
Abstract
Obesity is associated with steep discounting of the future and increased food reinforcement. Episodic future thinking (EFT), a type of prospective thinking, has been observed to reduce delay discounting (DD) and improve dietary decision making. In contrast, negative income shock (i.e., abrupt transitions to poverty) has been shown to increase discounting and may worsen dietary decision making. Scalability of EFT training and protective effects of EFT against simulated negative income shock on DD and demand for food were assessed. In two experiments, we showed online-administered EFT reliably reduced DD. Furthermore, EFT reduced DD and demand for fast foods even when challenged by negative income shock. Our findings suggest EFT is a scalable intervention that has implications for improving public health by reducing discounting of the future and demand for high energy dense food.
Keywords
Obesity involves a series of choices that contributes to, in part, positive energy balance in which energy intake exceeds energy expenditure. For example, when provided with the choice between a small immediate reward and a larger delayed reward, obese individuals reliably choose the smaller immediate reward (Amlung, Petker, Jackson, Balodis, & MacKillop, 2016; Bickel, George Wilson, et al., 2014; Graham Thomas, Seiden, Koffarnus, Bickel, & Wing, 2015; Rasmussen, Lawyer, & Reilly, 2010; Weller, Cook, Avsar, & Cox, 2008). This bias for the smaller immediate rewards can be described by delay discounting (DD). In addition, food reinforcement, a fundamental determinant of choice that shapes and strengthens food-seeking behaviors, is cross-sectionally related to obesity (Epstein, Jankowiak, Fletcher, et al., 2014; Temple & Epstein, 2012) and prospectively related to weight gain (Carr, Lin, Fletcher, & Epstein, 2014). The effects of reinforcing value on energy intake (Rollins, Dearing, & Epstein, 2010) and obesity (Epstein, Jankowiak, Fletcher, et al., 2014) are moderated by discounting of the future, such that those who find food more reinforcing, and discount the future more steeply, consume the most food (Rollins et al., 2010) and are the most obese (Epstein, Jankowiak, Fletcher, et al., 2014). This interaction is described as reinforcement pathology (Bickel et al., 2012; Carr, Daniel, Lin, & Epstein, 2011).
In addition, obesity is associated with economic poverty; those with low income are more likely to become obese (Braveman et al., 2005; Schoenborn, Adams, & Barnes, 2002). This disparity may be due to, in part, decision biases arising from exposure to scarce resources (Epstein, Jankowiak, Lin, et al., 2014; Lin, Carr, Fletcher, & Epstein, 2013). Research findings suggest a lack of resources along with the associated stress may shift attention toward short-term needs, even at the expense of longer-term goals (Bickel, Moody, Quisenberry, Ramey, & Sheffer, 2014; Lawrance, 1991). Identifying interventions that shift the temporal orientation from immediate to long term can improve allocation of resources and facilitate health behavior change.
Episodic future thinking (EFT), a type of prospective thinking (Atance & O’Neill, 2001), is believed to reduce impulsive decision making by increasing the value of delayed outcomes (Benoit, Gilbert, & Burgess, 2011) and encouraging individuals toward choices with long-term benefits (Boyer, 2008). EFT has been shown to reduce discounting rates in alcohol-dependent and nondependent adults (Snider, LaConte, & Bickel, 2016), obese and nonobese adults (Daniel & Epstein, 2013; Daniel, Stanton, & Epstein, 2013; Dassen, Jansen, Nederkoorn, & Houben, 2016), adolescents (Bromberg, Wiehler, & Peters, 2015), and children (Daniel, Said, Stanton, & Epstein, 2015). In addition, EFT reduces energy intake in laboratory (Daniel et al., 2013) and field settings (O’Neill, Daniel, & Epstein, 2016) and can improve weight loss achieved in a brief behavioral weight loss intervention (Sze, Daniel, Kilanowski, Collins, & Epstein, 2015).
To date, the implementation of EFT has been limited to in-person administration and development of episodic cues. An advancement would be to implement EFT remotely, thus improving its scalability. Because EFT cues are temporally sensitive (i.e., future oriented) and expire once the events have occurred, it is imperative to update EFT cues to maintain utility when using it long term. For example, if a person develops a narrative for a month in the future, the EFT cue needs to be updated before that month has elapsed (otherwise that cue would be considered a past cue, rather than a future one). The ability to implement EFT remotely would enable people to use EFT even if they were not in close proximity to a trained EFT interventionist. Moreover, other advantages would include flexibility (e.g., allowing people to use EFT training based on their everyday schedules) and the ability to reach a large number of people at relatively low cost.
The current article is designed to extend research on EFT in four ways. First, to improve scalability of EFT, a new approach to implement EFT was developed, delivered online, and its effectiveness was tested. Second, we assessed the effects of online-administered EFT to mitigate the countertherapeutic increases in DD observed with negative income shock (i.e., abrupt transitions to poverty; Bickel, Wilson, Chen, Koffarnus, & Franck, 2016; Haushofer, Schunk, & Fehr, 2013). Third, we examined for the first time the effects of EFT on the reinforcing efficacy of fast food. If EFT shifts attention away from immediate rewards, EFT may reduce food demand. Finally, because poverty is associated with higher valuation of food reinforcement, abrupt shifts in economic status due to income scarcity could make food more reinforcing. Therefore, it is important to examine the effects of EFT on food reinforcement after negative income shock (Bickel et al., 2016).
Experiment 1
In this first study, we assessed the efficacy of online EFT training by comparing it with episodic recent thinking (ERT), a strong control condition that controls for the development of episodic cues and nonspecific components of EFT (i.e., temporal perspective, episodic thinking, personalization). Moreover, ERT has not been shown to influence temporal discounting (Daniel, Sawyer, Dong, Bickel, & Epstein, 2016). Retrospection involving attending to past memories is not an ideal control as it shares similar memory based processes as EFT (Schacter & Addis, 2007; Schacter, Addis, & Buckner, 2007) and has been previously demonstrated to influence temporal discounting (Daniel et al., 2016).
Method
Participants
Participants were recruited through Amazon Mechanical Turk (AMT), a crowdsourcing Internet marketplace where small tasks are posted as human intelligence tasks (HITs) for human workers to complete. Only AMT users who had a 95% acceptance rate on previous HITs and who currently resided in the United States could access the survey. Because weight loss requires foregoing immediate food and sedentary activity rewards for the delayed reward of weight loss, and weight control is desired across all demographics (Serdula et al., 1999), only participants interested in weight loss were recruited. Participants were excluded from completing the survey if they did not indicate they were interested in personal weight loss and were not at least 18 years of age.
Participants were awarded a bonus if they followed instructions and carefully completed 100% of the survey questions. Of the 66 participants, 54 were awarded the bonus. A total of 66 participants were studied, and no differences between groups were observed in participant characteristics. Participants were 37.29 ± 13.80 (M ± SD) years of age, 68% (45 out of 66) female, 80% (53 out of 66) nonminority and non-Hispanic, 33.29 ± 9.49 BMI, with 14.91 ± 2.12 years of education, $55,454 ± $37,362 household income, 3.49 ± 0.71 average Consideration of Future Consequences score, 4.18 ± 0.70 average motivation score to lose 23.46 ± 14.99 pounds of weight, and −4.62 ± 1.78 log k baseline discounting rate. No differences were observed in participant baseline characteristics in the sample that excluded those that missed the attention check item (n = 54). Based on the federal minimum hourly wage (U.S. Department of Labor, 2016), participants were compensated $8.74 for their complete participation in this study.
Procedures
Before participation, participants were provided with an overview of the study. Subjects were informed they could participate in multiple study phases, the amount of time each phase would take, and the compensation for completing each phase. Implied consent was obtained when participants indicated they understood the description and continued on to the survey. In Session 1, participants completed demographic measures, questions related to their weight loss goal, time perspective, and a standard DD task. They were then randomly assigned to either the EFT condition (n = 33) or ERT control (n = 33). Session 2 consisted of EFT/ERT training followed by a DD task in which EFT/ERT cues were implemented. All study procedures were approved by the University at Buffalo Social and Behavioral Sciences Institutional Review Board.
Delay Discounting Task
The 27-item monetary-choice questionnaire was used to measure discount rate (Kirby, Petry, & Bickel, 1999). Participants were presented with a fixed set of choices between smaller, immediate rewards and larger, delayed rewards. An estimate of the participant’s discounting rate parameter, k, was made from the participant’s pattern of choices. DD rates were calculated using the technique used by Kirby and colleagues (1999). The k value typically has a skewed distribution, thus we used natural log-transformed k parameters for statistical analyses consistent with prior research (Baker, Johnson, & Bickel, 2003; Kirby & Marakovic, 1996).
Episodic future thinking (EFT) task
EFT participants generated episodic future events similar to those used in previous EFT study procedures (Daniel & Epstein, 2013; Daniel et al., 2013; Daniel et al., 2015). Participants in the EFT condition generated personalized future events that they were looking forward to and could vividly imagine for three different future periods. The periods were matched approximately with the delays in the DD task, which were grouped into three general future periods (1 month, 2–3 months, and 4–6 months). Participants were instructed to imagine, state, and describe in detail future events that were positive, specific, and vivid. To help participants think about autobiographical details of their events, participants rated the valence, salience, arousal, frequency, and vividness of each event on scales of 1 (very low) to 5 (very high). Participants were also prompted to describe specific details of their events, including who would be there, what they would be doing, where they would be going, and how they would be feeling. Participants were instructed to describe the events as though they were currently happening. Detailed and positive future event examples, along with vague and negative future event examples, were provided and labeled as “good” and “bad” examples to emphasize the importance of positivity, specificity, and vividness in the events. In addition, a checklist of task requirements (i.e., positive, vivid, specific) was given at the end of each event generation to use as a reference.
Episodic Recent Thinking (ERT) Task
Participants in the ERT control condition generated personalized recent past events that they enjoyed and could vividly remember for three different periods. The periods were approximately matched with the delays in the DD task in terms of recent past periods (1 day ago, 2–3 days ago, and 4–6 days ago). Participants were instructed to think about, state, and describe recent past events that were positive, specific, and vivid. All other procedures (e.g., event ratings and prompts) were identical to those described for the EFT group.
Episodic thinking during the delay-discounting task
Participants were instructed to read and think about their events during each decision in the DD task. Each choice was displayed on its own page along with the participant’s self-generated event that corresponded to the delay for that choice. For example, when making a choice between $31 now or $85 in 7 days, EFT participants was instructed to think about their future event that will occur in about 1 month and ERT participants was instructed to think about their recent past event that occurred 1 day ago before making their choice.
Manipulation check
To detect if participants were thinking about their events during the DD task, participants provided imagery ratings on a 5-point Likert-type scale (i.e., 1 = not at all, 5 = very much) on (a) how much they thought about their event and (b) how vividly they imagined their event after each monetary decision. A cue imagery score was calculated as the average of overall thoughts and vividness ratings.
To estimate whether participants were carefully reading the instructions and attending to each monetary choice, one nonsensical item (considered an “attention check”) was added in the middle of the DD task. Participants were informed in the instructions that a question that would not make sense would be found in the task to determine if they were paying attention. This question asked them to make a choice between nonsensical rewards for a nonsensical period, “Would you prefer $# today or %& in O days?” and participants were instructed to select a “refuse to answer” option when they identified the “attention check” item.
Other measures
Demographics
Race/ethnicity, income, and educational level were obtained using a standardized questionnaire adapted from MacArthur’s network for studies on socioeconomic status and health (Adler, Epel, Castellazzo, & Ickovics, 2000).
Motivation for weight loss
Participants were asked to provide their weight loss goal for the next 6 months then rated how motivated they were to lose their desired weight loss on a 5-point Likert-type scale (1 = not at all, 5 = extremely). Motivation was defined as “how hard you are willing to work and achieve your weight loss goal (e.g., changing eating and activity habits).”
Time perspective
Participants completed the Consideration of Future Consequences Scale in Session 1 to assesses the extent to which individuals consider the potential future outcomes of their current behavior and the extent to which they are influenced by the imagined outcomes (Strathman, Gleicher, Boninger, & Edwards, 1994). Time perspective is associated with risky behaviors and health behaviors (Daugherty & Brase, 2010).
Analytical plan
Separate one-way analysis of variance (ANOVA) for continuous variables and chi-square tests for categorical variables were conducted to determine group differences in participant characteristics. Subject characteristics that might serve as covariates were assessed by examining between group differences and whether potential covariates correlated with changes in discount rate (log k). Analyses were conducted using the full sample (N = 66), as well as the sample that excluded the 12 participants who did not correctly answer the attention check item (n = 54). Variables that predicted outcome (BMI, baseline discounting rates) were entered as covariates. In addition, comparisons were made for discounting changes in small, medium, and large reward magnitudes. Robust prior research indicates that discounting is greater for smaller rather than larger delayed rewards (Green, Myerson, & McFadden, 1997); therefore, examination across the different levels of reward magnitude provides an idea of the strength of the intervention. An overall average was calculated for comparison between groups. Effect sizes (partial eta-squared, η2) and 90th percentile η2 confidence intervals (Steiger, 2004) were calculated for changes in discounting between EFT and ERT conditions. Regression models with centered predictors were used to assess whether the amount of targeted weight loss and the motivation to lose weight moderated the effect of EFT on DD in separate models. Data analyses were completed using SYSTAT version 11 and Preacher and Hayes SAS Process Macro (Hayes, 2013; Hayes & Preacher, 2014).
Results
Results showed baseline discounting was a strong predictor of pre to post discounting changes in small, medium, and large reward magnitudes and overall log k (rs between −.31 and −.41, ps ≤ .01). BMI also predicted changes in large magnitude discounting (r = .25, p = .04). Baseline DD and BMI were thus used as covariates in the regression analyses. As shown in Figure 1, EFT participants significantly reduced their average pre-post discounting rate, log k = −0.97 ± 1.37, compared to ERT participants, log k = 0.30 ± 1.37, F(1, 62) = 14.04, p < .001, η2 = .18, 90% CI [0.06, 0.32]. Similarly, significant between group differences were observed for small, F(1, 62) = 8.36, p = .005, η2 = .12, 90% CI [0.02, 0.25], medium, F(1, 62) = 8.06, p = .006, η2 = .12, 90% CI [0.02, 0.24], and large, F(1, 62) = 15.24, p < .001, η2 = .20, 90% CI [0.07, 0.33], reward magnitudes. No differences were found in cue imagery ratings for EFT (4.19 ± 0.77) versus ERT (4.15 ± 0.77) during the DD tasks, F(1, 62) = 0.05, p = .83. Regression analyses showed that neither the motivation to lose weight (p = .51) nor the targeted amount of weight loss (p = .47) moderated the effects of EFT on DD.
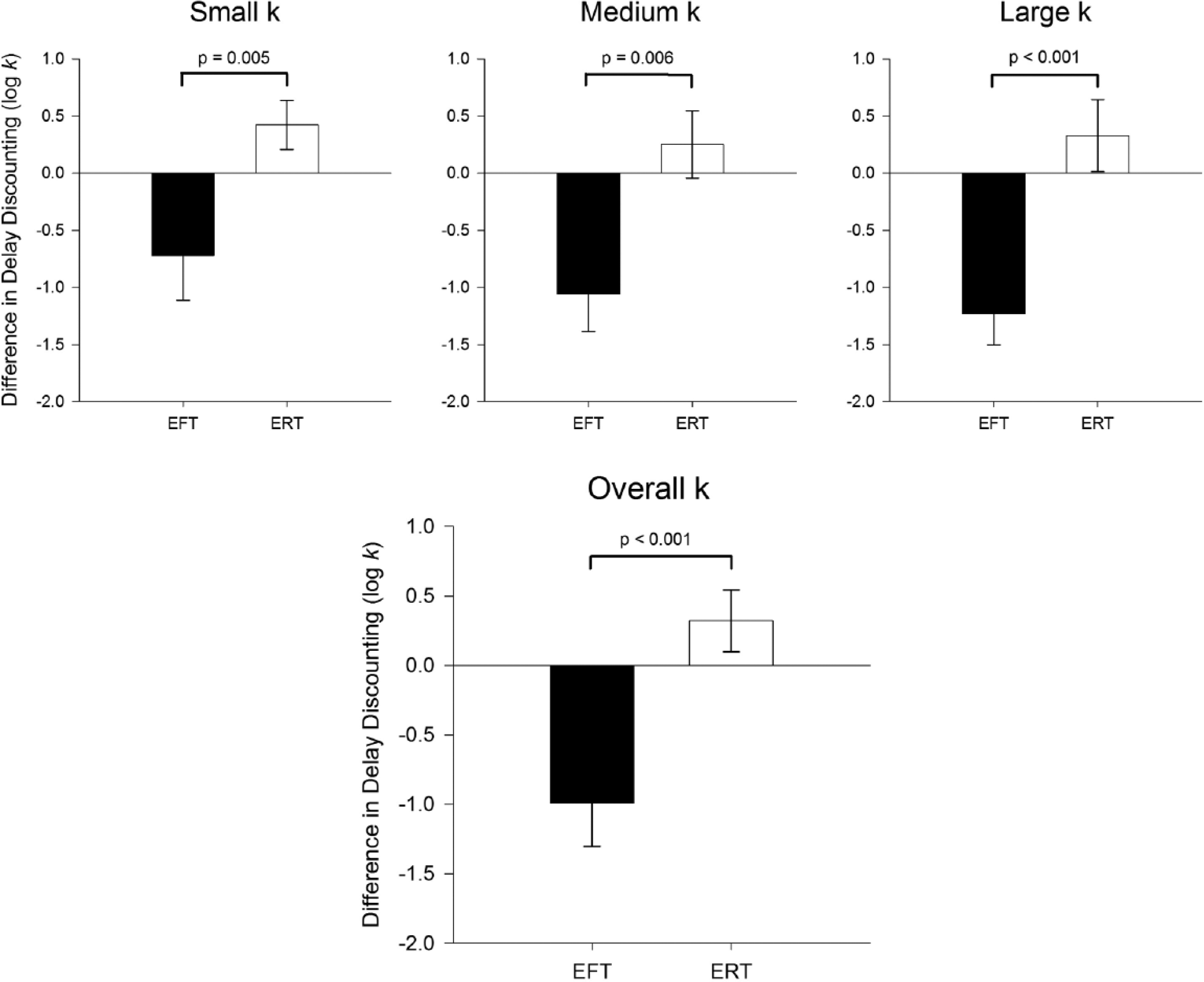
Mean log k changes from baseline to posttraining (mean ± SEM) for small, medium, large reward magnitudes and overall log k between episodic future thinking (EFT) and episodic recent thinking (ERT) condition. A reduction in log k indicates less discounting of the future. As indicated in the figure, EFT was significantly different from ERT in each analysis.
When excluding the 12 participants who did not correctly answer the attention check item (n = 54), similar differences between conditions were observed with EFT participants, log k = −0.72 ± 1.25 (n = 25), versus ERT, log k = 0.46 ± 1.24 (n = 29), significantly reducing DD, F(1, 50) = 11.87, p = .001, η2 = .19, 90% CI [0.05, 0.34]. In addition, differences were found between EFT and ERT for small, F(1, 50) = 6.91, p = .01, η2 = .12, 90% CI [0.02, 0.26], medium, F(1, 50) = 5.22, p = .02, η2 = .09, 90% CI [0.01, 0.23], and large, F(1, 50) = 13.77, p = 0.001, η2 = .22, 90% CI [0.07, 0.36], reward magnitudes. No differences were found in EFT (4.18 ± 0.79) versus ERT (4.12 ± 0.79) cue imagery ratings, F(1, 54) = 0.04, p = .81. Once again, neither the motivation to lose weight (p = .76) nor the targeted amount of weight loss (p = .54) moderated the effects of EFT/ERT on DD.
Discussion
Experiment 1 is the first demonstration that EFT administered online and independent of in-person administration can produce changes in DD. Our results suggest online EFT training can increase the scalability of EFT interventions. Experiment 2 was designed to further assess the replicability and efficacy of online EFT training in persons with overweight/obese statuses. In addition, Experiment 2 examines whether EFT can reduce DD during immediate scarcity of economic resources, a situation that typically increases DD (Epper, Fehr-Duda, & Bruhin, 2011; Haushofer & Fehr, 2014).
Increased DD is associated with low educational achievement (de Wit, Flory, Acheson, McCloskey, & Manuck, 2007; Jaroni, Wright, Lerman, & Epstein, 2004) and increased mortality cues (Griskevicius, Tybur, Delton, & Robertson, 2011). The reduction in immediate resources forces people to focus on the present, rather than engage in long-range planning. This occurs across the socioeconomic spectrum (Mullainathan & Shafir, 2013), and narrows attention toward present needs, increasing discounting. Thus, individuals in vulnerable environments are at greater risk at making poor economic and behavioral decisions.
Higher rates of obesity are also more likely to be found in those with lower incomes (Schoenborn et al., 2002), Accessibility to food outlets (e.g., supermarkets versus fast foods; Smoyer-Tomic et al., 2008) can contribute to these rates and demand for food. In addition, increases in food reinforcement are also observed for those with lower income and education (Lin et al., 2013) with greater increases in food reinforcement observed in relation to stress (Adam & Epel, 2007).
Experiment 2 is the first study to access whether EFT can modify the reinforcing value or demand for food. Demand for food represents its reinforcing value. More specifically, changes in purchasing in response to price increase provides an index of the reinforcing value of food. For example, if Person A is sensitive to price, such that consumption decreases dramatically with increases in price and Person B decreases slowly with increasing price, then Person A’s consumption would be considered more elastic and the reinforcing value of food is less. In contrast, if Person A finds food very reinforcing, they will continue to purchase it even as the price rises, thus being less elastic.
We have shown that DD moderates the effect of food reinforcement on eating and obesity (Lin et al., 2013). If EFT also reduces both the demand for food as well as reduces DD, the two major components of reinforcement pathology (Bickel et al., 2012; Bickel, Jarmolowicz, Mueller, & Gatchalian, 2011; Carr et al., 2011), then these findings would provide additional support for EFT as a clinical intervention.
In Experiment 1, the Kirby monetary choice questionnaire (Kirby et al., 1999) was used to measure DD. The Kirby estimates DD by assessing choice between 27 isolated outcomes. In Experiment 2 we measured DD using an adjusting amount procedure that adjusts the choices based on the participants responding to provide a more sensitive index of DD (Du, Green, & Myerson, 2002).
Experiment 2
Method
Participants
In all, 219 AMT users who were at least 18 years of age, had a 90% acceptance rate on previous HITs, and currently resided in the United States completed the study. Implied consent was obtained when participants indicated they understood the description and continued on to the survey. Participants were excluded from completing the survey if they did not indicate they were overweight/obese (BMI ≥ 25) and expressed greater than moderate symptoms of depression (a score ≥ 10 on the Patient Health Questionnaire; PHQ-9; Kroenke & Spitzer, 2002). Depression was an exclusion criterion because prior data suggest depression is common in obese persons (Stunkard, Faith, & Allison, 2003), and depression can compromise positive temporal thoughts and experiences (MacLeod & Salaminiou, 2001).
Data were excluded from analysis if a participant did not follow instructions and carefully complete the survey questions. The analytical sample consisted of 204 of the 219 individuals studied. We excluded from analysis data from 15 participants who did not complete 100% of the survey items (n = 3), contributed data that were not systematically affected by the delay in the DD task (n = 2) or price in the purchase task (n = 9; Johnson & Bickel, 2008; Stein, Koffarnus, Snider, Quisenberry, & Bickel, 2015), or contributed data from which BMI could not be determined (n = 1).
A total of 204 participants were studied, and no differences between groups were observed in participant characteristics. Participants were 37.93 ±12.00 (M ± SD) years of age, 52% (106 out of 204) female, 81% (166 out of 204) nonminority and non-Hispanic, with 33.47 ± 5.99 BMI, 14.67 ± 1.87 years of education, $55,074 ± $39,685 household income, and a PHQ-9 score of 4.22 ± 2.89 (Kroenke & Spitzer, 2002). Participants were compensated $2.00 for completing the survey and earned an additional $4.00 bonus if their data were eligible for data analysis. Compensation was based on the federal minimum hourly wage (U.S. Department of Labor, 2016). The University at Buffalo and Virginia Tech Institutional Review Boards approved our study protocol.
Procedures
Participants were randomized to an income narrative (negative income shock vs. neutral income) and episodic thinking (EFT vs. ERT vs. no episodic thinking [NoET]) condition in a 2 × 3 factorial design. We approached this study using a factorial design that varies EFT/ERT/NoET, and neutral/negative narrative. This design provides the opportunity to determine whether any episodic thinking can influence DD, as well as comparing EFT to ERT and NoET.
Three conditions served as control conditions: (a) neutral income narrative was a control condition designed to isolate the effects of negative income shock, (b) ERT was a control episodic condition designed to isolate the effects of prospection in EFT, and (c) NoET was a control episodic condition designed to isolate the effects of any episodic thinking. All participants completed a demographics questionnaire, completed one of three episodic thinking tasks, and read one of two income narratives, which they were told to assume was true. Afterward, participants completed a DD task, food purchasing task, and the Positive Affect and Negative Affect Schedule (PANAS).
Participants in the EFT and ERT conditions generated events similar to the study procedures in Experiment 1. EFT participants generated personalized future events that they were looking forward to and could vividly imagine for three general different future periods (1 month, 2–6 months, and 7–12 months), and ERT participants, in contrast, generated personalized recent past events that they have enjoyed and could vividly remember for three general different recent past periods (1 day ago, 2–6 days ago, and 7–12 days ago). Participants in the NoET condition did not complete an episodic thinking task.
Next, participants were presented with their randomly assigned narrative and were asked to consider it for 15 seconds. Each narrative remained on the screen for 30 seconds before participants could continue to ensure consistent narrative exposure across participants. Participants were instructed to assume they were actually experiencing the conditions described in each narrative. The negative and neutral narratives (Bickel et al., 2016) read as follows:
“You have just been fired from your job. You will now have to move in with a relative who lives in a part of the country you dislike, and you will have to spend all of your savings to move there. You do not qualify for unemployment, so you will not be making any income until you find another job.”
“At your job, you have just been transferred to a different department in a location across town. It is a similar distance from where you live so you will not have to move. You will be making 2% more than you previously were.”
Participants then completed an adjusting-amount monetary DD task with choices between smaller amounts of hypothetical money available immediately or a larger, delayed amount ($100). Across consecutive trials, participants’ choices titrated the smaller amount until reaching a point at which participants were indifferent between choice options (Du et al., 2002). These indifference points index the discounted value of the larger, delayed option and were obtained at five different delays (1 day, 1 week, 1 month, 6 months, and 1 year; order randomized). Each choice was displayed on its own page along with the EFT/ERT participant’s self-generated event that corresponded to the delay for that choice. Participants were asked to imagine each event in detail as they were making choices. After each choice, participants provided imagery ratings on a 5-point Likert-type scale as described in Experiment 1. In contrast, NoET participants were not presented with events. Area under the curve (AUC), in which higher values of AUC reflect lower levels of DD, was calculated for this DD task (Myerson, Green, & Warusawitharana, 2001).
Finally, participants completed the food purchase task, which was modeled after the reinforcer efficacy questionnaire (Jacobs & Bickel, 1999; Murphy & MacKillop, 2006), adapted for food reinforcers (Epstein, Dearing, & Roba, 2010). Participants were provided a fixed list of common fast foods which included one medium order of McDonald’s French fries, one McDonald’s cheeseburger, one medium Arby’s curly fries, one Arby’s roast beef sandwich, one Taco Bell burrito or taco, one slice of Pizza Hut or Domino’s pizza, one Kentucky Fried Chicken breast, 12 Chick-fil-A chicken nuggets, one Panera or Starbucks bagel, and one Dunkin’ Donuts or Krispy Kreme donut and were instructed to select their favorite. At each of the 13 different prices per serving ($0.00–$160.00), participants reported the number of servings of their favorite fast-food item they would consume over a continuous, 7-day period. A week period was used to generate enough purchasing to provide granularity. Participants were asked to assume (a) that they could not save or stockpile food for a later date, (b) that they had no other access to their chosen food, but could purchase and eat other foods as they normally would, (c) that the available serving sizes were those specified earlier, (d) that they could not give away or share any of the purchased food, and (e) that they had the same income/savings they did now.
During each price, EFT and ERT participants were presented with textual episodic cues associated with the 1-year time frame and were asked to vividly imagine the associated events. NoET participants were not presented with cues and were not asked to engage in episodic thinking during the food purchase task. The food purchase task provides five distinct aspects of food reinforcement: demand intensity (consumption unconstrained by price), demand elasticity (sensitivity of consumption to increases in price), Pmax (the price at which maximal purchasing is observed), Omax (the total amount of money spent at maximal purchasing price), and breakpoint (the price at which no more purchasing occurs). The observed values for each of these demand indices were used with the exception of demand elasticity, which was calculated for individual participants by fitting the empirical demand curves with the following equation (Koffarnus, Franck, Stein, & Bickel, 2015; MacKillop & Murphy, 2007; Yu, Liu, Collins, Vincent, & Epstein, 2014) modified from the exponential demand equation introduced by Hursh and Silberberg (2008):

Here, Q is consumption, P is price, k is span of consumption in log10 units, and Q0 and α served as dependent measures of demand intensity and elasticity, respectively.
Manipulation check
To test the valence of narratives and episodic thinking conditions, participants were asked to rate their current mood. To detect if participants were thinking about their events, in between each delay in the DD task, and after each measure, participants were asked to rate on a scale from 1 to 5 (1 = not at all, 5 = very much) how much they thought about and how vivid their thoughts were about their cues. A cue imagery score was calculated as the average of overall thoughts and vividness ratings.
In addition, to estimate if participants were attending to each monetary choice, two attention check items were interspersed randomly among existing trials in the DD task. In one item, participants chose between $50 now and $0 in 1 day; in the other item, participants chose between $0 now and $100 in 1 day.
Other measures
Demographics
Information about age, race/ethnicity, income, and educational level was obtained using a standardized questionnaire adapted from MacArthur’s network for studies on socioeconomic status and health (Adler et al., 2000).
The Patient Health Questionnaire (PHQ-9)
Severity of depression was screened using the PHQ-9, a 9-item questionnaire that rates the frequency of depressive symptoms and scores of 5, 10, 15, and 20 represents mild, moderate, moderately severe, and severe depression, respectively (Kroenke & Spitzer, 2002).
Positive Affect and Negative Affect Schedule (PANAS)
Participants rated on two primary dimensions of mood, positive and negative affect, on a 20-item scale consisting of 10 positive affect items (e.g., “proud”) and 10 negative affect items (e.g., “afraid”; Watson, Clark, & Tellegen, 1988). Participants rated the extent to which they were experiencing each affect “right now,” using a 5-point Likert-type scale ranging from 1 (very slightly or not at all) to 5 (extremely). The ratio of positive to negative affect (Larsen & Prizmic, 2008) was used as the dependent variable, calculated as the sum of all ratings of positive affect items divided by the sum of all ratings of negative affect items.
Analytic plan
Separate one-way ANOVAs for continuous variables and chi-square tests for categorical variables were conducted to determine group differences in participant characteristics. Subject characteristics that might serve as covariates were assessed by examining between group differences and whether potential covariates correlated with the primary measures (i.e., AUC, food demand). A 3 × 2 factorial ANCOVA with type of cue (EFT/ERT/NoET) × income narrative (negative/neutral) as the between variable was used to access differences in AUC, food demand, PANAS ratio, and cue imagery. Effect sizes (η2) and 90th percentile η2 confidence intervals were calculated (Steiger, 2004) for the AUC and demand indices. All demand indices were natural log transformed prior to analysis to obtain a normal distribution. In addition, correlations between the demand indices were determined. Data analyses were completed using SYSTAT and SPSS.
Results
Overall, average AUC discounting rate was 0.57 ± 0.27, and the log transformed food demand indices were −4.47 ± 1.06 elasticity (α), 2.34 ± 1.01 intensity (Q0), 0.22 ± 1.23 Pmax, 1.87 ± 1.10 Omax, and 1.75 ± 1.07 breakpoint. Sex predicted elasticity, intensity, Pmax, Omax, and breakpoint (rs = .32, −.21, −.17, −.29, −.21; ps ≤ .001, .003, .02, .001, .003, respectively), consistent with previous research showing men find food more reinforcing than women (Epstein et al., 2004), BMI predicted Pmax (r = –.15, p = .03), consistent with previous research (Epstein, Jankowiak, Fletcher, et al., 2014), and age predicted intensity (r = −.16, p = .03) and breakpoint (r = −.18, p = .01). Sex, BMI, and age were used as covariates in the ANCOVAs.
DD was greater for the negative income shock narrative compared to the neutral income narrative condition, F(1, 195) = 32.08, p < .001, η2 = .14, 90% CI [0.07, 0.21], shown in the top panel of Figure 2, and cue type influenced AUC, F(2, 195) = 9.30, p < .001, η2 = .09, 90% CI = 0.03 − 0.15. As shown in the bottom panel of Figure 2, linear contrasts showed EFT discounted less than both ERT, F(1, 195) = 14.92, p < .001, and NoET control, F(1, 195) = 13.18, p < .001, and no differences in AUC were observed comparing ERT to NoET controls, F(1, 195) = 0.02, p = .88. No interaction of cue type by narratives were observed.
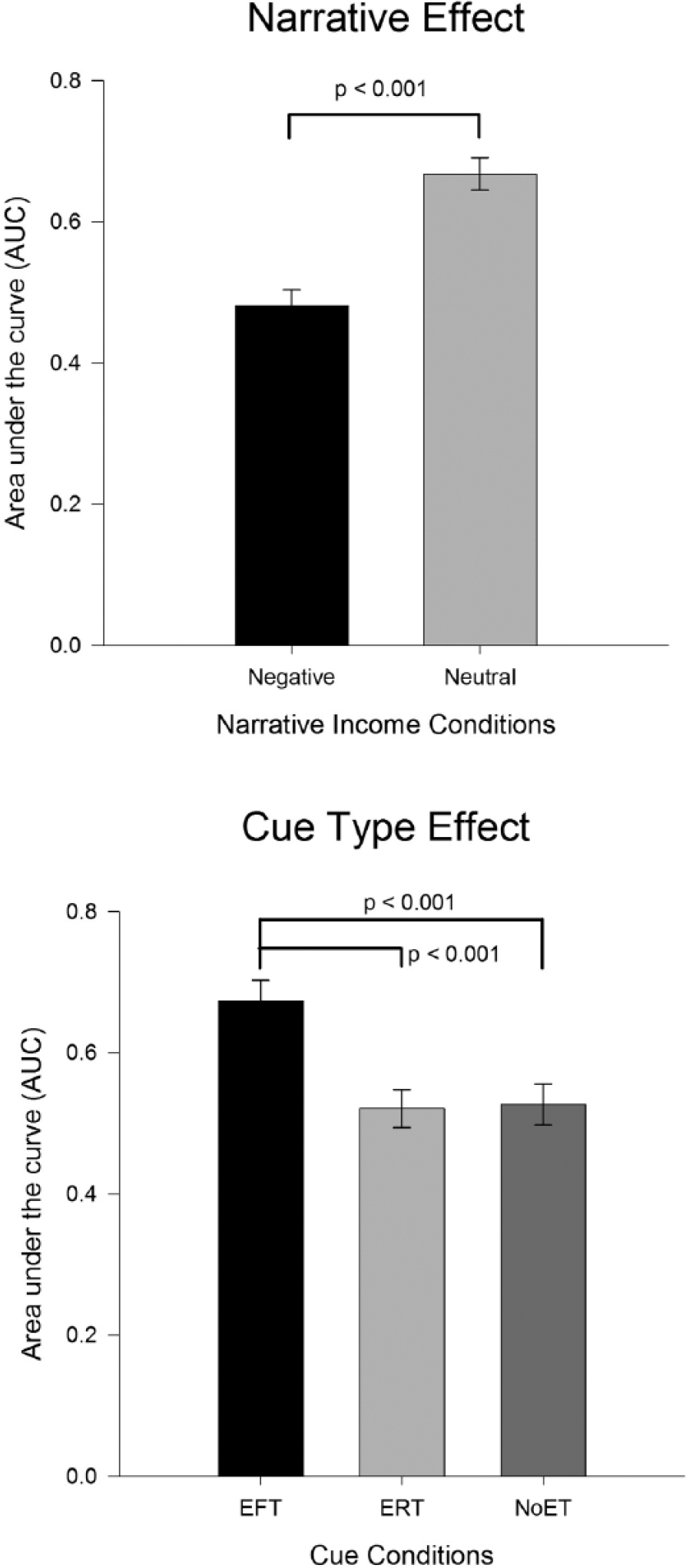
Mean area under the curve (AUC) values (mean ± SEM) for main effects of narrative type (upper panel) and cue type (lower panel). Greater AUC indicates less discounting of the future.
Indices of food reinforcement and cue type are shown in Figure 3. An effect of cue type was observed for demand elasticity, F(2, 195) = 12.97, p < .001, η2 = .12, 90% CI [0.05, 0.18], with lower elasticity in EFT compared to ERT, F(1, 195) = 10.29, p = .002, and NoET control, F(1, 195) = 25.42, p < .001, and no significant difference observed when comparing ERT and NoET, F(1, 195) = 3.84, p > .05; demand intensity, F(2, 195) = 11.02, p < .001, η2 = .10, 90% CI [0.04, 0.17], with EFT showing lower demand for food than NoET control, F(1, 195) = 21.67 p < .001, and ERT significantly different from NoET control, F(1, 195) = 8.46, p = .004; Omax, F(2, 195) = 15.24, p < .001, η2 = .14, 90% CI [0.06, 0.21], with EFT showing lower Omax than ERT, F(1, 195) = 9.21, p = .003, and NoET control, F(1, 195) = 30.43, p < .001, and ERT significantly different from NoET control, F(1, 195) = 6.85, p = .01; breakpoint, F(2, 195) = 3.45, p = .03, η2 = .03, 90% CI [0.00, 0.08], with EFT showing lower breakpoint than ERT, F(1, 195) = 5.49, p = .02, and NoET control, F(1, 195) = 4.96, p = .02, and no difference with ERT compared to NoET control, F(1, 195) = 0.004, p = .95.
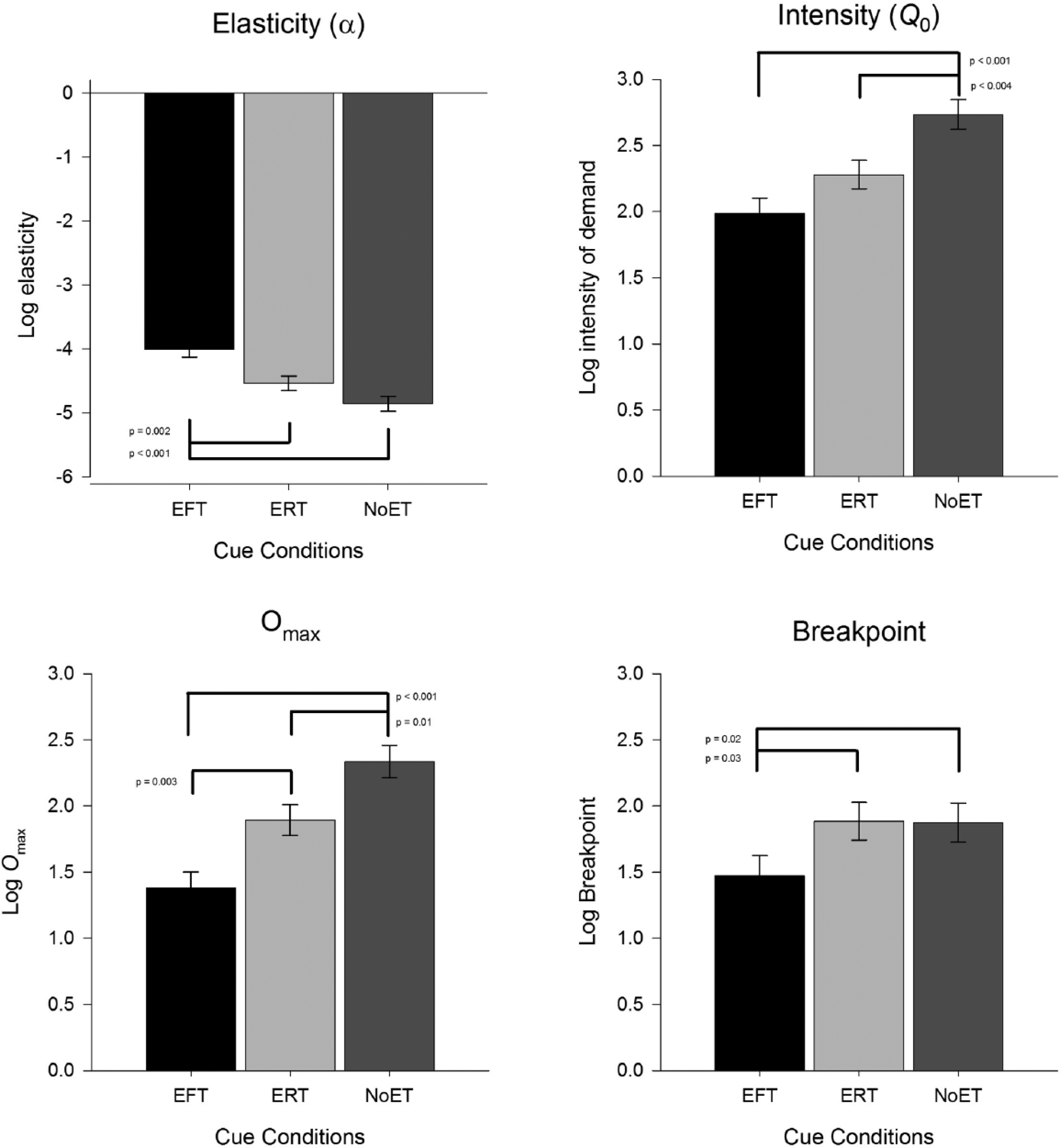
Mean indices of food reinforcement (mean ± SEM) for main effects of cue type (elasticity, top left panel; intensity, top right panel; Omax, bottom left panel; breakpoint, bottom right panel. Greater elasticity values indicate more sensitive to price.
Narrative influenced demand intensity, F(1, 195) = 10.39, p = .001, η2 = .05, 90% CI [0.01, 0.11], as intensity was greater for the neutral narrative (Fig. 4). No effects were observed for narrative conditions in elasticity, F(1, 195) = 0.01, p = .93, Omax, F(1, 195) = 0.89, p = .35, and breakpoint, F(1, 195) = 2.17, p = .14.
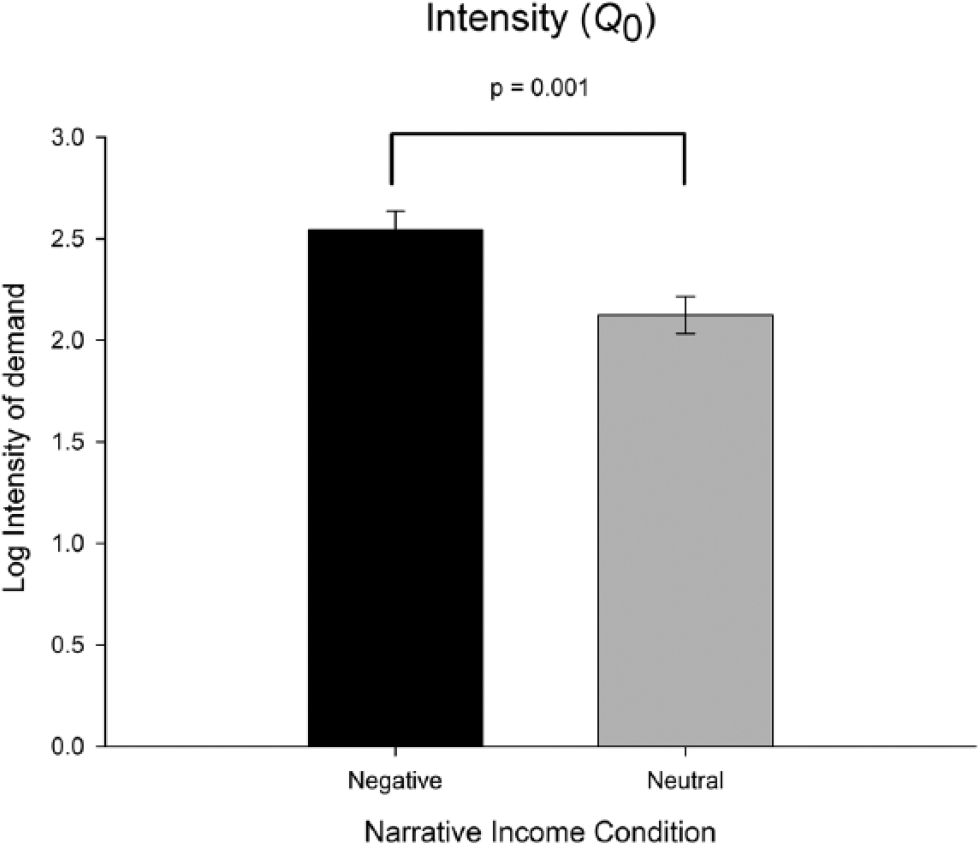
Mean intensity of demand for fast foods (mean ± SEM) for main effects of income narrative.
No effects of cue type or narrative, or the interaction of cue type by narrative were observed for Pmax, F(2, 195) = 1.22, p = .30; F(1, 195) = 1.01, p = .32; F(2, 195) = 0.62, p = .54, respectively. In addition, no interaction of cue type by narrative was observed for elasticity, F(2, 195) = 0.13, p = .88, intensity, F(1, 195) = 1.92, p = .15, Omax, F(2, 195) = 0.02, p = .98, breakpoint between cue type and narrative, F(2, 195) = 0.22, p = .80.
Correlations between the demand indices showed that elasticity is significantly related to intensity, Pmax, Omax and breakpoint (rs = –.53, –.40, –.92, –.62; ps < .001), intensity is significantly related to Omax and breakpoint (rs = .55, .14; ps < .05), breakpoint is related to Pmax and Omax (rs = .82, .73; ps < .001), and Omax is related to Pmax (r = .61, p < .001).
Narrative influenced the positive/negative affect ratios from the PANAS, F(1, 195) = 35.11, p < .001, η2 = .15, 90% CI [0.08, 0.23], as the ratio was lower in the negative (1.82 ± 0.95) than neutral (2.55 ± 0.83) narrative conditions. No effect of cue type, F(2, 195) = 2.25, p = .11, or interaction of cue type × narrative, F(2, 195) = 2.32, p = .10, was observed. Consistent with Experiment 1, no between group differences were observed in cue imagery ratings for EFT versus ERT, negative versus neutral cues, or cue imagery × narrative.
Discussion
Experiment 2 replicated our findings in Experiment 1 suggesting that online-administered EFT reliably reduces DD. Replication strengthens our confidence in the reliability of the results (Yong, 2012). No differences in discounting rates between ERT and NoET participants suggest that ERT is a strong control for the development of episodic cues without influencing temporal orientation and discounting. Consistent with previous findings, we observed that negative income shock increased DD and worsened mood (Bickel et al., 2016; Haushofer et al., 2013). Nevertheless, we showed that EFT reduced discounting rates and demand of high energy, dense fast foods, even when challenged by the harmful effects of negative income shock.
General Discussion
This study provided the first evidence that EFT can be effectively administered remotely, specifically online. This effect was replicated in two studies, across people who were interested in losing weight as well as individuals with overweight/obese statuses. Moreover, EFT’s effect was shown using two different measures of DD (i.e., Kirby and adjusting amount). The extension of EFT training to an online environment increases the scalability of the intervention, and may complement existing treatments. Advantages to remote implementation may be reduced expenses (e.g., travel), time, participant burden, and reduced cost of treatment implementation. In addition, research supports the use of crowdsourcing as a complement to traditional health related research and treatments (Swan, 2012) and has observed positive behavioral outcomes for online interventions (Couper et al., 2010; Hill & Weinert, 2004).
Negative income shock, a laboratory analogue that induces scarcity, is related to greater discounting of the future (Bickel et al., 2016; Haushofer et al., 2013). However, when provided with EFT training, EFT participants reduced discounting rates, suggesting EFT can improve decision making in those who may be more vulnerable to the effects of scarcity. For instance, EFT could mitigate the effects of food insecurity, which is associated with low income and related to obesity (Epstein, Jankowiak, Lin, et al., 2014). We also found that EFT participants reduced discounting regardless of the type of income narrative suggesting EFT effects are not limited to specific demographical groups.
We showed for the first time that EFT can influence measures of food reinforcement. The effect of EFT on demand elasticity, intensity, amount of money spent on food at maximal price, and breakpoint for buying fast food was observed equally across both income narratives, with an increased sensitivity to price (elasticity) and a general reduction demand intensity, the amount of money spent on food at maximal price and breakpoint for EFT participants. EFT’s effects on food reinforcement suggest that EFT reduces discounting of the future, but also reduces the reinforcing value of food. Thus, EFT may proactively influence key elements of reinforcement pathology (Bickel et al., 2012; Carr et al., 2011). In other research we have found DD moderates the influence of the reinforcing value food on eating (Epstein, Carr, Lin, & Fletcher, 2011; Rollins et al., 2010) and obesity (Epstein, Jankowiak, Fletcher, et al., 2014). If food reinforcement is low, not much self-control is needed, but if food reinforcement is high, then the ability to delay gratification is essential. However, the focus of EFT in prior research has been on DD (Bromberg et al., 2015; Daniel et al., 2016; Snider et al., 2016). Demonstrating EFT’s ability to concurrently reduce DD and food reinforcement could comprehensively modify critical aspects of overeating and obesity.
Although the effect of episodic thinking on four food demand indices suggests a strong effect of EFT and the correlations between the indices suggest they are related, it is not clear why the maximal price people are willing to spend on food (Pmax) was not affected. Future research is needed to examine the relevance of Pmax compared with the other indices of food demand, and whether EFT can influence demand indices of other commodities.
The clinical utility of EFT will depend on, in part, how EFT can be used to modify the hundreds of decisions people make daily that can influence their health. We envision several different scenarios in which EFT can be used. First, people can use EFT when they are experiencing a tempting situation that involves an immediate reward related to less healthy behaviors so that they can make the choice to not engage in that behavior for the greater future good of a larger, but remote, reward. This could involve engaging in EFT as many times per day as needed to effectively reorient the person from focusing on immediate unhealthy behaviors to focusing on delayed but healthier outcomes. This can also involve engaging in EFT strategically at certain times of the day when a person may be more vulnerable to impulsive decisions (e.g., immediately prior to meal times or prior to times the person normally snacks). These approaches can now be feasible because EFT is easily transportable and easy to implement. A second approach is to carefully assess the durability of a single EFT experience on subsequent choices. The duration of the EFT’s effects is unknown, but it’s possible that one period of reallocating attention from immediate rewards to delayed rewards may activate prospective thinking across the day. This may be more likely if a person feels that EFT was effective in helping to fight cravings or not to give in to impulsive temptations. Perhaps a third approach would be to train people to engage in more prospective thinking. We conceptualize this as a matter of conditioning prospective thought. For most people, the stimulus of encountering a craved object leads to wanting to obtain that craved object. but what if the same stimulus led to automatic prospective thought so that seeing an object of desire that negatively impacts health led to putting the brakes on that response and deciding to engage in behaviors that make it more likely to be healthy later? Our future research will explore ways to condition people to experience the imagery associated with EFT when they are presented tempting, highly reinforcing stimuli that normally lead to unhealthy behavior. Changing a person’s time perspective from wanting small immediate rewards to thinking about and planning for the future and making decisions for the greater future good could have profound effects on a person’s health.
Our studies have potential limitations. Only depression was used as an exclusionary criterion in Experiment 2, and although depression is common in the overweight/obese, these persons can also experience a range of other psychiatric symptoms that may moderate the influence of EFT on temporal orientation. Nevertheless, EFT was still effective in Experiment 1, although individuals were not excluded for psychiatric reasons. Further exploration could determine if EFT can combat the negative effects of psychiatric symptoms.
The rewards in this DD task were all hypothetical and perhaps may not reflect the discounting of actual outcomes. However, many studies have demonstrated the comparability of real and hypothetical discounting in both behavioral and neural imaging studies (Bickel, Pitcock, Yi, & Angtuaco, 2009; Johnson & Bickel, 2002; Lagorio & Madden, 2005; Madden, Begotka, Raiff, & Kastern, 2003). Likewise, although the food purchasing task uses hypothetical purchasing of food we have shown that examining food reinforcement in terms of hypothetical purchasing of food is similar to laboratory based methods in which participants physically work for food (Epstein et al., 2010). Moreover, others have also shown within-subject correspondence between purchasing of real and hypothetical commodities in similar purchase tasks (Amlung, Acker, Stojek, Murphy, & MacKillop, 2012).
Generalizing from crowdsourcing samples to participants who are not recruited using crowdsourcing may be challenged. However, research suggests crowd sourced samples may be more representative of the general population than convenience samples often used in studies of decision making (Berinsky, Huber, & Lenz, 2012). Crowdsourcing is a viable research method (Paolacci, Chandler, & Ipeirotis, 2010), and other studies from our laboratory have demonstrated interventions can be evaluated using crowdsourcing (Wen, Higgins, Xie, & Epstein, 2015). Furthermore, research suggest that crowdsourcing software offers several advantages for clinical research while providing insight into potential problems, such as misrepresentation, that researchers should address when collecting data online (Shapiro, Chandler, & Mueller, 2013). It is interesting that, when comparing the effects of in-person training to online training, the magnitude of the effects of EFT were greater in our study than observed for individuals recruited from the local community (Lin & Epstein, 2014). Perhaps these differences were contributed to the delivery of EFT training, thus an EFT training that could provide independent of in-person administration could standardize delivery of the most effective EFT treatment.
Lastly, as our study only provided one training session and examined changes in discounting rate and food reinforcement, the effect on behavioral outcomes such as energy intake or body weight is not known. However, previous studies have shown one session of EFT can influence energy intake in adults (Daniel et al., 2013; O’Neill et al., 2016) and children (Daniel et al., 2015), and EFT implemented in treatment programs can facilitate weight control (Sze et al., 2015). This evidence suggests treatment programs that include a web-based component could provide a unique and very scalable approach in reducing discounting of the future in obese persons. Moreover, it could even be adapted and used by any patient group that has steep discounting rates. Although we are focusing on the strength of these current results, we look to the future for integration of scalable EFT interventions into clinical treatment programs.
Footnotes
Acknowledgements
We sincerely appreciate Tinuke Oluyomi Daniel and Colleen K. Kilanowski for feedback on study design, and Liqa Athamneh, Akshata Chaudhary, and Elaine M. Slaven for assisting in material preparation.
Declaration of Conflicting Interests
We disclose that Leonard H. Epstein has equity in Kurbo and Warren K. Bickel has equity or contributions in HealthSim LLC, NotifiUs LLC, Sober Grid Inc., DxRx Inc., ProPhase LLC, and Teva Branded Pharmaceutical Products R&D.
Funding
This study was funded in part by Grant RO1 HD080292 from the National Institute of Child Health and Human Development, awarded to Leonard H. Epstein; and the National Institutes of Health (NIH) Science of Behavior Change Common Fund Program through an award administered by the National Institute of Diabetes and Digestive and Kidney Diseases (1UH2DK109543-01), awarded to Leonard H. Epstein and Warren K. Bickel.