
Abstract
This commentary serves as a reply to Hoffart and Johnson’s article contending that psychodynamic psychotherapy (PDT) models cannot be examined with regard to mechanism of change or represent within-person causal relationships. Hoffart and Johnson cite purportedly paradigmatic examples of PDT and cognitive therapy and examine them with respect to Kazdin’s requirements for investigation of mechanisms of change. We highlight inaccuracies in Hoffart and Johnson’s representation of PDT and, in doing so, provide reasoning in support of the empirical examinability of PDT. We conclude by recommending a metatheoretical system (i.e., functionalism) and empirical methodologies that clinical scientists may consider when investigating mechanisms of PDT in the future.
Hoffart and Johnson (2017) discuss Leichsenring, Beutel, and Leibing’s (2007) supportive-expressive therapy (SET) and Clark and Wells’s (1995) cognitive therapy (CT) as purportedly paradigmatic examples of psychodynamic psychotherapy (PDT) and CT, respectively. Using Kazdin’s (2009) well-established requirements, they argue that mechanisms of change in PDT, in contrast to those in CT, cannot be submitted to empirical scrutiny. The distinctions that Hoffart and Johnson draw between CT and PDT, however, rest on four inaccurate assumptions: (a) PDT models do not involve bidirectional relationships among symptoms and between symptoms and core conflicts, (b) core conflicts are unobservable, (c) core conflicts are defined by their associated symptoms, and (d) core conflicts are static, prohibiting the examination of within-person variation.
Although we concur with Hoffart and Johnson that understanding the metatheoretical underpinnings of psychotherapy models is essential for the advancement of the psychotherapeutic project, we disagree with their contentions that PDT explanatory concepts cannot be empirically examined or represent within-person causal relationships between observable phenomena. We seek to (a) highlight the ways in which Hoffart and Johnson’s characterization of PDT is inaccurate, and in so doing provide reasoning in support of the empirical examinability of PDT explanatory concepts, and (b) recommend a theoretical system and empirical methodologies that researchers may consider when examining mechanisms of change of PDT.
Psychodynamic Models Are More Complex Than Portrayed
Hoffart and Johnson assert that in Leichsenring and colleagues’ (2007) SET (and therefore PDT) symptoms are relevant only as locally independent indicators of core conflicts, rather than as constituents of a larger syndrome that may have causal influence on core conflicts and other symptoms. Indeed, Leichsenring and colleagues write that “psychiatric symptoms are conceptualized in psychodynamic therapy as the consequence of unresolved conflicts or impairments in ego–function” (p. 59). Notably, there is no further mention about the nature of symptom relationships in social anxiety disorder (SAD).
PDT models of other anxiety disorders, including panic disorder (e.g., Shear, Cooper, Klerman, Busch, & Shapiro, 1993) and generalized anxiety disorder (GAD; e.g., Crits-Christoph, Crits-Christoph, Wolf-Palacio, Fichter, & Rudick, 1995), explicitly recognize the importance of causal relationships between symptoms and between symptoms and core conflicts. Thus, if it is Leichsenring and colleagues’ contention that in SET symptoms are not causally related, then their model is not representative of PDT models more broadly. For instance, influenced by Barlow’s earlier work, Shear and colleagues (1993) write,
Efforts to ignore the presence of negative affects may mean that somatic aspects of these affects become the focus of attention and the stimulus for conscious as well as unconscious cognitive catastrophizing. This begins a vicious cycle, well-described by cognitive psychologists of escalation of fear, physiological symptoms, more fear, and more physiological symptoms, culminating in a panic episode. (p. 862)
Moreover, in their PDT model of GAD, Crits-Christoph and colleagues (1995) write that “symptoms of GAD—for example somatic symptoms—can also be a defense response as well as simply a part of the physiology of the fear response” (p. 19). In both models, there is an interaction between symptoms and core conflicts; it is not necessarily the case that symptoms are epiphenomena caused by (perhaps unconscious) conflicts.
The causal relationships between symptoms in PDT date to the earliest days of psychodynamic thought. In a case study of Lanzer (referred to as Rat Man for deidentification), Freud (1909) writes, The same captain had handed him a packet that had arrived by the post and had said: “Lieutenant A. has paid the charges for you. You must pay him back.” The packet had contained the pince-nez that he had wired for. At that instant, however, a “sanction” had taken shape in his mind, namely, that he was not to pay back the money or it would happen. . . . And immediately, in accordance with a typical of procedure with which he was familiar, to combat this sanction there had arisen a command in the shape of a vow: “You must pay back the 3.80 crowns to Lieutenant A.” He had said these words to himself almost half aloud. (p. 168, italics added)
Freud provides an example of how a behavior (i.e., handing of a packet) influences the generation of a thought (i.e., not to pay the money back), which leads to another thought about planning behavior (i.e., paying back 3.80 crowns). Although Freud discusses how Lanzer’s obsessions and compulsions were influenced by his unconscious conflict between love and hatred, he also indicates that his symptoms were caused by other symptoms. Other case studies of Freud’s illustrate similar causal mechanisms (e.g., Little Hans; Freud, 1909). In psychodynamic thought, core conflicts can influence symptoms, symptoms can influence core conflicts, and symptoms can influence one another. The relative weight of these relationships is open to and worthy of empirical investigation.
PDT’s consideration for the causality between symptoms can also be seen in the process of free association, a bedrock of psychoanalytic process (Freud, 1916). The aim of free association is to examine, in real time, the manner in which patients’ observables are related. For example, Peter may tell his therapist about an episode at work when he spilled coffee, which leads him to state that he is anxious, and then to him asking to pause the session to use the bathroom. Although these symptoms are born of a common core conflict, they are causally related, each helping to generate the next observable in the associative chain.
Insofar as symptoms causally influence other symptoms and core conflicts, Hoffart and Johnson’s use of SET to represent PDT is insufficient, limiting the validity of their subsequent distinctions between PDT and CT (see Hoffart & Johnson, 2017, p. 1076). We do not believe that PDT fits as cleanly into the essentialist model as Hoffart and Johnson suggest. We have sought to depict this relationship in Figure 1, an altered version of the PDT model presented by Hoffart and Johnson.
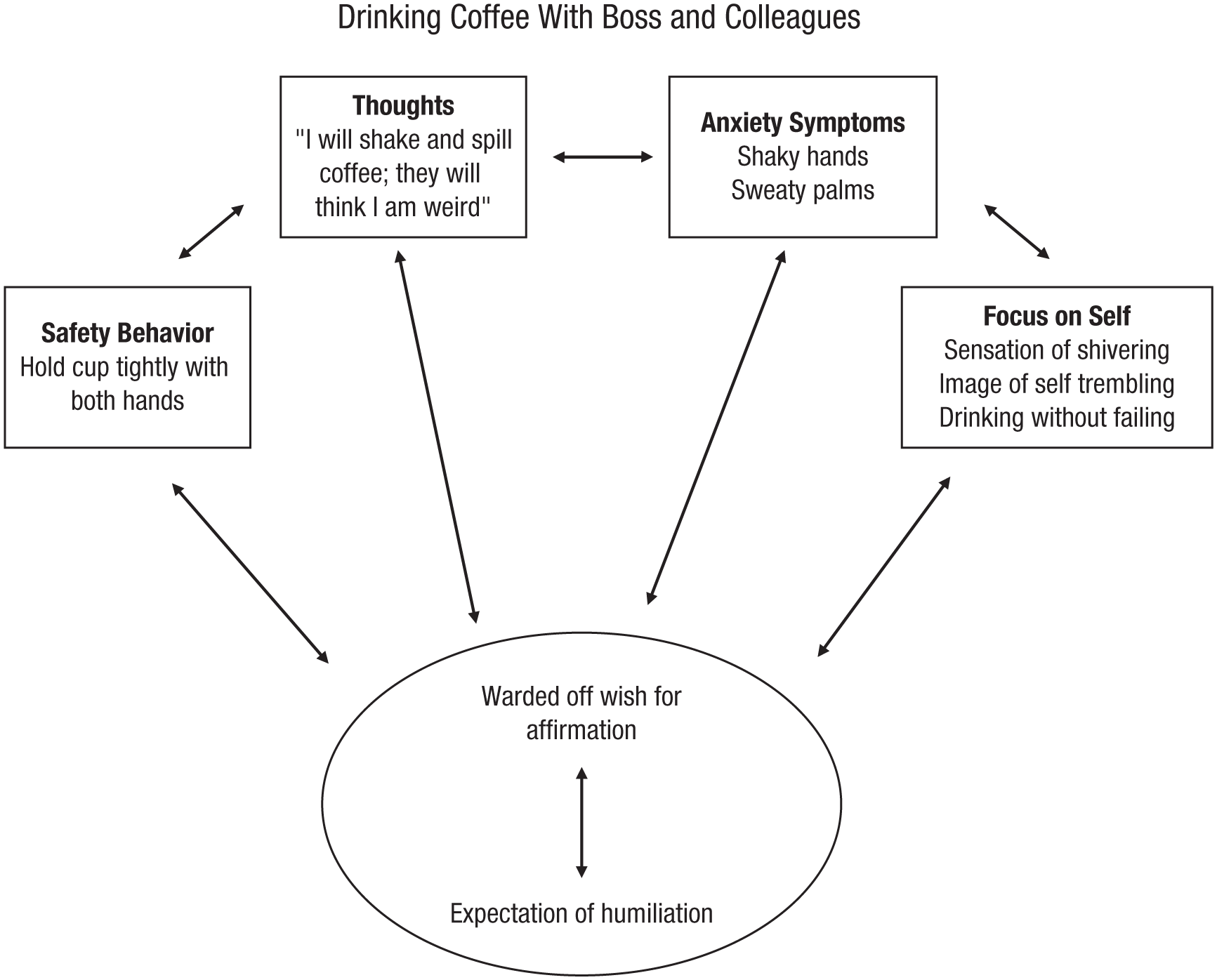
Revised model of psychodynamic psychotherapy. An internal conflict generates symptoms of social anxiety disorder and symptoms reinforce or detract from the magnitude of the conflict, symbolized by the bidirectional arrows between conflict and symptoms. Bidirectional arrows between symptoms depict causal relationships among them. Because of the transitive property, all symptoms may causally interact with one another (not explicitly shown).
Psychodynamic Explanatory Concepts Are Observable
Hoffart and Johnson base many of their arguments on the assertion that unconscious conflicts are not directly observable and are attributed to a patient only on the basis of the symptoms he or she expresses. In contrast, they assert that constructs in Clark and Wells’s (1995) CT model are observable, meaning that they can be “rather unambiguously identified, either by introspection or by behavioral observation” (pp. 1072). It is important that they note that introspection is a valid method of observation, citing Ericsson and Simon’s (1980) work on the importance of directed attention in the processing of internal experience. In short, if a phenomenon is introspectable, it is observable. 1
At the heart of psychodynamic theory is the notion that unconscious conflicts can be made conscious if one’s attention is directed appropriately. The aim of bringing unconscious material into consciousness so that it can be examined, worked through, and ultimately resolved originated with Freud (1914) and is supported by contemporary science. For instance, Fox and colleagues (2012) demonstrated that expert meditators practicing insight-oriented meditation showed significantly higher introspective accuracy than novices during a body scan exercise. In addition, deficits in interoceptive awareness in depressed patients resolved following mindfulness training (Fissler et al., 2016). Research also suggests that when material is brought into awareness it can be modified. For example, consolidated memories become labile when reactivated, allowing them to be reconsolidated (Tronson & Taylor, 2007). Nader, Schafe, and Le Doux (2000) demonstrated that inhibition of protein synthesis in the amygdala following retrieval of a consolidated memory led to amnesia for the retrieved memory, but not for consolidated memories that were not retrieved.
CT is similar to PDT in its acknowledgment that internal experience is not always immediately observable. For example, in their well-recognized cognitive treatment of SAD, Hope, Heimberg, and Turk (2010) describe the process of identifying core beliefs: “Even though the layers underneath have always been there, you may not be able to see them until you remove the outer layers” (p. 207). They compare this process to the discovery of automatic thoughts (ATs): “As you have been conducting the exposures and challenging your ATs, you have probably discovered some ATs that you did not know about at first” (p. 207). Patients are often unable to observe these internal phenomena at the beginning of treatment; one goal of therapy is to learn to identify ATs and core beliefs in order to work with them. In this way, core beliefs parallel unconscious conflicts in PDT.
Models of CT that construe ATs as functions of core beliefs are similar to models of PDT that consider thoughts as functions of core conflicts. However, in clinical practice, these aspects are given varying emphases. PDT places greater emphasis on the treatment of core conflicts (rather than symptoms), whereas CT places greater emphasis on the treatment of symptoms (rather than core beliefs). However, the theoretical underpinnings of these models are more alike than they are dissimilar.
Furthermore, although introspection is sufficient to observe and study core conflicts, it is not the only mechanism for observing unconscious content. The Implicit Association Test (Greenwald, McGhee, & Schwartz, 1998) can identify biases outside of conscious awareness that conflict with self-report. For example, differences between self-reported and implicit self-esteem were found among a socially anxious sample (de Jong, 2002). In addition, fMRI studies have begun to reveal the neural correlates of unconscious processing. Using a backward-masking paradigm, Lamy, Salti, and Bar-Haim (2009) compared event-related potentials for circumstances in which participants were and were not subjectively aware of the stimulus. In another study, Jiang, Bailey, Xiang, Zhang, and Zhang (2016) provided evidence for quantitative difference in the neural substrates of conscious versus unconscious control.
The introspectable nature of core conflicts problematizes Hoffart and Johnson’s claim that these conflicts are observable only via symptoms. Unconscious core conflicts can be identified and brought into consciousness, permitting the time ordering of PDT mechanisms and outcomes.
Psychodynamic Mechanisms Are Not Tautological
Hoffart and Johnson’s claim that PDT does not meet Kazdin’s (2009) third, fourth, and fifth criteria follows from their argument that it does not meet the second criterion: a strong association between the proposed mechanism (core conflict) and therapeutic change. They claim that wishes and fears (i.e., components of core conflicts) are “defined by certain behaviors in particular circumstances” (p. 1078). Hoffart and Johnson argue that because denying the relation between core conflicts and symptoms is a logical contradiction (insofar as it would deny a definition), the relationship between the two is not falsifiable and therefore cannot be empirically established.
For one concept to define another, there must be a tautological relationship between the definiendum and definiens—each must be necessary and sufficient for the other. A paradigmatic example is the bachelor and unmarried male; being an unmarried male is necessary for being a bachelor (no bachelor is married) and sufficient for being a bachelor (every unmarried male is a bachelor). The same holds in the opposite direction. Thus, if one shows that certain SAD symptoms are neither necessary nor sufficient for a particular core conflict, one has rebutted the authors’ argument as the denial of the relationship between a core conflict and symptoms would not be a logical contradiction.
Consider the imagined case of Smith who suffers from SAD. One of Smith’s core conflicts is between his wish for others to consider him clever and his fear that others consider him dull. If Hoffart and Johnson’s claim is true, then one can move a priori from Smith’s conflict to Smith’s symptoms and vice versa. Yet, the exact compromises between his wish and fear do not follow strictly from the definitions of wish and fear and the conflict between the two. For instance, Smith may produce a number of art objects, which he litters in the vicinity of those who he wishes would consider him clever. From observing this behavior, one could not immediately infer that Smith had this particular core conflict, thus showing that the behavior is not sufficient. Nor could one conclude another individual did not have SAD on the basis of his not exhibiting art object littering, thus showing that the behavior is not necessary. Because this behavior is neither necessary nor sufficient, its relationship to the core conflict is not definitional.
The nondefinitional nature of the relationship between core conflicts and symptoms in PDT is further illustrated by the imagined case of Laura. Laura has symptoms A to Z and core conflict “C.” Laura participates in PDT for SAD and, via a relationship episode interview, indicates a resolution of C by a reduction in verbal expressions (i.e., verbal behavior) consistent with C. Laura’s symptoms A to W also remit. One plausible reading of this is that symptoms X, Y, and Z were not caused by C, and thus were not symptoms of Laura’s particular manifestation of SAD. Crucially, this is revealed a posteriori over the course of PDT. Whether a symptom of SAD is a result of a core conflict is revealed during therapy, and cannot be decided prior to investigation. Hoffart and Johnson are correct to state that tautological relationships between mechanisms and therapeutic change do not permit empirical examination; however, they incorrectly assert that core conflicts are defined by symptoms in PDT.
Within-Person Relationships Are Measurable in Psychodynamic Models
Hoffart and Johnson assert that psychodynamic models do not permit the examination of within-person change. Core conflicts, they contend, are static insofar as they do not change and cannot be used to model changes in symptom expression. However, given our arguments that (a) PDT accounts for causal relationships among symptoms and between core conflicts and symptoms, (b) explanatory concepts of PDT are observable, and (c) the relationship between PDT mechanisms and symptoms is not tautological, it follows that within-subjects examination of PDT mechanisms is possible.
Furthermore, PDT is not committed to the idea that core conflicts must be static. Although core conflicts may influence symptoms (and are also influenced by symptoms), they exist in context. The strength and saliency of core conflicts may change depending on whether an individual is in a particularly threat-salient environment or whether this individual has undergone therapy, for example. Similarly, a person may always carry an HIV diagnosis, but may also undergo changes in his or her viral load contingent on a host of contextual factors (e.g., medication compliance, other viral infections). Given points a to c detailed earlier and that core conflicts are not necessarily static, within-person changes are determinable.
Mental States as Behavioral Dispositions: A Functionalist Perspective
One possible reason for Hoffart and Johnson’s claim that the relationship between a core conflict and symptoms is definitional is their reliance on an overly narrow way of understanding mental states. The authors claim that one must understand specific mental states as definitionally related to specific behavior types, unless one is willing to accept a form of Cartesianism, in which mental states are essentially private affairs (p. 1079). They rightly reject the Cartesian view, but fail to consider alternative ways of understanding mental states.
For instance, functionalists (e.g., Armstrong, 1980) argue that mental states are dispositions to behave in certain ways when specific circumstances arise. For Armstrong, the full inventory of behavioral manifestations and the conditions that would lead to them are not specified by the theory but are left open to specification via empirical investigation.
In the context of PDT for SAD, functionalists would treat core conflicts as dispositions for symptoms of SAD. These behaviors and the contexts that elicit them would be uncovered by examining situations that involved display of paradigmatic symptom behavior (e.g., verbal expressions of anxiety, avoidance). A therapist would probe the patient about those situations, assessing whether the context caused distress or avoidance—indeed, this is the procedure in the empirically based Anxiety Disorders Interview Schedule (Brown & Barlow, 2013). A therapist-patient pair may examine conditions for the manifestation of symptoms by considering contexts in which symptoms occur. During the investigation, the symptoms and the conditions in which they manifest may turn out to be idiosyncratic, consistent with research on latent symptom classes of SAD (Potter, Drabick, & Heimberg, 2014). Functionalism may be one metatheoretical system by which to consider mechanisms of change in PDT.
Recommendations for Empirical Directions for PDT
Research supports the foundational assertions of contemporary psychodynamic theory and practice (see Solms, 2017), and functionalism may offer a useful theoretical architecture for PDT. However, further investigation is needed to clarify specific mechanisms of change. Use of emerging technologies, methods, and statistical practices may help identify unconscious content. Implicit associations, subliminal perceptions, and functional neurological correlates will be essential in furthering our scientific understanding of PDT. Statistical approaches such as time-varying effects models (Molenaar & Campbell, 2009) can probe intraindividual change and account for lived-experiences over time. These models may be useful in elucidating the interconnectedness between core conflicts and symptoms as a function of experiences, such as psychotherapeutic intervention.
Finally, given our belief that PDT and CT models are more alike than they are dissimilar (despite differences in clinical practice), future research should directly compare, via empirical investigation, the hypothesized mechanisms of change in these models. The identification of important similarities and differences between models could have important implications for treatment process and outcome.
Conclusions
Empirical research pertaining to PDT mechanisms lags behind CT. We have sought to demonstrate that this is an issue of empirical inquiry in practice rather than in principle. Psychodynamic models consist of the type of causal relationships between observable variables that are necessary for empirical investigation, meeting all standards put forth by Kazdin (2009). Thus, both CT and PDT models can lead to testable predictions and knowledge accumulation.
Footnotes
Author Contributions
J. N. Cohen coordinated the project and was responsible for the sections concerning the representation of psychodynamic psychotherapy and the subsequent comparisons with cognitive behavioral therapy. R. McElhaney was responsible for sections pertaining to metatheoretical concerns. D. Jensen was responsible for sections concerning the observable nature of psychodynamic concepts. All the authors contributed to idea generation and provided revisions. All the authors approved the final version of the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.