycle and provides insights as to possible causal mechanisms linking these diverse symptoms. Finally, we test whether attributional style changes across the menstrual cycle, whether this change varies across individuals, and whether it covaries with cyclical change in other symptoms. This provides insights regarding one potential contributing factor of an individual’s attributional style (the menstrual cycle) and regarding the broader context of psychological changes associated with the menstrual cycle.
Taken together, findings are expected to enrich our understanding of the heterogeneity in how women experience the menstrual cycle and to provide insights to help generate hypotheses for why cyclical change across diverse symptoms are associated with each other.
Method
Participants
Participants were 163 female university students with a mean age of M = 19.54 years (SD = 1.22; range = 18–28 years, with 95% 19–21 years; 97% Italian, 2% Italian and other, 1% other). Recruitment and measurement procedures closely followed those from a previous study (Kiesner, 2011).
All first-year female psychology students were asked to participate, and efforts were made to include women both with and without menstrual difficulties (see the later discussion). Individuals could not participate if they were using hormonal contraceptives or hormone therapy. Individuals who had been diagnosed with a psychological or medical condition for which they had been, or were being treated, were welcome to participate. However, participants with a seasonal illness (cold/flu) were asked to wait until it had passed before starting the study to avoid the conflation of illness symptoms with menstrual cycle symptoms. Participation was anonymous, voluntary, and did not result in compensation. The Ethics Committee of Psychological Research of the University of Padova approved this study, and all participants signed an informed consent.
Recruitment was conducted at the end of lectures in first-year psychology classes, after all male students were asked to leave the lecture hall. A brief explanation of the study was given, without providing specific information regarding study hypotheses. A central point that was emphasized during the explanation was the importance of including women who have very different experiences during the menstrual cycle, and that it would be equally important for women with and without menstrual difficulties to participate. Other emphasized points included (a) the personal nature of the questions and (b) the degree of participation required (daily questionnaires for two menstrual cycles). These points were emphasized to avoid surprise on the part of participants that could contribute to attrition. The overall presentation, including questions and responses, lasted approximately 15 minutes.
Of the 618 individuals who were asked to participate, 184 (30%) agreed to participate and 434 (70%) did not. Those who declined participation were given the option to indicate anonymously why they chose to not participate, using a single-question multiple-choice format response (asked to choose only one response). The distribution of responses was as follows: 31% did not have a regular menstrual cycle, 45% were using oral contraceptives or some other hormonal-based treatment, 6% had no computer access, 11% were not interested, and 7% cited some other reason. Of the 184 individuals who agreed to participate, 163 (86%) participated for the full study, providing data for two cycles. The data from these 163 participants are analyzed in the present study. Information on socioeconomic status was not collected.
Research assistants met each participant individually to provide an explanation and demonstration of the online data collection procedure and to review all questions and provide explanations when needed.
The average length of the two menstrual cycles was M = 29.78 days for Cycle 1 and M = 30.32 days for Cycle 2 (average length of two consecutive cycles M = 60.09 days). The average number of questionnaires for each participant was M = 57.26. Thus, on average, participants missed only 2.8 of the daily questionnaires across the two menstrual cycles, and a total of 9,334 questionnaires were included in the following analyses.
Measures
Online questionnaire and procedure
With the use of an individual password, participants had access to an online questionnaire assessing a variety of physical and psychological symptoms. This questionnaire is an adaptation of the scale used by Kiesner and Pastore (2010). All questions referred to the past 24 hours. Responses were given on a visual analogue scale with the anchors not at all to very much. Questions were presented individually, and participants could click anywhere along the line/slider extending between the two anchors. Following the click, the next question was presented.
Participants were asked to begin completing questionnaires on the first or second day of menstruation and to indicate on which day they were starting. The time and date of completion was automatically recorded and saved with each questionnaire. Participants were asked to complete one questionnaire each day. However, if they were not able to do so, or accidentally missed a day, the online questionnaire also allowed participants to complete one questionnaire for the prior day and one questionnaire for the actual day. To control for this, the first question on each questionnaire was whether it was in relation to “yesterday” or “today.” Of the total N = 9,334 questionnaires included in analyses, 79% (n = 7,338) were completed on the actual day and 21% were completed for “yesterday.”
Menstrual-cycle-related symptoms
Four types of symptoms were assessed: affective symptoms, attributional style, physical symptoms, and headaches. Although headaches were originally considered to be a physical symptom, initial analyses showed very low correlations between that item and all other physical symptoms; therefore, it was treated as a separate construct from the other physical symptoms. Notably, this finding is consistent with the recent decision to exclude headaches from the PMDD symptom list of the Diagnostic and Statistical Manual of Mental Disorders, based on a lack of evidence for synchronicity with other cyclical symptoms (American Psychiatric Association [APA], 2013). Specific items used are presented in Table 1. Past research using the same questionnaire, format, and computerized daily reporting provides evidence that this method and these questions are valid and sensitive to menstrual-cycle-related changes (Kiesner, 2011; Kiesner & Martin, 2013; Kiesner & Pastore, 2010).
Specific Items Used to Measure Symptoms Change

Note: Each question was preceded with “In the last 24 hours. . . .”
Reverse coded.
Although most of the measured symptoms have been used in past research (Kiesner & Pastore, 2010) and are included in diagnostic criteria for PMDD (APA, 2013), the questions regarding attributional style have not been studied on a daily basis in relation to the menstrual cycle. As presented in Table 1, two questions were used to measure attributional style, one question regarding self-blame (when things went badly) and the other regarding self-merit (when things went well). For the present analyses the self-merit item was reverse coded so that the final latent construct would reflect a negative attributional style. Because these questions have not been used in previous research, nor has this method of daily reports been used to examine day-to-day fluctuations in attributional style, evidence for validity of this specific strategy is limited.
Time
Because the focus of the present study was on changes in symptoms across time, the time and date of completion for each questionnaire was recoded to represent the proportion of each cycle that had passed since the first day of that cycle (day within cycle/total number of days in that cycle). Therefore, all participants, regardless of how many days their cycle lasted, were put on the same metric, ranging from 0 to 1 for each cycle (a 1 was then added to all days in the second cycle). Therefore, the time variable ranged from 0 to 2, with 0 corresponding to the first day of the first cycle, 1 corresponding to the last day of the first cycle, and 2 corresponding to the last day of the second cycle.
Data analysis
All analyses involve cosine regressions, or the saved amplitude coefficients from those analyses. Because cosine regressions are not common, we provide a detailed explanation of this technique to aid interpretation. In the present study, the goal of cosine regressions is to estimate the amplitude and pattern of change for nonlinear time-series data. To illustrate, Figure 1 provides the least squares cosine regression function for three participants on three separate symptoms (depression, self-blame, and headaches). In this figure, a W-shaped trajectory is characteristic of a premenstrual increase in that symptom, whereas an M-shaped trajectory is characteristic of a midcycle increase in that symptom. Thus, Participant 1 demonstrates a midcycle peak in self-blame, and little to no change in headaches or depression; Participant 2 demonstrates a midcycle peak in both self-blame and headaches, and little change in depression; and Participant 3 demonstrates a perimenstrual increase in all three symptoms, but with differing magnitudes.

Examples of estimated cosine functions for three variables for three participants, including the numerical value of the amplitude coefficient for Participant 1 (self-blame) and Participant 3 (depressed).
The cosine waves presented in Figure 1 are based on the estimated amplitude coefficients (and intercepts) from the individual-level analyses. To illustrate how these coefficients are interpreted, the specific values for two of the cosine waves are presented within the graph in Figure 1: the cosine amplitude for self-blame (Participant 1) and for depression (Participant 3). Numerically, the amplitude of the cosine wave is simply the difference between the average level across both cycles and the first peak/trough. An amplitude with a negative value corresponds to an M-shaped wave (across two cycles), and an amplitude with a positive value corresponds to a W-shaped wave (across two cycles). Note that because the numerical value of the amplitude is from the least squares regression of the cosine wave, and not the minimum/maximum value of the raw data, the peaks and troughs are smoothed and should not be interpreted as the extremes that were experienced by each participant.
Analyses were conducted in two main steps. First, multilevel analyses were conducted testing for both fixed effects (average effects of a predictor in the sample) and random effects (individual differences in the effects of a predictor). Specifically, for each of the 11 symptoms a series of multilevel analyses was conducted testing for the fixed effect of the cosine amplitude (i.e., the average cosine function across participants) and the random effects of both the slope (i.e., cosine amplitude) and the intercept (mean level across both cycles), varying across participants. In these models, the cosine function was modeled by regressing the dependent variable (i.e., symptom) on the cosine function of the time variable: Cosine(2π⋅Time). The primary result of interest is the random effect of the cosine amplitude for each variable. Specifically, the test of random effects determines whether there is significant between-person variation in the cosine amplitude, or whether the average group level amplitude provides an adequate description of change across time for all participants. Significant differences across participants are required to justify further analyses of the associations among the cosine amplitudes across symptoms.
Although our main interest lies in the random slopes (cosine amplitude), multilevel analyses were conducted with three incremental models, allowing us to calculate effect sizes for (a) individual mean-level differences (random intercepts), (b) fixed effects of the cosine function (average slope across participants), and (c) individual differences in the cosine amplitude (random slopes). The effect size for random intercepts is the intraclass correlation (ICC) and is calculated as the variance component for the random intercepts divided by the total variance from the same model (random intercepts only); the ICC is interpreted as the proportion of the total variance attributable to between-person differences in mean level. The effect size for the fixed effect of the cosine amplitude is calculated as the change in residual from the first model (random intercepts only) to the second model (random intercepts and fixed effect of the cosine function) divided by the residual from the first model, and it quantifies the proportion of within-person variance accounted for by the average effect of the cosine function (Raudenbush & Bryk, 2002). Finally, the effect size for the random slopes is calculated as the change in residual from the first model (random intercepts only) to the third model (random slopes and random intercepts) divided by the residual from the first model, and it quantifies the proportion of within-person variance accounted for by individual differences in the cosine function (Raudenbush & Bryk, 2002).
Next, the cosine amplitude coefficients were saved for each variable and for each participant to be used in a series of four structural equation models, treating the cosine amplitudes as measured variables. These four structural equation models allowed us to test whether cyclical change is best modeled as a single latent construct or as separate symptom types and to examine the associations among the different symptom types, at both a construct and symptom-specific level.
These four models were nested, thus allowing us to compare each successive model against the preceding model. The first model tested a one-factor measurement model in which the cosine amplitude coefficients for all measured variables were loaded onto a single latent construct. This model was then compared with a second model that included four uncorrelated latent constructs, for headaches, physical symptoms, psychological symptoms, and attributional style. This second model was then compared with the third model that further included the correlations among the latent constructs. Finally, the last model included the correlated residuals among the measured cosine amplitude coefficients, thus allowing us to test for symptom-specific associations, after controlling for associations among the latent constructs.
Results
Multilevel analyses
The first model included only random intercepts, testing for mean-level differences across individuals. Significant effects were observed for all variables (i.e., the 95% CI for the relevant variance component excluded zero), with the following ICCs (in order of increasing magnitude): cramps (ICC = .17), breast (ICC = .26), GI (ICC = .26), depressed (ICC = .27), anxiety (ICC = .29), headaches (ICC = .29), pain (ICC = .29), mood swings (ICC = .33), self-blame (ICC = .36), skin (ICC = .43), self-merit (ICC = .55). It is worth noting that these are proportions of variance explained by between-person differences, with the remaining variance existing within individuals. Thus, higher ICCs indicate more stable trait-like variables (e.g., self-merit), whereas lower ICCs indicate variables with high levels of within person variability (cramps).
In the second model the fixed effect of the cosine function was added, and was found to be significant for all variables (all ps ≤ .001). Specifically, at the group level there was a significant positive cosine amplitude for all symptoms, representing a perimenstrual increase in symptoms (e.g., a W-shaped change across two cycles). This is consistent with, although not demonstrative of, the prevailing perspective that experiencing perimenstrual worsening in mood, behavior, and physical well-being is normative. The effect sizes (percentage of within-person variance explained by the average effects of the cosine function) are presented in Figure 2. These results demonstrate that, although the fixed effects were significant for all variables, the effect sizes differ dramatically (ranging from 0.1% to 18%). It should be noted, however, that for variables demonstrating both positive and negative cosine amplitudes (e.g., both M- and W-shaped trajectories), the average effect approaches zero, but does not indicate null effects at the individual level.
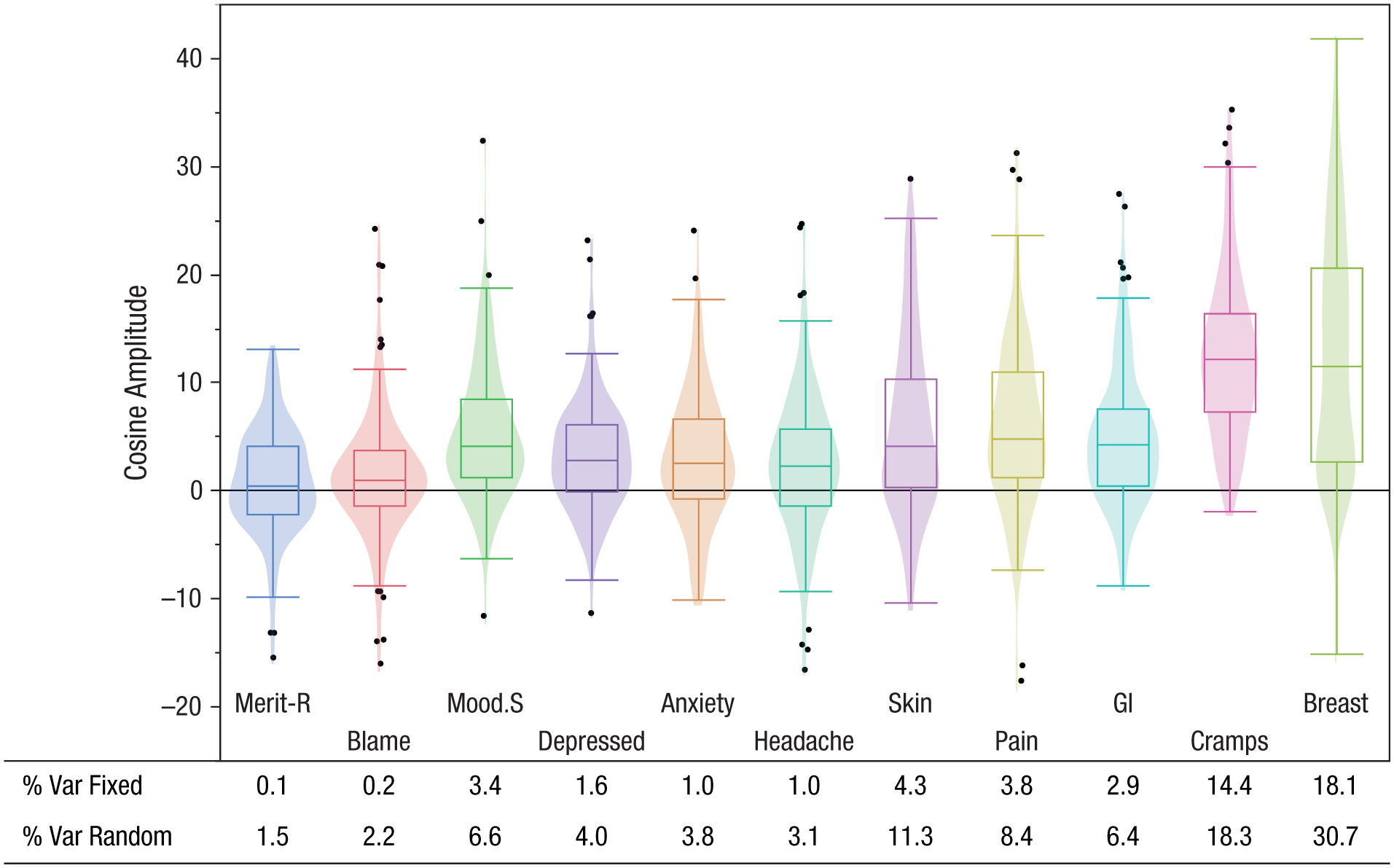
Box plots, contour plots, and effect sizes of cosine amplitude coefficients for all symptoms. Self-merit was reverse coded.
In the third model, the random effects of the cosine amplitude coefficients were added and found to be significant for all variables (i.e., the 95% CI for the relevant variance component excluded zero), indicating that the average cosine function is not sufficient for describing individual change, and confirming the presence of individual differences in the strength and direction of symptom cyclicity across individuals. These significant random effects are consistent with past research showing that women vary greatly in their sensitivity to ovarian steroid hormones (Schmidt et al., 1998). The effect sizes (the percentage of within-person variance explained by individual differences in the cosine function) are presented in Figure 2. Results again show dramatic differences in effect sizes (ranging from 1.5% to 30.7%). It is worth noting that the effect sizes for the random effects tend to be around twice the size of those for the fixed effects.
Figure 2 provides a graphic summary of the median level and variability of the cosine amplitude coefficients for all 11 symptoms, taken from the final full model. This figure illustrates the significant variability across individuals and also across symptoms.
Following the mixed-model analyses, individual cosine regressions were conducted at the individual level and the amplitude coefficients for each symptom for each participant were saved to be used as variables in the structural equation models. Note that the cosine functions presented in Figure 1 were taken from these individual-level analyses. It should also be noted that the coefficients predicted by these separate regressions correlated at near identity (≈ .99) with those produced by the multilevel analyses (i.e., best linear unbiased predictors) for all symptoms.
Structural equation models
Because much of the information regarding the associations among the cosine amplitude coefficients is presented in Figure 3, the full correlation matrix is not presented. However, it should be noted that almost all correlations were significant and positive (with self-merit reverse coded), and those that were not significant could be grouped in relation to three variables. First, as could be expected by the model presented in Figure 3, cyclical changes in headaches were not correlated with cyclical changes in most of the physical symptoms, although they were correlated with back/joint pain and GI symptoms (r = .19 and r = .17, respectively, p < .05, n = 163). Second, cyclical changes in breast swelling or pain were not correlated with cyclical changes in any of the psychological symptoms with the exception of mood swings (r = .22, p <.01, n = 163). Finally, although cyclical change in self-blame was associated with cyclical change in headaches and three of the five physical symptoms, self-merit was correlated only with headaches and none of the physical symptoms (both were significantly correlated with all psychological symptoms).
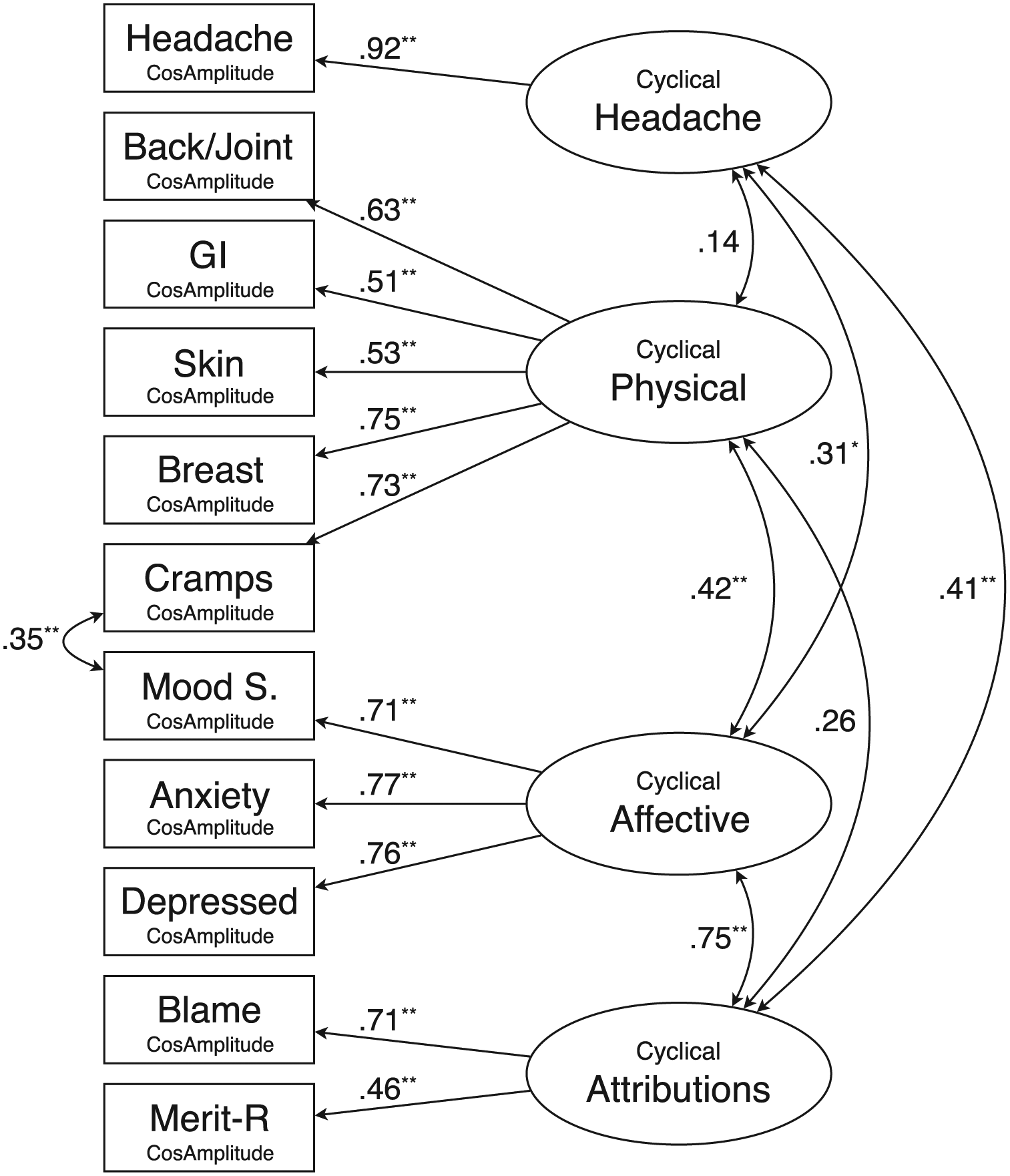
Final structural equation model testing measurement characteristics and correlations among latent constructs, including a single correlated residual between cramps and mood swings. Self-merit was reverse coded.
To determine covariation across different symptoms, structural equation models were conducted using R (R Core Team, 2015) and the lavaan package (Rosseel, 2012). It is worth repeating that the observed variables are the saved cosine amplitudes for each variable for each participant. The first model was a one-factor measurement model, with all measures loading onto the same single factor. This model did not fit the data well (χ2 = 153.34, df = 44, p < .001; comparative fit index [CFI] = .56; nonnormed fit index [NNFI] = .45; root mean square error of approximation [RMSEA] = .12) and was rejected. The second model was a four-factor measurement model, including the four factors presented in Figure 3, but with the correlations among the latent factors fixed to zero. This model did not converge. The third model was similar to the second, but included the correlations among the four latent factors. Although this model converged, it did not fit the data well (χ2 = 55.87, df = 39, p = .04; CFI = .93; NNFI = .90; RMSEA = .05). Finally, for the last model, modification indices regarding the correlations among residuals were used to make changes. Only one correlation (between cramps and mood swings) was suggested. The final model including this correlation fit the data well (see Figure 3; χ2 = 46.35, df = 38, p = .17; CFI = .97; NNFI = .95; RMSEA = .04) and also resulted in a significant improvement in fit as compared with the third model (Δχ2 = 9.52, df = 1, p < 002).
Path coefficients from the final model are presented in Figure 3. It should be emphasized that these constructs specifically represent the menstrual-cycle-linked cyclical variation in these symptoms. Four specific findings are worth noting. First, the physical symptoms construct was not correlated with either the headache or attributional style constructs, but demonstrated a significant association with the affective symptom construct (sharing about 18% of their variance). Second, the affective symptoms construct was also significantly associated with the headache and attributional style constructs (sharing about 10% of its variance with headaches and 56% with attributional style). Third, the latent construct for attributional style was as strongly correlated with the affective symptoms construct as it was with the specific symptoms used to measure that construct (see factor loadings). Finally, the attributional style construct was significantly associated with the headache construct (sharing about 17% it their variance).
Finally, to ensure that findings reflect normal cyclical variation and cannot be explained by extremely short or long menstrual cycles, the structural equation models described earlier were rerun excluding those participants who had at least one cycle that was less than 25 days or more than 35 days. In all, 54 participants were excluded, resulting in a reduced sample of n = 109. Results from these analyses were similar to those from the full sample and led to the same conclusions. For example, the final model (see Figure 3) fit the data well also with this reduced sample (χ2 = 42.68, df = 38, p = .28; CFI = .97; NNFI = .96; RMSEA = .03), and all path coefficients remained in the same range and none changed significance (those that were significant remained significant and those that were not remained so). Therefore, these results are robust to a fairly large exclusion of participants based on cycle length.
Discussion
Our results suggest that significant individual differences exist in the magnitude and direction of cyclical change for a variety of different physical and emotional symptoms, and that the associations between cyclical change in symptoms depends on symptom specificity.
As a starting point for this discussion, we should comment on the distributions of the cosine amplitude coefficients across the 11 symptoms (Figure 2). There is a general group tendency to demonstrate a positive amplitude coefficient and thus a perimenstrual increase in the symptom. However, all symptoms demonstrated significant variability across individuals as well as different distributional characteristics. For example, lower abdominal cramps, which are almost exclusively associated with menstruation (Kiesner & Pastore, 2010), show almost exclusively positive coefficients (i.e., perimenstrual increase). In itself, this confirms what should be expected by a symptom that occurs only in association with menstruation, but it can also be contrasted with other symptoms, such as headaches, affective symptoms, and self-blame, that demonstrate both positive and negative coefficients (premenstrual and midcycle increases). This is an important distinction because it provides a dissociation between a symptom that follows only one type of cyclical change, and most other symptoms that demonstrate both types of cyclical change.
Results also showed that the different symptom types should be considered as distinct, but correlated. This has implications for research on menstrual-cycle-related changes as well as for a diagnosis of PMDD (APA, 2013). For example, although both affective and physical symptoms are included as diagnostic criteria for PMDD, cyclical changes in these symptom types were only moderately correlated (r = .42; sharing about 18% of their variance). An important question that must be addressed is this: If these diverse symptoms have distinct etiological pathways, should they be considered to be a part of the same pathology? Although many studies do analyze distinct subgroups of symptoms (depressive, physical, anger/irritable; see Pearlstein, Yonkers, Fayyad, & Gillespie, 2005), the end diagnostic decision is based on symptom presence, without a clear understanding of shared etiology or causal associations among the different symptom types. Thus, more work is needed to understand which symptoms share common etiology and prognostic value and which symptoms are causally associated with others.
Moreover, although all four constructs examined showed a general pattern of positive associations, there were clear differences in these associations, supporting the idea that there are different processes and underlying causal pathways leading to them. For example, although both headaches and the other physical symptoms are associated with discomfort and pain, and both types of symptoms clearly show menstrual-cycle-related change, there is essentially no association between cyclicity of these symptom types, thus suggesting distinct causal pathways. Consistent with this hypothesis, different pathways for diverse physical symptoms have been suggested regarding, for example, headaches and menstrual cramps. Research has shown that menstrual migraines can be triggered by estradiol withdrawal if it has been maintained at a high level for several days, but not following progesterone withdrawal (Somerville, 1971, 1972a, 1972b, 1975) and that menstrual migraines involve response properties and inflammation of the trigeminal ganglia (Martin, Lee, & Behbehani, 2007; Puri et al., 2006; Waeber & Moskowitz, 2005). This can be contrasted with findings suggesting that the physiological trigger of cramps involve inflammation and prostanoid signaling in the endometrium (Jabbour & Sales, 2004; Marjoribanks, Ayeleke, Farquhar, & Proctor, 2015) leading to hypercontractility of the uterus (Dawood, 2006; Dawood & Khan-Dawood, 2007). The fact that these different types of symptoms are associated with different risk for psychological symptoms is noteworthy.
The loading coefficients for the different latent constructs provide similar insights. For example, the generally higher level of internal consistency for the affective symptoms than for physical symptoms suggests that the underlying causal pathway may be more similar for the affective symptoms, as compared with the physical symptoms. This would not be surprising given the vastly different tissues involved in the physical symptoms (intestinal, breast, uterine, dermal) and the likely limited neurological tissues involved in the affective symptoms. However, an important question that must be addressed is why cyclical changes in such diverse physical symptoms are correlated at all. The presence of these correlations suggests the involvement of an early step in steroid signaling (steroid receptor morphology/activity), rather than later steps related to specific genes that are transcribed and their resulting proteins.
Classically, attributional style has been viewed as an individual characteristic that is stable across time and that functions as a risk factor for depression (Beck, 1967). Consistent with this idea, in the present study attributional style was found to be the most stable/trait like of all the variables measured. However, attributional style was also found to vary cyclically for some women and also to covary with menstrual-cycle-related affective symptoms and headaches. This finding is consistent with recent work demonstrating that, compared with controls, women with PMDD show greater cyclicity of self-focused attention, another cognitive risk factor for psychopathology (Craner et al., 2016).
The causal mechanism for this association, however, is unknown. As suggested in the introduction, there are multiple mechanisms that could account for this association. For example, it is possible that affective symptoms associated with changes in serotonergic regulation across the menstrual cycle (Freeman, 2004; Rubinow, Schmidt, & Roca, 1998) lead to similar changes in attributional style. On the other hand, cyclical changes in attributional style may lead to similar changes in affective symptoms, as suggested by past research linking depressive attributional style with developmental changes in depression (Cole et al., 2008; Metalsky, Abramson, Seligman, Semmel, & Peterson, 1982; Nolen-Hoeksema, Girgus, & Seligman, 1992). This association could also reflect a general steroid sensitivity across neurological structures involved in both affective symptoms and cognitive processes related to attributional styles. Finally, changes in attributional style may result from behavioral dysregulation or compromised success in school or work that may vary across the menstrual cycle (Borenstein et al., 2005; Borenstein et al., 2007; Freeman et al., 1996; Klump et al., 2014; Racine et al., 2013; Steiner et al., 2011).
The only two symptoms that demonstrated an association outside of the latent constructs were lower abdominal cramps and mood swings. This finding is similar to past research showing that lower abdominal cramps were more strongly associated with mood swings than with depressive symptoms or cognitive symptoms of the menstrual cycle (van Iersel, Kiesner, Pastore, & Scholte, 2016). It was proposed that this may be explained by the acute and transitory nature of both symptoms. That is, whereas headaches and depressed affect are likely to be relatively stable across hours or days, cramps and mood swings are acute and transitory and may demonstrate a tight temporal linkage across short time periods throughout the day. It is important that if such a temporal link is found between cramps and mood swings this would provide a possible explanatory model for one of the psychological symptoms commonly associated with the menstrual cycle.
In the present study cyclicity of symptom change was modeled as a bipolar construct with Ms and Ws at different ends of the spectrum. Although this provides an elegant and simple approach to studying cyclical change relative to the menstrual cycle, there is a risk that it confounds hormone sensitivity as reflected in the magnitude of change, with the direction of that change. That is, it could be hypothesized that there are two mechanisms required to explain the full effect: one explaining the direction of change and the other explaining the magnitude of change. Past research on individual differences of steroid effects has also overlooked this possibility. For example, past research has shown significant individual differences in the relation between serum testosterone and depression (Vermeersch, T’Sjoen, Kaufman, Vincke, & Van Houtte, 2010), with the (cytosine-adenine-guanine) trinucleotide repeat length in the androgen receptor gene being the sole mechanism presumed to explain both the direction and magnitude of the association. Although it may be reasonable to hypothesize a single common cause, it is not reasonable to assume it, and future research should attempt to test this hypothesis specifically.
Finally, an important and novel perspective offered by these results is that each of the symptoms studied can be conceptualized as depending on average effects of the menstrual cycle (fixed cosine effect), individual differences in response the menstrual cycle (random cosine effect), and how those individual differences are related to individual differences in cyclical changes in all other variables. For example, affective symptoms were found to be partially attributable to an average effect of the menstrual cycle and partially attributable to individual response to the menstrual cycle, and finally those individual patterns of cyclical change in affective symptoms were correlated with cyclical change in other variables. Thus, when considering the broader question of whether the menstrual cycle influences mood, the current results demonstrate that it differs across women and that understanding the individual’s full experience of the menstrual cycle must be considered. This perspective is best illustrated by the differences in effect sizes across levels of analysis, which suggest that the average level of change (i.e., the fixed effect of the cycle) is the least important and that an individual’s unique degree and direction of change (i.e., random effect of the cycle) considered in the context of other symptoms will provide the most information.
There are several limitations of this study worth considering. First, sample bias in research on the menstrual cycle remains an unknown entity. For example, it could be hypothesized that women who experience higher levels of symptoms are more motivated to participate, thus biasing the sample toward higher levels of cyclical change in symptoms. On the other hand, many women who experience significant cyclical symptom changes are often prescribed hormonal contraceptives (Pearlstein & Steiner, 2008), even in the absence of a clinical diagnosis of PMDD, and would therefore be excluded from participation. Second, no measures of steroids or other biological processes (e.g., inflammation) were included. Although the data used in this study were well suited for modeling cyclical change across a variety symptoms, including biological measures would allow for richer and more informative analyses regarding underlying pathways.
The present study sets the stage for future research that should address a very basic question that has received surprisingly little attention: Why and how are such a broad range of symptoms linked together in a cyclical fluctuation across the menstrual cycle? Although research has listed many symptoms and grouped them according to empirically derived factor structures, hypotheses and data regarding potential causal pathways have been sorely lacking. As a result, much research has attempted to explain the causes of this very heterogeneous set of symptoms, each affecting a distinct tissue, and many with an unexplained relevance to psychological symptoms (acne, cramps, GI), without proposing or testing causal mechanisms linking them. As suggested earlier, the associations among these distinct variables suggests the involvement of an early step in steroid signaling (steroid receptor morphology/activity), rather than later steps related to specific genes and proteins. Moreover, symptom expression will likely also involve environmental pathways stemming from social interactions, school or work performance, or mechanistic psychological variables such as attributional style. Regardless of whether these pathways are biologically mediated, environmentally mediated, or both, future experimental and longitudinal studies must begin test specific causal pathways linking these diverse symptom types.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
Tory Eisenlohr-Moul’s work is supported by a training grant in reproductive mood disorders funded by the National Institute of Mental Health (T32MH093315).