
Abstract
This research assessed the association between the adherence to a Mediterranean lifestyle beyond the Mediterranean diet and the risk of depression in a prospective cohort of Spanish university graduates. Through a dynamic cohort study method, diet was assessed with a validated semiquantitative food-frequency questionnaire. The baseline assessment included a validated questionnaire on physical activity and average time spent with friends (socializing). Mediterranean lifestyle was defined as the joint exposure to Mediterranean diet, level of physical activity, and level of socializing. After a median follow-up of 8.5 years, 806 cases of depression among 11,800 participants were observed. Participants with the highest adherence to the Mediterranean lifestyle showed a 50% relative risk reduction in depression risk as compared to those participants with the lowest adherence (multivariable hazard ratio = 0.50; 95% confidence interval = [0.32, 0.81]). The Mediterranean lifestyle might reduce depression risk in the Seguimiento Universidad de Navarra cohort study beyond the known effects of the Mediterranean diet.
The term Mediterranean diet refers to dietary patterns found in olive-growing areas of the Mediterranean region. Although some heterogeneity in traditional patterns of food consumption exists in these countries, there are also common features, such as consumption of abundant plant foods (e.g., high intake of fruits, nuts, vegetables, bread, pulses, potatoes, seeds, cereals, and pasta), fresh and varied fruits as the main and usual dessert, olive oil as the main source of fat and commonly used for salads and cooking, frequent consumption of fish, moderate wine consumption with meals, low amounts of meat (mainly poultry instead of beef and pork), and low to moderate consumption of dairy products.
The beneficial role of the Mediterranean diet in several diseases such as cardiovascular disease (CVD) (Estruch et al., 2013), cancer (Schwingshackl & Hoffmann, 2014), Type 2 Diabetes (T2D) (Koloverou, Esposito, Giugliano, & Panagiotakos, 2014), or dementia (Singh et al., 2014) has been extensively evaluated and confirmed.
Furthermore, other nonnutritional aspects such as social, cultural, economic, and environmental features have been suggested to contribute to the beneficial effects attributed to the Mediterranean dietary pattern. Thus, cultural and nutritional aspects, jointly with regular physical activity, are fundamental parts of this comprehensive Mediterranean model of lifestyle (Donini, Serra-Majem, Bulló, Gil, & Salas-Salvadó, 2015).
Although the effect of the Mediterranean diet on depression has already been evaluated through several observational and experimental epidemiological studies (Rienks, Dobson, & Mishra, 2013; Sánchez-Villegas et al., 2013; Sánchez-Villegas et al., 2015; Skarupski, Tangney, Li, Evans, & Morris, 2013), to our knowledge there are no studies that have analyzed the Mediterranean lifestyle (beyond diet and including other features such as physical activity or social aspects) and its relationship with depression risk. Thus, the aim of our analysis was to longitudinally assess the association between the adherence to an overall Mediterranean lifestyle and the risk of depression in a cohort of a Spanish university graduates, the Seguimiento Universidad de Navarra (SUN) Project.
Materials and Methods
Study population
The SUN Project is a prospective, dynamic cohort study, initiated in December 1999 in Spain. The sample comprises Spanish university graduates. Its methods have been previously described elsewhere (Martínez-González, 2006; Seguí-Gómez, de la Fuente, Vázquez, de Irala, & Martínez-González, 2006). Information is gathered biennially by mailed or Web-based questionnaires referred to as Q2 for the 2-year follow-up, Q4 for the 4-year follow-up, and so on until the Q14, which was completed by participants after the 14-year follow-up. The overall retention in the cohort approaches 90%.
Up to June 2014, 22,045 participants had completed the baseline questionnaire of the SUN Project. Participants who were lost to follow-up, who had not completed at least one follow-up questionnaire, who were outside of predefined limits for baseline total energy intake (less than 800 Kcal/day or more than 4,000 Kcal/day in men, and less than 500 Kcal/day or more than 3,500 Kcal/day in women), and participants with missing values in the variables of interest were excluded from the analyses. We also excluded those participants who were users of antidepressant medication at baseline or had reported a present or previous history of clinical diagnosis of depression at baseline. Finally, 11,800 participants were included in the prospective analyses for the present study.
The study was approved by the Institutional Review Board of the University of Navarra. Written informed consent was not requested from the participants. Voluntary completion of the first questionnaire was considered to imply informed consent.
Exposure assessment
Mediterranean diet
Dietary intake was assessed at baseline with a 136-item, validated, semiquantitative food-frequency questionnaire (FFQ) (De la Fuente-Arrillaga, Vázquez Ruiz, Bes-Rastrollo, Sampson, & Martinez-González, 2010; Fernandez-Ballart et al., 2009). Nutrient intakes were calculated as frequency multiplied by nutrient composition of specified portion size for each food item using an ad hoc computer program specifically developed for this aim. A trained dietician updated the nutrient database using the latest available information included in food composition tables for Spain.
Mediterranean diet was defined a priori as follows: For each food or nutrient, we fitted a regression model in which total energy intake was the independent variable and each food or nutrient was the dependent variable. Residuals for each variable were standardized. These nutrients and foods were daily consumption of legumes, cereals (including bread and potatoes), fruit, vegetables, meat and meat products, milk and dairy products, fish, and trans fatty acids. Moreover, the ratio of monounsaturated to saturated fatty acids was also directly standardized as a z value. For scoring moderate alcohol consumption, a transformation centered at the level of consuming 30 g/day for men (30-absolute value [30-alcohol intake]) and 20 g/day for women (20-absolute value [20-alcohol intake]) was used to obtain the highest value for men consuming 30 g/day or women consuming 20 g/day and progressive lower values as the consumption was lower or higher than these values. The results of these transformations of alcohol intake were also standardized as z values. The final score was the sum of standardized residuals of items considered favorable minus the standardized residuals of items considered unfavorable. The total score for the Mediterranean diet weighted favorably the consumption of legumes, cereals, fruits, vegetables, fish, moderate consumption of alcohol, and the ratio of monounsaturated to saturated fats and weighted unfavorably the consumption of meats and dairy products and trans fatty acids. The final score was converted to relative percentage of adherence using the range of values of the sample. A participant with the maximum value of adherence in the sample obtained 100% of adherence. A participant with a minimum value of adherence obtained 0% in the relative percentage (Beunza et al., 2010; Sánchez-Villegas, Martínez, De Irala, & Martínez-González, 2002). Finally, the relative percentage was categorized into tertiles.
Physical activity
The baseline questionnaire (Q0) included a leisure-time physical activity questionnaire collecting information about 17 activities. Average time spent in physical activity variables was measured on a 10-point frequency scale (none to more than 11 hours per week), combined with a 3-point scale reflecting number of months per year (<3, 3–6, >6) that the activity was undertaken. To quantify the volume of activity during leisure time, an activity metabolic equivalent (MET) index was computed. We assigned a multiple of resting metabolic rate (MET score) to each activity based on existing literature (Ainsworth et al., 2011). Time spent in each of the activities was multiplied by the MET score specific to each activity and then summed over all activities to obtain a value of overall weekly MET hours. Finally, the continuous variable was categorized into tertiles. Leisure-time physical activity estimated using the questionnaire was previously validated in a Spanish sample using a triaxial accelerometer as the gold standard. Leisure-time physical activity (estimated as MET hours per week) derived from the questionnaire moderately correlated with kilocalories per day assessed through the accelerometer (Spearman’s r = 0.507, 95% confidence interval [CI] = [0.232, 0.707], p < .001) (Martínez-González, López-Fontana, Varo, Sánchez-Villegas, & Martinez, 2005).
Social activity/socializing
Average time spent with friends in the previous year was measured at baseline with a question with 11 possible answers, ranging from none to more than 9 hours per week in a typical week day or in a typical weekend day. We multiplied the first number of hours by 5 and the second by 2 and then divided the total by 7 to obtain mean hours per day spent hanging out with friends and then categorized them in tertiles.
Total activity level
Additionally, physical and socializing activities were analyzed together as total activity. Level of total activity was categorized into four categories (low, medium, high, and very high) according to participants’ tertile distribution for the two activity variables. For example, those participants in the lowest tertile for both activities or in the first tertile for one and in the middle tertile for the other were included in the low category. Thus, the groups were created as follows—low: T1 and T1, T1 and T2, or T2 and T1; medium: T1 and T3, T3 and T1, or T2 and T2; high: T2 and T3 or T3 and T2; and very high: T3 and T3.
Mediterranean lifestyle
A participant was considered with high adherence to the Mediterranean lifestyle if he or she reported a high adherence to the Mediterranean diet, a high level of physical activity, and a high level of socializing. Only participants in the highest tertile of the three exposure variables were included in this category. Contrarily, if the participant belonged to the lowest tertile of adherence to the Mediterranean diet and the lowest tertiles of physical activity and socializing, he or she was included in the low Mediterranean lifestyle category. The rest of the possible combinations were considered as medium adherence to this lifestyle.
Outcome assessment
Incident cases of depression were defined as participants who were free of any previous history of depression at baseline; were not using any antidepressant treatment at baseline; positively responded to the question, “Have you ever been diagnosed with depression by a medical doctor?”; or reported the habitual use of antidepressant drugs in any of the seven biennial follow-up questionnaires (Q2 to Q14). Although antidepressants could have been prescribed for conditions other than depression, this situation is extremely unusual in Spain. So we considered both the use of antidepressants and physician diagnosis as valid criteria to operationally define incident cases of depression.
The self-reported diagnosis of depression performed by a physician was validated in a subsample of our cohort using the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (4th edition) by an expert psychiatrist as the gold standard. The percentages of confirmed depression and nondepression were 74.2% (95% CI = [63.3, 85.1]) and 81.1% (95% CI = [69.1, 92.9]), respectively (Sánchez-Villegas et al., 2008).
Other covariates
Energy intake was also calculated through the information collected from the semiquantitative FFQ administered at baseline. Information regarding sociodemographic (e.g., sex, age, marital status, employment status) and lifestyle-related variables (e.g., smoking status, supplement use, special diets) was obtained from the baseline questionnaire.
Body Mass Index (BMI) was calculated as weight (in kilograms) divided by the square of height (in meters) using data collected at baseline.
The prevalence and history of CVD, cancer, dyslipidaemia, hypertension, T2D, and obesity was also collected.
Statistical methods
The distribution of several baseline characteristics of the participants according to the main variables of the analysis is presented as percentages (categorical variables) or means and standard deviations (numerical variables). For each participant we computed person–years of follow-up from the date of returning the baseline questionnaire to the date of depression diagnosis, the date of death, or the date of returning the last follow-up questionnaire, whichever came first. Cox proportional-hazards regression models were fitted to assess the relationship between each exposure variable (diet, physical activity, socializing, and total activity) and the incidence of depression during follow-up. Hazard ratios (HRs) and their 95% CIs were calculated considering the lowest tertiles as the reference categories. To control for potential confounding factors, the analyses were adjusted for sex, age (years, continuous), BMI (Kg/m2, continuous), smoking (nonsmoker, ex-smoker, current smoker, missing), special diet at baseline, total energy intake (Kcal/day, continuous), and the presence of several diseases at baseline (CVD, T2D, and hypertension). An indicator variable for missing responses (n = 131) was created for smoking. Other confounding factors, such as marital status, special diets, employment status, or presence of cancer or dyslipidaemia at baseline, were also explored but not included in the final models, as they showed no evidence of introducing any relevant confounding influence. Moreover, each exposure was also adjusted for the others in an additional analysis.
In further analyses, possible combinations between adherence to the Mediterranean diet (in tertiles) and level of total activity were created. The association of the possible combinations with the risk of depression was also ascertained through Cox regression models considering the same confounding factors as in the main analysis. Finally, the joint effect of the three different exposures (adherence to the Mediterranean lifestyle) was evaluated in multivariable analyses considering the lowest adherence as the reference category.
Moreover, Nelson-Aalen curves of the incidence of depression according to the joint effect of the adherence to Mediterranean diet and physical and socializing activities were calculated.
All p values were two-tailed, and p < .05 was considered significant. Statistical analysis was performed using STATA version 12.0 (StataCorp).
Results
Table 1 shows the distribution of several characteristics of the sample according to extreme tertiles of adherence to Mediterranean diet, physical activity, or socializing. Participants in the highest tertile of the Mediterranean diet were more likely to be older, married, and ex-smokers and showed higher prevalence of several chronic diseases, physical activity level, and total energy intake. Those participants with the highest level of physical activity were more likely to be males, nonmarried, and nonsmokers and to show a higher adherence to the Mediterranean diet and higher energy intake. On the other hand, participants in the third tertile of socializing (those who spent more than 1.6 hours/day with friends) were more likely to be younger, females, nonmarried, and current smokers and to have a lower prevalence of chronic diseases and BMI and a higher level of physical activity.
Characteristics of Participants According to Extreme Tertiles of Adherence to the Mediterranean Diet and Physical and Social Activities

Note: METs = metabolic equivalents.
This includes use of at least one of the following vitamin supplements: A, B1, B2, B3, B6, folic acid, B12, C, D, or E.
After a median 8.5 years of follow-up, 806 cases of depression were reported. The association between tertiles of different features of the Mediterranean lifestyle and depression risk is shown in Table 2. The three exposure variables were inversely associated with depression risk with significant dose–response relationships. The multivariable HRs and 95% CIs for extreme tertiles were as follows: HR = 0.82, 95% CI = [0.69, 0.97] for Mediterranean diet; HR = 0.81, 95% CI = [0.69, 0.97] for physical activity; and HR = 0.77, 95% CI = [0.64, 0.93] for socializing. Further adjustment for each exposure slightly attenuated the reported associations. Level of total activity was also associated with a reduction in the relative risk of depression. The HRs and 95% CIs for high and very high levels of total activity as compared to low activity were 0.79 and [0.64, 0.96] and 0.72 and [0.55, 0.93], respectively.
Risk of Depression (HR, 95% CI) According to Adherence to the Mediterranean Diet and Physical and Socializing Activities
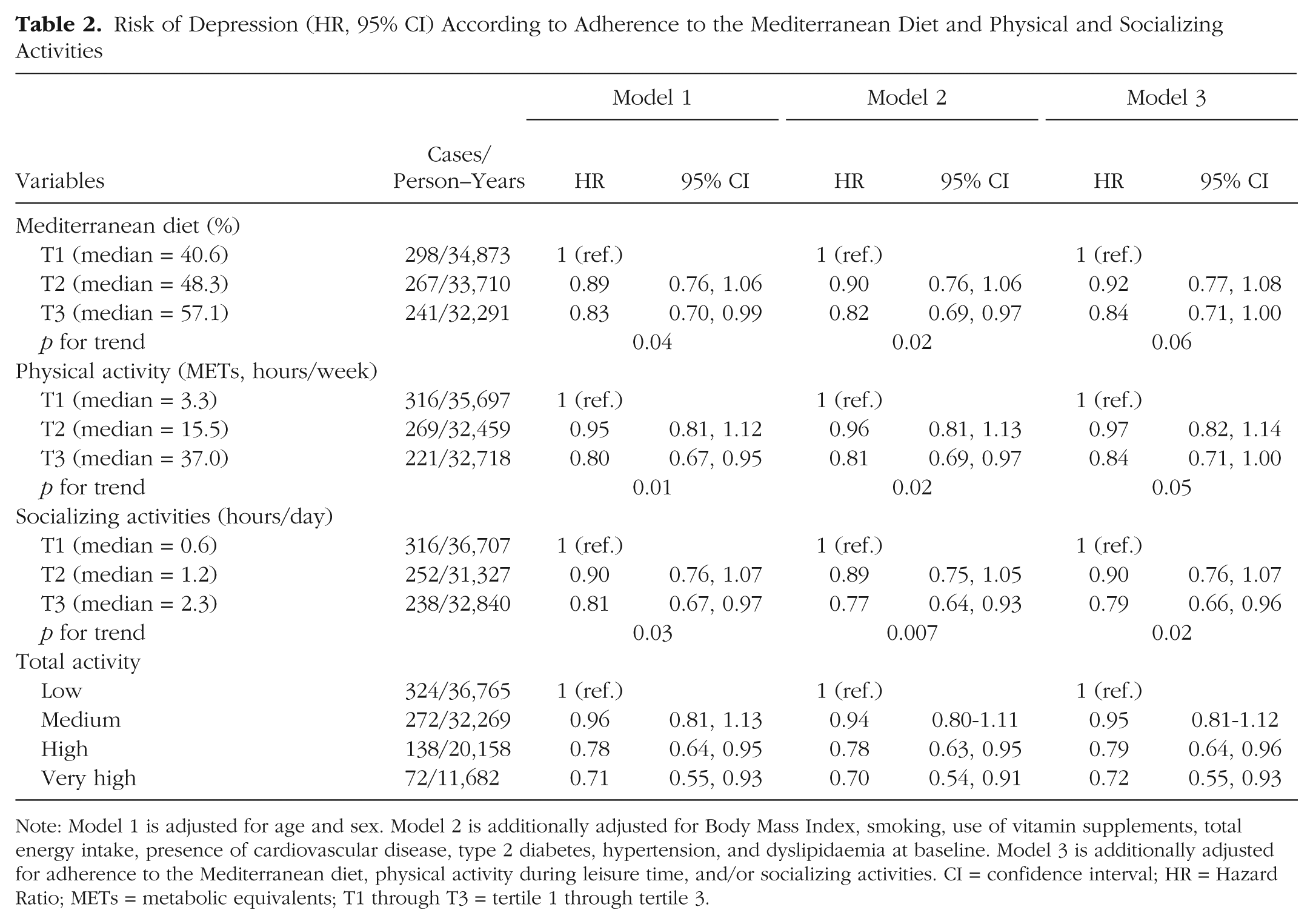
Note: Model 1 is adjusted for age and sex. Model 2 is additionally adjusted for Body Mass Index, smoking, use of vitamin supplements, total energy intake, presence of cardiovascular disease, type 2 diabetes, hypertension, and dyslipidaemia at baseline. Model 3 is additionally adjusted for adherence to the Mediterranean diet, physical activity during leisure time, and/or socializing activities. CI = confidence interval; HR = Hazard Ratio; METs = metabolic equivalents; T1 through T3 = tertile 1 through tertile 3.
When level of total activity was analyzed together with adherence to the Mediterranean diet, a reduction of around 40% in the relative risk of depression was observed for those participants in the highest level of activity (third tertiles of both physical activity and socializing) and intermediate–high level of adherence to the Mediterranean diet (second and third tertiles of adherence) (Table S1 in the Supplemental Material available online).
Finally, those participants with the highest adherence to the Mediterranean lifestyle (participants with the highest adherence to Mediterranean diet, the highest level of physical activity, and the highest level of socializing) showed a 50% reduction in the relative risk of depression as compared to those participants with the lowest adherence to this lifestyle (multivariable HR = 0.50, 95% CI = [0.32, 0.81]) (Table 3).
Risk of Depression (HR, 95% CI) According to the Joint Effect of Adherence to the Mediterranean Diet and Physical and Social Activities
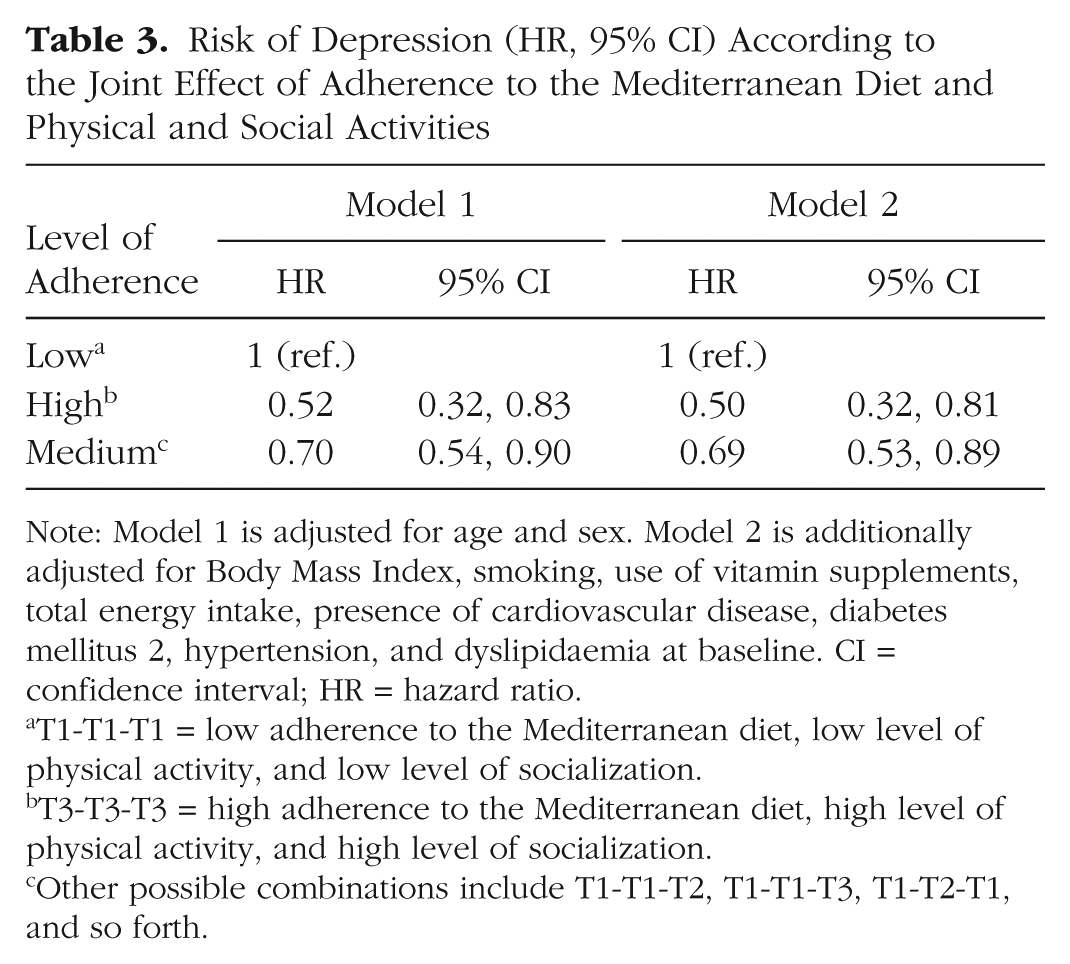
Note: Model 1 is adjusted for age and sex. Model 2 is additionally adjusted for Body Mass Index, smoking, use of vitamin supplements, total energy intake, presence of cardiovascular disease, diabetes mellitus 2, hypertension, and dyslipidaemia at baseline. CI = confidence interval; HR = hazard ratio.
T1-T1-T1 = low adherence to the Mediterranean diet, low level of physical activity, and low level of socialization.
T3-T3-T3 = high adherence to the Mediterranean diet, high level of physical activity, and high level of socialization.
Other possible combinations include T1-T1-T2, T1-T1-T3, T1-T2-T1, and so forth.
The Nelson-Aalen curves (Figure S1 in the Supplemental Material) showed differences in the incidence of depression according to the level of adherence to the Mediterranean lifestyle, with a higher incidence for those participants situated in the lowest category.
Discussion
In this analysis of the SUN Project, a high adherence to the Mediterranean diet, a high level of physical activity, and a high level of socializing were independently associated with a lower risk of developing depression. According to our results, level of activity (both physical activity and socializing) could be at least as important as diet to reduce the risk of depression. When the three features were considered together, the reduction in the relative risk was even higher, with a reduction of 50%.
The role of the Mediterranean diet in depression was first evaluated in 2009 within the SUN Project (Sánchez-Villegas et al., 2009). Recently, these results have been confirmed in an updated analysis including repeated measures of Mediterranean diet adherence (Sánchez-Villegas et al., 2015). Other longitudinal studies, both observational and experimental, have found a protective effect of this pattern on depression development (Rienks et al., 2013; Sánchez-Villegas et al., 2013; Skarupski et al., 2013). Some food items characteristic of this protective pattern, such as olive oil, nuts, fruits, legumes, or fish, could be responsible for the reported effect through their anti-inflammatory and antioxidant properties as well as their capacity to improve endothelial function and neuronal membranes composition.
On the other hand, engagement in physical activity has also been associated with a lower risk of depression in several epidemiological studies (McKercher et al., 2014; Pinto Pereira, Geoffroy, & Power, 2014; Roh et al., 2015). Several mechanisms may underlie the potentially protective effect of physical activity on depression, including its anti-inflammatory and neurochemical effects, the large amounts of encephalins and endorphins secreted during exercise (McMurray, Berry, & Katz, 1990), sustained cerebral blood flow (Rogers, Meyer, & Mortel, 1990), improved aerobic capacity and cerebral nutrient supply (Dustman et al., 1984), as well as growth factors, specifically the brain-derived neurotropic factor, which is a peptide that increases neuronal survival and plasticity (Erickson, Gildengers, & Butters, 2013). Other authors have suggested improvements in some psychosocial parameters such as body image, self-esteem, self-efficacy, or self-worth and a decrease in social isolation as a result of a greater recreational physical activity (Liu, Wu, & Ming, 2015). In this sense, social isolation could increase depression risk. In fact, several studies have found a protective effect of socializing or social relationships on depression (Chiao, Weng, & Botticello, 2011; Cruwys et al., 2013; Sánchez-Villegas et al., 2009, Teo, Choi, & Valenstein, 2013; Teo et al., 2015). In a recent study based on a cohort of 4,642 American adults ages 25 to 75 followed for 10 years, Teo et al. (2013) found that the quality of social relationships predicted future depression. According to these authors, social relationships might influence mental health outcomes through multiple mechanisms, including influence on health-related behaviors, engagement in social activities, transfer and exchange of social support, and access to material resources (Kawachi & Berkman, 2001). In agreement with our results, a recent analysis within that same cohort found that the frequency of in-person social contact with friends was inversely associated with depressive symptoms (Teo et al., 2015).
According to the Mediterranean Diet Foundation (2016), “the Mediterranean diet is a valuable cultural heritage that is much more than just nutritional, tasty and healthy pattern. It is a balanced lifestyle that includes recipes, cooking methods, celebrations, customs, local products and various human activities.” Beyond dietary features, the current Mediterranean pyramid includes adequate rest, conviviality, and physical activity as essential parts of its setup (Mediterranean Diet Foundation, 2016). Moreover, according to the United Nations Educational, Scientific and Cultural Organization (UNESCO), the traditional Mediterranean diet involves a set of skills, knowledge, rituals, symbols, and traditions, including the sharing and consumption of food. Eating together is the foundation of the cultural identity and continuity of communities throughout the Mediterranean basin. It is a moment of social exchange and communication, and an affirmation and renewal of family, group, or community identity (UNESCO, 2013). Thus, the Mediterranean lifestyle includes not only a food consumption pattern but also other features related to human activities, such as physical activity or engagement in social aspects like going out with friends. All factors in combination would be responsible for the health benefits associated with this lifestyle (Gerber & Hoffman, 2015). In this line of thought, age-adjusted rates of depression and suicide are known to be lower in Southern Europe (Spain, Italy, and Greece) than in Northern or Central European countries (Chishti et al., 2003). A suggested hypothesis that could explain the south-to-north gradient in depression rates is the difference observed in food patterns and habits between Mediterranean and non-Mediterranean countries. Consequently, the traditional Mediterranean lifestyle might have contributed to lowering the risk of depression.
To our knowledge, this is the first time that an overall Mediterranean lifestyle is analyzed in association with depression. Recently, the combined association of physical activity and fruit and vegetable consumption with depression was analyzed in a cohort study in Taiwan (Chi, Wang, & Tsai, 2016). In this study, the simultaneous presence of several good lifestyle habits increased the beneficial effect of reducing the risk of developing depressive symptoms (Chi et al., 2016). In the last decades, nutritional epidemiologists have increased their interest to study overall dietary patterns more than specific food items or nutrients, as the analysis of a single component does not take into account the interaction with other nutrients and their synergistic effects (Jacobs & Tapsell, 2013). Using this analogy, the cluster of several features (e.g., diet, physical activity, and socializing) could add extra protection against depression, as we have found in the present study (Houtjes et al., 2014). In our line of thought, a recent study by Knight, Bryan, and Murphy (2016) analyzing the feasibility of an intervention with the Mediterranean diet on preventing cognitive impairment in elders from Western countries suggests examining not only the dietary intervention but also its combination with other postulated factors such as physical activity, smoking, or social engagement.
Several strengths have to be highlighted in our study. The inclusion of a large number of participants, a high retention rate near 90%, the existence of previously published validation studies regarding the exposure and the outcome, and some other important covariables should be mentioned. Some limitations should also be acknowledged. Dietary intake, physical activity level, social activities, and clinical diagnosis of depression were self-reported. Dietary intake, physical activity level, and depression diagnosis were validated in subsamples of participants of the cohort (Fernández-Ballart et al., 2009; Martínez-González et al., 2005; Sánchez-Villegas et al., 2008). However, some degree of misclassification might exist for these assessments and for social activity. Nevertheless, this misclassification is more likely to be nondifferential and therefore would bias the results towards the null expecting rather than a higher magnitude of effects than those found in the present analysis.
Another caveat to take into account is the possible presence of reverse causation bias. Although participants with a prevalence of depression or who used antidepressants at baseline were excluded from the analysis, some participants with a subclinical (undiagnosed) depression could have responded to the questions regarding diet, physical activity, and socializing at the beginning of the study. Participants with subclinical depression may have changed their food habits and social relationships because of their mood disorder. In fact, it is known that social isolation is present among depressed patients (Jacobs & Tapsell, 2013). However, the prospective design of the SUN cohort study reduces the possibility of reverse causation bias on the reported associations. Moreover, the results for the association between adherence to the Mediterranean lifestyle and depression did not change after eliminating the cases of depression reported in the first follow-up questionnaire (n = 251) in a sensitivity analysis of our data (data not shown).
In conclusion, some already stated protective factors of depression such as adherence to the Mediterranean diet and the engagement in physical and social activities have also been described in the present study. However, we found an even higher inverse association between the cluster of all these protective factors in a labeled Mediterranean lifestyle and depression risk within the SUN cohort study based on a middle-aged population from a Mediterranean country. In fact, a 50% reduction in the relative risk of depression was found for those participants with a higher adherence to this lifestyle.
Supplemental Material
Sanchez_Villegas_Supplemental_Material – Supplemental material for The Association Between the Mediterranean Lifestyle and Depression
Supplemental material, Sanchez_Villegas_Supplemental_Material for The Association Between the Mediterranean Lifestyle and Depression by Almudena Sánchez-Villegas, Miguel Ruíz-Canela, Alfredo Gea, Francisca Lahortiga and Miguel A. Martínez-González in Clinical Psychological Science
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
The SUN Project has received funding from the Spanish Government-Instituto de Salud Carlos III and the European Regional Development Fund (FEDER) (RD 06/0045, CIBER-OBN, Grants PI10/02658, PI10/02293, PI13/00615, PI14/01668, PI14/01798, PI14/01764, and G03/140), the Navarra Regional Government (45/2011, 122/2014), and the University of Navarra.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.