
Abstract
The experience of pain during nonsuicidal self-injury (NSSI) remains enigmatic. Ultimately, there is a dearth of evidence regarding whether pain is actually experienced during NSSI behavior and, if it is, to what extent that pain offsets following cessation of the NSSI episode. Using a smartphone app to collect information on self-injury episodes reported by adolescents and young adults in their daily lives, we found that across 143 NSSI episodes comprising 442 NSSI behaviors, most participants reported feeling significant and substantial pain onset during most NSSI episodes. A small effect was established for pain offset, with pain diminishing somewhat for most at NSSI completion. Furthermore, those who had higher negative emotion at the start of NSSI episodes but experienced less pain onset reported more NSSI behaviors during such episodes. The evidence supports a dynamic experience of pain during self-injury that can vary between people and episodes.
After I cut myself . . . it starts to hurt a little bit . . . and then I focus on that because it hurts.
Elucidating the role of pain during nonsuicidal self-injury (NSSI) is one of the most perplexing challenges faced by modern mental health researchers and clinicians. NSSI, which refers to the deliberate and direct destruction of bodily tissue without lethal intent (Nock, 2010), is closely linked to future suicidal behavior (Guan, Fox, & Prinstein, 2012) and represents a serious enough health concern that it is currently under consideration for inclusion as a future diagnostic entity (Selby, Kranzler, Fehling, & Panza, 2015). Despite the growing research attention to NSSI, the functional nature of the behavior is complex (Bentley, Nock, & Barlow, 2014). NSSI can be difficult for clinicians and families to understand because the behavior challenges our assumption that people generally strive to avoid or minimize experiences of pain. Contrary to this general principle, people who engage in NSSI intentionally and repeatedly inflict physical injury on their bodies despite, or perhaps because of, the physical pain it elicits.
It is therefore critical to understand the way pain is experienced during NSSI and the role pain may play in reinforcing the behavior. Yet despite the centrality of this question, existing research has revealed inconsistent and seemingly conflicting models of pain in NSSI. In some studies, self-injurers have denied experiencing pain during NSSI, leading some to conclude that those who engage in NSSI may naturally have or develop reduced pain perception and therefore actually experience these behaviors as less painful than those who do not regularly engage in NSSI. According to this model, pain may not pose a barrier to engaging in NSSI because NSSI is not experienced as painful. In contrast, other studies have found that the physical pain elicited by NSSI may have paradoxically positive effects by helping self-injurers escape from emotional pain (Chapman, Gratz, & Brown, 2006; Nock & Prinstein, 2004). According to this model, physical pain is not only tolerated but may be intentionally elicited as the primary purpose of engaging in NSSI. These different conceptualizations of the role of pain in NSSI have important implications for the treatment of NSSI and therefore represent a critical area for further clarification. To date, empirical studies have provided support for different models of pain, and it remains unclear whether these disparate findings are the result of methodological weaknesses or whether they reflect the reality that pain is experienced in a plurality of different and even seemingly opposing ways by different self-injurers at different times. The goal of the current study was to use experience sampling methodology (also referred to as ecological momentary assessment) to examine evidence for three of the most commonly discussed models of pain in NSSI and the way each may contribute to our understanding of why people self-injure.
The three models of pain during NSSI that have been most clearly documented include: (a) a pain analgesia effect (Schmahl et al., 2006), in which little or no pain is reported during NSSI or NSSI experimental proxies; (b) a pain onset effect (Chapman et al., 2006; Selby & Joiner, 2009; Selby, Nock, & Kranzler, 2014), in which pain is elicited by NSSI with the potential purpose of distracting from upsetting thoughts or emotions; and (c) a pain offset effect (Franklin et al., 2010; Franklin, Lee, et al., 2013; Franklin, Puzia, et al., 2013), in which pain quickly offsets following the cessation of NSSI behavior, resulting in concomitant feelings of relief due to fading sensations of pain. Each of these models of pain during NSSI is elaborated in further detail in the following, as are their concordant limits in empirical investigation, followed by discussion of the role of negative emotion as a moderator of pain and self-injury experiences.
Pain Analgesia During Self-Injury
Some of the earliest studies of pain in NSSI uncovered the possibility that some participants experience a pain analgesia effect. For example, Russ et al. (1992) found that self-injurers who reported feeling no pain during NSSI also reported lower ratings of pain during a cold pressor task than self-injurers who did feel pain during NSSI. Additional experimental studies then found evidence for specific psychological and biological characteristics among those who report pain analgesia during self-injury (Kemperman et al., 1997; Russ et al., 1996). More recently, in an adolescent psychiatric sample, self-report data showed that 47% of those who self-injured reported experiencing no pain at all during the behavior (Nock, Joiner, Gordon, Lloyd-Richardson, & Prinstein, 2006).
The pain analgesia models of NSSI are still understudied, and the reason for this analgesia effect is not understood. It may be that diminished pain perception leads to increased risk for developing NSSI behavior, since more recent research indicates that those who self-injure regularly are more likely to exhibit higher pain thresholds and endure pain longer (Bohus et al., 2000; Glenn, Michel, Franklin, Hooley, & Nock, 2014; Hooley, Ho, Slater, & Lockshin, 2010). Alternatively, it is possible that pain perception may change as a function of self-injury, with repeated self-injury leading to habituation to pain over time (Glenn et al., 2014). Supporting this latter possibility is the finding that reductions in the experience of pain during NSSI have been linked to length of NSSI history (Claes, Vandereycken, & Vertommen, 2006). Another potential explanation for pain analgesia during NSSI is the release of endorphins, endogenous opioids that reduce pain (Bresin & Gordon, 2013). However, research has not consistently identified opiates’ role in the onset or potential treatment of NSSI (Russ, Roth, Kakuma, Harrison, & Hull, 1994). Furthermore, a number of studies indicate that many if not most of those who self-injure do experience pain during the NSSI. In one study of adolescents, for example, although about half of those who self-injured reported feeling no pain during NSSI, the other half experienced at least some pain during NSSI (Nock et al., 2006); and in another study, more severe self-injurers were more likely to report more pain during NSSI (Lloyd-Richardson, Perrine, Dierker, & Kelley, 2007). A study using experience sampling methods found that 24% of adolescent self-injurers reported engaging in NSSI specifically to feel pain (Selby et al., 2014). However, most previous studies of the pain analgesia model have been restricted to retrospective self-report or experimental investigation using NSSI proxies, and it remains unclear how pain is actually perceived in real time during NSSI behaviors. Thus, there appears to be initial support for a pain analgesia model of NSSI, but pain analgesia is unlikely to be a characteristic representative of all or most self-injurers.
Pain Onset During Self-Injury
The second category of experiences of pain during NSSI is referred to in this article as pain onset models, although these models previously have not been classified as such. We have categorized them accordingly here because such models explicitly state or imply that pain is elicited by self-injury and that this pain has counterintuitively desired effects in that physical pain may lead to distraction from and reduction in emotional pain. A vast array of literature supports the notion that most self-injurers report engaging in NSSI specifically to reduce feelings of emotional distress (Bentley et al., 2014; Klonsky, 2007). Experience sampling data also support this effect, with participants reporting significant decreases in negative emotion immediately following NSSI (Kranzler et al., 2018). Although the specific mechanism through which NSSI reduces negative emotion is still not clear, we can conclude that a large portion of those who self-injure feel pain during NSSI (Nock et al., 2006; Selby et al., 2014) and may even do so specifically to feel pain (Laye-Gindhu & Schonert-Reichl, 2005). Indeed, one self-injuring patient explained synchronous feelings of physical pain and relaxation during NSSI: “Right after I hurt myself, I felt physical pain, but my mind and body were much more at ease than before” (Leibenluft, Gardner, & Cowdry, 1987, p. 320). Ultimately, such pain may negatively reinforce NSSI by reducing negative emotion through distraction (Chapman et al., 2006), potentially increasing the frequency of the behavior.
Building on this notion, multiple models of NSSI have posited or implied that self-injury may result in negative reinforcement of NSSI by reducing negative emotion via distraction, potentially through physical pain or potential opioid release (Armey, Crowther, & Miller, 2011; Chapman et al., 2006; Muehlenkamp et al., 2009). One model in particular, the emotional cascade model (ECM; Selby, Anestis, Bender, & Joiner, 2009; Selby & Joiner, 2009), has identified pain onset as playing an essential role in facilitating the negative reinforcement of NSSI by reducing negative emotion. The ECM proposes that NSSI is used specifically to distract from self-perpetuating and progressively intensifying cycles of distressing thoughts, rumination, and negative emotion and that the pain elicited by NSSI is a potent physical sensation that allows an individual to short-circuit an emotional cascade, thus diminishing negative emotion and negatively reinforcing the self-injurious behavior. Importantly, rumination and emotional cascades have been cross-sectionally and prospectively linked to NSSI behavior (Selby, Franklin, Carson-Wong, & Rizvi, 2013; Selby & Joiner, 2013; Tuna and Bozo, 2014). One study that enacted thermal pain during a negative emotion induction with self-injuring participants found that greater experiences of pain during the task resulted in greater reductions in negative affect (Bresin & Gordon, 2013). Thus, initial research supports the possibility that pain elicited by NSSI may contribute to the paradoxical effects of the behavior by contributing to distraction from emotional distress. However, to date, no studies have used ecologically valid methodology to demonstrate that pain increases during NSSI behavior or investigated whether magnitude of pain onset predicts frequency of NSSI behavior.
Pain Offset After Self-Injury
The third and most recently suggested model of pain experiences during NSSI suggests that those who self-injure may experience a sense of relief during the offset of pain following NSSI completion, otherwise known as pain-offset relief (Franklin, Lee, et al., 2013). In this model, it is not the pain itself that has an emotion regulatory effect but rather the subsequent subsiding of the pain. The exploration into the role of pain-offset relief in NSSI was spurred by findings that many people report experiencing relief or pleasantness when pain is removed (Leknes, Brooks, Wiech, & Tracey, 2008). According to this model, pain offset is a normative experience, wherein because of the high overlap between physical and emotional pain, the removal of one form of pain offsets or reduces the other. Self-injurers do not differ from non-self-injurers in their experience of this phenomenon but rather in their intentional engagement in physically painful behaviors to access this effect. The emotional relief associated with pain offset is then thought to positively reinforce NSSI behavior (rather than negatively reinforce it by removing a previous aversive emotional state, as conceptualized in the pain onset models).
In a seminal study with self-injuring participants, Franklin, Puzia, et al. (2013) found that after painful shocks, self-injuring participants demonstrated simultaneous decreases in physiologically indexed negative affect as well as increases in physiologically indexed positive affect (i.e., relief). Additional experimental psychophysiological evidence with self-injuring participants also supports the notion that positive emotion may increase after NSSI (Franklin et al., 2010), as does experience sampling data demonstrating increases in positive emotion after NSSI (Kranzler et al., 2018). Both findings may potentially be a function of pain offset. Accordingly, there appears to be growing evidence that the removal of the painful stimulus following NSSI results in both a reduction in pain and an increase in associated relief. However, few studies have specifically examined pain offset following NSSI or investigated whether magnitude of pain offset predicts frequency of NSSI behavior.
Negative Emotion as a Moderator of Pain Onset, Offset, and Self-Injury Frequency
Both pain onset and pain offset models posit that experiences of pain associated with NSSI may reinforce the behavior by serving emotion regulation functions. Thus, the impact of both pain onset and pain offset on NSSI frequency may be moderated by an individual’s level of emotional distress. NSSI has been associated with “negative emotional instability,” which refers to an individual’s tendency to experience frequent and intense fluctuations in negative emotional distress. Using experience sampling data with a behaviorally dysregulated group, Selby and colleagues (2013) demonstrated that negative emotional instability during experience sampling significantly predicted more NSSI behaviors during the study above and beyond main effects for elevated negative emotion. This indicates that an episode of NSSI may be particularly likely to occur in the context of acutely intense rises in negative emotions, as opposed to in the context of chronic elevations in negative emotion (as might be seen in major depression). In line with this possibility, previous experience sampling studies have found that momentary negative emotion increases in the time leading up to episodes of NSSI (Armey et al., 2011; Muehlenkamp et al., 2009).
In addition to impacting the number of episodes of NSSI a person initiates, negative emotionality may also impact the number of self-injurious acts (i.e., number of cuts) a person initiates within a single NSSI episode. This distinction is important; many episodes of NSSI comprise multiple different self-injurious behaviors (Horrocks, Price, House, & Owens, 2003). In the context of elevated emotion, when there is a greater need for emotional regulation, there may also be a need for higher levels of pain onset and/or pain offset to provide sufficient emotion regulation. Thus, individuals may engage in a greater number of self-injurious behaviors within a NSSI episode when they are experiencing momentary elevations in negative emotion. However, to date, little research has examined predictors of the number of NSSI behaviors within an NSSI episode.
The Current Study
Existing studies have been limited in their ability to assess the dynamics of pain. Most have used cross-sectional self-report methods, which are limited by recall biases and are unable to assess pain experiences in real time. Other studies have utilized experimental laboratory protocols and made significant advances in our understanding of the behavior; however, for ethical reasons, these studies have used NSSI proxies or images rather than actual NSSI behaviors. Experience sampling methods improve ecological validity by allowing for the examination of pain during experiences of NSSI in real time in natural settings. Although studies have begun to use experience sampling to examine experiences of NSSI (e.g., Kranzler et al., 2018; Nock, Prinstein, & Sterba, 2009), only one study to date has used this methodology to examine the role of pain during NSSI (Selby et al., 2014). Though this study of adolescent self-injurers provided an important contribution, it was still limited in that participants only reported whether eliciting pain was a primary motivation for NSSI, and dynamic fluctuations in pain during and after self-injury were not examined. In the current study, we utilized experience sampling with a sample of actively self-injuring adolescents and young adults, who reported on NSSI and pain in their daily life over a 2-week period of time, to examine the dynamics of pain before, during, and after NSSI was experienced in real time. By examining how pain changed at each report of NSSI for each individual, we aimed to provide a more direct, granular, and ecologically valid examination of the three models of pain previously discussed.
Study hypotheses
Although pain analgesia, pain onset, and pain offset hypotheses may initially appear to be competing models, in reality, most self-injurers report multiple motivations and functions of the behavior (Bentley et al., 2014). It is likely that all three models depict true experiences of pain during NSSI. For example, pain onset and pain offset experiences may both occur (with pain potentially increasing during NSSI and then decreasing following the behavior), providing both positive and negative reinforcement for the behavior. Similarly, pain analgesia may be experienced by some self-injurers some of the time. For example, self-injurers may not experience pain analgesia with their initial NSSI but develop it later because of habituation to pain that increases with more frequent NSSI (Claes et al., 2006; Glenn et al., 2014; Selby, Connell, & Joiner, 2010). Thus, rather than attempting to identify one universal model of pain in NSSI, it may be most accurate and clinically useful to examine the potentially overlapping experiences of all three models and the way each predicts the frequency of NSSI behaviors. Furthermore, given that the latter two models both suggest that either the onset or offset of pain functions to regulate emotional distress, we expect that varying levels of negative emotionality may moderate the extent to which pain reinforces NSSI. Therefore, we specified the following hypotheses:
Pain analgesia during self-injury. Hypothesis 1a: Multiple participants would report multiple NSSI episodes in which they feel no pain, and participants who retrospectively reported feeling no pain during NSSI at baseline would be more likely to experience no pain during NSSI reported during experience sampling, as evidenced by no increase in pain ratings from before to during NSSI. Hypothesis 1b: Participants who reported at least one experience sampling NSSI episode with no pain onset would report increased frequency of NSSI episodes, and NSSI episodes in which no pain was experienced would be characterized by more NSSI behaviors during the episode, potentially because the absence of pain would allow them to continue self-injuring.
Pain onset during self-injury. Hypothesis 2a: During NSSI, most participants would experience pain onset, as evidenced by a significant increase in pain from before to during NSSI. Hypothesis 2b: Those participants experiencing larger average increases in pain during NSSI (e.g., more pain onset) would report more frequent NSSI episodes and behaviors during experience sampling, suggesting that the behavior is being negatively reinforced, consistent with emotion regulation models of NSSI.
Pain offset after self-injury. Hypothesis 3a: After NSSI, most participants would experience pain offset, as evidenced by a significant decrease in pain from during to after NSSI was completed. Hypothesis 3b: Participants who experienced larger average decreases in pain after NSSI (e.g., more pain offset) would report more frequent NSSI episodes and behaviors during experience sampling, suggesting that the behavior is being positively reinforced, consistent with pain offset relief models of NSSI.
Negative emotion and pain onset and offset during self-injury. Hypotheses 4a and 4b: Negative emotion would moderate pain experiences during and/or after NSSI such that participants who experienced more frequent and intense fluctuations in negative emotion during experience sampling (negative emotion instability) and experienced either higher average pain onset (Hypothesis 4a) during NSSI or higher average pain offset (Hypothesis 4b) after NSSI would report more frequent NSSI episodes. Hypotheses 4c and 4d: During experience sampling, participants who reported experiencing elevated negative emotion prior to NSSI but who experienced less pain onset during NSSI (Hypothesis 4c) or less pain offset (Hypothesis 4d) after NSSI would report a greater number of NSSI behaviors (e.g., more cuts, burns) during such episodes of NSSI, potentially in an effort to elicit more pain.
Method
Participants
Participants consisted of a community-based sample of 47 self-injuring adolescents and young adults (age range = 15–21 years, M = 19.07, SD = 1.77). Participants were recruited by seeking referrals from local treatment centers and through flyers and print/online advertisements. Inclusion criteria for participation required that participants be aged 15 to 21 years and have engaged in NSSI behavior at least twice over the past 2 weeks. Recent and frequent self-injury was necessary to ensure that some participants reported self-injuring during monitoring period. Participants were excluded if they (a) were non-English speaking, (b) were determined to be at severe or extreme risk for suicide during our baseline assessment, or (c) had received a diagnosis of a schizophrenia spectrum disorder, psychotic disorder, life-threatening anorexia, or developmental delays.
Of the final sample, 68.1% (n = 32) were female, 29.8% were male (n = 14), and 1 participant identified as transgender. In terms of race/ethnicity, the sample was quite diverse, with 38.3% of the sample (n = 18) self-identifying as White, 14.9% as African American (n = 7), 19.1% as Asian (n = 9), 17.0% as Hispanic/Latino (n = 8), and 10.6% as multiracial (n = 5). In terms of sexual orientation, 66.0% (n = 31) identified as heterosexual, 17.0% identified as bisexual (n = 8), 6.4% identified as gay/lesbian (n = 3), 6.4% (n = 3) identified as other (e.g., pansexual), and 4.3% (n = 2) did not wish to report their sexual orientation. Household income ranged from under $9,999 (14.9%) to $150,000 and over (6.4%). All participants provided written informed consent to participate in the study. For participants younger than 18 years, both participant assent and parental consent were obtained. This study was approved by the Rutgers University Institutional Review Board (Protocol No. 14-185Rc).
Procedure
Phone screen
Referrals, flyers, and online advertisements instructed interested participants to contact the research project personnel via e-mail. Project personnel then spoke by phone with interested participants to describe the study and conduct prescreening procedures. For participants under the age of 18, project personnel asked to speak with a parent or legal guardian to receive verbal consent before asking any questions or providing any additional information. Prescreening consisted of a brief set of questions regarding NSSI and exclusion criteria. NSSI was defined to potential participants as “behaviors intentionally meant to cause damage to your own body that you engaged in without intent to die.” Participants meeting eligibility criteria at this time were scheduled for an in-person baseline assessment.
Baseline visit
Following the consent process, eligible participants completed a 2-hr baseline session, which consisted of semi-structured clinical diagnostic interviews, self-report measures, and training in the use of our smartphone app (Track It!). As part of this training, the definitions of NSSI and all terms used in the Track It! assessment were explained to participants. Participants were also provided with a user “cheat sheet,” which included directions for the use of the app and definitions of key terms used in the assessment, as well as the contact information of study personnel in case they encountered any difficulties.
Experience sampling protocol
The Track It! phone app was designed specifically for this study and created for the Android KitKat platform in conjunction with computer engineering specialists (J. Lindqvist). The app was programmed to employ both signal-contingent and event-contingent assessments. Signal-contingent entries prompted participants to complete assessments five times throughout the day in response to alarms they received through the app. These alarms were designed to signal participants at random times within five predetermined time intervals: 9:00 a.m. to 11:30 a.m., 11:30 a.m. to 2:00 p.m., 2:00 p.m. to 4:30 p.m., 4:30 p.m. to 7:00 p.m., and 7:00 p.m. to 9:00 p.m. Participants had 1 hr to complete these assessments. For event-contingent assessments, participants were asked to complete an assessment after engaging in any NSSI behaviors. Entries took approximately 3 to 7 min to complete. Data were transmitted via Wi-Fi and stored on a remote server managed by the investigative team using Transport Layer Security (TLS), the same protocol used in online banking. Participants were also encouraged to lock their phones with passcodes. Following their baseline visit, participants used the app for 2 practice days, followed by a 2-week monitoring period, which is standard protocol for experience sampling (Shiffman, Stone, & Hufford, 2008). Data from practice days were not utilized in our analyses. All participants were compensated $150 for completion of the 2-week monitoring period, and to ensure strong compliance with the experience sampling protocol, participants who completed at least 80% of the random prompted entries received a compensation bonus of an additional $150.
Measures
Baseline visit
Lifetime self-injury
The Inventory of Statements About Self-Injury (ISAS; Klonsky & Glenn, 2009) is a self-report measure of the frequency and functions of NSSI. The first section of the ISAS assesses the lifetime frequency of 12 different methods of NSSI. These items were added together to generate a count variable for lifetime frequency of self-injury. The ISAS also asks a number of questions about motivations for and experiences during NSSI, including whether one typically experiences pain during NSSI or not (rated yes, sometimes, or no)—which was used to investigate the experience of pain analgesia during NSSI.
Experience sampling protocol
Self-injury assessment
At each momentary assessment, participants were asked separately about whether they had any thoughts to self-injure and whether they had engaged in any NSSI behaviors since the last assessment. If participants responded in the affirmative to NSSI behavior (indicating that an NSSI episode had occurred), they were then asked to report the frequency of this behavior during the episode (“How many times did you engage in self-injury?”). Thus, participants could report multiple NSSI behaviors during a single NSSI episode. They also were asked to rate the duration of NSSI episodes from 1 (less than 5 s), 2 (less than a minute), 3 (1–30 min), 4 (30–60 min), to 5 (1–5 hr). Finally, participants were asked to select from a list of methods of NSSI that occurred during the episode (including cutting, biting, punching self/wall/object, scratching, getting into a physical fight in order to get hurt, burning, pulling hair out, banging head, hitting myself with object, or other).
Physical pain and self-injury
If participants reported having engaged in NSSI at any monitoring assessment, they were asked to report on the experience of “physical pain” before, during, and after the NSSI episode (rather than for each individual NSSI behavior reported during that NSSI episode). Participants rated pain on a visual analog sliding scale that ranged from 0 (no pain) to 10 (extremely painful), following the general methodology of medical pain assessment studies (Hawker, Mian, Kendzerska, & French, 2011). Within-person variance to error ratios were used, and the pain ratings demonstrated a high degree of reliability across participants and days of recording in this sample (Rkf = .85; Cranford et al., 2006). For individual NSSI reports, pain ratings before NSSI were significantly correlated with pain during (r = .19, p < .05) and after NSSI (r = .36, p < .001), and pain during NSSI was significantly correlated with pain after NSSI (r = .64, p < .001).
Negative emotion assessment
During each momentary assessment, participants were first asked to rate the extent to which they were feeling each of 21 emotions “right now” using a 10-point scale ranging from 0 (not at all) to 10 (extremely). Emotions were chosen for momentary assessment based on Klonsky’s (2009) findings of the most commonly endorsed positive and negative emotions experienced immediately before and after NSSI. In the current study, however, we only examined negative emotion items. Negative emotions included: overwhelmed, sad, frustrated, angry, hurt emotionally/rejected, anxious/afraid, lonely, empty/numb inside, guilty, ashamed, and embarrassed. At each assessment in which NSSI behavior was endorsed, participants were also asked to rate the extent to which they experienced the same 21 emotions immediately before and immediately after engaging in NSSI. The sum of these items demonstrated good reliability across participants and days of recording in this sample (Rkf = .94).
Using the momentary negative emotion items, we examined the interplay between negative emotion and pain during NSSI in two ways. First, we created an index capturing the instability of negative emotion (summed into one scale) during the course of experience sampling by utilizing the mean squared successive difference (MSSD) equation. 1 We opted to use this index of emotional instability over other standard measures of variability (e.g., standard deviation) because instability indices account for temporally chained, correlated observations by incorporating information on changes in the magnitude of the variable from one recording to the next (Ebner-Priemer, Eid, Kleindienst, Stabenow, & Trull, 2009). For example, an individual with a high standard deviation in momentary negative emotion may experience multiple days with elevated negative emotion that does not deviate. However, this individual would have a low instability index because the individual did not experience significant fluctuations in negative emotion between recordings.
The MSSD equation is displayed in the following:

The MSSD equation takes into account both the amplitude and frequency of a variable (x), which in this case represents the negative emotion rating at each momentary observation, for each individual (i). Differences in emotion ratings from one signal to the next are then squared and summed. The n in the equation refers to the total number of observations per participant. Ultimately, the MSSD generates a single index for fluctuations in negative emotion during the course of experience sampling, and this index was then used to examine the moderation of pain experienced during NSSI to predict frequency of NSSI episodes during the monitoring period.
The second way we examined the interplay between negative emotion and pain during self-injury was at the discrete self-injury episode level. In these analyses, we utilized the negative emotion ratings (again summed into one scale) that participants provided specifically before they engaged in NSSI. We then used negative emotion reported prior to NSSI in moderation of pain levels reported during NSSI to predict number of NSSI episodes during the monitoring period.
Data analytic strategy
First, we examined the descriptive features of NSSI events reported during experience sampling, NSSI and pain reported on the ISAS self-report measure at baseline, and within versus between levels of variance in physical pain reported during monitoring. We then proceeded to test Hypotheses 1 through 4. Because experience sampling data are complex and composed of multiple observations/assessments for each participant, we utilized mixed modeling analyses to test all hypotheses. This approach is essential because most participants reported numerous instances of NSSI and participants provided negative emotion ratings at every momentary assessment. To account for this nonindependence of observations, mixed modeling analyses allow for the specification of a random intercept for each participant, which allows participants to have different starting levels on a variable (e.g., differing initial level of pain). Because we had different hypotheses about the role of pain during self-injury and its interplay with negative emotion, we estimated several different models to test these hypotheses. All predictors and covariates were entered as fixed effects in these models. Because each of these models provided differential evidence for the various study hypotheses (e.g., Hypothesis 2a vs. 2b), we have organized the subsequent results conceptually for ease of interpretation rather than analytically by model.
The first analytic model, which we employed to specifically test Hypotheses 1a, 2a, and 3a, was meant to specifically examine the role of time phases surrounding the various episodes of NSSI (before NSSI, during NSSI, and after NSSI) on pain reported by participants during NSSI. In these models, only episodes in which NSSI was reported were included, and all other observations were excluded. To examine changes in pain that took place during each phase of each individual NSSI episode, we constructed a time index variable that specified level of pain participants reported before NSSI, during NSSI, and after NSSI had concluded. Because this was a mixed model, participants were allowed to have more than one NSSI episode; if the participant reported no NSSI episodes during experience sampling, they were not included in these analyses. Time was then entered as a Level 1 within-subjects predictor (momentary observation level), and levels of time were then contrasted to determine if there were significant changes in pain from one phase to another. The basic equations for this model are displayed in the following: Level 1 (Physical Pain) = β0k + β1k(Time)
jk
+ r
jk
Level 2 (Individual): β0k = β00 β1k = β01.
In this model, we estimated a random intercept (β0k) for individual pain level, a fixed intercept (β00) for average pain level, the contrasted effects of time (β01) on pain level, and residual error (r jk ). Following the examination of main effects for time in the base model, we then examined the analyses with key covariates. Because participants differed in their number of NSSI episodes reported during experience sampling, we controlled for total number of NSSI episodes reported to ensure effects weren’t because of some participants self-injuring more than others. In addition, we controlled for lifetime history of NSSI frequency as determined by the ISAS since it has been theorized that frequent engagement in NSSI may result in habituation to pain and alterations in pain responding (Claes et al., 2006; Glenn et al., 2014; Selby et al., 2010). We also included age, gender, and current medication status as well as their cross-level interactions with time because of their potential influence on NSSI, and all were entered as Level 2 between-subjects covariates (person level). Finally, we also controlled for the day the recording took place to account for day-specific effects and the number of self-injury behaviors that occurred during each NSSI episode, in case the number of behaviors within an NSSI episode influenced pain levels, along with their same-level interaction with time, and these variables were entered as a Level 1 covariates.
The second analytic model was used to examine the predictive role of pain experiences during NSSI episodes to predict the total number of NSSI episodes experienced during monitoring, thus allowing us to test Hypotheses 1b, 2b, 3b, 4a, and 4b. In these models, generalized mixed linear modeling was used to examine total frequency of NSSI episodes across monitoring. Because number of NSSI episodes was a skewed count variable, these analyses utilized a negative binomial distribution with a log link. 2 To examine the relationship between pain onset and pain offset with frequency of NSSI episodes across monitoring, two variables were created to reflect change over time: (a) magnitude of pain increase during NSSI (pain before each NSSI episode was subtracted from pain during the NSSI episode) and (b) pain offset following NSSI (pain during NSSI was subtracted from pain reported after the NSSI episode). For the second analytic model, because the outcome was 2-week monitoring period frequency of NSSI and because of high within- and between-person variability in observation-level pain reporting during experience sampling studies (Schneider et al., 2012; Stone, Broderick, Shiffman, & Schwartz, 2004), the pain onset and offset change variables were aggregated to create average pain changes for each participant based on number of self-injury episodes reported. Participants that did not self-injure during monitoring were not included in these analyses.
We then used these variables in Model 2, the base equations for which are displayed in the following: Response Distribution: NSSI Episodes
k
| μ
k
~ Negative Binomial(μ
k
) Link Function: η
k
= log(μ
k
) Linear Predictor: Level 1 (Momentary Observation): η
k
= β0k + r
jk
Level 2 (Individual): β0k = β00 + β01(Average Pain Onset)
k
+ β02(Average Pain Offset)k.
The response distribution for NSSI episodes was negative binomial, which accounts for the count-nature distribution of total NSSI behaviors per person (μ k ). The link function transforms the outcome of the identity analysis (η k ) with a logarithm transformation such that it is consistent with the negative binomial distribution. Level 1 included a random intercept (β0k) and residual error (r jk ), and Level 2 included a fixed intercept (β00), fixed effects for average pain onset (β01), and average pain offset (β02). After examination of the base model, age, gender, and medication status were then entered as either Level 1 or Level 2 covariates. To test Hypothesis 4a, we then added participant negative emotional instability score (MSSD) as a Level 2 main effect and same-level interaction term with either average pain onset or pain offset in predicting number of NSSI episodes. Furthermore, because different emotional states (e.g., anger, sadness) have been linked to NSSI (Nock et al., 2009; Selby et al., 2013), we then examined exploratory analyses using MSSD indices for the following individual emotion items: embarrassed, angry, sad, overwhelmed, and afraid.
Finally, a third model was used to test Hypotheses 4c and 4d. In this model, we desired to predict the number of NSSI behaviors that occurred during each individual NSSI episode. For this model, we again implemented a generalized mixed linear model with a negative binomial distribution and log link. We then used negative emotion reported prior to NSSI (person-centered) to predict self-injury behaviors during each episode as well as in an interaction with person-centered episode level pain onset and pain offset during NSSI. The model equations were as follows: Response Distribution: NSSI Behaviors/Episode
jk
| μ
jk
~ Negative Binomial(μ
jk
) Link Function: η
jk
= log(μ
jk
) Linear Predictor: Level 1 (Momentary Observation): η
jk
= β0k + β1k(Negative Emotion Before NSSI) + β2k(Episode Pain Onset) + β3k(Episode Pain Offset) + β4k(Negative Emotion Before × Episode Pain Onset) + β5k(Negative Emotion Before × Episode Pain Offset) + r
jk
Level 2 (Individual): β0k = β00 β1k = β01 β2k = β02 β3k = β03 β4k = β04 β5k = β05.
This model allowed for the examination of a random intercept (β0k), a fixed intercept (β00), Level 1 main effect for negative emotion prior to NSSI (β01), NSSI episode pain onset (β02) and episode pain offset (β03), and the observation-level interactions between negative emotion prior to NSSI and pain onset (β04) or pain offset (β05).
All analyses were completed using SPSS statistical software, and there were no concerns with missing data because the Track It! app recorded only initiated entries and mixed modeling techniques are robust to differing frequency of observations for each individual.
Results
Preliminary analyses
At baseline, the average sample mean for lifetime NSSI as measured by the ISAS was 297 instances (SD = 582; range = 8–2,880), indicating this was a highly relevant sample for studying NSSI. There was no attrition of participants during the study, and 84% met criteria for good compliance in completing at least 80% of the signal-contingent assessments that they were prompted to complete during the study. A total of 143 NSSI episodes were reported, and a total of 442 discrete NSSI behaviors were reported during the study. Eighty-five percent of participants reported at least one NSSI episode during the study (range: 0–15), and the average number of NSSI behaviors that occurred during each episode (e.g., number of cuts, burns) was 3.05 (SD = 3.65, range: 1–25). The most frequent methods of NSSI were cutting (40.7%), punching (32.4%), severe scratching (17.9%), burning (9%), and biting (9.7%). Hair pulling and scab picking were assessed and reported during monitoring; however, such behaviors accounted for only 7.6% of NSSI behaviors, and no episodes of self-injury comprised only those behaviors. The modal duration of NSSI episodes was between 1 min and 30 min. During the baseline clinical interviews, 53.2% (n = 25) of participants met criteria for major depressive disorder, and 27.7% (n = 13) met criteria for borderline personality disorder. Additional information on the characteristics of NSSI behavior in this sample can be found in Kranzler et al. (2018).
An initial examination of an intercepts-only mixed linear model for reports of physical pain during experience sampling indicated that there was a significant random intercept variance (b = 1.59, SE = .53, Wald Z = 3.04, p < .01), meaning that individual participants exhibited differing levels of pain depending on the observation. The intraclass correlation (ICC) for all pain ratings was .20, indicating that 20% of the variance in NSSI pain reports was due to between-persons variance and the remaining 80% was due to within-persons variance. When examined independently, the pain ratings had the following ICCs: pre-NSSI pain rating ICC = .26, during-NSSI pain rating ICC = .29, and post-NSSI pain rating ICC= .37. These findings indicated that most of the variance in pain ratings was within individuals; however, there was a somewhat larger proportion of between-person variance for pain ratings after NSSI. Accordingly, NSSI observation-level analyses were conducted with pain onset and offset person-centered. 3
Pain at baseline, pain during self-injury, and pain analgesia
At baseline, 62% of participants reported feeling pain during NSSI often on the ISAS, whereas only 36% felt pain only sometimes, and only 1 participant reported feeling an absence of any pain during NSSI. Regarding the experience sampling data, 28% of all reported NSSI episodes recorded either a zero increase or a decrease in physical pain during NSSI relative to immediately prior to engaging in NSSI. However, many of these no pain episodes were reported by the same participants, with 36% (n = 17) of the total sample reporting experiencing at least one NSSI episode in which no pain increase was felt (or pain decreased during NSSI), but only 3 (6%) participants reported feeling no pain during any episode. Of those 17 participants who had at least one NSSI episode without pain, 8 reported having one such episode, 2 had two episodes, 6 had between three and six episodes, and 1 had nine such episodes. These findings indicate that although the majority of NSSI episodes for most participants were accompanied by at least a minor increase in pain during NSSI, a smaller but noteworthy portion of NSSI episodes were accompanied by pain analgesia—and 16 out of 17 who had at least one episode with no pain onset reported experiencing both pain and pain analgesia during different NSSI episodes.
When combined, those who reported feeling either no pain (n = 1) or pain only sometimes during NSSI (n = 17) on the ISAS at baseline were more likely to report feeling no pain onset during at least one NSSI episode during monitoring (b = 2.69, SE = 0.58, Wald Z = 21.38, p < .001, odds ratio [OR] = 14.77). Thus, Hypothesis 1a was supported in that multiple NSSI episodes and multiple participants reported feeling no pain during actual self-injury episodes, and those who reported having such experiences at baseline were more likely to experience pain analgesia during at least one actual NSSI episode. In further support of Hypothesis 1a, examination of the first mixed linear analytic model in which ISAS report of pain was examined as a moderator of time (before, during, and after NSSI completion) indicated that those who reported experiencing less pain during NSSI on the baseline ISAS were more likely to report actually feeling smaller pain onset during NSSI relative to pain felt before NSSI, b = 7.91, SE = 1.88, t(390) = 4.2, p < .001, d = 0.43. However, there were no differences between participants’ baseline ISAS ratings of pain during NSSI with regard to pain offset after NSSI relative to pain felt during NSSI (p > .05).
Hypothesis 1b was also supported. When examining analytic Model 2, which allowed for the prediction of total NSSI episodes during experience sampling, those who reported no pain during at least one NSSI episode were more likely to report moderately more NSSI episodes overall during monitoring (b = 0.63, SE = 0.22, t = 2.9, p < .01, relative risk ratio [RR] = 1.88). Further, in analytic Model 3, which examined individual NSSI episodes, significantly more NSSI behaviors were reported during episodes in which no pain was felt (b = 0.59, SE = 0.15, t = 4.03, p < .001, RR = 1.80). Finally, an exploratory follow-up analysis tested the notion that lifetime frequency of NSSI may reduce pain during NSSI via habituation (Claes et al., 2006; Glenn et al., 2014; Selby et al., 2010), potentially leading to increased NSSI behavior due to reduced aversive barriers (Franklin, Puzia, Lee, & Prinstein, 2014). Findings from a negative binomial regression indicated that those who reported no pain during at least one NSSI episode over the monitoring reported significantly more lifetime ISAS NSSI episodes (M = 345.21, SD = 518.07; B = 1.24, SE = 0.02, Wald Z = 157.33, p < .001, RR = 3.46) than those who experienced pain during all NSSI episodes (M = 272.68, SD = 583.49). This finding suggests that absence of pain during NSSI may arise as a function of past NSSI behavior and then may further facilitate the behavior, at least for some individuals.
Pain onset during self-injury and pain persistence
Table 1 and Figure 1 display the average level of pain reported by participants across the multiple NSSI episodes that were reported during monitoring. The first mixed linear analytic model, which included time (before, during, and after NSSI) as a predictor of pain level, indicated support for Hypothesis 2a. There was a significant increase in pain during NSSI (M = 4.20, SD = 2.4) relative to before NSSI (M = 1.96, SD = 2.77) such that there was a large effect for pain onset during NSSI, b = 2.26, SE = 0.27, t(390) = 8.01, d = 0.81. Furthermore, there was a significantly persistent increase in pain after NSSI completion (M = 3.37, SD = 2.91) relative to before NSSI such that it was a medium effect size, b = 1.42, SE = 0.28, t(390) = 5.08, p < .001, d = 0.51, suggesting that for many NSSI episodes, pain continued to persist or linger even after NSSI had ceased. Diminished but significant increases in pain during NSSI, b = 13.04, SE = 4.44, t(349) = 2.94, p < .01, d = 0.31, and after NSSI, b = 10.00, SE = 4.45, t(349) = 2.25, p < .05, d = 0.24, relative to before NSSI, were maintained even when covariates, including ISAS lifetime NSSI frequency (p > .05), along with their cross-level interactions with time, were included in the model.
Descriptive Information for Self-Injury Episodes, Pain, and Negative Emotion

Note: NSSI = nonsuicidal self-injury.
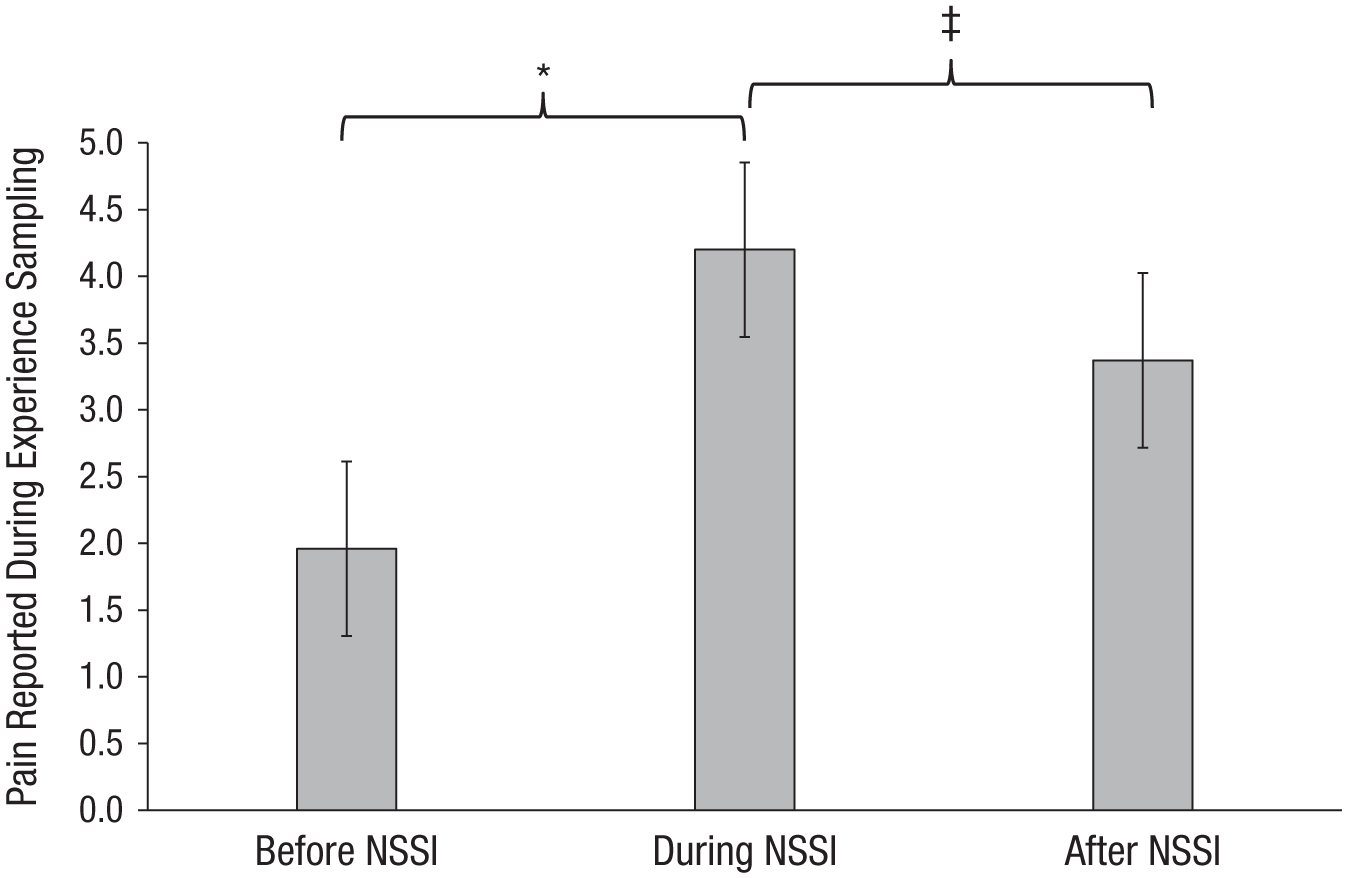
Pain levels before, during, and after self-injury. * indicates p < .01 before and after including covariates. ‡ indicates p < .01 before covariates were entered but a p > .05 after covariates were entered. NSSI = nonsuicidal self-injury.
Pain offset after self-injury
Figure 1 also demonstrates a noticeable decrease in pain after NSSI completion (M = 3.37, SD = 2.91) relative to during NSSI (M = 4.20, SD = 2.4), an effect that, based on the first analytic model, was statistically significant with a small effect size, b = 0.84, SE = .28, t(390) = 3.03, p < .01, d = 0.31, providing support for Hypothesis 3a. However, although there was a small decrease in pain after NSSI completion, pain was still significantly higher than it was before NSSI was initiated, suggesting that pain did not completely offset after NSSI had terminated. Furthermore, when covariates were included in the model, the pain offset effect was diminished and no longer significant, b = 3.02, SE = 4.16, t(349) = .68, p = .49, d = 0.07. Further examination of individual reports of pain from during to after NSSI potentially explained this effect. As displayed in Figure 2, which shows average changes scores for pain before, during, and after NSSI for each self-injuring participant, although a majority of NSSI episodes were characterized by a modest to moderate reduction in pain after NSSI relative to during NSSI, approximately 20% of the sample exhibited average increases in physical pain that continued following NSSI. Thus, a pain-offset effect appears to occur for most people who self-injure, but there may be a subset of those who experience either increased levels of pain or persistent levels of pain even after NSSI ceases.
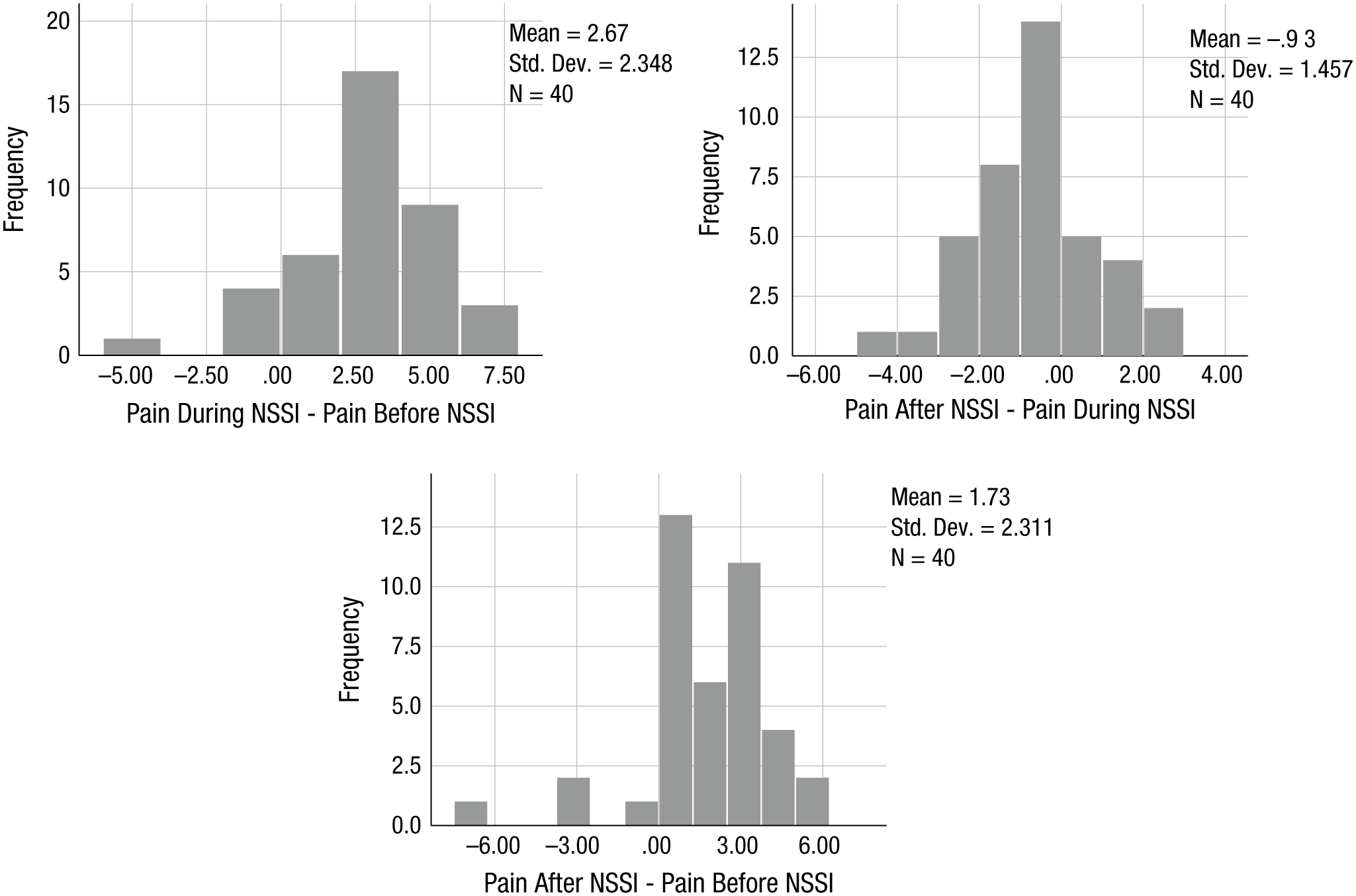
Relative changes in pain before, during, and after self-injury. Average changes in pain across NSSI episodes for each participant from before to during NSSI (During – Before; initial pain onset), during NSSI to after (After – During; pain offset), and from before to after NSSI (After – Before; pain persistence). In these histograms, a positive score represents an increase in pain relative to the previous time point referenced, whereas a negative score represents a decrease in pain. NSSI = nonsuicidal self-injury.
Pain dynamics and self-injury episode frequency across monitoring
To examine the role of magnitude of pain onset and pain offset in predicting frequency of NSSI during experience sampling monitoring, we created two change variables indicating the average increase in pain across all self-injury episodes for each participant as well as the average pain offset for all NSSI episodes per participant. These aggregate measures were utilized because of the high within-person variance in pain onset and offset and to standardize these variables across participants with different NSSI frequency. When these indices of pain onset and pain offset were entered as predictors in generalized linear mixed models, we found that average magnitude of pain onset during NSSI did not significantly predict NSSI episodes (b = −0.05, SE = 0.05, t = 0.93, p > .05), nor did average magnitude of pain offset during NSSI (b = 0.03, SE = 0.08, t = 0.39, p > .05). These findings failed to provide support for Hypotheses 2b and 3b. However, given that the influence of pain onset and offset on total NSSI frequency may be impacted by the negative emotional experience surrounding NSSI behavior, we investigated negative emotional experiences as a moderator of pain experiences during NSSI.
Contextual role of negative emotion with pain and self-injury
To examine the role of negative emotional experience in conjunction with pain experienced during and after NSSI, we examined two mixed models. The first model (the second analytic model) examined emotional instability, or a general tendency toward reactive negative emotional distress, and average pain onset/offset 4 in predicting number of NSSI episodes during monitoring. The interaction between negative emotion instability and average level of pain onset experienced during NSSI was significant in predicting increased frequency of NSSI episodes (b = 0.002, SE = 0.001, t = 2.75, p = .006, RR = 1.002). Further exploration of the interaction term supported Hypothesis 4a in that those participants who demonstrated the most frequent and intense fluctuations in negative emotion during the monitoring period and who experienced the most pain onset during NSSI also reported the most frequent NSSI episodes. These findings were also supported by simple slopes analyses that demonstrated that high negative emotional instability (one standard deviation above the mean) was a significant predictor of more NSSI episodes when more pain onset on average was experienced during NSSI (slope = 0.31, SE = 0.16, t = 2.87, p < .01), and negative emotional instability was also a predictor of NSSI episodes even when low pain onset was experienced (slope = 0.46, SE = 0.09, t = 3.65, p < .001). Findings remained unchanged when including gender, age, lifetime NSSI frequency, and medication status as covariates, and the interaction remained significant (p < .05). With regards to pain offset, the interaction between negative emotion instability and pain offset was not significant in predicting NSSI episodes (b = −0.001, SE = 0.002, t = −0.14, p = .88), failing to provide support for Hypothesis 4b.
Because the role of specific emotions in NSSI has only received limited attention, we conducted exploratory analyses on the interaction between negative emotion instability and average pain onset using instability indices for the following specific subset of emotions: embarrassed, angry, overwhelmed, afraid, and guilty. When these specific emotion instability indices were examined in moderation with average pain onset, only three of the emotions significantly predicted increased NSSI episodes (following the manner of the main interaction): instability of anger (B = 0.03, SE = 0.01, t = 2.42, p < .05, RR = 1.02), instability of sadness (B = 0.09, SE = 0.04, t = 2.49, p < .05, RR = 1.09), and instability of feeling overwhelmed (B = 0.09, SE = 0.03, t = 2.61, p < .05, RR = 1.09).
For the second analysis of negative emotion, we conducted a mixed model examining NSSI at the episode level (analytic Model 3), in which participants’ report of person-centered negative emotion prior to engaging in NSSI moderated person-centered level of pain onset and offset during NSSI episodes in predicting the number of NSSI behaviors during each NSSI episode. In this analysis, we found a significant main effect for negative emotion before NSSI (b = 0.02, SE = 0.006, t = 3.11, p < .01, RR = 1.02), which indicated that experiencing higher levels of negative emotion prior to NSSI predicted more NSSI behaviors during the episode. A significant interaction term was then obtained for negative emotion level before NSSI by average pain onset during NSSI (b = −0.005, SE = 0.002, t = 2.78, p < .01, RR = 0.99). Figure 3 displays the interaction term and demonstrates that those who experienced increased negative emotion prior to NSSI but felt less pain onset during the NSSI episode reported significantly more NSSI behaviors, which supported Hypothesis 4c. Further examination with simple slopes analyses indicated that high levels of negative emotion before NSSI (by one standard deviation) were predictive of increased number of self-injurious behaviors during episodes when low pain onset was observed (slope = −0.72, SE = 0.16, t = −4.49, p < .001) but not when high pain onset was observed (slope = 0.01, SE = 0.005, t = 1.25, p = .21). In contrast, Hypothesis 4d was not supported since level of pain offset during NSSI did not interact with level of negative emotion prior to NSSI in predicting number of NSSI behaviors during each episode (b = 0.02, SE = 0.004, t = 0.37, p > .05).

Negative emotion and number of self-injury behaviors occurring during self-injury episodes with low pain. * indicates significant simple slopes (p < .001). Increased negative emotion prior to NSSI interacted with a decreased magnitude of pain onset during NSSI episodes to predict an increased number of NSSI behaviors during NSSI episodes. NE = negative emotion; NSSI = nonsuicidal self-injury.
To build on Hypothesis 4c, a follow-up analysis was conducted using analytic Model 3 to test whether NSSI episodes in which no pain was felt tended to be characterized by more NSSI behaviors. The interaction term was significant (b = 0.02, SE = 0.007, t = 2.59, p < .05, RR = 1.02) such that those who had elevated negative emotion before NSSI and felt no pain during that episode tended to report more NSSI behaviors during the episode. This finding was also supported by simple slopes analyses that indicated higher negative emotion (one standard deviation above) was predictive of more NSSI behaviors for those who endorsed no pain during an episode (slope = 2.75, SE = 0.51, t = 5.40, p < .001) as well as for those who endorsed pain during NSSI (slope = 1.25, SE = 0.27, t = 4.56, p < .001).
Discussion
The present study provides one of the most in-depth and ecologically valid examinations of the nature of physical pain in NSSI that has been conducted to date. Overall, support was found for pain analgesia during some NSSI episodes, substantial pain onset during most NSSI episodes, and modest to moderate pain offset during most NSSI episodes. These findings suggest that the role of pain during NSSI is complex and multifaceted and can be most accurately understood by considering these differing pain models of NSSI as coexisting and complementary rather than competing. Given the multiple findings relevant to the three differing models of pain experience during NSSI, we summarize the primary findings relevant to each theoretical model in the following.
Pain analgesia during NSSI
Substantial support was found for Hypotheses 1a and 1b. Multiple participants reported multiple NSSI episodes in which they felt no pain, and those reporting no pain during NSSI at baseline were more likely to report at least one NSSI episode in which pain did not increase (OR = 14.77), whereas those reporting feeling less pain during NSSI at baseline were more likely to report feeling less pain across NSSI episodes. Furthermore, those who felt no pain during at least one NSSI episode reported more NSSI episodes overall and more NSSI behaviors during those episodes, and a follow-up analysis indicated that when NSSI episodes without pain onset were preceded by elevations in negative emotion, even more NSSI behaviors were reported during the episode.
These findings are important because they demonstrate that for at least a subset of self-injurers, pain analgesia occurs and may be contributing to the frequency of the behavior. Whereas the pain onset and pain offset models both suggest that the experience of pain during NSSI serves an emotion regulatory function, the pain analgesia model in contrast posits that for some self-injurers and in some instances, these classically painful behaviors may not actually elicit much or any pain. This has important clinical implications because for this subset of self-injurers, the absence of pain may lead them to more severe NSSI and to be less motivated to engage in interventions designed to reduce the behavior.
To date, the reasons that some self-injurers experience pain analgesia remain unclear. According to the habituation hypothesis (Glenn et al., 2014), one possibility may be that individuals who engage in NSSI habituate to pain over time with repeated exposure, thereby altering their pain sensitivity through recurrent exposure to pain. Consistent with this possibility, in the current study, those who felt no pain during at least one episode tended to report more frequent NSSI during the study (RR = 1.88) as well as higher lifetime NSSI (RR = 3.5). However, the direction of this effect is difficult to establish, and it could alternatively be that feeling less or no pain makes one more prone to NSSI episodes. Another possible mechanism may be through endogenous opioids or endorphins, which are released following NSSI behaviors and may reduce experiences of pain and elicit feelings of euphoria (Van Ree et al., 2000). Individuals who engage in NSSI may have higher levels of endorphins, or NSSI may increase baseline levels of endorphins, resulting in this decreased pain sensitivity. Research examining this mechanism, however, has been inconsistent. Thus, further research is needed exploring the mechanisms of pain analgesia and clarifying why it may occur for some self-injurers and in some episodes of NSSI and not in others.
Pain onset during and after NSSI
Hypotheses 2a, 4a, and 4c were all supported (but not 2b), providing substantial evidence for pain onset effects during NSSI. Most participants who self-injured during the study experienced at least some pain during the episode, and many continued to feel pain, or even an increase in pain, after NSSI was over. Furthermore, participants characterized by high negative emotional instability using the MSSD index and who felt more pain on average during NSSI were more likely to report more NSSI episodes during monitoring. In particular, instability in anger, sadness, and feeling overwhelmed specifically interacted with average pain onset to predict increased self-injury frequency, consistent with other studies that have identified anger (Nock et al., 2009) and sadness (Selby et al., 2013) as key predictors of NSSI. Finally, participants who felt less pain onset during an NSSI episode and expressed elevated negative emotion prior to the episode reported more self-injurious behaviors during such episodes.
The findings for pain onset suggest that for many who self-injure and for many of their NSSI episodes, pain is a common outcome and the role of pain is moderated by negative emotional instability. Indeed, those with more negative emotional instability who felt more pain onset during NSSI were more likely to self-injure more frequently, suggesting that pain may negatively reinforce NSSI by regulating elevated emotional distress. This finding is consistent with emotion regulation pain onset models of NSSI (Chapman et al., 2006; Selby, Anestis, & Joiner, 2008). However, there was no main effect of pain onset in predicting NSSI frequency, suggesting that the presence of pain may only negatively reinforce NSSI in the presence of negative emotional instability. This finding makes conceptual sense and suggests that physical pain may only be reinforcing in the context of increased demands for emotion regulation, supporting the role of pain as a form of emotion regulation.
However, though findings from this study are consistent with previous research demonstrating that NSSI often results in significant reductions in negative emotion (Kranzler et al., 2018), it remains unclear how pain experienced during NSSI may serve this emotion regulation function. Existing theories posit that pain may have a cognitive impact, functioning as a potent distraction from rumination or emotional cascades (Selby et al., 2013), or may have an impact on the biological level, resulting in a biological change in emotional experience (Franklin et al., 2010). This is a critical question for future research to continue to investigate.
Considering our Hypothesis 4c findings, that those who experienced less pain onset during NSSI tended to engage in more NSSI behaviors during episodes that were preceded by elevated negative emotion, it is not evident why more NSSI behaviors were needed in this emotional context. Presumably, if pain experienced during NSSI serves to distract from emotional distress, then feeling less pain from NSSI may lead an individual to engage in more subsequent NSSI behaviors during the episode in an attempt to elicit more pain. However, as discussed in the pain analgesia model, it may also be true that feeling less pain enabled the individual to self-injure more during the episode. Unfortunately, neither of these potential hypotheses could be tested with the present methods, but they may serve as important future directions for elaborating on why people might self-injure more during an episode in which they felt less or no pain, particularly in the context of elevated negative emotion.
Pain offset following NSSI
Initial support was found for Hypothesis 3a, indicating that many participants also experienced pain offset following NSSI. However, a small effect size was found for this effect, and it was no longer significant after controlling for key covariates. We suspect that this might have been a function of some participants experiencing either no pain offset or an unexpected pain increase following NSSI. Future research should explore why some participants don’t experience pain offset after NSSI and why still others report experiencing even more pain after NSSI has ceased. It is possible that endogenous opioid effects mask the experience of pain during NSSI but wear off for some shortly after, leading to an increased perception of pain.
Although we found initial support for Hypothesis 3a, we did not find support for Hypotheses 3b, 4b, or 4d in that magnitude of pain offset during NSSI did not significantly predict frequency of NSSI episodes, even in the context of emotional instability, and it did not predict more behaviors during individual NSSI episodes that were preceded by elevated negative emotion. These findings did not provide evidence in support of a positive reinforcement effect for NSSI that arises from pain offset. Therefore, it is unclear if and to what extent pain offset is reinforcing of NSSI behavior. However, it is likely that the current study did not measure pain offset in a way that would provide the best test of the process. First, pain offset is difficult to measure with NSSI since after the behavior is concluded, a real physical injury continues to exist (in most cases), which may reduce the pain offset reinforcement. Second, the reinforcing effects of pain offset may be very short-lived, occurring immediately at cessation of self-injury and then fading. Previous work on pain offset relief has utilized psychophysiological indices (Franklin, Lee, et al., 2013; Franklin, Puzia, et al., 2013), which may tap such experience in a more nuanced way than experience sampling is currently capable of. Such methods may be able to demonstrate that physiological indices of reward processing increase in synchrony with pain offset reported following NSSI. Furthermore, previous experience sampling research has found that participants report significant increases in positive emotion following NSSI, particularly for feelings such as “relief” (e.g., Kranzler et al., 2018), which are likely influenced by pain offset. Thus, further research should continue to study the construct of pain offset relief following NSSI to further tease apart whether participants are experiencing emotional relief, physical relief, or a combination of both.
Strengths, limitations, and future directions
There are several substantial strengths to the current study. We obtained data from a clinically relevant, diverse, actively self-injuring sample of adolescents and young adults using experience sampling methodology, which is time- and resource-intensive. Over 400 NSSI behaviors across 143 NSSI episodes occurring in real time were reported during this study, which is among the first to analyze NSSI at the inter- and intra-episode level. Furthermore, we used intensive, fine-grained analytic modeling to tease apart complex and nuanced experiences of pain during NSSI and examine how such experiences relate to the overall psychopathology of NSSI. The findings also have substantial clinical relevance, particularly with regard to replacing self-injurious pain as a “distraction” from negative emotion. Future clinical treatments may benefit from alternative mental distractions to negative emotion (e.g., mindfulness) or even from alternative benign sensory distractors to replace self-injury (e.g., massaging, tactile sensations).
Although there were numerous strengths to the current study, there are also limitations to experience sampling methodology and therefore related limitations to the conclusions we can draw from these data. First, pain was subjectively assessed, and there is some evidence that retrospective self-report of pain by participants can be unreliable (Gendreau, Hufford, & Stone, 2003) and demonstrate substantial within- and between-person variance (Schneider et al., 2012; Stone et al., 2004). However, the use of experience sampling is thought to be one of the best ways to reduce recall bias in self-reports of pain (Gendreau et al., 2003), and in this study, having participants estimate their “pain before” NSSI may also have ameliorated this issue to some extent by allowing for comparisons of subjective ratings of pain during and after NSSI relative to this initial anchor. Even so, there is a subjective nature to reporting of pain, and within-person variability in pain may be high because of potential differences in localized (finger, spot on skin) versus generalized pain (stomach, back), physical illness, hunger, and fatigue and difficulty for participants with anchoring pain across observations (Stone et al., 2004). Future research on pain experienced during NSSI should include examination of observation-level pain reporting versus aggregate-level pain reporting and person versus grand mean centering of pain reports. Future experience sampling studies may also benefit from objective measurement of indices related to pain, such as psychophysiological indices, or facial observations assessments of pain obtained through home video assessment (Cohn, Ambadar, & Ekman, 2007).
Second, although the real-time nature of the data collection may increase accuracy and ecological validity, findings from this study are still self-report in nature and nonexperimental, and thus causal relationships cannot be concluded. Future research should incorporate more longitudinal methods, such as by collecting experience sampling data for 2 weeks and then using those data to predict NSSI during a later monitoring period. The current study also allowed a longer response window for participants to respond after being signaled (1 hr) than in other studies. This was done to increase response completion, especially after NSSI episodes, which can be variable in duration, but future studies should examine NSSI with tighter response windows after signaling to ensure further ecological validity.
Third, although this is one of the most intensive experience sampling studies of NSSI conducted to date, low power may still affect our findings. Our sample size was unlikely large enough to detect some between-participant effects, and this may have contributed to some nonsignificant analyses in the prediction of total NSSI episodes over monitoring. Similarly, although we obtained information on a substantial number of NSSI episodes and total behaviors, future research should attempt to recruit larger samples and obtain more data from more NSSI episodes to replicate these findings and provide a more powerful test for the pain offset hypotheses that were not supported.
Finally, although we were able to evaluate individual episodes of NSSI and look at differences in behavioral responses during each of those episodes, we were only able to obtain levels of pain and negative emotion rated for the whole episode (before, during, and after) but not for each individual NSSI behavior during the full NSSI episode (which often had multiple behaviors). Future research should also strive to replicate and build on the findings of this study at the individual NSSI behavior level within an episode, potentially examining multiple pain recordings for each behavior that occurs during an episode.
Conclusion
Findings from this study suggest that there is no single universal experience of pain during NSSI. Instead, pain is experienced in multiple different ways and may serve multiple different functions for self-injurers. Some may feel intense pain while engaging in NSSI, others none at all. Researchers and clinicians alike are therefore best served by understanding the plurality of experiences of pain that are possible with NSSI. A better understanding of the complex way these different experiences of pain interact in reinforcing the behavior and the way pain is influenced by and in turn influences the negative emotional context surrounding the behavior is needed to further enhance our current treatments for this complex and understudied behavior.
Footnotes
Acknowledgements
Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the National Science Foundation or the American Psychological Association.
Action Editor
Christopher G. Beevers served as action editor for this article.
Author Contributions
E. A. Selby, A. Kranzler, and K. B. Fehling conceptualized and oversaw study data collection, data analysis, and manuscript preparation. J. Brillante, F. Yuan, and X. Gao contributed to data collection, smartphone app creation, and assistance with data analysis and manuscript preparation. J. Lindqvist oversaw smart app creation and contributed to study conceptualization and manuscript preparation. A. L. Miller contributed to study data collection and manuscript preparation. All the authors approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
Funding
This work was supported by National Science Foundation Grant No. 1211079 (PI: J. Lindqvist) and a Dissertation Research Award from the American Psychological Association (A. Kranzler).