
Abstract
Previous research has paid little attention to the role of kinship in understanding the specific profiles of complicated grief (CG) reactions. To address this underinvestigated topic, the Inventory of Complicated Grief was used in five groups of bereaved participants (N = 1,105) that differed in their family relationship with the deceased (child, spouse/romantic partner, sibling, parent, and grandparent). Results identified kinship relationship as the variable that predicted the highest amount of variance in the intensity of CG (standardized β = –.55), above other predictors such as gender, time since loss, or circumstances of death. More important, distinct profiles of CG reactions were found depending on kinship. These results highlight kinship as a major predictor of CG and open a new line of research that serves to clarify the role of kinship along with other risk factors.
Between 10% and 15% of bereaved people could develop pathological or complicated grief (CG), which is characterized by intense and prolonged feelings of yearning accompanied by separation anxiety symptoms and difficulties to continue living. CG is considered a single and unidimensional construct (Maciejewski, Maercker, Boelen, & Prigerson, 2016). The criteria for persistent, complex bereavement-related disorder included in the appendix of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as a diagnosis that needs further research highlight specific grief reactions among children but do not differentiate reactions among adults (American Psychiatric Association, 2013). Different profiles of grief reactions are thus not expected to occur among adults. However, because “relationships serve different functions and fulfill different needs in people” (Kosminsky & Jordan, 2016, p. 76), losing someone of a different kinship is expected to make the grief process a different experience, leading to different reactions and intensities. In fact, most handbooks on bereavement present independent chapters that address the loss of a spouse, a child, a parent, a grandparent, or a sibling as separate entities (e.g., Neimeyer, Klass, & Dennis, 2014; Stroebe, Hansson, Schut, & Stroebe, 2008). This distinction is also found in research articles, where the vast majority of studies focus on a single type of lost relationship. Nevertheless, empirical data have in fact rarely directly compared profiles of grief reactions according to the kin lost. In sum, it is not known if one or multiple grief profiles should be expected according to different kinship relationship losses.
In the present article, we propose that the kinship relationship to the deceased person (KR) is a powerful determinant of differences, not only in intensity, but in profiles of grief reactions among bereaved adults. Previous literature has found kinship to be associated with different grief intensities or CG prevalence rates (e.g., Kersting, Brähler, Glaesmer, & Wagner, 2011; Neria et al., 2007). The DSM-5 outlines that the death of a child is a risk factor of CG. Research indeed found that it leads to higher intensity or prevalence rates than the death of a spouse, which in turn is associated with higher intensity of grief reactions than the death of a sibling, parent, or grandparent.
Although kinship was associated with general grief intensity, different theoretical perspectives explain why it should in fact be linked to different types of grief reactions. From an evolutionary and attachment perspective, different KR play different basic functions (Archer, 2008), such as emotional support, companionship, labor sharing, mutual caregiving for a spouse/partner, protection and nurturing for parents, sense of continuity to personal identity, and history for siblings (Kosminsky & Jordan, 2016). The loss of these different functions should imply different types of reactions such as shock, sadness, anger or frustration, loneliness, and guilt. According to emotion theories, the appraisals of the event determine the types and intensity of emotional reactions that occur (e.g., Moors, Ellsworth, Scherer, & Frijda, 2013). Appraisal of the deceased likely depends on KR. Indeed, the death of a child or a spouse may be subjectively experienced as a more uncontrollable and impactful event, leading to more intense shock and yearning, than the loss of a parent or grandparent. Third, from a socioconstructivist perspective, the death of a relative may shatter one’s assumptive world and basic beliefs about life, oneself, others, and the world (Neimeyer et al., 2014). In Western culture, the loss of a child in particular may provoke a dissonance in one’s meaning structures, triggering a complex process of search for meaning, and leading to feelings of shock, anger, and disbelief (Gillies & Neimeyer, 2006). Likewise, from a memory theory perspective, such deaths should be more complex to integrate into one’s biographical self and identity (Maccallum & Bryant, 2013), leading to more intrusive thoughts of the death or deceased. Finally, a social and interactionist perspective obviously concurs with the hypothesis that the loss of a different kin will differently impact daily living and family interactions as well as different secondary stressors: administrative and financial difficulties, loss of social connections, or identity changes (Stroebe & Schut, 2015).
The differential effects of KR on specific profiles of grief reactions remain mainly untested. Only a few studies have directly tested whether particular CG reactions occurred as a function of KR. In comparison to those having lost a spouse or a parent, people that have lost a child reported higher scores on despair, anger, somatization, death anxiety, search for explanation, abandonment (Esmaeilpour & Bakhshalizadeh Moradi, 2015; Sanders, 1980), and depressive symptoms (Leahy, 1992–1993). Using the Inventory of Complicated Grief (ICG), in a sample of participants endorsing CG, Zetumer et al. (2015) consistently found that those who had lost a child presented higher symptoms of yearning, anger, and shock than another group of participants that had experienced other types of losses, without systematically differentiating them. These results suggest that profiles of grief reactions might depend on KR. However, these studies on KR did not cover the distinct representative symptoms of CG and one cannot therefore ascertain that profiles of CG reactions indeed depend on KR. More generally, previous studies have limitations such as (a) the lack of a systematic comparison between distinct kinship groups, (b) the heterogeneity of instruments used to assess grief outcomes, and (c) the small sample sizes (i.e., N < 180; Esmaeilpour & Bakhshalizadeh Moradi, 2015; Sanders, 1980).
The aim of the current investigation was to examine whether the kinship relationship between the bereaved and the deceased explains different profiles of grief reactions. In the present study, we compared five different kinship groups within a large sample of bereaved individuals using the most widely known measure of CG. Recent studies have found that the ICG comprises a series of clusters of grief reactions including anger, shock, yearning, estrangement from others, hallucinations, and behavior change (Simon et al., 2011). The present study thus examined whether these clusters of reactions were different according to KR. Based on previous research on kinship, we (a) checked whether grief intensity and CG prevalence rates would be higher with child loss than with spouse and sibling loss, which in turn should be higher than parent or grandparent loss, (b) checked whether CG intensity would be explained by the KR of the deceased, above other classical variables such as gender and circumstances of death, and (c) tested whether the grief reactions associated with the death of a child would be characterized by more intense reactions of shock, anger, yearning, estrangement from others, and hallucinations (memories and images) in comparison to other deaths.
Method
Participants
A total of 1,613 participants were gathered from 13 studies conducted between 2002 and 2014 under the supervision of the second author. No data have previously been published, with the exception of one study on attachment and grief reactions (Anonymous Reference (Delespaux, Ryckebosch-Dayez, Heeren, & Zech, 2013)). Two modes of recruitment were used: (a) direct contact through obituaries (n = 478, 36.8%) and (b) indirect contact through the Internet (n = 821, 63.2%). The inclusion criterion for taking part in the studies was having experienced the loss of a grandparent, parent, sibling, spouse/romantic partner, or child. The exclusion criteria were having experienced (a) the loss less than 6 months ago and (b) other types of loss (i.e., friends, aunts/uncles, cousins, other relatives). Accordingly, a total of 508 participants (31.49%) were removed from the sample.
The final sample was composed of 1,105 participants. All participants were born in France or Belgium and had French as their mother tongue. These were mainly women (n = 844, 76.40 %) contacted through the Internet (n = 627, 56.70%). Their mean age was 43.42 years old (SD = 16.04; min = 18 years, max = 88 years). Regarding civil status, 31.50% (n = 348) of the participants were widowed, 24.30% (n = 268) single, 16.7 % (n = 185) married, and 3.80% (n = 42) divorced (n = 262 had missing data). The delay since loss was on average 27.22 months (SD = 38.12), ranging from 6 to 454 months. The family member who had died was a child in 6.30% of the cases (n = 70), a spouse or romantic partner in 55.80% of the cases (n = 617), a sibling in 2.0% of the cases (n = 22), a parent in 19.70% of the cases (n = 218), and a grandparent in 16.10% of the cases (n = 178). The majority of deceased persons were men (n = 733, 69.30%) and were on average 55.53 years old at the moment of death (SD = 22.12, age range from 0 to 105 years old). The circumstances of death were grouped in natural (n = 743, 67.20%) or traumatic deaths (n = 232, 21.00%; 11.80% missing data).
Measures
The ICG (Prigerson et al., 1995) is a self-report measure comprising 19 items that assess the appearance of symptoms related to CG (on a 5-point Likert-type scale ranging from 0 to 4). Psychometric studies have shown high internal consistency (Cronbach’s α = .94) and test-retest reliability (rtest-retest = .80). The measure provides a single score of the intensity of grief symptomatology as well as six dimensions of grief reactions (Simon et al., 2011). It has been widely used as a valid measure to distinguish between complicated and noncomplicated grief. Two cutoff points were reported to identify caseness of CG: The first was >25 (Prigerson et al., 1995), whereas recent research considered a second cutoff of >30 (Simon et al., 2011). It has been suggested that these cutoff points should be used with caution, being indicators for clinicians rather than for diagnosing CG (Stroebe et al., 2000). In the current study, we used the French version of the ICG (Zech, 2006). The Cronbach’s alpha in the current sample was .93. The ICG mean score was 28.97 (SD = 16.63).
Procedure
Participants were recruited from two sources: obituaries and the Internet. In the first case, the obituary section of national and local newspapers was reviewed to identify participants that had lost a family relative in the last 6 to 75 months. Participants were then sent a letter and further contacted by phone to present the objectives of the research; they were then asked to participate. Upon acceptance, the researchers sent them a stamped and addressed return envelope containing the questionnaires. In the second case, advertisements were posted on Internet and forum web pages. The questionnaire was available online for anyone who had lost a family member and who wanted to participate.
The data available in each of the 13 studies were merged into a single database to make the analyses on kinship. Although each initial study varied on specific objectives, all included at least the ICG, demographic variables related to the bereaved individual (age, gender, civil status, and relationship to the deceased) and descriptive variables of the death or the deceased (circumstances of death, age, gender of the deceased). Participants were informed about the objectives of each study and voluntarily signed a written informed consent form. Each study composing the present database was approved by the ethical committee of the university.
Data analysis
First, an ANCOVA using kinship difference as independent variable, time elapsed since loss, type of death, and gender as covariates and the ICG score as dependent variable was performed. Second, a hierarchical linear regression was carried out including three blocks of variables: (a) the mode of recruitment (0 = Internet, 1 = obituary), (b) the usual predictors, including age, gender (0 = male, 1 = female), gender of the deceased (0 = male, 1 = female), circumstances of death (0 = traumatic, 1 = natural), and time elapsed (in months) since loss, and (c) kin lost (0 = child, 1 = spouse/partner, 2 = sibling, 3 = parent, 4 = grandparent). Third, chi-square tests were used to examine kinship differences according to specific CG diagnostic models. Finally, a confirmatory factor analysis (CFA) using maximum likelihood method estimation, followed by ANCOVAs (using time elapsed since loss, type of death, and gender as covariates) were used to test differences in each specific cluster of grief reactions. SPSS Version 22 (SPSS Inc., Chicago, IL, USA) and Mplus Version 9 (Muthén & Muthén, 2010) were used.
Results
Intensity and diagnostic criteria of CG depending on kinship
In line with previous research, the ANCOVA yielded a statistically significant difference in the ICG according to kinship, F(43, 967) = 67.75, p < .001, partial η2 = .22 (see Fig. 1A and Table 1). The main effects of covariates are shown in Supplementary Material (SM) 1 (available online). It is interesting, and contrary to previous research, that Bonferroni post hoc tests indicated that the death of a child induced similar grief reactions to the death of a spouse and the death of a sibling. The death of a child or a spouse induced more intense grief reactions than the death of a parent, which was in turn related to more intense grief reactions than the loss of a grandparent (p < .001 in both cases).

Differences in complicated grief according to kinship relationships. (A) Differences in CG reactions’ intensity (means) depending on kinship groups. (B–D) Percentage of participants endorsing CG following three different criteria depending on the kinship loss.
Estimated Means, Standard Errors, and Results of the ANCOVA (Including Time Elapsed Since Loss, Type of Death, and Gender as Covariates) and Post Hoc Analyses for the Total Score and for Each of the Six Factors of the ICG Depending on the Kinship Relationship
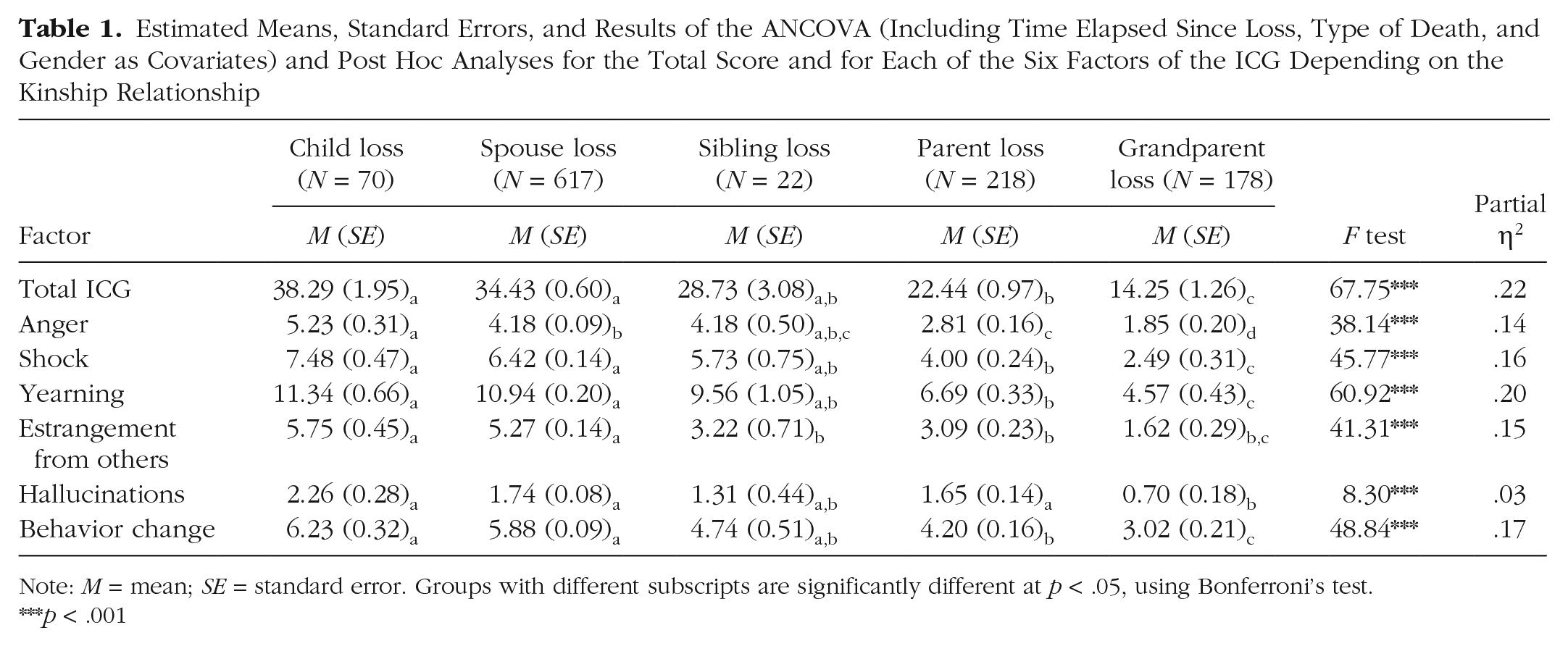
Note: M = mean; SE = standard error. Groups with different subscripts are significantly different at p < .05, using Bonferroni’s test.
p < .001
The hierarchical linear regression analysis showed that the last model, which included three blocks of variables, was statistically significant, F(7, 965) = 64.45, p < .001, and explained about 32% of the variance, R2 = .319 (see SM 2). Five variables from the last model had significant effects, indicating that CG intensity was positively related, in decreasing order of association, with the loss of a child or spouse (kinship, standardized β = –.55), Internet recruitment mode (mode of recruitment, standardized β = –.17), being a woman (participant’s gender, standardized β = .14), a shorter time elapsed since loss (time elapsed since loss, standardized β = –.08), and having experienced a traumatic death (circumstances of death, standardized β = –.07). Adding kinship to the third block explained an additional 19% of the variance in CG intensity (ΔR2 = .190, p < .001).
Descriptive statistics and chi-square analyses were used to explore the variability in CG prevalence depending on kinship (see Fig. 1 and SM 3). When using the ICG > 25 criterion (Prigerson et al., 1995), 78% of participants who had lost a child and the 73% who had lost a spouse were diagnosed with CG (see Fig. 1B and SM 3). Significant differences in prevalence rates between the five kinship groups were found, χ2(4, N = 1,105) = 223.32, p < .001, and further comparisons between groups indicated that those participants who had lost a child, a spouse, or a sibling had higher probability of having CG than participants who had lost a parent or a grandparent. The same pattern of results was found for the ICG > 30 criterion (Simon et al., 2011), χ2(4, N = 1,105) = 205.26, p < .001, but with a less prevalent endorsement of CG by about 10% for each type of kinship (see Fig. 1C and SM 3). In the revised model of prolonged grief disorder (Prigerson et al., 2009), yearning is considered as an inclusion criterion for the diagnosis of CG. Using this additional criterion (i.e., the score on the yearning item ≥ 3 [often or always]), the prevalence decreased (about 10% in spouse and parent loss groups, about 5% in child and sibling loss, whereas it did not vary in the grandparent loss group) and bereaved individuals who endorsed these criteria again differed significantly by kinship, χ2(4, N = 581) = 79.21, p < .001 (see Fig. 1D and SM 3). These results suggested that including the yearning criterion yielded more sensitive caseness identification and revealed prevalence rates closer to those found in the literature.
Specific grief reactions depending on kinship
To identify groups of grief reactions that best fit the current data set, two CFAs were performed and compared (see SM 4). First, all symptoms of CG were included in one factor, yielding poor fit statistics: root mean square error of approximation (RMSEA) = .089, χ2(152, N = 1,105) = 1483.61, p < .001, comparative fit index (CFI) = .866, Tucker-Lewis index (TLI) = .849, standardized root mean square residual (SRMR) = .056. Second, we tested the six-factor solution proposed by Simon et al. (2011): (a) yearning (Items 1, 4, 13, 16, and 19), (b) anger (Items 6 and 17), (c) shock (Items 3, 7, and 8), (d) estrangement from others (Items 9, 10, and 18), (e) hallucinations (Items 11, 14, and 15), and (f) behavior change (Items 2, 5, and 12). Item 11 (“I have pain in the same area of the body or have some of the same symptoms as the person who died”) did not have an adequate factor loading on Factor 5 and the modification index suggested including it in Factor 4 (estrangement from others). This six-factor model was supported by good fit statistics: RMSEA = .064, χ2(137, N = 1,105) = 753.11, p < .001, CFI = .938, TLI = .922, SRMR = .041.
Finally, a series of ANCOVAs and post hoc Bonferroni comparisons were performed on each factor to test if kinship explained specific symptom clusters differently (see Table 1). First, reactions of anger were more intense after child loss, followed by spouse and sibling, parent, and grandparent loss. Second, reactions of shock, yearning, and behavior change did not differ between child and spouse loss. Sibling or parent loss were not different from these two groups, but all were more present than after grandparent loss. Third, child and spouse loss did not differ in estrangement from others, but were significantly more intense than after sibling, parent, and grandparent loss. Finally, hallucinations were not different between child, spouse, sibling, and parent loss, but were more intense than in the grandparent loss group.
Discussion
The present investigation sheds light on an underinvestigated topic, the differential role of kinship in the profile of grief reactions. Our results suggest that not only CG intensity but also profiles of grief reactions significantly vary depending on KR. In line with previous studies, kinship was identified as a major predictor of CG intensity. It explained 19% of the variance of CG intensity. In comparison with the death of a parent or a grandparent, the loss of a child, but also of a spouse or a sibling, was associated with more intense CG symptoms and a higher prevalence of CG. Other classical predictors such as gender, circumstances of death, and time elapsed since loss together explained 13% of the remaining variance in the model. This indicates that kinship should be considered as a core variable in future CG models. We propose that kinship is a potential parsimonious explanatory variable because it represents an integration of major known risk factors of CG. Indeed, it is intrinsically related to (a) the loss event and its appraisals (e.g., expectedness, valence, importance), (b) biological (gender and age of the bereaved), (c) psychological (functions of and attachment to the deceased, identity, world views, meaning making, memory), and (d) cultural (representations of the family relationships and death) risk factors.
For the first time, a study proposed a multidimensional perspective applied to the distinctions between profiles of CG reactions according to kinship. The CFA results confirmed six clusters of grief reactions: anger, shock, yearning, estrangement from others, hallucinations, and behavior changes. Distinct profiles of grief were found for each kinship. First, the death of a child was significantly associated with more intense reactions of anger. This concurs with a study mainly comprising parents who had lost a child, in which hostility levels were identified as a significant predictor of CG intensity (Fernández-Alcántara, Pérez-Marfil, Catena-Martínez, Pérez-García, & Cruz-Quintana, 2016) and with qualitative studies that outline the central importance of anger after the loss of a child (e.g., Cacciatore, Erlandsson, & Radestad, 2013). Second, in contrast with other studies, grief reactions of shock, yearning, and behavior change had a similar pattern for participants who had lost a child, a spouse or a sibling. However, in Zetumer et al.’s (2015) study, the bereaved parents group was compared with a heterogeneous group including spouses and siblings together, whereas the current study made a specific distinction between them. In these KR, bereaved individuals are more likely to face family-level stressors in addition to individual ones (Stroebe & Schut, 2015). Also, they have usually shared a lot of time and life together in the same home and expect less to lose their family member than is the case for a parent or grandparent in adulthood. Third, estrangement from others was stronger after child and spouse loss than after sibling, parent, and grandparent loss, making the first two types of bereavement experiences comprise more loneliness and detachment or avoidance of others. Finally, our results indicated that hallucinations figuring the deceased may be less common after the death of a grandparent than other kinships. Post-bereavement hallucinatory experiences are common for those who lost a loved one, with an appearance rate that varies from 30% to 60% (Castelnovo, Cavallotti, Gambini, & Agostino, 2015). Such experiences were found to occur as a function of the emotional attachment to the deceased. In most cases, at least in Western culture, grandparents are not people’s main attachment figures, and this could explain why hallucinatory reactions are less prevalent among grandchildren. Another explanation relates to sensory and experiential memories that may be more frequent for members of the nuclear family. They usually share and spend more time together than might be the case with grandparents, thus leading to more frequent intrusive memories, vivid thoughts, images, and hallucinations of the lost person.
Limitations
The present study has several limitations. First, although the ICG has previously been employed as a diagnostic tool, clinical interviews should be used to confirm the accuracy of CG diagnosis. The ICG was found to overestimate the rate of CG by three times in comparison to other instruments (Maciejewski et al., 2016), probably leading, even with the most restrictive criteria, to nearly half the participants who had lost a child or a spouse to be positively screened for CG. It is possible that one should use even more stringent criteria in determining CG. Also, the ICG covers a range of grief reactions that does not include guilt or avoidance reactions, even if these are currently under discussion for inclusion in CG diagnosis. Second, the sample size of the sibling loss group was small, in comparison with the other four groups. Third, we did not examine possible processes through which kinship might influence grief reactions (e.g., meaning making, appraisals or coping strategies). Fourth, ICG scores were obtained from individual studies that used other instruments and had various objectives. This may have influenced participants’ responses. However, the ICG was always presented in a similar manner and an additional analysis considering the potential effect of the origin of the study and mode of recruitment offered the same pattern of results. Finally, our results need to be contextualized in Western individualistic culture. Further cross-cultural studies are needed because one can expect that bereaved people belonging to collectivistic cultures, where family structures and functions are different, should present different profiles of grief reactions according to KR.
Clinical implications
If further studies confirm the patterns found in this study, these results may provide meaningful guidance for clinicians involved in grief and end-of-life processes. Due to its high predictive value, kinship may be used along with other screening measures and risk factors of CG outcomes. Losing a child, a spouse, or a sibling may be seen as a risk factor of CG that deserves special attention from professional and social support systems. Intense feelings of anger could be considered less worrying in the case of bereaved parents, whereas hallucinatory experiences after the loss of a grandparent might be a possible indicator of CG. In conclusion, kinship relationship is an important and potentially parsimonious predictor of CG.
Footnotes
Acknowledgements
The authors wish to thank Pierre Gérain for his help in compiling the different data files. The authors are also grateful to A. Ancre, L. Coulange, E. Delespaux, S. De Paoli, N. Dessambre, E. Duchêne, L. Gauthier, A. Gosset, J. Laloo, V. Laloux, F. Lantreibecq, S. Molens, B. Peeters, A.-S. Ryckebosch-Dayez, I. Sievert, E. Vaessen, C. Van Achter, C. Van Der Beken, and J. Vercauteren who helped in data collection.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.